Asthma: Definition, Etiology, Pathogenesis, Signs and Symptoms, Interventions, and Nursing Implications
VerifiedAdded on 2023/06/04
|10
|2137
|423
AI Summary
This article discusses asthma, including its definition, etiology, pathogenesis, signs and symptoms, interventions, and nursing implications. It also mentions the role of genetic and environmental factors in asthma predisposing and allowing for progression of asthma.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: ASTHMA 1
Health Variations
Name
Institutional Affiliation
Health Variations
Name
Institutional Affiliation
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ASTHMA 2
Question 1
a) Definition and etiology
Asthma is a chronic airway disease characterized by airway hypersensitivity, reversible
airflow obstruction and variable airflow obstruction. Generally, the pathogenesis of asthma
involves genetic and environmental factors. Genetic factors include atopy, a positive family
history of asthma and polygenic intolerance. Others include gender and ethnicity (Ferreira, et al.,
2017). Environmental factors that can predispose one to asthma include outdoor pollutants like
pollen, smoke and exhaust fumes. Dietary factors can also contribute to the progression of
asthma. Dietary deficiency of vitamin C and foods rich in antioxidants have been shown to
enhance progression of asthma. Indoor pollutants comprise of house dust, ciggerate smoking and
smoke from firewood (Lambrecht & Hammad, 2015). Drugs like Non-steroidal anti-
inflammatory (NSAIDS) like aspirin and oral contraceptives also predisposes one to developing
asthma. Jackson Smith may have had a history of asthma in the family, which was triggered by
an allergen (Kumar, Abbas, & Aster, 2015). Both genetic and environmental factors play a role
in asthma predisposing and allowing for progression of asthma. The hall mark of the disease is
airway inflammation, bronchoconstriction, bronchial smooth muscle and mucous glands
hypertrophy (Wagner, 2014).
b) pathogenesis
Genetic predisposition to type 1 hypersensitivity reaction (atopy) has been attributed to
be the major etiologic evidence of asthma (Craft et al, 2015). After being exposed to an
offending stimuli, inflammation ensues. Major inflammatory cells are eosinophils and
neutrophils. In atopic asthma, TH2 production is excessive. It stimulates production of IL-4
Question 1
a) Definition and etiology
Asthma is a chronic airway disease characterized by airway hypersensitivity, reversible
airflow obstruction and variable airflow obstruction. Generally, the pathogenesis of asthma
involves genetic and environmental factors. Genetic factors include atopy, a positive family
history of asthma and polygenic intolerance. Others include gender and ethnicity (Ferreira, et al.,
2017). Environmental factors that can predispose one to asthma include outdoor pollutants like
pollen, smoke and exhaust fumes. Dietary factors can also contribute to the progression of
asthma. Dietary deficiency of vitamin C and foods rich in antioxidants have been shown to
enhance progression of asthma. Indoor pollutants comprise of house dust, ciggerate smoking and
smoke from firewood (Lambrecht & Hammad, 2015). Drugs like Non-steroidal anti-
inflammatory (NSAIDS) like aspirin and oral contraceptives also predisposes one to developing
asthma. Jackson Smith may have had a history of asthma in the family, which was triggered by
an allergen (Kumar, Abbas, & Aster, 2015). Both genetic and environmental factors play a role
in asthma predisposing and allowing for progression of asthma. The hall mark of the disease is
airway inflammation, bronchoconstriction, bronchial smooth muscle and mucous glands
hypertrophy (Wagner, 2014).
