Population Needs Assessment for Afghan Migrants in Western Australia
VerifiedAdded on 2023/06/10
|11
|3406
|232
AI Summary
This paper conducts a community needs assessment for Afghan migrants in Western Australia, analyzing their demographics, health issues, and social determinants of health. The paper highlights the need for mental health counseling, employment opportunities, and eradication of social stigmatization.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: POPULATION NEEDS ASSESSMENT
Population Needs Assessment
Name of the Student
Name of the University
Author Note
Population Needs Assessment
Name of the Student
Name of the University
Author Note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
POPULATION NEEDS ASSESSMENT
Introduction
Immigration is an integral part of the development of the Australian economy, society
and population. Today 27% of the population in Australia are migrants (Australian
Demographic Statistics, 2017). Like the rest of Australia, migration have increased and
shaped the population of Western Australia (WA). Today, WA has fastest growing
population of all States and Territories in Australia (Government of Western Australia, 2012).
The following paper aims to conduct community need assessment and the chosen community
is Afghan migrants in Western Australia. The analysing the health needs of the community,
the paper will initiate with the demographic study of the Afghan migrants in Australia
followed by their health care needs. At the end, the paper will highlight the three leading
social determinates of health underlying the major health issue identified among the Afghan
migrants in Australia. Identification of the poor social determinants of health in relation to
health issue and demography will help to highlight the specific health needs of the chosen
community. This in turn will to act on specific policies to uplift their health condition within
the society.
Demographics
The population of WA has increased by 2.9% since 31st December 2011 in
comparison to the overall 1.4% of the total increase in the Australian population. At least
60% of the growth rate is contributed by the international migration. At present 31% of
people residing in WA are born overseas in comparison to the rest of the Australia where
27% were born overseas (Australian Demographic Statistics, 2017). Among the migrants in
WA, a significant number of populations include Afghan immigrants. According to
Australian Bureau of Statistics (2016), 28,597 Afghanistan-born people reside in Australia
and this percentage has increased by 70.7% in comparison to the 2006 Census. The 2011
1
Introduction
Immigration is an integral part of the development of the Australian economy, society
and population. Today 27% of the population in Australia are migrants (Australian
Demographic Statistics, 2017). Like the rest of Australia, migration have increased and
shaped the population of Western Australia (WA). Today, WA has fastest growing
population of all States and Territories in Australia (Government of Western Australia, 2012).
The following paper aims to conduct community need assessment and the chosen community
is Afghan migrants in Western Australia. The analysing the health needs of the community,
the paper will initiate with the demographic study of the Afghan migrants in Australia
followed by their health care needs. At the end, the paper will highlight the three leading
social determinates of health underlying the major health issue identified among the Afghan
