Applying Wound Management Principles in a Clinical Burn Injury Case
VerifiedAdded on 2023/06/10
|24
|8587
|441
Case Study
AI Summary
This case study focuses on the wound management of Carol Mitchell, a 64-year-old patient admitted to the burns unit after sustaining burns to her left lower leg and foot. The case details the initial assessment in the emergency room, including the classification of the burn as a full-thickness injury around her inner left ankle, necessitating surgical debridement and a skin graft. The solution provides a detailed explanation of the wound healing process, including the stages of hemostasis, inflammation, proliferation, and maturation. It outlines the steps for a comprehensive skin assessment, strategies for pain management, and the rationale behind surgical debridement. Furthermore, it describes how skin heals with the assistance of a skin graft, emphasizing the importance of optimizing the healing process through holistic wound assessment. This assignment showcases the application of wound management principles in a clinical setting. Desklib offers a range of similar solved assignments and study tools for students.
Apply principles of wound management in
the clinical environment
123 TMP E – Assessment Template – Written v1.3 Page 1 of 24
the clinical environment
123 TMP E – Assessment Template – Written v1.3 Page 1 of 24
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Case Study Scenario 1 – Burn Injury:
Carol Mitchell, aged 64 was admitted to the burns unit after sustaining burns to the front and back of her left
lower leg and foot. Carol had been cooking in her kitchen, when she accidently knocked a saucepan full of hot
oil over herself. Carol’s husband drove her to the nearest medical centre where Carol’s burn was treated and
then she was transported by ambulance to the hospital for further assessment.
15595171 / Bork / shutterstock.com
In the emergency room, Carol was conscious and in evident distress. Her admission notes were: areas of
variable depth of injury over her posterior lower leg and foot only; dark pink discoloration with sluggish capillary
refill, blistering is evident; an area on her inner left ankle has an area of blotchy red/white with sluggish to
absent capillary refill, patient is complaining of pain on her lower leg, but states that her ankle is somewhat
pain free.
After consultation with the Burns team, the burns are to be surgically debrided and a small skin graft will be
applied to her inner ankle injury.
123 TMP E – Assessment Template – Written v1.3 Page 2 of 24
Carol Mitchell, aged 64 was admitted to the burns unit after sustaining burns to the front and back of her left
lower leg and foot. Carol had been cooking in her kitchen, when she accidently knocked a saucepan full of hot
oil over herself. Carol’s husband drove her to the nearest medical centre where Carol’s burn was treated and
then she was transported by ambulance to the hospital for further assessment.
15595171 / Bork / shutterstock.com
In the emergency room, Carol was conscious and in evident distress. Her admission notes were: areas of
variable depth of injury over her posterior lower leg and foot only; dark pink discoloration with sluggish capillary
refill, blistering is evident; an area on her inner left ankle has an area of blotchy red/white with sluggish to
absent capillary refill, patient is complaining of pain on her lower leg, but states that her ankle is somewhat
pain free.
After consultation with the Burns team, the burns are to be surgically debrided and a small skin graft will be
applied to her inner ankle injury.
123 TMP E – Assessment Template – Written v1.3 Page 2 of 24
Case Study 1 - Short answer questions: word count and referencing stated where
required
Read each question carefully and ensure you answer each part.
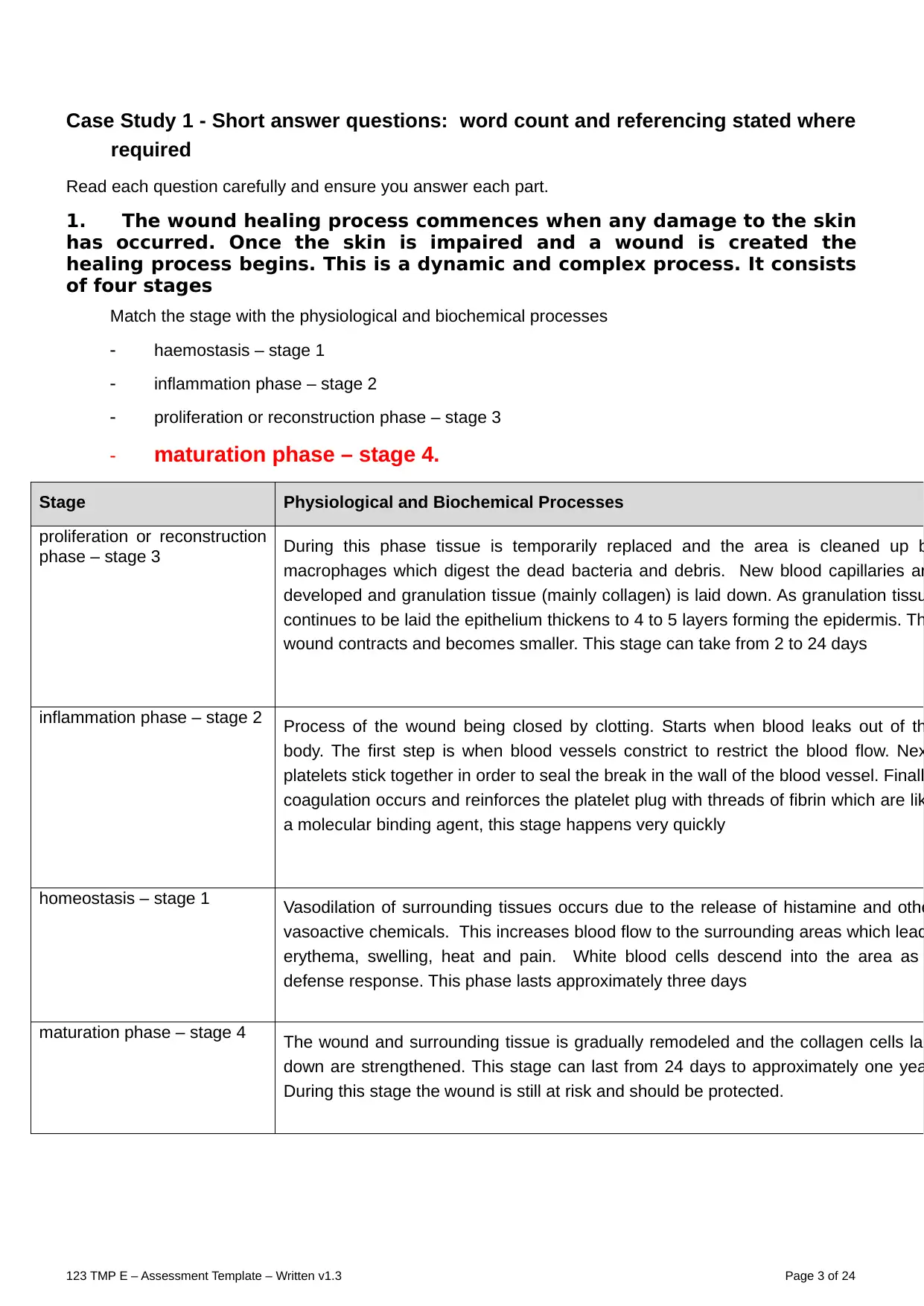
1. The wound healing process commences when any damage to the skin
has occurred. Once the skin is impaired and a wound is created the
healing process begins. This is a dynamic and complex process. It consists
of four stages
Match the stage with the physiological and biochemical processes
haemostasis – stage 1
inflammation phase – stage 2
proliferation or reconstruction phase – stage 3
maturation phase – stage 4.
