Tenerife 1977 Crash: Fault Tree Analysis and Lessons Learned
VerifiedAdded on 2023/06/15
|10
|2868
|417
Case Study
AI Summary
This case study examines the catastrophic Tenerife Airport disaster of 1977, where a collision between two Boeing 747s, KLM flight 4805 and Pan Am flight, resulted in 583 fatalities, marking it as the deadliest aviation accident in history. The report details the circumstances leading to the disaster, including the diversion of flights due to a bomb threat at Gran Canaria Airport, communication failures between air traffic control and the flight crews, and adverse weather conditions that reduced visibility. A fault tree analysis identifies the various failures and human factors that contributed to the catastrophe. Furthermore, the case study draws parallels with similar incidents, such as the 1990 Detroit Metropolitan Airport collision, and emphasizes the importance of Crew Resource Management (CRM) and Project Resource Management to mitigate human error and improve overall safety in aviation. The analysis concludes with recommendations to prevent similar disasters, focusing on enhanced communication protocols, improved training programs, and better coordination among all stakeholders involved in air traffic control and flight operations. Desklib offers additional resources, including past papers and solved assignments, to aid in further understanding of aviation safety and risk management.

Running head: TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Tenerife 1977 crash with Fault Tree Analysis
Name of student
Name of University
Author’s Note
Tenerife 1977 crash with Fault Tree Analysis
Name of student
Name of University
Author’s Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Table of Contents
Introduction..................................................................................................................................................2
Describe Tenerife system and its working environment.............................................................................2
Catastrophic failure of Tenerife and its effect.............................................................................................3
Failures and their causes to the catastrophe.................................................................................................4
Catastrophic events Similar to Tenerife Disaster........................................................................................6
Recommendation of Tenerife disaster occur and to manage such issue raised...........................................7
Conclusion...................................................................................................................................................7
References....................................................................................................................................................8
Table of Contents
Introduction..................................................................................................................................................2
Describe Tenerife system and its working environment.............................................................................2
Catastrophic failure of Tenerife and its effect.............................................................................................3
Failures and their causes to the catastrophe.................................................................................................4
Catastrophic events Similar to Tenerife Disaster........................................................................................6
Recommendation of Tenerife disaster occur and to manage such issue raised...........................................7
Conclusion...................................................................................................................................................7
References....................................................................................................................................................8
2TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Introduction
The large scale disaster are the actual cost of separation of small events and this become
amplified and linked in such a way that are unpredictable and incomprehensible. The
amplification and linkage of such scenario are less linear and more tightly coupled. With any
discussion of the processes, crises are set in motion. The main purpose of this report is to
describe the Tenerife system and the working environment. This report provides catastrophic
failure of Tenerife and the effect it has in the surrounding environment. It describes the failure
and the causes contributed to the catastrophe. Moreover, the report covers similar catastrophic
events that have previously taken place. Finally, it will conclude recommending the top events
that were stop from recurring which will discuss the issues that were raised.
Describe Tenerife system and its working environment
The Tenerife disaster was worst accident in the history of aviation that happened in 1977
and it was hazardous situation that impacted large number of people. The Tenerife disaster was
severe affecting many lives. The disastrous event happened on island of Tenerife. The incident
happened due to collision between KLM flight 4805 and Pan Am flight which was passenger jets
of Boeing 747 (Roudet, Thurat and Turcot 2016). The incident happened due to the diversion of
both flights in the same direction as the expected destination was closed because of bomb blast.
The Tenerife disaster was due to misunderstanding in communication among the controllers of
the aircraft. The Tenerife was not a major platform and the landing of two aircrafts was not
possible. The Pan Am flight was expected to park behind the KLM plane flight. The KLM plane
flight after waiting some time made 180 degree turn reporting that they are now at takeoff to the
controllers of Pan Am flight. However, the controllers of Pan AM flight and airport crew did not
understand the reporting of KLM plane flight. This was the major miscommunication that
happened and between the controllers and crew members which resulted in the collision. The
event existed for 13 seconds and as per report 583 people died in this disastrous event (Aren’t
Indicated and Boyd 2016). The number of deaths in KLM flight was 234 passengers and 14 crew
members (Wong 2017). The number of deaths in Pan Am flight was 319 including passengers
and crew members. This resulted in closing of the airport for two days in Tenerife in the year
1977. Single cause incidents are rare, but when small incidents are chained together that results
to disastrous outcome. People must be able to diagnose a problem rather than being detected any
potential problem before it emerges, people wait for the crisis to occur before diagnosing the
problem. Disaster is to anticipate and understand the regularities in small events to have large
effects. The process induced the Tenerife air disaster were 583 people killed in the incident
(Bucher, Jäger and Cardoza 2018).
The working environment of Tenerife system in this disastrous situation was stressful.
