BSBWHS401 Assessment 2: Incident Report, Training Plan and Agreement
VerifiedAdded on 2023/01/12
|4
|455
|37
Homework Assignment
AI Summary
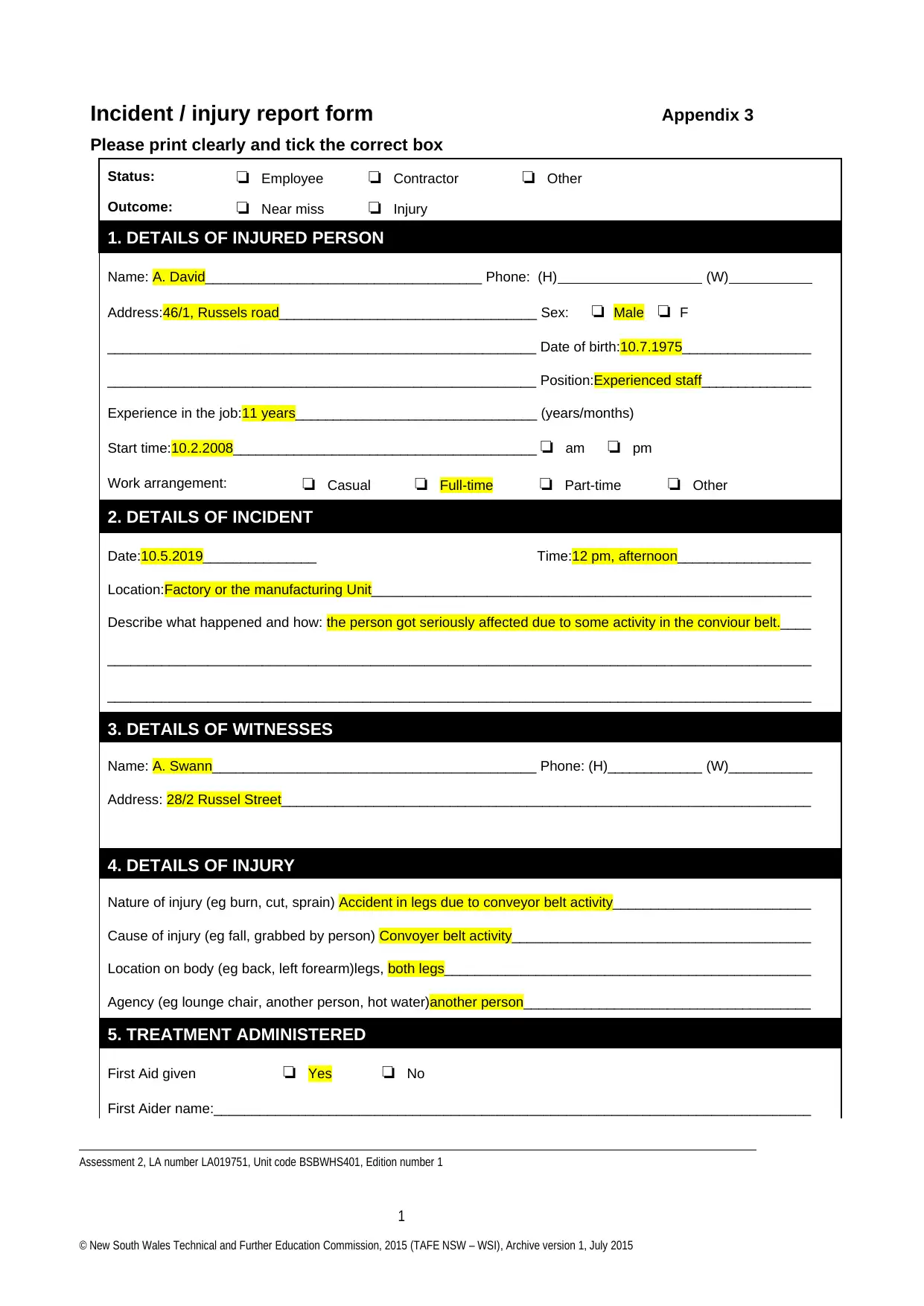
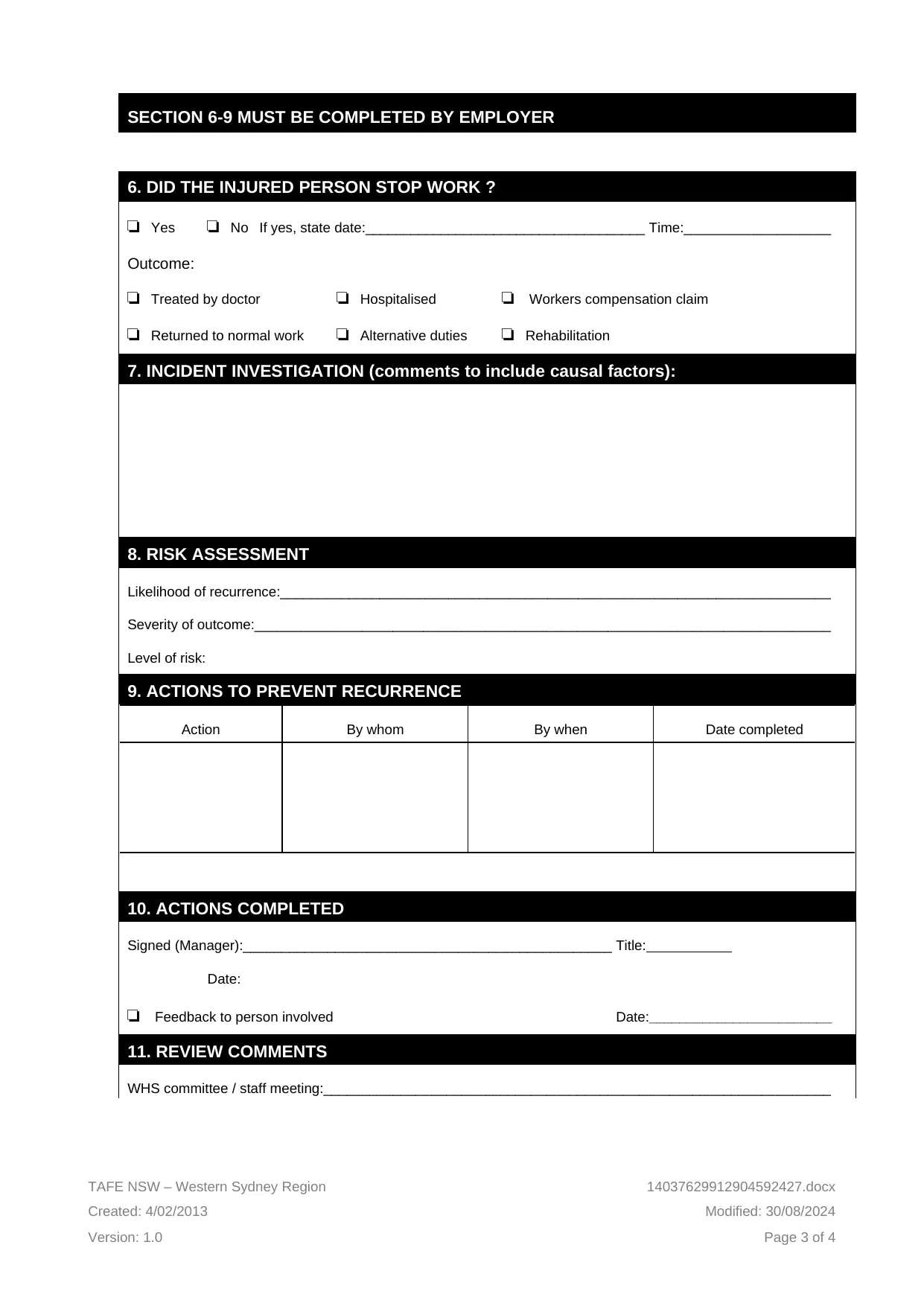
This document presents a completed incident report, aligned with the BSBWHS401 unit requirements. The report details an incident involving an employee injured by a conveyor belt, including witness information, nature of the injury, and treatment administered. The report covers the incident's specifics, including date, time, and location, alongside details of the injured person and witness. It also incorporates sections for the employer to complete, such as whether the injured person stopped work, incident investigation comments, risk assessment, and actions to prevent recurrence. Furthermore, the assessment brief highlights the need for a structured training plan using coaching or mentoring to address workplace health and safety gaps, along with the importance of accurate record-keeping. The report also includes a section for review comments from the WHS committee and relevant managers. This assignment provides a practical example of how to document workplace incidents and assess training needs in line with WHS regulations.


1 out of 4

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.