Uganda Health Workforce Planning: Analysis, Issues, & Solutions
VerifiedAdded on 2023/03/31
|15
|2783
|311
Report
AI Summary
This report provides an overview of health workforce planning in Uganda, highlighting the critical issues and challenges the country faces in ensuring adequate healthcare personnel. It begins with an environmental scan, revealing a severe shortage of healthcare workers, particularly in rural areas, and an imbalance in the distribution of professionals. The report analyzes the data profile of the health workforce, emphasizing the scarcity of skilled workers and the dominance of nurses within the sector. Identified critical issues include workforce concentration in central regions, financial constraints, poor infrastructure, and a lack of awareness and education. To address these challenges, the report recommends strategies such as job creation, improved education and training, and skills enhancement, drawing from World Health Organization guidelines to strengthen the healthcare workforce and improve overall healthcare delivery in Uganda. Desklib provides access to similar documents and study resources for students.

Running head: HEALTH WORK FORCE PLANNING – UGANDA
Health Work Force Planning – Uganda
Name of the Student
Name of the University
Author’s Note:
Health Work Force Planning – Uganda
Name of the Student
Name of the University
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1HEALTH WORK FORCE PLANNING – UGANDA
Executive Summary:
The main objective of health work force planning is to create an outline of Uganda's health work
force based on its strategy developments, in which the country's policies and problems are
addressed. In terms of human resources for health and economic considerations, Uganda is faced
with many issues as a low-income nation. The health workers strategy focuses primarily on the
improvement of people's health resources and the quality of care growth. The appeal for higher
incomes and opportunity however, are considerations that cause qualified workers to migrate or
join the independent sector. It is necessary to monitor all these problems and to draw up a
stronger work force leadership strategy. To create a stronger plan, the following study would also
outline a recommendation to address the issue.
Executive Summary:
The main objective of health work force planning is to create an outline of Uganda's health work
force based on its strategy developments, in which the country's policies and problems are
addressed. In terms of human resources for health and economic considerations, Uganda is faced
with many issues as a low-income nation. The health workers strategy focuses primarily on the
improvement of people's health resources and the quality of care growth. The appeal for higher
incomes and opportunity however, are considerations that cause qualified workers to migrate or
join the independent sector. It is necessary to monitor all these problems and to draw up a
stronger work force leadership strategy. To create a stronger plan, the following study would also
outline a recommendation to address the issue.
2HEALTH WORK FORCE PLANNING – UGANDA
Table of Contents
1. Introduction:................................................................................................................................3
2. Environmental scan of health care work force in Uganda:..........................................................4
3. Data profile of the health care work force:..................................................................................6
4. Identified critical issues:..............................................................................................................9
5. Recommendation for the improvement of the situation:...........................................................10
6. Conclusion:................................................................................................................................12
7. References:................................................................................................................................13
Table of Contents
1. Introduction:................................................................................................................................3
2. Environmental scan of health care work force in Uganda:..........................................................4
3. Data profile of the health care work force:..................................................................................6
4. Identified critical issues:..............................................................................................................9
5. Recommendation for the improvement of the situation:...........................................................10
6. Conclusion:................................................................................................................................12
7. References:................................................................................................................................13
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3HEALTH WORK FORCE PLANNING – UGANDA
1. Introduction:
The World Health Organization defines the health workers as all the workers whose function is
to safeguard and enhance the health of the populations. The word workforce is used here to
represent the extended role and higher amount of females in health jobs (African Health
Observatory, 2019). The resources are being evaluated in order to identify the amount of experts
accessible to provide services. Health care personnel are a significant part of the operation and
efficiency of labor intensive health systems depends on them. The health professionals are not
just people; however some nations in the face of health professional shortages have been
unwilling to devise comprehensive health human resources strategies, or strategic plans, which
are essential to direct and construct the necessary human facilities in their health care structures.
They also contribute distinct abilities to distinct functions in the workplace (Ono, Lafortune &
Schoenstein, 2013). Therefore, it is crucial, using evidence based initiatives for domestic health
human resources measures and approaches to rationalize choices about a country's health care
workforce. These strategies can decrease employee imbalances, increase employee efficiency
and enhance employee retention and adaptation to any kind of health sector reform.
Uganda, Africa is one of such country which has been facing health care work force shortage in
the recent years. Human resources in Uganda are adverse in relation to health service provision
and therefore have a negative impact on the industry because of health issues. They have adverse
consequences for the whole industry's utilization ability. The place to start for enhancing the
general efficiency of the health care sector should therefore be to improve the level of personnel
and the health motivating human resources (Namakula & Witter, 2014). A full mix of actions is
necessary, as higher salaries or employee accommodations are not sufficient. Improved
economic conditions should be accompanied by changes in the leadership of human resources.