The Tenerife people were taxed and labeled as threatening event. There was pressure on KLM
flight crew from three sources and they were Dutch law, unpredictable weather and maneuvers,
Introduction
The large scale disaster are the actual cost of separation of small events and this become
amplified and linked in such a way that are unpredictable and incomprehensible. The
amplification and linkage of such scenario are less linear and more tightly coupled. With any
discussion of the processes, crises are set in motion. The main purpose of this report is to
describe the Tenerife system and the working environment. This report provides catastrophic
failure of Tenerife and the effect it has in the surrounding environment. It describes the failure
and the causes contributed to the catastrophe. Moreover, the report covers similar catastrophic
events that have previously taken place. Finally, it will conclude recommending the top events
that were stop from recurring which will discuss the issues that were raised.
Describe Tenerife system and its working environment
The Tenerife disaster was worst accident in the history of aviation that happened in 1977
and it was hazardous situation that impacted large number of people. The Tenerife disaster was
severe affecting many lives. The disastrous event happened on island of Tenerife. The incident
happened due to collision between KLM flight 4805 and Pan Am flight which was passenger jets
of Boeing 747 (Roudet, Thurat and Turcot 2016). The incident happened due to the diversion of
both flights in the same direction as the expected destination was closed because of bomb blast.
The Tenerife disaster was due to misunderstanding in communication among the controllers of
the aircraft. The Tenerife was not a major platform and the landing of two aircrafts was not
possible. The Pan Am flight was expected to park behind the KLM plane flight. The KLM plane
flight after waiting some time made 180 degree turn reporting that they are now at takeoff to the
controllers of Pan Am flight. However, the controllers of Pan AM flight and airport crew did not
understand the reporting of KLM plane flight. This was the major miscommunication that
happened and between the controllers and crew members which resulted in the collision. The
event existed for 13 seconds and as per report 583 people died in this disastrous event (Aren’t
Indicated and Boyd 2016). The number of deaths in KLM flight was 234 passengers and 14 crew
members (Wong 2017). The number of deaths in Pan Am flight was 319 including passengers
and crew members. This resulted in closing of the airport for two days in Tenerife in the year
1977. Single cause incidents are rare, but when small incidents are chained together that results
to disastrous outcome. People must be able to diagnose a problem rather than being detected any
potential problem before it emerges, people wait for the crisis to occur before diagnosing the
problem. Disaster is to anticipate and understand the regularities in small events to have large
effects. The process induced the Tenerife air disaster were 583 people killed in the incident
(Bucher, Jäger and Cardoza 2018).
The working environment of Tenerife system in this disastrous situation was stressful.
The Tenerife people were taxed and labeled as threatening event. There was pressure on KLM
flight crew from three sources and they were Dutch law, unpredictable weather and maneuvers,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
which were difficult. The actions taken by the authority at the time of the disaster were that
certain changes were made to the rules and regulations of airport. The reporting phrases were
changed after this incident occurred. The procedures of Cockpit were also changed to emphasis
more on mutual agreement of decisions among the crew members (Ogliastri and Zúñiga 2016).
Hence, the airport incident was carefully handled.
The First concept was the temporary system concept that seems to be resuscitating as task
forces, project teams and aircrews are doing plentiful and consequential work. The second
concept was to make the stress more precise. This concept blends the anxiety, emotion, pressure,
arousal, and strain together. Third is the accuracy and cohesion in a group. Fourth is to restudy
the pluralistic ignorance that has applied to an incipient crisis. Fifth is that the context of pre-
crisis become more complex and tightly coupled. In this case, failure occurs often because of the
complexity and farther it spread more quickly because of such tight coupling. Sixth is to check
whether complexity of the task decreases with the improvement in the group interaction. Finally,
need to see the increase in stress level of the formal structure and relation with the authority.
Catastrophic failure of Tenerife and its effect
The catastrophic failures of Tenerife disaster are discussed as follows. The failure of
Tenerife was that both flights had been routinely departed and were routinely approaching on the
island (López et al. 2015). The news of bomb explosion was reported to the Gran Canaria
International Airport authority. This news was followed by the news of second bomb planted at
the airport terminals. Thus, the authorities closed the airport terminals temporarily to avoid any
complications. The airport authority diverted the incoming plane flights (Cowlagi and Saleh
2015). The airport is built in small areas and therefore it was not possible for all the flights to
accommodate in the airport. The space of taxiway was used for landing of flights (Hubbard et al.
2015). The airport authority then reopened the airport terminal to depart the Pan Am flight
however KLM plane flight obstructed the access of Pan Am flight. The KLM flight was
instructed to make a 180 degree turn and this is the situation where the miscommunication
occurred. The KLM flight then collided with the Pan Am flight which was behind the KLM
flight. This was the situation were KLM flight and Pan Am flight collided and caused the major
destruction to hundreds of people. The weather condition was also one of the factors which
contributed to the collision of the two flights (Hernandez, Guimarães Pereira and Barbosa 2018).
