Executive Summary: Value Stream Mapping in Emergency Department Report
VerifiedAdded on 2022/10/12
|10
|3486
|224
Report
AI Summary
This report presents an executive summary of a value stream mapping (VSM) analysis conducted in a hospital's emergency department (ED). The primary goal is to assess and optimize patient turnaround time by identifying and reducing waiting times, considered as waste within the Lean Six Sigma framework. The study examines the current state VSM to pinpoint system archetypes that impede performance, such as overcrowding, understaffing, and inefficient information flow. The report proposes a new state VSM, implementing changes like a triage station, division of the ED into care units, and electronic communication channels. These changes aim to improve patient flow, reduce waiting times, and enhance the overall quality of care. The analysis includes a discussion on the intended and unintended consequences of the modified system, emphasizing the need for continuous improvement and adaptation within the dynamic healthcare environment. The report concludes by highlighting the potential benefits of the proposed changes and provides recommendations for future implementation and research.
1
Systems Thinking
Executive Summary
The given report deals with the use of lean six sigma tool of value stream mapping in
the context of a hospital emergency department. The aim of the mapping tool is to be
able to assess how the time of the patient is utilized in an emergency department and
identify the waiting time as waste. It is necessary to decrease the delays and waiting
time of the patients in the ED so that the quality of care provided them is enhanced.
Moreover, in some cases patients with complications are brought in who require to be
treated urgently. Through the use of the value stream mapping tool a system will be
created in the ED that minimizes the time when the patients have to wait. This has been
achieved in the proposed recommendation by deploying the workforce in a systematic
manner.
Systems Thinking
Executive Summary
The given report deals with the use of lean six sigma tool of value stream mapping in
the context of a hospital emergency department. The aim of the mapping tool is to be
able to assess how the time of the patient is utilized in an emergency department and
identify the waiting time as waste. It is necessary to decrease the delays and waiting
time of the patients in the ED so that the quality of care provided them is enhanced.
Moreover, in some cases patients with complications are brought in who require to be
treated urgently. Through the use of the value stream mapping tool a system will be
created in the ED that minimizes the time when the patients have to wait. This has been
achieved in the proposed recommendation by deploying the workforce in a systematic
manner.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Systems Thinking
Table of Contents
Introduction/ Background............................................................................................................. 3
Body............................................................................................................................................ 3
Identification and analysis of the System Archetypes that may impede performance..................3
Analysis of the current State Value Stream Map of the emergency department based on System
Archetypes................................................................................................................................... 4
Recommended new State Value Stream Map with the desired reduction in patient turnaround
time.............................................................................................................................................. 5
Discussions on intended and unintended consequences of the modified system........................8
Conclusion................................................................................................................................... 8
References................................................................................................................................ 10
Systems Thinking
Table of Contents
Introduction/ Background............................................................................................................. 3
Body............................................................................................................................................ 3
Identification and analysis of the System Archetypes that may impede performance..................3
Analysis of the current State Value Stream Map of the emergency department based on System
Archetypes................................................................................................................................... 4
Recommended new State Value Stream Map with the desired reduction in patient turnaround
time.............................................................................................................................................. 5
Discussions on intended and unintended consequences of the modified system........................8
Conclusion................................................................................................................................... 8
References................................................................................................................................ 10
3
Systems Thinking
Introduction/ Background
Assessing the movement of time is enormously significant in healthcare conditions.
Time is of the embodiment of patients' lives which are at risk Healthcare specialists,
supervisors and nursing facilitators are especially worried about understanding where
postponements happen in healthcare administration. The aim is to identify those
deferrals and ensure they are improved and patients get the most ideal treatment as
fast as possible. In order to comprehend the delays, a Lean improvement device: Value
Stream Mapping (VSM) has been connected to the Emergency Department (ED) in the
given hospital in the case study. This report writes about the discoveries from that VSM
look into and especially the utilization of the VSM perception. It features the issues of
patient delays utilizing the VSM approach and how this immensely significant research
territory requires an improved VSM chart to pass on data to therapeutic and clinical
agents about patients.
Body
The clinical crisis medicinal consideration frameworks, and patient experience of these
frameworks were inspected from the point of view of 'Lean theory', and utilizing the
quantitative methodological methodology of VSM (Donley, 2019). It portrays care
procedures and holding up times between procedure steps, researching the effects of
various consideration models on patient experience. The report depicts care procedures
and holding up times between procedure steps, examining the effects of various
consideration models on patient experience.
