PLOS ONE Systematic Review: Wellbeing, Burnout, and Patient Safety
VerifiedAdded on 2023/03/20
|10
|8156
|91
Report
AI Summary
This report presents a systematic review published in PLOS ONE, investigating the correlation between healthcare staff wellbeing, burnout, and patient safety outcomes. The review analyzed 46 studies, revealing a significant association between poor wellbeing and high burnout levels with adverse patient safety outcomes like medical errors. The research highlights the need for healthcare organizations to address staff mental health and create safer work environments. The review utilized databases like PsychInfo, Medline, Embase, and Scopus, adhering to PRISMA guidelines. The study found that poor wellbeing and moderate to high levels of burnout are associated with poor patient safety outcomes. Further prospective studies, research in primary care, conducted within the UK, and a clearer definition of healthcare staff wellbeing are needed.
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 1/10
Abstract
Objective
To determine whether there is an association between healthcare professionals’ wellbeing and burnout, with patient safety.
Design
Systematic research review.
Data Sources
PsychInfo (1806 to July 2015), Medline (1946 to July 2015), Embase (1947 to July 2015) and Scopus (1823 to July 2015) were
searched, along with reference lists of eligible articles.
Eligibility Criteria for Selecting Studies
Quantitative, empirical studies that included i) either a measure of wellbeing or burnout, and ii) patient safety, in healthcare staff
populations.
Results
Forty-six studies were identified. Sixteen out of the 27 studies that measured wellbeing found a significant correlation between poor
wellbeing and worse patient safety, with six additional studies finding an association with some but not all scales used, and one
study finding a significant association but in the opposite direction to the majority of studies. Twenty-one out of the 30 studies that
measured burnout found a significant association between burnout and patient safety, whilst a further four studies found an
association between one or more (but not all) subscales of the burnout measures employed, and patient safety.
Conclusions
Poor wellbeing and moderate to high levels of burnout are associated, in the majority of studies reviewed, with poor patient safety
outcomes such as medical errors, however the lack of prospective studies reduces the ability to determine causality. Further
prospective studies, research in primary care, conducted within the UK, and a clearer definition of healthcare staff wellbeing are
needed.
Implications
This review illustrates the need for healthcare organisations to consider improving employees’ mental health as well as creating
safer work environments when planning interventions to improve patient safety.
Systematic Review Registration
PROSPERO registration number: CRD42015023340.
Citation: Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB (2016) Healthcare Staff Wellbeing, Burnout, and Patient Safety: A
Systematic Review. PLoS ONE 11(7): e0159015. https://doi.org/10.1371/journal.pone.0159015
Editor: Fiona Harris, University of Stirling, UNITED KINGDOM
Received: March 18, 2016; Accepted: June 24, 2016; Published: July 8, 2016
Copyright: © 2016 Hall et al. This is an open access article distributed under the terms of the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and
source are credited.
Data Availability: All relevant data are within the paper and the Supporting Information files.
Published: July 8, 2016 https://doi.org/10.1371/journal.pone.0159015
Healthcare Sta Wellbeing, Burnout, and Patient Safety: A
Systematic Review
Louise H. Hall , Judith Johnson, Ian Watt, Anastasia Tsipa, Daryl B. O’Connor
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 1/10
Abstract
Objective
To determine whether there is an association between healthcare professionals’ wellbeing and burnout, with patient safety.
Design
Systematic research review.
Data Sources
PsychInfo (1806 to July 2015), Medline (1946 to July 2015), Embase (1947 to July 2015) and Scopus (1823 to July 2015) were
searched, along with reference lists of eligible articles.
Eligibility Criteria for Selecting Studies
Quantitative, empirical studies that included i) either a measure of wellbeing or burnout, and ii) patient safety, in healthcare staff
populations.
Results
Forty-six studies were identified. Sixteen out of the 27 studies that measured wellbeing found a significant correlation between poor
wellbeing and worse patient safety, with six additional studies finding an association with some but not all scales used, and one
study finding a significant association but in the opposite direction to the majority of studies. Twenty-one out of the 30 studies that
measured burnout found a significant association between burnout and patient safety, whilst a further four studies found an
association between one or more (but not all) subscales of the burnout measures employed, and patient safety.
Conclusions
Poor wellbeing and moderate to high levels of burnout are associated, in the majority of studies reviewed, with poor patient safety
outcomes such as medical errors, however the lack of prospective studies reduces the ability to determine causality. Further
prospective studies, research in primary care, conducted within the UK, and a clearer definition of healthcare staff wellbeing are
needed.
Implications
This review illustrates the need for healthcare organisations to consider improving employees’ mental health as well as creating
safer work environments when planning interventions to improve patient safety.
Systematic Review Registration
PROSPERO registration number: CRD42015023340.
Citation: Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB (2016) Healthcare Staff Wellbeing, Burnout, and Patient Safety: A
Systematic Review. PLoS ONE 11(7): e0159015. https://doi.org/10.1371/journal.pone.0159015
Editor: Fiona Harris, University of Stirling, UNITED KINGDOM
Received: March 18, 2016; Accepted: June 24, 2016; Published: July 8, 2016
Copyright: © 2016 Hall et al. This is an open access article distributed under the terms of the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and
source are credited.
Data Availability: All relevant data are within the paper and the Supporting Information files.
Published: July 8, 2016 https://doi.org/10.1371/journal.pone.0159015
Healthcare Sta Wellbeing, Burnout, and Patient Safety: A
Systematic Review
Louise H. Hall , Judith Johnson, Ian Watt, Anastasia Tsipa, Daryl B. O’Connor
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 2/10
Funding: This research was undertaken as part of a PhD funded by the University of Leeds, UK (www.leeds.ac.uk), and
National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care
(CLAHRCs) under the Evidence Based Transformation Theme (www.clahrcpp.co.uk).
Competing interests: The authors have declared that no competing interests exist.
Introduction
Research suggests that 16.6% of all hospital inpatient episodes in Australia and 3.7% in America lead to harmful adverse events,
and in primary care, 1 in 20 prescriptions contain an error[1, 2]. In total, errors are estimated to cost the NHS £1.3 billion in litigation
costs, and £2 billion in additional bed days annually[1]. Alarmingly, these statistics are likely to be an underestimate due to the
complexity of trying to capture errors and adverse events within such settings.
Many factors, latent and active, system and individual, interact to cause patient safety incidents. Human factors are important
contributors, and recent research indicates an important role for staff wellbeing[3–5]. Wellbeing can be conceptualised as a
spectrum, with flourishing, happiness and high wellbeing at one end, and elevated depression, anxiety and low wellbeing at the
other[6]. Example measures for wellbeing include the Hospital Depression and Anxiety Scale[7], the General Health
Questionnaire[8], stress measures such as the Perceived Stress Scale[9], and the Positive and Negative Affect Schedule[10].
Burnout, a conceptually different variable from wellbeing, also has implications for patient safety. The burnout concept was
originally developed amongst healthcare staff and is a ‘state of vital exhaustion’[11] in response to chronic organisational stress,
which results in feelings of work-related exhaustion (Emotional Exhaustion; EE), depersonalisation (DP), and reduced personal
accomplishment (PA)[12]. Although both wellbeing and burnout may be linked with patient safety, the current literature suffers from
three limitations. First, the results of studies investigating the association between wellbeing or burnout and patient safety have
been equivocal. Whilst several studies have reported an association, this finding has not always been replicated[3, 13–17]. Second,
burnout has often been treated as a proxy measure for wellbeing, but the determinants, symptoms and consequences of burnout
and wellbeing are distinct, and it is unclear which is more reliably associated with patient safety [18]. Third, the mechanisms
underlying the association between these variables and patient safety are unclear.
Research on these associations is imperative now more than ever, due to pressures upon healthcare service budgets causing
growing concerns around working conditions and the wellbeing of healthcare staff. In the UK, the financial pressures on the NHS
are impacting staffing levels, causing unmanageable workloads and subsequently impacting doctors’ morale and stress levels[19–
21]. Similar pressures are evident in health systems elsewhere, for example, in the US, there is growing concern over a caregiver
shortage occurring, due to population increases, chronic disease growth, and increased life expectancies[22]. In light of this, we
conducted a systematic review to investigate the extent to which wellbeing and burnout are associated with patient safety.
Aims and Objectives
The overarching aim of the review was to synthesize existing research investigating the association between wellbeing and/or
burnout in healthcare professionals with the safety of patient care. The review had three specific aims:
1. To explore the association between wellbeing in health care professionals and patient safety.
2. To explore the association between burnout in health care professionals and patient safety.
3. To explore the studies that measure both wellbeing and burnout in relation to patient safety.
Method
The protocol for this systematic review was registered in advance on PROSPERO, in which the inclusion criteria and methods of
analysis were specified: registration number: CRD42015023340. The protocol can be accessed here:
http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015023340. This review has not been subject to meta-
analysis due to the heterogeneity of the measures. This review was conducted in line with the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) guidelines[23], see S1 File.
Search strategy
Four electronic bibliographic databases were last searched on the 20/07/2015, see Table 1, along with reference searching of all
eligible articles. Authors of inaccessible articles were contacted to attain full texts. Both MeSH terms and keyword terms were used
in a multi-field search, based on terms commonly used within systematic reviews in the fields of patient safety, and wellbeing and
burnout.
Table 1. Electronic databases searched and number of results.
https://doi.org/10.1371/journal.pone.0159015.t001
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 2/10
Funding: This research was undertaken as part of a PhD funded by the University of Leeds, UK (www.leeds.ac.uk), and
National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Health Research and Care
(CLAHRCs) under the Evidence Based Transformation Theme (www.clahrcpp.co.uk).
Competing interests: The authors have declared that no competing interests exist.
Introduction
Research suggests that 16.6% of all hospital inpatient episodes in Australia and 3.7% in America lead to harmful adverse events,
and in primary care, 1 in 20 prescriptions contain an error[1, 2]. In total, errors are estimated to cost the NHS £1.3 billion in litigation
costs, and £2 billion in additional bed days annually[1]. Alarmingly, these statistics are likely to be an underestimate due to the
complexity of trying to capture errors and adverse events within such settings.