migrants in Australia. Identification of the poor social determinants of health in relation to
health issue and demography will help to highlight the specific health needs of the chosen
community. This in turn will to act on specific policies to uplift their health condition within
the society.
Demographics
The population of WA has increased by 2.9% since 31st December 2011 in
comparison to the overall 1.4% of the total increase in the Australian population. At least
60% of the growth rate is contributed by the international migration. At present 31% of
people residing in WA are born overseas in comparison to the rest of the Australia where
27% were born overseas (Australian Demographic Statistics, 2017). Among the migrants in
WA, a significant number of populations include Afghan immigrants. According to
Australian Bureau of Statistics (2016), 28,597 Afghanistan-born people reside in Australia
and this percentage has increased by 70.7% in comparison to the 2006 Census. The 2011
1
POPULATION NEEDS ASSESSMENT
distribution by state and territory indicated that 3926 Afghan migrants reside in Australia
(Australian Government – Department of Social Services, 2014). Median age of Afghanistan-
born in 2011 was 30 years. The distribution of age highlighted that 10% of the Afghan
population are age between 0 to 14 years and 26.7 per cent of the population are aged
between 15 to 24 years and 43.5% of the population fall between age group of 25 to 44 years.
Among the total population, 16,835 are males (58.9%) and 11,764 are females (41.1%). The
sex ratio is 143.1 males per 100 females. The lack of parity in gender indicates that in Afghan
population male child are given more preference than female child (Australian Government
Department of Social Services, 2014).
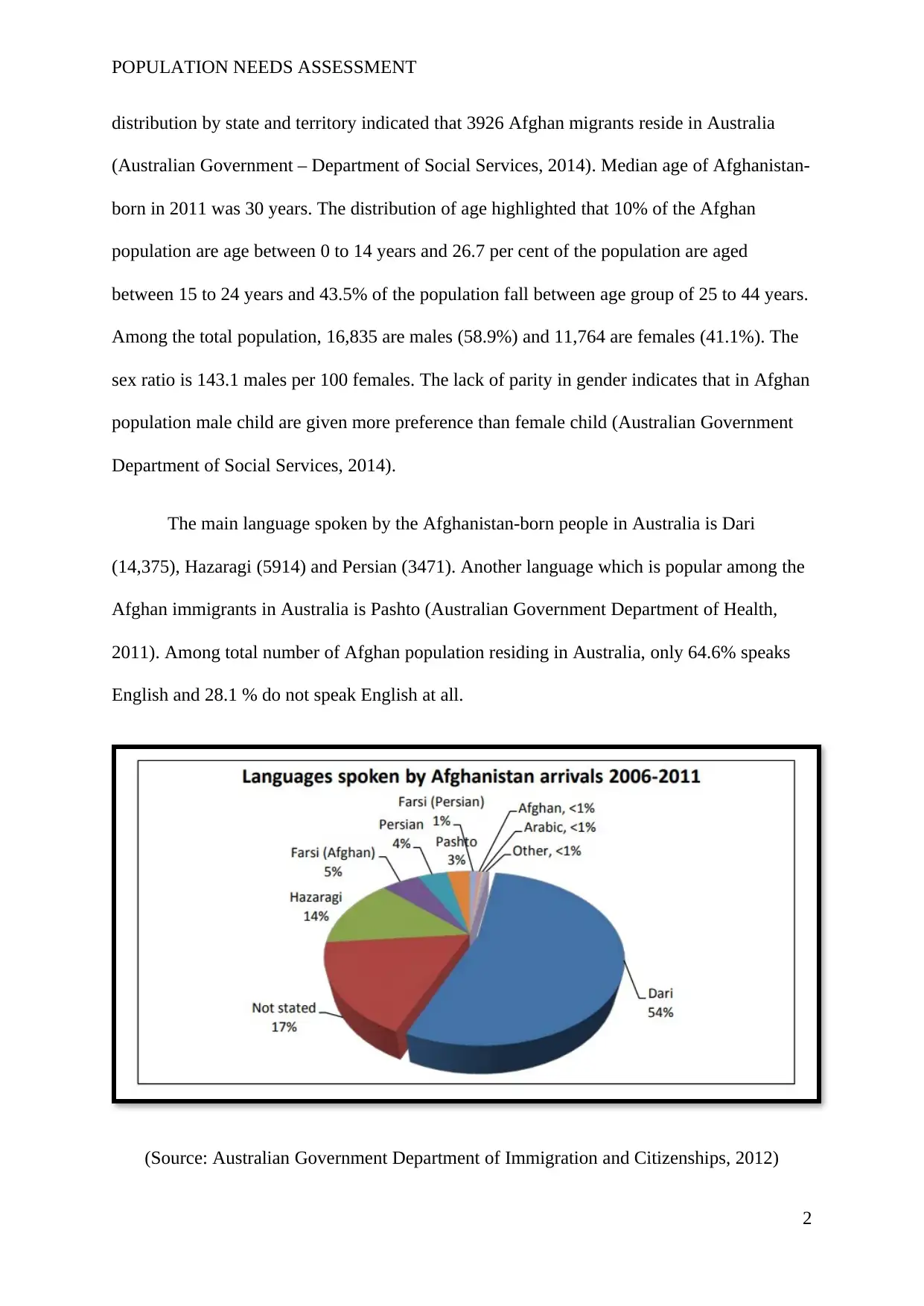
The main language spoken by the Afghanistan-born people in Australia is Dari
(14,375), Hazaragi (5914) and Persian (3471). Another language which is popular among the
Afghan immigrants in Australia is Pashto (Australian Government Department of Health,
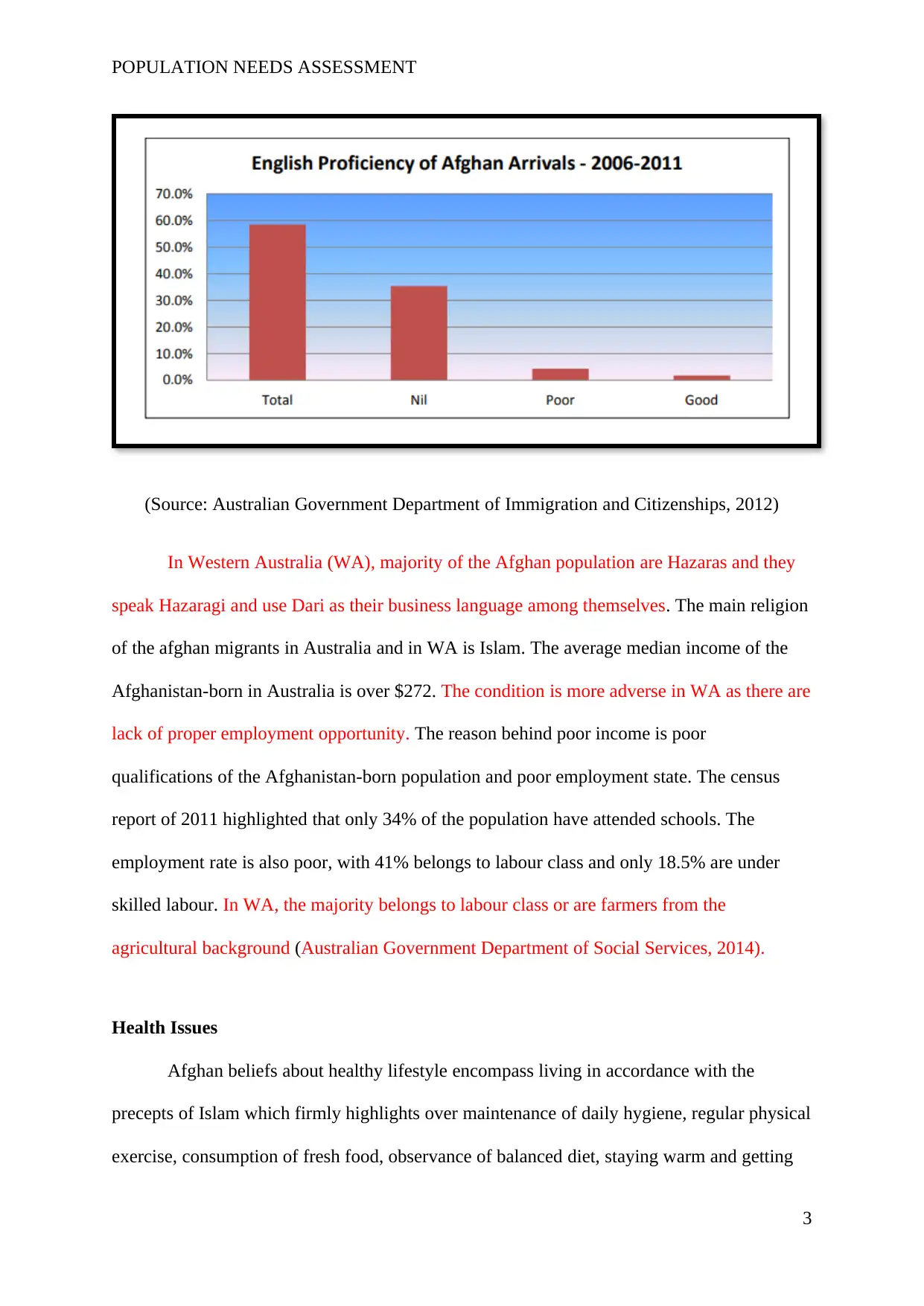
2011). Among total number of Afghan population residing in Australia, only 64.6% speaks
English and 28.1 % do not speak English at all.
(Source: Australian Government Department of Immigration and Citizenships, 2012)
2
distribution by state and territory indicated that 3926 Afghan migrants reside in Australia
(Australian Government – Department of Social Services, 2014). Median age of Afghanistan-
born in 2011 was 30 years. The distribution of age highlighted that 10% of the Afghan
population are age between 0 to 14 years and 26.7 per cent of the population are aged
between 15 to 24 years and 43.5% of the population fall between age group of 25 to 44 years.
Among the total population, 16,835 are males (58.9%) and 11,764 are females (41.1%). The
sex ratio is 143.1 males per 100 females. The lack of parity in gender indicates that in Afghan
population male child are given more preference than female child (Australian Government
Department of Social Services, 2014).
The main language spoken by the Afghanistan-born people in Australia is Dari
(14,375), Hazaragi (5914) and Persian (3471). Another language which is popular among the
Afghan immigrants in Australia is Pashto (Australian Government Department of Health,
2011). Among total number of Afghan population residing in Australia, only 64.6% speaks
English and 28.1 % do not speak English at all.
