Wearable Tech & Office Health: A Review of Pedometer Interventions
VerifiedAdded on 2023/06/04
|13
|4412
|197
Literature Review
AI Summary
This literature review explores the impact of pedometer interventions and wearable technology on the health and physical activity levels of office workers. It begins by defining physical activity and highlighting the global physical activity guidelines, emphasizing the disease and economic burden of physical inactivity. The review investigates the role of sedentary behavior and occupational factors in contributing to poor health outcomes. It further examines the potential benefits of physical activity interventions in the workplace, focusing on the effectiveness of pedometer-based programs and wearable technology in reducing sedentary time, improving cardio metabolic biomarkers, and increasing overall physical activity. The methodology section details the systematic approach used for the review, including the PICO framework and adherence to PRISMA guidelines. The objective is to determine whether wearable technology interventions improve cardio metabolic outcomes and increase physical activity levels among office workers, contributing to a better understanding of workplace health programs. Desklib provides access to this and other solved assignments.
Chapter 1
Introduction
Background:
1.1 Definition of physical activity
Physical activity is any movement of the body produced by muscles, which requires energy
outlay. This includes any movement that is done throughout the day except during lying down or
sitting still. For example; exercise, occupational work, housework, leisure time activity and
transportation (World Health Organization, 2018).
Physical activity can be categorized into light, moderate, or vigorous intensity level of physical
activity. Most health benefits have been associated with moderate to vigorous intensity physical
activity (National Advisory Committee on Health and Disability 1998; US Surgeon General
1996).
Light intensity physical activity does not cause noticeable increase in breathing rate and results
in small increase in energy expenditure, while moderate intensity physical activity (eg, brisk
walking), and vigorous physical activity (eg, jogging) both create noticeable increase in
breathing rate and energy expenditure (see glossary for further information).
Sedentary behavior indicate as the time spent lying or sitting and engaging in less than 30
minutes of moderate-intensity physical activity per week (Tremblay et al., 2018).
1.2 Physical activity guideline
There has been a dramatic increase in the rate of obesity in the western world. This has led to the
development of physical activity guidelines for the general public.
The Global physical activity Guidelines has recommended a minimum of 150-300 minutes of
moderate intensity physical activity per week, or 75-150 minutes of vigorous intensity physical
activity per week for adults aged 18-64 years. This recommendation has been proposed to gain
the health benefits along with reducing the risk of chronic illnesses (Who.int, 2018).
Additionally, World Health Organization recommended two or more days per week of a muscle
strengthening training involving main muscle groups. (Who.int, 2018).
1
Introduction
Background:
1.1 Definition of physical activity
Physical activity is any movement of the body produced by muscles, which requires energy
outlay. This includes any movement that is done throughout the day except during lying down or
sitting still. For example; exercise, occupational work, housework, leisure time activity and
transportation (World Health Organization, 2018).
Physical activity can be categorized into light, moderate, or vigorous intensity level of physical
activity. Most health benefits have been associated with moderate to vigorous intensity physical
activity (National Advisory Committee on Health and Disability 1998; US Surgeon General
1996).
Light intensity physical activity does not cause noticeable increase in breathing rate and results
in small increase in energy expenditure, while moderate intensity physical activity (eg, brisk
walking), and vigorous physical activity (eg, jogging) both create noticeable increase in
breathing rate and energy expenditure (see glossary for further information).
Sedentary behavior indicate as the time spent lying or sitting and engaging in less than 30
minutes of moderate-intensity physical activity per week (Tremblay et al., 2018).
1.2 Physical activity guideline
There has been a dramatic increase in the rate of obesity in the western world. This has led to the
development of physical activity guidelines for the general public.
The Global physical activity Guidelines has recommended a minimum of 150-300 minutes of
moderate intensity physical activity per week, or 75-150 minutes of vigorous intensity physical
activity per week for adults aged 18-64 years. This recommendation has been proposed to gain
the health benefits along with reducing the risk of chronic illnesses (Who.int, 2018).
Additionally, World Health Organization recommended two or more days per week of a muscle
strengthening training involving main muscle groups. (Who.int, 2018).
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1.3 Disease burden of physical inactivity
Physical inactivity is associated with poor health and well-being at all ages. It is considered to be
the fourth leading cause of death worldwide (Who.int, 2018), which leads it to be one of the
major public health concerns as it is estimated to cause 3.2 million mortalities annually, due to its
related diseases (Who.int, 2018).
One of the most significant challenges facing the global the global public health system is to
reverse the patterns of expanding physical inactivity that threaten the health and well-being of
the people. Individuals who are physically inactive are at 20-30% higher risk of dying compared
to individuals who are physical active (Who.int, 2018).
Physical inactivity is a lifestyle factor that is closely correlated with the development of many
chronic diseases. Hence, it is considered as the main intervention for primary and secondary
prevention of chronic disease (Durstine et al, 2013). Being physically active is essential for the
general health, beside the benefit in reducing the risk of chronic illnesses such as diabetes
mellitus, cardiovascular disease (CVD), hyper-lipidemia, HTN, stroke, cancers, osteoarthritis
and depression (MacEwen, MacDonald and Burr, 2015). Who.int, (2018) estimated that physical
inactivity cause 10-16% cases of colorectal carcinoma, breast cancer and type2 diabetes mellitus
and approximately 22% of ischemic heart diseases in both men and women globally (Who.int,
2018).
In the United Kingdom, physical inactivity cause 17-18.7% cases of breast and colorectal
carcinoma, 13% of type 2 diabetes mellitus,10.5% of coronary heart diseases and 16.9% of
premature mortalities from all causes (Ssehsactive.org.uk, 2018). It was presented that, women
spending at least 2 hours a week in moderate to vigorous activity can reduce the risk of breast
cancer by 5%, and up to 30% reduction in endometrial cancers (GOV.UK, 2018).
In addition, it was also reported by Weyerer (1992) that inactive individual have 3 times more
risk of developing moderate to severe depression than active individual (Weyerer, 1992), and
NICE guideline recommended, that individual with mild depression to be involved in a physical
activity program as a part of the treatment (GOV.UK, 2018).
