Case Study Analysis of Asthma
VerifiedAdded on 2022/08/26
|11
|2258
|16
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: CASE STUDY ANALYSIS
CASE STUDY ANALYSIS
Name of the student
Name of the university
Author’s name
CASE STUDY ANALYSIS
Name of the student
Name of the university
Author’s name
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CASE STUDY ANALYSIS
Introduction
Asthma is characterised by the function of airways in combination with airway
hyperresponsiveness (AHR) and inflammation. Asthma is a reversible airflow barrier. More than
300 million people in the world suffer from the disease, with about 250,000 deaths annually. The
mortality of asthma has decreased over the last few decades since the inhaled corticosteroid
became the main asthma treatment agent. In the past half decades, over conjunction with
urbanization, respiratory conditions such as asthma have dramatically risen. By contrast to other
age categories, children have the highest proportion of asthma. Therefore, by 2025 the number of
patients is expected to grow by over 100 million (Kudo, Ishigatsubo & Aoki, 2013). In this
paper, the pathophysiology of childhood Asthma and its effective management will be discussed
with the help of a case study given.
Discussion
Part-A
Pathophysiology of Asthma:
Asthma is referred to as a chronic inflammatory disorder of the airways. It is a pulmonary
condition characterised with chronic inflammation of the respiratory tubes, respiratory smooth
muscle tightening and an episode of bronchoconstriction (Félix et al., 2020). Inflamed airways
respond to environmental triggers including smoke, dust, or pollen throughout an asthma
episode. The airways are narrowing and producing excess mucus, making breathing difficult.
Essentially, asthma in the bronchial airways is the result of an immune response. Asthma patients
Introduction
Asthma is characterised by the function of airways in combination with airway
hyperresponsiveness (AHR) and inflammation. Asthma is a reversible airflow barrier. More than
300 million people in the world suffer from the disease, with about 250,000 deaths annually. The
mortality of asthma has decreased over the last few decades since the inhaled corticosteroid
became the main asthma treatment agent. In the past half decades, over conjunction with
urbanization, respiratory conditions such as asthma have dramatically risen. By contrast to other
age categories, children have the highest proportion of asthma. Therefore, by 2025 the number of
patients is expected to grow by over 100 million (Kudo, Ishigatsubo & Aoki, 2013). In this
paper, the pathophysiology of childhood Asthma and its effective management will be discussed
with the help of a case study given.
Discussion
Part-A
Pathophysiology of Asthma:
Asthma is referred to as a chronic inflammatory disorder of the airways. It is a pulmonary
condition characterised with chronic inflammation of the respiratory tubes, respiratory smooth
muscle tightening and an episode of bronchoconstriction (Félix et al., 2020). Inflamed airways
respond to environmental triggers including smoke, dust, or pollen throughout an asthma
episode. The airways are narrowing and producing excess mucus, making breathing difficult.
Essentially, asthma in the bronchial airways is the result of an immune response. Asthma patients
CASE STUDY ANALYSIS
' airways are "hypersensitive" to some triggers, also referred to as stimuli. Typically it is graded
as type I hype (Félix et al., 2020).
The most commonly understood causative factors are the pathways causing allergic
asthma, i.e., immune response to inhaled allergens. A variety of cell called antigen-prone cells or
APCs is absorbed in both individuals with asthma as well as in people who are free from the
disorder (Herzog & Cunningham‐Rundles, 2011). Inhaled allergens are present to the inner
airways these other immune cells in most individuals search and usually ignore allergens in the
other immune (TH0 cells). However, for reasons which are not well-comprehended, these cells
in asthma patients transform into a different type of cell (TH2). A potential reason may be that
Interleukin-4 is released to Mast cells which induce the differentiation between Th2 cells of
naive T support cells (Th0 cells) (Kudo, Ishigatsubo & Aoki, 2013).
Asthma in children can trigger troublesome everyday symptoms, interfering with
exercise, playing, school and sleep. Unmanaged asthma can lead to dangerous attacks on asthma
in some children. Common signs and symptoms for childhood asthma include frequent coughing
that gets worse when the child suffers from a viral infection, whistling or sound while breathing
out, shortness of breath or chest congestion or tightness which were evident in Zachy.
Part- B
Prioritised care plan for Zachy:
1. An urgent and accurate assessment of his severity by assessing his vitals. Focused physical
evaluation to measure the functional extent of the airway obstruction, to monitor the function of
accessory muscles, the air intake in both the lungs and wheezing, the alertness, speech and
' airways are "hypersensitive" to some triggers, also referred to as stimuli. Typically it is graded
as type I hype (Félix et al., 2020).