b) pathogenesis
Genetic predisposition to type 1 hypersensitivity reaction (atopy) has been attributed to
be the major etiologic evidence of asthma (Craft et al, 2015). After being exposed to an
offending stimuli, inflammation ensues. Major inflammatory cells are eosinophils and
neutrophils. In atopic asthma, TH2 production is excessive. It stimulates production of IL-4
ASTHMA 3
which then stimulates production of IgE. IgE production is also produced by B cells which is
activated by IL-13. IL-13 also stimulates mucous production. IL-5 activates eosinophils (Craft et
al, 2015). When IgE coats mast cells on exposure to allergen, degranulation occurs and an early
and late wave of reaction occurs (Magge, Pascanu, & Salerno, 2017). Early wave is
predominantly characterized by bronchoconstriction, increased production of mucus and variable
vasodilation. Constriction of bronchial smooth muscles is triggered by direct stimulation of vagal
receptors. The late phase has inflammation which leads to activation of eosinophils, neutrophils
and T cells. Inflammatory reaction is amplified by continues chemotaxis and activation of
eosinophils due to chemokines released by TH2 cells (Kumar, Abbas & Aster, 2013). Repeated
exposure to allergen causes hypertrophy of bronchial smooth muscles and mucus glands.
Signs and symptoms
Jackson Smith presents with Acute Severe Asthma (ASA). ASA is an acute
excercubation of asthma that does not respond to standard treatment with bronchodilators or
corticosteroids, (Kumar, Abbas & Aster, 2013). Severe dyspnea that Jackson presented with is
due to airway hyperactivity to an allergen. The bronchial smooth muscles undergo inflammation
and increased mucus production that limit amount of air entry and outflow. Airway remodeling
is also a contributing factor. Due to repeated exposure to allergen, the smooth muscles and
mucous glands undergo hypertrophy (therefore narrowing). This makes the patient have and
increased respiratory effort due to buildup of carbon dioxide (Aitken, Marshall & Chaboyer,
2015). Carbon dioxide (CO2) sensitizes the respiratory center to increase respiratory rate (as
Jackson Smith’s) so that excess CO2 can be expelled. As a result, saturation at room air was to be
low, as it was 90% in Smith’s case.
which then stimulates production of IgE. IgE production is also produced by B cells which is
activated by IL-13. IL-13 also stimulates mucous production. IL-5 activates eosinophils (Craft et
al, 2015). When IgE coats mast cells on exposure to allergen, degranulation occurs and an early
and late wave of reaction occurs (Magge, Pascanu, & Salerno, 2017). Early wave is
predominantly characterized by bronchoconstriction, increased production of mucus and variable
vasodilation. Constriction of bronchial smooth muscles is triggered by direct stimulation of vagal
receptors. The late phase has inflammation which leads to activation of eosinophils, neutrophils
and T cells. Inflammatory reaction is amplified by continues chemotaxis and activation of
eosinophils due to chemokines released by TH2 cells (Kumar, Abbas & Aster, 2013). Repeated
exposure to allergen causes hypertrophy of bronchial smooth muscles and mucus glands.
Signs and symptoms
Jackson Smith presents with Acute Severe Asthma (ASA). ASA is an acute
excercubation of asthma that does not respond to standard treatment with bronchodilators or
corticosteroids, (Kumar, Abbas & Aster, 2013). Severe dyspnea that Jackson presented with is
due to airway hyperactivity to an allergen. The bronchial smooth muscles undergo inflammation
and increased mucus production that limit amount of air entry and outflow. Airway remodeling
is also a contributing factor. Due to repeated exposure to allergen, the smooth muscles and
mucous glands undergo hypertrophy (therefore narrowing). This makes the patient have and
increased respiratory effort due to buildup of carbon dioxide (Aitken, Marshall & Chaboyer,
2015). Carbon dioxide (CO2) sensitizes the respiratory center to increase respiratory rate (as
Jackson Smith’s) so that excess CO2 can be expelled. As a result, saturation at room air was to be
low, as it was 90% in Smith’s case.
