NURS 725 - Evidence Table: Translation Research in Population Health
VerifiedAdded on 2023/06/04
|4
|1370
|455
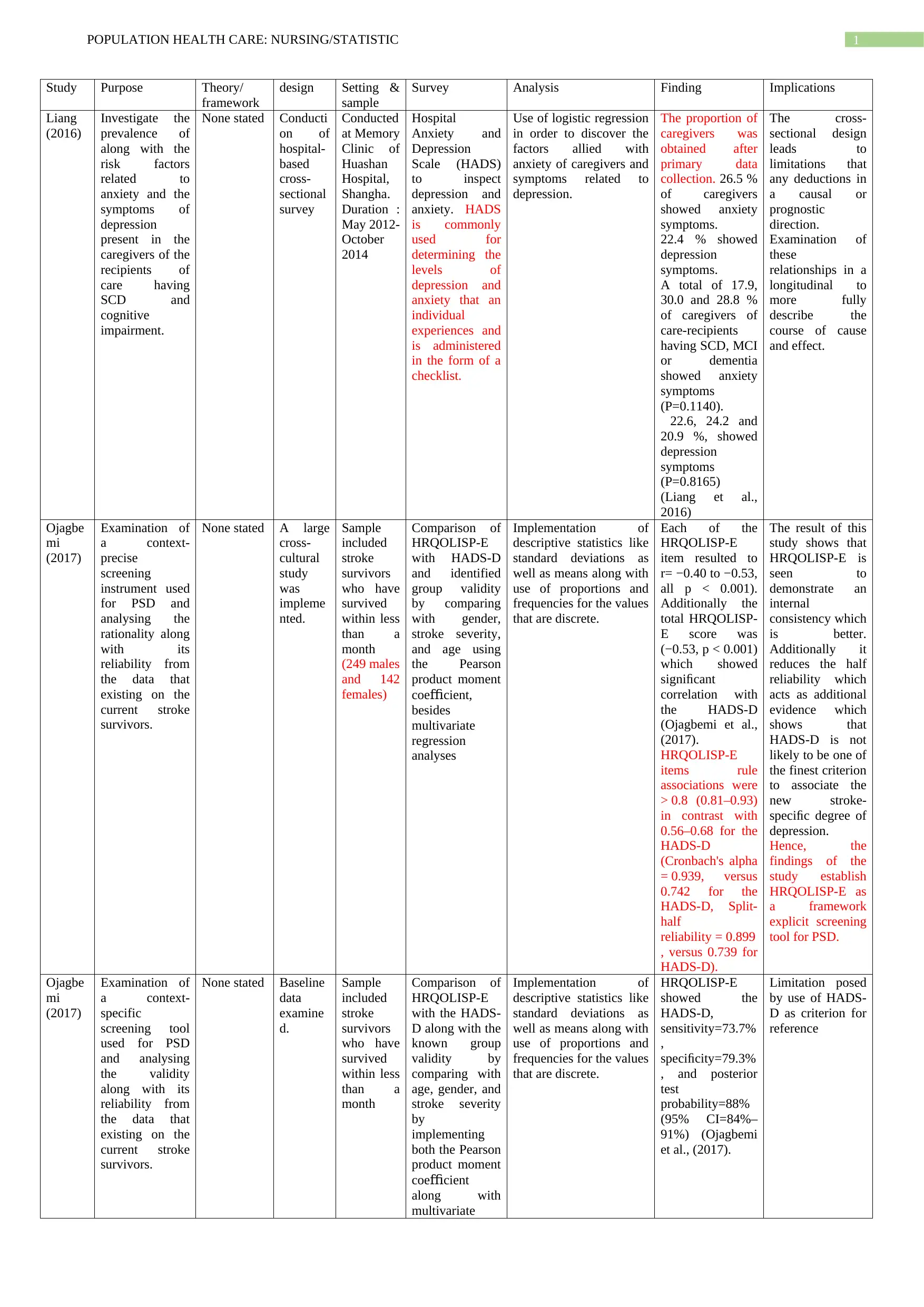
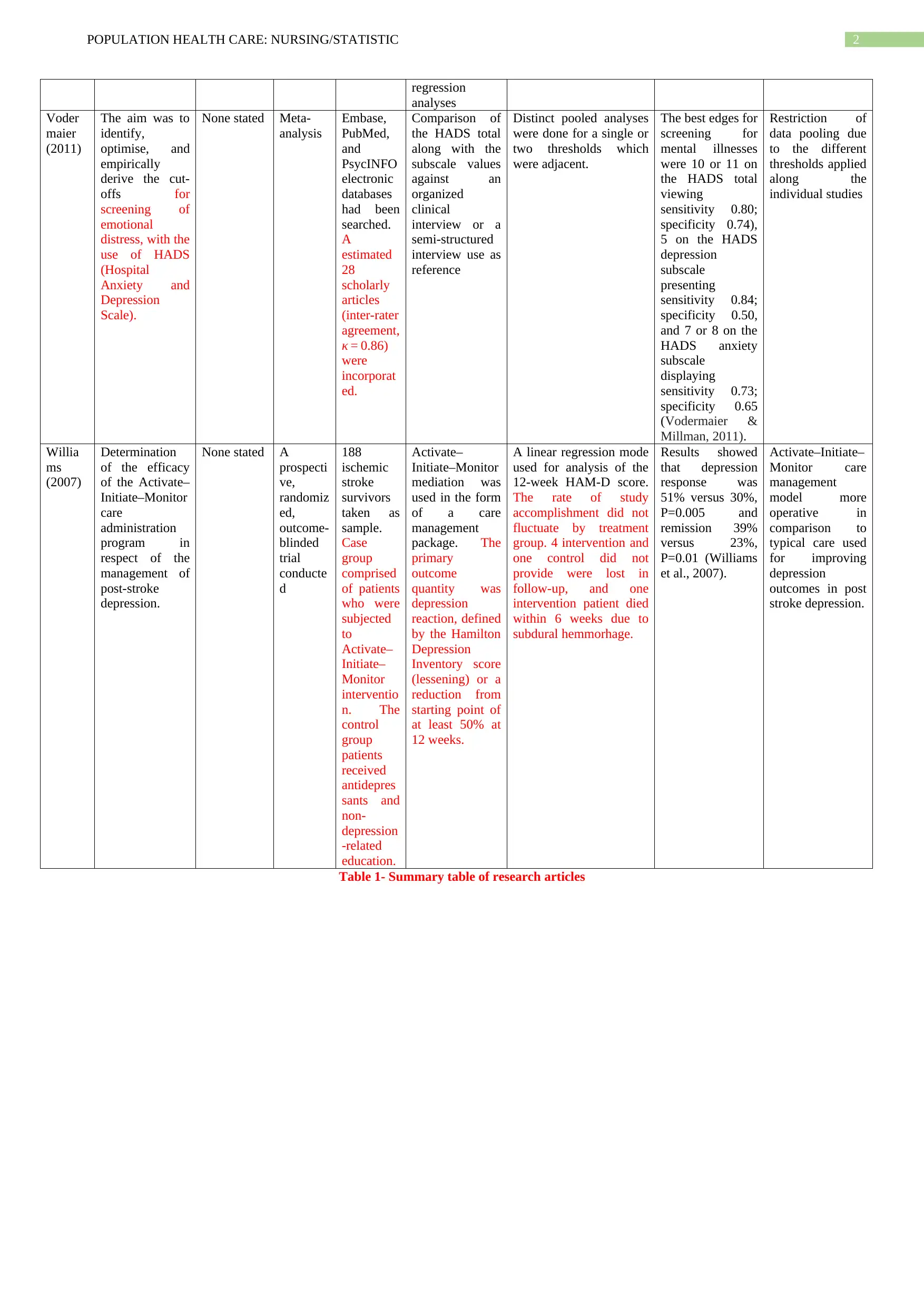
Literature Review
AI Summary
This document presents a literature review in the form of an evidence table, focusing on population health care, nursing, and statistics. It summarizes key research articles, examining study designs, settings, samples, surveys/instruments used, and findings related to topics such as anxiety and depression in caregivers of individuals with cognitive decline, screening tools for post-stroke depression, and the effectiveness of care management programs for post-stroke depression. The table includes details like study purpose, theoretical frameworks, statistical analyses, and implications for practice or limitations of the research. Studies included utilize designs such as cross-sectional surveys, meta-analyses, and randomized controlled trials to investigate various aspects of population health and mental health outcomes. The evidence table is designed to provide a concise overview of relevant research for translation research, as part of the NURS 725 course.

1 out of 4
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.