The most commonly understood causative factors are the pathways causing allergic
asthma, i.e., immune response to inhaled allergens. A variety of cell called antigen-prone cells or
APCs is absorbed in both individuals with asthma as well as in people who are free from the
disorder (Herzog & Cunningham‐Rundles, 2011). Inhaled allergens are present to the inner
airways these other immune cells in most individuals search and usually ignore allergens in the
other immune (TH0 cells). However, for reasons which are not well-comprehended, these cells
in asthma patients transform into a different type of cell (TH2). A potential reason may be that
Interleukin-4 is released to Mast cells which induce the differentiation between Th2 cells of
naive T support cells (Th0 cells) (Kudo, Ishigatsubo & Aoki, 2013).
Asthma in children can trigger troublesome everyday symptoms, interfering with
exercise, playing, school and sleep. Unmanaged asthma can lead to dangerous attacks on asthma
in some children. Common signs and symptoms for childhood asthma include frequent coughing
that gets worse when the child suffers from a viral infection, whistling or sound while breathing
out, shortness of breath or chest congestion or tightness which were evident in Zachy.
Part- B
Prioritised care plan for Zachy:
1. An urgent and accurate assessment of his severity by assessing his vitals. Focused physical
evaluation to measure the functional extent of the airway obstruction, to monitor the function of
accessory muscles, the air intake in both the lungs and wheezing, the alertness, speech and
CASE STUDY ANALYSIS
activity levels (Ortiz-Alvarez, Mikrogianakis, Canadian Paediatric Society & Acute Care
Committee, 2012).
2. Medical intervention to alleviate respiratory distress and enhance oxygenation immediately
and successfully either with the help of some medications or through oxygen therapy.
3. A proper treatment and monitoring during emergency management.
4. Proper follow up.
5. Involvement of a multidisciplinary team to access Zachy’s condition and implement
intervention strategies from every aspect.
Nursing Care plan for Zachy:
Goal Intervention Rationale Expected
outcome
Family coping/ Patient
education
It is important to listen to
and address the family’s
concern about the
management of asthma so
that the parents comply
with the care
recommended for the
child.
The parents
concern are
different to that of
the nurse. They
might not know
about the
appropriate dose
recommended to
alleviate asthma
symptoms. Thus, it
The parents
will show a
greater
compliance to
the treatment
approach
recommended
that will
eventually
increase health
activity levels (Ortiz-Alvarez, Mikrogianakis, Canadian Paediatric Society & Acute Care
Committee, 2012).
2. Medical intervention to alleviate respiratory distress and enhance oxygenation immediately
and successfully either with the help of some medications or through oxygen therapy.
3. A proper treatment and monitoring during emergency management.
4. Proper follow up.
5. Involvement of a multidisciplinary team to access Zachy’s condition and implement
intervention strategies from every aspect.
Nursing Care plan for Zachy:
Goal Intervention Rationale Expected
outcome
Family coping/ Patient
education
It is important to listen to
and address the family’s
concern about the
management of asthma so
that the parents comply
with the care
recommended for the
child.
The parents
concern are
different to that of
the nurse. They
might not know
about the
appropriate dose
recommended to
alleviate asthma
symptoms. Thus, it
The parents
will show a
greater
compliance to
the treatment
approach
recommended
that will
eventually
increase health
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CASE STUDY ANALYSIS
The parents must be made
aware about the treatment
approaches or options
available for the child and
the assessments to
diagnose the child’s
condition.
is important to
include them in the
care plan and
educate them to
increase the child’s
health outcome.
outcome of the
child and
prevent risk of
further acute
conditions
such as asthma
attack.
Ineffective breathing
pattern in relation to
chest wall distention
and fatigue because of
increased work of rate
or pattern of breath.
Monitoring frequency and
depth and rhythm of
breathing.
Positioning in Semi-
Fowler position to enable
expansion of the lungs
since gravity pulls the
diaphragm towards down
that subsequently allows
for ventilation and
expansion (Chanif, &
Prastika, 2019).
Zachy
demonstrates
coughing and a
clear sound of
breath. He was also
having expiratory
wheeze and
prolonged
expiration.
Zachy’s
breathing
pattern will be
improved.
Activity intolerance Response of breathing
during activity will be
monitored.
