Federation University Angina Analysis: Clinical Reasoning Essay
VerifiedAdded on 2023/04/10
|13
|2810
|479
Essay
AI Summary
This essay analyzes a clinical case study of a patient, Jon, suffering from angina. It details the pathophysiology of angina, including risk factors like smoking, high cholesterol, hypertension, and obesity, and discusses treatment options such as medication, surgery, and lifestyle changes. The essay outlines three types of physical nursing assessments, including chest pain assessment, nuclear stress tests, and coronary angiography, with rationales for their use in Jon's case. It further explores three nursing interventions (excluding pharmacological) aimed at improving Jon's chest pain, emphasizing patient education, elevating the head of the bed, and monitoring anxiety. The administration of sublingual glyceryl trinitrate is discussed, including its benefits, risks, contraindications, and patient education. Finally, the essay reports the abnormal finding of atrial fibrillation from Jon's ECG and explains the need for immediate reporting to the doctor. The content is presented in a question-and-answer format, adhering to the assignment brief's requirements.

Running head: ANALYSIS OF ANGINA
ANALYSIS OF ANGINA
Name of the Student:
Name of the University:
Author note:
ANALYSIS OF ANGINA
Name of the Student:
Name of the University:
Author note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1ANALYSIS OF ANGINA
Q1) Describe the pathophysiology (cause, progression and outcome) of Angina. Include in
your answer risk factors for Angina and the treatment options for Angina. Demonstrate links
to Jon’s case.
Angina is considered as a condition, which leads to discomfort in chest or chest pain
due to inadequate supply of blood in the heart. Angina result in insufficient amount of oxygen
in the blood, which is mainly due to thinning of coronary artery (Healthywa.wa.gov.au,
2019).
The primary cause of angina is coronary artery disease (CAD) also denoted as
coronary heart disease (CHD). Arteries are accountable for distributing oxygen-rich blood to
the heart muscle and in this condition the function of artery is effected due to narrowing of
arteries hence, restricting the heart muscle to supply adequate amount of blood. The major
cause of angina is due to mismatch in the amount oxygen demand and the blood flow
(Healthdirect.gov.au, 2019). Restriction in the quantity of blood flow to meet the oxygen
demand leads to narrowing of artery. The myocardial cells in this situation switch to
anaerobic metabolism from aerobic metabolism; leading to advanced damage of electrical,
metabolic and mechanical function. Adenosine is the major trigger for anginal pain (Kloner
& Chaitman, 2017). Hence, during the condition of ischemia, adenosine tri-phosphate (ATP)
is converted to adenosine, which is diffused to extracellular space leading in anginal pain and
dilation of artery.
In the case study, it was clear that Jon was suffering from angina as he had continuous
chest pain. Various risk factors were responsible for his condition such as (Ohman, 2016):
Tobacco consumption- Active or passive smoking can damage the artery by either
deposition of cholesterol or by blocking the path of blood flow. In this case, Jon was a
chain smoker and used to smoke regularly for past 25 years.
Q1) Describe the pathophysiology (cause, progression and outcome) of Angina. Include in
your answer risk factors for Angina and the treatment options for Angina. Demonstrate links
to Jon’s case.
Angina is considered as a condition, which leads to discomfort in chest or chest pain
due to inadequate supply of blood in the heart. Angina result in insufficient amount of oxygen
in the blood, which is mainly due to thinning of coronary artery (Healthywa.wa.gov.au,
2019).
The primary cause of angina is coronary artery disease (CAD) also denoted as
coronary heart disease (CHD). Arteries are accountable for distributing oxygen-rich blood to
the heart muscle and in this condition the function of artery is effected due to narrowing of
arteries hence, restricting the heart muscle to supply adequate amount of blood. The major
cause of angina is due to mismatch in the amount oxygen demand and the blood flow
(Healthdirect.gov.au, 2019). Restriction in the quantity of blood flow to meet the oxygen
demand leads to narrowing of artery. The myocardial cells in this situation switch to
anaerobic metabolism from aerobic metabolism; leading to advanced damage of electrical,
metabolic and mechanical function. Adenosine is the major trigger for anginal pain (Kloner
& Chaitman, 2017). Hence, during the condition of ischemia, adenosine tri-phosphate (ATP)
is converted to adenosine, which is diffused to extracellular space leading in anginal pain and
dilation of artery.
In the case study, it was clear that Jon was suffering from angina as he had continuous
chest pain. Various risk factors were responsible for his condition such as (Ohman, 2016):
Tobacco consumption- Active or passive smoking can damage the artery by either
deposition of cholesterol or by blocking the path of blood flow. In this case, Jon was a
chain smoker and used to smoke regularly for past 25 years.
2ANALYSIS OF ANGINA
High blood cholesterol level- Cholesterol deposits in the inner walls of artery leading
to narrowing of artery throughout the patient body including heart. Excess amount of
bad cholesterol level in the artery proliferates the threat of cardiac attack and angina.
The patient was already suffering from hypercholesterolemia, a condition that
develops due to excess deposition of cholesterol in the artery (Iqbal et al., 2016).