(Source: Australian Government Department of Immigration and Citizenships, 2012)
2
POPULATION NEEDS ASSESSMENT
(Source: Australian Government Department of Immigration and Citizenships, 2012)
In Western Australia (WA), majority of the Afghan population are Hazaras and they
speak Hazaragi and use Dari as their business language among themselves. The main religion
of the afghan migrants in Australia and in WA is Islam. The average median income of the
Afghanistan-born in Australia is over $272. The condition is more adverse in WA as there are
lack of proper employment opportunity. The reason behind poor income is poor
qualifications of the Afghanistan-born population and poor employment state. The census
report of 2011 highlighted that only 34% of the population have attended schools. The
employment rate is also poor, with 41% belongs to labour class and only 18.5% are under
skilled labour. In WA, the majority belongs to labour class or are farmers from the
agricultural background (Australian Government Department of Social Services, 2014).
Health Issues
Afghan beliefs about healthy lifestyle encompass living in accordance with the
precepts of Islam which firmly highlights over maintenance of daily hygiene, regular physical
exercise, consumption of fresh food, observance of balanced diet, staying warm and getting
3
(Source: Australian Government Department of Immigration and Citizenships, 2012)
In Western Australia (WA), majority of the Afghan population are Hazaras and they
speak Hazaragi and use Dari as their business language among themselves. The main religion
of the afghan migrants in Australia and in WA is Islam. The average median income of the
Afghanistan-born in Australia is over $272. The condition is more adverse in WA as there are
lack of proper employment opportunity. The reason behind poor income is poor
qualifications of the Afghanistan-born population and poor employment state. The census
report of 2011 highlighted that only 34% of the population have attended schools. The
employment rate is also poor, with 41% belongs to labour class and only 18.5% are under
skilled labour. In WA, the majority belongs to labour class or are farmers from the
agricultural background (Australian Government Department of Social Services, 2014).
Health Issues
Afghan beliefs about healthy lifestyle encompass living in accordance with the
precepts of Islam which firmly highlights over maintenance of daily hygiene, regular physical
exercise, consumption of fresh food, observance of balanced diet, staying warm and getting
3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
POPULATION NEEDS ASSESSMENT
adequate rest (ACT Government, 2014). In spite to maintaining daily hygiene, oral health is a
concern among the Afghan migrants residing in Australia. Keboa, Hiles and Macdonald
(2016) conducted a research via scoping review methodology in order to analyse the overall
burden of oral disease over Afghan migrants in Australia. The analysis of 3321 records from
eight different databases highlighted that there exist oral health disparities among the migrant
population throughput Australia and mainly in the WA. Mengesha, Perz, Dune and Ussher
(2017) conducted qualitative interview by the healthcare professionals over Australian
refuges and migrants in WA. The thematic analysis of the interview highlighted that migrant
or refugee women do not have proper access to sexual and reproductive health due to
multifaceted challenge. The people residing in WA mainly have faith in herbal medicines and
believe that the disease of any infectious disease is an outcome of sin (Australian
Government Department of Immigration and Citizenships, 2012). However, there is lack of
significant data about the physical health status of the Afghan migrants residing in WA.
Giallo et al. (2017) conducted cross sectional survey with aim to study the physical
and mental health of the migrant Afghan fathers. The population based study highlighted
fathers of refugee background, experience poor mental health and physical health condition
in comparison to the Australian-born fathers. The migrated fathers from the non-English
speaking countries like Afghanistan report higher psychological distress in comparison to the
Australian-born fathers. This undermines the requirement for the primary healthcare services
to optimise the efforts to decrease inequalities in health outcomes of the refugee populations
that may be vulnerable under certain circumstances. However, it must also be taken into
consideration that the refugee father are less likely to indulge alcohol abuse and are less
likely to be overweight in comparison to the Australian-born fathers (Giallo et al., 2017).
Moreover, as a result of the experiences of war and displacement and their ill-treatment as
refugees, the Afghan people experiences high risk of developing mental health issues and
4
adequate rest (ACT Government, 2014). In spite to maintaining daily hygiene, oral health is a
concern among the Afghan migrants residing in Australia. Keboa, Hiles and Macdonald
(2016) conducted a research via scoping review methodology in order to analyse the overall
burden of oral disease over Afghan migrants in Australia. The analysis of 3321 records from
eight different databases highlighted that there exist oral health disparities among the migrant
population throughput Australia and mainly in the WA. Mengesha, Perz, Dune and Ussher
(2017) conducted qualitative interview by the healthcare professionals over Australian
refuges and migrants in WA. The thematic analysis of the interview highlighted that migrant
or refugee women do not have proper access to sexual and reproductive health due to
multifaceted challenge. The people residing in WA mainly have faith in herbal medicines and
believe that the disease of any infectious disease is an outcome of sin (Australian
Government Department of Immigration and Citizenships, 2012). However, there is lack of
significant data about the physical health status of the Afghan migrants residing in WA.
Giallo et al. (2017) conducted cross sectional survey with aim to study the physical
and mental health of the migrant Afghan fathers. The population based study highlighted
fathers of refugee background, experience poor mental health and physical health condition
in comparison to the Australian-born fathers. The migrated fathers from the non-English
speaking countries like Afghanistan report higher psychological distress in comparison to the
Australian-born fathers. This undermines the requirement for the primary healthcare services
to optimise the efforts to decrease inequalities in health outcomes of the refugee populations
that may be vulnerable under certain circumstances. However, it must also be taken into
consideration that the refugee father are less likely to indulge alcohol abuse and are less
likely to be overweight in comparison to the Australian-born fathers (Giallo et al., 2017).
