Child psychology: a scientific study of developmental changes
VerifiedAdded on 2022/08/14
|16
|4815
|82
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Name of the Student
Name of the University
Author Note
CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Name of the Student
Name of the University
Author Note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Introduction
Child psychology is a scientific study of developmental changes that considers the
mental, behavioural, and emotional aspects of a child. It is seen mainly at the period of childhood
and adolescence. This term broadly explains about cognitive development, social, and emotional
development. It includes persons thinking, learning, and memorization, interaction with the
family or society, and personality development. Cognitive development describes mental issues,
such as language and problem-solving. Social development deals with the system where
individual promotes relationships and interacts with each other. Emotional development is
concerned with person efforts to handle different situations. However, any of these progressive
changes can produce psychological misbalance in people. It is more susceptible in children and
young adults. Many reasons are responsible for hampering the healthy condition of the mind of
people. Specific factors are the sudden death of a person, genetic basis, stressful situations that
can trigger the risk of some mental illness. Possible treatments are available to treat the patient
with this. Psychotherapy, medication, peer supports and especially person-centred care can be
beneficial to recover and support this type of patients. In this paper, a case study of a young adult
is discussed. From the case study, it is known that Jessica has been gone through some mental
health conditions. Hence, possible primary diagnosis, its challenges and the proper justification
are proposed to provide appropriate treatment to the patient. After that, her problems are
constructed with the consideration of predisposition, source and protective factors that she is
facing currently. Finally, the best treatment is intervened based on her disease formulation and
primary diagnosis, and proper justification is also given related to the chosen treatment
procedure.
Introduction
Child psychology is a scientific study of developmental changes that considers the
mental, behavioural, and emotional aspects of a child. It is seen mainly at the period of childhood
and adolescence. This term broadly explains about cognitive development, social, and emotional
development. It includes persons thinking, learning, and memorization, interaction with the
family or society, and personality development. Cognitive development describes mental issues,
such as language and problem-solving. Social development deals with the system where
individual promotes relationships and interacts with each other. Emotional development is
concerned with person efforts to handle different situations. However, any of these progressive
changes can produce psychological misbalance in people. It is more susceptible in children and
young adults. Many reasons are responsible for hampering the healthy condition of the mind of
people. Specific factors are the sudden death of a person, genetic basis, stressful situations that
can trigger the risk of some mental illness. Possible treatments are available to treat the patient
with this. Psychotherapy, medication, peer supports and especially person-centred care can be
beneficial to recover and support this type of patients. In this paper, a case study of a young adult
is discussed. From the case study, it is known that Jessica has been gone through some mental
health conditions. Hence, possible primary diagnosis, its challenges and the proper justification
are proposed to provide appropriate treatment to the patient. After that, her problems are
constructed with the consideration of predisposition, source and protective factors that she is
facing currently. Finally, the best treatment is intervened based on her disease formulation and
primary diagnosis, and proper justification is also given related to the chosen treatment
procedure.

2CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Discussion
Preliminary diagnosis
In the case study, Jessica is facing some problems for 2 yrs. She has rapid mood swings;
one moment she feels low and irritable and then she seems happy and energetic. Nowadays,
Jessica gets angry quickly, often gets involved in arguments and screams at friends, family and
even with school teachers. She then locked herself in a room after this event. Following this
event, and ends with tears. She considers herself as "horrible" and can't understand the reason of
this happenings. She feels sleepy all the time and difficulties to share her feelings. In the end, she
feels lonely and reflected her as a not good human being. By correlating with the symptoms, it is
deliberated that the patient has bipolar disorder. It is a kind of mental illness where the patient
suffers from mood swings, difficulties in sleeping or extra sleeping. The patient gets angry very
quickly and shouts at people, sometimes feels energetic, loses interest from activity. In this
disorder, behavioural changes are seen in the patient. Bipolar disorder is also called manic
depressive illness, bipolar mood disorder, and bipolar affective disorder. Bipolar disorder is
classified into four types- bipolar I, bipolar II, cyclothymic disorder, bipolar disorder not
otherwise specified. This disease is seen in children, adolescents and adults also. The symptoms
