Detailed Report on Wound Healing: Inflammation, Hypoxia & Smoking
VerifiedAdded on 2023/06/08
|7
|1326
|199
Report
AI Summary
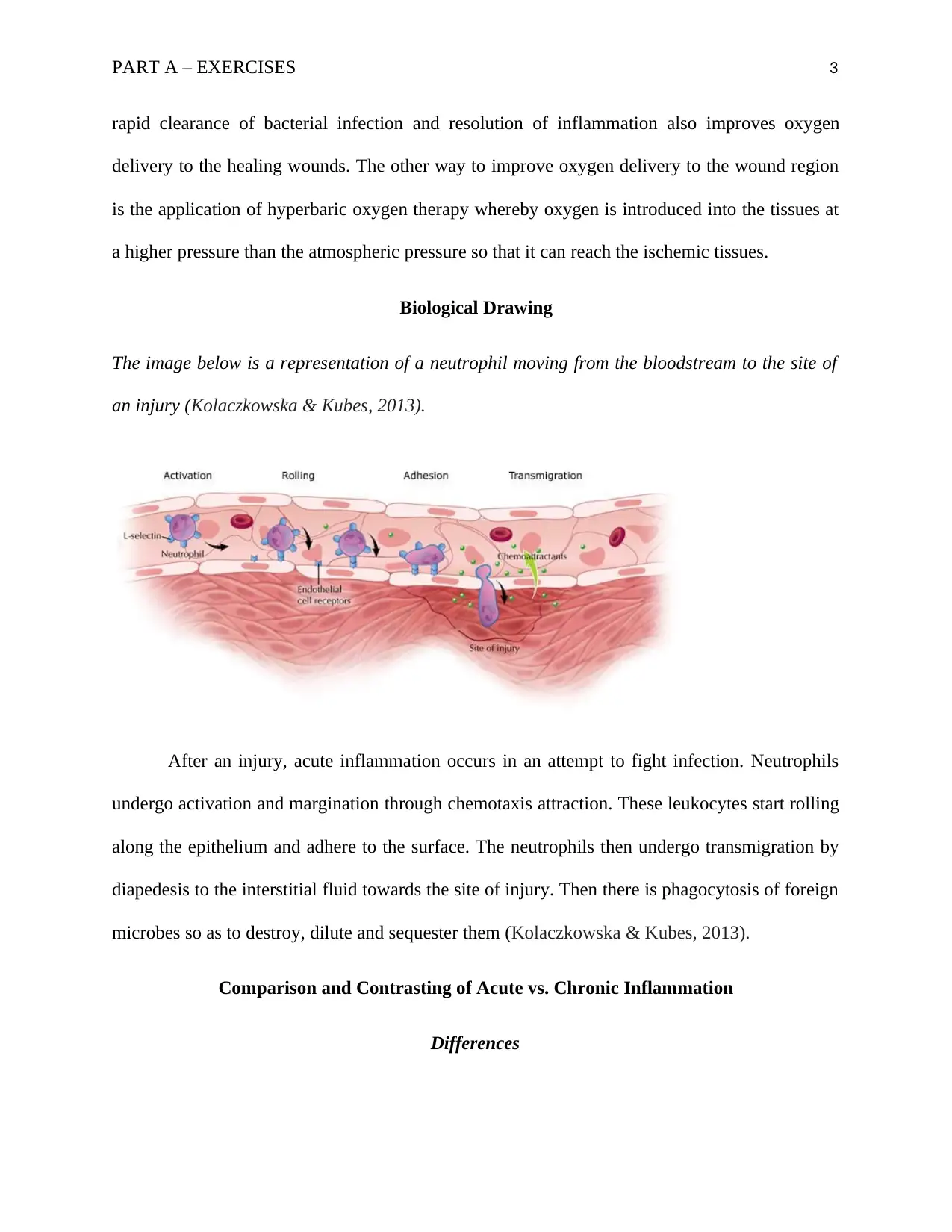
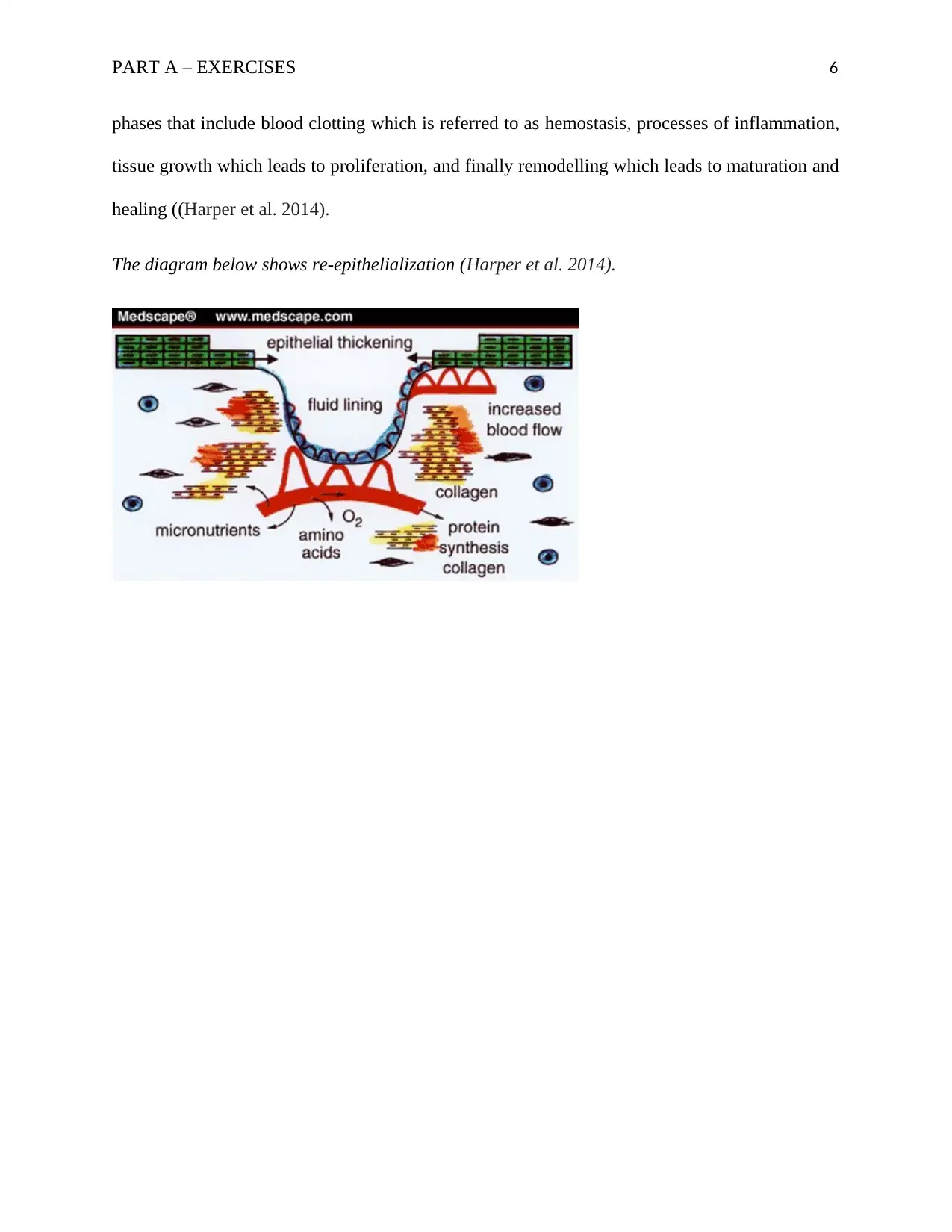
This report provides a detailed analysis of wound healing processes, focusing on the impact of hypoxia and inflammation. It discusses how hypoxia, caused by restricted blood supply, impairs wound healing by affecting cellular respiration and the function of Hypoxia-inducible factor-1. Strategies to improve oxygen delivery to ischemic tissues, such as oedema drainage and hyperbaric oxygen therapy, are also explored. The report includes a biological drawing illustrating neutrophil movement during inflammation and compares acute versus chronic inflammation, highlighting their differences and similarities. Furthermore, the report includes case studies, one examining the adverse effects of smoking on wound healing due to vasoconstriction and reduced oxygen perfusion, and another classifying a wound and describing the healing process by primary intention. The document concludes with relevant references.

1 out of 7
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.