Stage Physiological and Biochemical Processes
proliferation or reconstruction
phase – stage 3 During this phase tissue is temporarily replaced and the area is cleaned up b
macrophages which digest the dead bacteria and debris. New blood capillaries ar
developed and granulation tissue (mainly collagen) is laid down. As granulation tissu
continues to be laid the epithelium thickens to 4 to 5 layers forming the epidermis. Th
wound contracts and becomes smaller. This stage can take from 2 to 24 days
inflammation phase – stage 2 Process of the wound being closed by clotting. Starts when blood leaks out of th
body. The first step is when blood vessels constrict to restrict the blood flow. Nex
platelets stick together in order to seal the break in the wall of the blood vessel. Finall
coagulation occurs and reinforces the platelet plug with threads of fibrin which are lik
a molecular binding agent, this stage happens very quickly
homeostasis – stage 1 Vasodilation of surrounding tissues occurs due to the release of histamine and othe
vasoactive chemicals. This increases blood flow to the surrounding areas which lead
erythema, swelling, heat and pain. White blood cells descend into the area as
defense response. This phase lasts approximately three days
maturation phase – stage 4 The wound and surrounding tissue is gradually remodeled and the collagen cells lai
down are strengthened. This stage can last from 24 days to approximately one yea
During this stage the wound is still at risk and should be protected.
123 TMP E – Assessment Template – Written v1.3 Page 3 of 24
required
Read each question carefully and ensure you answer each part.
1. The wound healing process commences when any damage to the skin
has occurred. Once the skin is impaired and a wound is created the
healing process begins. This is a dynamic and complex process. It consists
of four stages
Match the stage with the physiological and biochemical processes
haemostasis – stage 1
inflammation phase – stage 2
proliferation or reconstruction phase – stage 3
maturation phase – stage 4.
Stage Physiological and Biochemical Processes
proliferation or reconstruction
phase – stage 3 During this phase tissue is temporarily replaced and the area is cleaned up b
macrophages which digest the dead bacteria and debris. New blood capillaries ar
developed and granulation tissue (mainly collagen) is laid down. As granulation tissu
continues to be laid the epithelium thickens to 4 to 5 layers forming the epidermis. Th
wound contracts and becomes smaller. This stage can take from 2 to 24 days
inflammation phase – stage 2 Process of the wound being closed by clotting. Starts when blood leaks out of th
body. The first step is when blood vessels constrict to restrict the blood flow. Nex
platelets stick together in order to seal the break in the wall of the blood vessel. Finall
coagulation occurs and reinforces the platelet plug with threads of fibrin which are lik
a molecular binding agent, this stage happens very quickly
homeostasis – stage 1 Vasodilation of surrounding tissues occurs due to the release of histamine and othe
vasoactive chemicals. This increases blood flow to the surrounding areas which lead
erythema, swelling, heat and pain. White blood cells descend into the area as
defense response. This phase lasts approximately three days
maturation phase – stage 4 The wound and surrounding tissue is gradually remodeled and the collagen cells lai
down are strengthened. This stage can last from 24 days to approximately one yea
During this stage the wound is still at risk and should be protected.
123 TMP E – Assessment Template – Written v1.3 Page 3 of 24
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
2a. Skin Assessment – outline the steps of the skin assessment for Carol’s burn that would be
carried out immediately on admission to the emergency department.
The burn assessment in Carol's burn case can include the assessment of airways, breathing,
circulation, disability, exposure as well as the requirement for the resuscitation of the fluids. In the
emergency department, the care nurses must visualize Carol's burn that can be sustained while the
victim accidentally knocked a saucepan which is full of hot oil over herself. As per the rule of nine, the
surface area of the body can be categorized into an anatomical area which can represent the 9%, or
multiple of 9% of overall body surface. However, the 9% each of the head and each of the upper limb,
about 18% for each lower limb, front of trunk as well as the back of trunk. The care nurse may consider
the depth of burn. As the burn wounds are generally dynamic and need a re-assessment within the first
24 to 72 hours because the depth can enhance as a result of an inadequate care treatments or a
supper-added contamination.
https://patient.info/doctor/burns-assessment-and-management
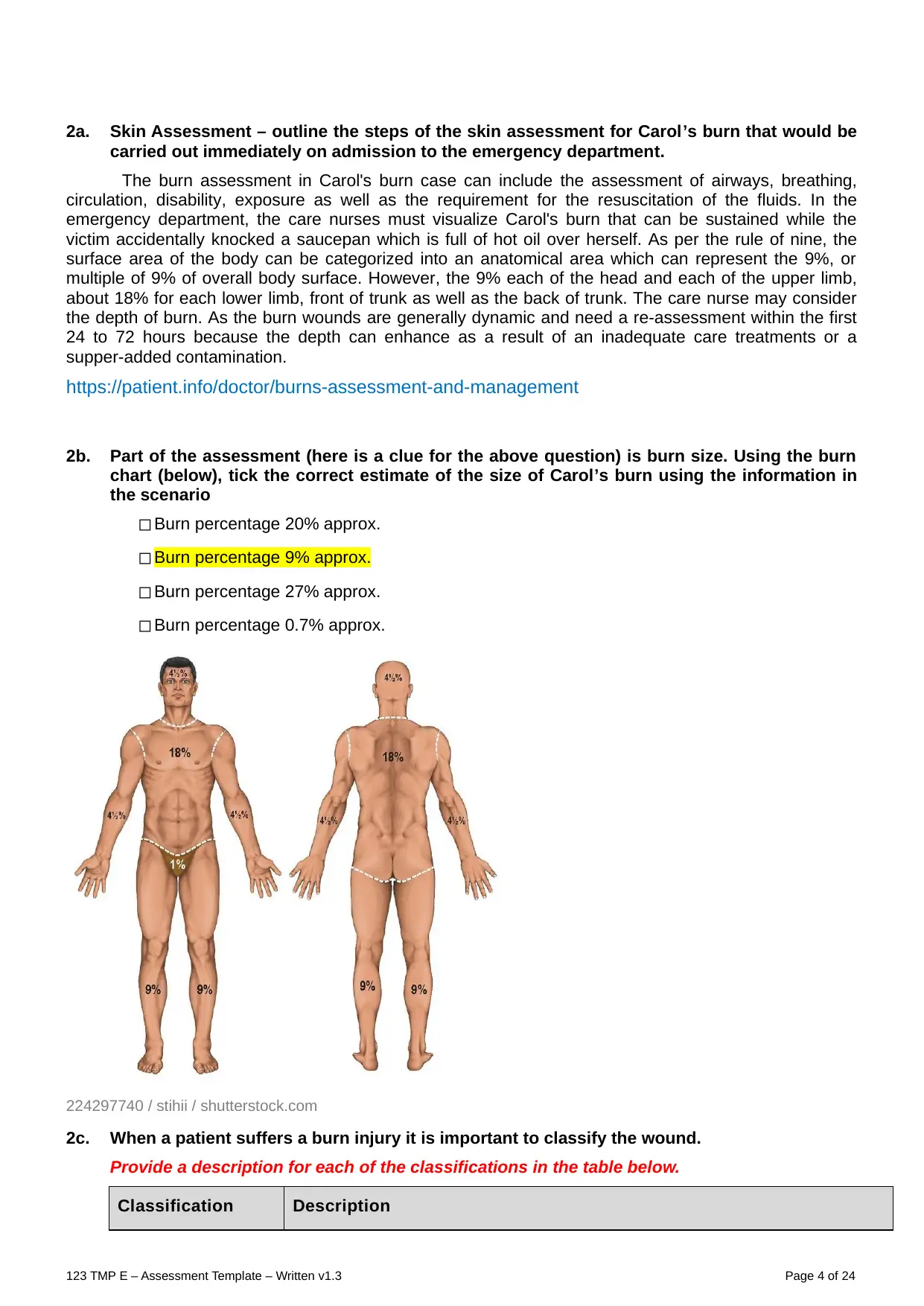
2b. Part of the assessment (here is a clue for the above question) is burn size. Using the burn
chart (below), tick the correct estimate of the size of Carol’s burn using the information in
the scenario
◻ Burn percentage 20% approx.