Many factors, latent and active, system and individual, interact to cause patient safety incidents. Human factors are important
contributors, and recent research indicates an important role for staff wellbeing[3–5]. Wellbeing can be conceptualised as a
spectrum, with flourishing, happiness and high wellbeing at one end, and elevated depression, anxiety and low wellbeing at the
other[6]. Example measures for wellbeing include the Hospital Depression and Anxiety Scale[7], the General Health
Questionnaire[8], stress measures such as the Perceived Stress Scale[9], and the Positive and Negative Affect Schedule[10].
Burnout, a conceptually different variable from wellbeing, also has implications for patient safety. The burnout concept was
originally developed amongst healthcare staff and is a ‘state of vital exhaustion’[11] in response to chronic organisational stress,
which results in feelings of work-related exhaustion (Emotional Exhaustion; EE), depersonalisation (DP), and reduced personal
accomplishment (PA)[12]. Although both wellbeing and burnout may be linked with patient safety, the current literature suffers from
three limitations. First, the results of studies investigating the association between wellbeing or burnout and patient safety have
been equivocal. Whilst several studies have reported an association, this finding has not always been replicated[3, 13–17]. Second,
burnout has often been treated as a proxy measure for wellbeing, but the determinants, symptoms and consequences of burnout
and wellbeing are distinct, and it is unclear which is more reliably associated with patient safety [18]. Third, the mechanisms
underlying the association between these variables and patient safety are unclear.
Research on these associations is imperative now more than ever, due to pressures upon healthcare service budgets causing
growing concerns around working conditions and the wellbeing of healthcare staff. In the UK, the financial pressures on the NHS
are impacting staffing levels, causing unmanageable workloads and subsequently impacting doctors’ morale and stress levels[19–
21]. Similar pressures are evident in health systems elsewhere, for example, in the US, there is growing concern over a caregiver
shortage occurring, due to population increases, chronic disease growth, and increased life expectancies[22]. In light of this, we
conducted a systematic review to investigate the extent to which wellbeing and burnout are associated with patient safety.
Aims and Objectives
The overarching aim of the review was to synthesize existing research investigating the association between wellbeing and/or
burnout in healthcare professionals with the safety of patient care. The review had three specific aims:
1. To explore the association between wellbeing in health care professionals and patient safety.
2. To explore the association between burnout in health care professionals and patient safety.
3. To explore the studies that measure both wellbeing and burnout in relation to patient safety.
Method
The protocol for this systematic review was registered in advance on PROSPERO, in which the inclusion criteria and methods of
analysis were specified: registration number: CRD42015023340. The protocol can be accessed here:
http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015023340. This review has not been subject to meta-
analysis due to the heterogeneity of the measures. This review was conducted in line with the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses (PRISMA) guidelines[23], see S1 File.
Search strategy
Four electronic bibliographic databases were last searched on the 20/07/2015, see Table 1, along with reference searching of all
eligible articles. Authors of inaccessible articles were contacted to attain full texts. Both MeSH terms and keyword terms were used
in a multi-field search, based on terms commonly used within systematic reviews in the fields of patient safety, and wellbeing and
burnout.
Table 1. Electronic databases searched and number of results.
https://doi.org/10.1371/journal.pone.0159015.t001
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 3/10
Papers were searched for those containing at least one term from each of the following blocks (although MeSH terms varied slightly
between databases): (health personnel) AND (well?being OR occupation* stress* OR burnout OR mental health OR “quality of life”)
AND (medical error OR patient safety OR quality of care OR error?). For an example of full search terms used for one of the
databases, see S2 File.
Study selection
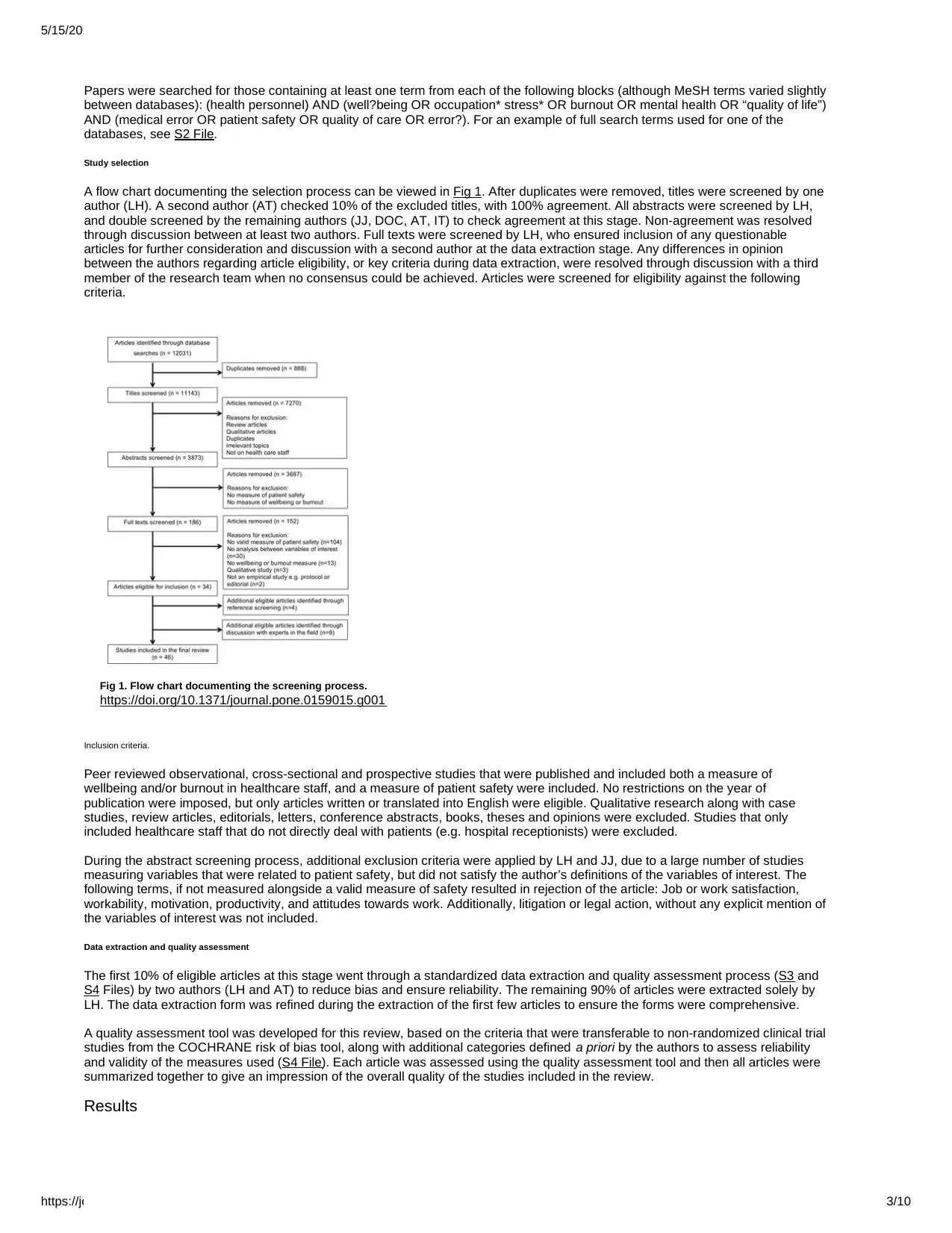
A flow chart documenting the selection process can be viewed in Fig 1. After duplicates were removed, titles were screened by one
author (LH). A second author (AT) checked 10% of the excluded titles, with 100% agreement. All abstracts were screened by LH,
and double screened by the remaining authors (JJ, DOC, AT, IT) to check agreement at this stage. Non-agreement was resolved
through discussion between at least two authors. Full texts were screened by LH, who ensured inclusion of any questionable
articles for further consideration and discussion with a second author at the data extraction stage. Any differences in opinion
between the authors regarding article eligibility, or key criteria during data extraction, were resolved through discussion with a third
member of the research team when no consensus could be achieved. Articles were screened for eligibility against the following
criteria.
Fig 1. Flow chart documenting the screening process.
https://doi.org/10.1371/journal.pone.0159015.g001
Inclusion criteria.
Peer reviewed observational, cross-sectional and prospective studies that were published and included both a measure of
wellbeing and/or burnout in healthcare staff, and a measure of patient safety were included. No restrictions on the year of
publication were imposed, but only articles written or translated into English were eligible. Qualitative research along with case
studies, review articles, editorials, letters, conference abstracts, books, theses and opinions were excluded. Studies that only
included healthcare staff that do not directly deal with patients (e.g. hospital receptionists) were excluded.
During the abstract screening process, additional exclusion criteria were applied by LH and JJ, due to a large number of studies
measuring variables that were related to patient safety, but did not satisfy the author’s definitions of the variables of interest. The
following terms, if not measured alongside a valid measure of safety resulted in rejection of the article: Job or work satisfaction,
workability, motivation, productivity, and attitudes towards work. Additionally, litigation or legal action, without any explicit mention of
the variables of interest was not included.
Data extraction and quality assessment
The first 10% of eligible articles at this stage went through a standardized data extraction and quality assessment process (S3 and
S4 Files) by two authors (LH and AT) to reduce bias and ensure reliability. The remaining 90% of articles were extracted solely by
LH. The data extraction form was refined during the extraction of the first few articles to ensure the forms were comprehensive.
A quality assessment tool was developed for this review, based on the criteria that were transferable to non-randomized clinical trial
studies from the COCHRANE risk of bias tool, along with additional categories defined a priori by the authors to assess reliability
and validity of the measures used (S4 File). Each article was assessed using the quality assessment tool and then all articles were
summarized together to give an impression of the overall quality of the studies included in the review.
Results
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 3/10
Papers were searched for those containing at least one term from each of the following blocks (although MeSH terms varied slightly
between databases): (health personnel) AND (well?being OR occupation* stress* OR burnout OR mental health OR “quality of life”)
AND (medical error OR patient safety OR quality of care OR error?). For an example of full search terms used for one of the
databases, see S2 File.
Study selection
A flow chart documenting the selection process can be viewed in Fig 1. After duplicates were removed, titles were screened by one
author (LH). A second author (AT) checked 10% of the excluded titles, with 100% agreement. All abstracts were screened by LH,
and double screened by the remaining authors (JJ, DOC, AT, IT) to check agreement at this stage. Non-agreement was resolved
through discussion between at least two authors. Full texts were screened by LH, who ensured inclusion of any questionable
articles for further consideration and discussion with a second author at the data extraction stage. Any differences in opinion
between the authors regarding article eligibility, or key criteria during data extraction, were resolved through discussion with a third
member of the research team when no consensus could be achieved. Articles were screened for eligibility against the following
criteria.