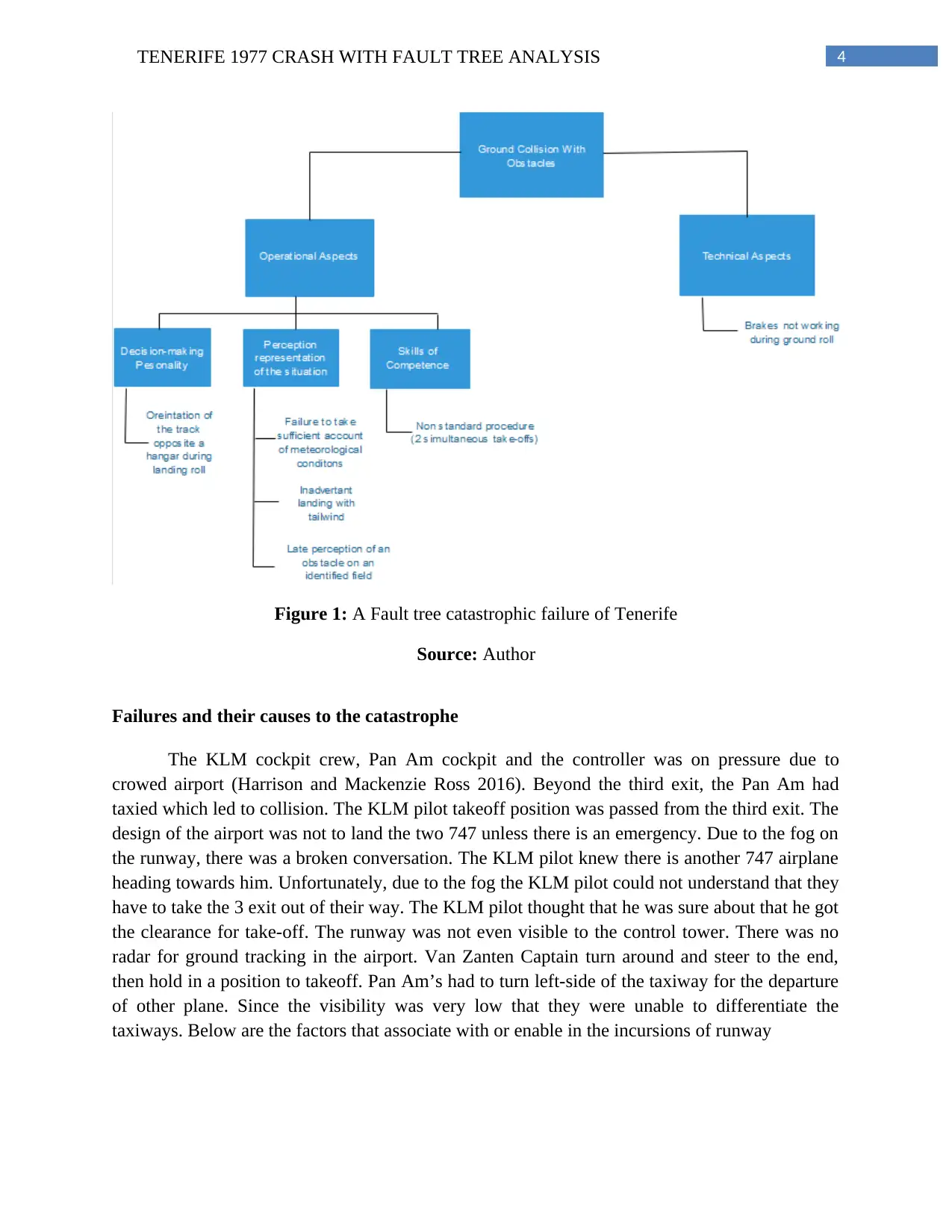
The weather condition unhindered the visibility of the controllers of the flight. The figure below
shows the fault tree analysis of the ground collision and the catastrophic failure of Tenerife,
which were difficult. The actions taken by the authority at the time of the disaster were that
certain changes were made to the rules and regulations of airport. The reporting phrases were
changed after this incident occurred. The procedures of Cockpit were also changed to emphasis
more on mutual agreement of decisions among the crew members (Ogliastri and Zúñiga 2016).
Hence, the airport incident was carefully handled.
The First concept was the temporary system concept that seems to be resuscitating as task
forces, project teams and aircrews are doing plentiful and consequential work. The second
concept was to make the stress more precise. This concept blends the anxiety, emotion, pressure,
arousal, and strain together. Third is the accuracy and cohesion in a group. Fourth is to restudy
the pluralistic ignorance that has applied to an incipient crisis. Fifth is that the context of pre-
crisis become more complex and tightly coupled. In this case, failure occurs often because of the
complexity and farther it spread more quickly because of such tight coupling. Sixth is to check
whether complexity of the task decreases with the improvement in the group interaction. Finally,
need to see the increase in stress level of the formal structure and relation with the authority.