vary according to age. Some factors are responsible for causing this disease condition. The
possible reasons are age, gender; hormonal changes along with these scientists also suggest that
other factors are environmental risks which include physical abuse, severe stress, death of a
closed person, daily life problems like money or work problems (Koenders et al., 2015). The
patients go through episodes of mania along with depression that is not a normal condition of
Discussion
Preliminary diagnosis
In the case study, Jessica is facing some problems for 2 yrs. She has rapid mood swings;
one moment she feels low and irritable and then she seems happy and energetic. Nowadays,
Jessica gets angry quickly, often gets involved in arguments and screams at friends, family and
even with school teachers. She then locked herself in a room after this event. Following this
event, and ends with tears. She considers herself as "horrible" and can't understand the reason of
this happenings. She feels sleepy all the time and difficulties to share her feelings. In the end, she
feels lonely and reflected her as a not good human being. By correlating with the symptoms, it is
deliberated that the patient has bipolar disorder. It is a kind of mental illness where the patient
suffers from mood swings, difficulties in sleeping or extra sleeping. The patient gets angry very
quickly and shouts at people, sometimes feels energetic, loses interest from activity. In this
disorder, behavioural changes are seen in the patient. Bipolar disorder is also called manic
depressive illness, bipolar mood disorder, and bipolar affective disorder. Bipolar disorder is
classified into four types- bipolar I, bipolar II, cyclothymic disorder, bipolar disorder not
otherwise specified. This disease is seen in children, adolescents and adults also. The symptoms
vary according to age. Some factors are responsible for causing this disease condition. The
possible reasons are age, gender; hormonal changes along with these scientists also suggest that
other factors are environmental risks which include physical abuse, severe stress, death of a
closed person, daily life problems like money or work problems (Koenders et al., 2015). The
patients go through episodes of mania along with depression that is not a normal condition of
3CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
happiness and sadness like healthy people. Actually, they undergo severe mood swings which
changes time to time (Kupfer, Frank & Ritchey, 2015). It is not the problem of the characteristic
of an individual; its just a disease condition that needs proper treatment.
In this case, the preliminary care that should be followed is - the patient must consult to a
doctor. The doctor may prescribe some tests like blood or urine to examine other symptoms.
Then the doctor may refer her to a mental health professional such as a psychologist or
psychiatrist. It is challenging to analyze the patient as rapid mood changes occur. It's tougher to
treat in children and adolescents. Hence, for Jessica, it is problematic to identify as she has
higher chances to change in behaviour, mood and energy level. The next consideration of
diagnosis is mental health evaluation. In this event, the patient sees a mental health professional
like a psychiatrist or psychologist. They evaluate the patient's mental condition and check for
signs and symptoms of bipolar disorder. After that, the doctor may prescribe her a mood journal.
It is nothing but maintenance of chart where Jessica will note down her moods and the timings of
consistence. The doctor may also suggest keeping a record of her sleeping and eating patterns.
According to the Diagnostic and Statistical Manual-5 criteria (DSM-5), the diagnosis
criteria states that the patients who experience at least two years of hypomanic and depressive
mood disorder and symptoms must be present for half of the time and the patient also must not
be without signs more than 2months at a time, then cyclothymic disease is present. In this case
study, the patient has similar feeling compared to these symptoms. Sometimes she feels so
enthusiastic that other persons think she is over, and after that moment, she also feels very low.
Jessica's mother further mentioned that she has this problem since 2yrs. In accordance with these
criteria, another factor that is responsible for developing the disease in the patient is the death of
happiness and sadness like healthy people. Actually, they undergo severe mood swings which
changes time to time (Kupfer, Frank & Ritchey, 2015). It is not the problem of the characteristic
of an individual; its just a disease condition that needs proper treatment.
In this case, the preliminary care that should be followed is - the patient must consult to a
doctor. The doctor may prescribe some tests like blood or urine to examine other symptoms.
Then the doctor may refer her to a mental health professional such as a psychologist or
psychiatrist. It is challenging to analyze the patient as rapid mood changes occur. It's tougher to
treat in children and adolescents. Hence, for Jessica, it is problematic to identify as she has
higher chances to change in behaviour, mood and energy level. The next consideration of
diagnosis is mental health evaluation. In this event, the patient sees a mental health professional
like a psychiatrist or psychologist. They evaluate the patient's mental condition and check for
signs and symptoms of bipolar disorder. After that, the doctor may prescribe her a mood journal.