Fig 1. Flow chart documenting the screening process.
https://doi.org/10.1371/journal.pone.0159015.g001
Inclusion criteria.
Peer reviewed observational, cross-sectional and prospective studies that were published and included both a measure of
wellbeing and/or burnout in healthcare staff, and a measure of patient safety were included. No restrictions on the year of
publication were imposed, but only articles written or translated into English were eligible. Qualitative research along with case
studies, review articles, editorials, letters, conference abstracts, books, theses and opinions were excluded. Studies that only
included healthcare staff that do not directly deal with patients (e.g. hospital receptionists) were excluded.
During the abstract screening process, additional exclusion criteria were applied by LH and JJ, due to a large number of studies
measuring variables that were related to patient safety, but did not satisfy the author’s definitions of the variables of interest. The
following terms, if not measured alongside a valid measure of safety resulted in rejection of the article: Job or work satisfaction,
workability, motivation, productivity, and attitudes towards work. Additionally, litigation or legal action, without any explicit mention of
the variables of interest was not included.
Data extraction and quality assessment
The first 10% of eligible articles at this stage went through a standardized data extraction and quality assessment process (S3 and
S4 Files) by two authors (LH and AT) to reduce bias and ensure reliability. The remaining 90% of articles were extracted solely by
LH. The data extraction form was refined during the extraction of the first few articles to ensure the forms were comprehensive.
A quality assessment tool was developed for this review, based on the criteria that were transferable to non-randomized clinical trial
studies from the COCHRANE risk of bias tool, along with additional categories defined a priori by the authors to assess reliability
and validity of the measures used (S4 File). Each article was assessed using the quality assessment tool and then all articles were
summarized together to give an impression of the overall quality of the studies included in the review.
Results
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 4/10
Forty-six studies were deemed eligible for inclusion in this review, and they were subsequently grouped based on whether they
measured wellbeing or burnout, or both.
Descriptive statistics and study characteristics
Nineteen studies measured burnout, sixteen measured wellbeing, and the remaining eleven included both a measure of burnout
and of wellbeing. Of the burnout studies, the vast majority of studies (n = 24) used some variant of the Maslach Burnout Inventory
(MBI) [24], such as the MBI-Human Services Survey, the EE scale of the MBI, or an international variation of the MBI. Alternative
measures were; Shirom-Melamed’s Burnout Scale, Copenhagen Burnout Inventory (CBI), Physician Well-Being Index, a single
question approach and a symptom-based stress survey. The wellbeing measures were far more varied and included; General
Health Questionnaire (GHQ), Harvard National Depression Screening Day Scale (HANDS), linear stress scales, Quality of Life
scales, and emotional distress, among others. For a full list of measures and other study characteristics, see S1 Table. Most of the
measures used were pre-existing, validated and reliable measures.
The most common approach to measuring patient safety was to use a question on the frequency of self-perceived errors over a
particular time frame, ranging from the previous four weeks to the past year. Other subjective and self reported measures included
stating the health professional’s accident propensity (from ‘not at all’ to ‘very likely’) and their perceived likelihood of making errors.
One study used a hand held computer device to gather medication events in real time[25]. Six studies included objective measures
of error, using chart audits, checking official error reports, and conducting observations of staff[5, 16, 26–29]. Fahrenkopf and
colleagues[28], and Garrouste-Orgeas and colleagues[29] were the only studies to use both objective and subjective measures of
error. Although Welp and colleagues[30] measured mortality rates and length of stay alongside a subjective measure of patient
safety, these objective measures were not within our criteria for patient safety outcomes.
The studies were conducted across 16 different countries and six continents, with a large proportion being based in America ( n =
19). Most (n = 33) utilised a cross-sectional survey design, with only nine using a prospective cohort study methodology. The most
commonly studied profession was nurses (n = 24 studies), followed by physicians (n = 7). The remaining study samples consisted
of pharmacists (n = 2), a variety of hospital staff (n = 2), paramedics (n = 1), surgeons (n = 2), anaesthetists (n = 1) and doctors still
in some form of training (n = 8). Only one study included primary care physicians, and they were grouped in with the hospital based
staff in all the analyses.
Wellbeing findings
Of the articles measuring wellbeing, over half (16/27, 59.3%) found that poor wellbeing, as measured using a variety of definitions
(depression, anxiety, job stress, mental health, distress), was associated with poorer patient safety [3–5, 17, 25, 29, 31–40]. An
additional six studies (22.2%) found some sort of relationship between wellbeing and patient safety, but with only some subscales
of the wellbeing measures or safety measures correlating[27, 28, 41–44]. Tanaka and colleagues’ prospective cohort study in
Japan[4] found that higher depression scores were significantly associated with more near misses, but not with adverse events, as
measured through frequency of self-perceived error in the previous 6 months. Of note is that both Houston and Allt’s study[41], and
Niven and Ciborowska’s study[42] found that anxiety, but not depression, was significantly associated with errors, despite using
different measures of anxiety, depression and errors from each other.
Five studies found no correlation between wellbeing and patient safety [13, 16, 45–47]. However, one of these, Dorrian and
colleagues’ 2006 study[13], was only a pilot study, with a sample size of 23. Their full study in 2008, however, did find that stress
significantly predicted error, suggesting that the pilot study was underpowered.
Amongst the studies of wellbeing, Hammer and colleagues’ cross-sectional study of 374 paramedics in the United States (US)[40]
was distinctive in that it indicated an association between low stress and increased error. They reported that those with less somatic
distress and lower total stress scores (on the MPSS-R) made significantly more errors. This could perhaps be due to the measures
used, which differ from all the other studies. The stress measure was of organisational stress, and did not measure the participants’
own stress levels. The distress measure is also questionable, as although it taps into some concepts associated with poor
wellbeing, such as, “I wake up feeling tired”, others questions ask about behaviours that are not necessarily indicative of poor
mental health, e.g. “I drink on the weekend to relax”.
Burnout Findings
Similarly to the wellbeing studies, the majority of studies (21/30, 70%) measuring burnout found that more errors were significantly
associated with health practitioner burnout[3, 14, 26, 30, 31, 33, 35, 37, 38, 46, 48–58]. Four studies additionally found partial
associations between burnout and error[28, 59–61]. For example, Halbesleben and colleagues’[59] cross-sectional survey of
nurses in the US found that higher burnout was significantly associated with a lower patient safety grade and near miss reporting
frequency, but not with event report frequency. Klein and colleagues [60]found that burnout, as measured by the Copenhagen
Burnout Inventory, was only significantly associated with therapeutic (OR = 2.54) and diagnostic errors (OR = 1.94) in male, but not
in female surgeons in Germany.
Five studies did not find any significant associations between burnout and error [16, 27, 62–64]. Of these studies, only one of them
used a full set of MBI questions, although this was a translated version[29]. The remaining studies used a single-item measure, only
the EE subscale of the MBI, and a symptom-based stress survey, which although it had been previously used to measure burnout,
the authors describe it as a stress, and not a burnout survey in this context [27].
Studies measuring both burnout and wellbeing
Eleven studies measured both burnout and wellbeing in relation to patient safety outcomes[3, 16, 27–29, 31, 33, 35, 37, 38, 46]. It
is these studies that may facilitate a more intricate understanding of which variable is linked with the greater risk of error. Although
the majority (7/11) found that both poor wellbeing and risk of burnout were significantly associated with errors, all these studies, bar
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 4/10
Forty-six studies were deemed eligible for inclusion in this review, and they were subsequently grouped based on whether they
measured wellbeing or burnout, or both.
Descriptive statistics and study characteristics
Nineteen studies measured burnout, sixteen measured wellbeing, and the remaining eleven included both a measure of burnout
and of wellbeing. Of the burnout studies, the vast majority of studies (n = 24) used some variant of the Maslach Burnout Inventory
(MBI) [24], such as the MBI-Human Services Survey, the EE scale of the MBI, or an international variation of the MBI. Alternative
measures were; Shirom-Melamed’s Burnout Scale, Copenhagen Burnout Inventory (CBI), Physician Well-Being Index, a single
question approach and a symptom-based stress survey. The wellbeing measures were far more varied and included; General
Health Questionnaire (GHQ), Harvard National Depression Screening Day Scale (HANDS), linear stress scales, Quality of Life
scales, and emotional distress, among others. For a full list of measures and other study characteristics, see S1 Table. Most of the
measures used were pre-existing, validated and reliable measures.
The most common approach to measuring patient safety was to use a question on the frequency of self-perceived errors over a
particular time frame, ranging from the previous four weeks to the past year. Other subjective and self reported measures included
stating the health professional’s accident propensity (from ‘not at all’ to ‘very likely’) and their perceived likelihood of making errors.
One study used a hand held computer device to gather medication events in real time[25]. Six studies included objective measures
of error, using chart audits, checking official error reports, and conducting observations of staff[5, 16, 26–29]. Fahrenkopf and
colleagues[28], and Garrouste-Orgeas and colleagues[29] were the only studies to use both objective and subjective measures of
error. Although Welp and colleagues[30] measured mortality rates and length of stay alongside a subjective measure of patient
safety, these objective measures were not within our criteria for patient safety outcomes.
The studies were conducted across 16 different countries and six continents, with a large proportion being based in America ( n =
19). Most (n = 33) utilised a cross-sectional survey design, with only nine using a prospective cohort study methodology. The most
commonly studied profession was nurses (n = 24 studies), followed by physicians (n = 7). The remaining study samples consisted
of pharmacists (n = 2), a variety of hospital staff (n = 2), paramedics (n = 1), surgeons (n = 2), anaesthetists (n = 1) and doctors still
in some form of training (n = 8). Only one study included primary care physicians, and they were grouped in with the hospital based
staff in all the analyses.
Wellbeing findings
Of the articles measuring wellbeing, over half (16/27, 59.3%) found that poor wellbeing, as measured using a variety of definitions
(depression, anxiety, job stress, mental health, distress), was associated with poorer patient safety [3–5, 17, 25, 29, 31–40]. An
additional six studies (22.2%) found some sort of relationship between wellbeing and patient safety, but with only some subscales
of the wellbeing measures or safety measures correlating[27, 28, 41–44]. Tanaka and colleagues’ prospective cohort study in
Japan[4] found that higher depression scores were significantly associated with more near misses, but not with adverse events, as
measured through frequency of self-perceived error in the previous 6 months. Of note is that both Houston and Allt’s study[41], and
Niven and Ciborowska’s study[42] found that anxiety, but not depression, was significantly associated with errors, despite using
different measures of anxiety, depression and errors from each other.
