BSBWHS401A - Detailed Incident Report: Workplace Safety & Prevention
VerifiedAdded on 2023/06/11
|5
|919
|277
Report
AI Summary
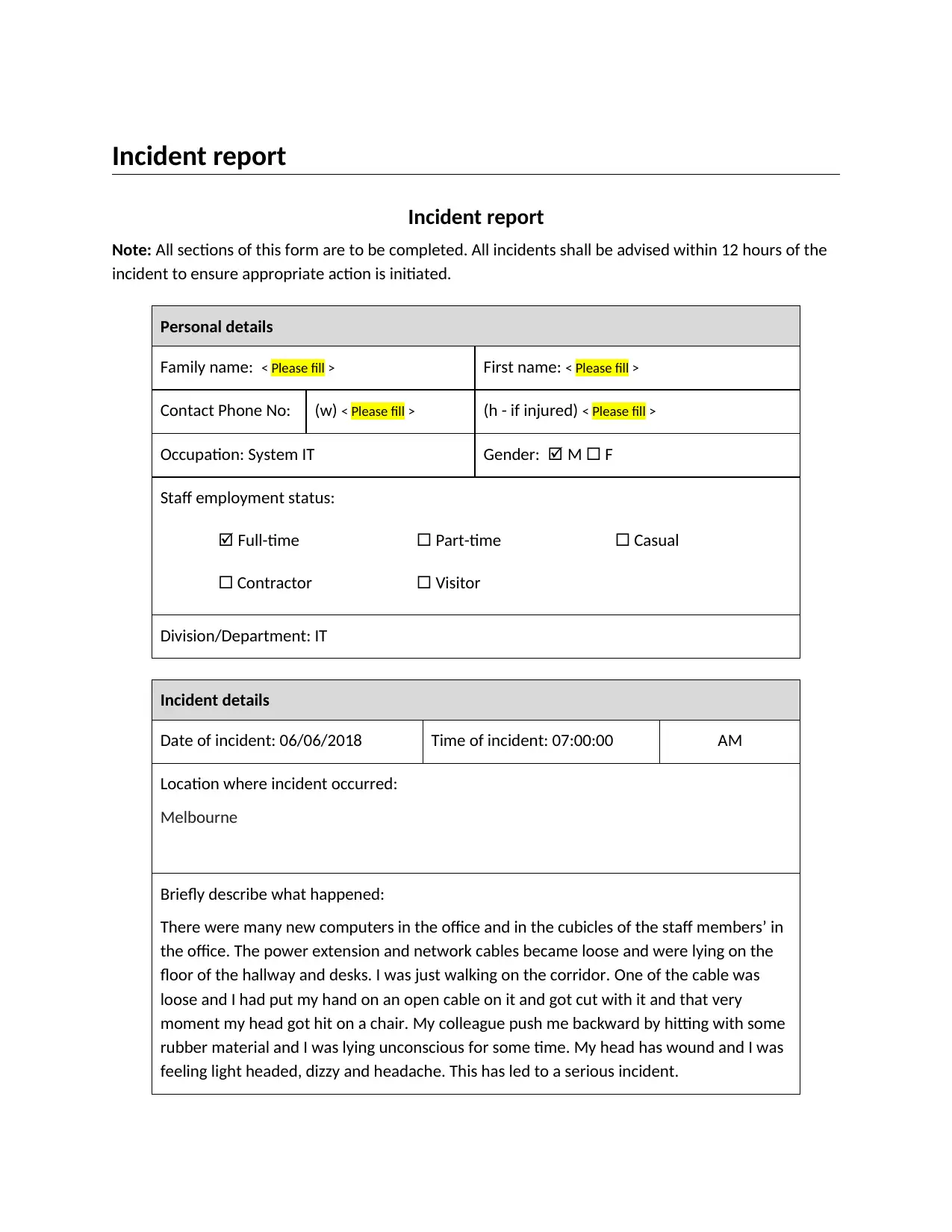
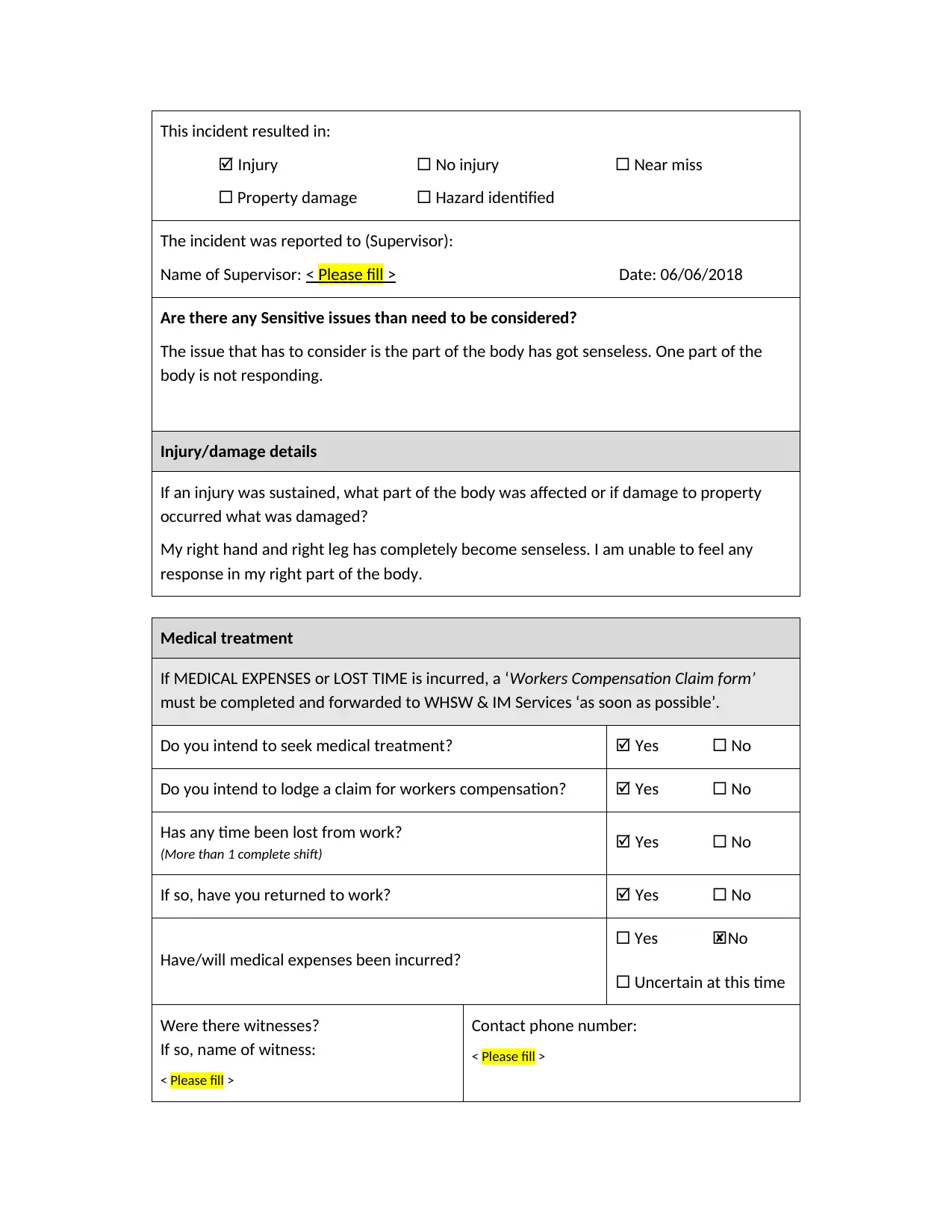
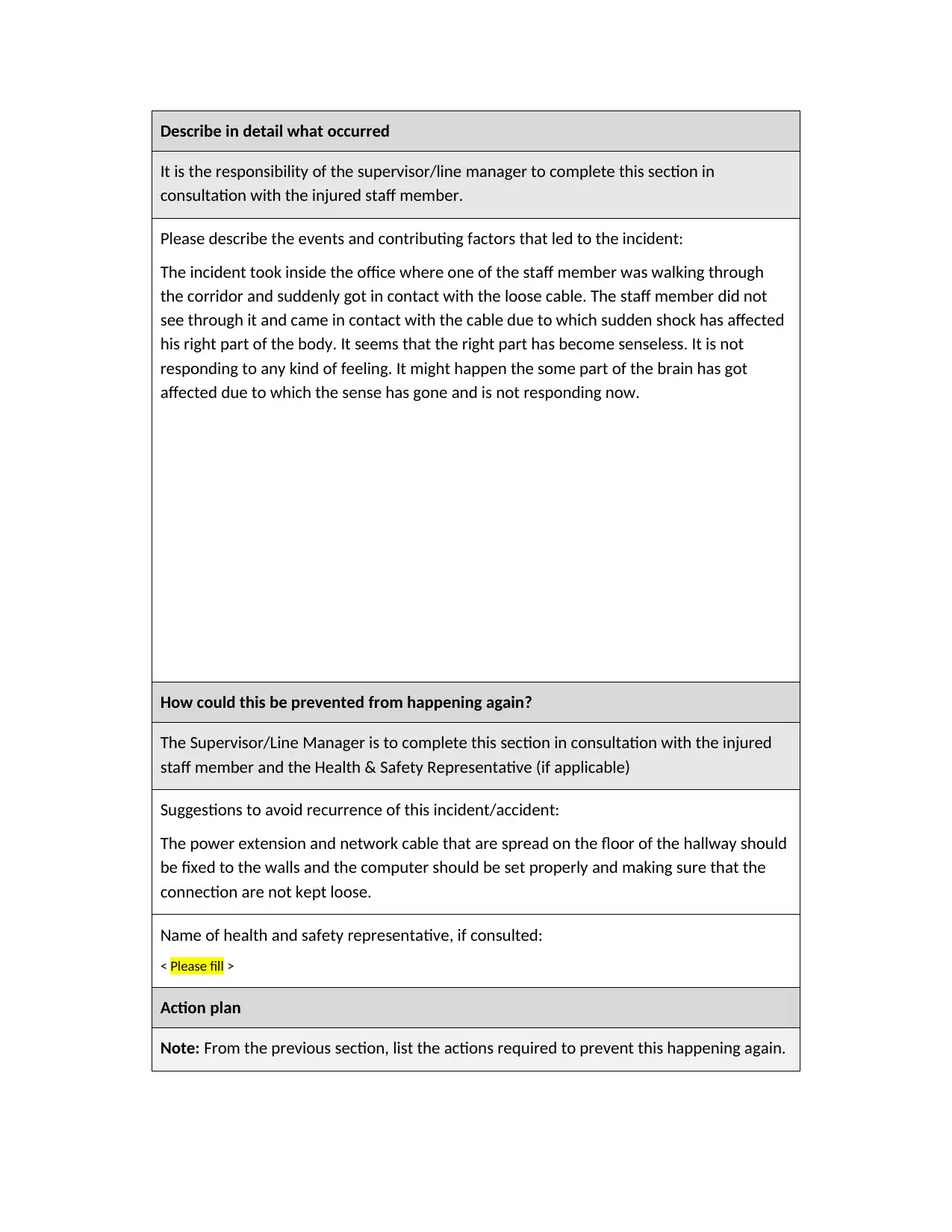
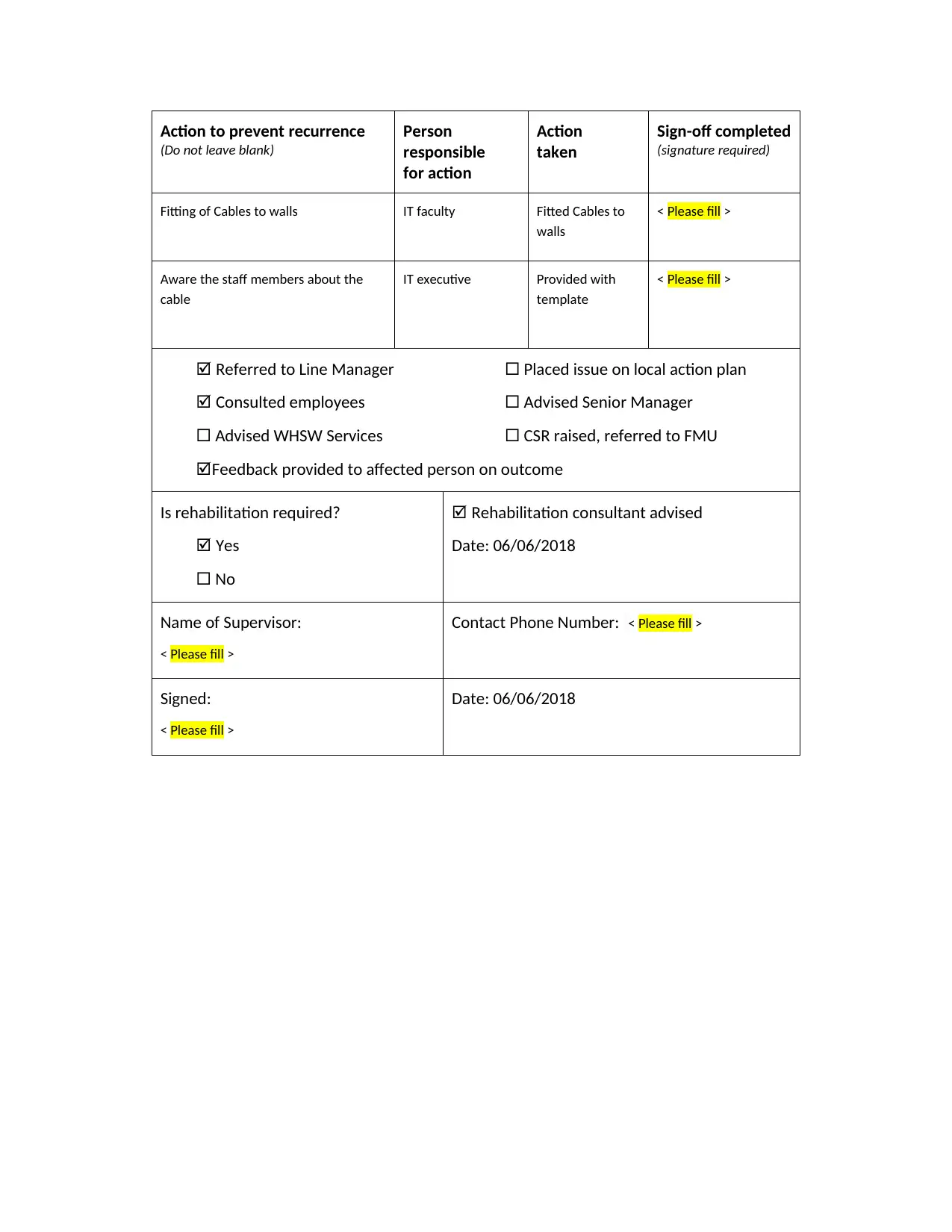
The provided document is an incident report detailing a workplace accident where an IT staff member was injured due to loose power and network cables in the office. The report outlines the incident, including the date, time, and location, and describes the injuries sustained. It also includes sections for supervisor comments on the events leading to the incident and proposed actions to prevent recurrence, such as securing cables and raising staff awareness. The report also covers medical treatment, potential worker's compensation claims, and witness information, concluding with an action plan for implementing preventative measures. Desklib offers a variety of solved assignments and past papers for students to explore.
1 out of 5



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.