Hypertension- Hypertension or excessive stress increases the risk of heart attack and
angina, as excess stress will increase the blood pressure, which can narrow down the
artery.
Background history of heart disease
Obesity
There are various treatment approaches for angina, which include use of medication or
change in lifestyles and is recommended for the patient well-being (Giannopoulos,
Giannoglou & Chatzizisis, 2016).
Surgery can also be an option for angina such as stenting and angioplasty in which
the doctor insert a balloon to broaden the artery in order to increase the supply of
blood.
Medicines such as aspirin, beta-blockers, statins, ACE inhibitors and calcium channel
blockers helps to broaden the narrowed artery.
Lifestyle change is the major part of treatment, which includes no consumption of
tobacco, consumption of low cholesterol, physical exercise, avoidance of stress and
consumption of healthy diet.
Q2) Discuss THREE types of physical nursing assessments that would be appropriate for
Jon’s complaint (excluding vital signs) you would initiate for Jon and provide a description of
High blood cholesterol level- Cholesterol deposits in the inner walls of artery leading
to narrowing of artery throughout the patient body including heart. Excess amount of
bad cholesterol level in the artery proliferates the threat of cardiac attack and angina.
The patient was already suffering from hypercholesterolemia, a condition that
develops due to excess deposition of cholesterol in the artery (Iqbal et al., 2016).
Hypertension- Hypertension or excessive stress increases the risk of heart attack and
angina, as excess stress will increase the blood pressure, which can narrow down the
artery.
Background history of heart disease
Obesity
There are various treatment approaches for angina, which include use of medication or
change in lifestyles and is recommended for the patient well-being (Giannopoulos,
Giannoglou & Chatzizisis, 2016).
Surgery can also be an option for angina such as stenting and angioplasty in which
the doctor insert a balloon to broaden the artery in order to increase the supply of
blood.
Medicines such as aspirin, beta-blockers, statins, ACE inhibitors and calcium channel
blockers helps to broaden the narrowed artery.
Lifestyle change is the major part of treatment, which includes no consumption of
tobacco, consumption of low cholesterol, physical exercise, avoidance of stress and
consumption of healthy diet.
Q2) Discuss THREE types of physical nursing assessments that would be appropriate for
Jon’s complaint (excluding vital signs) you would initiate for Jon and provide a description of
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3ANALYSIS OF ANGINA
each of these in the context of Jon’s complaint with rationale as to why these would be your
priority.
The three major types of physical nursing assessment that would be appropriate for Jon
complaint is chest pain assessment, stress assessment and assessment of coronary artery.
1. Chest pain assessment- Chest pain assessment is performed for the patient who are
suffering from severe chest pain and is used to detect if the pain is cardiac in nature or
not (Abid et al., 2015). The most widely used method is ‘PQRST’ pain assessment
where,
P- Stands for provoking factors or position. This is used for locating the area of pain,
condition, which can improve or worse the pain and situation responsible for onset of
pain.
Q- Stands for quality. This is used for describing the pain and the type of pain such as
sharp, dull ache, crushing or stabbing pain.
R- Stands for radiation. This is used to check if the pain is radiating to any other part
of the patient body and it is detectable or not.
S- Stands for symptoms or severity. This is used to rate the complexity or severity of
pain at a scale of ten and to determine any other additional symptom (such as nausea
or vomiting) responsible for onset of pain.
T- Stands for time. This is used to estimate the total time of pain that the patient is
suffering and to check if the pain is continuous or intermittent (starts and stops).
Hence, chest pain assessment will determine the severity of pain and the detail nature of
pain, which was the major symptom of angina in Jon (Denn, Noonan & Condon, 2017).
2. Nuclear stress test- As the patient was suffering from hypertension i.e. excess stress,
the assessment of his stress level was important to check to determine the severity of
each of these in the context of Jon’s complaint with rationale as to why these would be your
priority.
The three major types of physical nursing assessment that would be appropriate for Jon
complaint is chest pain assessment, stress assessment and assessment of coronary artery.
1. Chest pain assessment- Chest pain assessment is performed for the patient who are
suffering from severe chest pain and is used to detect if the pain is cardiac in nature or
not (Abid et al., 2015). The most widely used method is ‘PQRST’ pain assessment
where,
P- Stands for provoking factors or position. This is used for locating the area of pain,
condition, which can improve or worse the pain and situation responsible for onset of
pain.
Q- Stands for quality. This is used for describing the pain and the type of pain such as
sharp, dull ache, crushing or stabbing pain.
R- Stands for radiation. This is used to check if the pain is radiating to any other part
of the patient body and it is detectable or not.
S- Stands for symptoms or severity. This is used to rate the complexity or severity of
pain at a scale of ten and to determine any other additional symptom (such as nausea
or vomiting) responsible for onset of pain.
T- Stands for time. This is used to estimate the total time of pain that the patient is
suffering and to check if the pain is continuous or intermittent (starts and stops).
Hence, chest pain assessment will determine the severity of pain and the detail nature of
pain, which was the major symptom of angina in Jon (Denn, Noonan & Condon, 2017).