Identification and analysis of the System Archetypes that may impede
performance
Customarily VSM has been utilized as an iterative procedure to improve hierarchical
productivity by lessening or disposing of waste; be that as it may, for our venture we
utilized the planning information to build comprehension of the occasions taken during
patient pathways. The VSM investigation inspected patient activities, during which the
proportion of action to holding up time was resolved. Movement watched was
transcendently patient contact time or activity identified with their consideration that was
seen or known to the patient; complying with the Lean idea of a worthy movement. The
Lean idea of waste does not make an interpretation of legitimately to the social
insurance setting, were holding up might be important to precisely evaluate a patient's
condition.
The greatest cause of delayed processes and treatments is overcrowding (Chen et al.
2015). The time that a patient considers as delay or wasteful may actually be used by
the healthcare professionals for other patients. The resources and workforce are limited
and all the patients have to be cared for through the use of these limited resources and
Systems Thinking
Introduction/ Background
Assessing the movement of time is enormously significant in healthcare conditions.
Time is of the embodiment of patients' lives which are at risk Healthcare specialists,
supervisors and nursing facilitators are especially worried about understanding where
postponements happen in healthcare administration. The aim is to identify those
deferrals and ensure they are improved and patients get the most ideal treatment as
fast as possible. In order to comprehend the delays, a Lean improvement device: Value
Stream Mapping (VSM) has been connected to the Emergency Department (ED) in the
given hospital in the case study. This report writes about the discoveries from that VSM
look into and especially the utilization of the VSM perception. It features the issues of
patient delays utilizing the VSM approach and how this immensely significant research
territory requires an improved VSM chart to pass on data to therapeutic and clinical
agents about patients.
Body
The clinical crisis medicinal consideration frameworks, and patient experience of these
frameworks were inspected from the point of view of 'Lean theory', and utilizing the
quantitative methodological methodology of VSM (Donley, 2019). It portrays care
procedures and holding up times between procedure steps, researching the effects of
various consideration models on patient experience. The report depicts care procedures
and holding up times between procedure steps, examining the effects of various
consideration models on patient experience.
Identification and analysis of the System Archetypes that may impede
performance
Customarily VSM has been utilized as an iterative procedure to improve hierarchical
productivity by lessening or disposing of waste; be that as it may, for our venture we
utilized the planning information to build comprehension of the occasions taken during
patient pathways. The VSM investigation inspected patient activities, during which the
proportion of action to holding up time was resolved. Movement watched was
transcendently patient contact time or activity identified with their consideration that was
seen or known to the patient; complying with the Lean idea of a worthy movement. The
Lean idea of waste does not make an interpretation of legitimately to the social
insurance setting, were holding up might be important to precisely evaluate a patient's
condition.
The greatest cause of delayed processes and treatments is overcrowding (Chen et al.
2015). The time that a patient considers as delay or wasteful may actually be used by
the healthcare professionals for other patients. The resources and workforce are limited
and all the patients have to be cared for through the use of these limited resources and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
Systems Thinking
within the stipulated time. It was seen in the VSM chart provided, that the patient also
has to wait for an available room. The infrastructure of the hospital is unable to meet the
increased demands and need to be extended as soon as possible.
The next reason can be that the hospital is understaffed or the equipment required for
care is not sufficient for the workload. As a result, care professionals and patients have
to wait for their turn.
In the given case scenario, it was clear from the VSM that a patient information is
handled from one person to another for processing and maintaining records. There is no
uniform flow of information which causes care professionals and the patients to move
from one end to another. It is clear that there is a need for streamlining the
communication channels in the emergency department (Montes et al. 2019).
Another issue noted was that there is no uniform procedure through which a patient
accesses care. In some cases, he is taken to a resident nurse first, in others he is
directly taken to the doctor and in some, they have to go through patient registration
processes first. The differences can be streamlined so that the care quality provided to
the patients are uniform.
Analysis of the current State Value Stream Map of the emergency department
based on System Archetypes
It is essential to note one factor when we make use of VSM for charting the delays that
it has been recorded from a patient’s or care seekers point of view. They have been
situated in the center of the whole scenario. The pause in an activity that they consider
as delays may actually be deployed for important procedures that they are not aware of.