1.4 Economic burden of physical inactivity
Statistics from 2009-2010 presented that physical inactivity direct cost to the United Kingdom
economy health care about £8.7 billion because of diagnosis of CVD and the total health care
cost on the economy was £18.9 billion (Ssehsactive.org.uk, 2018). Most recent data collected by
Clinical Commissioning Groups (CCGs) in 2013-2014 found that physical inactivity cost NHS
£455 million in England only (Assets.publishing.service.gov.uk, 2018).
In 2010/2011, it was estimated that coronary heart disease (CHD) would cost the NHS over £6.7
billion a year in the UK (Ssehsactive.org.uk, 2018), while data of 2012 revealed that, NHS spent
2
Physical inactivity is associated with poor health and well-being at all ages. It is considered to be
the fourth leading cause of death worldwide (Who.int, 2018), which leads it to be one of the
major public health concerns as it is estimated to cause 3.2 million mortalities annually, due to its
related diseases (Who.int, 2018).
One of the most significant challenges facing the global the global public health system is to
reverse the patterns of expanding physical inactivity that threaten the health and well-being of
the people. Individuals who are physically inactive are at 20-30% higher risk of dying compared
to individuals who are physical active (Who.int, 2018).
Physical inactivity is a lifestyle factor that is closely correlated with the development of many
chronic diseases. Hence, it is considered as the main intervention for primary and secondary
prevention of chronic disease (Durstine et al, 2013). Being physically active is essential for the
general health, beside the benefit in reducing the risk of chronic illnesses such as diabetes
mellitus, cardiovascular disease (CVD), hyper-lipidemia, HTN, stroke, cancers, osteoarthritis
and depression (MacEwen, MacDonald and Burr, 2015). Who.int, (2018) estimated that physical
inactivity cause 10-16% cases of colorectal carcinoma, breast cancer and type2 diabetes mellitus
and approximately 22% of ischemic heart diseases in both men and women globally (Who.int,
2018).
In the United Kingdom, physical inactivity cause 17-18.7% cases of breast and colorectal
carcinoma, 13% of type 2 diabetes mellitus,10.5% of coronary heart diseases and 16.9% of
premature mortalities from all causes (Ssehsactive.org.uk, 2018). It was presented that, women
spending at least 2 hours a week in moderate to vigorous activity can reduce the risk of breast
cancer by 5%, and up to 30% reduction in endometrial cancers (GOV.UK, 2018).
In addition, it was also reported by Weyerer (1992) that inactive individual have 3 times more
risk of developing moderate to severe depression than active individual (Weyerer, 1992), and
NICE guideline recommended, that individual with mild depression to be involved in a physical
activity program as a part of the treatment (GOV.UK, 2018).
1.4 Economic burden of physical inactivity
Statistics from 2009-2010 presented that physical inactivity direct cost to the United Kingdom
economy health care about £8.7 billion because of diagnosis of CVD and the total health care
cost on the economy was £18.9 billion (Ssehsactive.org.uk, 2018). Most recent data collected by
Clinical Commissioning Groups (CCGs) in 2013-2014 found that physical inactivity cost NHS
£455 million in England only (Assets.publishing.service.gov.uk, 2018).
In 2010/2011, it was estimated that coronary heart disease (CHD) would cost the NHS over £6.7
billion a year in the UK (Ssehsactive.org.uk, 2018), while data of 2012 revealed that, NHS spent
2
£8.8 billion in the direct (treatment, intervention and complication) NHS patient care for type 2
diabetes mellitus patients and estimated approximately £13 billion for the indirect (e.g loss of
productivity) cost (Ssehsactive.org.uk, 2018). The review of 2008/2009 statistics showed that
NHS spent £5.13 billion on all cancer treatments (Ssehsactive.org.uk, 2018). Moreover, diseases
related to overweight and obesity cost the NHS over £5 billion in 2006/07 (Ssehsactive.org.uk,
2018). Hence, these figures give estimation regarding the direct and indirect cost implication of
being physically inactive and suggest the need to implement interventions to promote physical
activity.
1.5 Sedentary behavior and Health
Population in the UK are about 20% inactive now than 1960s, and its estimated by 2030,
approximately 35% of them will be physically inactive, if the existing trend of inactivity
continues (GOV.UK, 2018).There are many factors found to be influencing physical inactivity.
One of the major cause is the domination of passive modes of transportation, which is associated
with decreased level of activity (GOV.UK, 2018) as well as an increase in the sedentary behavior
during occupational domestic activaties (GOV.UK, 2018). Furthermore, increase in urbanization
(which leads to several environmental factors) may discourage involvement in physical activity
E.g: air pollution, increase in traffic, violence and lack of sidewalks, parks, and sports/recreation
facilities. (Who.int, 2018).
1.6 Occupational related illness
The work environment and characteristics of work also has a major role in influencing health
outcome of people. Majority of existing sedentary behavior is linked with the large proportion of
employees spending the day sitting in front of desktop computers (Carr et al., 2016).
Since 1950, sedentary occupations have increased for approximately 83%, and it accounts for
about 43% of jobs in the U.S (Carr et al., 2016), and 70% in the UK (GOV.UK, 2018).
More precisely, time spent sitting is significantly associated with increase in the risks of
developing metabolic syndrome, obesity, and type-2 diabetes mellitus (MacEwen, MacDonald
and Burr, 2015). In addition, upper body musculoskeletal symptoms and disorders were also
associated with sedentary computer work (Carr et al., 2016). It has been found that 1 in 3 of the
working age individuals have a minimum of one long term chronic disease and 1 in 7 having
more than one chronic disease (GOV.UK, 2018).
Hence, workplace has become a main target for health promotion programs intending to increase
physical activity level and prevent chronic illnesses (WHO/WEF 2008).
3
diabetes mellitus patients and estimated approximately £13 billion for the indirect (e.g loss of
productivity) cost (Ssehsactive.org.uk, 2018). The review of 2008/2009 statistics showed that
NHS spent £5.13 billion on all cancer treatments (Ssehsactive.org.uk, 2018). Moreover, diseases
related to overweight and obesity cost the NHS over £5 billion in 2006/07 (Ssehsactive.org.uk,
2018). Hence, these figures give estimation regarding the direct and indirect cost implication of
being physically inactive and suggest the need to implement interventions to promote physical
activity.