Catastrophic failure of Tenerife and its effect
The catastrophic failures of Tenerife disaster are discussed as follows. The failure of
Tenerife was that both flights had been routinely departed and were routinely approaching on the
island (López et al. 2015). The news of bomb explosion was reported to the Gran Canaria
International Airport authority. This news was followed by the news of second bomb planted at
the airport terminals. Thus, the authorities closed the airport terminals temporarily to avoid any
complications. The airport authority diverted the incoming plane flights (Cowlagi and Saleh
2015). The airport is built in small areas and therefore it was not possible for all the flights to
accommodate in the airport. The space of taxiway was used for landing of flights (Hubbard et al.
2015). The airport authority then reopened the airport terminal to depart the Pan Am flight
however KLM plane flight obstructed the access of Pan Am flight. The KLM flight was
instructed to make a 180 degree turn and this is the situation where the miscommunication
occurred. The KLM flight then collided with the Pan Am flight which was behind the KLM
flight. This was the situation were KLM flight and Pan Am flight collided and caused the major
destruction to hundreds of people. The weather condition was also one of the factors which
contributed to the collision of the two flights (Hernandez, Guimarães Pereira and Barbosa 2018).
The weather condition unhindered the visibility of the controllers of the flight. The figure below
shows the fault tree analysis of the ground collision and the catastrophic failure of Tenerife,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Figure 1: A Fault tree catastrophic failure of Tenerife
Source: Author
Failures and their causes to the catastrophe
The KLM cockpit crew, Pan Am cockpit and the controller was on pressure due to
crowed airport (Harrison and Mackenzie Ross 2016). Beyond the third exit, the Pan Am had
taxied which led to collision. The KLM pilot takeoff position was passed from the third exit. The
design of the airport was not to land the two 747 unless there is an emergency. Due to the fog on
the runway, there was a broken conversation. The KLM pilot knew there is another 747 airplane
heading towards him. Unfortunately, due to the fog the KLM pilot could not understand that they
have to take the 3 exit out of their way. The KLM pilot thought that he was sure about that he got
the clearance for take-off. The runway was not even visible to the control tower. There was no
radar for ground tracking in the airport. Van Zanten Captain turn around and steer to the end,
then hold in a position to takeoff. Pan Am’s had to turn left-side of the taxiway for the departure
of other plane. Since the visibility was very low that they were unable to differentiate the