ASTHMA 4
The body also responds in a bid to compensate for inadequate oxygen delivery in tissues
by increasing the heart rate and blood pressure, (Craft et al, 2015). In asthma attack, there is
inadequate oxygen delivery to tissues. This means that blood has to be redirected to vital organs
like brain so that adequate oxygen is supplied. As a physiological compensatory mechanism,
Smith’s blood pressure and pulse rate were increased so that more oxygen can be delivered in
tissues per unit time. During physical examination, auscultation of Smith’s lung field revealed
diminished breath sounds and widespread wheeze. The breath sounds are reduced because of
narrowing of bronchi thus there is limited air entry and outflow (Pijnenburg, et al., 2015).
Wheeze is explained by air turbulent as it rushes in the narrowed lumen of the bronchi. Chest X-
ray showed hyper inflated lungs due to buildup of air since there is limited outflow.
Blood gas analysis done on Smith showed deranged values. He has a renal compensation
of respiratory acidosis as evidenced by high PaCO2 of 50 mmHg (Normal is 35-45 mmHg in
arterial blood) (Reddel, et al., 2015). This shows that Smith had been in respiratory distress for a
long time. In asthma attack, there is inadequate exhalation of CO2 therefore it accumulates in the
lungs. Respiratory acidosis occurs when excess CO2 dissolves in blood to form weak carbonic
acid that further degrades to hydrogen ions as shown by Magge, Pascanu & Salerno, (2017).
Excess hydrogen ions have to be buffered by bicarbonate ions. The kidneys increases absorption
of hydrogen ions to buffer the low pH. In an acute state, the patient hyperventilates to expel
excess carbon dioxide in the system.
Question 2
The two high priority interventions by the nurse to Smith’s problem is administration of a
short acting bronchodilator like salbutamol and oxygen therapy. This is after assessing the
severity of the asthma attack (National Asthma Council Australia, 2017).
The body also responds in a bid to compensate for inadequate oxygen delivery in tissues
by increasing the heart rate and blood pressure, (Craft et al, 2015). In asthma attack, there is
inadequate oxygen delivery to tissues. This means that blood has to be redirected to vital organs
like brain so that adequate oxygen is supplied. As a physiological compensatory mechanism,
Smith’s blood pressure and pulse rate were increased so that more oxygen can be delivered in
tissues per unit time. During physical examination, auscultation of Smith’s lung field revealed
diminished breath sounds and widespread wheeze. The breath sounds are reduced because of
narrowing of bronchi thus there is limited air entry and outflow (Pijnenburg, et al., 2015).
Wheeze is explained by air turbulent as it rushes in the narrowed lumen of the bronchi. Chest X-
ray showed hyper inflated lungs due to buildup of air since there is limited outflow.
Blood gas analysis done on Smith showed deranged values. He has a renal compensation
of respiratory acidosis as evidenced by high PaCO2 of 50 mmHg (Normal is 35-45 mmHg in
arterial blood) (Reddel, et al., 2015). This shows that Smith had been in respiratory distress for a
long time. In asthma attack, there is inadequate exhalation of CO2 therefore it accumulates in the
lungs. Respiratory acidosis occurs when excess CO2 dissolves in blood to form weak carbonic
acid that further degrades to hydrogen ions as shown by Magge, Pascanu & Salerno, (2017).
Excess hydrogen ions have to be buffered by bicarbonate ions. The kidneys increases absorption
of hydrogen ions to buffer the low pH. In an acute state, the patient hyperventilates to expel
excess carbon dioxide in the system.
Question 2
The two high priority interventions by the nurse to Smith’s problem is administration of a
short acting bronchodilator like salbutamol and oxygen therapy. This is after assessing the
severity of the asthma attack (National Asthma Council Australia, 2017).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ASTHMA 5
Bronchodilator therapy is provided by giving Smith 12 puffs of salbutamol (100
micrograms per actuation) using a pressurized metered dose inhaler (pMDI) plus a spacer
(Pijnenburg, et al., 2015). If the patient cannot breathe, an intermittent nebulizer can be used,
giving 5 mg salbutamol. Oxygen therapy via a venture system should be given, titrating to target
a saturation of above 94% for Smith (National Asthma Council Australia, 2017).