◻ Burn percentage 9% approx.
◻ Burn percentage 27% approx.
◻ Burn percentage 0.7% approx.
224297740 / stihii / shutterstock.com
2c. When a patient suffers a burn injury it is important to classify the wound.
Provide a description for each of the classifications in the table below.
Classification Description
123 TMP E – Assessment Template – Written v1.3 Page 4 of 24
carried out immediately on admission to the emergency department.
The burn assessment in Carol's burn case can include the assessment of airways, breathing,
circulation, disability, exposure as well as the requirement for the resuscitation of the fluids. In the
emergency department, the care nurses must visualize Carol's burn that can be sustained while the
victim accidentally knocked a saucepan which is full of hot oil over herself. As per the rule of nine, the
surface area of the body can be categorized into an anatomical area which can represent the 9%, or
multiple of 9% of overall body surface. However, the 9% each of the head and each of the upper limb,
about 18% for each lower limb, front of trunk as well as the back of trunk. The care nurse may consider
the depth of burn. As the burn wounds are generally dynamic and need a re-assessment within the first
24 to 72 hours because the depth can enhance as a result of an inadequate care treatments or a
supper-added contamination.
https://patient.info/doctor/burns-assessment-and-management
2b. Part of the assessment (here is a clue for the above question) is burn size. Using the burn
chart (below), tick the correct estimate of the size of Carol’s burn using the information in
the scenario
◻ Burn percentage 20% approx.
◻ Burn percentage 9% approx.
◻ Burn percentage 27% approx.
◻ Burn percentage 0.7% approx.
224297740 / stihii / shutterstock.com
2c. When a patient suffers a burn injury it is important to classify the wound.
Provide a description for each of the classifications in the table below.
Classification Description
123 TMP E – Assessment Template – Written v1.3 Page 4 of 24
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Superficial The superficial burn wound can involve only the epidermal layers of the skin.
these generally do not blister but are very painful, red, blanch with pressure,
and dry as well. in this, the slight alterations within the air current moving past
to the exposed superficial burn can cause a patient to experience a
excruciating pain.
Partial thickness The partial thickness is generally the second degree burn which can include
the epidermis as well as a part of the dermis layer of the skin. the site of the
burn can appear blistered, red as well as can be swollen and painful as well.
the burn can cause a mild pain and slight discomfort, specifically when
something like a cloth rubbing against the burned area.
Full thickness In the full thickness burns, the skin of a patient either be black, white, brown,
leathery in appearance and many more. in this, in the burn it can frequently
form an eschar around the wound. since the nerve endings are generally
damaged along with the dermis, and these such types of wound are quite
painless (Full Thickness Burns are a Life- Threatening Injury that require
medical attention, 2018).
State which one would most likely apply to Carol’s area of her burn around her inner left
ankle and give a rationale for your choice.
From the above scenario of Carol’s area of burn, it is identified that her injury can involve a full
thickness type of burn wound. it is because the nerve endings are mainly responsible for the sensations
that are damaged. From her case scenario, it is analyzed that the third degree burn can damage the
epidermis and dermis of a patient.
2d. When undertaking a wound assessment, the main purpose is to optimize the healing
process and to produce a baseline status against which the healing process can be
measured
Outline four (4) aspects you may consider when conducting a holistic wound assessment.
Provide a reason for each of your choices.
In this, a holistic wound assessment can include the medical history of a patient, consisting the current
and past medical conditions, it can also include the psychological, social as well as the spiritual history,
their wound care environment as well as can assess to the specialized well-being care services. the
wound healing process can include the four phases which are as mentioned below:
Hemostasis Stage: It is generally an easy pathway to identify that the body has started the hemostasis
stage is that the blood will begin to clot. if a patient can experience a break within the skin as well as are
begin to bleed, then their blood vessels will work to constrict the flow of blood. the platelets then
generally stick collaboratively to seal the break within the skin.
Inflammatory Stage: This particular stage can occur right when the skin can break. when a person gets
injured, then their blood vessels begin to leak, and swelling can occur. In this, the swelling as well as
inflammation can aid to control the bleed as well as can prevent the infections. the white blood cells
known as Neutrophils that can enter the wound to remove the bacteria and debris as well.
Proliferative Stage: It is mainly the third stage, when the wound can rebuild itself as well as the new
skin can rise the new tissue oxygen and nutrients as well. in this, the cells known as fibroblast can work
to effectively heal the wound by gripping the edges of the wound as well as pull them combined.
Maturation Stage: It is the stage also known as remodeling stage is when the collagen within the skin is
regenerated as well as the wound can completely close. in context with earlier stage, the collagen which
can rebuild the skin is generally uneven and thick as well. within the maturation stage, the collagen fibre
can begin to align more efficiently with each other as well as can lie more close combined to cross-link
(Wound Care Stage, 2021).
123 TMP E – Assessment Template – Written v1.3 Page 5 of 24
these generally do not blister but are very painful, red, blanch with pressure,
and dry as well. in this, the slight alterations within the air current moving past
to the exposed superficial burn can cause a patient to experience a
excruciating pain.
Partial thickness The partial thickness is generally the second degree burn which can include
the epidermis as well as a part of the dermis layer of the skin. the site of the
burn can appear blistered, red as well as can be swollen and painful as well.
the burn can cause a mild pain and slight discomfort, specifically when
something like a cloth rubbing against the burned area.
Full thickness In the full thickness burns, the skin of a patient either be black, white, brown,
leathery in appearance and many more. in this, in the burn it can frequently
form an eschar around the wound. since the nerve endings are generally
damaged along with the dermis, and these such types of wound are quite
painless (Full Thickness Burns are a Life- Threatening Injury that require
medical attention, 2018).
State which one would most likely apply to Carol’s area of her burn around her inner left
ankle and give a rationale for your choice.
From the above scenario of Carol’s area of burn, it is identified that her injury can involve a full
thickness type of burn wound. it is because the nerve endings are mainly responsible for the sensations
that are damaged. From her case scenario, it is analyzed that the third degree burn can damage the
epidermis and dermis of a patient.