Moreover, as a result of the experiences of war and displacement and their ill-treatment as
refugees, the Afghan people experiences high risk of developing mental health issues and
4
POPULATION NEEDS ASSESSMENT
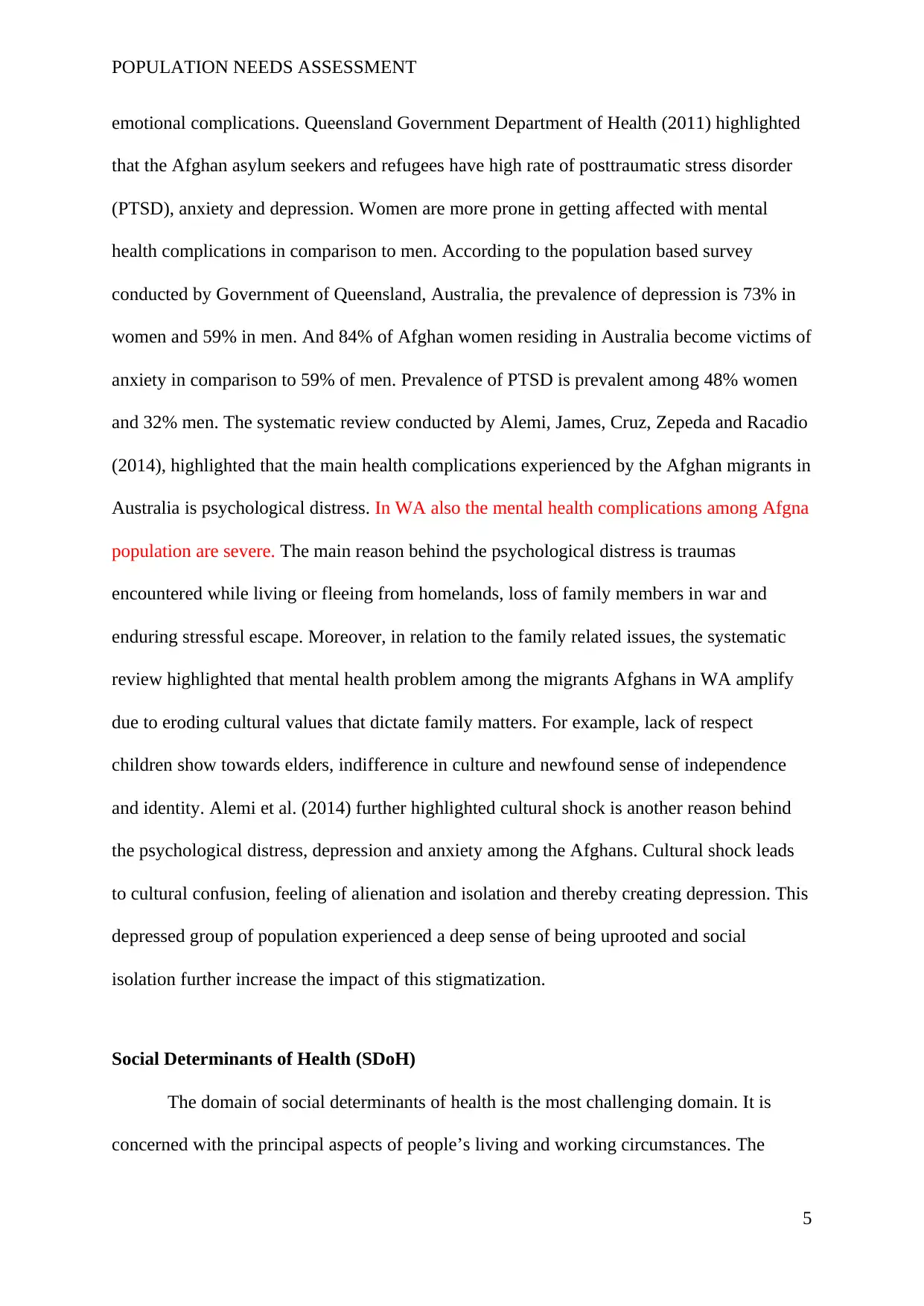
emotional complications. Queensland Government Department of Health (2011) highlighted
that the Afghan asylum seekers and refugees have high rate of posttraumatic stress disorder
(PTSD), anxiety and depression. Women are more prone in getting affected with mental
health complications in comparison to men. According to the population based survey
conducted by Government of Queensland, Australia, the prevalence of depression is 73% in
women and 59% in men. And 84% of Afghan women residing in Australia become victims of
anxiety in comparison to 59% of men. Prevalence of PTSD is prevalent among 48% women
and 32% men. The systematic review conducted by Alemi, James, Cruz, Zepeda and Racadio
(2014), highlighted that the main health complications experienced by the Afghan migrants in
Australia is psychological distress. In WA also the mental health complications among Afgna
population are severe. The main reason behind the psychological distress is traumas
encountered while living or fleeing from homelands, loss of family members in war and
enduring stressful escape. Moreover, in relation to the family related issues, the systematic
review highlighted that mental health problem among the migrants Afghans in WA amplify
due to eroding cultural values that dictate family matters. For example, lack of respect
children show towards elders, indifference in culture and newfound sense of independence
and identity. Alemi et al. (2014) further highlighted cultural shock is another reason behind
the psychological distress, depression and anxiety among the Afghans. Cultural shock leads
to cultural confusion, feeling of alienation and isolation and thereby creating depression. This
depressed group of population experienced a deep sense of being uprooted and social
isolation further increase the impact of this stigmatization.
Social Determinants of Health (SDoH)
The domain of social determinants of health is the most challenging domain. It is
concerned with the principal aspects of people’s living and working circumstances. The
5
emotional complications. Queensland Government Department of Health (2011) highlighted
that the Afghan asylum seekers and refugees have high rate of posttraumatic stress disorder
(PTSD), anxiety and depression. Women are more prone in getting affected with mental
health complications in comparison to men. According to the population based survey
conducted by Government of Queensland, Australia, the prevalence of depression is 73% in
women and 59% in men. And 84% of Afghan women residing in Australia become victims of
anxiety in comparison to 59% of men. Prevalence of PTSD is prevalent among 48% women
and 32% men. The systematic review conducted by Alemi, James, Cruz, Zepeda and Racadio
(2014), highlighted that the main health complications experienced by the Afghan migrants in
Australia is psychological distress. In WA also the mental health complications among Afgna
population are severe. The main reason behind the psychological distress is traumas
encountered while living or fleeing from homelands, loss of family members in war and
enduring stressful escape. Moreover, in relation to the family related issues, the systematic
review highlighted that mental health problem among the migrants Afghans in WA amplify
due to eroding cultural values that dictate family matters. For example, lack of respect
children show towards elders, indifference in culture and newfound sense of independence
and identity. Alemi et al. (2014) further highlighted cultural shock is another reason behind
the psychological distress, depression and anxiety among the Afghans. Cultural shock leads
to cultural confusion, feeling of alienation and isolation and thereby creating depression. This
depressed group of population experienced a deep sense of being uprooted and social
isolation further increase the impact of this stigmatization.
Social Determinants of Health (SDoH)
The domain of social determinants of health is the most challenging domain. It is
concerned with the principal aspects of people’s living and working circumstances. The
5
POPULATION NEEDS ASSESSMENT
social determinants of health are also highlights health implications of economic and social
policies along with the benefits that investing in those health policies will bring (Wilkinson &
Marmot, 2003). Key social determinants of health (SDoH) are influence by socio-economic
position, employment and work and residential environment (Australian Institute of Health
and Welfare, 2016). However, Talbot and Verrinder (2014) stated that choice and decision-
making capabilities of individuals modulates SDoH rather than complex situations outside.
According to McMurray and Clendon (2015) SDoH Assessment circle mainly
highlights 10 different categories and these include biology or genetic characteristics; healthy
development of child; support from social networks; education and literacy rates,
employment and working conditions, social environment; physical environment; health
practice and coping skills; health service and resources; gender and culture.