The nurse should the re-assess the severity and if Smith’s condition has improved, he can
be transferred to asthma clinic. If there is no improvement, bronchodilator therapy is continued.
A repeat dose every 20 minutes for first one hour, totaling to 3 doses or as sooner as needed
(Magge, Pascanu, & Salerno, 2017). If the response is still poor, ipratropium bromide is added, 8
puffs via pMDI or 500 mcg nebule added to salbutamol, (National Asthma Council Australia,
2017). Systemic corticosteroids (oral prednisolone 37.5-50 mg for 5-10 days or IV
hydrocortisone 100 mg every 6 hours) should also be added to slow down inflammation of
bronchial muscles. Systemic corticosteroids should be administered within the first hour of
treatment (Aitken, Marshall, & Chaboyer, 2015).
Re assessment and spirometry can be done if patient is able to. If no improvement is
recorded, smith should be admitted to hospital for continued bronchodilator, oxygen support and
steroid treatment (Craft, et al., 2015).
Question 3
a) Mode of action of drugs
Salbutamol is a short acting beta 2 -adrenergic receptor stimulant (Katzung, 2006). After
stimulating the beta 2 adrenergic receptors, G-protein is stimulated and adenylyl cyclase
Bronchodilator therapy is provided by giving Smith 12 puffs of salbutamol (100
micrograms per actuation) using a pressurized metered dose inhaler (pMDI) plus a spacer
(Pijnenburg, et al., 2015). If the patient cannot breathe, an intermittent nebulizer can be used,
giving 5 mg salbutamol. Oxygen therapy via a venture system should be given, titrating to target
a saturation of above 94% for Smith (National Asthma Council Australia, 2017).
The nurse should the re-assess the severity and if Smith’s condition has improved, he can
be transferred to asthma clinic. If there is no improvement, bronchodilator therapy is continued.
A repeat dose every 20 minutes for first one hour, totaling to 3 doses or as sooner as needed
(Magge, Pascanu, & Salerno, 2017). If the response is still poor, ipratropium bromide is added, 8