2d. When undertaking a wound assessment, the main purpose is to optimize the healing
process and to produce a baseline status against which the healing process can be
measured
Outline four (4) aspects you may consider when conducting a holistic wound assessment.
Provide a reason for each of your choices.
In this, a holistic wound assessment can include the medical history of a patient, consisting the current
and past medical conditions, it can also include the psychological, social as well as the spiritual history,
their wound care environment as well as can assess to the specialized well-being care services. the
wound healing process can include the four phases which are as mentioned below:
Hemostasis Stage: It is generally an easy pathway to identify that the body has started the hemostasis
stage is that the blood will begin to clot. if a patient can experience a break within the skin as well as are
begin to bleed, then their blood vessels will work to constrict the flow of blood. the platelets then
generally stick collaboratively to seal the break within the skin.
Inflammatory Stage: This particular stage can occur right when the skin can break. when a person gets
injured, then their blood vessels begin to leak, and swelling can occur. In this, the swelling as well as
inflammation can aid to control the bleed as well as can prevent the infections. the white blood cells
known as Neutrophils that can enter the wound to remove the bacteria and debris as well.
Proliferative Stage: It is mainly the third stage, when the wound can rebuild itself as well as the new
skin can rise the new tissue oxygen and nutrients as well. in this, the cells known as fibroblast can work
to effectively heal the wound by gripping the edges of the wound as well as pull them combined.
Maturation Stage: It is the stage also known as remodeling stage is when the collagen within the skin is
regenerated as well as the wound can completely close. in context with earlier stage, the collagen which
can rebuild the skin is generally uneven and thick as well. within the maturation stage, the collagen fibre
can begin to align more efficiently with each other as well as can lie more close combined to cross-link
(Wound Care Stage, 2021).
123 TMP E – Assessment Template – Written v1.3 Page 5 of 24
3a. As stated in the case study, Carol is complaining of pain
Which of the following strategies may be utilised to provide comfort to Carol? (There is
more than one)
◻ Provide pain relief
◻ Provide distraction therapy
◻ Elevate Carol’s foot above heart level (not much recommded in burn cases)
◻ Ensure bed comfort
◻ Assess stress / anxiety levels and look at reducing these
◻ Inform Carol that pain is a normal aspect of a burn and there is not much that can be done to
reduce all pain
3b. Describe an appropriate pain assessment tool and then explain why it is important to
reduce pain levels in patient with wounds?
The pain assessment tool is generally a multidimensional observational assessment of the vulnerable
patients who can experience the pain. The pain measurement tools are the instruments which are
specifically designed to measure the pain of a person. The tools have been used for the pain
assessment at the healthcare organization and generally been chosen on the reliability, validity and
usability as well as are mainly recognized by the pain specialist to be clinically effective while assessing
the acute pain. It is considered as an essential component as it can enable the management of pain to
be effectively titrated as well as tailored to the needs of the patient, more specifically during the
management of wound procedures (Pain assessment and measurement, 2019).
4. It was noted in the case study for Carol that she required “surgical debridement” to her
burns. Explain what surgical wound debridement is and why is it done?
The debridement is mainly a procedure for treating a wound within the skin. It can involve the thoroughly
cleaning of the wound as well as removing all the hyperkeratotic such as the thickened callus or skin
part, contaminated as well as non-viable tissue, the foreign debris as well as the residual material from
the dressings. It is generally a main step in the entire protocol for effectively treating the diabetic foot
ulcers that is generally occurs among 20% of the diabetic patients as well as can precede about 85% of
all the diabetes-associated lower leg amputations. Such that in the above case scenario of Carol, she
needs surgical debridement to her burn towards the hyperkeratotic, infected as well as the non-viable
tissues can be surgically removed by using a scalpel as well. It is done because it can effectively
reduces the developing risk of infection or contamination as well as can give comfort in the minor burns
as well.
5. Describe how the skin heals with the assistance of a skin graft.
In this, a graft is generally a skin that is surgically placed over a deeply burned region or to cover an
opening of the wounds. The skin grafting technique can enable the healthcare providers to stretch the
skin on the wide region. It can aid the region heal after the procedure. The care providers can place the
healthy skin over the damaged skin. They generally secure the skin in place with the stitches or staples
and put a dressing over the region. In addition to this, when the surface area of the burn in body is
broad, the sheet grafts are generally saved for the neck, face and hands, as well as making the most
clear parts of the human body can appears less scarred. Furthermore, when a burn is minute and there
is some of the donor skin available, a sheet graft may be used to cover the whole burned region. It can
aid the region to heal after surgery.
6. When assessing a patient’s wound discuss 2 common problems / complications you may
encounter.
The two possible common issues or complications that can be encountered while assessing the
patient's wound such as:
An infection occurs on a wound: It can occur when the germs such as the bacteria can grow
over the damaged or abrasion skin of the wound. In this, the symptoms can involve the
123 TMP E – Assessment Template – Written v1.3 Page 6 of 24
Which of the following strategies may be utilised to provide comfort to Carol? (There is
more than one)
◻ Provide pain relief
◻ Provide distraction therapy
◻ Elevate Carol’s foot above heart level (not much recommded in burn cases)
◻ Ensure bed comfort
◻ Assess stress / anxiety levels and look at reducing these
◻ Inform Carol that pain is a normal aspect of a burn and there is not much that can be done to
reduce all pain
3b. Describe an appropriate pain assessment tool and then explain why it is important to
reduce pain levels in patient with wounds?
The pain assessment tool is generally a multidimensional observational assessment of the vulnerable
patients who can experience the pain. The pain measurement tools are the instruments which are
specifically designed to measure the pain of a person. The tools have been used for the pain
assessment at the healthcare organization and generally been chosen on the reliability, validity and
usability as well as are mainly recognized by the pain specialist to be clinically effective while assessing
the acute pain. It is considered as an essential component as it can enable the management of pain to
be effectively titrated as well as tailored to the needs of the patient, more specifically during the
management of wound procedures (Pain assessment and measurement, 2019).
4. It was noted in the case study for Carol that she required “surgical debridement” to her
burns. Explain what surgical wound debridement is and why is it done?
The debridement is mainly a procedure for treating a wound within the skin. It can involve the thoroughly
cleaning of the wound as well as removing all the hyperkeratotic such as the thickened callus or skin
part, contaminated as well as non-viable tissue, the foreign debris as well as the residual material from
the dressings. It is generally a main step in the entire protocol for effectively treating the diabetic foot
ulcers that is generally occurs among 20% of the diabetic patients as well as can precede about 85% of
all the diabetes-associated lower leg amputations. Such that in the above case scenario of Carol, she
needs surgical debridement to her burn towards the hyperkeratotic, infected as well as the non-viable
tissues can be surgically removed by using a scalpel as well. It is done because it can effectively
reduces the developing risk of infection or contamination as well as can give comfort in the minor burns
as well.