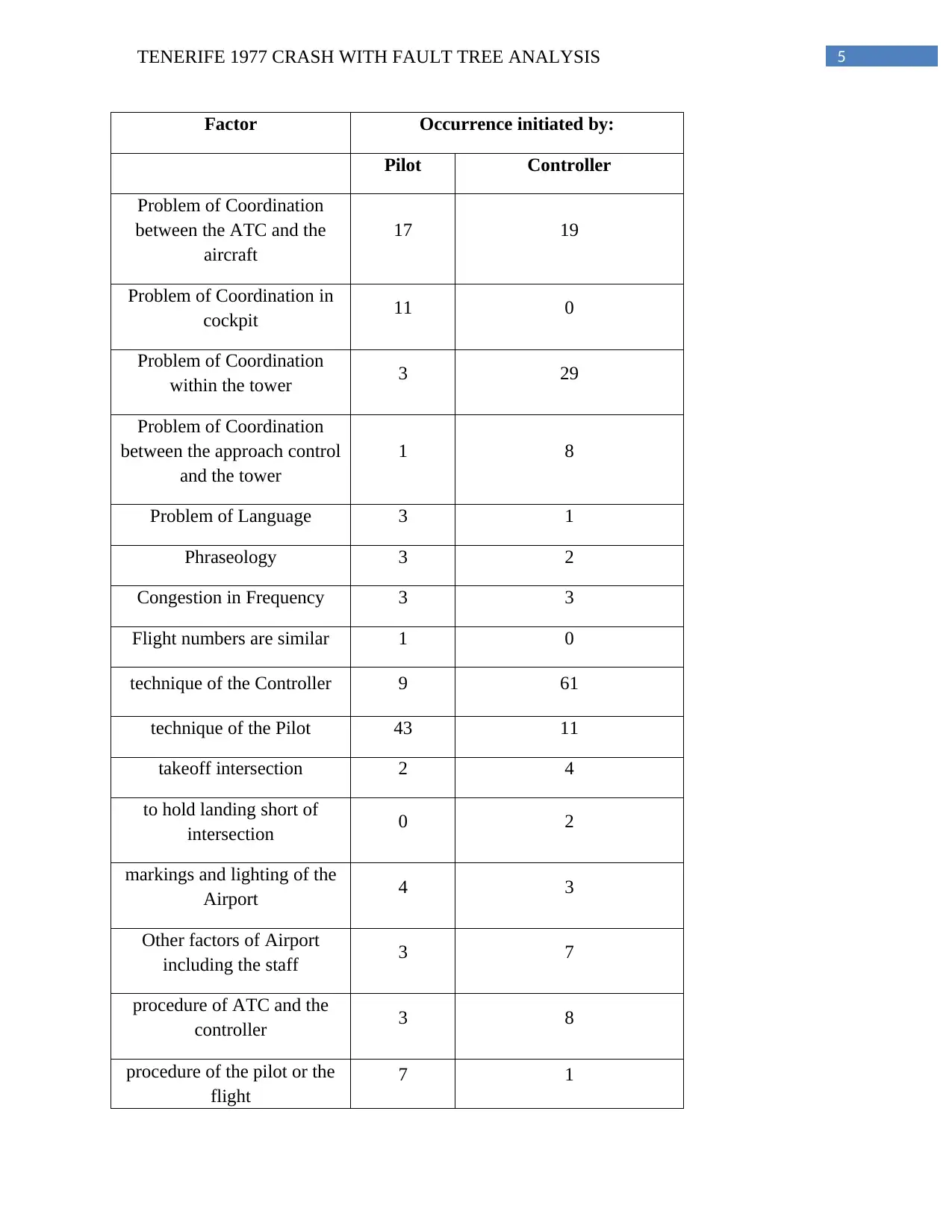
taxiways. Below are the factors that associate with or enable in the incursions of runway
Figure 1: A Fault tree catastrophic failure of Tenerife
Source: Author
Failures and their causes to the catastrophe
The KLM cockpit crew, Pan Am cockpit and the controller was on pressure due to
crowed airport (Harrison and Mackenzie Ross 2016). Beyond the third exit, the Pan Am had
taxied which led to collision. The KLM pilot takeoff position was passed from the third exit. The
design of the airport was not to land the two 747 unless there is an emergency. Due to the fog on
the runway, there was a broken conversation. The KLM pilot knew there is another 747 airplane
heading towards him. Unfortunately, due to the fog the KLM pilot could not understand that they
have to take the 3 exit out of their way. The KLM pilot thought that he was sure about that he got
the clearance for take-off. The runway was not even visible to the control tower. There was no
radar for ground tracking in the airport. Van Zanten Captain turn around and steer to the end,
then hold in a position to takeoff. Pan Am’s had to turn left-side of the taxiway for the departure
of other plane. Since the visibility was very low that they were unable to differentiate the
taxiways. Below are the factors that associate with or enable in the incursions of runway
5TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Factor Occurrence initiated by:
Pilot Controller
Problem of Coordination
between the ATC and the
aircraft
17 19
Problem of Coordination in
cockpit 11 0
Problem of Coordination
within the tower 3 29
Problem of Coordination
between the approach control
and the tower
1 8
Problem of Language 3 1
Phraseology 3 2
Congestion in Frequency 3 3
Flight numbers are similar 1 0
technique of the Controller 9 61
technique of the Pilot 43 11
takeoff intersection 2 4
to hold landing short of
intersection 0 2
markings and lighting of the
Airport 4 3
Other factors of Airport
including the staff 3 7
procedure of ATC and the
controller 3 8
procedure of the pilot or the
flight
7 1
Factor Occurrence initiated by:
Pilot Controller
Problem of Coordination
between the ATC and the
aircraft
17 19
Problem of Coordination in
cockpit 11 0
Problem of Coordination
within the tower 3 29
Problem of Coordination
between the approach control
and the tower
1 8
Problem of Language 3 1
Phraseology 3 2
Congestion in Frequency 3 3
Flight numbers are similar 1 0
technique of the Controller 9 61
technique of the Pilot 43 11
takeoff intersection 2 4
to hold landing short of
intersection 0 2
markings and lighting of the
Airport 4 3
Other factors of Airport
including the staff 3 7
procedure of ATC and the
controller 3 8
procedure of the pilot or the
flight
7 1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