1.5 Sedentary behavior and Health
Population in the UK are about 20% inactive now than 1960s, and its estimated by 2030,
approximately 35% of them will be physically inactive, if the existing trend of inactivity
continues (GOV.UK, 2018).There are many factors found to be influencing physical inactivity.
One of the major cause is the domination of passive modes of transportation, which is associated
with decreased level of activity (GOV.UK, 2018) as well as an increase in the sedentary behavior
during occupational domestic activaties (GOV.UK, 2018). Furthermore, increase in urbanization
(which leads to several environmental factors) may discourage involvement in physical activity
E.g: air pollution, increase in traffic, violence and lack of sidewalks, parks, and sports/recreation
facilities. (Who.int, 2018).
1.6 Occupational related illness
The work environment and characteristics of work also has a major role in influencing health
outcome of people. Majority of existing sedentary behavior is linked with the large proportion of
employees spending the day sitting in front of desktop computers (Carr et al., 2016).
Since 1950, sedentary occupations have increased for approximately 83%, and it accounts for
about 43% of jobs in the U.S (Carr et al., 2016), and 70% in the UK (GOV.UK, 2018).
More precisely, time spent sitting is significantly associated with increase in the risks of
developing metabolic syndrome, obesity, and type-2 diabetes mellitus (MacEwen, MacDonald
and Burr, 2015). In addition, upper body musculoskeletal symptoms and disorders were also
associated with sedentary computer work (Carr et al., 2016). It has been found that 1 in 3 of the
working age individuals have a minimum of one long term chronic disease and 1 in 7 having
more than one chronic disease (GOV.UK, 2018).
Hence, workplace has become a main target for health promotion programs intending to increase
physical activity level and prevent chronic illnesses (WHO/WEF 2008).
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1.7 Benefits of physical activity interventions in the workplace
Introducing physical activity programs in the workplace can lead to varying success rates in the
reduction of employee absence over a year. Additional benefit of the physical activity program is
that it would lead to an increase in physical activity and decrease in sedentary time (WHO/WEF
2008; Ssehsactive.org.uk, 2018). It was elaborated that, if the program is 1% effective in
reducing the number of absenteeism’s, the employers will have possibility to save between
£2,870 and £6,244 every year. If the program was 50% effective in increasing physical activity
level among employees and decrease in number of absentees, the employer will save over
£312,217 per year (Ssehsactive.org.uk, 2018).
Surveys such as that conducted by KATZMARZYK et al. (2009) showed that individual who
spends more time sitting have increased risk of death more than who stands and walk during
worktime, despite their physical activity level. An independent association between body mass
index (BMI) and both deaths and spending time sitting is also seen (KATZMARZYK et al.,
2009).
To date, a considerable amount of literatures have been published that reveals overall
effectiveness of existing workplace interventions in reducing sedentary time, improving cardio-
metabolic biomarkers and increasing physical activity. These studies have examined different
types of interventions including the use of wearable technology devices, such as pedometers in
promoting physical activity. Nevertheless, a trend of step counting has come up targeting ‘10,000
step per day’ with the increase use of pedometers, which has been implemented in numerous
intervention studies. One example includes implementation of a multi- approach physical activity
intervention in a big community “10,000 Steps Ghent” which offered an opportunity to assess
the outcomes of a whole-community physical activity intervention on sitting time (De Cocker et
al., 2007).
In recent years, many studies have focused on the usage and the feasibility of sit-stand and
treadmill workstations, which yielded positive physical and psychological outcome as seen in the
systematic review study done by MacEwen, MacDonald and Burr (2015). Loitz et al. (2015)
conducted a review of different types of workplace interventions, which included active
workstations, educational, counseling and challenging or competition interventions and revealed
a significant effect of different interventions on decreasing sedentary time and increasing
physical activity.
A number of researchers have reported from different trials of pedometer based interventions an
effectiveness of pedometer in increasing level of physical activity and its positive effect on the
cardio-metabolic bio markers as it delivers direct, detailed feedback on the levels of physical
activity. Such interventions can motivate individuals to increase their physical activity over time
(Matevey et al., 2006).
4
Introducing physical activity programs in the workplace can lead to varying success rates in the
reduction of employee absence over a year. Additional benefit of the physical activity program is
that it would lead to an increase in physical activity and decrease in sedentary time (WHO/WEF
2008; Ssehsactive.org.uk, 2018). It was elaborated that, if the program is 1% effective in
reducing the number of absenteeism’s, the employers will have possibility to save between
£2,870 and £6,244 every year. If the program was 50% effective in increasing physical activity
level among employees and decrease in number of absentees, the employer will save over
£312,217 per year (Ssehsactive.org.uk, 2018).
Surveys such as that conducted by KATZMARZYK et al. (2009) showed that individual who
spends more time sitting have increased risk of death more than who stands and walk during
worktime, despite their physical activity level. An independent association between body mass
index (BMI) and both deaths and spending time sitting is also seen (KATZMARZYK et al.,
2009).
To date, a considerable amount of literatures have been published that reveals overall
effectiveness of existing workplace interventions in reducing sedentary time, improving cardio-
metabolic biomarkers and increasing physical activity. These studies have examined different
types of interventions including the use of wearable technology devices, such as pedometers in
promoting physical activity. Nevertheless, a trend of step counting has come up targeting ‘10,000
step per day’ with the increase use of pedometers, which has been implemented in numerous
intervention studies. One example includes implementation of a multi- approach physical activity
intervention in a big community “10,000 Steps Ghent” which offered an opportunity to assess
the outcomes of a whole-community physical activity intervention on sitting time (De Cocker et
al., 2007).
In recent years, many studies have focused on the usage and the feasibility of sit-stand and
treadmill workstations, which yielded positive physical and psychological outcome as seen in the
systematic review study done by MacEwen, MacDonald and Burr (2015). Loitz et al. (2015)
conducted a review of different types of workplace interventions, which included active
workstations, educational, counseling and challenging or competition interventions and revealed
a significant effect of different interventions on decreasing sedentary time and increasing
physical activity.
A number of researchers have reported from different trials of pedometer based interventions an
effectiveness of pedometer in increasing level of physical activity and its positive effect on the
cardio-metabolic bio markers as it delivers direct, detailed feedback on the levels of physical
activity. Such interventions can motivate individuals to increase their physical activity over time
(Matevey et al., 2006).