5. Describe how the skin heals with the assistance of a skin graft.
In this, a graft is generally a skin that is surgically placed over a deeply burned region or to cover an
opening of the wounds. The skin grafting technique can enable the healthcare providers to stretch the
skin on the wide region. It can aid the region heal after the procedure. The care providers can place the
healthy skin over the damaged skin. They generally secure the skin in place with the stitches or staples
and put a dressing over the region. In addition to this, when the surface area of the burn in body is
broad, the sheet grafts are generally saved for the neck, face and hands, as well as making the most
clear parts of the human body can appears less scarred. Furthermore, when a burn is minute and there
is some of the donor skin available, a sheet graft may be used to cover the whole burned region. It can
aid the region to heal after surgery.
6. When assessing a patient’s wound discuss 2 common problems / complications you may
encounter.
The two possible common issues or complications that can be encountered while assessing the
patient's wound such as:
An infection occurs on a wound: It can occur when the germs such as the bacteria can grow
over the damaged or abrasion skin of the wound. In this, the symptoms can involve the
123 TMP E – Assessment Template – Written v1.3 Page 6 of 24
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
enhanced pain, redness and swelling as well. In addition to this, the more severe
contamination can cause nausea, fever or chills as well.
A blood infection: The infection of blood is also known as sepsis that is a serious
complication of the septicemia. It is generally a life-threatening issue of an infection or
contamination. Sepsis can occurs when the released chemicals within the bloodstream to
fight against an infection which can trigger the inflammation via all over the body.
Case study
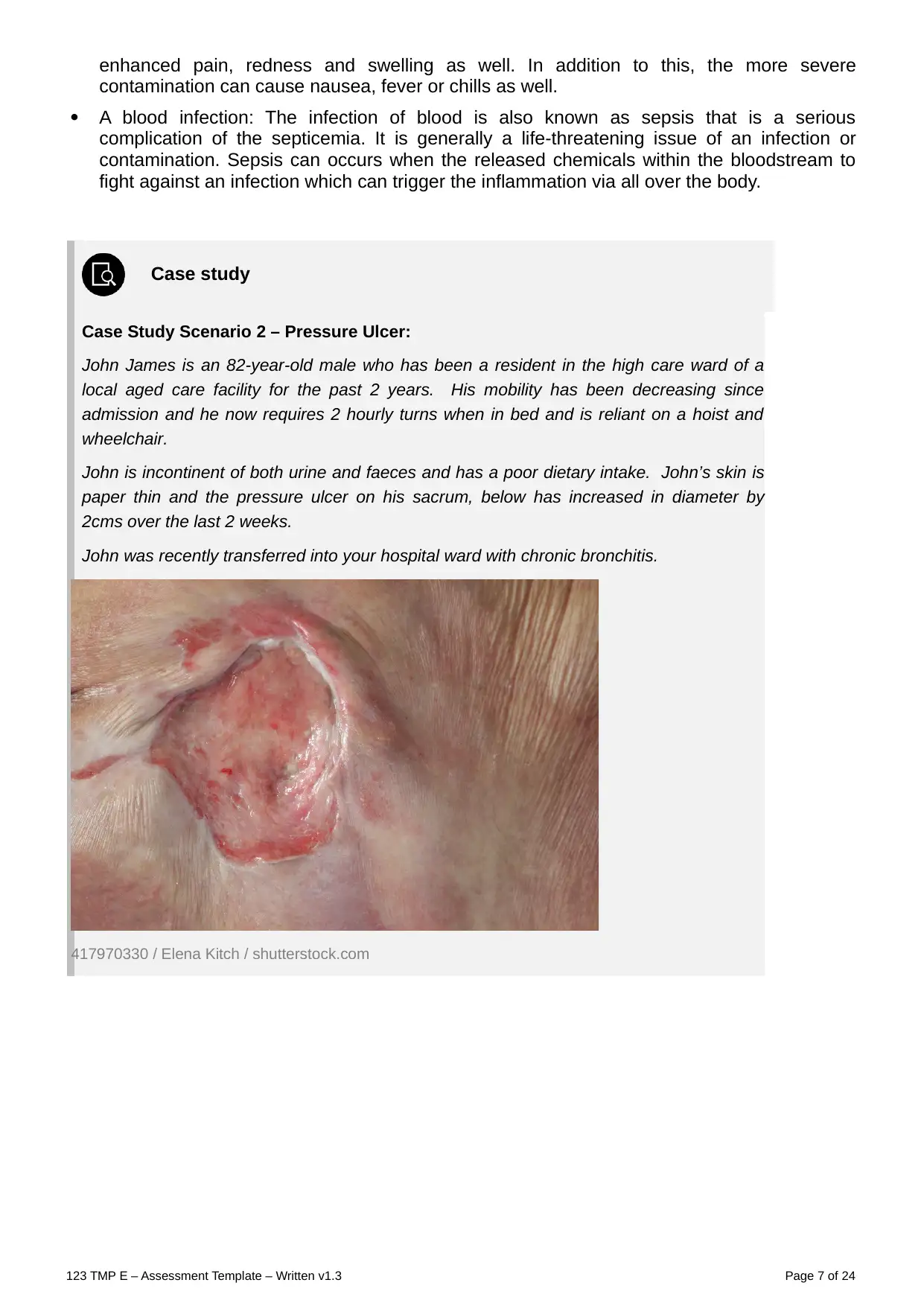
Case Study Scenario 2 – Pressure Ulcer:
John James is an 82-year-old male who has been a resident in the high care ward of a
local aged care facility for the past 2 years. His mobility has been decreasing since
admission and he now requires 2 hourly turns when in bed and is reliant on a hoist and
wheelchair.
John is incontinent of both urine and faeces and has a poor dietary intake. John’s skin is
paper thin and the pressure ulcer on his sacrum, below has increased in diameter by
2cms over the last 2 weeks.
John was recently transferred into your hospital ward with chronic bronchitis.
417970330 / Elena Kitch / shutterstock.com
123 TMP E – Assessment Template – Written v1.3 Page 7 of 24
contamination can cause nausea, fever or chills as well.
A blood infection: The infection of blood is also known as sepsis that is a serious
complication of the septicemia. It is generally a life-threatening issue of an infection or
contamination. Sepsis can occurs when the released chemicals within the bloodstream to
fight against an infection which can trigger the inflammation via all over the body.
Case study
Case Study Scenario 2 – Pressure Ulcer:
John James is an 82-year-old male who has been a resident in the high care ward of a
local aged care facility for the past 2 years. His mobility has been decreasing since
admission and he now requires 2 hourly turns when in bed and is reliant on a hoist and
wheelchair.
John is incontinent of both urine and faeces and has a poor dietary intake. John’s skin is
paper thin and the pressure ulcer on his sacrum, below has increased in diameter by
2cms over the last 2 weeks.
John was recently transferred into your hospital ward with chronic bronchitis.
417970330 / Elena Kitch / shutterstock.com
123 TMP E – Assessment Template – Written v1.3 Page 7 of 24
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Case Study 2 - Short answer questions: word count and referencing stated where
required
Read each question carefully and ensure you answer each part.
1a. You have been asked to attend to the dressing of John’s wound. What would be a suitable
dressing to use on John’s wound? (you must give a rationale for your choice).
Type of dressing: From the above case scenario, the care nurse must provide him a hydrocolloid
dressings that can include a gel which can supports the growth of a new skin cells within the ulcer, while
maintaining the surrounding skin dry. In this the other types of dressing can involve such as foam,
hydrofibres, gels and antimicrobial dressings can also be used (Treatment Pressure Ulcer, 2020).