As a result, VSM charting is a very user-centric modelling tool. The main inference is
that the patient may not be aware of the overcrowding and the limited resources that are
present in the emergency department but will expect top grade service.
From a close inspection of the value stream map, it is clear that the flow of information
is chaotic and goes through various channels which need to be simplified. The attending
nurse has been allocated with too many duties in the emergency department and also
has to be deal with the patient first hand. They are required to collect information from
the patient, process the information and present the vital data to the doctor, look for
available resources like rooms and equipment (Chiu et al. 2018). They are also required
to fetch supplies like medicines and other paraphernalia. Burdening single person with
many responsibilities is likely to slow down the process. This may be because the
department is understaffed or there is not a clear channel of communication and
understanding of roles.
The patient information is transferred from one attendee to another and finally to the
doctor or the physician. Moreover, the information is collected at various steps and not
in one go. The first phase of enquiry deals with insurance details and about the nature
of the injury. Depending on the issue of the patient, they are delegated to another
attendee who collects the patient's history and present condition (Oh et al. 2016).
Another nurse enters the process to record the patient’s vitals. If more probing tests are
required then the patient has to wait further for their turn for the equipment to be
available. The information is summed up and only the critical information is forwarded to
Systems Thinking
within the stipulated time. It was seen in the VSM chart provided, that the patient also
has to wait for an available room. The infrastructure of the hospital is unable to meet the
increased demands and need to be extended as soon as possible.
The next reason can be that the hospital is understaffed or the equipment required for
care is not sufficient for the workload. As a result, care professionals and patients have
to wait for their turn.
In the given case scenario, it was clear from the VSM that a patient information is
handled from one person to another for processing and maintaining records. There is no
uniform flow of information which causes care professionals and the patients to move
from one end to another. It is clear that there is a need for streamlining the
communication channels in the emergency department (Montes et al. 2019).
Another issue noted was that there is no uniform procedure through which a patient
accesses care. In some cases, he is taken to a resident nurse first, in others he is
directly taken to the doctor and in some, they have to go through patient registration
processes first. The differences can be streamlined so that the care quality provided to
the patients are uniform.
Analysis of the current State Value Stream Map of the emergency department
based on System Archetypes
It is essential to note one factor when we make use of VSM for charting the delays that
it has been recorded from a patient’s or care seekers point of view. They have been
situated in the center of the whole scenario. The pause in an activity that they consider
as delays may actually be deployed for important procedures that they are not aware of.
As a result, VSM charting is a very user-centric modelling tool. The main inference is
that the patient may not be aware of the overcrowding and the limited resources that are
present in the emergency department but will expect top grade service.
From a close inspection of the value stream map, it is clear that the flow of information
is chaotic and goes through various channels which need to be simplified. The attending
nurse has been allocated with too many duties in the emergency department and also
has to be deal with the patient first hand. They are required to collect information from
the patient, process the information and present the vital data to the doctor, look for
available resources like rooms and equipment (Chiu et al. 2018). They are also required
to fetch supplies like medicines and other paraphernalia. Burdening single person with
many responsibilities is likely to slow down the process. This may be because the
department is understaffed or there is not a clear channel of communication and
understanding of roles.
The patient information is transferred from one attendee to another and finally to the
doctor or the physician. Moreover, the information is collected at various steps and not
in one go. The first phase of enquiry deals with insurance details and about the nature
of the injury. Depending on the issue of the patient, they are delegated to another
attendee who collects the patient's history and present condition (Oh et al. 2016).
Another nurse enters the process to record the patient’s vitals. If more probing tests are
required then the patient has to wait further for their turn for the equipment to be
available. The information is summed up and only the critical information is forwarded to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
Systems Thinking
the doctor or the attending physician. At each step, the patient has to wait for his turn
and for the paperwork to be cleared. The paperwork and treatment information they
need to be carried forward to the record department and to the insurance company. The
patient does not have to wait much for the last step (Doğan & Unutulmaz, 2016).
However, they are required to stay in contact with the hospital until their dues have
been cleared by the insurance company.