Five studies found no correlation between wellbeing and patient safety [13, 16, 45–47]. However, one of these, Dorrian and
colleagues’ 2006 study[13], was only a pilot study, with a sample size of 23. Their full study in 2008, however, did find that stress
significantly predicted error, suggesting that the pilot study was underpowered.
Amongst the studies of wellbeing, Hammer and colleagues’ cross-sectional study of 374 paramedics in the United States (US)[40]
was distinctive in that it indicated an association between low stress and increased error. They reported that those with less somatic
distress and lower total stress scores (on the MPSS-R) made significantly more errors. This could perhaps be due to the measures
used, which differ from all the other studies. The stress measure was of organisational stress, and did not measure the participants’
own stress levels. The distress measure is also questionable, as although it taps into some concepts associated with poor
wellbeing, such as, “I wake up feeling tired”, others questions ask about behaviours that are not necessarily indicative of poor
mental health, e.g. “I drink on the weekend to relax”.
Burnout Findings
Similarly to the wellbeing studies, the majority of studies (21/30, 70%) measuring burnout found that more errors were significantly
associated with health practitioner burnout[3, 14, 26, 30, 31, 33, 35, 37, 38, 46, 48–58]. Four studies additionally found partial
associations between burnout and error[28, 59–61]. For example, Halbesleben and colleagues’[59] cross-sectional survey of
nurses in the US found that higher burnout was significantly associated with a lower patient safety grade and near miss reporting
frequency, but not with event report frequency. Klein and colleagues [60]found that burnout, as measured by the Copenhagen
Burnout Inventory, was only significantly associated with therapeutic (OR = 2.54) and diagnostic errors (OR = 1.94) in male, but not
in female surgeons in Germany.
Five studies did not find any significant associations between burnout and error [16, 27, 62–64]. Of these studies, only one of them
used a full set of MBI questions, although this was a translated version[29]. The remaining studies used a single-item measure, only
the EE subscale of the MBI, and a symptom-based stress survey, which although it had been previously used to measure burnout,
the authors describe it as a stress, and not a burnout survey in this context [27].
Studies measuring both burnout and wellbeing
Eleven studies measured both burnout and wellbeing in relation to patient safety outcomes[3, 16, 27–29, 31, 33, 35, 37, 38, 46]. It
is these studies that may facilitate a more intricate understanding of which variable is linked with the greater risk of error. Although
the majority (7/11) found that both poor wellbeing and risk of burnout were significantly associated with errors, all these studies, bar
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 5/10
one[28], used only self-perceived errors as the outcome indicator. All but one[46] of the remaining studies that found either no link
at all or only an association between either wellbeing or burnout with safety, were those that used objective measures of error,
suggesting that perhaps objective measures are not sensitive enough[16, 27, 29]. Linzer and colleagues[16] conducted chart audits
and found no associations between errors and wellbeing or burnout. Dugan and colleagues[27] checked hospital records for errors
and found that stress scores (stress continuum scale) but not a symptom-based stress survey (a possible burnout measure)
correlated with patient incidents. Finally, Garrouste-Orgeas and colleagues[29] found that in their prospective cohort study,
depression was an independent risk factor for error (as assessed by chart audit), but that burnout was not. The one study that used
both objective and subjective measures of error found that different measurement methods resulted in different findings for burnout
than for wellbeing[28]. In this study, depressed resident doctors made significantly more errors than those who were not depressed,
but only when using the objective, and not when using the subjective, measure of error. Additionally, they found that burnt-out
residents made more errors than non-burnt-out residents when using subjective self-reported, but not objective, measures of error.
Four studies [29, 31, 33, 37] conducted analyses that could determine whether burnout and poor wellbeing were each independent
predictors of error, or whether one explained the variance in the other. Garrouste-Orgeas and colleagues[29] concluded that
burnout was not directly associated with error, even when depression was controlled for in the analysis. Depression however, was
found to be an independent predictor of error. The three remaining studies [31, 33, 37] reported that both burnout and wellbeing
were independent predictors of error when multivariate analyses were conducted.
Study quality and risk of bias
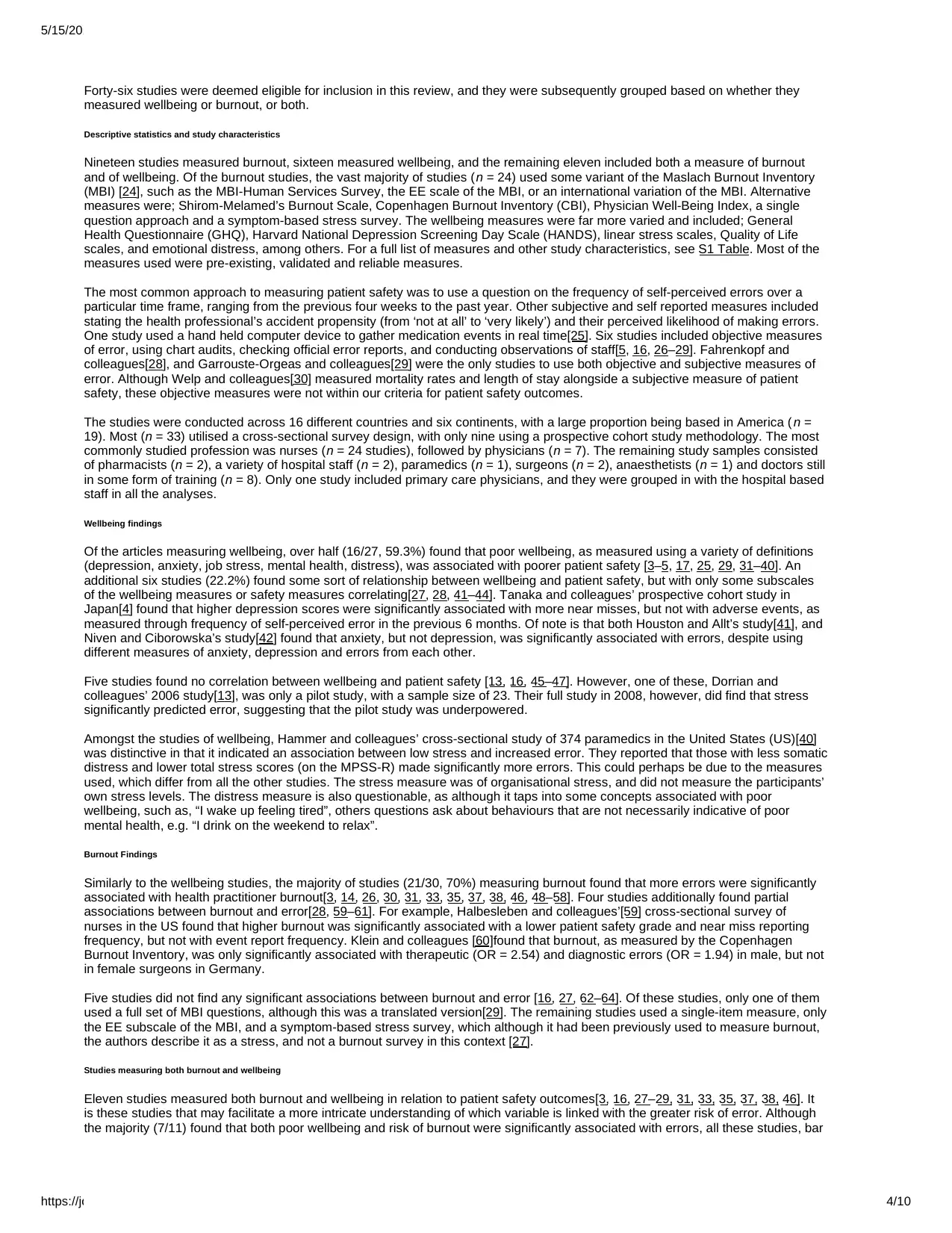
See Fig 2 for an overview of all the studies combined risks of bias, based on the format suggested by the COCHRANE guidelines.
For separate quality rating graphs for the wellbeing and burnout studies, see S5 File.
Fig 2. Risk of bias graph displaying the overall study quality for all 46 studies.
https://doi.org/10.1371/journal.pone.0159015.g002
A common concern amongst the studies with regards to quality was the measure of patient safety used, as the majority of studies
used solely self-reported measures of error, which has a number of limitations including social desirability and fear of blame and
retribution. This shall be discussed further in the following section.
There was not much variability in study quality/risk of bias between those that measured wellbeing and those that measured
burnout. The criteria in which the burnout studies generally displayed a lower risk of bias than the wellbeing studies were
representativeness (73.3% v. 44.4%), and measures of burnout/wellbeing (93.3% v. 77.7%), respectively. There were a similar
number of studies demonstrating a medium to large effect size for the relationship between patient safety and burnout as there
were for patient safety and wellbeing (33.3% v. 25.9%).
Discussion
The majority of studies provided evidence that both wellbeing and burnout are associated with patient safety. In particular, poor
wellbeing, as characterized by depression, anxiety, poor quality of life and stress, and high levels of burnout, were found to be
significantly associated with more self-reported errors, with a smaller number of studies showing an association of these factors
with objective measures of error. A similar percentage of studies found significant associations between wellbeing and error (88.9%
of studies) as those for burnout and error (83.3%), indicating the importance of both variables. Studies reporting that both burnout
and poor wellbeing were independently associated with poorer patient safety suggest the importance of both variables on their own
[31, 33, 37]. Indeed, one study[31] found that when resident doctors suffered from both high burnout and risk of depression, they
reported even more errors than those who suffered solely from burnout or depression alone. These studies signify that both staff
wellbeing and burnout may be important targets for patient safety interventions. However further research is needed first to properly
understand the nature of the relationships between these factors. Too few prospective studies have been conducted to definitively
propose a causal relationship. West and colleagues’ study[3] attempts to clarify this, with a circular relationship between burnout
and error being reported. However this circular relationship was not found for wellbeing and error, with errors significantly predicting
subsequent quality of life and depression ratings, but not vice versa. An explanatory model for how wellbeing and burnout are
associated is also needed, to enable the implementation of effective interventions. Fahrenkopf and colleagues’ study[28] found that
96% of depressed residents were also burnt-out, but only 25% of burnt-out residents were depressed, indicating that burnout may
be a possible precursor to depression. If the findings from these studies could be extrapolated into an overarching model, it could
be proposed that overworked staff become burnt-out, which may eventually lead to depression. Thus burnout and depression may
manifest itself through fatigue, irritability and reduced cognitive functioning[65], all of which puts pressure on team relationships
causing a poorer safety climate, and on their own individual work performance, resulting in more distanced staff, poorer quality of
care and ultimately a higher risk of making errors.