1. Introduction:
The World Health Organization defines the health workers as all the workers whose function is
to safeguard and enhance the health of the populations. The word workforce is used here to
represent the extended role and higher amount of females in health jobs (African Health
Observatory, 2019). The resources are being evaluated in order to identify the amount of experts
accessible to provide services. Health care personnel are a significant part of the operation and
efficiency of labor intensive health systems depends on them. The health professionals are not
just people; however some nations in the face of health professional shortages have been
unwilling to devise comprehensive health human resources strategies, or strategic plans, which
are essential to direct and construct the necessary human facilities in their health care structures.
They also contribute distinct abilities to distinct functions in the workplace (Ono, Lafortune &
Schoenstein, 2013). Therefore, it is crucial, using evidence based initiatives for domestic health
human resources measures and approaches to rationalize choices about a country's health care
workforce. These strategies can decrease employee imbalances, increase employee efficiency
and enhance employee retention and adaptation to any kind of health sector reform.
Uganda, Africa is one of such country which has been facing health care work force shortage in
the recent years. Human resources in Uganda are adverse in relation to health service provision
and therefore have a negative impact on the industry because of health issues. They have adverse
consequences for the whole industry's utilization ability. The place to start for enhancing the
general efficiency of the health care sector should therefore be to improve the level of personnel
and the health motivating human resources (Namakula & Witter, 2014). A full mix of actions is
necessary, as higher salaries or employee accommodations are not sufficient. Improved
economic conditions should be accompanied by changes in the leadership of human resources.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4HEALTH WORK FORCE PLANNING – UGANDA
The health employee ratio in Uganda per 1000 population is still below a minimum of 2.3 health
employees per 1000 population suggested by the World Health Organization (African Health
Observatory, 2019).
Therefore, the aim of this report is to highlight current state of health work force in Uganda,
identify the critical issue facing in this area and provide recommendation according to the issues
identified.
2. Environmental scan of health care work force in Uganda:
From the recent report, it has been noted that there is a severe shortage of work force in the
health care sector of Uganda. It has been reported that, in the year 2012, only 58 per cent of the
total position of the health care force was filled. According to the WHO guideline, there should
be a minimum of 2.3 health workers per 1000 individuals to meet the standard developmental
health care goals. While considering the total health care work force, Uganda ratio of health care
workers per 1000 population was at 1.8 in the year 2012 (Sandin, 2013). In addition to that, there
has been a huge bias and imbalance among the rural and urban region of the country in relation
to the medical profession present. More health care professionals are available in the central
region of the country and less and less health care workers are available in the rural and remote
area. It has been reported in the study that the central region of the country consists of only 27
per cent of the total populace, but contains 64 per cent of the total midwifery and nurses
professionals available in the country. In addition to that, central region also contains 76 per cent