Recommended new State Value Stream Map with the desired reduction in patient
turnaround time
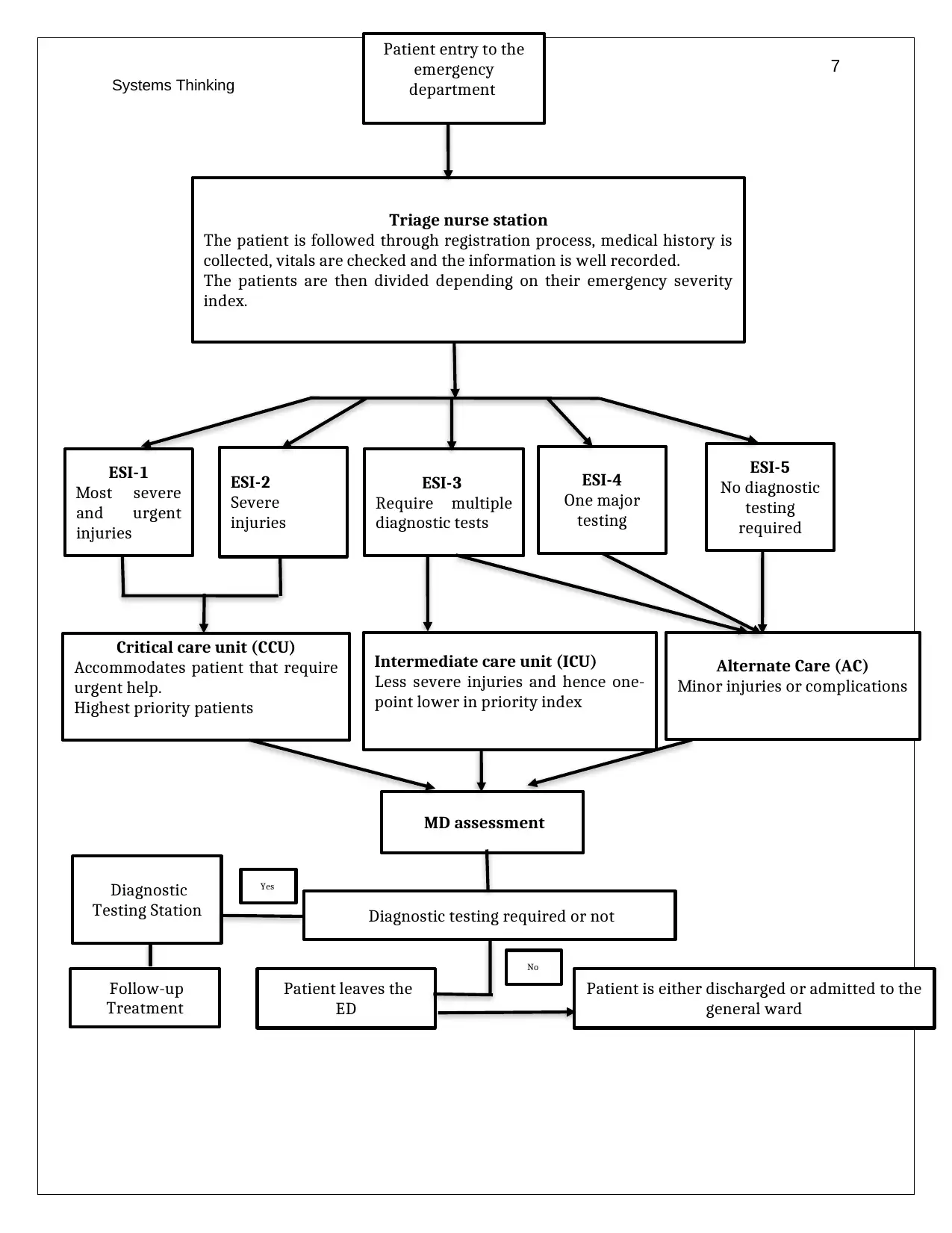
The changes established in the new system and shown in the value stream map are as
follows:
1. Triage station: earlier in the case study VSM it was seen that the patient was
intimated in a haphazard manner. They were at times registered at the front
office whereas at other times a registered nurse or attendee collected their
information. In some situations, it was also seen that the patient was also allowed
to directly reach out to the doctor as well. This system was dependent on the
availability of healthcare professionals. In the recommended system, a triage
consisting of a nurse, a physician and an attendee (Wang, Yang, Yang & Chan,
2015). They will be responsible for collecting information from the patient and for
dividing them upon the severity of their complications. This will provide clear
identification of roles and the nurses will forward them towards the next phase of
treatment. This is an important phase as the basic level diagnosis provided the
prognosis and the approach of treatment.