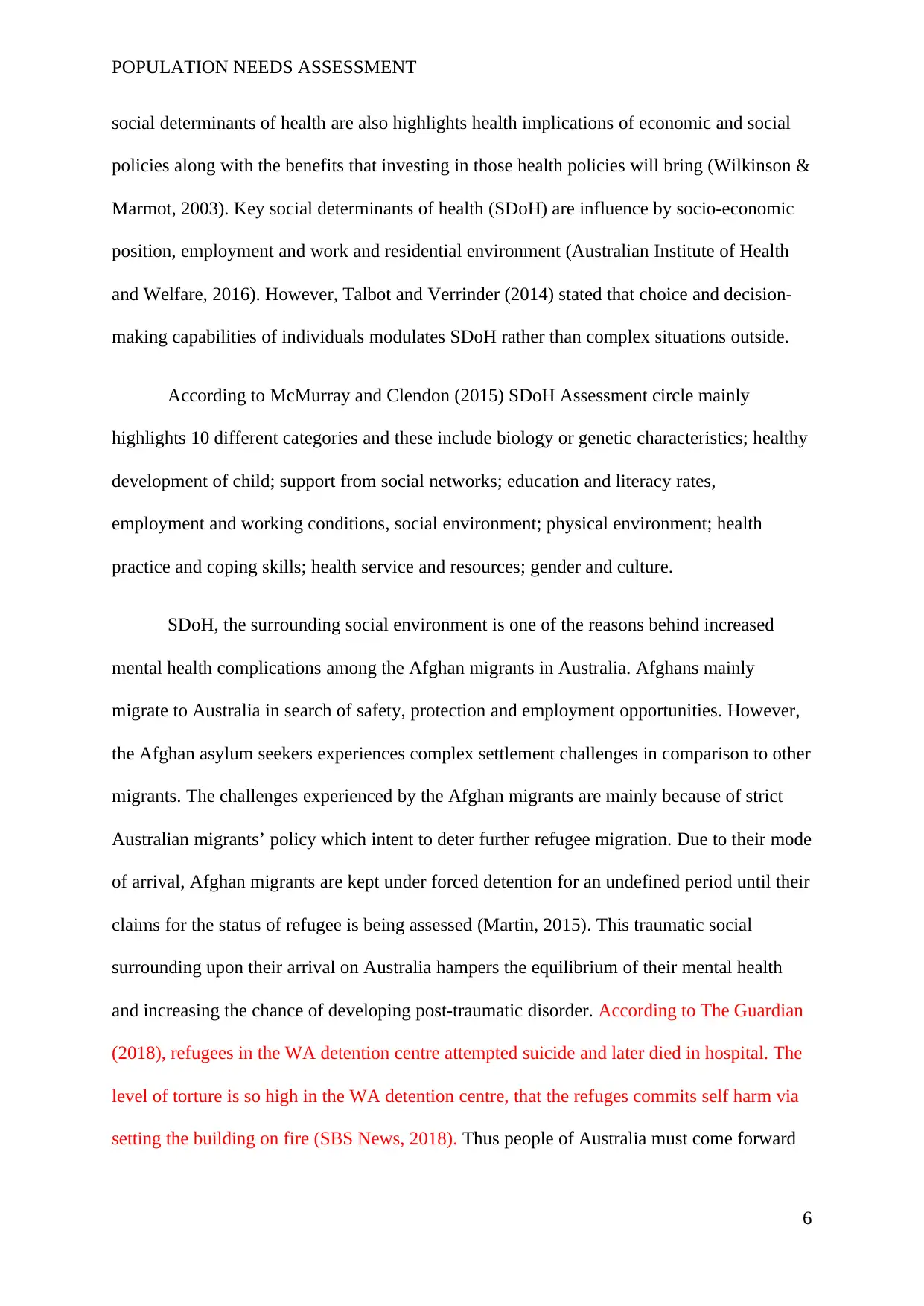
SDoH, the surrounding social environment is one of the reasons behind increased
mental health complications among the Afghan migrants in Australia. Afghans mainly
migrate to Australia in search of safety, protection and employment opportunities. However,
the Afghan asylum seekers experiences complex settlement challenges in comparison to other
migrants. The challenges experienced by the Afghan migrants are mainly because of strict
Australian migrants’ policy which intent to deter further refugee migration. Due to their mode
of arrival, Afghan migrants are kept under forced detention for an undefined period until their
claims for the status of refugee is being assessed (Martin, 2015). This traumatic social
surrounding upon their arrival on Australia hampers the equilibrium of their mental health
and increasing the chance of developing post-traumatic disorder. According to The Guardian
(2018), refugees in the WA detention centre attempted suicide and later died in hospital. The
level of torture is so high in the WA detention centre, that the refuges commits self harm via
setting the building on fire (SBS News, 2018). Thus people of Australia must come forward
6
social determinants of health are also highlights health implications of economic and social
policies along with the benefits that investing in those health policies will bring (Wilkinson &
Marmot, 2003). Key social determinants of health (SDoH) are influence by socio-economic
position, employment and work and residential environment (Australian Institute of Health
and Welfare, 2016). However, Talbot and Verrinder (2014) stated that choice and decision-
making capabilities of individuals modulates SDoH rather than complex situations outside.
According to McMurray and Clendon (2015) SDoH Assessment circle mainly
highlights 10 different categories and these include biology or genetic characteristics; healthy
development of child; support from social networks; education and literacy rates,
employment and working conditions, social environment; physical environment; health
practice and coping skills; health service and resources; gender and culture.
SDoH, the surrounding social environment is one of the reasons behind increased
mental health complications among the Afghan migrants in Australia. Afghans mainly
migrate to Australia in search of safety, protection and employment opportunities. However,
the Afghan asylum seekers experiences complex settlement challenges in comparison to other
migrants. The challenges experienced by the Afghan migrants are mainly because of strict
Australian migrants’ policy which intent to deter further refugee migration. Due to their mode
of arrival, Afghan migrants are kept under forced detention for an undefined period until their
claims for the status of refugee is being assessed (Martin, 2015). This traumatic social
surrounding upon their arrival on Australia hampers the equilibrium of their mental health
and increasing the chance of developing post-traumatic disorder. According to The Guardian
(2018), refugees in the WA detention centre attempted suicide and later died in hospital. The
level of torture is so high in the WA detention centre, that the refuges commits self harm via
setting the building on fire (SBS News, 2018). Thus people of Australia must come forward
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
POPULATION NEEDS ASSESSMENT
in order to decrease social stigmatization so that the Afghan migrants might feel welcomed
(Li, Liddell & Nickerson, 2016).