of all the available dentists, 71 per cent of all the available doctors and 81 percent of all the
available pharmacists (Sandin, 2013). Thus, from the above data, it can be deduced that almost
70 per cent of the remaining population of the country had make do with the less 40 to 30 per
cent of total available health care professionals. It has also been noted that the deteriorating
The health employee ratio in Uganda per 1000 population is still below a minimum of 2.3 health
employees per 1000 population suggested by the World Health Organization (African Health
Observatory, 2019).
Therefore, the aim of this report is to highlight current state of health work force in Uganda,
identify the critical issue facing in this area and provide recommendation according to the issues
identified.
2. Environmental scan of health care work force in Uganda:
From the recent report, it has been noted that there is a severe shortage of work force in the
health care sector of Uganda. It has been reported that, in the year 2012, only 58 per cent of the
total position of the health care force was filled. According to the WHO guideline, there should
be a minimum of 2.3 health workers per 1000 individuals to meet the standard developmental
health care goals. While considering the total health care work force, Uganda ratio of health care
workers per 1000 population was at 1.8 in the year 2012 (Sandin, 2013). In addition to that, there
has been a huge bias and imbalance among the rural and urban region of the country in relation
to the medical profession present. More health care professionals are available in the central
region of the country and less and less health care workers are available in the rural and remote
area. It has been reported in the study that the central region of the country consists of only 27
per cent of the total populace, but contains 64 per cent of the total midwifery and nurses
professionals available in the country. In addition to that, central region also contains 76 per cent
of all the available dentists, 71 per cent of all the available doctors and 81 percent of all the
available pharmacists (Sandin, 2013). Thus, from the above data, it can be deduced that almost
70 per cent of the remaining population of the country had make do with the less 40 to 30 per
cent of total available health care professionals. It has also been noted that the deteriorating
5HEALTH WORK FORCE PLANNING – UGANDA
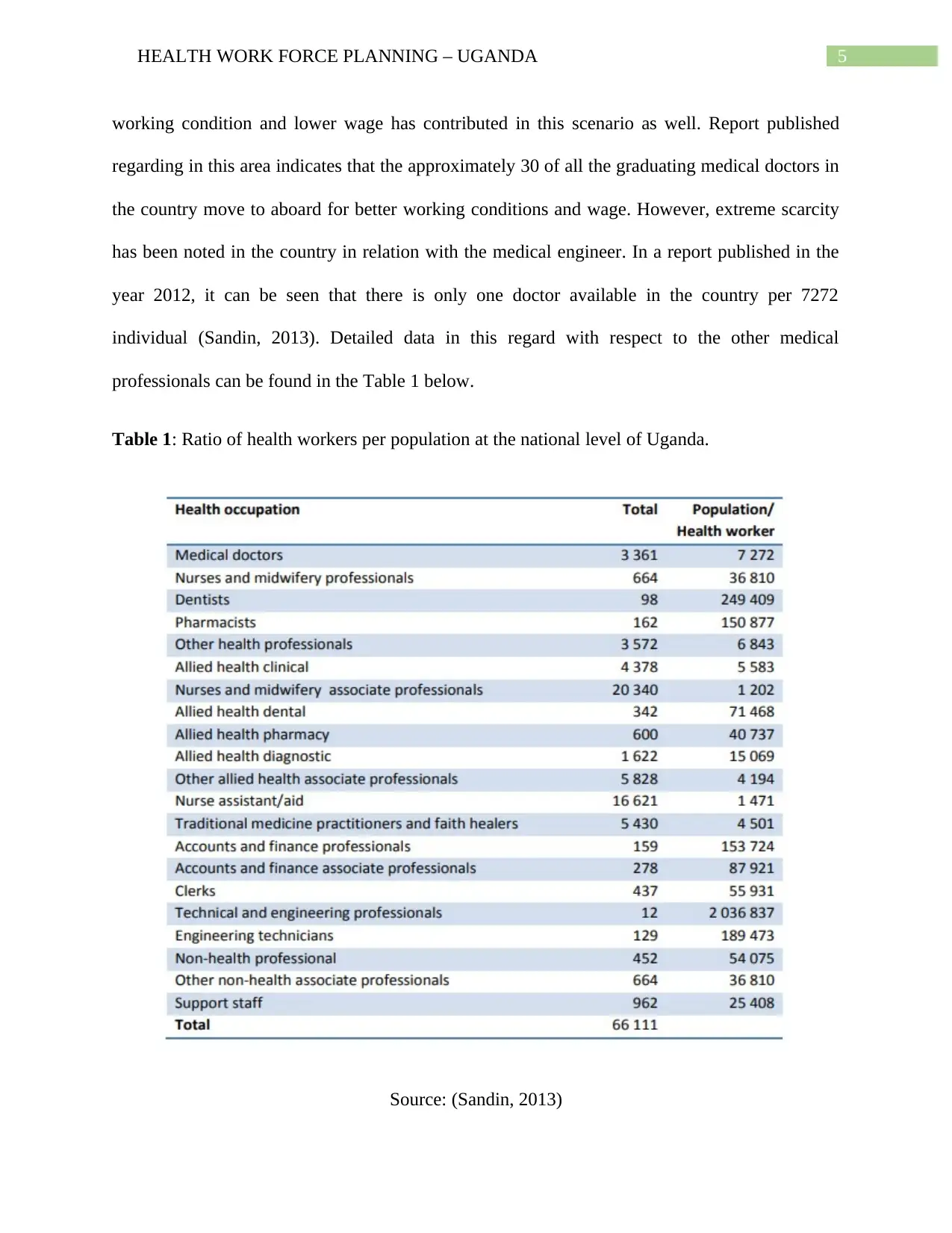
working condition and lower wage has contributed in this scenario as well. Report published
regarding in this area indicates that the approximately 30 of all the graduating medical doctors in
the country move to aboard for better working conditions and wage. However, extreme scarcity
has been noted in the country in relation with the medical engineer. In a report published in the
year 2012, it can be seen that there is only one doctor available in the country per 7272
individual (Sandin, 2013). Detailed data in this regard with respect to the other medical
professionals can be found in the Table 1 below.
Table 1: Ratio of health workers per population at the national level of Uganda.
Source: (Sandin, 2013)
working condition and lower wage has contributed in this scenario as well. Report published
regarding in this area indicates that the approximately 30 of all the graduating medical doctors in
the country move to aboard for better working conditions and wage. However, extreme scarcity
has been noted in the country in relation with the medical engineer. In a report published in the
year 2012, it can be seen that there is only one doctor available in the country per 7272
individual (Sandin, 2013). Detailed data in this regard with respect to the other medical
professionals can be found in the Table 1 below.
Table 1: Ratio of health workers per population at the national level of Uganda.