2. The emergency department has been divided into three units: the critical care
unit, the intermediate care unit and the alternate care unit. The nurses are
required to assess the patients based on the intensity of their injuries or
complications. Depending on this they will be forwarded to one of the suitable
care units within the emergency department. This ensures that the resources and
facilities are managed in a manner that the ones that require immediate help are
prioritized. Moreover, patients are also assessed whether they would require
further diagnostic tests or not. This factor will position them in a ward from the
diagnostic labs are near and the time otherwise used to shift the patients or their
specimens from one area to another. Also, all positioning all the patients that
require a given laboratory test also ensures that the lab attendants are able to
manage the time better so that the waiting time is decreased (Ncbi, 2018).
3. The patients that are ready to be discharged from the ER units will be first
reviewed by another doctor and tests may be required in this case. This
physician will decide if the patient requires further care and should be admitted in
the general ward. This is another addition in the emergency department
processes and is aimed to ensure patient wellbeing and health. This way the
patient is attended upon by an experienced physician who provides them with the
prognosis after their stay and treatment.
4. One aspect that has not been included in the VSM, is the establishment of
electronic communication channels through which patient history will be
Systems Thinking
the doctor or the attending physician. At each step, the patient has to wait for his turn
and for the paperwork to be cleared. The paperwork and treatment information they
need to be carried forward to the record department and to the insurance company. The
patient does not have to wait much for the last step (Doğan & Unutulmaz, 2016).
However, they are required to stay in contact with the hospital until their dues have
been cleared by the insurance company.
Recommended new State Value Stream Map with the desired reduction in patient
turnaround time
The changes established in the new system and shown in the value stream map are as
follows:
1. Triage station: earlier in the case study VSM it was seen that the patient was
intimated in a haphazard manner. They were at times registered at the front
office whereas at other times a registered nurse or attendee collected their
information. In some situations, it was also seen that the patient was also allowed
to directly reach out to the doctor as well. This system was dependent on the
availability of healthcare professionals. In the recommended system, a triage
consisting of a nurse, a physician and an attendee (Wang, Yang, Yang & Chan,
2015). They will be responsible for collecting information from the patient and for
dividing them upon the severity of their complications. This will provide clear
identification of roles and the nurses will forward them towards the next phase of
treatment. This is an important phase as the basic level diagnosis provided the
prognosis and the approach of treatment.
2. The emergency department has been divided into three units: the critical care
unit, the intermediate care unit and the alternate care unit. The nurses are
required to assess the patients based on the intensity of their injuries or
complications. Depending on this they will be forwarded to one of the suitable
care units within the emergency department. This ensures that the resources and
facilities are managed in a manner that the ones that require immediate help are
prioritized. Moreover, patients are also assessed whether they would require
further diagnostic tests or not. This factor will position them in a ward from the
diagnostic labs are near and the time otherwise used to shift the patients or their
specimens from one area to another. Also, all positioning all the patients that
require a given laboratory test also ensures that the lab attendants are able to
manage the time better so that the waiting time is decreased (Ncbi, 2018).
3. The patients that are ready to be discharged from the ER units will be first
reviewed by another doctor and tests may be required in this case. This
physician will decide if the patient requires further care and should be admitted in
the general ward. This is another addition in the emergency department
processes and is aimed to ensure patient wellbeing and health. This way the
patient is attended upon by an experienced physician who provides them with the
prognosis after their stay and treatment.
4. One aspect that has not been included in the VSM, is the establishment of
electronic communication channels through which patient history will be
6
Systems Thinking
maintained and updated. Also, the communication of key information will be
made easy as many people will be informed at the same time. IN the VSM chart
provided along with the case study, the channel of communication was
overlapping one another as a result of which a lot of time was wasted in
assembling the information from the various sources who have collected it from
the patient.