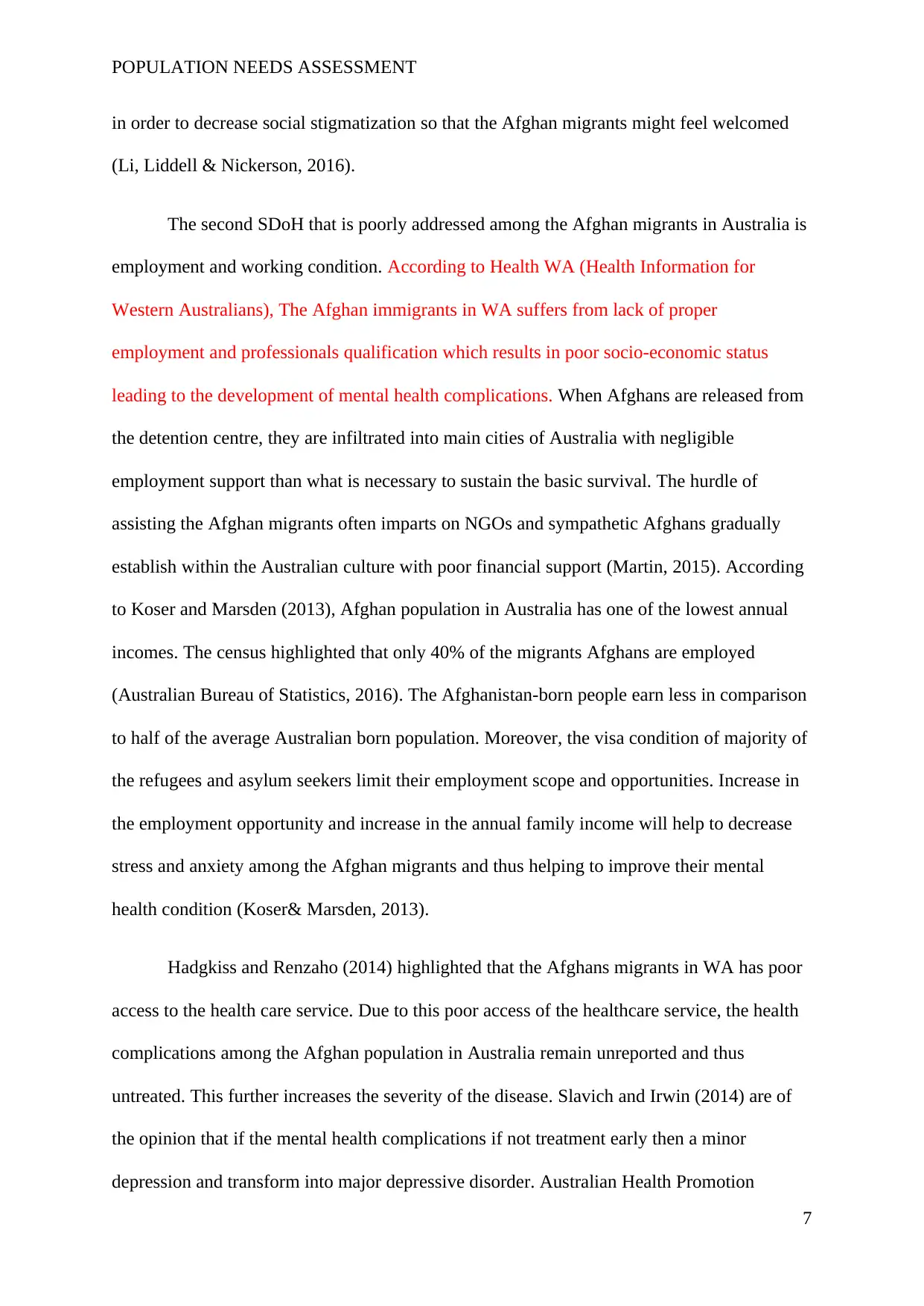
The second SDoH that is poorly addressed among the Afghan migrants in Australia is
employment and working condition. According to Health WA (Health Information for
Western Australians), The Afghan immigrants in WA suffers from lack of proper
employment and professionals qualification which results in poor socio-economic status
leading to the development of mental health complications. When Afghans are released from
the detention centre, they are infiltrated into main cities of Australia with negligible
employment support than what is necessary to sustain the basic survival. The hurdle of
assisting the Afghan migrants often imparts on NGOs and sympathetic Afghans gradually
establish within the Australian culture with poor financial support (Martin, 2015). According
to Koser and Marsden (2013), Afghan population in Australia has one of the lowest annual
incomes. The census highlighted that only 40% of the migrants Afghans are employed
(Australian Bureau of Statistics, 2016). The Afghanistan-born people earn less in comparison
to half of the average Australian born population. Moreover, the visa condition of majority of
the refugees and asylum seekers limit their employment scope and opportunities. Increase in
the employment opportunity and increase in the annual family income will help to decrease
stress and anxiety among the Afghan migrants and thus helping to improve their mental
health condition (Koser& Marsden, 2013).
Hadgkiss and Renzaho (2014) highlighted that the Afghans migrants in WA has poor
access to the health care service. Due to this poor access of the healthcare service, the health
complications among the Afghan population in Australia remain unreported and thus
untreated. This further increases the severity of the disease. Slavich and Irwin (2014) are of
the opinion that if the mental health complications if not treatment early then a minor
depression and transform into major depressive disorder. Australian Health Promotion
7
in order to decrease social stigmatization so that the Afghan migrants might feel welcomed
(Li, Liddell & Nickerson, 2016).
The second SDoH that is poorly addressed among the Afghan migrants in Australia is
employment and working condition. According to Health WA (Health Information for
Western Australians), The Afghan immigrants in WA suffers from lack of proper
employment and professionals qualification which results in poor socio-economic status
leading to the development of mental health complications. When Afghans are released from
the detention centre, they are infiltrated into main cities of Australia with negligible
employment support than what is necessary to sustain the basic survival. The hurdle of
assisting the Afghan migrants often imparts on NGOs and sympathetic Afghans gradually
establish within the Australian culture with poor financial support (Martin, 2015). According
to Koser and Marsden (2013), Afghan population in Australia has one of the lowest annual
incomes. The census highlighted that only 40% of the migrants Afghans are employed
(Australian Bureau of Statistics, 2016). The Afghanistan-born people earn less in comparison
to half of the average Australian born population. Moreover, the visa condition of majority of
the refugees and asylum seekers limit their employment scope and opportunities. Increase in
the employment opportunity and increase in the annual family income will help to decrease
stress and anxiety among the Afghan migrants and thus helping to improve their mental
health condition (Koser& Marsden, 2013).
Hadgkiss and Renzaho (2014) highlighted that the Afghans migrants in WA has poor
access to the health care service. Due to this poor access of the healthcare service, the health
complications among the Afghan population in Australia remain unreported and thus
untreated. This further increases the severity of the disease. Slavich and Irwin (2014) are of
the opinion that if the mental health complications if not treatment early then a minor
depression and transform into major depressive disorder. Australian Health Promotion
7
POPULATION NEEDS ASSESSMENT
Association (APHA) is working actively in order to reduce these health inequalities. They
mainly work through leadership, advocacy in order to support health promotion action in
policy, practice and research.