Source: (Sandin, 2013)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6HEALTH WORK FORCE PLANNING – UGANDA
From the data presented in the above section it can be stated that the scenario is particularly
bleak with respect to the available technical and engineering professionals available and the
situation of the Dentists is not so good either. Hence, from the above discussion, it can be stated
that the Uganda is need desperate need of fresh injection of health care professionals in the
health care system of the country.
3. Data profile of the health care work force:
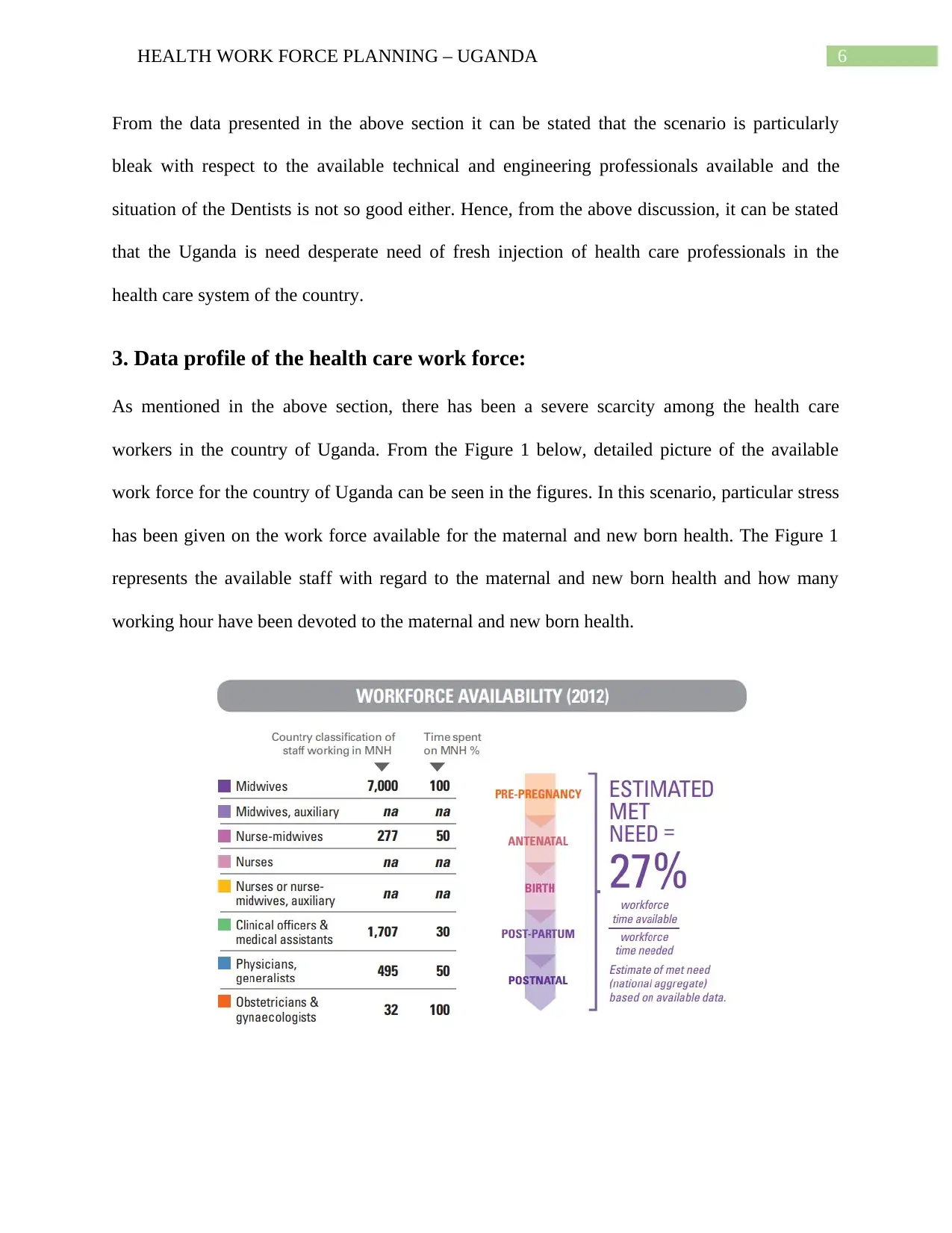
As mentioned in the above section, there has been a severe scarcity among the health care
workers in the country of Uganda. From the Figure 1 below, detailed picture of the available
work force for the country of Uganda can be seen in the figures. In this scenario, particular stress
has been given on the work force available for the maternal and new born health. The Figure 1
represents the available staff with regard to the maternal and new born health and how many
working hour have been devoted to the maternal and new born health.
From the data presented in the above section it can be stated that the scenario is particularly
bleak with respect to the available technical and engineering professionals available and the
situation of the Dentists is not so good either. Hence, from the above discussion, it can be stated
that the Uganda is need desperate need of fresh injection of health care professionals in the
health care system of the country.
