CMHA OM005: Productivity Matrices Analysis of Emergency Department
VerifiedAdded on 2022/10/02
|6
|932
|423
Report
AI Summary
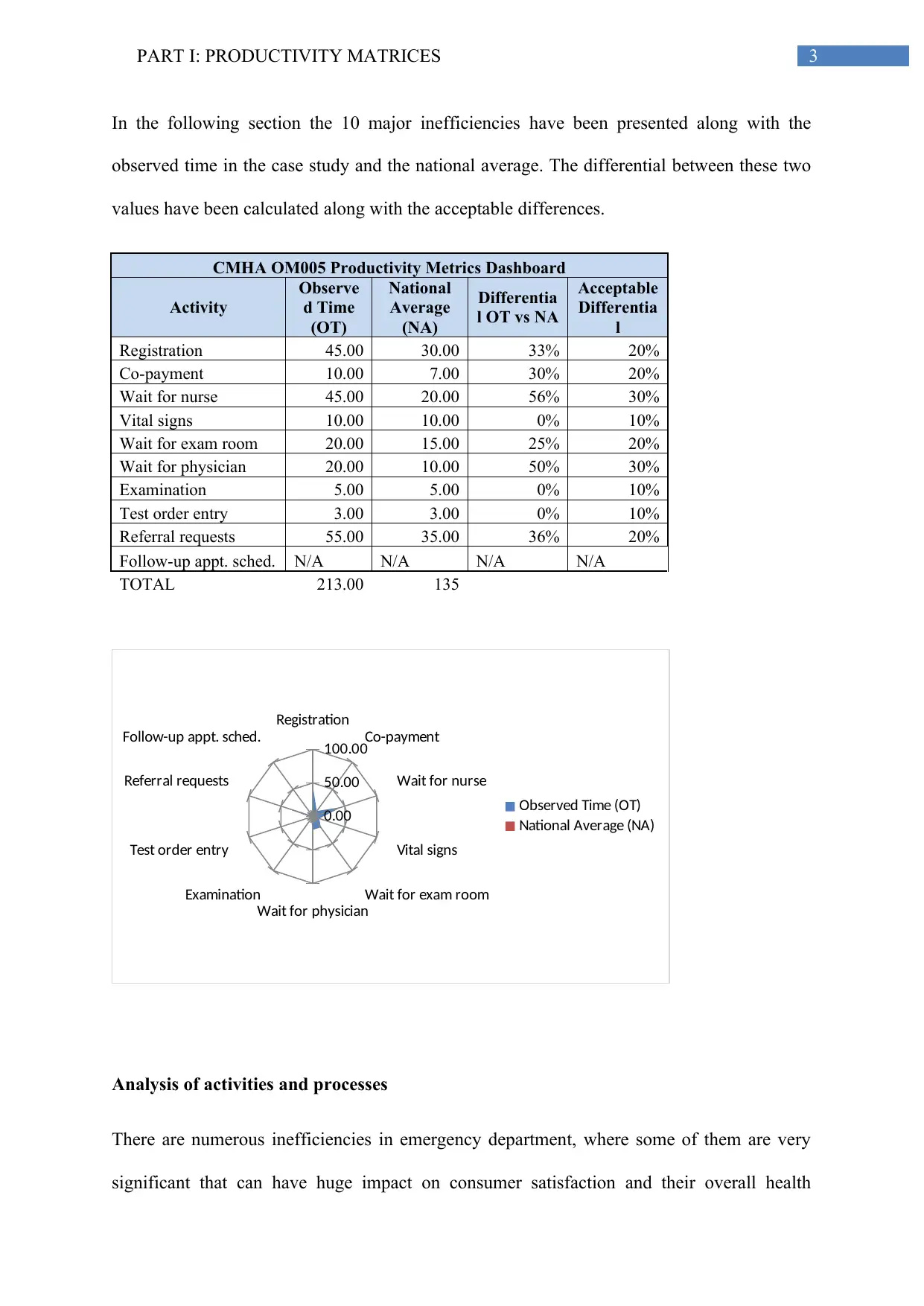
This report evaluates the productivity metrics of United General Hospital's emergency department based on a case study of a patient's experience. The analysis identifies ten major inefficiencies, including delays in registration, co-payment processing, waiting for nurses and physicians, and referral requests. The report compares observed times for these activities with national averages, calculating differentials and acceptable differences. It then focuses on the five most inefficient areas, providing rationales for their selection and reflecting the discrepancies with national benchmarks. The findings highlight significant areas for improvement, aiming to enhance patient satisfaction and overall healthcare delivery within the emergency department. The report also includes a bibliography of relevant sources to support the analysis.

1 out of 6
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.