Abnormal response in
It is important to
assess the changes
in vital signs and
temperature
He will be
relieved from
shortness of
breath and
The parents must be made
aware about the treatment
approaches or options
available for the child and
the assessments to
diagnose the child’s
condition.
is important to
include them in the
care plan and
educate them to
increase the child’s
health outcome.
outcome of the
child and
prevent risk of
further acute
conditions
such as asthma
attack.
Ineffective breathing
pattern in relation to
chest wall distention
and fatigue because of
increased work of rate
or pattern of breath.
Monitoring frequency and
depth and rhythm of
breathing.
Positioning in Semi-
Fowler position to enable
expansion of the lungs
since gravity pulls the
diaphragm towards down
that subsequently allows
for ventilation and
expansion (Chanif, &
Prastika, 2019).
Zachy
demonstrates
coughing and a
clear sound of
breath. He was also
having expiratory
wheeze and
prolonged
expiration.
Zachy’s
breathing
pattern will be
improved.
Activity intolerance Response of breathing
during activity will be
monitored.
Abnormal response in
It is important to
assess the changes
in vital signs and
temperature
He will be
relieved from
shortness of
breath and
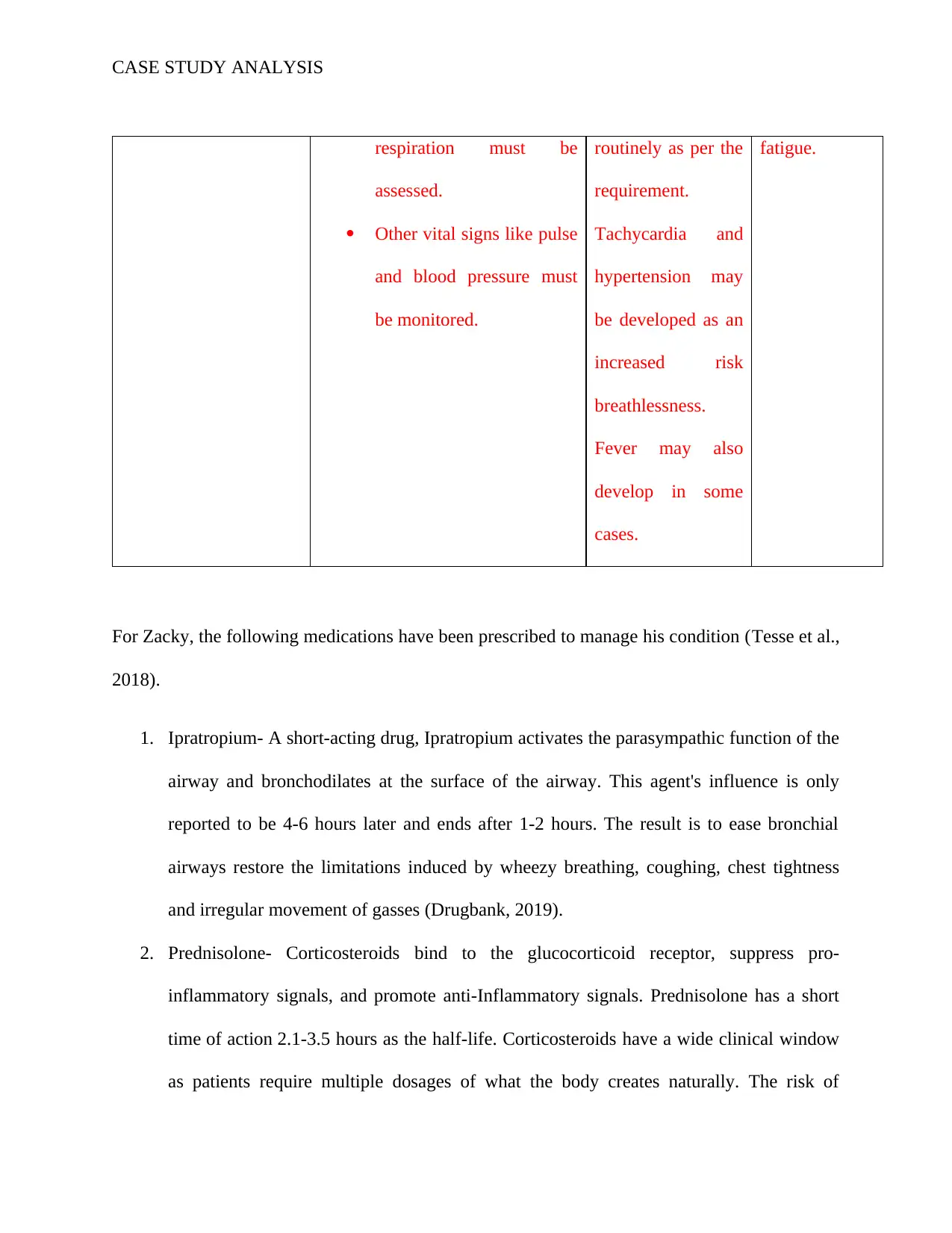
CASE STUDY ANALYSIS
respiration must be
assessed.