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
World Economic Forum and World Health Organization (WHO/WEF 2008) have
recommended that more research is required to reinforce current
understanding of work place health programs, especially on the
effectiveness and the usage of simple gadgets.
Hence, the objective of this literature review to explore existing literatures examining the amount
of health benefits from the use of pedometer interventions and to determine whether wearable
technology intervention improves cardio metabolic outcomes in office workers or not. The
research also aims to analyze whether wearable technology intervention increases the level of
physical activity in office workers or not.
5
recommended that more research is required to reinforce current
understanding of work place health programs, especially on the
effectiveness and the usage of simple gadgets.
Hence, the objective of this literature review to explore existing literatures examining the amount
of health benefits from the use of pedometer interventions and to determine whether wearable
technology intervention improves cardio metabolic outcomes in office workers or not. The
research also aims to analyze whether wearable technology intervention increases the level of
physical activity in office workers or not.
5
Chapter 2.
Methodology
2.1 Study design:
As the main purpose of this study is to explore the benefit of different pedometer intervention on
increasing level of physical activity among workers, secondary research design is considered
appropriate for this research design. Secondary research design is appropriate when the purpose
is to clarify the research question and understand the applicability of past research in a large
scale (Walliman 2017). Literature review using systematic method has been used to retrieve both
qualitative and quantitative research papers on the research topic. The main benefits of using this
type of research design is that it is a rigorous and transparent form of literature review and it has
the potential to generate a robust answer to a research question (Mallett et al. 2012) The step that
has been used in conducting a systematic review is deconstruction of research question using the
population, intervention, outcome and comparator (PICO). The next step was to develop search
strategy and retrieve relevant articles from academic and institutional databases. Inclusion and
exclusion criteria were defined and the detailed process to screen and select research articles
were provided. The final part of the methodology will define the approach needed to directly
compare and interpret results and determine the implications for application in target setting.
To enhance the quality of reporting of the research, the PRISMA (Preferred Reporting Items for
Systematic Reviews and Meta-Analyses) guidelines were followed. It is an evidence based
document that defines the list of items that is necessary while reporting in systematic (Moher et
al. 2015). Hence, adherence to the PRISMA guideline can promote transparency of the work.
2.2 PICO question:
The first step of the literature review is to deconstruct the research question and define the PICO
for the study. Based on the analysis of research objective, it can be said that the main question
for the review are as follows:
How effective is pedometer intervention and wearable technology intervention in
improving cardio metabolic outcome and increasing physical activity in office workers compared
to no intervention?
After the deconstruction of the research question, the following information emerged:
P (Population): Office workers or employee
I (Intervention): pedometer intervention and wearable technology intervention
C (Comparator): no intervention
Outcome: Improving cardio metabolic outcome and increasing physical activity
The deconstruction of the question will help to define search strategy and identify appropriate
terms that can be used for the search process. This has informed developing inclusion and
exclusion criteria too.
2.3 Eligibility criteria:
6
Methodology
2.1 Study design:
As the main purpose of this study is to explore the benefit of different pedometer intervention on
increasing level of physical activity among workers, secondary research design is considered
appropriate for this research design. Secondary research design is appropriate when the purpose
is to clarify the research question and understand the applicability of past research in a large
scale (Walliman 2017). Literature review using systematic method has been used to retrieve both
qualitative and quantitative research papers on the research topic. The main benefits of using this
type of research design is that it is a rigorous and transparent form of literature review and it has
the potential to generate a robust answer to a research question (Mallett et al. 2012) The step that
has been used in conducting a systematic review is deconstruction of research question using the
population, intervention, outcome and comparator (PICO). The next step was to develop search
strategy and retrieve relevant articles from academic and institutional databases. Inclusion and
exclusion criteria were defined and the detailed process to screen and select research articles
were provided. The final part of the methodology will define the approach needed to directly
compare and interpret results and determine the implications for application in target setting.
To enhance the quality of reporting of the research, the PRISMA (Preferred Reporting Items for
Systematic Reviews and Meta-Analyses) guidelines were followed. It is an evidence based
document that defines the list of items that is necessary while reporting in systematic (Moher et
al. 2015). Hence, adherence to the PRISMA guideline can promote transparency of the work.
2.2 PICO question:
The first step of the literature review is to deconstruct the research question and define the PICO
for the study. Based on the analysis of research objective, it can be said that the main question
for the review are as follows:
How effective is pedometer intervention and wearable technology intervention in
improving cardio metabolic outcome and increasing physical activity in office workers compared
to no intervention?
After the deconstruction of the research question, the following information emerged:
P (Population): Office workers or employee
I (Intervention): pedometer intervention and wearable technology intervention
C (Comparator): no intervention
Outcome: Improving cardio metabolic outcome and increasing physical activity
The deconstruction of the question will help to define search strategy and identify appropriate
terms that can be used for the search process. This has informed developing inclusion and
exclusion criteria too.
2.3 Eligibility criteria:
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Defining eligibility criteria is necessary to get necessary guidance regarding the approach used to
search for relevant research papers for the review.
Studies were evaluated for eligibility according to the following inclusion criteria:
1. Population: Only those research papers were reviewed that has taken office workers or
employees as the main research participant. Adults above 18 years were taken as the age
limit so that children and adolescent group is not taken for the review.
2. Intervention: Any intervention that used used wearable technology or pedometer were
included in the review
3. Outcome: Only thus studies were included which reported about level of physical activity
and cardiometabolic outcome
4. Time period: Only those studies were included in the literature review which were
published within 2008 to 2018
5. Types of studies: Both qualitative and quantitative research were included if they met the
above inclusion criteria.
6. Language: All research papers must be published in English.
2.4 Exclusion criteria:
(1) Studies which included beside wearable technology device another intervention.
(2) Studies which used the wearable device for measuring only were excluded.
(3) Studies which were not office-based workplace were excluded.
2.5 Types of outcome measures:
2.5.1 Primary outcomes:
The primary outcome for this literature was measuring the cardiovascular
biomarkers
o Biochemical measures for e.g; blood cholesterol (total
cholesterol, LDL, HDL, blood triglycerides) and blood glucose.
o Anthropometric measures such as; body mass index and body
fat.
o Blood pressure for example; diastolic blood pressure and systolic
blood pressure.