Rationale: The pressure region care are generally an essential part of the nursing practice. While
handling the patients having such ulcers, it is identified that patients preferences must be taken in to
consideration is also important factor.
1b. Explain the goal of this treatment as per Q1a – what are you trying to achieve by
maintaining a moist wound environment.
The decubitus ulcers are also known as the bedsores or the pressure ulcers are the soft and skin tissue
harms which can form as an outcome of the constant or a prolonged pressure that is exerted on the skin.
These such ulcers can occur at the bony regions of the human body like ischium, greater trochanter,
heel, sacrum and many other as well. The possible goal of the specific care treatment is to reduce the
pressure which is being exerted over the ulcer, reduces the contact of the ulcer with a hard surface,
reduces the moisture as well as to keep it as a aseptic or least septic as possible. The goal is not only to
keep the integrity of the skin but can also to give the vulnerable patient-centered plan of a care that is
geared towards the positive results (Pressure Injury/Ulcer Risk Assessment, 2018).
1c. Explain whether John required a primary or secondary dressing, or both, and provide a
rationale for your choice.
The primary dressing is generally a therapeutic or a protective covering that can be applied directly over
the wound on the skin or can be caused by an opening to the skin as well.
The secondary dressing are generally the material which can serve as a protective or a therapeutic
function as well as are required to secure a primary dressing as well. As per the above case scenario,
the care treatment of the patient having pressure ulcer is generally a two folds consisting the relief of the
pressure generally allied with the management of wound (Hydrocolloid dressing for treating pressure
ulcers, 2018).
2a. Most infections agents are micro-organisms, these include: – (choose one answer)
◻ Bacteria, viruses, Soil, protozoa and prions
◻ Bacteria, Candida, fungi, protozoa and prions
◻ Bacteria, viruses, fungi, protozoa and prions
◻ Bacteria, viruses, fungi, protozoa and dust
2b. Match the common fungal infections with their major reservoir
Common fungal infection: Candida albicans, Aspergillus organisms
Common fungal infection Major reservoir
123 TMP E – Assessment Template – Written v1.3 Page 8 of 24
required
Read each question carefully and ensure you answer each part.
1a. You have been asked to attend to the dressing of John’s wound. What would be a suitable
dressing to use on John’s wound? (you must give a rationale for your choice).
Type of dressing: From the above case scenario, the care nurse must provide him a hydrocolloid
dressings that can include a gel which can supports the growth of a new skin cells within the ulcer, while
maintaining the surrounding skin dry. In this the other types of dressing can involve such as foam,
hydrofibres, gels and antimicrobial dressings can also be used (Treatment Pressure Ulcer, 2020).
Rationale: The pressure region care are generally an essential part of the nursing practice. While
handling the patients having such ulcers, it is identified that patients preferences must be taken in to
consideration is also important factor.
1b. Explain the goal of this treatment as per Q1a – what are you trying to achieve by
maintaining a moist wound environment.
The decubitus ulcers are also known as the bedsores or the pressure ulcers are the soft and skin tissue
harms which can form as an outcome of the constant or a prolonged pressure that is exerted on the skin.
These such ulcers can occur at the bony regions of the human body like ischium, greater trochanter,
heel, sacrum and many other as well. The possible goal of the specific care treatment is to reduce the
pressure which is being exerted over the ulcer, reduces the contact of the ulcer with a hard surface,
reduces the moisture as well as to keep it as a aseptic or least septic as possible. The goal is not only to
keep the integrity of the skin but can also to give the vulnerable patient-centered plan of a care that is
geared towards the positive results (Pressure Injury/Ulcer Risk Assessment, 2018).
1c. Explain whether John required a primary or secondary dressing, or both, and provide a
rationale for your choice.
The primary dressing is generally a therapeutic or a protective covering that can be applied directly over
the wound on the skin or can be caused by an opening to the skin as well.
The secondary dressing are generally the material which can serve as a protective or a therapeutic
function as well as are required to secure a primary dressing as well. As per the above case scenario,
the care treatment of the patient having pressure ulcer is generally a two folds consisting the relief of the
pressure generally allied with the management of wound (Hydrocolloid dressing for treating pressure
ulcers, 2018).
2a. Most infections agents are micro-organisms, these include: – (choose one answer)
◻ Bacteria, viruses, Soil, protozoa and prions
◻ Bacteria, Candida, fungi, protozoa and prions
◻ Bacteria, viruses, fungi, protozoa and prions
◻ Bacteria, viruses, fungi, protozoa and dust
2b. Match the common fungal infections with their major reservoir
Common fungal infection: Candida albicans, Aspergillus organisms
Common fungal infection Major reservoir
123 TMP E – Assessment Template – Written v1.3 Page 8 of 24
Aspergillus organisms Soil, dust, mouth, skin, colon, genital tract
Candida albicans Mouth, skin, colon, genital tract
2c. Match the common viral infections with their major reservoir.
Common viral infections Viral infection, Hepatitis A virus, Hepatitis B virus, Hepatitis C virus,
Human immunodeficiency virus (HIV), Herpes simplex virus (type I)
Common viral infection Major reservoir
Viral infection Reservoir
Hepatitis A virus Faeces
Human
immunodeficiency
virus
Blood and body fluids
Hepatitis C virus Blood
Hepatitis B virus Blood, semen, vaginal secretions (also isolated in saliva, tears,
urine and breast milk, but not proved to be sources of
transmission)
Herpes simplex virus Lesions of mouth or skin, saliva, genitalia plus herpes zoster
(shingles) or viral warts or herpangina (oral ulcers)
123 TMP E – Assessment Template – Written v1.3 Page 9 of 24
Candida albicans Mouth, skin, colon, genital tract
2c. Match the common viral infections with their major reservoir.
Common viral infections Viral infection, Hepatitis A virus, Hepatitis B virus, Hepatitis C virus,
Human immunodeficiency virus (HIV), Herpes simplex virus (type I)
Common viral infection Major reservoir
Viral infection Reservoir
Hepatitis A virus Faeces
Human
immunodeficiency
virus
Blood and body fluids
Hepatitis C virus Blood
Hepatitis B virus Blood, semen, vaginal secretions (also isolated in saliva, tears,
urine and breast milk, but not proved to be sources of
transmission)
Herpes simplex virus Lesions of mouth or skin, saliva, genitalia plus herpes zoster
(shingles) or viral warts or herpangina (oral ulcers)
123 TMP E – Assessment Template – Written v1.3 Page 9 of 24
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
2d. On the picture below, place an X on each of the areas that pressure sores can develop (if
your computer doesn’t allow you to do this, you may write the answers underneath).
The pressure sores can be developed on the back or the sides of a head, the shoulder blades, lower
back or hips or can be tail bone, the ankle, heel as well as the skin behind the knees, back of the arms
and legs where they rest against the chair, shoulder blades and spine as well.
132726884 / Anna Rassadnikova / shutterstock.com
Discuss 4 pressure relieving devices that may be used for John either in hospital or when he
goes back to the aged care facility.