2. Nuclear stress test- As the patient was suffering from hypertension i.e. excess stress,
the assessment of his stress level was important to check to determine the severity of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4ANALYSIS OF ANGINA
hypertension in onset of angina. This test allows the nurse to determine the amount of
blood flow to the patient heart under stress (Colquhpun et al., 2015). The patient is
made to perform any physical activity so that the heart has to work hard in pumping
blood. A radioactive substance is introduced into the patients’ blood and through a
scanner; proper image is created of the patients’ heart muscle. Inadequate supply of
oxygenated blood will be visible in the scanner due to lack or absence of radioactive
substance (Fredriksson et al., 2015). Hence, it will be helpful in assessing the level of
stress suffered by Jon and accordingly the nurse can conduct stress-free therapy.
3. Coronary angiography- Coronary angiography is used as a physical assessment tool,
which is used to examine the inner part of the blood vessel in the heart. This
assessment tool detects the narrowing of artery due to accumulation of plaque or
cholesterol (Arbab & Fuster, 2016). As Jon was suffering from hypercholesterolemia,
this assessment will help the nurse to understand the severity of accumulation thereby
identifying the nursing intervention to help the patient recover from angina.
Q3) Discuss THREE nursing interventions (excluding pharmacological) you would initiate
and provide rationale as to how these would improve physiological outcomes of Jon’s chest
pain.
Jon was had continuous discomfort in chest, which is the major symptom of angina.
Nursing intervention is performed to manage the complexity of chest pain in the patient by
handling the duration, severity and frequency of pain. Hence, different nursing intervention is
performed to manage the acute chest pain in Jon as described below (Hylands, Duarte &
Raphael, 2017):
Condition Nursing intervention Rationale
Chest pain Educate the patient to
inform the nurse
Reduced cardiac output and
pain might excite the
hypertension in onset of angina. This test allows the nurse to determine the amount of
blood flow to the patient heart under stress (Colquhpun et al., 2015). The patient is
made to perform any physical activity so that the heart has to work hard in pumping
blood. A radioactive substance is introduced into the patients’ blood and through a
scanner; proper image is created of the patients’ heart muscle. Inadequate supply of
oxygenated blood will be visible in the scanner due to lack or absence of radioactive
substance (Fredriksson et al., 2015). Hence, it will be helpful in assessing the level of
stress suffered by Jon and accordingly the nurse can conduct stress-free therapy.
3. Coronary angiography- Coronary angiography is used as a physical assessment tool,
which is used to examine the inner part of the blood vessel in the heart. This
assessment tool detects the narrowing of artery due to accumulation of plaque or
cholesterol (Arbab & Fuster, 2016). As Jon was suffering from hypercholesterolemia,
this assessment will help the nurse to understand the severity of accumulation thereby
identifying the nursing intervention to help the patient recover from angina.
Q3) Discuss THREE nursing interventions (excluding pharmacological) you would initiate
and provide rationale as to how these would improve physiological outcomes of Jon’s chest