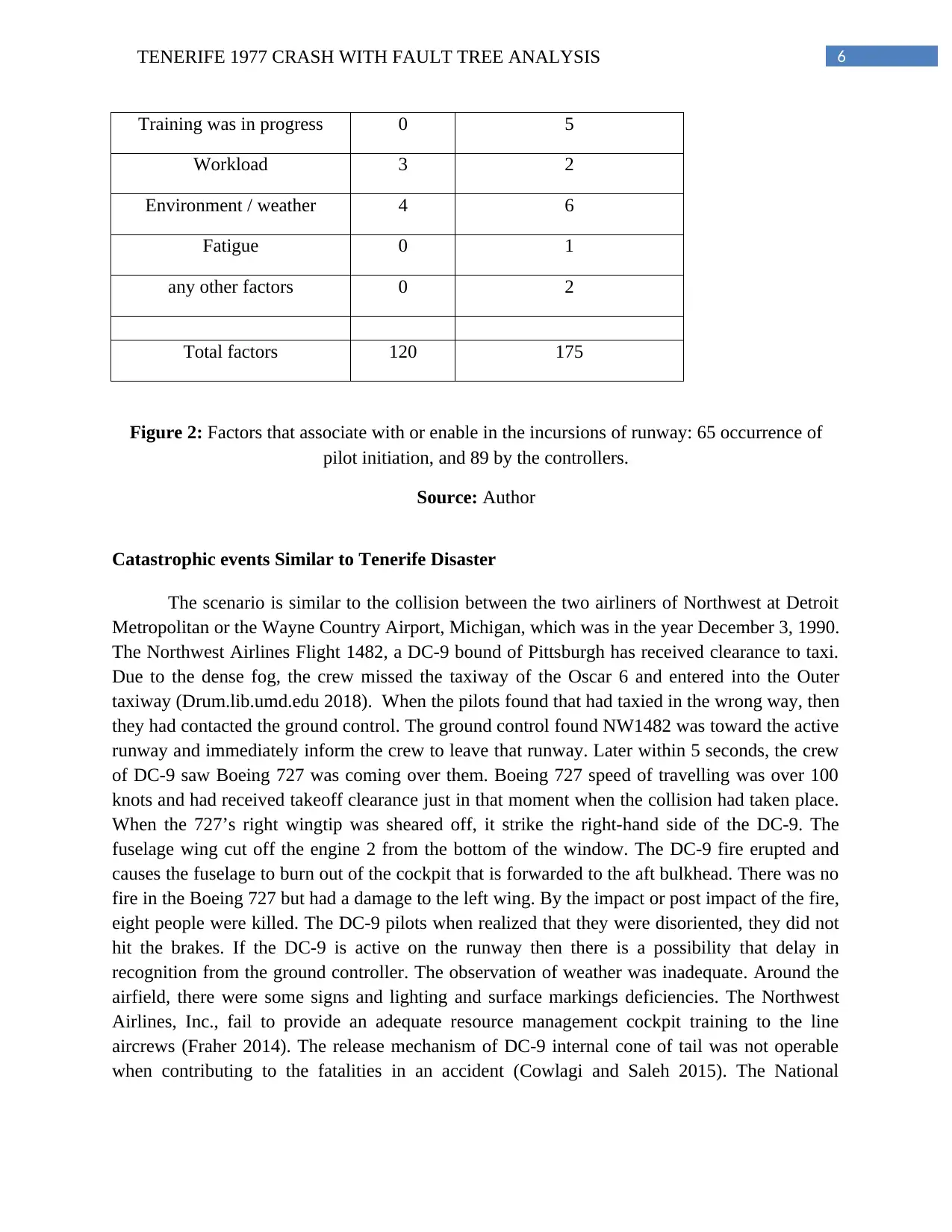
Training was in progress 0 5
Workload 3 2
Environment / weather 4 6
Fatigue 0 1
any other factors 0 2
Total factors 120 175
Figure 2: Factors that associate with or enable in the incursions of runway: 65 occurrence of
pilot initiation, and 89 by the controllers.
Source: Author
Catastrophic events Similar to Tenerife Disaster
The scenario is similar to the collision between the two airliners of Northwest at Detroit
Metropolitan or the Wayne Country Airport, Michigan, which was in the year December 3, 1990.
The Northwest Airlines Flight 1482, a DC-9 bound of Pittsburgh has received clearance to taxi.
Due to the dense fog, the crew missed the taxiway of the Oscar 6 and entered into the Outer
taxiway (Drum.lib.umd.edu 2018). When the pilots found that had taxied in the wrong way, then
they had contacted the ground control. The ground control found NW1482 was toward the active
runway and immediately inform the crew to leave that runway. Later within 5 seconds, the crew
of DC-9 saw Boeing 727 was coming over them. Boeing 727 speed of travelling was over 100
knots and had received takeoff clearance just in that moment when the collision had taken place.
When the 727’s right wingtip was sheared off, it strike the right-hand side of the DC-9. The
fuselage wing cut off the engine 2 from the bottom of the window. The DC-9 fire erupted and
causes the fuselage to burn out of the cockpit that is forwarded to the aft bulkhead. There was no
fire in the Boeing 727 but had a damage to the left wing. By the impact or post impact of the fire,
eight people were killed. The DC-9 pilots when realized that they were disoriented, they did not
hit the brakes. If the DC-9 is active on the runway then there is a possibility that delay in
recognition from the ground controller. The observation of weather was inadequate. Around the
airfield, there were some signs and lighting and surface markings deficiencies. The Northwest
Airlines, Inc., fail to provide an adequate resource management cockpit training to the line
aircrews (Fraher 2014). The release mechanism of DC-9 internal cone of tail was not operable
when contributing to the fatalities in an accident (Cowlagi and Saleh 2015). The National
Training was in progress 0 5
Workload 3 2
Environment / weather 4 6
Fatigue 0 1
any other factors 0 2
Total factors 120 175
Figure 2: Factors that associate with or enable in the incursions of runway: 65 occurrence of
pilot initiation, and 89 by the controllers.
Source: Author
Catastrophic events Similar to Tenerife Disaster
The scenario is similar to the collision between the two airliners of Northwest at Detroit
Metropolitan or the Wayne Country Airport, Michigan, which was in the year December 3, 1990.
The Northwest Airlines Flight 1482, a DC-9 bound of Pittsburgh has received clearance to taxi.