Systems Thinking
maintained and updated. Also, the communication of key information will be
made easy as many people will be informed at the same time. IN the VSM chart
provided along with the case study, the channel of communication was
overlapping one another as a result of which a lot of time was wasted in
assembling the information from the various sources who have collected it from
the patient.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
Systems Thinking
Patient is either discharged or admitted to the
general ward
Patient leaves the
ED
Diagnostic
Testing Station
Yes
Diagnostic testing required or not
MD assessment
Patient entry to the
emergency
department
Alternate Care (AC)
Minor injuries or complications
Intermediate care unit (ICU)
Less severe injuries and hence one-
point lower in priority index
Critical care unit (CCU)
Accommodates patient that require
urgent help.
Highest priority patients
ESI-5
No diagnostic
testing
required
ESI-4
One major
testing
ESI-1
Most severe
and urgent
injuries
ESI-3
Require multiple
diagnostic tests
Triage nurse station
The patient is followed through registration process, medical history is
collected, vitals are checked and the information is well recorded.
The patients are then divided depending on their emergency severity
index.
ESI-2
Severe
injuries
No
Follow-up
Treatment
Systems Thinking
Patient is either discharged or admitted to the
general ward
Patient leaves the
ED
Diagnostic
Testing Station
Yes
Diagnostic testing required or not
MD assessment
Patient entry to the
emergency
department
Alternate Care (AC)
Minor injuries or complications
Intermediate care unit (ICU)
Less severe injuries and hence one-
point lower in priority index
Critical care unit (CCU)
Accommodates patient that require
urgent help.
Highest priority patients
ESI-5
No diagnostic
testing
required
ESI-4
One major
testing
ESI-1
Most severe
and urgent
injuries
ESI-3
Require multiple
diagnostic tests
Triage nurse station
The patient is followed through registration process, medical history is
collected, vitals are checked and the information is well recorded.
The patients are then divided depending on their emergency severity
index.
ESI-2
Severe
injuries
No
Follow-up
Treatment
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
Systems Thinking
Discussions on intended and unintended consequences of the modified system
The intended consequences
The proposed VSM model sets a triage of the nurse, physician and other healthcare
personnel is positioned at the start of the chart. The patients need to go through them
and are segregated in the process into various departments. Setting this triage at the
first step ensures that the information is collected from the patients. The information is
available to all three professionals and hence the patient needs not to be harangued. All
critical information will be scanned by the nurses and then will be transferred to the
required attendee. This will ensure that the communication channel regarding at least
patient information is streamlined. The triage nurses will look over the registration as
well as the medical history of the patient (Improta et al. 2018). They will be also
responsible for
Another issue that will be resolved in this system is that there is no need to transfer the
patient from one department to another and also forward their specimens. The
information will be collected in an ordered manner and in a consequence that minimizes
the need for transferring the test records or specimens. This will also decrease the time
that a patient has to wait for their turn.
The unintended consequences
The VSM chart masks a great number of processes and happenings that are key to the
healthcare system and happen behind the eye of the patient. The chart is unable to
account for these processes and as pointed out earlier is a user-centric model. One
unintended consequence could be that in order to fasten the process in which a patient
gets help can mean that the processes that are not portrayed in the chart have to be
hurried up. For instance, the proceedings between the hospital and the insurance
provider cannot be covered in the chart and are not directly disclosed to the patient. Yet
it is one of the most time-consuming steps in the emergency department.
Since, it has been assumed that the emergency department is understaffed and
workload is too great, focusing the nurse triage in step one may put pressure on other
areas that they were earlier looking after (Grzywinski et al. 2019). The recommended
VSM should also be with approved along with hiring more staff so that the present staff
are not overworked. Another consequence could be that a sudden change in the system
may require some time for the involved personnel to get acquainted with. During this
time, it is likely that they will not be able to provide quality care or may take more time
than usual.