pain.
Jon was had continuous discomfort in chest, which is the major symptom of angina.
Nursing intervention is performed to manage the complexity of chest pain in the patient by
handling the duration, severity and frequency of pain. Hence, different nursing intervention is
performed to manage the acute chest pain in Jon as described below (Hylands, Duarte &
Raphael, 2017):
Condition Nursing intervention Rationale
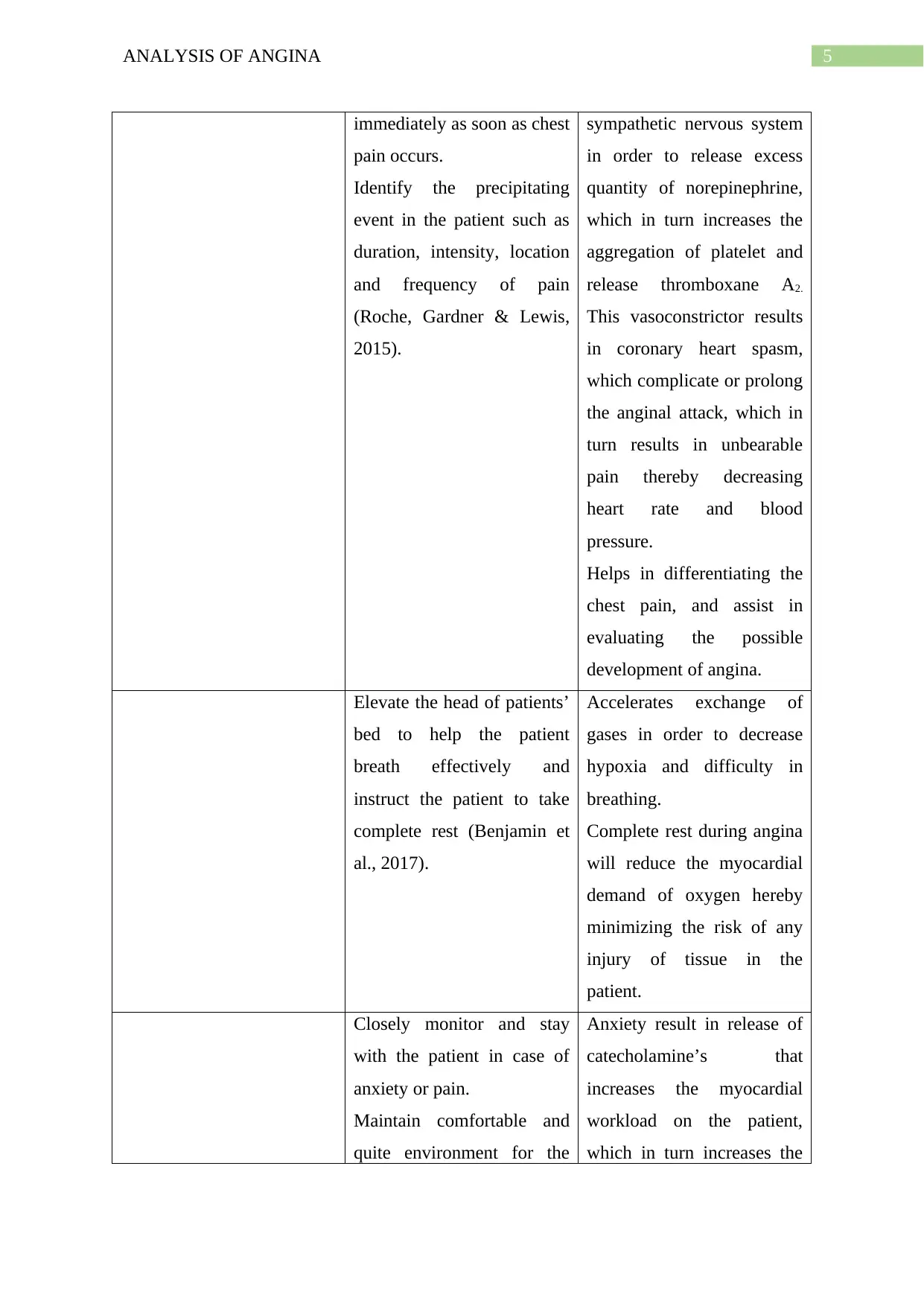
Chest pain Educate the patient to
inform the nurse
Reduced cardiac output and
pain might excite the
5ANALYSIS OF ANGINA
immediately as soon as chest
pain occurs.
Identify the precipitating
event in the patient such as
duration, intensity, location
and frequency of pain
(Roche, Gardner & Lewis,
2015).
sympathetic nervous system
in order to release excess
quantity of norepinephrine,
which in turn increases the
aggregation of platelet and
release thromboxane A2.
This vasoconstrictor results
in coronary heart spasm,
which complicate or prolong
the anginal attack, which in
turn results in unbearable
pain thereby decreasing
heart rate and blood
pressure.
Helps in differentiating the
chest pain, and assist in
evaluating the possible
development of angina.
Elevate the head of patients’
bed to help the patient
breath effectively and
instruct the patient to take
complete rest (Benjamin et
al., 2017).
Accelerates exchange of
gases in order to decrease
hypoxia and difficulty in
breathing.
Complete rest during angina
will reduce the myocardial
demand of oxygen hereby
minimizing the risk of any
injury of tissue in the
patient.
Closely monitor and stay
with the patient in case of
anxiety or pain.
Maintain comfortable and
quite environment for the
Anxiety result in release of
catecholamine’s that
increases the myocardial
workload on the patient,
which in turn increases the
immediately as soon as chest
pain occurs.
Identify the precipitating
event in the patient such as
duration, intensity, location
and frequency of pain
(Roche, Gardner & Lewis,
2015).
sympathetic nervous system
in order to release excess
quantity of norepinephrine,
which in turn increases the
aggregation of platelet and
release thromboxane A2.
This vasoconstrictor results
in coronary heart spasm,
which complicate or prolong
the anginal attack, which in
turn results in unbearable
pain thereby decreasing
heart rate and blood
pressure.
Helps in differentiating the
chest pain, and assist in
evaluating the possible
development of angina.
Elevate the head of patients’
bed to help the patient
breath effectively and
instruct the patient to take
complete rest (Benjamin et
al., 2017).
Accelerates exchange of
gases in order to decrease
hypoxia and difficulty in
breathing.
Complete rest during angina
will reduce the myocardial
demand of oxygen hereby
minimizing the risk of any
injury of tissue in the
patient.
Closely monitor and stay
with the patient in case of
anxiety or pain.
Maintain comfortable and
quite environment for the
Anxiety result in release of
catecholamine’s that
increases the myocardial
workload on the patient,
which in turn increases the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6ANALYSIS OF ANGINA
patient (Huffman, Adams &
Celano, 2018).
duration of ischemic pain.
Supervision of nurse will
help the patient to reduce
helplessness and fear.
Emotional or mental stress
or hypertension increases
the myocardial workload in
the patient.