The pressure relieving devices which can be used in John's case when he goes back to an aged care
facility such as:
Crash mats
Hip and elbow pads
Pressure relieving mattresses
Pressure cushions for elder people (Using Pressure Relieveing Equipment In a Care Home,
2018).
3. Match the Ulcer type with their specific characteristic
Ulcer type: Venous ulcers, Diabetic ulcers, Arterial ulcers, Pressure ulcer:
Ulcer type Characteristic
Arterial ulcers Caused by ischemia; related to the presence of arterial occlusive
disease; symptoms include pain and tissue loss
Venous ulcers Local losses of epidermis and various levels of dermis and
subcutaneous tissue, occurring over or near the malleoli at the
distal lower extremities; caused by edema and other sequalae of
impaired venous return.
Diabetic ulcers Caused by trauma or pressure secondary to neuropathy or
vascular disease related to diabetes mellitus.
123 TMP E – Assessment Template – Written v1.3 Page 10 of 24
your computer doesn’t allow you to do this, you may write the answers underneath).
The pressure sores can be developed on the back or the sides of a head, the shoulder blades, lower
back or hips or can be tail bone, the ankle, heel as well as the skin behind the knees, back of the arms
and legs where they rest against the chair, shoulder blades and spine as well.
132726884 / Anna Rassadnikova / shutterstock.com
Discuss 4 pressure relieving devices that may be used for John either in hospital or when he
goes back to the aged care facility.
The pressure relieving devices which can be used in John's case when he goes back to an aged care
facility such as:
Crash mats
Hip and elbow pads
Pressure relieving mattresses
Pressure cushions for elder people (Using Pressure Relieveing Equipment In a Care Home,
2018).
3. Match the Ulcer type with their specific characteristic
Ulcer type: Venous ulcers, Diabetic ulcers, Arterial ulcers, Pressure ulcer:
Ulcer type Characteristic
Arterial ulcers Caused by ischemia; related to the presence of arterial occlusive
disease; symptoms include pain and tissue loss
Venous ulcers Local losses of epidermis and various levels of dermis and
subcutaneous tissue, occurring over or near the malleoli at the
distal lower extremities; caused by edema and other sequalae of
impaired venous return.
Diabetic ulcers Caused by trauma or pressure secondary to neuropathy or
vascular disease related to diabetes mellitus.
123 TMP E – Assessment Template – Written v1.3 Page 10 of 24
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
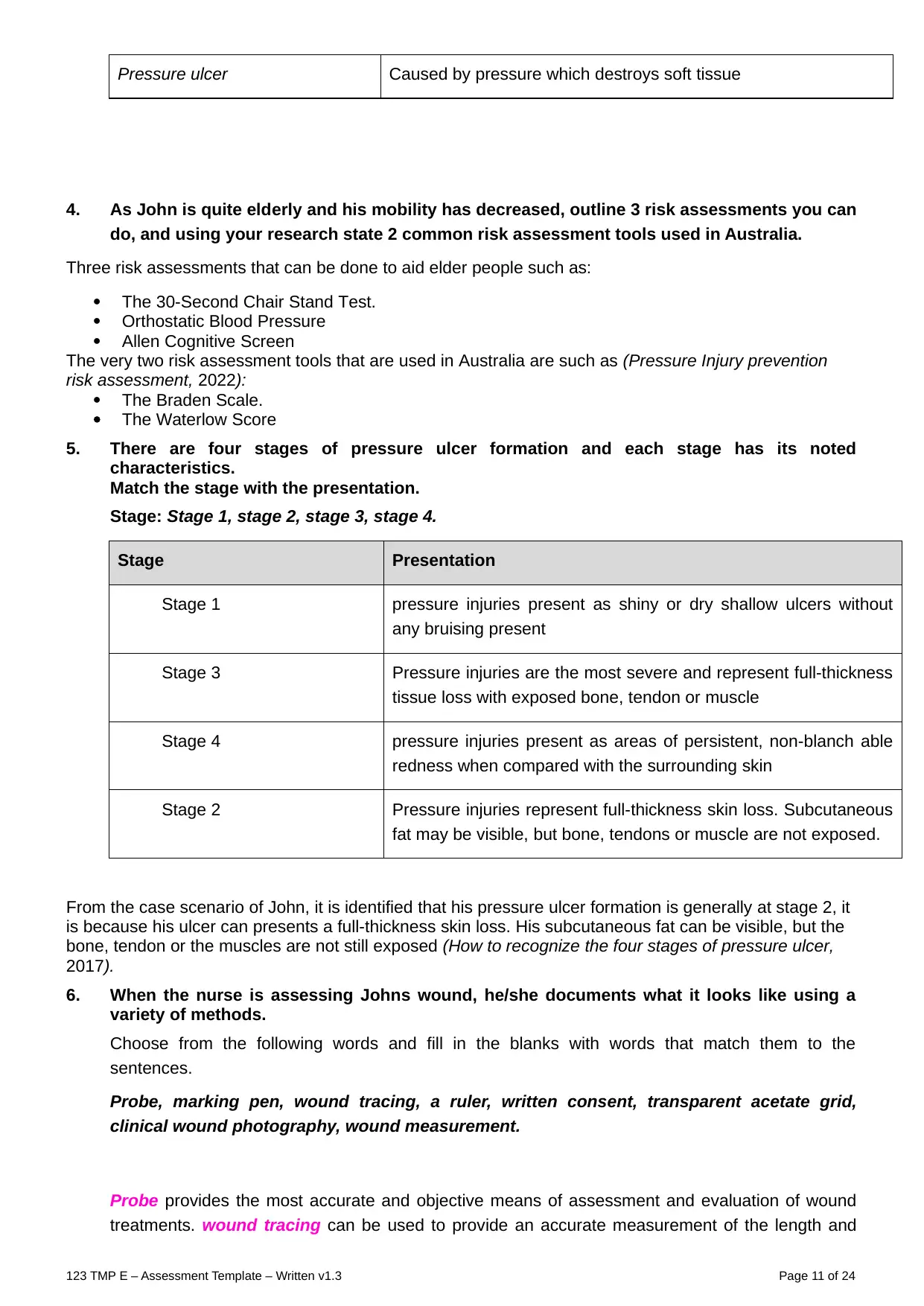
Pressure ulcer Caused by pressure which destroys soft tissue
4. As John is quite elderly and his mobility has decreased, outline 3 risk assessments you can
do, and using your research state 2 common risk assessment tools used in Australia.
Three risk assessments that can be done to aid elder people such as:
The 30-Second Chair Stand Test.
Orthostatic Blood Pressure
Allen Cognitive Screen
The very two risk assessment tools that are used in Australia are such as (Pressure Injury prevention
risk assessment, 2022):
The Braden Scale.
The Waterlow Score
5. There are four stages of pressure ulcer formation and each stage has its noted
characteristics.
Match the stage with the presentation.
Stage: Stage 1, stage 2, stage 3, stage 4.
Stage Presentation
Stage 1 pressure injuries present as shiny or dry shallow ulcers without
any bruising present
Stage 3 Pressure injuries are the most severe and represent full-thickness
tissue loss with exposed bone, tendon or muscle
Stage 4 pressure injuries present as areas of persistent, non-blanch able
redness when compared with the surrounding skin
Stage 2 Pressure injuries represent full-thickness skin loss. Subcutaneous
fat may be visible, but bone, tendons or muscle are not exposed.