Conclusion
The goal of picturing time information in EDs is indispensably significant. VSM is one
approach to do this yet it requires improvement so as to satisfy the necessities of
medicinal services specialist co-ops. This would require that the VSM is upgraded to
pass on key data about territories of deferral, all together that clinical chiefs, ED
directors and stream facilitators can comprehend the ED procedure as effectively and
as rapidly as could be expected under the circumstances. The VSM in the given case
Systems Thinking
Discussions on intended and unintended consequences of the modified system
The intended consequences
The proposed VSM model sets a triage of the nurse, physician and other healthcare
personnel is positioned at the start of the chart. The patients need to go through them
and are segregated in the process into various departments. Setting this triage at the
first step ensures that the information is collected from the patients. The information is
available to all three professionals and hence the patient needs not to be harangued. All
critical information will be scanned by the nurses and then will be transferred to the
required attendee. This will ensure that the communication channel regarding at least
patient information is streamlined. The triage nurses will look over the registration as
well as the medical history of the patient (Improta et al. 2018). They will be also
responsible for
Another issue that will be resolved in this system is that there is no need to transfer the
patient from one department to another and also forward their specimens. The
information will be collected in an ordered manner and in a consequence that minimizes
the need for transferring the test records or specimens. This will also decrease the time
that a patient has to wait for their turn.
The unintended consequences
The VSM chart masks a great number of processes and happenings that are key to the
healthcare system and happen behind the eye of the patient. The chart is unable to
account for these processes and as pointed out earlier is a user-centric model. One
unintended consequence could be that in order to fasten the process in which a patient
gets help can mean that the processes that are not portrayed in the chart have to be
hurried up. For instance, the proceedings between the hospital and the insurance
provider cannot be covered in the chart and are not directly disclosed to the patient. Yet
it is one of the most time-consuming steps in the emergency department.
Since, it has been assumed that the emergency department is understaffed and
workload is too great, focusing the nurse triage in step one may put pressure on other
areas that they were earlier looking after (Grzywinski et al. 2019). The recommended
VSM should also be with approved along with hiring more staff so that the present staff
are not overworked. Another consequence could be that a sudden change in the system
may require some time for the involved personnel to get acquainted with. During this
time, it is likely that they will not be able to provide quality care or may take more time
than usual.
Conclusion
The goal of picturing time information in EDs is indispensably significant. VSM is one
approach to do this yet it requires improvement so as to satisfy the necessities of
medicinal services specialist co-ops. This would require that the VSM is upgraded to
pass on key data about territories of deferral, all together that clinical chiefs, ED
directors and stream facilitators can comprehend the ED procedure as effectively and
as rapidly as could be expected under the circumstances. The VSM in the given case

9
Systems Thinking
study presented a key information about how the system archetype in the Emergency
department was chaotic and had unnecessary channels through which the information
was passed and the patient had to wait. These channels need to be simplified and the
issues of understaffing need to be resolved.
Tragically, the present VSM representation instruments do not fit perfectly into the
healthcare and insurance setting. Significant enhancements are required with the goal
that planning information is graphed from a patient's point of view, also, shows how the
time is utilized by the healthcare professionals. However, it does not account for how
the time during which the patient appears to be waiting is used by the professionals.
They are deployed to care for other patients and have different responsibilities to fulfil.
As a result, as long as the patient to healthcare professional ratio is not balanced the
delay will always be there. However, the aim of the report was to use VSM to chart the
journey of the patient and in the meantime decrease the waiting time.
Systems Thinking
study presented a key information about how the system archetype in the Emergency
department was chaotic and had unnecessary channels through which the information
was passed and the patient had to wait. These channels need to be simplified and the
issues of understaffing need to be resolved.
Tragically, the present VSM representation instruments do not fit perfectly into the
healthcare and insurance setting. Significant enhancements are required with the goal
that planning information is graphed from a patient's point of view, also, shows how the
time is utilized by the healthcare professionals. However, it does not account for how
the time during which the patient appears to be waiting is used by the professionals.
They are deployed to care for other patients and have different responsibilities to fulfil.
As a result, as long as the patient to healthcare professional ratio is not balanced the
delay will always be there. However, the aim of the report was to use VSM to chart the
journey of the patient and in the meantime decrease the waiting time.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
Systems Thinking
References
Chen, J., Bellomo, R., Flabouris, A., Hillman, K., Assareh, H., & Ou, L. (2015). Delayed
emergency team calls and associated hospital mortality: a multicenter
study. Critical care medicine, 43(10), 2059-2065.
Chiu, I. M., Lin, Y. R., Syue, Y. J., Kung, C. T., Wu, K. H., & Li, C. J. (2018). The
influence of crowding on clinical practice in the emergency department. The
American journal of emergency medicine, 36(1), 56-60.