Q4) Discuss the administration (including administration, benefits, risks and
contraindications) of sublingual Glyceryl Trinitrate for Jon’s pain. Include in your
explanation what education you need to provide to Jon on its administration.
Glyceryl trinitrate (GTN) is a medicine prescribed for the patient suffering from chest
pain linked to angina. For rapid relief, spray or tablet formulation of GTN is refereed as the
effect of medicine persists for approximately 30 minutes. The medicine can be consumed by
the patient while onset of chest pain or before any physical activity, which can lead to chest
pain (Wee, Burns & Bett, 2015). The doctor or nurse regarding the administration of the drug
should educate the patient properly. The side effect and health benefits of the drug must be
explained to the patient so that the patient has a clear idea regarding the usage of drug. The
doctor should conduct routine check-up sessions to be updated on the patient’s health and the
response of medicine towards well-being of the patient (Hauerslev et al., 2018).
Jon was recommended sublingual mode of administration of the drug. Sublingual route of
administration is recommended for instant relief to the patient suffering from anginal attack.
Sublingual mode of administration includes the use of either spray or tablets (Sani et al.,
2015). The patient was prescribed with sublingual glyceryl trinitrate spray. In this method,
glyceryl trinitrate is sprayed under the tongue of the patient as soon as pain develops. Initial
patient (Huffman, Adams &
Celano, 2018).
duration of ischemic pain.
Supervision of nurse will
help the patient to reduce
helplessness and fear.
Emotional or mental stress
or hypertension increases
the myocardial workload in
the patient.
Q4) Discuss the administration (including administration, benefits, risks and
contraindications) of sublingual Glyceryl Trinitrate for Jon’s pain. Include in your
explanation what education you need to provide to Jon on its administration.
Glyceryl trinitrate (GTN) is a medicine prescribed for the patient suffering from chest
pain linked to angina. For rapid relief, spray or tablet formulation of GTN is refereed as the
effect of medicine persists for approximately 30 minutes. The medicine can be consumed by
the patient while onset of chest pain or before any physical activity, which can lead to chest
pain (Wee, Burns & Bett, 2015). The doctor or nurse regarding the administration of the drug
should educate the patient properly. The side effect and health benefits of the drug must be
explained to the patient so that the patient has a clear idea regarding the usage of drug. The
doctor should conduct routine check-up sessions to be updated on the patient’s health and the
response of medicine towards well-being of the patient (Hauerslev et al., 2018).
Jon was recommended sublingual mode of administration of the drug. Sublingual route of
administration is recommended for instant relief to the patient suffering from anginal attack.
Sublingual mode of administration includes the use of either spray or tablets (Sani et al.,
2015). The patient was prescribed with sublingual glyceryl trinitrate spray. In this method,
glyceryl trinitrate is sprayed under the tongue of the patient as soon as pain develops. Initial
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

7ANALYSIS OF ANGINA
dose of the spray do not work effectively hence, the patient should again take two spray. The
pain is relieved mostly within a minute (Docherty, Jackson & Gardner, 2016).
The benefits of using sublingual glyceryl trinitrate are as follows (Corcoran et al., 2018):
Glyceryl trinitrate is converted into chemical known as nitric oxide, which is
present naturally in the body thus dilating and relaxing the artery.
It also helps to dilate the artery present in the heart thereby increasing the
oxygenated blood supply to the heart muscle.
Glyceryl trinitrate enhances the supply of oxygen in the heart.
Glyceryl trinitrate spray is used for preventing a predictable attack such as
emotional stress or physical activity.
The risk of using sublingual glyceryl trinitrate can be stated as the possible side effect
the medicine has on the patient. Side effect can be summarized in four categories namely
very common effect, little common effect, uncommon effect and rare effect (Bath et al.,
2016). The risk includes dizziness, headache, weakness, feeling sick, fainting, bradycardia
and tachycardia, skin allergy and tongue blistering.
The contradictions of the drug defines the situation in which the drug should never be
consumed, as it can be harmful for the patient. The condition include people with
hypotension, nitrate allergy, hypovolaemia, aortic stenosis, severe anaemia and cerebral
haemorrhage (Charlton & Thompson, 2018).
Q5) Report the major abnormal finding and apply your findings to Jon’s case. Explain why
this finding would need to be reported immediately to the Doctor.
From the Electro Cardiogram report of the patient, the major abnormal finding
reported was atrial fibrillation. This condition arises due to decreased blood flow in the heart,
which effects the heart rate of the patient thereby leading to atrial fibrillation. The irregular
dose of the spray do not work effectively hence, the patient should again take two spray. The
pain is relieved mostly within a minute (Docherty, Jackson & Gardner, 2016).
The benefits of using sublingual glyceryl trinitrate are as follows (Corcoran et al., 2018):
Glyceryl trinitrate is converted into chemical known as nitric oxide, which is
present naturally in the body thus dilating and relaxing the artery.
It also helps to dilate the artery present in the heart thereby increasing the
oxygenated blood supply to the heart muscle.
Glyceryl trinitrate enhances the supply of oxygen in the heart.
Glyceryl trinitrate spray is used for preventing a predictable attack such as
emotional stress or physical activity.