3. Data profile of the health care work force:
As mentioned in the above section, there has been a severe scarcity among the health care
workers in the country of Uganda. From the Figure 1 below, detailed picture of the available
work force for the country of Uganda can be seen in the figures. In this scenario, particular stress
has been given on the work force available for the maternal and new born health. The Figure 1
represents the available staff with regard to the maternal and new born health and how many
working hour have been devoted to the maternal and new born health.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7HEALTH WORK FORCE PLANNING – UGANDA
Figure 1: Work force availability in Uganda in the year 2012. MNH here denotes: Maternity and
Newborn Health. Source: (UNFPA, 2014)
From the Figure 1 above, it can be seen that with relation to maternal and new born health only
27 per cent of the demand have been met (UNFPA, 2014).
Nurses
56%
Allied Health
14%
Medical Officer
9%
Clinical Officer
9%
Pharmacist
3%
Other
9%
Category of health work force in uganda by
percentage
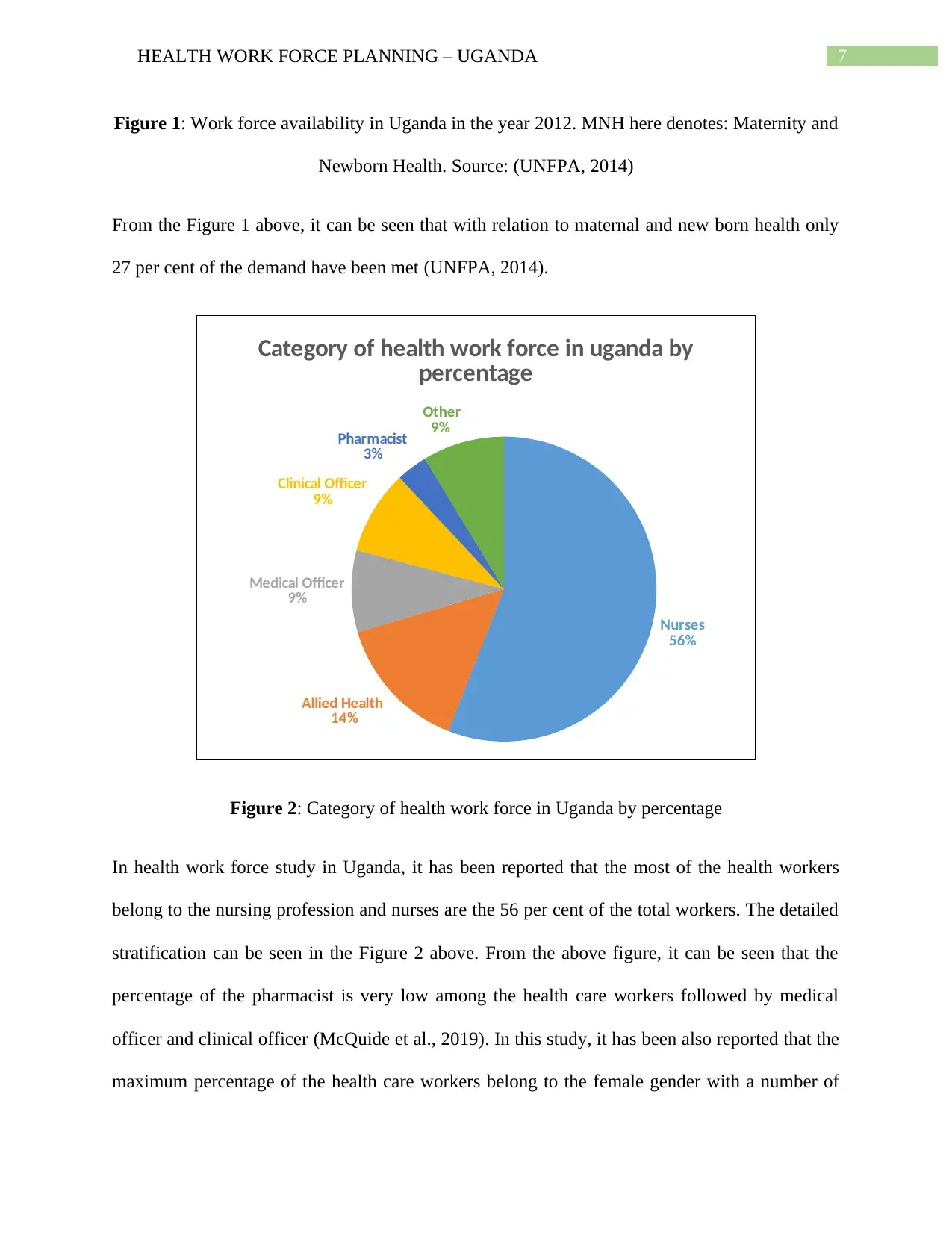
Figure 2: Category of health work force in Uganda by percentage
In health work force study in Uganda, it has been reported that the most of the health workers
belong to the nursing profession and nurses are the 56 per cent of the total workers. The detailed
stratification can be seen in the Figure 2 above. From the above figure, it can be seen that the
percentage of the pharmacist is very low among the health care workers followed by medical
officer and clinical officer (McQuide et al., 2019). In this study, it has been also reported that the
maximum percentage of the health care workers belong to the female gender with a number of
Figure 1: Work force availability in Uganda in the year 2012. MNH here denotes: Maternity and
Newborn Health. Source: (UNFPA, 2014)
From the Figure 1 above, it can be seen that with relation to maternal and new born health only
27 per cent of the demand have been met (UNFPA, 2014).