Limitations of the studies
This review is limited in its ability to determine the nature of the associations between wellbeing, burnout and patient safety, due to
the limitations of the studies included. The primary limitation was the measure of safety, which is a general problem within patient
safety research. The measures used often relied on self-reported errors with recall as long as a year ago, making the results
vulnerable to a variety of memory biases and cognitive failures. However despite these limitations, self-reported measures do
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 5/10
one[28], used only self-perceived errors as the outcome indicator. All but one[46] of the remaining studies that found either no link
at all or only an association between either wellbeing or burnout with safety, were those that used objective measures of error,
suggesting that perhaps objective measures are not sensitive enough[16, 27, 29]. Linzer and colleagues[16] conducted chart audits
and found no associations between errors and wellbeing or burnout. Dugan and colleagues[27] checked hospital records for errors
and found that stress scores (stress continuum scale) but not a symptom-based stress survey (a possible burnout measure)
correlated with patient incidents. Finally, Garrouste-Orgeas and colleagues[29] found that in their prospective cohort study,
depression was an independent risk factor for error (as assessed by chart audit), but that burnout was not. The one study that used
both objective and subjective measures of error found that different measurement methods resulted in different findings for burnout
than for wellbeing[28]. In this study, depressed resident doctors made significantly more errors than those who were not depressed,
but only when using the objective, and not when using the subjective, measure of error. Additionally, they found that burnt-out
residents made more errors than non-burnt-out residents when using subjective self-reported, but not objective, measures of error.
Four studies [29, 31, 33, 37] conducted analyses that could determine whether burnout and poor wellbeing were each independent
predictors of error, or whether one explained the variance in the other. Garrouste-Orgeas and colleagues[29] concluded that
burnout was not directly associated with error, even when depression was controlled for in the analysis. Depression however, was
found to be an independent predictor of error. The three remaining studies [31, 33, 37] reported that both burnout and wellbeing
were independent predictors of error when multivariate analyses were conducted.
Study quality and risk of bias
See Fig 2 for an overview of all the studies combined risks of bias, based on the format suggested by the COCHRANE guidelines.
For separate quality rating graphs for the wellbeing and burnout studies, see S5 File.
Fig 2. Risk of bias graph displaying the overall study quality for all 46 studies.
https://doi.org/10.1371/journal.pone.0159015.g002
A common concern amongst the studies with regards to quality was the measure of patient safety used, as the majority of studies
used solely self-reported measures of error, which has a number of limitations including social desirability and fear of blame and
retribution. This shall be discussed further in the following section.
There was not much variability in study quality/risk of bias between those that measured wellbeing and those that measured
burnout. The criteria in which the burnout studies generally displayed a lower risk of bias than the wellbeing studies were
representativeness (73.3% v. 44.4%), and measures of burnout/wellbeing (93.3% v. 77.7%), respectively. There were a similar
number of studies demonstrating a medium to large effect size for the relationship between patient safety and burnout as there
were for patient safety and wellbeing (33.3% v. 25.9%).
Discussion
The majority of studies provided evidence that both wellbeing and burnout are associated with patient safety. In particular, poor
wellbeing, as characterized by depression, anxiety, poor quality of life and stress, and high levels of burnout, were found to be
significantly associated with more self-reported errors, with a smaller number of studies showing an association of these factors
with objective measures of error. A similar percentage of studies found significant associations between wellbeing and error (88.9%
of studies) as those for burnout and error (83.3%), indicating the importance of both variables. Studies reporting that both burnout
and poor wellbeing were independently associated with poorer patient safety suggest the importance of both variables on their own
[31, 33, 37]. Indeed, one study[31] found that when resident doctors suffered from both high burnout and risk of depression, they
reported even more errors than those who suffered solely from burnout or depression alone. These studies signify that both staff
wellbeing and burnout may be important targets for patient safety interventions. However further research is needed first to properly
understand the nature of the relationships between these factors. Too few prospective studies have been conducted to definitively
propose a causal relationship. West and colleagues’ study[3] attempts to clarify this, with a circular relationship between burnout
and error being reported. However this circular relationship was not found for wellbeing and error, with errors significantly predicting
subsequent quality of life and depression ratings, but not vice versa. An explanatory model for how wellbeing and burnout are
associated is also needed, to enable the implementation of effective interventions. Fahrenkopf and colleagues’ study[28] found that
96% of depressed residents were also burnt-out, but only 25% of burnt-out residents were depressed, indicating that burnout may
be a possible precursor to depression. If the findings from these studies could be extrapolated into an overarching model, it could
be proposed that overworked staff become burnt-out, which may eventually lead to depression. Thus burnout and depression may
manifest itself through fatigue, irritability and reduced cognitive functioning[65], all of which puts pressure on team relationships
causing a poorer safety climate, and on their own individual work performance, resulting in more distanced staff, poorer quality of
care and ultimately a higher risk of making errors.
Limitations of the studies
This review is limited in its ability to determine the nature of the associations between wellbeing, burnout and patient safety, due to
the limitations of the studies included. The primary limitation was the measure of safety, which is a general problem within patient
safety research. The measures used often relied on self-reported errors with recall as long as a year ago, making the results
vulnerable to a variety of memory biases and cognitive failures. However despite these limitations, self-reported measures do
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 6/10
1.
2.
3.
View Article PubMed/NCBI Google Scholar
4.
provide a number of advantages over subjective measures; they are more sensitive, they can provide information across all types
of errors, and they can be measured at the individual level more easily than objective measures can. There is a lack of studies
measuring both objective and subjective measures of safety, with those that measured both differing in the type of errors measured
by the two different methods [28].
Limitations of this review, and further research
This review is restricted by its exclusion of non-English language papers. Additional limitations include the possibility of a
publication bias due to the exclusion of grey literature, and the inability to quantitatively determine whether wellbeing or burnout is
more strongly associated with patient safety due to the heterogeneity of the wellbeing and safety measures used. However, the
eligible studies were from a wide range of locations and included a variety of job roles (nurses, surgeons etc.). Future research is
needed to address these issues, and interventions need to be trialed at various points of the organisational, staff and patient levels
to determine where the most effective intervention for staff wellbeing and patient safety will fit.
Conclusion
The finding that burnout and poor wellbeing are both, in the majority of studies reviewed, associated with poorer patient safety has
significant implications for policymakers and management teams within healthcare settings. To deliver quality patient care, the care
must first and foremost be safe, and the findings from this review suggest that staff wellbeing may play an important role in patient
safety. It would seem prudent that healthcare organisations provide a work environment that fosters staff wellbeing and protects
against burnout, to subsequently provide a safe service to their patients.
Supporting Information
S1 Table. Summary table of results.
https://doi.org/10.1371/journal.pone.0159015.s001
(PDF)
S1 File. PRISMA checklist.
https://doi.org/10.1371/journal.pone.0159015.s002
(PDF)
S2 File. Search criteria for Medline (Ovid).
https://doi.org/10.1371/journal.pone.0159015.s003
(PDF)
S3 File. Data extraction template.
https://doi.org/10.1371/journal.pone.0159015.s004
(PDF)
S4 File. Quality assessment tool and scoring guide.
https://doi.org/10.1371/journal.pone.0159015.s005
(PDF)
S5 File. Quality assessment graphs grouped by wellbeing and burnout studies.
https://doi.org/10.1371/journal.pone.0159015.s006
(PDF)
Acknowledgments
This paper presents independent research by the National Institute for Health Research Collaboration for Leadership in Applied
Health Research and Care Yorkshire and Humber (NIHR CLAHRC YH). www.clahrc-yh.nir.ac.uk. The views and opinions
expressed are those of the authors, and not necessarily those of the NHS, the NIHR or the Department of Health.
Author Contributions
Conceived and designed the experiments: LHH JJ IW DBO. Performed the experiments: LHH JJ AT IW DBO. Analyzed the data:
LHH JJ IW DBO. Contributed reagents/materials/analysis tools: LHH JJ IW AT DBO. Wrote the paper: LHH JJ IW DBO.
References
Health Do. An Organisation with a Memory: Report of an Expert Group on Learning from Adverse Events in the NHS Chaired by the Chief Medical Officer:
The Stationery Office London; 2000.
Avery T, Barber N, Ghaleb M, Franklin BD, Armstrong S, Crowe S, et al. Investigating the prevalence and causes of prescribing errors in general practice.
London: The General Medical Council: PRACtICe Study. 2012.
West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, et al. Association of perceived medical errors with resident distress and
empathy: A prospective longitudinal study. Journal of the American Medical Association. 2006;296(9):1071–8. pmid:2006434742.
Tanaka M, Tanaka K, Takano T, Kato N, Watanabe M, Miyaoka H. Analysis of risk of medical errors using structural-equation modelling: A 6-month
prospective cohort study. BMJ Quality and Safety. 2012;21(9):784–90. pmid:2012558277.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 6/10
1.
2.
3.
View Article PubMed/NCBI Google Scholar
4.
provide a number of advantages over subjective measures; they are more sensitive, they can provide information across all types
of errors, and they can be measured at the individual level more easily than objective measures can. There is a lack of studies
measuring both objective and subjective measures of safety, with those that measured both differing in the type of errors measured
by the two different methods [28].
Limitations of this review, and further research
This review is restricted by its exclusion of non-English language papers. Additional limitations include the possibility of a
publication bias due to the exclusion of grey literature, and the inability to quantitatively determine whether wellbeing or burnout is
more strongly associated with patient safety due to the heterogeneity of the wellbeing and safety measures used. However, the
eligible studies were from a wide range of locations and included a variety of job roles (nurses, surgeons etc.). Future research is
needed to address these issues, and interventions need to be trialed at various points of the organisational, staff and patient levels
to determine where the most effective intervention for staff wellbeing and patient safety will fit.