The risk of using sublingual glyceryl trinitrate can be stated as the possible side effect
the medicine has on the patient. Side effect can be summarized in four categories namely
very common effect, little common effect, uncommon effect and rare effect (Bath et al.,
2016). The risk includes dizziness, headache, weakness, feeling sick, fainting, bradycardia
and tachycardia, skin allergy and tongue blistering.
The contradictions of the drug defines the situation in which the drug should never be
consumed, as it can be harmful for the patient. The condition include people with
hypotension, nitrate allergy, hypovolaemia, aortic stenosis, severe anaemia and cerebral
haemorrhage (Charlton & Thompson, 2018).
Q5) Report the major abnormal finding and apply your findings to Jon’s case. Explain why
this finding would need to be reported immediately to the Doctor.
From the Electro Cardiogram report of the patient, the major abnormal finding
reported was atrial fibrillation. This condition arises due to decreased blood flow in the heart,
which effects the heart rate of the patient thereby leading to atrial fibrillation. The irregular
8ANALYSIS OF ANGINA
heart beat results in either discomfort or chest pain, which in turn creates a confusion in
angina and atrial fibrillation (Merriel, 2017). Jon was suffering from severe chest pain while
he was taking shower, which may be due to atrial fibrillation instead of angina pain. Hence,
to differentiate the cause of pain it was very important that the patient visit the doctor for
assessment. As atrial fibrillation can weaken the cardiac muscle, thereby making the heart
incapable to supply adequate amount of blood to fulfil the requirement of the body. Chances
of cardiac stroke is higher in the patient and can be only cured if proper medication is
provided to the patient (Kwon & Rosendorff, 2017). Since this health condition was
recognized in Jon’s ECG report, it was very important for him to visit the doctor and undergo
proper medication therapy in order to recover soon.
heart beat results in either discomfort or chest pain, which in turn creates a confusion in
angina and atrial fibrillation (Merriel, 2017). Jon was suffering from severe chest pain while
he was taking shower, which may be due to atrial fibrillation instead of angina pain. Hence,
to differentiate the cause of pain it was very important that the patient visit the doctor for
assessment. As atrial fibrillation can weaken the cardiac muscle, thereby making the heart
incapable to supply adequate amount of blood to fulfil the requirement of the body. Chances
of cardiac stroke is higher in the patient and can be only cured if proper medication is
provided to the patient (Kwon & Rosendorff, 2017). Since this health condition was
recognized in Jon’s ECG report, it was very important for him to visit the doctor and undergo
proper medication therapy in order to recover soon.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9ANALYSIS OF ANGINA
References
Abid, S., Shuaib, W., Ali, S., Evans, D. D., Khan, M. S., Edalat, F., & Khan, M. J. (2015).
Chest pain assessment and imaging practices for nurse practitioners in the emergency
department. Advanced Emergency Nursing Journal, 37(1), 12-22. doi:
10.1097/TME.0000000000000048
Arbab-Zadeh, A., & Fuster, V. (2016). The risk continuum of atherosclerosis and its
implications for defining CHD by coronary angiography. Journal of the American
College of Cardiology, 68(22), 2467-2478. DOI: 10.1016/j.jacc.2016.08.069
Bath, P. M., Woodhouse, L., Krishnan, K., Anderson, C., Berge, E., Ford, G. A & in Acute
Stroke Collaboration. (2016). Effect of treatment delay, stroke type, and thrombolysis
on the effect of glyceryl trinitrate, a nitric oxide donor, on outcome after acute stroke:
a systematic review and meta-analysis of individual patient from randomised trials.
Stroke research and treatment, 2016. http://dx.doi.org/10.1155/2016/9706720
Benjamin, E. J., Blaha, M. J., Chiuve, S. E., Cushman, M., Das, S. R., Deo, R., ... & Jiménez,
M. C. (2017). Heart disease and stroke statistics-2017 update: a report from the
American Heart Association. Circulation, 135(10), e146-e603. doi:
10.1161/CIR.0000000000000485
Charlton, M., & Thompson, J. P. (2018). Drugs acting on the heart: heart failure and coronary
insufficiency. Anaesthesia & Intensive Care Medicine.
https://doi.org/10.1016/j.mpaic.2018.04.006
Colquhoun, D., Freedman, B., Cross, D., Fitzgerald, B., Forge, B., Hare, D. L., ... & Zecchin,
R. (2015). Clinical exercise stress testing in adults (2014). Heart, Lung and
Circulation, 24(8), 831-837. https://doi.org/10.1016/j.hlc.2015.01.022
Corcoran, D., Young, R., Cialdella, P., McCartney, P., Bajrangee, A., Hennigan, B., ... &
Watkins, S. (2018). The effects of remote ischaemic preconditioning on coronary
References
Abid, S., Shuaib, W., Ali, S., Evans, D. D., Khan, M. S., Edalat, F., & Khan, M. J. (2015).