Conclusion
Analysis of the available literature highlighted that there is lack of significant data
about the physical health condition of the Afghan migrant groups residing in Australia.
However, there are reports which highlights that the Afghan migrants suffer from severe
mental health complications like post traumatic stress disorder, depression and anxiety. The
migrant Afghan women are the major victims of these mental health related complications.
The analysis of the social determinants of health highlighted that poor social environment in
the detention centre, lack of proper income or employment, social exclusion and lack of
proper access to the healthcare service are main reasons behind high occurrence of the mental
complications among the Afghan migrants. In order to reduce these health inequalities among
the migrants, Australian Health Promotion Association (APHA) is coming forward active
leadership and advocacy. Other important health promotion involves proper mental health
counselling, employment opportunity and eradication of the social stigmatization of the
Afghan migrants.
References
ACT Government. (2014). ACT Health Community Profile Afghanistan. Access date: 27th
August 2018. Retrieved from: https://www.health.act.gov.au/sites/default/files/ACT
%20Health%20Community%20Profile%20-%20Afganistan%20%282014%29.pdf
Alemi, Q., James, S., Cruz, R., Zepeda, V., & Racadio, M. (2014). Psychological distress in
Afghan refugees: A mixed-method systematic review. Journal of immigrant and
minority health, 16(6), 1247-1261. doi: 10.1007/s10903-013-9861-1
8
Association (APHA) is working actively in order to reduce these health inequalities. They
mainly work through leadership, advocacy in order to support health promotion action in
policy, practice and research.
Conclusion
Analysis of the available literature highlighted that there is lack of significant data
about the physical health condition of the Afghan migrant groups residing in Australia.
However, there are reports which highlights that the Afghan migrants suffer from severe
mental health complications like post traumatic stress disorder, depression and anxiety. The
migrant Afghan women are the major victims of these mental health related complications.
The analysis of the social determinants of health highlighted that poor social environment in
the detention centre, lack of proper income or employment, social exclusion and lack of
proper access to the healthcare service are main reasons behind high occurrence of the mental
complications among the Afghan migrants. In order to reduce these health inequalities among
the migrants, Australian Health Promotion Association (APHA) is coming forward active
leadership and advocacy. Other important health promotion involves proper mental health
counselling, employment opportunity and eradication of the social stigmatization of the
Afghan migrants.
References
ACT Government. (2014). ACT Health Community Profile Afghanistan. Access date: 27th
August 2018. Retrieved from: https://www.health.act.gov.au/sites/default/files/ACT
%20Health%20Community%20Profile%20-%20Afganistan%20%282014%29.pdf
Alemi, Q., James, S., Cruz, R., Zepeda, V., & Racadio, M. (2014). Psychological distress in
Afghan refugees: A mixed-method systematic review. Journal of immigrant and
minority health, 16(6), 1247-1261. doi: 10.1007/s10903-013-9861-1
8
POPULATION NEEDS ASSESSMENT
Australian Bureau of Statistics. (2016). 2016 Census QuickStats. Access date: 30th August
2018. Retrieved from:
http://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/
quickstat/5?opendocument
Australian Demographic Statistics, Dec 2017. December Key Figures. Access date: 27th
August 2018. Retrieved from: http://www.abs.gov.au/ausstats/abs@.nsf/mf/3101.0
Australian Government Department of Immigration and Citizenships. (2012). Afghan
Community Profile. Access date: 9th September 2018. Retrieved from:
https://www.dss.gov.au/sites/default/files/documents/11_2013/community-profile-
afghan.pdf
Australian Government Department of Social Services. (2014). The Afghanistan-born
Community. Access date: 27th August 2018. Retrieved from:
https://www.dss.gov.au/our-responsibilities/settlement-services/programs-policy/a-
multicultural-australia/programs-and-publications/community-information-
summaries/the-afghanistan-born-community
Australian Health Promotion Association (APHA) (2018). About Us: what we do. Access
date: 30th August 2018. Retrieved from: https://www.healthpromotion.org.au/
Australian Institute of Health and Welfare. (2016). Australia’s Health 2016. Access date: 30th
August 2018. Retrieved from:
https://www.aihw.gov.au/reports/australias-health/australias-health-2016/contents/
determinants
Giallo, R., Riggs, E., Lynch, C., Vanpraag, D., Yelland, J., Szwarc, J., ...& Brown, S. J.
(2017). The physical and mental health problems of refugee and migrant fathers:
findings from an Australian population-based study of children and their
families. BMJ open, 7(11), e015603. http://dx.doi.org/10.1136/bmjopen-2016-015603
Government of Western Australia – Department of Local Government Office of Multicultural
Interests. (2012). The Economic and Social Contribution of Migrants to Western
Australia. Access date: 27th August 2018. Retrieved from:
https://www.omi.wa.gov.au/StatsInfoGuides/Documents/lga_guides/Economic_Social
_Contributions_MigrantsWA_Final_Report.pdf
Hadgkiss, E. J., &Renzaho, A. M. (2014). The physical health status, service utilisation and
barriers to accessing care for asylum seekers residing in the community: a systematic
review of the literature. Australian Health Review, 38(2), 142-159.
https://doi.org/10.1071/AH13113
Health WA Health Information for Western Australians. (2018). Migrant and refugee mental
health. Access date: 9th September 2018. Retrieved from:
https://www.sbs.com.au/news/riot-breaks-out-in-wa-detention-centre-after-detainee-
self-harms
Keboa, M. T., Hiles, N., & Macdonald, M. E. (2016). The oral health of refugees and asylum
seekers: a scoping review. Globalization and health, 12(1), 59. doi: 10.1186/s12992-
016-0200-x
9
Australian Bureau of Statistics. (2016). 2016 Census QuickStats. Access date: 30th August
2018. Retrieved from:
http://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/
quickstat/5?opendocument
Australian Demographic Statistics, Dec 2017. December Key Figures. Access date: 27th
August 2018. Retrieved from: http://www.abs.gov.au/ausstats/abs@.nsf/mf/3101.0
Australian Government Department of Immigration and Citizenships. (2012). Afghan
Community Profile. Access date: 9th September 2018. Retrieved from:
https://www.dss.gov.au/sites/default/files/documents/11_2013/community-profile-
afghan.pdf
Australian Government Department of Social Services. (2014). The Afghanistan-born
Community. Access date: 27th August 2018. Retrieved from:
https://www.dss.gov.au/our-responsibilities/settlement-services/programs-policy/a-
multicultural-australia/programs-and-publications/community-information-
summaries/the-afghanistan-born-community
Australian Health Promotion Association (APHA) (2018). About Us: what we do. Access
date: 30th August 2018. Retrieved from: https://www.healthpromotion.org.au/
Australian Institute of Health and Welfare. (2016). Australia’s Health 2016. Access date: 30th
August 2018. Retrieved from:
https://www.aihw.gov.au/reports/australias-health/australias-health-2016/contents/
determinants
Giallo, R., Riggs, E., Lynch, C., Vanpraag, D., Yelland, J., Szwarc, J., ...& Brown, S. J.
