Comprehensive Analysis of Liver Cirrhosis: From Cause to Treatment
VerifiedAdded on 2023/05/28
|9
|2259
|189
Report
AI Summary
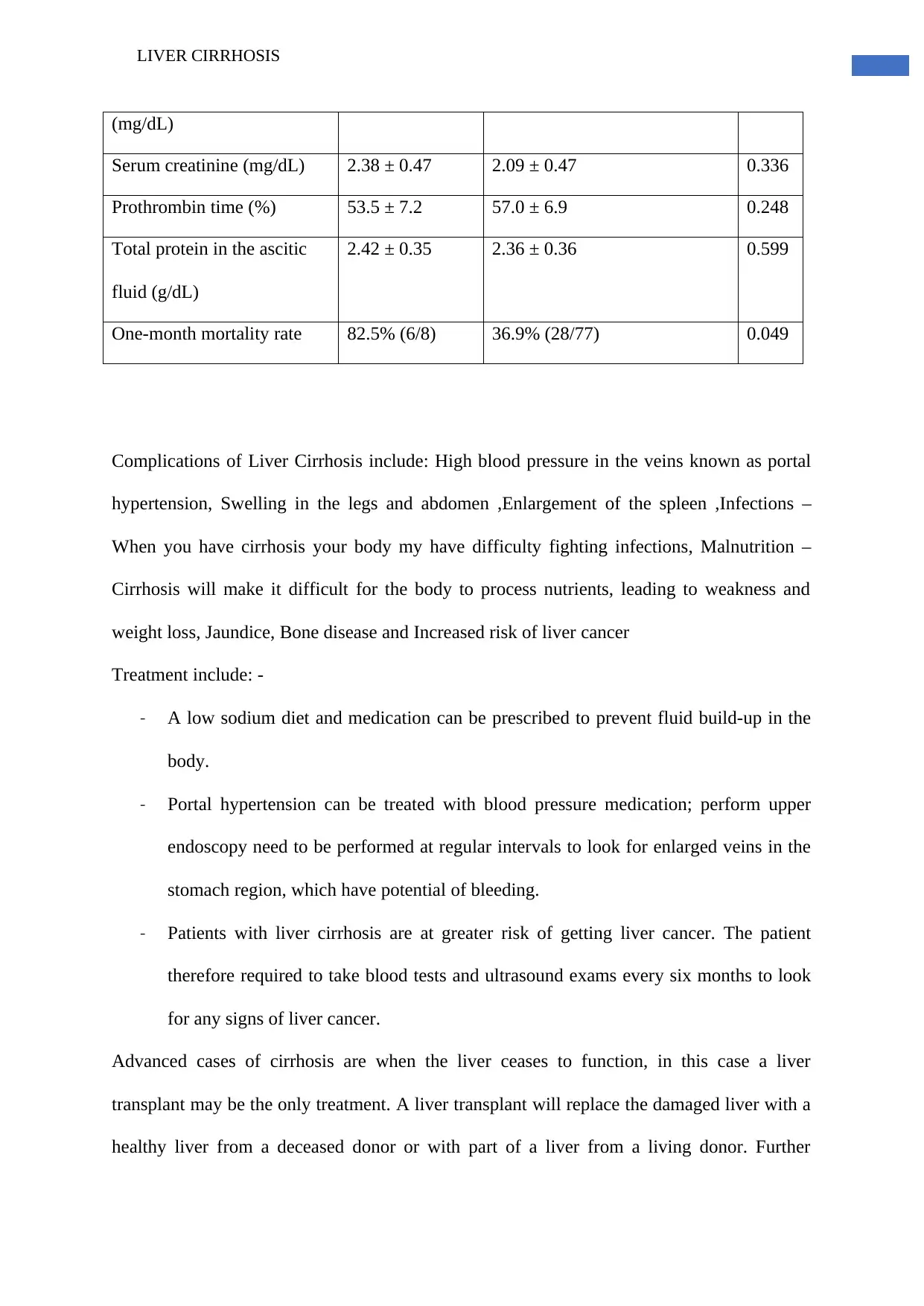
This project report provides a comprehensive analysis of liver cirrhosis, focusing on its causes, particularly the contribution of alcohol, symptoms, diagnostic procedures, and treatment options. It begins by outlining the anatomy and normal functions of the liver, followed by a detailed examination of alcohol's effects on the liver, leading to conditions like alcoholic hepatitis and cirrhosis. Diagnostic methods such as CT scans, MRI, blood tests, liver endoscopy, and biopsy are discussed, along with treatment strategies for managing liver cirrhosis and its complications, including portal hypertension, ascites, and increased risk of liver cancer. The report also presents experimental results comparing patients with fungal and bacterial infections related to liver cirrhosis, analyzing mortality rates and serological findings. It concludes by highlighting the importance of early diagnosis, lifestyle changes, and medical interventions to improve the condition and prevent further liver damage, emphasizing that Desklib offers a platform for students to access similar solved assignments and study resources.








1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.