Doğan, N. Ö., & Unutulmaz, O. (2016). Lean production in healthcare: a simulation-
based value stream mapping in the physical therapy and rehabilitation
department of a public hospital. Total Quality Management & Business
Excellence, 27(1-2), 64-80.
Donley, E. (2019). Delays in admitting aged persons to the mental health ward from the
emergency department. Emergency Medicine and Health Care, 6(1), 1.
Grzywinski, M., Carlisle, S., Coleman, J., Cook, C., Hayden, G., Pugliese, R., ... & Ku,
B. (2019). Development of a Novel Emergency Department Mapping
Tool. HERD: Health Environments Research & Design Journal,
1937586719842349.
Improta, G., Romano, M., Di Cicco, M. V., Ferraro, A., Borrelli, A., Verdoliva, C., ... &
Cesarelli, M. (2018). Lean thinking to improve emergency department throughput
at AORN Cardarelli hospital. BMC health services research, 18(1), 914.
Montes, F. R., Vásquez, S. M., Camargo-Rojas, C. M., Rueda, M. V., Góez-Mogollón,
L., Alvarado, P. A., ... & Villar, J. C. (2019). Association between emergency
department length of stay and adverse perioperative outcomes in emergency
surgery: a cohort study in two Colombian University hospitals. BMC emergency
medicine, 19(1), 27.
Ncbi, (2018), Value stream mapping of patient journeys in hospital mergency medical
care Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK338864/
Oh, C., Novotny, A. M., Carter, P. L., Ready, R. K., Campbell, D. D., & Leckie, M. C.
(2016). Use of a simulation-based decision support tool to improve emergency
department throughput. Operations research for health care, 9, 29-39.
Wang, T. K., Yang, T., Yang, C. Y., & Chan, F. T. (2015). Lean principles and simulation
optimization for emergency department layout design. Industrial Management &
Data Systems, 115(4), 678-699.
Systems Thinking
References
Chen, J., Bellomo, R., Flabouris, A., Hillman, K., Assareh, H., & Ou, L. (2015). Delayed
emergency team calls and associated hospital mortality: a multicenter
study. Critical care medicine, 43(10), 2059-2065.
Chiu, I. M., Lin, Y. R., Syue, Y. J., Kung, C. T., Wu, K. H., & Li, C. J. (2018). The
influence of crowding on clinical practice in the emergency department. The
American journal of emergency medicine, 36(1), 56-60.
Doğan, N. Ö., & Unutulmaz, O. (2016). Lean production in healthcare: a simulation-
based value stream mapping in the physical therapy and rehabilitation
department of a public hospital. Total Quality Management & Business
Excellence, 27(1-2), 64-80.
Donley, E. (2019). Delays in admitting aged persons to the mental health ward from the
emergency department. Emergency Medicine and Health Care, 6(1), 1.
Grzywinski, M., Carlisle, S., Coleman, J., Cook, C., Hayden, G., Pugliese, R., ... & Ku,
B. (2019). Development of a Novel Emergency Department Mapping
Tool. HERD: Health Environments Research & Design Journal,
1937586719842349.
Improta, G., Romano, M., Di Cicco, M. V., Ferraro, A., Borrelli, A., Verdoliva, C., ... &
Cesarelli, M. (2018). Lean thinking to improve emergency department throughput
at AORN Cardarelli hospital. BMC health services research, 18(1), 914.
Montes, F. R., Vásquez, S. M., Camargo-Rojas, C. M., Rueda, M. V., Góez-Mogollón,
L., Alvarado, P. A., ... & Villar, J. C. (2019). Association between emergency
department length of stay and adverse perioperative outcomes in emergency
surgery: a cohort study in two Colombian University hospitals. BMC emergency
medicine, 19(1), 27.
Ncbi, (2018), Value stream mapping of patient journeys in hospital mergency medical
care Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK338864/
Oh, C., Novotny, A. M., Carter, P. L., Ready, R. K., Campbell, D. D., & Leckie, M. C.
(2016). Use of a simulation-based decision support tool to improve emergency
department throughput. Operations research for health care, 9, 29-39.
Wang, T. K., Yang, T., Yang, C. Y., & Chan, F. T. (2015). Lean principles and simulation
optimization for emergency department layout design. Industrial Management &
Data Systems, 115(4), 678-699.
1 out of 10
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.