Case Study: Tetanus Booster, Wound Observations, and Antibiotic Use
VerifiedAdded on 2019/11/19
|5
|2139
|1131
Case Study
AI Summary
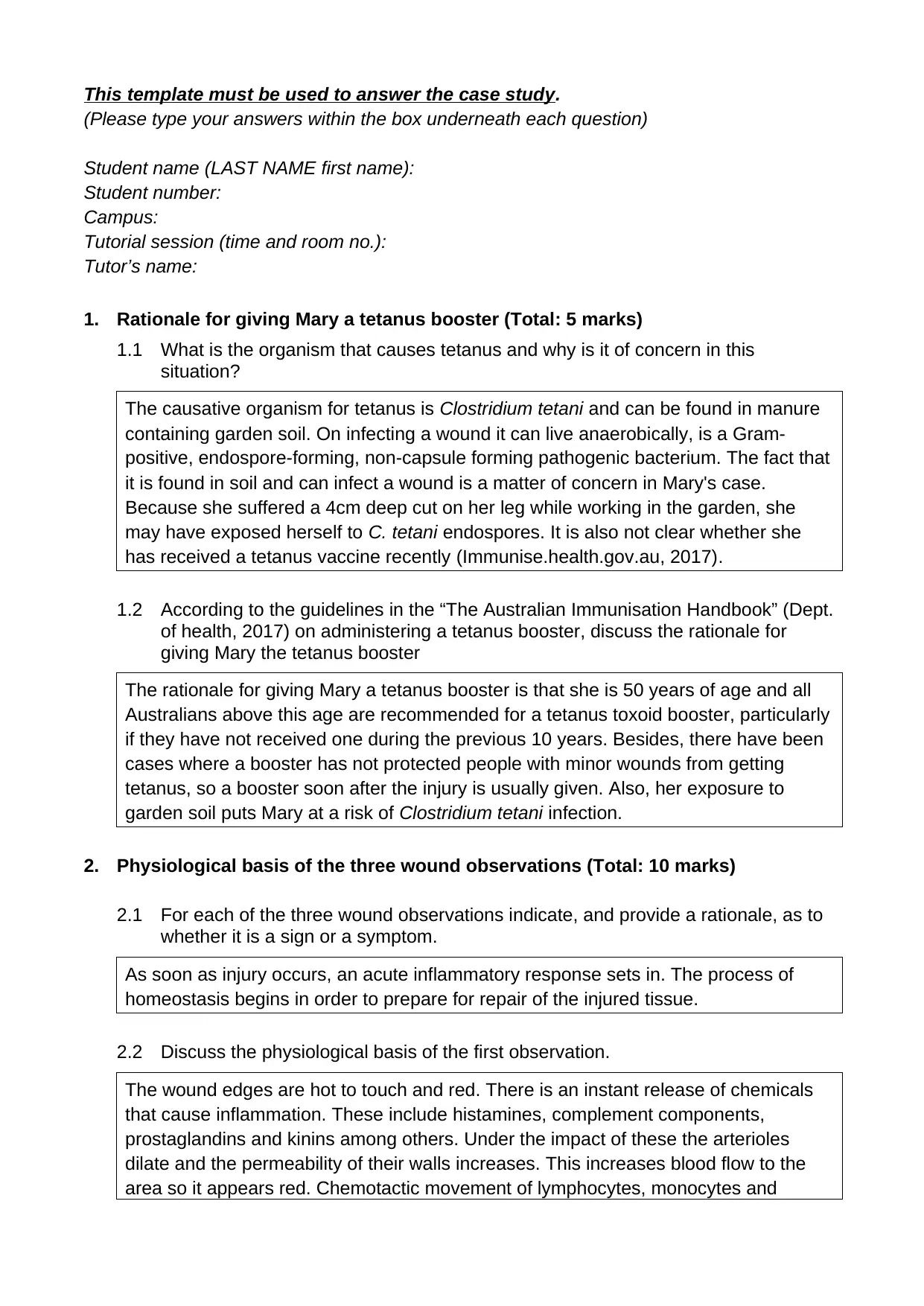
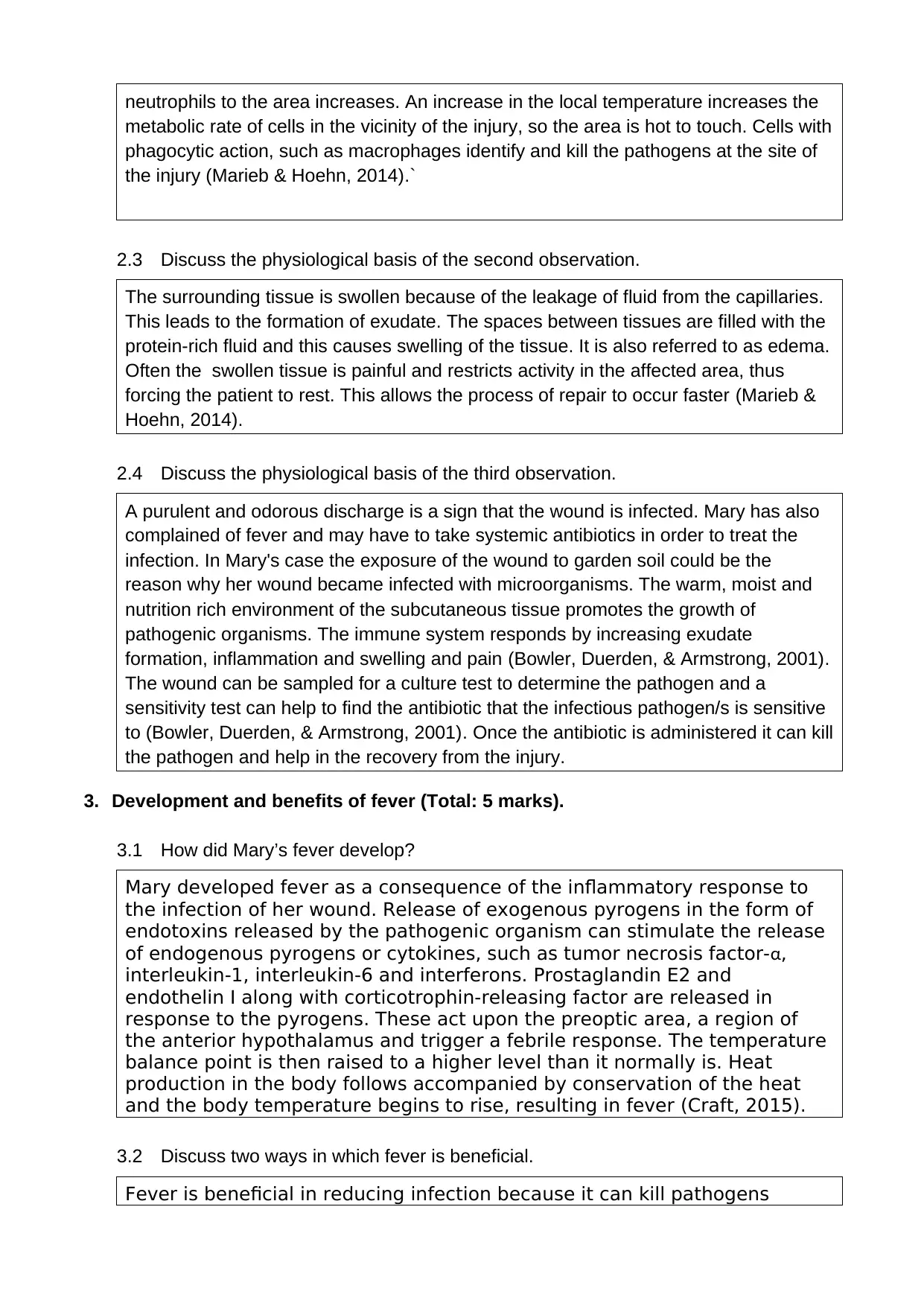
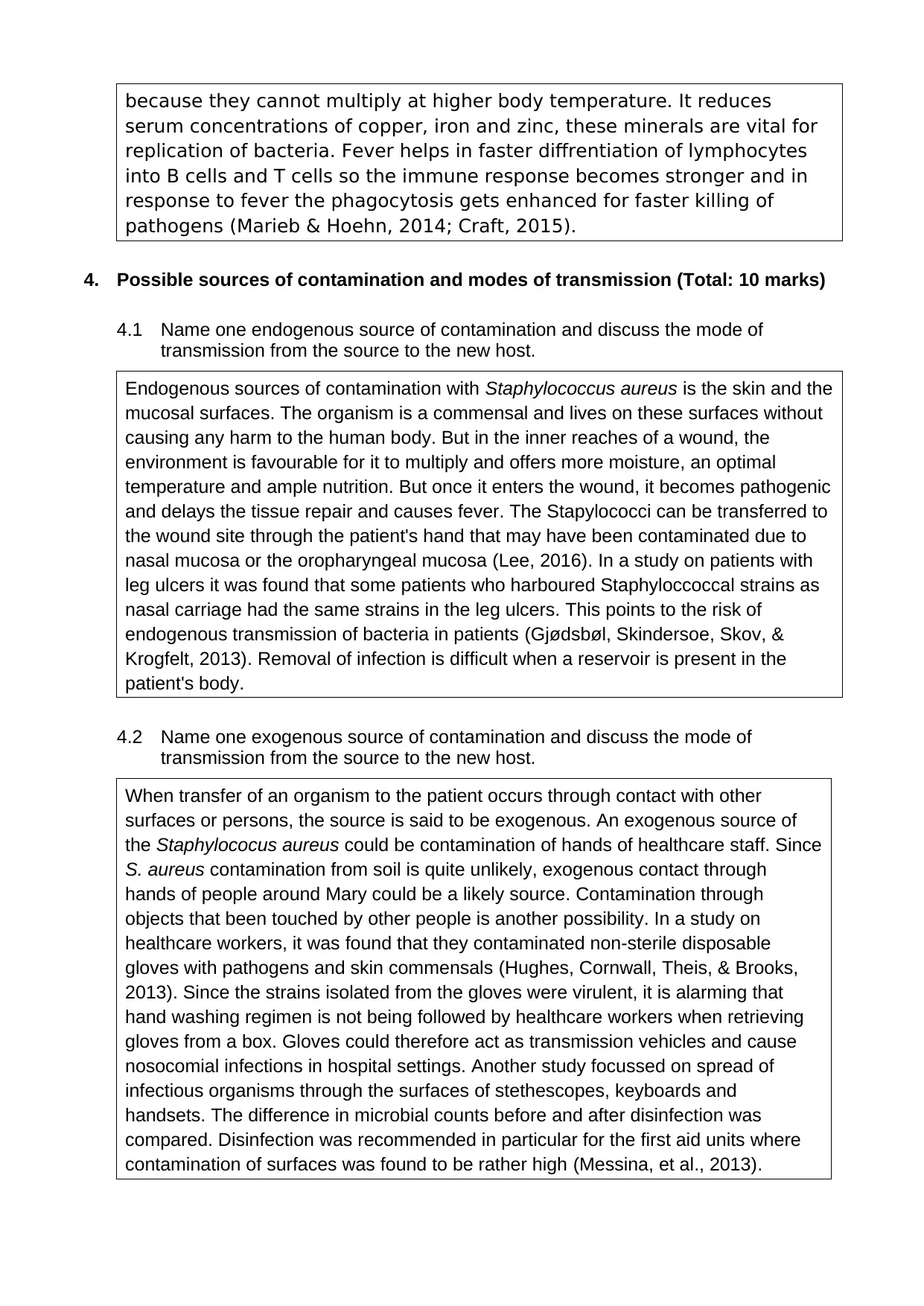
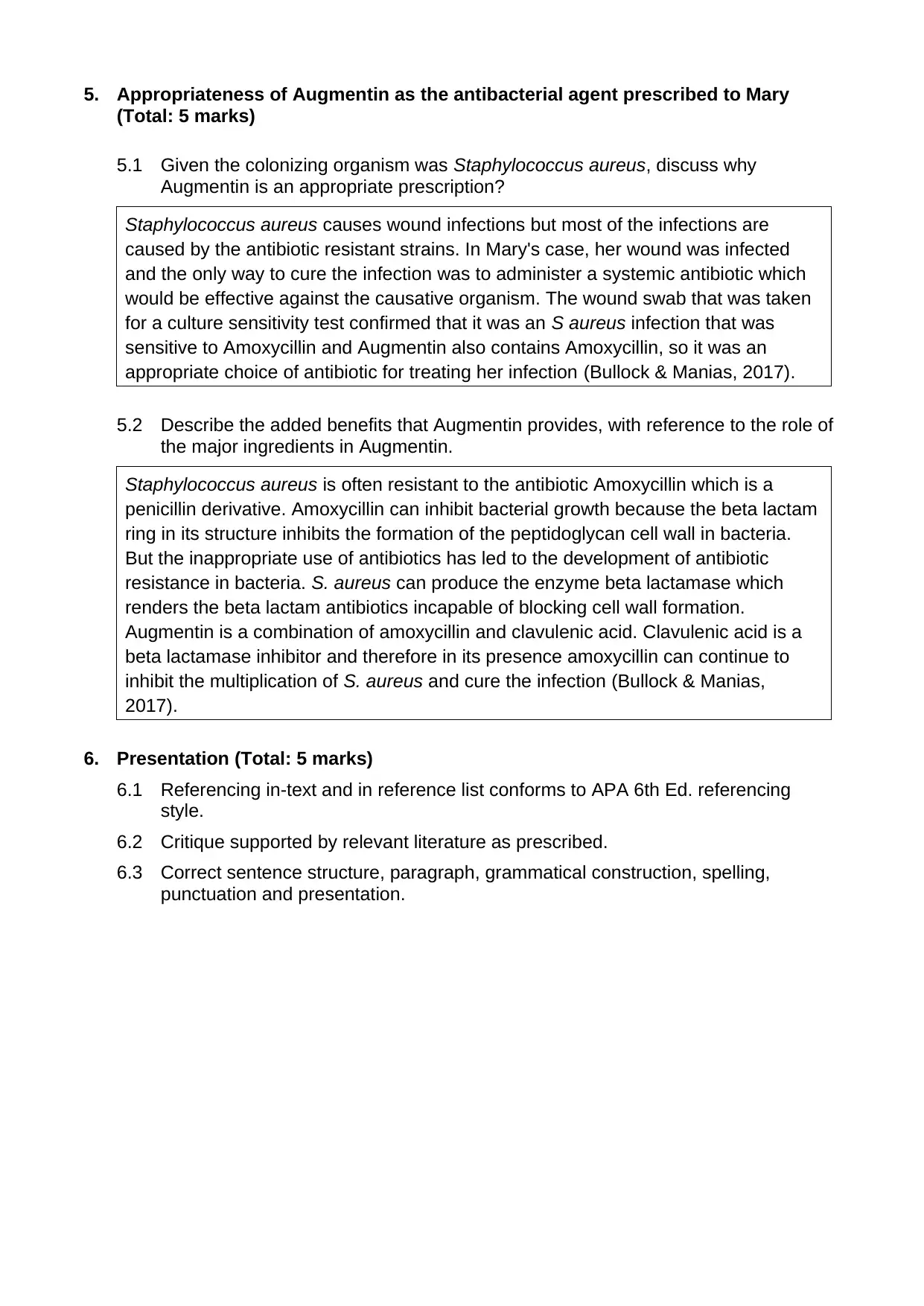
This case study analyzes a patient, Mary, who sustained a deep wound while gardening, raising concerns about potential tetanus infection. The case study explores the rationale for administering a tetanus booster based on age and potential exposure to Clostridium tetani. It delves into the physiological basis of wound observations, including redness, heat, swelling, and purulent discharge, linking them to the inflammatory response. The study further examines the development and benefits of fever, discussing how it helps combat infection. It also identifies possible endogenous and exogenous sources of wound contamination, particularly focusing on Staphylococcus aureus. The appropriateness of Augmentin as the prescribed antibacterial agent is discussed, highlighting its benefits and the role of its ingredients in combating antibiotic-resistant strains. Finally, the case study adheres to APA 6th Ed. referencing style and correct presentation, supported by relevant literature.
1 out of 5
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.