Other vital signs like pulse
and blood pressure must
be monitored.
routinely as per the
requirement.
Tachycardia and
hypertension may
be developed as an
increased risk
breathlessness.
Fever may also
develop in some
cases.
fatigue.
For Zacky, the following medications have been prescribed to manage his condition (Tesse et al.,
2018).
1. Ipratropium- A short-acting drug, Ipratropium activates the parasympathic function of the
airway and bronchodilates at the surface of the airway. This agent's influence is only
reported to be 4-6 hours later and ends after 1-2 hours. The result is to ease bronchial
airways restore the limitations induced by wheezy breathing, coughing, chest tightness
and irregular movement of gasses (Drugbank, 2019).
2. Prednisolone- Corticosteroids bind to the glucocorticoid receptor, suppress pro-
inflammatory signals, and promote anti-Inflammatory signals. Prednisolone has a short
time of action 2.1-3.5 hours as the half-life. Corticosteroids have a wide clinical window
as patients require multiple dosages of what the body creates naturally. The risk of
respiration must be
assessed.
Other vital signs like pulse
and blood pressure must
be monitored.
routinely as per the
requirement.
Tachycardia and
hypertension may
be developed as an
increased risk
breathlessness.
Fever may also
develop in some
cases.
fatigue.
For Zacky, the following medications have been prescribed to manage his condition (Tesse et al.,
2018).
1. Ipratropium- A short-acting drug, Ipratropium activates the parasympathic function of the
airway and bronchodilates at the surface of the airway. This agent's influence is only
reported to be 4-6 hours later and ends after 1-2 hours. The result is to ease bronchial
airways restore the limitations induced by wheezy breathing, coughing, chest tightness
and irregular movement of gasses (Drugbank, 2019).
2. Prednisolone- Corticosteroids bind to the glucocorticoid receptor, suppress pro-
inflammatory signals, and promote anti-Inflammatory signals. Prednisolone has a short
time of action 2.1-3.5 hours as the half-life. Corticosteroids have a wide clinical window
as patients require multiple dosages of what the body creates naturally. The risk of
CASE STUDY ANALYSIS
hypothalamic hypophysis-adrenal axis suppression and increased susceptibility to
infections should be consulted in patients with corticosteroids (Drugbank, 2019).
3. Salbutamol- Salbutamol (INN) is a modestly potent, Terbutaline-like beta (2)-receptor
agonist, used widely in the treatment of chronic obstructive asthma disorder and other
asthma. The R-isomer, the levalbuterol, is responsible for bronchodilating the bronchial
reactivity of the S-isomer. The R-enantiomer is available and marketed as levalbuterol as
pure and may therefore cause fewer side effects just with the R-enantiomer-even if not
officially confirmed (Drugbank, 2019).
4. Amoxicillin- Amoxicillin is an antibiotic of moderate spectrum with a vast array
of Gram-positive and a small array of Gram-negative organisms. Amoxicillin is often
selected for use compared to other peers in the cluster of beta-lactam antibiotics because
it tends to show better absorption following oral administration. Bacteria that produce β-
lactamase are susceptible to β-degradation and can therefore be given to increased
susceptibility by clavulanic acid (Drugbank, 2019).
5. Paracetamol- It is the most used global analgesic and is approved by the World Health
Organization (WHO) as first-line treatment in pain situations. The drug is also used to
reduce fever. This medicine was initially approved by the US. It has antipyretic effects.
FDA produced it in 1951 in a range of forms, including syrup, regular tablets, sparkling
tablets, injection, suppositories and other forms (Drugbank, 2019).
hypothalamic hypophysis-adrenal axis suppression and increased susceptibility to
infections should be consulted in patients with corticosteroids (Drugbank, 2019).