2.5.2 Secondary outcomes:
The secondary outcome is measuring the level of physical activity, self-
reported, using personal calendar or website diary such as;
www.peifirststep.ca.
7
search for relevant research papers for the review.
Studies were evaluated for eligibility according to the following inclusion criteria:
1. Population: Only those research papers were reviewed that has taken office workers or
employees as the main research participant. Adults above 18 years were taken as the age
limit so that children and adolescent group is not taken for the review.
2. Intervention: Any intervention that used used wearable technology or pedometer were
included in the review
3. Outcome: Only thus studies were included which reported about level of physical activity
and cardiometabolic outcome
4. Time period: Only those studies were included in the literature review which were
published within 2008 to 2018
5. Types of studies: Both qualitative and quantitative research were included if they met the
above inclusion criteria.
6. Language: All research papers must be published in English.
2.4 Exclusion criteria:
(1) Studies which included beside wearable technology device another intervention.
(2) Studies which used the wearable device for measuring only were excluded.
(3) Studies which were not office-based workplace were excluded.
2.5 Types of outcome measures:
2.5.1 Primary outcomes:
The primary outcome for this literature was measuring the cardiovascular
biomarkers
o Biochemical measures for e.g; blood cholesterol (total
cholesterol, LDL, HDL, blood triglycerides) and blood glucose.
o Anthropometric measures such as; body mass index and body
fat.
o Blood pressure for example; diastolic blood pressure and systolic
blood pressure.
2.5.2 Secondary outcomes:
The secondary outcome is measuring the level of physical activity, self-
reported, using personal calendar or website diary such as;
www.peifirststep.ca.
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
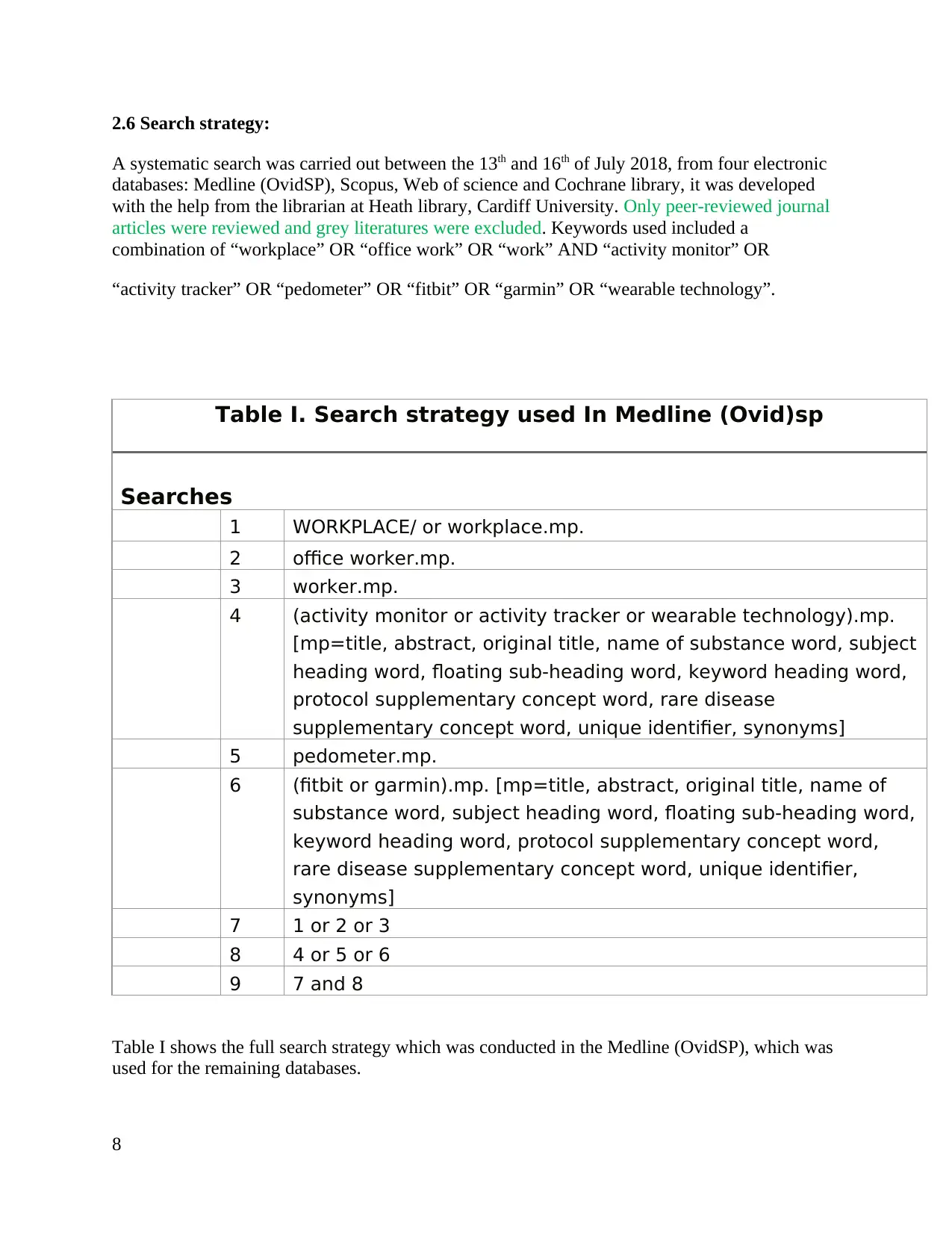
2.6 Search strategy:
A systematic search was carried out between the 13th and 16th of July 2018, from four electronic
databases: Medline (OvidSP), Scopus, Web of science and Cochrane library, it was developed
with the help from the librarian at Heath library, Cardiff University. Only peer-reviewed journal
articles were reviewed and grey literatures were excluded. Keywords used included a
combination of “workplace” OR “office work” OR “work” AND “activity monitor” OR
“activity tracker” OR “pedometer” OR “fitbit” OR “garmin” OR “wearable technology”.
Table I. Search strategy used In Medline (Ovid)sp
Searches
1 WORKPLACE/ or workplace.mp.
2 office worker.mp.
3 worker.mp.