Nurses
56%
Allied Health
14%
Medical Officer
9%
Clinical Officer
9%
Pharmacist
3%
Other
9%
Category of health work force in uganda by
percentage
Figure 2: Category of health work force in Uganda by percentage
In health work force study in Uganda, it has been reported that the most of the health workers
belong to the nursing profession and nurses are the 56 per cent of the total workers. The detailed
stratification can be seen in the Figure 2 above. From the above figure, it can be seen that the
percentage of the pharmacist is very low among the health care workers followed by medical
officer and clinical officer (McQuide et al., 2019). In this study, it has been also reported that the
maximum percentage of the health care workers belong to the female gender with a number of
8HEALTH WORK FORCE PLANNING – UGANDA
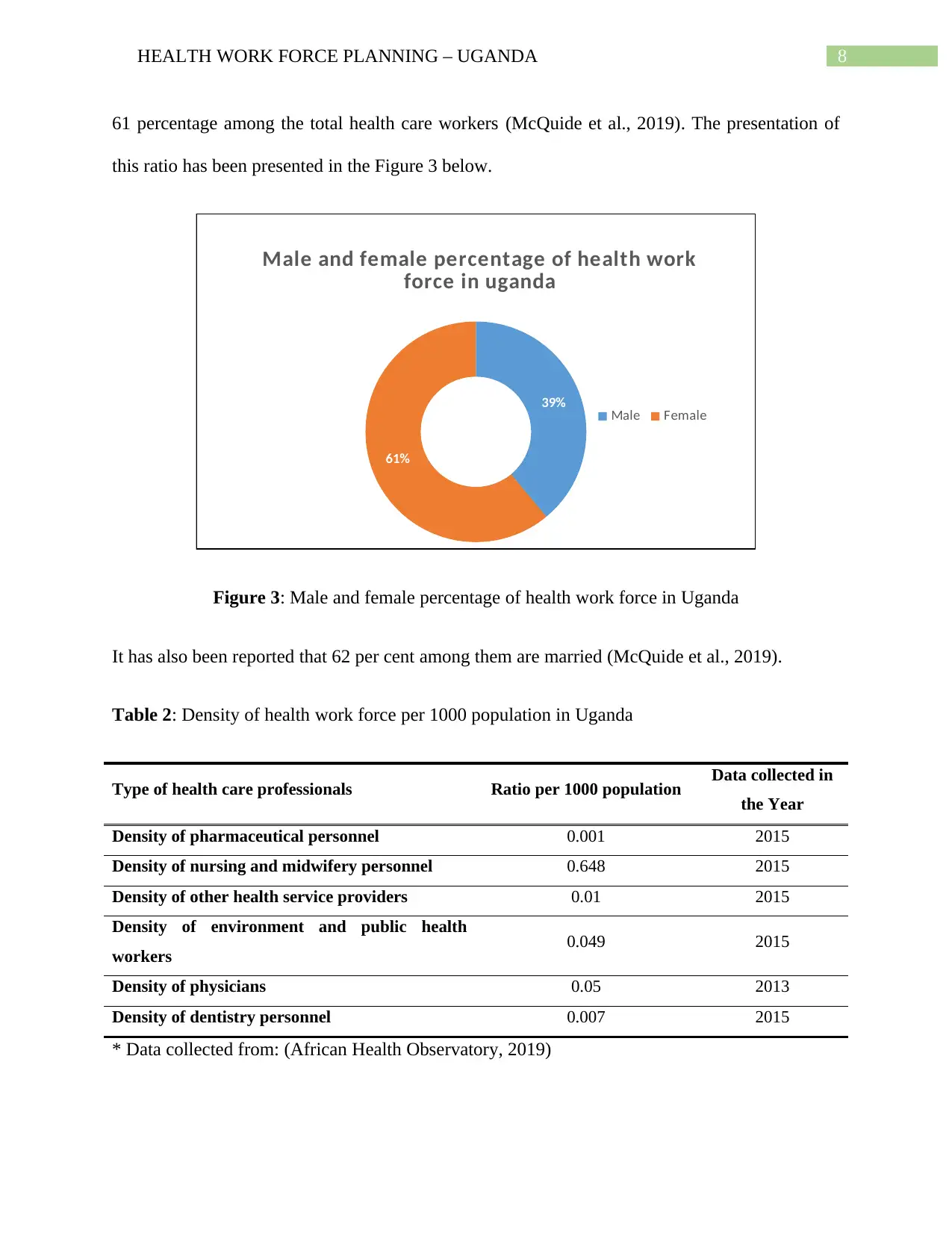
61 percentage among the total health care workers (McQuide et al., 2019). The presentation of
this ratio has been presented in the Figure 3 below.