Due to the dense fog, the crew missed the taxiway of the Oscar 6 and entered into the Outer
taxiway (Drum.lib.umd.edu 2018). When the pilots found that had taxied in the wrong way, then
they had contacted the ground control. The ground control found NW1482 was toward the active
runway and immediately inform the crew to leave that runway. Later within 5 seconds, the crew
of DC-9 saw Boeing 727 was coming over them. Boeing 727 speed of travelling was over 100
knots and had received takeoff clearance just in that moment when the collision had taken place.
When the 727’s right wingtip was sheared off, it strike the right-hand side of the DC-9. The
fuselage wing cut off the engine 2 from the bottom of the window. The DC-9 fire erupted and
causes the fuselage to burn out of the cockpit that is forwarded to the aft bulkhead. There was no
fire in the Boeing 727 but had a damage to the left wing. By the impact or post impact of the fire,
eight people were killed. The DC-9 pilots when realized that they were disoriented, they did not
hit the brakes. If the DC-9 is active on the runway then there is a possibility that delay in
recognition from the ground controller. The observation of weather was inadequate. Around the
airfield, there were some signs and lighting and surface markings deficiencies. The Northwest
Airlines, Inc., fail to provide an adequate resource management cockpit training to the line
aircrews (Fraher 2014). The release mechanism of DC-9 internal cone of tail was not operable
when contributing to the fatalities in an accident (Cowlagi and Saleh 2015). The National
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Transportation Safety Board (NTSB) has also noted that contributing to number and the severity
of the injuries fails the crew of the DC-9 in proper evacuation of the passenger.
Recommendation of Tenerife disaster occur and to manage such issue raised
a) Crew Resource Management: The Tenerife accident investigation led to
recommendations of new and innovative training to cope up with the human error (McAndrew
and Wise 2014). The training of Cockpit Resource Management has expanded to aircraft crew
member and later became a Crew Resource Management. The design of this training was to
avoid the situation of the crisis which will improve the competencies of the team as a whole. It
will help to identify, avoid and address the errors of human (Alavosius et al. 2017).
b) Project Resource Management: the content of CRM-training can be a part of the
project-management trainings. They will focus on the error of human in combination with the
training of systematic rollout to make a unique approach. With the implementation of Company
Resource Management or Project Resource Management, it will be easier to recognize the errors
and the chain of the error, a better decision making model can be put and could address the
problem openly.
Conclusion
It has been examine in the report about the Tenerife incident. In general, Tenerife is a
system vulnerability prototype. Implications of the process of research and practice in which the
prototype has been observed throughout the preceding account and it has conclude some special
review. In this report, most of the crises and behavior of the news remain viable. The report has
assembled a plausible configuration which is a set of speculations for a new variables. After
reformulating, editing and assembling the existing idea, some of the future research has
identified.
Transportation Safety Board (NTSB) has also noted that contributing to number and the severity
of the injuries fails the crew of the DC-9 in proper evacuation of the passenger.
Recommendation of Tenerife disaster occur and to manage such issue raised
a) Crew Resource Management: The Tenerife accident investigation led to
recommendations of new and innovative training to cope up with the human error (McAndrew
and Wise 2014). The training of Cockpit Resource Management has expanded to aircraft crew
member and later became a Crew Resource Management. The design of this training was to
avoid the situation of the crisis which will improve the competencies of the team as a whole. It
will help to identify, avoid and address the errors of human (Alavosius et al. 2017).
b) Project Resource Management: the content of CRM-training can be a part of the
project-management trainings. They will focus on the error of human in combination with the
training of systematic rollout to make a unique approach. With the implementation of Company
Resource Management or Project Resource Management, it will be easier to recognize the errors
and the chain of the error, a better decision making model can be put and could address the
problem openly.
Conclusion
It has been examine in the report about the Tenerife incident. In general, Tenerife is a
system vulnerability prototype. Implications of the process of research and practice in which the
prototype has been observed throughout the preceding account and it has conclude some special
review. In this report, most of the crises and behavior of the news remain viable. The report has
assembled a plausible configuration which is a set of speculations for a new variables. After
reformulating, editing and assembling the existing idea, some of the future research has
identified.
8TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
References
Alavosius, M.P., Houmanfar, R.A., Anbro, S.J., Burleigh, K. and Hebein, C., 2017. Leadership
and Crew Resource Management in High-Reliability Organizations: A Competency Framework
for Measuring Behaviors. Journal of Organizational Behavior Management, 37(2), pp.142-170.
Aren’t Indicated, O.S.T. and Boyd, T., 2016. AMA Journal of Ethics®. Ethics, 18(8), pp.759-
858.
Bucher, S., Jäger, U. and Cardoza, G. (2018). FUNDES: Becoming a strategically mindful
nonprofit.
Cowlagi, R.V. and Saleh, J.H., 2015. Coordinability and consistency: Application of systems
theory to accident causation and prevention. Journal of Loss Prevention in the Process
Industries, 33, pp.200-212.