4 (activity monitor or activity tracker or wearable technology).mp.
[mp=title, abstract, original title, name of substance word, subject
heading word, floating sub-heading word, keyword heading word,
protocol supplementary concept word, rare disease
supplementary concept word, unique identifier, synonyms]
5 pedometer.mp.
6 (fitbit or garmin).mp. [mp=title, abstract, original title, name of
substance word, subject heading word, floating sub-heading word,
keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier,
synonyms]
7 1 or 2 or 3
8 4 or 5 or 6
9 7 and 8
Table I shows the full search strategy which was conducted in the Medline (OvidSP), which was
used for the remaining databases.
8
A systematic search was carried out between the 13th and 16th of July 2018, from four electronic
databases: Medline (OvidSP), Scopus, Web of science and Cochrane library, it was developed
with the help from the librarian at Heath library, Cardiff University. Only peer-reviewed journal
articles were reviewed and grey literatures were excluded. Keywords used included a
combination of “workplace” OR “office work” OR “work” AND “activity monitor” OR
“activity tracker” OR “pedometer” OR “fitbit” OR “garmin” OR “wearable technology”.
Table I. Search strategy used In Medline (Ovid)sp
Searches
1 WORKPLACE/ or workplace.mp.
2 office worker.mp.
3 worker.mp.
4 (activity monitor or activity tracker or wearable technology).mp.
[mp=title, abstract, original title, name of substance word, subject
heading word, floating sub-heading word, keyword heading word,
protocol supplementary concept word, rare disease
supplementary concept word, unique identifier, synonyms]
5 pedometer.mp.
6 (fitbit or garmin).mp. [mp=title, abstract, original title, name of
substance word, subject heading word, floating sub-heading word,
keyword heading word, protocol supplementary concept word,
rare disease supplementary concept word, unique identifier,
synonyms]
7 1 or 2 or 3
8 4 or 5 or 6
9 7 and 8
Table I shows the full search strategy which was conducted in the Medline (OvidSP), which was
used for the remaining databases.
8
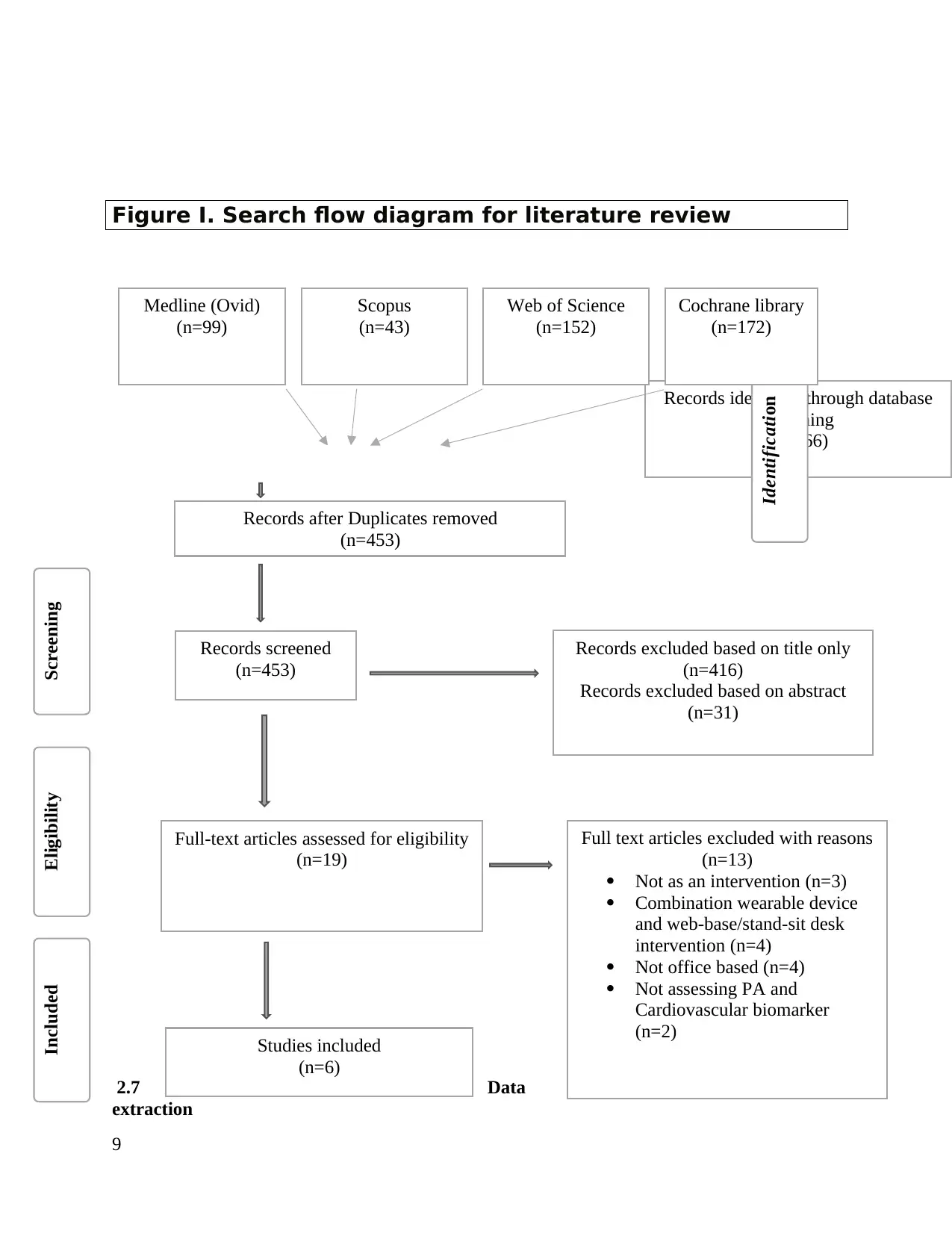
Figure I. Search flow diagram for literature review
2.7 Data
extraction
9
Records identified through database
searching
(n=466)
Studies included
(n=6)
Records after Duplicates removed
(n=453)
Records screened
(n=453)
Full text articles excluded with reasons
(n=13)
Not as an intervention (n=3)
Combination wearable device
and web-base/stand-sit desk
intervention (n=4)
Not office based (n=4)
Not assessing PA and
Cardiovascular biomarker
(n=2)
Full-text articles assessed for eligibility
(n=19)
Records excluded based on title only
(n=416)
Records excluded based on abstract
(n=31)
Identification
ScreeningEligibilityIncluded
Medline (Ovid)
(n=99)
Scopus
(n=43)
Web of Science
(n=152)
Cochrane library
(n=172)
2.7 Data
extraction
9
Records identified through database
searching
(n=466)
Studies included
(n=6)
Records after Duplicates removed
(n=453)
Records screened
(n=453)
Full text articles excluded with reasons
(n=13)
Not as an intervention (n=3)
Combination wearable device
and web-base/stand-sit desk
intervention (n=4)
Not office based (n=4)
Not assessing PA and
Cardiovascular biomarker
(n=2)
Full-text articles assessed for eligibility
(n=19)
Records excluded based on title only
(n=416)
Records excluded based on abstract
(n=31)
Identification
ScreeningEligibilityIncluded
Medline (Ovid)
(n=99)
Scopus
(n=43)
Web of Science
(n=152)
Cochrane library
(n=172)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Data extraction was done by developing a summary table and extracting information related to
research design, participant, intervention type, outcome and findings.