puffs via pMDI or 500 mcg nebule added to salbutamol, (National Asthma Council Australia,
2017). Systemic corticosteroids (oral prednisolone 37.5-50 mg for 5-10 days or IV
hydrocortisone 100 mg every 6 hours) should also be added to slow down inflammation of
bronchial muscles. Systemic corticosteroids should be administered within the first hour of
treatment (Aitken, Marshall, & Chaboyer, 2015).
Re assessment and spirometry can be done if patient is able to. If no improvement is
recorded, smith should be admitted to hospital for continued bronchodilator, oxygen support and
steroid treatment (Craft, et al., 2015).
Question 3
a) Mode of action of drugs
Salbutamol is a short acting beta 2 -adrenergic receptor stimulant (Katzung, 2006). After
stimulating the beta 2 adrenergic receptors, G-protein is stimulated and adenylyl cyclase
ASTHMA 6
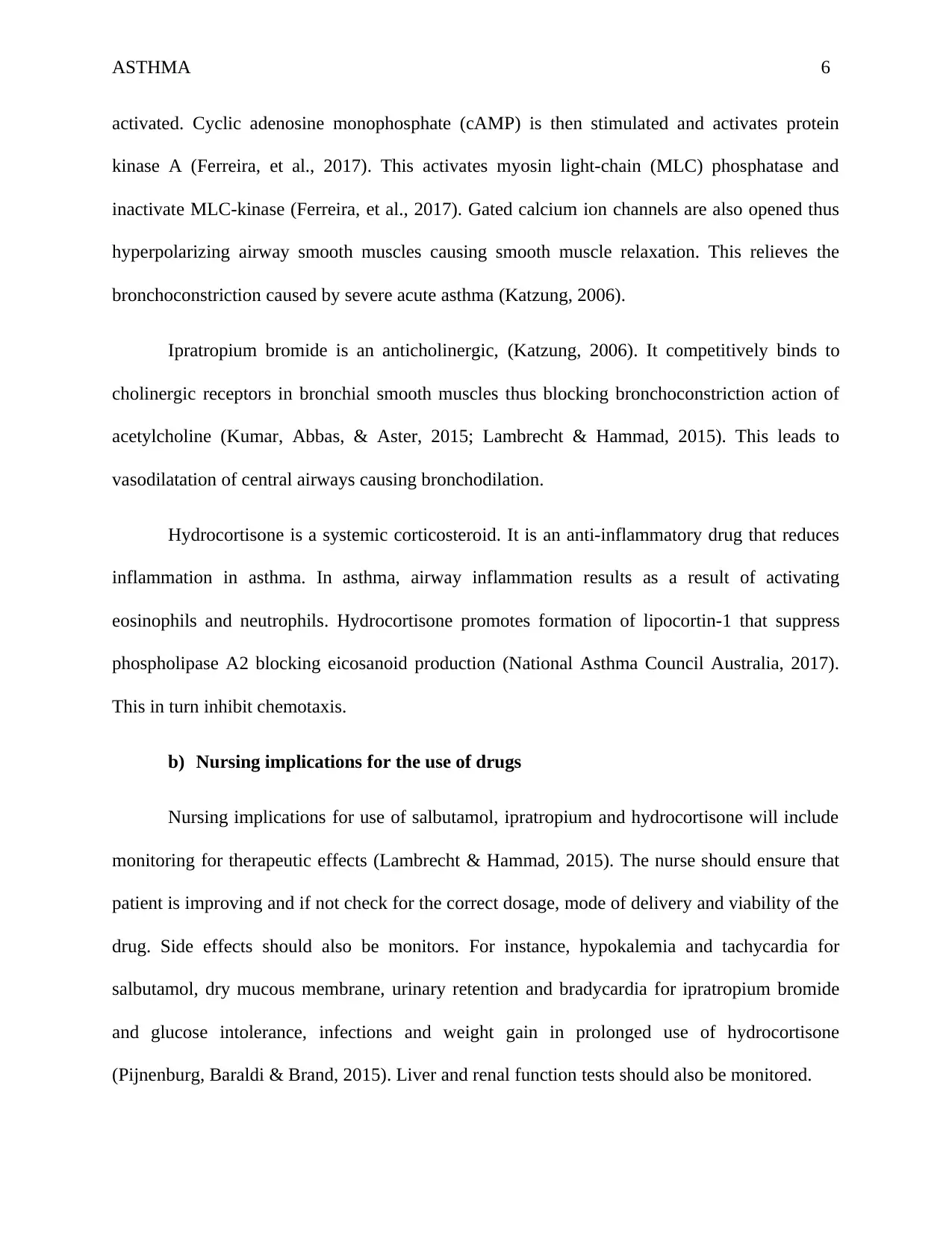
activated. Cyclic adenosine monophosphate (cAMP) is then stimulated and activates protein
kinase A (Ferreira, et al., 2017). This activates myosin light-chain (MLC) phosphatase and
inactivate MLC-kinase (Ferreira, et al., 2017). Gated calcium ion channels are also opened thus
hyperpolarizing airway smooth muscles causing smooth muscle relaxation. This relieves the
bronchoconstriction caused by severe acute asthma (Katzung, 2006).
Ipratropium bromide is an anticholinergic, (Katzung, 2006). It competitively binds to
cholinergic receptors in bronchial smooth muscles thus blocking bronchoconstriction action of
acetylcholine (Kumar, Abbas, & Aster, 2015; Lambrecht & Hammad, 2015). This leads to
vasodilatation of central airways causing bronchodilation.
Hydrocortisone is a systemic corticosteroid. It is an anti-inflammatory drug that reduces
inflammation in asthma. In asthma, airway inflammation results as a result of activating
eosinophils and neutrophils. Hydrocortisone promotes formation of lipocortin-1 that suppress
phospholipase A2 blocking eicosanoid production (National Asthma Council Australia, 2017).