Conclusion
The finding that burnout and poor wellbeing are both, in the majority of studies reviewed, associated with poorer patient safety has
significant implications for policymakers and management teams within healthcare settings. To deliver quality patient care, the care
must first and foremost be safe, and the findings from this review suggest that staff wellbeing may play an important role in patient
safety. It would seem prudent that healthcare organisations provide a work environment that fosters staff wellbeing and protects
against burnout, to subsequently provide a safe service to their patients.
Supporting Information
S1 Table. Summary table of results.
https://doi.org/10.1371/journal.pone.0159015.s001
(PDF)
S1 File. PRISMA checklist.
https://doi.org/10.1371/journal.pone.0159015.s002
(PDF)
S2 File. Search criteria for Medline (Ovid).
https://doi.org/10.1371/journal.pone.0159015.s003
(PDF)
S3 File. Data extraction template.
https://doi.org/10.1371/journal.pone.0159015.s004
(PDF)
S4 File. Quality assessment tool and scoring guide.
https://doi.org/10.1371/journal.pone.0159015.s005
(PDF)
S5 File. Quality assessment graphs grouped by wellbeing and burnout studies.
https://doi.org/10.1371/journal.pone.0159015.s006
(PDF)
Acknowledgments
This paper presents independent research by the National Institute for Health Research Collaboration for Leadership in Applied
Health Research and Care Yorkshire and Humber (NIHR CLAHRC YH). www.clahrc-yh.nir.ac.uk. The views and opinions
expressed are those of the authors, and not necessarily those of the NHS, the NIHR or the Department of Health.
Author Contributions
Conceived and designed the experiments: LHH JJ IW DBO. Performed the experiments: LHH JJ AT IW DBO. Analyzed the data:
LHH JJ IW DBO. Contributed reagents/materials/analysis tools: LHH JJ IW AT DBO. Wrote the paper: LHH JJ IW DBO.
References
Health Do. An Organisation with a Memory: Report of an Expert Group on Learning from Adverse Events in the NHS Chaired by the Chief Medical Officer:
The Stationery Office London; 2000.
Avery T, Barber N, Ghaleb M, Franklin BD, Armstrong S, Crowe S, et al. Investigating the prevalence and causes of prescribing errors in general practice.
London: The General Medical Council: PRACtICe Study. 2012.
West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, et al. Association of perceived medical errors with resident distress and
empathy: A prospective longitudinal study. Journal of the American Medical Association. 2006;296(9):1071–8. pmid:2006434742.
Tanaka M, Tanaka K, Takano T, Kato N, Watanabe M, Miyaoka H. Analysis of risk of medical errors using structural-equation modelling: A 6-month
prospective cohort study. BMJ Quality and Safety. 2012;21(9):784–90. pmid:2012558277.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 7/10
View Article PubMed/NCBI Google Scholar
5.
View Article PubMed/NCBI Google Scholar
6.
View Article Google Scholar
7.
View Article PubMed/NCBI Google Scholar
8.
View Article Google Scholar
9.
View Article PubMed/NCBI Google Scholar
10.
View Article PubMed/NCBI Google Scholar
11.
12.
View Article Google Scholar
13.
View Article PubMed/NCBI Google Scholar
14.
View Article PubMed/NCBI Google Scholar
15.
View Article Google Scholar
16.
View Article PubMed/NCBI Google Scholar
17.
View Article PubMed/NCBI Google Scholar
18.
19.
20.
View Article Google Scholar
21.
22.
23.
View Article PubMed/NCBI Google Scholar
24.
Saleh AM, Awadalla NJ, El-masri YM, Sleem WF. Impacts of nurses' circadian rhythm sleep disorders, fatigue, and depression on medication
administration errors. Egyptian Journal of Chest Diseases and Tuberculosis. 2014;63(1):145–53. pmid:2014074246.
Johnson J, Wood AM. Integrating Positive and Clinical Psychology: Viewing Human Functioning as Continua from Positive to Negative Can Benefit
Clinical Assessment, Interventions and Understandings of Resilience. Cognitive Therapy and Research. 2016:1–15.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta psychiatrica scandinavica. 1983;67(6):361–70. pmid:6880820
Goldberg DP, Hillier VF. A scaled version of the General Health Questionnaire. Psychological medicine. 1979;9(01):139–45.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of health and social behavior. 1983:385–96. pmid:6668417
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of personality
and social psychology. 1988;54(6):1063. pmid:3397865
Organization WH. International statistical classification of diseases and health related problems (The) ICD-10: World Health Organization; 2004.
Maslach C, Jackson SE. The measurement of experienced burnout. Journal of occupational behavior. 1981;2(2):99–113.
Dorrian J, Lamond N, Van Den Heuvel C, Pincombe J, Rogers AE, Dawson D. A pilot study of the safety implications of Australian nurses' sleep and work
hours. Chronobiology international. 2006;23(6):1149–63. pmid:17190702
Holden RJ, Patel NR, Scanlon MC, Shalaby TM, Arnold JM, Karsh B-T. Effects of mental demands during dispensing on perceived medication safety and
employee well-being: a study of workload in pediatric hospital pharmacies. Research in social and administrative Pharmacy. 2010;6(4):293–306.
pmid:21111387
Holden RJ, Scanlon MC, Patel NR, Kaushal R, Escoto KH, Brown RL, et al. A human factors framework and study of the effect of nursing workload on
patient safety and employee quality of working life. BMJ quality & safety. 2011;20(1):15–24.
Linzer M, Manwell LB, Williams ES, Bobula JA, Brown RL, Varkey AB, et al. Working conditions in primary care: physician reactions and care quality.
Annals of internal medicine. 2009;151(1):28–36. pmid:19581644
Suzuki K, Ohida T, Kaneita Y, Yokoyama E, Miyake T, Harano S, et al. Mental health status, shift work, and occupational accidents among hospital nurses
in Japan. Journal of occupational health. 2004;46(6):448–54. pmid:15613767
Schaufeli W, Enzmann D. The burnout companion to study and practice: A critical analysis: CRC press; 1998.
Raymond J. BMA quarterly tracker survey, April 2014. British Medical Association. April 2014.
Association BM. BMA quarterly tracker survey: Current views from across the medical profession. Quarter 2: April 2015. April 2015.
Gibson J, Checkland K, Coleman A, Hann M, McCall R, Spooner S, et al. Eight national GP worklife survey. 2015.
http://www.csc.com/health_services/insights/48705-u_s_healthcare_workforce_shortages_caregivers.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal
medicine. 2009;151(4):264–9. pmid:19622511
Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory manual. Mountain View, CA: CPP. Inc, and Davies-Black. 1996.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 7/10
View Article PubMed/NCBI Google Scholar
5.
View Article PubMed/NCBI Google Scholar
6.
View Article Google Scholar
7.
View Article PubMed/NCBI Google Scholar
8.
View Article Google Scholar
9.
View Article PubMed/NCBI Google Scholar
10.
View Article PubMed/NCBI Google Scholar
11.
12.
View Article Google Scholar
13.
View Article PubMed/NCBI Google Scholar
14.
View Article PubMed/NCBI Google Scholar
15.
View Article Google Scholar
16.
View Article PubMed/NCBI Google Scholar
17.
View Article PubMed/NCBI Google Scholar
18.
19.
20.
View Article Google Scholar
21.
22.
23.
View Article PubMed/NCBI Google Scholar
24.
Saleh AM, Awadalla NJ, El-masri YM, Sleem WF. Impacts of nurses' circadian rhythm sleep disorders, fatigue, and depression on medication
administration errors. Egyptian Journal of Chest Diseases and Tuberculosis. 2014;63(1):145–53. pmid:2014074246.
Johnson J, Wood AM. Integrating Positive and Clinical Psychology: Viewing Human Functioning as Continua from Positive to Negative Can Benefit
Clinical Assessment, Interventions and Understandings of Resilience. Cognitive Therapy and Research. 2016:1–15.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta psychiatrica scandinavica. 1983;67(6):361–70. pmid:6880820
Goldberg DP, Hillier VF. A scaled version of the General Health Questionnaire. Psychological medicine. 1979;9(01):139–45.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of health and social behavior. 1983:385–96. pmid:6668417
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of personality
and social psychology. 1988;54(6):1063. pmid:3397865
Organization WH. International statistical classification of diseases and health related problems (The) ICD-10: World Health Organization; 2004.
Maslach C, Jackson SE. The measurement of experienced burnout. Journal of occupational behavior. 1981;2(2):99–113.
Dorrian J, Lamond N, Van Den Heuvel C, Pincombe J, Rogers AE, Dawson D. A pilot study of the safety implications of Australian nurses' sleep and work
hours. Chronobiology international. 2006;23(6):1149–63. pmid:17190702
Holden RJ, Patel NR, Scanlon MC, Shalaby TM, Arnold JM, Karsh B-T. Effects of mental demands during dispensing on perceived medication safety and
employee well-being: a study of workload in pediatric hospital pharmacies. Research in social and administrative Pharmacy. 2010;6(4):293–306.
pmid:21111387
Holden RJ, Scanlon MC, Patel NR, Kaushal R, Escoto KH, Brown RL, et al. A human factors framework and study of the effect of nursing workload on
patient safety and employee quality of working life. BMJ quality & safety. 2011;20(1):15–24.
Linzer M, Manwell LB, Williams ES, Bobula JA, Brown RL, Varkey AB, et al. Working conditions in primary care: physician reactions and care quality.
Annals of internal medicine. 2009;151(1):28–36. pmid:19581644
Suzuki K, Ohida T, Kaneita Y, Yokoyama E, Miyake T, Harano S, et al. Mental health status, shift work, and occupational accidents among hospital nurses
in Japan. Journal of occupational health. 2004;46(6):448–54. pmid:15613767
Schaufeli W, Enzmann D. The burnout companion to study and practice: A critical analysis: CRC press; 1998.
Raymond J. BMA quarterly tracker survey, April 2014. British Medical Association. April 2014.
Association BM. BMA quarterly tracker survey: Current views from across the medical profession. Quarter 2: April 2015. April 2015.
Gibson J, Checkland K, Coleman A, Hann M, McCall R, Spooner S, et al. Eight national GP worklife survey. 2015.
http://www.csc.com/health_services/insights/48705-u_s_healthcare_workforce_shortages_caregivers.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal
medicine. 2009;151(4):264–9. pmid:19622511
Maslach C, Jackson SE, Leiter MP. Maslach burnout inventory manual. Mountain View, CA: CPP. Inc, and Davies-Black. 1996.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 8/10
25.