From the case scenario of John, it is identified that his pressure ulcer formation is generally at stage 2, it
is because his ulcer can presents a full-thickness skin loss. His subcutaneous fat can be visible, but the
bone, tendon or the muscles are not still exposed (How to recognize the four stages of pressure ulcer,
2017).
6. When the nurse is assessing Johns wound, he/she documents what it looks like using a
variety of methods.
Choose from the following words and fill in the blanks with words that match them to the
sentences.
Probe, marking pen, wound tracing, a ruler, written consent, transparent acetate grid,
clinical wound photography, wound measurement.
Probe provides the most accurate and objective means of assessment and evaluation of wound
treatments. wound tracing can be used to provide an accurate measurement of the length and
123 TMP E – Assessment Template – Written v1.3 Page 11 of 24
4. As John is quite elderly and his mobility has decreased, outline 3 risk assessments you can
do, and using your research state 2 common risk assessment tools used in Australia.
Three risk assessments that can be done to aid elder people such as:
The 30-Second Chair Stand Test.
Orthostatic Blood Pressure
Allen Cognitive Screen
The very two risk assessment tools that are used in Australia are such as (Pressure Injury prevention
risk assessment, 2022):
The Braden Scale.
The Waterlow Score
5. There are four stages of pressure ulcer formation and each stage has its noted
characteristics.
Match the stage with the presentation.
Stage: Stage 1, stage 2, stage 3, stage 4.
Stage Presentation
Stage 1 pressure injuries present as shiny or dry shallow ulcers without
any bruising present
Stage 3 Pressure injuries are the most severe and represent full-thickness
tissue loss with exposed bone, tendon or muscle
Stage 4 pressure injuries present as areas of persistent, non-blanch able
redness when compared with the surrounding skin
Stage 2 Pressure injuries represent full-thickness skin loss. Subcutaneous
fat may be visible, but bone, tendons or muscle are not exposed.
From the case scenario of John, it is identified that his pressure ulcer formation is generally at stage 2, it
is because his ulcer can presents a full-thickness skin loss. His subcutaneous fat can be visible, but the
bone, tendon or the muscles are not still exposed (How to recognize the four stages of pressure ulcer,
2017).
6. When the nurse is assessing Johns wound, he/she documents what it looks like using a
variety of methods.
Choose from the following words and fill in the blanks with words that match them to the
sentences.
Probe, marking pen, wound tracing, a ruler, written consent, transparent acetate grid,
clinical wound photography, wound measurement.
Probe provides the most accurate and objective means of assessment and evaluation of wound
treatments. wound tracing can be used to provide an accurate measurement of the length and
123 TMP E – Assessment Template – Written v1.3 Page 11 of 24
width of a wound Assessment of the depth or length of a wound can be performed using a wound
measurement. Using a two-dimensional method, such as by tracing the margins of the wound,
can be assessed using a ruler and marking pen. It is essential that written consent is obtained
from the patient/relative or carer prior to taking photographs.
7. Johns doctor has ordered a Doppler ultrasound, explain what this means and how it is
performed?
Doppler ultrasound is generally a noninvasive test which can be used to determine the flow of blood via
the blood vessels by simply bouncing the high-frequency sound waves off circulating the red blood cells.
The healthcare professional of John have ordered one for him it is because it is more often used for
evaluating the inflammation of a subcutaneous tissue that is caused by the pressure ulcers, but the color
Doppler mode can aid to improve the determination of an inflammatory edema in the subcutaneous fat
and a necrotic tissue in the pressure ulcers as well (Color Doppler Ultrasonography to Evaluate
Hypoechoic Areas in Pressure Ulcers, 2018).
8. Identify and discuss 2 effects on wound healing in regards to complex and challenging)
wounds.
Factor Effect on wound healing
Age of the patient Everything can slow down as age of a person enhances. In
this, an inflammatory response is decreased or delayed as is
the proliferative response. The remodeling can occur, but to a
lesser degree as well as the collagen is formed is qualitatively
different.
Poor Blood
Circulation
It is generally the most dramatic element which can influence
the healing of a wound. The nutrients as well as the oxygen
which a new blood can carry towards the wound are generally
the key to a successful healing.
9. Many factors affect the wound-healing process. Therefore, wound management strategies
must be tailored to meet the individual holistic needs of the patient, their wound and their
environment.
Tick the sentence that best outlines the principles of wound management
◻ Assess and correct cause of tissue damage
◻ Assess wound history and characteristics
◻ Ensure adequate tissue perfusion
◻ Wound-bed preparation
◻ Wound cleansing
◻ Wound-cleansing solutions and techniques
◻ All of the above
Case study
Case Study Scenario 3 – Infected Surgical Wound:
Ms Maggie Malone is an obese 52-year-old female, who was admitted to the orthopaedic
ward for a total left knee replacement. Staples were the method of wound closure.
123 TMP E – Assessment Template – Written v1.3 Page 12 of 24
measurement. Using a two-dimensional method, such as by tracing the margins of the wound,
can be assessed using a ruler and marking pen. It is essential that written consent is obtained
from the patient/relative or carer prior to taking photographs.
7. Johns doctor has ordered a Doppler ultrasound, explain what this means and how it is
performed?
Doppler ultrasound is generally a noninvasive test which can be used to determine the flow of blood via
the blood vessels by simply bouncing the high-frequency sound waves off circulating the red blood cells.
The healthcare professional of John have ordered one for him it is because it is more often used for
evaluating the inflammation of a subcutaneous tissue that is caused by the pressure ulcers, but the color
Doppler mode can aid to improve the determination of an inflammatory edema in the subcutaneous fat
and a necrotic tissue in the pressure ulcers as well (Color Doppler Ultrasonography to Evaluate
Hypoechoic Areas in Pressure Ulcers, 2018).
8. Identify and discuss 2 effects on wound healing in regards to complex and challenging)
wounds.
Factor Effect on wound healing
Age of the patient Everything can slow down as age of a person enhances. In
this, an inflammatory response is decreased or delayed as is
the proliferative response. The remodeling can occur, but to a
lesser degree as well as the collagen is formed is qualitatively
different.
Poor Blood
Circulation
It is generally the most dramatic element which can influence
the healing of a wound. The nutrients as well as the oxygen
which a new blood can carry towards the wound are generally
the key to a successful healing.
9. Many factors affect the wound-healing process. Therefore, wound management strategies
must be tailored to meet the individual holistic needs of the patient, their wound and their
environment.
Tick the sentence that best outlines the principles of wound management
◻ Assess and correct cause of tissue damage
◻ Assess wound history and characteristics
◻ Ensure adequate tissue perfusion
◻ Wound-bed preparation
◻ Wound cleansing
◻ Wound-cleansing solutions and techniques
◻ All of the above
Case study
Case Study Scenario 3 – Infected Surgical Wound:
Ms Maggie Malone is an obese 52-year-old female, who was admitted to the orthopaedic
ward for a total left knee replacement. Staples were the method of wound closure.
123 TMP E – Assessment Template – Written v1.3 Page 12 of 24
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 24

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.