This in turn inhibit chemotaxis.
b) Nursing implications for the use of drugs
Nursing implications for use of salbutamol, ipratropium and hydrocortisone will include
monitoring for therapeutic effects (Lambrecht & Hammad, 2015). The nurse should ensure that
patient is improving and if not check for the correct dosage, mode of delivery and viability of the
drug. Side effects should also be monitors. For instance, hypokalemia and tachycardia for
salbutamol, dry mucous membrane, urinary retention and bradycardia for ipratropium bromide
and glucose intolerance, infections and weight gain in prolonged use of hydrocortisone
(Pijnenburg, Baraldi & Brand, 2015). Liver and renal function tests should also be monitored.
activated. Cyclic adenosine monophosphate (cAMP) is then stimulated and activates protein
kinase A (Ferreira, et al., 2017). This activates myosin light-chain (MLC) phosphatase and
inactivate MLC-kinase (Ferreira, et al., 2017). Gated calcium ion channels are also opened thus
hyperpolarizing airway smooth muscles causing smooth muscle relaxation. This relieves the
bronchoconstriction caused by severe acute asthma (Katzung, 2006).
Ipratropium bromide is an anticholinergic, (Katzung, 2006). It competitively binds to
cholinergic receptors in bronchial smooth muscles thus blocking bronchoconstriction action of
acetylcholine (Kumar, Abbas, & Aster, 2015; Lambrecht & Hammad, 2015). This leads to
vasodilatation of central airways causing bronchodilation.
Hydrocortisone is a systemic corticosteroid. It is an anti-inflammatory drug that reduces
inflammation in asthma. In asthma, airway inflammation results as a result of activating
eosinophils and neutrophils. Hydrocortisone promotes formation of lipocortin-1 that suppress
phospholipase A2 blocking eicosanoid production (National Asthma Council Australia, 2017).
This in turn inhibit chemotaxis.
b) Nursing implications for the use of drugs
Nursing implications for use of salbutamol, ipratropium and hydrocortisone will include
monitoring for therapeutic effects (Lambrecht & Hammad, 2015). The nurse should ensure that
patient is improving and if not check for the correct dosage, mode of delivery and viability of the
drug. Side effects should also be monitors. For instance, hypokalemia and tachycardia for
salbutamol, dry mucous membrane, urinary retention and bradycardia for ipratropium bromide
and glucose intolerance, infections and weight gain in prolonged use of hydrocortisone
(Pijnenburg, Baraldi & Brand, 2015). Liver and renal function tests should also be monitored.
ASTHMA 7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ASTHMA 8
References
Aitken, L., Marshall, A. & Chaboyer, W. (2015). ACCCN’s critical care nursing (3rd ed.).
Chatswood, NSW: Elsevier Australia. Chapter 10.
Craft, J.A., Gordon, C.J., Huether, S.E., McCance, K.L., Brashers, V.L. & Rote, N.E. (2015).
Understanding pathophysiology – ANZ adaptation (2nd ed.). Chatswood, NSW: Elsevier
Australia. Chapter 24 & 25.
Ferreira, M. A., Jansen, R., Willemsen, G., Penninx, B., Bain, L. M., Vicente, C. T., & Baltic, S.
(2017). Gene-based analysis of regulatory variants identifies 4 putative novel asthma risk
genes related to nucleotide synthesis and signaling. Journal of Allergy and Clinical
Immunology, 139(4), 1148-1157.
Kumar, V., Abbas, A., & Aster, J. (2013). Robbins Basic Pathology (9th ed., pp. 468-470).
Canada: Elsevier Saunders.
Lambrecht, B. N., & Hammad, H. (2015). The immunology of asthma. Nature immunology,
16(1), 45.