2.8 Study selection:
After entering the search terms in relevant databases, all the studies were screening according to title and
abstract. Studies were included for screening if they were in relevance with the research question. Once relevant
papers were identified, the remaining articles were screened based on inclusion and exclusion criteria. The final
eligibility criteria was to ensure that appropriate research design was used and any disagreement regarding exclusion
was discussed with other research members. In this way, only those studies were included for which consensus was
achieved. The details for this have been provided in the result section.
2.9 Data analysis:
The assessment of rigor for the selected studies was done using validated Cochrane risk of bias assessment tool. As
both quantitative and qualitative papers were included in the literature review, different data analysis method was
taken for qualitative and quantitative papers. For quantitative data, statistical test like correlation test was done to
find relationship between two quantitative variables used in the study. In addition, for papers using qualitative
approach, data analyse was done by finding common themes from the study and using those theme to makes
conclusion about the impact of the chosen intervention on level of physical activities among employee.
Chapter 3: Results
Results:
Literature search yielded 466 studies. Initially, the articles were selected by screening the titles,
screening the abstracts for information about the outcomes and the intervention, and exploring
the entire paper, if the title and abstract did not specify enough information to decide if it met the
inclusion criteria. articles which have not meet the inclusion criteria were excluded.
Nineteen papers selected, thirteen were excluded after exploring entire paper, three of the
article’s pedometer was not used as an intervention, four studies had a combination of wearable
device with other interventions such as: web-based intervention and sit-stand desk, four studies
were not office-based intervention and two studies did not assess physical activity and
cardiovascular biomarker as their primary and secondary outcomes. Reporting six studies, met
the inclusion criteria. Additional searches were done from the included articles
references.
Studies included in this review are which having pedometer as the only
component of intervention but was reinforced by additional components of
the intervention such as; diaries, step counts or rewards in order to increase
the motivation.
10
research design, participant, intervention type, outcome and findings.
2.8 Study selection:
After entering the search terms in relevant databases, all the studies were screening according to title and
abstract. Studies were included for screening if they were in relevance with the research question. Once relevant
papers were identified, the remaining articles were screened based on inclusion and exclusion criteria. The final
eligibility criteria was to ensure that appropriate research design was used and any disagreement regarding exclusion
was discussed with other research members. In this way, only those studies were included for which consensus was
achieved. The details for this have been provided in the result section.
2.9 Data analysis:
The assessment of rigor for the selected studies was done using validated Cochrane risk of bias assessment tool. As
both quantitative and qualitative papers were included in the literature review, different data analysis method was
taken for qualitative and quantitative papers. For quantitative data, statistical test like correlation test was done to
find relationship between two quantitative variables used in the study. In addition, for papers using qualitative
approach, data analyse was done by finding common themes from the study and using those theme to makes
conclusion about the impact of the chosen intervention on level of physical activities among employee.
Chapter 3: Results
Results:
Literature search yielded 466 studies. Initially, the articles were selected by screening the titles,
screening the abstracts for information about the outcomes and the intervention, and exploring
the entire paper, if the title and abstract did not specify enough information to decide if it met the
inclusion criteria. articles which have not meet the inclusion criteria were excluded.
Nineteen papers selected, thirteen were excluded after exploring entire paper, three of the
article’s pedometer was not used as an intervention, four studies had a combination of wearable
device with other interventions such as: web-based intervention and sit-stand desk, four studies
were not office-based intervention and two studies did not assess physical activity and
cardiovascular biomarker as their primary and secondary outcomes. Reporting six studies, met
the inclusion criteria. Additional searches were done from the included articles
references.
Studies included in this review are which having pedometer as the only
component of intervention but was reinforced by additional components of
the intervention such as; diaries, step counts or rewards in order to increase
the motivation.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Reference’s:
1- Who.int. (2018). WHO | Physical Activity and Adults. [online] Available at:
http://www.who.int/dietphysicalactivity/factsheet_adults/en/ [Accessed 12 Jul. 2018].
2- Carr, L., Leonhard, C., Tucker, S., Fethke, N., Benzo, R. and Gerr, F. (2016). Total Worker
Health Intervention Increases Activity of Sedentary Workers. American Journal of Preventive
Medicine, 50(1), pp.9-17.
3- MacEwen, B., MacDonald, D. and Burr, J. (2015). A systematic review of standing and
treadmill desks in the workplace. Preventive Medicine, 70, pp.50-58.
4- KATZMARZYK, P., CHURCH, T., CRAIG, C. and BOUCHARD, C. (2009). Sitting Time
and Mortality from All Causes, Cardiovascular Disease, and Cancer. Medicine & Science in
Sports & Exercise, 41(5), pp.998-1005.
5- De Cocker, K., De Bourdeaudhuij, I., Brown, W. and Cardon, G. (2008). The effect of a
pedometer-based physical activity intervention on sitting time. Preventive Medicine, 47(2),
pp.179-181.