View Article PubMed/NCBI Google Scholar
26.
View Article PubMed/NCBI Google Scholar
27.
View Article PubMed/NCBI Google Scholar
28.
View Article PubMed/NCBI Google Scholar
29.
View Article PubMed/NCBI Google Scholar
30.
View Article PubMed/NCBI Google Scholar
31.
View Article Google Scholar
32.
View Article PubMed/NCBI Google Scholar
33.
View Article PubMed/NCBI Google Scholar
34.
View Article PubMed/NCBI Google Scholar
35.
36.
View Article PubMed/NCBI Google Scholar
37.
View Article PubMed/NCBI Google Scholar
38.
View Article PubMed/NCBI Google Scholar
39.
View Article PubMed/NCBI Google Scholar
40.
View Article PubMed/NCBI Google Scholar
41.
Dollarhide AW, Rutledge T, Weinger MB, Fisher ES, Jain S, Wolfson T, et al. A Real‐Time Assessment of Factors Influencing Medication Events. Journal
for Healthcare Quality. 2014;36(5):5–12. pmid:23551380
Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care–associated infection. American journal of infection control.
2012;40(6):486–90. pmid:22854376
Dugan J, Lauer E, Bouquot Z, Dutro BK, Smith M, Widmeyer G. Stressful nurses: the effect on patient outcomes. Journal of Nursing Care Quality.
1996;10(3):46–58. pmid:8634470
Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, et al. Rates of medication errors among depressed and burnt out residents:
prospective cohort study. Bmj. 2008;336(7642):488–91. pmid:18258931; PubMed Central PMCID: PMC2258399.
Garrouste-Orgeas M, Perrin M, Soufir L, Vesin A, Blot F, Maxime V, et al. The Iatroref study: medical errors are associated with symptoms of depression
in ICU staff but not burnout or safety culture. Intensive care medicine. 2015;41(2):273–84. pmid:25576157
Welp A, Meier LL, Manser T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Frontiers in psychology. 2015;5:1573.
pmid:25657627
de Oliveira GS Jr, Chang R, Fitzgerald PC, Almeida MD, Castro-Alves LS, Ahmad S, et al. The prevalence of burnout and depression and their
association with adherence to safety and practice standards: a survey of United States anesthesiology trainees. Anesthesia & Analgesia.
2013;117(1):182–93.
Dorrian J, Tolley C, Lamond N, van den Heuvel C, Pincombe J, Rogers AE, et al. Sleep and errors in a group of Australian hospital nurses at work and
during the commute. Applied ergonomics. 2008;39(5):605–13. pmid:18395183
Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in distress. Journal of general internal medicine.
2013;28(3):421–7. pmid:23129161
Fogarty GJ, McKeon C. Patient safety during medication administration: the influence of organizational and individual variables on unsafe work practices
and medication errors. Ergonomics. 2006;49(5–6):444–56. pmid:16717003
Hayashino Y, Utsugi-Ozaki M, Feldman MD, Fukuhara S. Hope modified the association between distress and incidence of self-perceived medical errors
among practicing physicians: prospective cohort study. 2012.
Pelliciotti JdSS, Kimura M. Medications errors and health-related quality of life of nursing professionals in intensive care units. Revista latino-americana de
enfermagem. 2010;18(6):1062–9. pmid:21340269
Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Annals of surgery.
2010;251(6):995–1000. pmid:19934755
West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress with perceived medical errors. Jama.
2009;302(12):1294–300. pmid:19773564
Arimura M, Imai M, Okawa M, Fujimura T, Yamada N. Sleep, mental health status, and medical errors among hospital nurses in Japan. Industrial health.
2010;48(6):811–7. pmid:20616466
Hammer JS, Mathews JJ, Lyons JS, Johnson NJ. Occupational stress within the paramedic profession: An initial report of stress levels compared to
hospital employees. Annals of emergency medicine. 1986;15(5):536–9. pmid:3963532
Houston DM, Allt SK. Psychological distress and error making among junior house officers. British Journal of Health Psychology. 1997;2(2):141–51.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 8/10
25.
View Article PubMed/NCBI Google Scholar
26.
View Article PubMed/NCBI Google Scholar
27.
View Article PubMed/NCBI Google Scholar
28.
View Article PubMed/NCBI Google Scholar
29.
View Article PubMed/NCBI Google Scholar
30.
View Article PubMed/NCBI Google Scholar
31.
View Article Google Scholar
32.
View Article PubMed/NCBI Google Scholar
33.
View Article PubMed/NCBI Google Scholar
34.
View Article PubMed/NCBI Google Scholar
35.
36.
View Article PubMed/NCBI Google Scholar
37.
View Article PubMed/NCBI Google Scholar
38.
View Article PubMed/NCBI Google Scholar
39.
View Article PubMed/NCBI Google Scholar
40.
View Article PubMed/NCBI Google Scholar
41.
Dollarhide AW, Rutledge T, Weinger MB, Fisher ES, Jain S, Wolfson T, et al. A Real‐Time Assessment of Factors Influencing Medication Events. Journal
for Healthcare Quality. 2014;36(5):5–12. pmid:23551380
Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care–associated infection. American journal of infection control.
2012;40(6):486–90. pmid:22854376
Dugan J, Lauer E, Bouquot Z, Dutro BK, Smith M, Widmeyer G. Stressful nurses: the effect on patient outcomes. Journal of Nursing Care Quality.
1996;10(3):46–58. pmid:8634470
Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, et al. Rates of medication errors among depressed and burnt out residents:
prospective cohort study. Bmj. 2008;336(7642):488–91. pmid:18258931; PubMed Central PMCID: PMC2258399.
Garrouste-Orgeas M, Perrin M, Soufir L, Vesin A, Blot F, Maxime V, et al. The Iatroref study: medical errors are associated with symptoms of depression
in ICU staff but not burnout or safety culture. Intensive care medicine. 2015;41(2):273–84. pmid:25576157
Welp A, Meier LL, Manser T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Frontiers in psychology. 2015;5:1573.
pmid:25657627
de Oliveira GS Jr, Chang R, Fitzgerald PC, Almeida MD, Castro-Alves LS, Ahmad S, et al. The prevalence of burnout and depression and their
association with adherence to safety and practice standards: a survey of United States anesthesiology trainees. Anesthesia & Analgesia.
2013;117(1):182–93.
Dorrian J, Tolley C, Lamond N, van den Heuvel C, Pincombe J, Rogers AE, et al. Sleep and errors in a group of Australian hospital nurses at work and
during the commute. Applied ergonomics. 2008;39(5):605–13. pmid:18395183
Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in distress. Journal of general internal medicine.
2013;28(3):421–7. pmid:23129161
Fogarty GJ, McKeon C. Patient safety during medication administration: the influence of organizational and individual variables on unsafe work practices
and medication errors. Ergonomics. 2006;49(5–6):444–56. pmid:16717003
Hayashino Y, Utsugi-Ozaki M, Feldman MD, Fukuhara S. Hope modified the association between distress and incidence of self-perceived medical errors
among practicing physicians: prospective cohort study. 2012.
Pelliciotti JdSS, Kimura M. Medications errors and health-related quality of life of nursing professionals in intensive care units. Revista latino-americana de
enfermagem. 2010;18(6):1062–9. pmid:21340269
Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, et al. Burnout and medical errors among American surgeons. Annals of surgery.
2010;251(6):995–1000. pmid:19934755
West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress with perceived medical errors. Jama.
2009;302(12):1294–300. pmid:19773564
Arimura M, Imai M, Okawa M, Fujimura T, Yamada N. Sleep, mental health status, and medical errors among hospital nurses in Japan. Industrial health.
2010;48(6):811–7. pmid:20616466
Hammer JS, Mathews JJ, Lyons JS, Johnson NJ. Occupational stress within the paramedic profession: An initial report of stress levels compared to
hospital employees. Annals of emergency medicine. 1986;15(5):536–9. pmid:3963532
Houston DM, Allt SK. Psychological distress and error making among junior house officers. British Journal of Health Psychology. 1997;2(2):141–51.
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 9/10
View Article Google Scholar
42.
View Article Google Scholar
43.
View Article PubMed/NCBI Google Scholar
44.
View Article PubMed/NCBI Google Scholar
45.
View Article Google Scholar
46.
View Article PubMed/NCBI Google Scholar
47.
View Article PubMed/NCBI Google Scholar
48.
View Article PubMed/NCBI Google Scholar
49.
View Article PubMed/NCBI Google Scholar
50.
View Article PubMed/NCBI Google Scholar
51.
View Article PubMed/NCBI Google Scholar
52.
View Article Google Scholar
53.
View Article Google Scholar
54.
View Article PubMed/NCBI Google Scholar
55.
View Article PubMed/NCBI Google Scholar
56.
View Article PubMed/NCBI Google Scholar
57.
View Article Google Scholar
Niven K, Ciborowska N. The hidden dangers of attending work while unwell: A survey study of presenteeism among pharmacists. International Journal of
Stress Management. 2015;22(2):207.
Park Y-M, Kim SY. Impacts of job stress and cognitive failure on patient safety incidents among hospital nurses. Safety and health at work. 2013;4(4):210–
5. pmid:24422177
Arakawa C, Kanoya Y, Sato C. Factors contributing to medical errors and incidents among hospital nurses-nurses' health, quality of life, and workplace
predict medical errors and incidents. Industrial health. 2011;49(3):381–8. pmid:21372434
Baldwin P, Dodd M, Wrate R. Young doctors' health—I. How do working conditions affect attitudes, health and performance? Social science & medicine.
1997;45(1):35–40.
Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Annals of internal
medicine. 2002;136(5):358–67. pmid:11874308
Wilkins K, Shields M. Correlates of medication error in hospitals. Health reports. 2008;19(2):7. pmid:18642515
Bao Y, Vedina R, Moodie S, Dolan S. The relationship between value incongruence and individual and organizational well‐being outcomes: an exploratory
study among Catalan nurses. Journal of advanced nursing. 2013;69(3):631–41. pmid:22632178
Block L, Wu AW, Feldman L, Yeh H-C, Desai SV. Residency schedule, burnout and patient care among first-year residents. Postgraduate medical journal.