Chest pain assessment and imaging practices for nurse practitioners in the emergency
department. Advanced Emergency Nursing Journal, 37(1), 12-22. doi:
10.1097/TME.0000000000000048
Arbab-Zadeh, A., & Fuster, V. (2016). The risk continuum of atherosclerosis and its
implications for defining CHD by coronary angiography. Journal of the American
College of Cardiology, 68(22), 2467-2478. DOI: 10.1016/j.jacc.2016.08.069
Bath, P. M., Woodhouse, L., Krishnan, K., Anderson, C., Berge, E., Ford, G. A & in Acute
Stroke Collaboration. (2016). Effect of treatment delay, stroke type, and thrombolysis
on the effect of glyceryl trinitrate, a nitric oxide donor, on outcome after acute stroke:
a systematic review and meta-analysis of individual patient from randomised trials.
Stroke research and treatment, 2016. http://dx.doi.org/10.1155/2016/9706720
Benjamin, E. J., Blaha, M. J., Chiuve, S. E., Cushman, M., Das, S. R., Deo, R., ... & Jiménez,
M. C. (2017). Heart disease and stroke statistics-2017 update: a report from the
American Heart Association. Circulation, 135(10), e146-e603. doi:
10.1161/CIR.0000000000000485
Charlton, M., & Thompson, J. P. (2018). Drugs acting on the heart: heart failure and coronary
insufficiency. Anaesthesia & Intensive Care Medicine.
https://doi.org/10.1016/j.mpaic.2018.04.006
Colquhoun, D., Freedman, B., Cross, D., Fitzgerald, B., Forge, B., Hare, D. L., ... & Zecchin,
R. (2015). Clinical exercise stress testing in adults (2014). Heart, Lung and
Circulation, 24(8), 831-837. https://doi.org/10.1016/j.hlc.2015.01.022
Corcoran, D., Young, R., Cialdella, P., McCartney, P., Bajrangee, A., Hennigan, B., ... &
Watkins, S. (2018). The effects of remote ischaemic preconditioning on coronary
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10ANALYSIS OF ANGINA
artery function in patients with stable coronary artery disease. International journal of
cardiology, 252, 24-30. https://doi.org/10.1016/j.ijcard.2017.10.082
Denn, P., Noonan, B., & Condon, C. (2017). Typical stable angina in a nurse-led chest pain
assessment unit. British Journal of Cardiac Nursing, 12(2), 92-97.
https://doi.org/10.12968/bjca.2017.12.2.92
Docherty, K. F., Jackson, A. M., & Gardner, R. S. (2016). Diagnosis and pharmacological
management of stable angina. Prescriber, 27(5), 27-33.
https://doi.org/10.1002/psb.1459
Fredriksson-Larsson, U., Brink, E., Grankvist, G., Jonsdottir, I. H., & Alsen, P. (2015). The
single-item measure of stress symptoms after myocardial infarction and its association
with fatigue. Open Journal of Nursing, 5(04), 345. doi: 10.1.1.993.1378
Giannopoulos, A. A., Giannoglou, G. D., & Chatzizisis, Y. S. (2016). Pharmacological
approaches of refractory angina. Pharmacology & therapeutics, 163, 118-131.
https://doi.org/10.1016/j.pharmthera.2016.03.008
Hauerslev, M., Mørk, S. R., Pryds, K., Contractor, H., Hansen, J., Jespersen, N. R., ... &
Bøtker, H. E. (2018). Influence of long-term treatment with glyceryl trinitrate on
remote ischemic conditioning. American Journal of Physiology-Heart and
Circulatory Physiology. https://doi.org/10.1152/ajpheart.00114.2018
Healthdirect.gov.au. (2019). Angina. Retrieved from https://www.healthdirect.gov.au/angina
Healthywa.wa.gov.au. (2019). Angina. Retrieved from
https://www.healthywa.wa.gov.au/Articles/A_E/Angina
Huffman, J. C., Adams, C. N., & Celano, C. M. (2018). Collaborative care and related
interventions in patients with heart disease: An update and new directions.
Psychosomatics, 59(1), 1-18. https://doi.org/10.1016/j.psym.2017.09.003
artery function in patients with stable coronary artery disease. International journal of
cardiology, 252, 24-30. https://doi.org/10.1016/j.ijcard.2017.10.082
Denn, P., Noonan, B., & Condon, C. (2017). Typical stable angina in a nurse-led chest pain
assessment unit. British Journal of Cardiac Nursing, 12(2), 92-97.
https://doi.org/10.12968/bjca.2017.12.2.92
Docherty, K. F., Jackson, A. M., & Gardner, R. S. (2016). Diagnosis and pharmacological
management of stable angina. Prescriber, 27(5), 27-33.
https://doi.org/10.1002/psb.1459
Fredriksson-Larsson, U., Brink, E., Grankvist, G., Jonsdottir, I. H., & Alsen, P. (2015). The
single-item measure of stress symptoms after myocardial infarction and its association
with fatigue. Open Journal of Nursing, 5(04), 345. doi: 10.1.1.993.1378
Giannopoulos, A. A., Giannoglou, G. D., & Chatzizisis, Y. S. (2016). Pharmacological
approaches of refractory angina. Pharmacology & therapeutics, 163, 118-131.