Magge, A., Pascanu, R., & Salerno, E. (2017). C58 CRITICAL CARE CASE REPORTS:
NOTABLE CAUSES AND COMPLICATIONS IN ACUTE RESPIRATORY
FAILURE: Extracorporeal Membrane Oxygenation in Patients with Acute Severe
Asthma. American Journal of Respiratory and Critical Care Medicine, 195.
National Asthma Council Australia. (2017) Australian Asthma Handbook – Quick Reference
Guide, Version 1.3. National Asthma Council Australia, Melbourne. Available from:
http://www.asthmahandbook.org.au
References
Aitken, L., Marshall, A. & Chaboyer, W. (2015). ACCCN’s critical care nursing (3rd ed.).
Chatswood, NSW: Elsevier Australia. Chapter 10.
Craft, J.A., Gordon, C.J., Huether, S.E., McCance, K.L., Brashers, V.L. & Rote, N.E. (2015).
Understanding pathophysiology – ANZ adaptation (2nd ed.). Chatswood, NSW: Elsevier
Australia. Chapter 24 & 25.
Ferreira, M. A., Jansen, R., Willemsen, G., Penninx, B., Bain, L. M., Vicente, C. T., & Baltic, S.
(2017). Gene-based analysis of regulatory variants identifies 4 putative novel asthma risk
genes related to nucleotide synthesis and signaling. Journal of Allergy and Clinical
Immunology, 139(4), 1148-1157.
Kumar, V., Abbas, A., & Aster, J. (2013). Robbins Basic Pathology (9th ed., pp. 468-470).
Canada: Elsevier Saunders.
Lambrecht, B. N., & Hammad, H. (2015). The immunology of asthma. Nature immunology,
16(1), 45.
Magge, A., Pascanu, R., & Salerno, E. (2017). C58 CRITICAL CARE CASE REPORTS:
NOTABLE CAUSES AND COMPLICATIONS IN ACUTE RESPIRATORY
FAILURE: Extracorporeal Membrane Oxygenation in Patients with Acute Severe
Asthma. American Journal of Respiratory and Critical Care Medicine, 195.
National Asthma Council Australia. (2017) Australian Asthma Handbook – Quick Reference
Guide, Version 1.3. National Asthma Council Australia, Melbourne. Available from:
http://www.asthmahandbook.org.au
ASTHMA 9
Network, G. A. (2014). The global asthma report 2014. Auckland, New Zealand, 769.
Pijnenburg, M. W., Baraldi, E., Brand, P. L., Carlsen, K. H., Eber, E., Frischer, T., ... &
Mantzouranis, E. (2015). Monitoring asthma in children. European respiratory journal,
45(4), 906-925.
Reddel, H. K., Bateman, E. D., Becker, A., Boulet, L. P., Cruz, A. A., Drazen, J. M., ... &
Lemanske, R. F. (2015). A summary of the new GINA strategy: a roadmap to asthma
control. European Respiratory Journal, 46(3), 622-639.
Wagner, K.D. (2014). High acuity nursing (6th ed.). Upper Saddler River, New Jersey: Pearson.
Chapter13.
Network, G. A. (2014). The global asthma report 2014. Auckland, New Zealand, 769.
Pijnenburg, M. W., Baraldi, E., Brand, P. L., Carlsen, K. H., Eber, E., Frischer, T., ... &
Mantzouranis, E. (2015). Monitoring asthma in children. European respiratory journal,
45(4), 906-925.
Reddel, H. K., Bateman, E. D., Becker, A., Boulet, L. P., Cruz, A. A., Drazen, J. M., ... &
Lemanske, R. F. (2015). A summary of the new GINA strategy: a roadmap to asthma
control. European Respiratory Journal, 46(3), 622-639.
Wagner, K.D. (2014). High acuity nursing (6th ed.). Upper Saddler River, New Jersey: Pearson.
Chapter13.

ASTHMA 10
Concept map
Concept map
1 out of 10
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.