2013;89(1055):495–500. pmid:23852828
Chen K-Y, Yang C-M, Lien C-H, Chiou H-Y, Lin M-R, Chang H-R, et al. Burnout, job satisfaction, and medical malpractice among physicians. International
journal of medical sciences. 2013;10(11):1471. pmid:24046520
Laschinger HKS, Leiter MP. The impact of nursing work environments on patient safety outcomes: The mediating role of burnout engagement. Journal of
Nursing Administration. 2006;36(5):259–67. pmid:16705307
Prins J, Van Der Heijden F, Hoekstra-Weebers J, Bakker A, Van de Wiel H, Jacobs B, et al. Burnout, engagement and resident physicians' self-reported
errors. Psychology, health & medicine. 2009;14(6):654–66.
Profit J, Sharek PJ, Amspoker AB, Kowalkowski MA, Nisbet CC, Thomas EJ, et al. Burnout in the NICU setting and its relation to safety culture. BMJ
quality & safety. 2014;23(10):806–13.
Teng C-I, Shyu Y-IL, Chiou W-K, Fan H-C, Lam SM. Interactive effects of nurse-experienced time pressure and burnout on patient safety: a cross-
sectional survey. International Journal of Nursing Studies. 2010;47(11):1442–50. pmid:20472237
Williams ES, Manwell LB, Konrad TR, Linzer M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error
and suboptimal patient care: results from the MEMO study. Health care management review. 2007;32(3):203–12. pmid:17666991
Zander B, Dobler L, Busse R. The introduction of DRG funding and hospital nurses’ changing perceptions of their practice environment, quality of care
and satisfaction: comparison of cross-sectional surveys over a 10-year period. International journal of nursing studies. 2013;50(2):219–29. pmid:22846589
Ramanujam R, Abrahamson K, Anderson JG. Influence of workplace demands on nurses' perception of patient safety. Nursing & Health Sciences.
2008;10(2):144–50.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 9/10
View Article Google Scholar
42.
View Article Google Scholar
43.
View Article PubMed/NCBI Google Scholar
44.
View Article PubMed/NCBI Google Scholar
45.
View Article Google Scholar
46.
View Article PubMed/NCBI Google Scholar
47.
View Article PubMed/NCBI Google Scholar
48.
View Article PubMed/NCBI Google Scholar
49.
View Article PubMed/NCBI Google Scholar
50.
View Article PubMed/NCBI Google Scholar
51.
View Article PubMed/NCBI Google Scholar
52.
View Article Google Scholar
53.
View Article Google Scholar
54.
View Article PubMed/NCBI Google Scholar
55.
View Article PubMed/NCBI Google Scholar
56.
View Article PubMed/NCBI Google Scholar
57.
View Article Google Scholar
Niven K, Ciborowska N. The hidden dangers of attending work while unwell: A survey study of presenteeism among pharmacists. International Journal of
Stress Management. 2015;22(2):207.
Park Y-M, Kim SY. Impacts of job stress and cognitive failure on patient safety incidents among hospital nurses. Safety and health at work. 2013;4(4):210–
5. pmid:24422177
Arakawa C, Kanoya Y, Sato C. Factors contributing to medical errors and incidents among hospital nurses-nurses' health, quality of life, and workplace
predict medical errors and incidents. Industrial health. 2011;49(3):381–8. pmid:21372434
Baldwin P, Dodd M, Wrate R. Young doctors' health—I. How do working conditions affect attitudes, health and performance? Social science & medicine.
1997;45(1):35–40.
Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Annals of internal
medicine. 2002;136(5):358–67. pmid:11874308
Wilkins K, Shields M. Correlates of medication error in hospitals. Health reports. 2008;19(2):7. pmid:18642515
Bao Y, Vedina R, Moodie S, Dolan S. The relationship between value incongruence and individual and organizational well‐being outcomes: an exploratory
study among Catalan nurses. Journal of advanced nursing. 2013;69(3):631–41. pmid:22632178
Block L, Wu AW, Feldman L, Yeh H-C, Desai SV. Residency schedule, burnout and patient care among first-year residents. Postgraduate medical journal.
2013;89(1055):495–500. pmid:23852828
Chen K-Y, Yang C-M, Lien C-H, Chiou H-Y, Lin M-R, Chang H-R, et al. Burnout, job satisfaction, and medical malpractice among physicians. International
journal of medical sciences. 2013;10(11):1471. pmid:24046520
Laschinger HKS, Leiter MP. The impact of nursing work environments on patient safety outcomes: The mediating role of burnout engagement. Journal of
Nursing Administration. 2006;36(5):259–67. pmid:16705307
Prins J, Van Der Heijden F, Hoekstra-Weebers J, Bakker A, Van de Wiel H, Jacobs B, et al. Burnout, engagement and resident physicians' self-reported
errors. Psychology, health & medicine. 2009;14(6):654–66.
Profit J, Sharek PJ, Amspoker AB, Kowalkowski MA, Nisbet CC, Thomas EJ, et al. Burnout in the NICU setting and its relation to safety culture. BMJ
quality & safety. 2014;23(10):806–13.
Teng C-I, Shyu Y-IL, Chiou W-K, Fan H-C, Lam SM. Interactive effects of nurse-experienced time pressure and burnout on patient safety: a cross-
sectional survey. International Journal of Nursing Studies. 2010;47(11):1442–50. pmid:20472237
Williams ES, Manwell LB, Konrad TR, Linzer M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error
and suboptimal patient care: results from the MEMO study. Health care management review. 2007;32(3):203–12. pmid:17666991
Zander B, Dobler L, Busse R. The introduction of DRG funding and hospital nurses’ changing perceptions of their practice environment, quality of care
and satisfaction: comparison of cross-sectional surveys over a 10-year period. International journal of nursing studies. 2013;50(2):219–29. pmid:22846589
Ramanujam R, Abrahamson K, Anderson JG. Influence of workplace demands on nurses' perception of patient safety. Nursing & Health Sciences.
2008;10(2):144–50.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
5/15/2019 Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 10/10
58.
View Article PubMed/NCBI Google Scholar
59.
View Article PubMed/NCBI Google Scholar
60.
View Article PubMed/NCBI Google Scholar
61.
View Article PubMed/NCBI Google Scholar
62.
View Article PubMed/NCBI Google Scholar
63.
View Article PubMed/NCBI Google Scholar
64.
View Article PubMed/NCBI Google Scholar
65.
View Article Google Scholar
Squires M, Tourangeau A, SPENCE LASCHINGER HK, Doran D. The link between leadership and safety outcomes in hospitals. Journal of Nursing
Management. 2010;18(8):914–25. pmid:21073565
Halbesleben JR, Wakefield BJ, Wakefield DS, Cooper LB. Nurse burnout and patient safety outcomes nurse safety perception versus reporting behavior.
Western Journal of Nursing Research. 2008;30(5):560–77. pmid:18187408
Klein J, Frie KG, Blum K, von dem Knesebeck O. Burnout and perceived quality of care among German clinicians in surgery. International Journal for
Quality in Health Care. 2010;22(6):525–30. pmid:20935011
Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: Impact of unit-level nurse practice
environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events—A cross-sectional
survey. International journal of nursing studies. 2014;51(8):1123–34. pmid:24444772
Holden RJ, Scanlon MC, Patel NR, Kaushal R, Escoto KH, Brown RL, et al. A human factors framework and study of the effect of nursing workload on
patient safety and employee quality of working life. BMJ Quality and Safety. 2011;20(1):15–24. pmid:2011316479.
Garrouste-Orgeas M, Perrin M, Soufir L, Vesin A, Blot F, Maxime V, et al. The Iatroref study: medical errors are associated with symptoms of depression
in ICU staff but not burnout or safety culture. Intensive Care Medicine. 2015;41(2):273–84. pmid:2015719476.
Kirwan M, Matthews A, Scott PA. The impact of the work environment of nurses on patient safety outcomes: a multi-level modelling approach.
International journal of nursing studies. 2013;50(2):253–63. pmid:23116681
Linden DVD, Keijsers GP, Eling P, Schaijk RV. Work stress and attentional difficulties: An initial study on burnout and cognitive failures. Work & Stress.
2005;19(1):23–36.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0159015 10/10
58.
View Article PubMed/NCBI Google Scholar
59.
View Article PubMed/NCBI Google Scholar
60.
View Article PubMed/NCBI Google Scholar
61.
View Article PubMed/NCBI Google Scholar
62.
View Article PubMed/NCBI Google Scholar
63.
View Article PubMed/NCBI Google Scholar
64.
View Article PubMed/NCBI Google Scholar
65.
View Article Google Scholar
Squires M, Tourangeau A, SPENCE LASCHINGER HK, Doran D. The link between leadership and safety outcomes in hospitals. Journal of Nursing
Management. 2010;18(8):914–25. pmid:21073565
Halbesleben JR, Wakefield BJ, Wakefield DS, Cooper LB. Nurse burnout and patient safety outcomes nurse safety perception versus reporting behavior.
Western Journal of Nursing Research. 2008;30(5):560–77. pmid:18187408
Klein J, Frie KG, Blum K, von dem Knesebeck O. Burnout and perceived quality of care among German clinicians in surgery. International Journal for
Quality in Health Care. 2010;22(6):525–30. pmid:20935011
Van Bogaert P, Timmermans O, Weeks SM, van Heusden D, Wouters K, Franck E. Nursing unit teams matter: Impact of unit-level nurse practice
environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events—A cross-sectional
survey. International journal of nursing studies. 2014;51(8):1123–34. pmid:24444772
Holden RJ, Scanlon MC, Patel NR, Kaushal R, Escoto KH, Brown RL, et al. A human factors framework and study of the effect of nursing workload on
patient safety and employee quality of working life. BMJ Quality and Safety. 2011;20(1):15–24. pmid:2011316479.
Garrouste-Orgeas M, Perrin M, Soufir L, Vesin A, Blot F, Maxime V, et al. The Iatroref study: medical errors are associated with symptoms of depression
in ICU staff but not burnout or safety culture. Intensive Care Medicine. 2015;41(2):273–84. pmid:2015719476.
Kirwan M, Matthews A, Scott PA. The impact of the work environment of nurses on patient safety outcomes: a multi-level modelling approach.
International journal of nursing studies. 2013;50(2):253–63. pmid:23116681
Linden DVD, Keijsers GP, Eling P, Schaijk RV. Work stress and attentional difficulties: An initial study on burnout and cognitive failures. Work & Stress.
2005;19(1):23–36.
1 out of 10
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.