39%
61%
Male and female percentage of health work
force in uganda
Male Female
Figure 3: Male and female percentage of health work force in Uganda
It has also been reported that 62 per cent among them are married (McQuide et al., 2019).
Table 2: Density of health work force per 1000 population in Uganda
Type of health care professionals Ratio per 1000 population Data collected in
the Year
Density of pharmaceutical personnel 0.001 2015
Density of nursing and midwifery personnel 0.648 2015
Density of other health service providers 0.01 2015
Density of environment and public health
workers 0.049 2015
Density of physicians 0.05 2013
Density of dentistry personnel 0.007 2015
* Data collected from: (African Health Observatory, 2019)
61 percentage among the total health care workers (McQuide et al., 2019). The presentation of
this ratio has been presented in the Figure 3 below.
39%
61%
Male and female percentage of health work
force in uganda
Male Female
Figure 3: Male and female percentage of health work force in Uganda
It has also been reported that 62 per cent among them are married (McQuide et al., 2019).
Table 2: Density of health work force per 1000 population in Uganda
Type of health care professionals Ratio per 1000 population Data collected in
the Year
Density of pharmaceutical personnel 0.001 2015
Density of nursing and midwifery personnel 0.648 2015
Density of other health service providers 0.01 2015
Density of environment and public health
workers 0.049 2015
Density of physicians 0.05 2013
Density of dentistry personnel 0.007 2015
* Data collected from: (African Health Observatory, 2019)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9HEALTH WORK FORCE PLANNING – UGANDA
World Health Organization have recommended that there should be 2.3 number of individual
present among per 1000 population for the proper development and provision of health care
services (African Health Observatory, 2019). In this regard, a detailed density of different health
care professionals with respect to per 1000 population is presented in the Table 2 above. From
the data presented in the Table 2 above, it can be seen that none of the density of health care
workers have met the recommended WHO level of 2.3. The ratio in the all of the categories have
does not even cross the ratio of 1. The situation is particularly bleak in case of Density of
dentistry personnel and Density of pharmaceutical personnel which have a ratio 0.007 and 0.001
respectively (African Health Observatory, 2019).
4. Identified critical issues:
From the data presented in the above section, it can be seen that the healthcare situation is not
very good in relation with the health care workers. Their health workers ratio per 1000 individual
is far below the WHO recommended level of ratio require for per 1000 individuals. One of the
primary reasons is that the lack of health care workers in the country. They have very severe gap
in the demand and reality of the health care workers (African Health Observatory, 2019). In
addition to that several other critical issues have been identified in the health care sector of the
Uganda. The identified critical issues are mentioned below:
Concentration of work force in central region
Financial gap in wages and deteriorating working condition
Lack of qualified and skilled health work force
Weak public accountability
Poor infrastructure
Lack of awareness and education
World Health Organization have recommended that there should be 2.3 number of individual
present among per 1000 population for the proper development and provision of health care
services (African Health Observatory, 2019). In this regard, a detailed density of different health
care professionals with respect to per 1000 population is presented in the Table 2 above. From
the data presented in the Table 2 above, it can be seen that none of the density of health care
workers have met the recommended WHO level of 2.3. The ratio in the all of the categories have
does not even cross the ratio of 1. The situation is particularly bleak in case of Density of
dentistry personnel and Density of pharmaceutical personnel which have a ratio 0.007 and 0.001
respectively (African Health Observatory, 2019).
4. Identified critical issues:
From the data presented in the above section, it can be seen that the healthcare situation is not
very good in relation with the health care workers. Their health workers ratio per 1000 individual
is far below the WHO recommended level of ratio require for per 1000 individuals. One of the
primary reasons is that the lack of health care workers in the country. They have very severe gap
in the demand and reality of the health care workers (African Health Observatory, 2019). In
addition to that several other critical issues have been identified in the health care sector of the
Uganda. The identified critical issues are mentioned below:
Concentration of work force in central region
Financial gap in wages and deteriorating working condition
Lack of qualified and skilled health work force
Weak public accountability
Poor infrastructure
Lack of awareness and education
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10HEALTH WORK FORCE PLANNING – UGANDA
Financial barriers
5. Recommendation for the improvement of the situation:
The World Health Organization has suggested a number of new strategies in order to tackle all
human resources in the area of health work force. In developing a stronger work force strategy,
which can be useful for the improvement and preservation of health workers, the following
strategies should be considered.