3. Salbutamol- Salbutamol (INN) is a modestly potent, Terbutaline-like beta (2)-receptor
agonist, used widely in the treatment of chronic obstructive asthma disorder and other
asthma. The R-isomer, the levalbuterol, is responsible for bronchodilating the bronchial
reactivity of the S-isomer. The R-enantiomer is available and marketed as levalbuterol as
pure and may therefore cause fewer side effects just with the R-enantiomer-even if not
officially confirmed (Drugbank, 2019).
4. Amoxicillin- Amoxicillin is an antibiotic of moderate spectrum with a vast array
of Gram-positive and a small array of Gram-negative organisms. Amoxicillin is often
selected for use compared to other peers in the cluster of beta-lactam antibiotics because
it tends to show better absorption following oral administration. Bacteria that produce β-
lactamase are susceptible to β-degradation and can therefore be given to increased
susceptibility by clavulanic acid (Drugbank, 2019).
5. Paracetamol- It is the most used global analgesic and is approved by the World Health
Organization (WHO) as first-line treatment in pain situations. The drug is also used to
reduce fever. This medicine was initially approved by the US. It has antipyretic effects.
FDA produced it in 1951 in a range of forms, including syrup, regular tablets, sparkling
tablets, injection, suppositories and other forms (Drugbank, 2019).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY ANALYSIS
Assessments for Zachy include:
Lung function tests (spirometry) - This test is used for diagnosing asthma, COPD and other
breathing conditions by assessing the efficiency of lungs by measuring the amount of air the
child can exhale and how quickly he can do it. Therefore, for Zachy’s case, spirometry is an
essential test for diagnosing his current health condition and then develop and implement
appropriate treatment strategy addressing his health concerns.
Exhaled nitric oxide test- This test is also used for diagnosing asthma other tests fail or there is
still uncertainty after other tests conducted to diagnose asthma. This is done by measuring the
nitric oxide level in an exhaled sample of the child’s breath. This testing also helps to determine
if steroid medications can be useful for the treatment of asthma.
Allergy or skin test- If a child is suffering from asthma which is triggered by allergies, the child
might be recommended to undergo an allergy test where the skin is exposed to some common
allergens like animal dander, dust mites or mold and monitored for signs of reaction (van
Aalderen, 2012).
The need for patient education:
Providing age appropriate information on the disease and its management is one of the key to
high-quality paediatric asthma management. According to some literatures, providing education
influences the health outcomes in patients with chronic diseases. However, the provision of
information alone is in many health care settings in most cases not adequate enough to change
the convictions and behaviour of health care (Everard et al., 2015). The most effective
management strategy for asthma is widely regarded as pharmacological treatment in combination
with proper environmental monitoring. Efficient management of the condition, however, can
Assessments for Zachy include:
Lung function tests (spirometry) - This test is used for diagnosing asthma, COPD and other
breathing conditions by assessing the efficiency of lungs by measuring the amount of air the
child can exhale and how quickly he can do it. Therefore, for Zachy’s case, spirometry is an
essential test for diagnosing his current health condition and then develop and implement
appropriate treatment strategy addressing his health concerns.
Exhaled nitric oxide test- This test is also used for diagnosing asthma other tests fail or there is
still uncertainty after other tests conducted to diagnose asthma. This is done by measuring the
nitric oxide level in an exhaled sample of the child’s breath. This testing also helps to determine
if steroid medications can be useful for the treatment of asthma.
Allergy or skin test- If a child is suffering from asthma which is triggered by allergies, the child
might be recommended to undergo an allergy test where the skin is exposed to some common
allergens like animal dander, dust mites or mold and monitored for signs of reaction (van
Aalderen, 2012).
The need for patient education:
Providing age appropriate information on the disease and its management is one of the key to
high-quality paediatric asthma management. According to some literatures, providing education
influences the health outcomes in patients with chronic diseases. However, the provision of
information alone is in many health care settings in most cases not adequate enough to change
the convictions and behaviour of health care (Everard et al., 2015). The most effective
management strategy for asthma is widely regarded as pharmacological treatment in combination
with proper environmental monitoring. Efficient management of the condition, however, can
CASE STUDY ANALYSIS
only be achieved with the cooperation of the doctor, the patient and their family, in many cases.
The first essential step is for a condition to be properly managed by a specialist who receives
asthma care. Afterwards, the extent to which the victim and the families take an active and
supportive part in the treatment strategy is highly dependent upon its implementation (van
Aalderen, 2012).
Conclusion
The basic problem with asthma tends to be immunological, with young children
displaying increased swelling of their airways at the early stages of asthma. Epidemiological
findings provide clues about pathogenesis. Asthma appears to have an increasing incidence
around the world and in rich countries asthma is now much more common.
only be achieved with the cooperation of the doctor, the patient and their family, in many cases.