Drum.lib.umd.edu. (2018). Cite a Website - Cite This For Me. [online] Available at:
https://drum.lib.umd.edu/bitstream/handle/1903/20279/Pires_umd_0117E_18445.pdf?
sequence=1&isAllowed=y [Accessed 24 Feb. 2018].
Fraher, A., 2014. The Manic Culture of the Post-9/11 Airline Industry in
America. Organisational and Social Dynamics, 14(1), pp.53-75.
Harrison, V. and Mackenzie Ross, S., 2016. An emerging concern: toxic fumes in airplane
cabins. cortex, 74, pp.297-302.
Hernandez, Y., Guimarães Pereira, Â. and Barbosa, P. (2018). Resilient futures of a small island:
A participatory approach in Tenerife (Canary Islands) to address climate change.
Hubbard, R., Regan, K., Strath, A. and Vosper, H., 2015. The Big Issue: ergonomics in
healthcare education. Communicare, 1(2).
López, E., Rengel, R., Mair, G.W. and Isorna, F., 2015, July. Analysis of high-pressure hydrogen
and natural gas cylinders explosions through TNT equivalent method. In Proceeding Hyceltec
2015. Iberian symposium on hydrogen, fuel cells and advanced batteries (pp. 5-8).
McAndrew, I.R. and Wise, G.P., 2014. Crew Resource Management and its possible role in
nursing risk management. WIT Transactions on Information and Communication
Technologies, 47, pp.251-261.
Ogliastri, E. and Zúñiga, R., 2016. An introduction to mindfulness and sensemaking by highly
reliable organizations in Latin America. Journal of Business Research, 69(10), pp.4429-4434.
References
Alavosius, M.P., Houmanfar, R.A., Anbro, S.J., Burleigh, K. and Hebein, C., 2017. Leadership
and Crew Resource Management in High-Reliability Organizations: A Competency Framework
for Measuring Behaviors. Journal of Organizational Behavior Management, 37(2), pp.142-170.
Aren’t Indicated, O.S.T. and Boyd, T., 2016. AMA Journal of Ethics®. Ethics, 18(8), pp.759-
858.
Bucher, S., Jäger, U. and Cardoza, G. (2018). FUNDES: Becoming a strategically mindful
nonprofit.
Cowlagi, R.V. and Saleh, J.H., 2015. Coordinability and consistency: Application of systems
theory to accident causation and prevention. Journal of Loss Prevention in the Process
Industries, 33, pp.200-212.
Drum.lib.umd.edu. (2018). Cite a Website - Cite This For Me. [online] Available at:
https://drum.lib.umd.edu/bitstream/handle/1903/20279/Pires_umd_0117E_18445.pdf?
sequence=1&isAllowed=y [Accessed 24 Feb. 2018].
Fraher, A., 2014. The Manic Culture of the Post-9/11 Airline Industry in
America. Organisational and Social Dynamics, 14(1), pp.53-75.
Harrison, V. and Mackenzie Ross, S., 2016. An emerging concern: toxic fumes in airplane
cabins. cortex, 74, pp.297-302.
Hernandez, Y., Guimarães Pereira, Â. and Barbosa, P. (2018). Resilient futures of a small island:
A participatory approach in Tenerife (Canary Islands) to address climate change.
Hubbard, R., Regan, K., Strath, A. and Vosper, H., 2015. The Big Issue: ergonomics in
healthcare education. Communicare, 1(2).
López, E., Rengel, R., Mair, G.W. and Isorna, F., 2015, July. Analysis of high-pressure hydrogen
and natural gas cylinders explosions through TNT equivalent method. In Proceeding Hyceltec
2015. Iberian symposium on hydrogen, fuel cells and advanced batteries (pp. 5-8).
McAndrew, I.R. and Wise, G.P., 2014. Crew Resource Management and its possible role in
nursing risk management. WIT Transactions on Information and Communication
Technologies, 47, pp.251-261.
Ogliastri, E. and Zúñiga, R., 2016. An introduction to mindfulness and sensemaking by highly
reliable organizations in Latin America. Journal of Business Research, 69(10), pp.4429-4434.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9TENERIFE 1977 CRASH WITH FAULT TREE ANALYSIS
Roudet, J., Thurat, P.E. and Turcot, N., 2016. Airport ground-traffic surveillance systems data
feed innovative comprehensive analysis. Transportation Research Procedia, 14, pp.3741-3750.
Wong, M., 2017. Doctor in the sky: Medico-legal issues during in-flight emergencies. Medical
Law International, 17(1-2), pp.65-98.
Roudet, J., Thurat, P.E. and Turcot, N., 2016. Airport ground-traffic surveillance systems data
feed innovative comprehensive analysis. Transportation Research Procedia, 14, pp.3741-3750.
Wong, M., 2017. Doctor in the sky: Medico-legal issues during in-flight emergencies. Medical
Law International, 17(1-2), pp.65-98.
1 out of 10


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.