https://doi.org/10.1016/j.pharmthera.2016.03.008
Hauerslev, M., Mørk, S. R., Pryds, K., Contractor, H., Hansen, J., Jespersen, N. R., ... &
Bøtker, H. E. (2018). Influence of long-term treatment with glyceryl trinitrate on
remote ischemic conditioning. American Journal of Physiology-Heart and
Circulatory Physiology. https://doi.org/10.1152/ajpheart.00114.2018
Healthdirect.gov.au. (2019). Angina. Retrieved from https://www.healthdirect.gov.au/angina
Healthywa.wa.gov.au. (2019). Angina. Retrieved from
https://www.healthywa.wa.gov.au/Articles/A_E/Angina
Huffman, J. C., Adams, C. N., & Celano, C. M. (2018). Collaborative care and related
interventions in patients with heart disease: An update and new directions.
Psychosomatics, 59(1), 1-18. https://doi.org/10.1016/j.psym.2017.09.003
11ANALYSIS OF ANGINA
Hylands-White, N., Duarte, R. V., & Raphael, J. H. (2017). An overview of treatment
approaches for chronic pain management. Rheumatology international, 37(1), 29-42.
https://doi.org/10.1007/s00296-016-3481-8
Iqbal, M. N., Ashraf, A., Muhammad, A., Alam, S., Xiao, S., Ali, S., & Irfan, M. (2016).
Prevalence of Angina Pectoris in relation to various risk factors. PSM Biological
Research, 1(1), 6-10. Retrieved from
https://journals.psmpublishers.org/index.php/biolres/article/view/14
Kloner, R. A., & Chaitman, B. (2017). Angina and its management. Journal of
cardiovascular pharmacology and therapeutics, 22(3), 199-209.
https://doi.org/10.1177/1074248416679733
Kwon, L., & Rosendorff, C. (2017). The Medical Treatment of Stable Angina. Chronic
Coronary Artery Disease: A Companion to Braunwald's Heart Disease, 280.
Retrieved from: https://books.google.co.in/books?
hl=en&lr=&id=fhXVDQAAQBAJ&oi=fnd&pg=PA280&dq=administration+of+glyc
eryl+trinitrate+in+angina+&ots=m8B2ZQMGhT&sig=Al7-
QMjpPDGJNJKt2ekSEp8qohU#v=onepage&q&f=false
Merriel, S. W. (2017). Management of angina in primary care. Nurse Prescribing, 15(10),
492-497. https://doi.org/10.12968/npre.2017.15.10.492
Ohman, E. M. (2016). Chronic stable angina. New England Journal of Medicine, 374(12),
1167-1176. DOI: 10.1056/NEJMcp1502240
Roche, T. E., Gardner, G., & Lewis, P. A. (2015). Effectiveness of an emergency nurse
practitioner service for adults presenting to rural hospitals with chest pain: protocol
for a multicentre, longitudinal nested cohort study. BMJ open, 5(2), e006997.
http://dx.doi.org/10.1136/bmjopen-2014-006997
Hylands-White, N., Duarte, R. V., & Raphael, J. H. (2017). An overview of treatment
approaches for chronic pain management. Rheumatology international, 37(1), 29-42.
https://doi.org/10.1007/s00296-016-3481-8
Iqbal, M. N., Ashraf, A., Muhammad, A., Alam, S., Xiao, S., Ali, S., & Irfan, M. (2016).
Prevalence of Angina Pectoris in relation to various risk factors. PSM Biological
Research, 1(1), 6-10. Retrieved from
https://journals.psmpublishers.org/index.php/biolres/article/view/14
Kloner, R. A., & Chaitman, B. (2017). Angina and its management. Journal of
cardiovascular pharmacology and therapeutics, 22(3), 199-209.
https://doi.org/10.1177/1074248416679733
Kwon, L., & Rosendorff, C. (2017). The Medical Treatment of Stable Angina. Chronic
Coronary Artery Disease: A Companion to Braunwald's Heart Disease, 280.
Retrieved from: https://books.google.co.in/books?
hl=en&lr=&id=fhXVDQAAQBAJ&oi=fnd&pg=PA280&dq=administration+of+glyc
eryl+trinitrate+in+angina+&ots=m8B2ZQMGhT&sig=Al7-
QMjpPDGJNJKt2ekSEp8qohU#v=onepage&q&f=false
Merriel, S. W. (2017). Management of angina in primary care. Nurse Prescribing, 15(10),
492-497. https://doi.org/10.12968/npre.2017.15.10.492
Ohman, E. M. (2016). Chronic stable angina. New England Journal of Medicine, 374(12),
1167-1176. DOI: 10.1056/NEJMcp1502240
Roche, T. E., Gardner, G., & Lewis, P. A. (2015). Effectiveness of an emergency nurse
practitioner service for adults presenting to rural hospitals with chest pain: protocol
for a multicentre, longitudinal nested cohort study. BMJ open, 5(2), e006997.
http://dx.doi.org/10.1136/bmjopen-2014-006997
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.