(2017). The physical and mental health problems of refugee and migrant fathers:
findings from an Australian population-based study of children and their
families. BMJ open, 7(11), e015603. http://dx.doi.org/10.1136/bmjopen-2016-015603
Government of Western Australia – Department of Local Government Office of Multicultural
Interests. (2012). The Economic and Social Contribution of Migrants to Western
Australia. Access date: 27th August 2018. Retrieved from:
https://www.omi.wa.gov.au/StatsInfoGuides/Documents/lga_guides/Economic_Social
_Contributions_MigrantsWA_Final_Report.pdf
Hadgkiss, E. J., &Renzaho, A. M. (2014). The physical health status, service utilisation and
barriers to accessing care for asylum seekers residing in the community: a systematic
review of the literature. Australian Health Review, 38(2), 142-159.
https://doi.org/10.1071/AH13113
Health WA Health Information for Western Australians. (2018). Migrant and refugee mental
health. Access date: 9th September 2018. Retrieved from:
https://www.sbs.com.au/news/riot-breaks-out-in-wa-detention-centre-after-detainee-
self-harms
Keboa, M. T., Hiles, N., & Macdonald, M. E. (2016). The oral health of refugees and asylum
seekers: a scoping review. Globalization and health, 12(1), 59. doi: 10.1186/s12992-
016-0200-x
9
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
POPULATION NEEDS ASSESSMENT
Koser, K., & Marsden, P. (2013). Migration and displacement impacts of Afghan transitions
in 2014: implications for Australia. Migration.
Li, S. S., Liddell, B. J., & Nickerson, A. (2016). The relationship between post-migration
stress and psychological disorders in refugees and asylum seekers. Current psychiatry
reports, 18(9), 82.https://doi.org/10.1007/s11920-016-0723-0
Martin, G. (2015). Stop the boats! Moral panic in Australia over asylum
seekers. Continuum, 29(3), 304-322. https://doi.org/10.1080/10304312.2014.986060
McMurray, A., & Clendon, J. (2015). Community Health and Wellness-E-book: Primary
Health Care in Practice. Elsevier Health Sciences.
Mengesha, Z. B., Perz, J., Dune, T., & Ussher, J. (2017). Refugee and migrant women's
engagement with sexual and reproductive health care in Australia: A socio-ecological
analysis of health care professional perspectives. PloS one, 12(7), e0181421.
https://doi.org/10.1371/journal.pone.0181421
Queensland Government Department of Health. (2011). Afghan Australians. Access date:
29th August 2018. Retrieved from:
https://www.health.qld.gov.au/__data/assets/pdf_file/0032/156398/afghan2011.pdf
SBS News. (2018). Detainees at a West Australian detention centre have caused damage and
set buildings alight after a detainee seriously injured himself. Access date: 9th
September 2018. Retrieved from: https://www.sbs.com.au/news/riot-breaks-out-in-
wa-detention-centre-after-detainee-self-harms
Slavich, G. M., & Irwin, M. R. (2014). From stress to inflammation and major depressive
disorder: a social signal transduction theory of depression. Psychological
bulletin, 140(3), 774. http://dx.doi.org/10.1037/a0035302
Talbot, L., &Verrinder, G. (2014). Promoting health: the primary health care approach.
Sydney:ChurchillLivingstone. Elsevier Health Sciences.
The Guardian. (2017). Maternal death rates in Afghanistan may be worse than previously
thought. Access date: 30th August 2018. Retrieved from:
https://www.theguardian.com/global-development/2017/jan/30/maternal-death-rates-
in-afghanistan-may-be-worse-than-previously-thought
The Guardian. (2018). Refugee who attempted suicide in WA detention centre dies in hospital.
Access date: 9th September 2018. Retrieved from:
https://www.theguardian.com/australia-news/2018/sep/06/refugee-who-attempted-
suicide-in-wa-detention-centre-dies-in-hospital
Wilkinson, R. G., & Marmot, M. (Eds.). (2003). Social determinants of health: the solid
facts. World Health Organization.
10
Koser, K., & Marsden, P. (2013). Migration and displacement impacts of Afghan transitions
in 2014: implications for Australia. Migration.
Li, S. S., Liddell, B. J., & Nickerson, A. (2016). The relationship between post-migration
stress and psychological disorders in refugees and asylum seekers. Current psychiatry
reports, 18(9), 82.https://doi.org/10.1007/s11920-016-0723-0
Martin, G. (2015). Stop the boats! Moral panic in Australia over asylum
seekers. Continuum, 29(3), 304-322. https://doi.org/10.1080/10304312.2014.986060
McMurray, A., & Clendon, J. (2015). Community Health and Wellness-E-book: Primary
Health Care in Practice. Elsevier Health Sciences.
Mengesha, Z. B., Perz, J., Dune, T., & Ussher, J. (2017). Refugee and migrant women's
engagement with sexual and reproductive health care in Australia: A socio-ecological
analysis of health care professional perspectives. PloS one, 12(7), e0181421.
https://doi.org/10.1371/journal.pone.0181421
Queensland Government Department of Health. (2011). Afghan Australians. Access date:
29th August 2018. Retrieved from:
https://www.health.qld.gov.au/__data/assets/pdf_file/0032/156398/afghan2011.pdf
SBS News. (2018). Detainees at a West Australian detention centre have caused damage and
set buildings alight after a detainee seriously injured himself. Access date: 9th
September 2018. Retrieved from: https://www.sbs.com.au/news/riot-breaks-out-in-
wa-detention-centre-after-detainee-self-harms
Slavich, G. M., & Irwin, M. R. (2014). From stress to inflammation and major depressive
disorder: a social signal transduction theory of depression. Psychological
bulletin, 140(3), 774. http://dx.doi.org/10.1037/a0035302
Talbot, L., &Verrinder, G. (2014). Promoting health: the primary health care approach.
Sydney:ChurchillLivingstone. Elsevier Health Sciences.
The Guardian. (2017). Maternal death rates in Afghanistan may be worse than previously
thought. Access date: 30th August 2018. Retrieved from:
https://www.theguardian.com/global-development/2017/jan/30/maternal-death-rates-
in-afghanistan-may-be-worse-than-previously-thought
The Guardian. (2018). Refugee who attempted suicide in WA detention centre dies in hospital.
Access date: 9th September 2018. Retrieved from:
https://www.theguardian.com/australia-news/2018/sep/06/refugee-who-attempted-
suicide-in-wa-detention-centre-dies-in-hospital
Wilkinson, R. G., & Marmot, M. (Eds.). (2003). Social determinants of health: the solid
facts. World Health Organization.
10
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.