The first essential step is for a condition to be properly managed by a specialist who receives
asthma care. Afterwards, the extent to which the victim and the families take an active and
supportive part in the treatment strategy is highly dependent upon its implementation (van
Aalderen, 2012).
Conclusion
The basic problem with asthma tends to be immunological, with young children
displaying increased swelling of their airways at the early stages of asthma. Epidemiological
findings provide clues about pathogenesis. Asthma appears to have an increasing incidence
around the world and in rich countries asthma is now much more common.
CASE STUDY ANALYSIS
References:
Chanif, C., & Prastika, D. (2019). Position of Fowler and Semi-fowler to Reduce of Shortness of
Breath (Dyspnea) Level While Undergoing Nebulizer Therapy. South East Asia Nursing
Research, 1(1), 14-19.
Drugbank. (2019). Acetaminophen - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00316
Drugbank. (2019). Amoxicillin - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB01060
Drugbank. (2019). Ipratropium - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00332
Drugbank. (2019). Prednisolone - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00860
Drugbank. (2019). Salbutamol - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB01001
Everard, M. L., Wahn, U., Dorsano, S., Hossny, E., & Le Souef, P. (2015). Asthma education
material for children and their families; a global survey of current resources. World Allergy
Organization Journal, 8(1), 1.
Félix, A. F. S., Lopes, B. A. B. R., Henriques, M. A. P., & Soares, M. D. L. S. R. (2020). Child
asthma control: main associated factors. Enfermería Global, (57), 29.
References:
Chanif, C., & Prastika, D. (2019). Position of Fowler and Semi-fowler to Reduce of Shortness of
Breath (Dyspnea) Level While Undergoing Nebulizer Therapy. South East Asia Nursing
Research, 1(1), 14-19.
Drugbank. (2019). Acetaminophen - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00316
Drugbank. (2019). Amoxicillin - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB01060
Drugbank. (2019). Ipratropium - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00332
Drugbank. (2019). Prednisolone - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB00860
Drugbank. (2019). Salbutamol - DrugBank. Retrieved 10 January 2020, from
https://www.drugbank.ca/drugs/DB01001
Everard, M. L., Wahn, U., Dorsano, S., Hossny, E., & Le Souef, P. (2015). Asthma education
material for children and their families; a global survey of current resources. World Allergy
Organization Journal, 8(1), 1.
Félix, A. F. S., Lopes, B. A. B. R., Henriques, M. A. P., & Soares, M. D. L. S. R. (2020). Child
asthma control: main associated factors. Enfermería Global, (57), 29.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CASE STUDY ANALYSIS
Herzog, R., & Cunningham‐Rundles, S. (2011). Pediatric asthma: natural history, assessment,
and treatment. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized
Medicine, 78(5), 645-660.
Kudo, M., Ishigatsubo, Y., & Aoki, I. (2013). Pathology of asthma. Frontiers in microbiology, 4,
263.
Ortiz-Alvarez, O., Mikrogianakis, A., Canadian Paediatric Society, & Acute Care Committee.
(2012). Managing the paediatric patient with an acute asthma exacerbation. Paediatrics & child
health, 17(5), 251-255.
Tesse, R., Borrelli, G., Mongelli, G., Mastrorilli, V., & Cardinale, F. (2018). Treating pediatric
asthma according guidelines. Frontiers in pediatrics, 6.
van Aalderen, W. M. (2012). Childhood asthma: diagnosis and treatment. Scientifica, 2012.
Herzog, R., & Cunningham‐Rundles, S. (2011). Pediatric asthma: natural history, assessment,
and treatment. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized
Medicine, 78(5), 645-660.
Kudo, M., Ishigatsubo, Y., & Aoki, I. (2013). Pathology of asthma. Frontiers in microbiology, 4,
263.
Ortiz-Alvarez, O., Mikrogianakis, A., Canadian Paediatric Society, & Acute Care Committee.
(2012). Managing the paediatric patient with an acute asthma exacerbation. Paediatrics & child
health, 17(5), 251-255.
Tesse, R., Borrelli, G., Mongelli, G., Mastrorilli, V., & Cardinale, F. (2018). Treating pediatric
asthma according guidelines. Frontiers in pediatrics, 6.
van Aalderen, W. M. (2012). Childhood asthma: diagnosis and treatment. Scientifica, 2012.
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.