1. Job creation: It is a beneficial element that can help to gain more staff in the field, according
to the World Health Organization, to create stronger employment possibilities in the health
industry. The focus should be mainly on the skilled females and young people. Their
participation is advised to keep their jobs in the health industry in the correct location
(Apps.who.int, 2016).
2. Education, Training and Skills: High-quality training and education will help address the
needs for adequate number of health care workers in the country. The key to improving the
quality of health care is continuous high quality training and education.
3. Health Service Delivery and Organisation: A beneficial shift in the performance of the care
would be the reform of the service designs that focus on patient care. The main objective of
service reform has to be high quality, community-based and affordable care. The fundamental
concept of the care service reform is to provide the underprivileged regions with adequate care
(Kaplan et al., 2013).
Financial barriers
5. Recommendation for the improvement of the situation:
The World Health Organization has suggested a number of new strategies in order to tackle all
human resources in the area of health work force. In developing a stronger work force strategy,
which can be useful for the improvement and preservation of health workers, the following
strategies should be considered.
1. Job creation: It is a beneficial element that can help to gain more staff in the field, according
to the World Health Organization, to create stronger employment possibilities in the health
industry. The focus should be mainly on the skilled females and young people. Their
participation is advised to keep their jobs in the health industry in the correct location
(Apps.who.int, 2016).
2. Education, Training and Skills: High-quality training and education will help address the
needs for adequate number of health care workers in the country. The key to improving the
quality of health care is continuous high quality training and education.
3. Health Service Delivery and Organisation: A beneficial shift in the performance of the care
would be the reform of the service designs that focus on patient care. The main objective of
service reform has to be high quality, community-based and affordable care. The fundamental
concept of the care service reform is to provide the underprivileged regions with adequate care
(Kaplan et al., 2013).
11HEALTH WORK FORCE PLANNING – UGANDA
4. Technology: It is also important to invest in cost-effective data and communication technology
to support high-quality care. It helps to improve health training, patient centred approach to
individuals and quality health services.
5. Financing: Funds for developing stronger work force and high-quality care should also be
raised. Financing from national and foreign sources should be obtained. The funding can be split
into personal and government facilities to improve the care facilities and to improve the right
abilities, better working conditions and other elements (Apps.who.int, 2016).
6. Partnership and Cooperation: The most beneficial element in investing in adequate work
force growth and elevated standard of care are incorporation, civil society and cooperation
between domestic, global and regional industries and organisation (Nakanjako et al., 2015).
7. Data, information and accountability: health work force research and analysis with
harmonized techniques of business studies would help to develop the responsibility of the skilled
health care system and the collection of proof for human resources (Nutley & Reynolds, 2013).
8. Gender and Women Rights: Women's participation in certain institutions is a measure of
women's empowerment through adequate recruitment. The main focus for work force growth by
involving females in the industry is management, gender inequality and adequate training
(Apps.who.int, 2016).
9. International Migration: Recognizing the sophisticated global skills of employees could be an
essential element to retain and prevent qualified health employees from migrating. The adverse
impacts of the relocation of health workers would be reduced, as would the standard of care
(Lutwama, Roos & Dolamo, 2013).
4. Technology: It is also important to invest in cost-effective data and communication technology
to support high-quality care. It helps to improve health training, patient centred approach to
individuals and quality health services.
5. Financing: Funds for developing stronger work force and high-quality care should also be
raised. Financing from national and foreign sources should be obtained. The funding can be split
into personal and government facilities to improve the care facilities and to improve the right
abilities, better working conditions and other elements (Apps.who.int, 2016).
6. Partnership and Cooperation: The most beneficial element in investing in adequate work
force growth and elevated standard of care are incorporation, civil society and cooperation
between domestic, global and regional industries and organisation (Nakanjako et al., 2015).
7. Data, information and accountability: health work force research and analysis with
harmonized techniques of business studies would help to develop the responsibility of the skilled
health care system and the collection of proof for human resources (Nutley & Reynolds, 2013).
8. Gender and Women Rights: Women's participation in certain institutions is a measure of
women's empowerment through adequate recruitment. The main focus for work force growth by
involving females in the industry is management, gender inequality and adequate training
(Apps.who.int, 2016).
9. International Migration: Recognizing the sophisticated global skills of employees could be an
essential element to retain and prevent qualified health employees from migrating. The adverse
impacts of the relocation of health workers would be reduced, as would the standard of care
(Lutwama, Roos & Dolamo, 2013).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.