6- De Cocker, K., De Bourdeaudhuij, I., Brown, W. and Cardon, G. (2007). Effects of “10,000
Steps Ghent”: A Whole-Community Intervention. [online] 33(6), pp.455-463. Available at:
https://doi.org/10.1016/j.amepre.2007.07.037 [Accessed 12 Jul. 2018].
7- Assets.publishing.service.gov.uk. (2018). [online] Available at:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/
file/524234/Physical_inactivity_costs_to_CCGs.pdf [Accessed 18 Jul. 2018].
11
1- Who.int. (2018). WHO | Physical Activity and Adults. [online] Available at:
http://www.who.int/dietphysicalactivity/factsheet_adults/en/ [Accessed 12 Jul. 2018].
2- Carr, L., Leonhard, C., Tucker, S., Fethke, N., Benzo, R. and Gerr, F. (2016). Total Worker
Health Intervention Increases Activity of Sedentary Workers. American Journal of Preventive
Medicine, 50(1), pp.9-17.
3- MacEwen, B., MacDonald, D. and Burr, J. (2015). A systematic review of standing and
treadmill desks in the workplace. Preventive Medicine, 70, pp.50-58.
4- KATZMARZYK, P., CHURCH, T., CRAIG, C. and BOUCHARD, C. (2009). Sitting Time
and Mortality from All Causes, Cardiovascular Disease, and Cancer. Medicine & Science in
Sports & Exercise, 41(5), pp.998-1005.
5- De Cocker, K., De Bourdeaudhuij, I., Brown, W. and Cardon, G. (2008). The effect of a
pedometer-based physical activity intervention on sitting time. Preventive Medicine, 47(2),
pp.179-181.
6- De Cocker, K., De Bourdeaudhuij, I., Brown, W. and Cardon, G. (2007). Effects of “10,000
Steps Ghent”: A Whole-Community Intervention. [online] 33(6), pp.455-463. Available at:
https://doi.org/10.1016/j.amepre.2007.07.037 [Accessed 12 Jul. 2018].
7- Assets.publishing.service.gov.uk. (2018). [online] Available at:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/
file/524234/Physical_inactivity_costs_to_CCGs.pdf [Accessed 18 Jul. 2018].
11
8- Ssehsactive.org.uk. (2018). [online] Available at:
http://www.ssehsactive.org.uk/userfiles/Documents/eonomiccosts.pdf [Accessed 18 Jul.
2018].
9- Weyerer, S. (1992). Physical Inactivity and Depression in the Community. International
Journal of Sports Medicine, 13(06), pp.492-496.
10- GOV.UK. (2018). Health matters: getting every adult active every day. [online] Available at:
https://www.gov.uk/government/publications/health-matters-getting-every-adult-active-every-
day/health-matters-getting-every-adult-active-every-day [Accessed 18 Jul. 2018].
11- Who.int. (2018). WHO | Physical Inactivity: A Global Public Health Problem. [online]
Available at: http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/ [Accessed 18
Jul. 2018].
12- Loitz, C., Potter, R., Walker, J., McLeod, N. and Johnston, N. (2015). The effectiveness of
workplace interventions to increase physical activity and decrease sedentary behaviour in
adults: protocol for a systematic review. Systematic Reviews, 4(1).
13- Matevey, C., Rogers, L., Dawson, E. and Tudor-Locke, C. (2006). Lack of Reactivity During
Pedometer Self-Monitoring in Adults. Measurement in Physical Education and Exercise
Science, 10(1), pp.1-11.
14- World Health Organization. (2018). Physical Activity. [online] Available at:
https://www.who.int/dietphysicalactivity/pa/en/
15- World Health Organization/World Economic Forum (WHO/WEF). Preventing
noncommunicable diseases in the workplace through diet and physical activity: WHO/World
Economic Forum report of a joint event. Geneva: World Health Organization, 2008.
16- Durstine, J.L., Gordon, B., Wang, Z. and Luo, X., 2013. Chronic disease and the link to
physical activity. Journal of Sport and Health Science, 2(1), pp.3-11.
17- Mallett, R., Hagen-Zanker, J., Slater, R. and Duvendack, M., 2012. The benefits and
challenges of using systematic reviews in international development research. Journal of
development effectiveness, 4(3), pp.445-455.
18- Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., Shekelle, P. and
Stewart, L.A., 2015. Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), p.1.
12
http://www.ssehsactive.org.uk/userfiles/Documents/eonomiccosts.pdf [Accessed 18 Jul.
2018].
9- Weyerer, S. (1992). Physical Inactivity and Depression in the Community. International
Journal of Sports Medicine, 13(06), pp.492-496.
10- GOV.UK. (2018). Health matters: getting every adult active every day. [online] Available at:
https://www.gov.uk/government/publications/health-matters-getting-every-adult-active-every-
day/health-matters-getting-every-adult-active-every-day [Accessed 18 Jul. 2018].
11- Who.int. (2018). WHO | Physical Inactivity: A Global Public Health Problem. [online]
Available at: http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/ [Accessed 18
Jul. 2018].
12- Loitz, C., Potter, R., Walker, J., McLeod, N. and Johnston, N. (2015). The effectiveness of
workplace interventions to increase physical activity and decrease sedentary behaviour in
adults: protocol for a systematic review. Systematic Reviews, 4(1).
13- Matevey, C., Rogers, L., Dawson, E. and Tudor-Locke, C. (2006). Lack of Reactivity During
Pedometer Self-Monitoring in Adults. Measurement in Physical Education and Exercise
Science, 10(1), pp.1-11.
14- World Health Organization. (2018). Physical Activity. [online] Available at:
https://www.who.int/dietphysicalactivity/pa/en/
15- World Health Organization/World Economic Forum (WHO/WEF). Preventing
noncommunicable diseases in the workplace through diet and physical activity: WHO/World
Economic Forum report of a joint event. Geneva: World Health Organization, 2008.
16- Durstine, J.L., Gordon, B., Wang, Z. and Luo, X., 2013. Chronic disease and the link to
physical activity. Journal of Sport and Health Science, 2(1), pp.3-11.
17- Mallett, R., Hagen-Zanker, J., Slater, R. and Duvendack, M., 2012. The benefits and
challenges of using systematic reviews in international development research. Journal of
development effectiveness, 4(3), pp.445-455.
18- Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., Shekelle, P. and
Stewart, L.A., 2015. Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), p.1.
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.