It is nothing but maintenance of chart where Jessica will note down her moods and the timings of
consistence. The doctor may also suggest keeping a record of her sleeping and eating patterns.
According to the Diagnostic and Statistical Manual-5 criteria (DSM-5), the diagnosis
criteria states that the patients who experience at least two years of hypomanic and depressive
mood disorder and symptoms must be present for half of the time and the patient also must not
be without signs more than 2months at a time, then cyclothymic disease is present. In this case
study, the patient has similar feeling compared to these symptoms. Sometimes she feels so
enthusiastic that other persons think she is over, and after that moment, she also feels very low.
Jessica's mother further mentioned that she has this problem since 2yrs. In accordance with these
criteria, another factor that is responsible for developing the disease in the patient is the death of
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
her father. Researchers find that this reason is also accountable for the advancement of bipolar
disorder (McIntyre et al., 2015) .
Physicians face some challenges in the time of initial diagnosis of this disease. First
confusion raises to treat depression event since the symptoms of unipolar depression and bipolar
disorder are the same. Both the depression is associated with irritable mood and looks similar
when the patient feels low in bipolar syndrome. In the case of Jessica, the same situation may
happen as she has been suffering from depressed mood, sleeping disturbance like she always
feels sleepy, or unable to sleep. Sometimes she locked herself after having arguments or shouting
at others that means she is withdrawing herself from family and friends.
Moreover, she thinks herself "horrible", losing her self-esteem, feels lonely. These are the
symptoms of depression also. In this way, it seems complicated to distinguish the actual
complication of Jessica since the patient having bipolar disease go along with these parallel
indications. Another challenge is put forward when the patient confronts with the difficulties like
hyperactivity, inattentive. These warning signs are identical with Attention Deficit Hyperactivity
Disorder (ADHD). Therefore confusion is formed in the period of analyzing the disease. During
the time of prognosis, Jessica's mother stated that she is struggling at school now. She had to
keep from advancing to the next level for a year because of not achieving her landmark for the
last year and a half. She also conducts uncharacteristic impulsive behaviour occasionally. She is
frequently aggressive and includes herself in arguments and shouts at friends, family and even
her school teachers too. These signs are typical for ADHD, and this disease is more common in
children and teenagers. As a result, it is possible to confuse a health professional to discriminate
between the two conditions. Since Jessica comes under this age, it is quite easy to assume her
her father. Researchers find that this reason is also accountable for the advancement of bipolar
disorder (McIntyre et al., 2015) .
Physicians face some challenges in the time of initial diagnosis of this disease. First
confusion raises to treat depression event since the symptoms of unipolar depression and bipolar
disorder are the same. Both the depression is associated with irritable mood and looks similar
when the patient feels low in bipolar syndrome. In the case of Jessica, the same situation may
happen as she has been suffering from depressed mood, sleeping disturbance like she always
feels sleepy, or unable to sleep. Sometimes she locked herself after having arguments or shouting
at others that means she is withdrawing herself from family and friends.
Moreover, she thinks herself "horrible", losing her self-esteem, feels lonely. These are the
symptoms of depression also. In this way, it seems complicated to distinguish the actual
complication of Jessica since the patient having bipolar disease go along with these parallel
indications. Another challenge is put forward when the patient confronts with the difficulties like
hyperactivity, inattentive. These warning signs are identical with Attention Deficit Hyperactivity
Disorder (ADHD). Therefore confusion is formed in the period of analyzing the disease. During
the time of prognosis, Jessica's mother stated that she is struggling at school now. She had to
keep from advancing to the next level for a year because of not achieving her landmark for the
last year and a half. She also conducts uncharacteristic impulsive behaviour occasionally. She is
frequently aggressive and includes herself in arguments and shouts at friends, family and even
her school teachers too. These signs are typical for ADHD, and this disease is more common in
children and teenagers. As a result, it is possible to confuse a health professional to discriminate
between the two conditions. Since Jessica comes under this age, it is quite easy to assume her
5CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
symptoms like ADHD and becomes very challenging to treat in the right direction (Hawi et al.,
2015)
Formulate problems
From the case study, it is known that Jessica, a patient, is a 14 years old girl who has been
suffering from rapid mood swings, disruptive behaviour changes for last 2years. Sometimes she
seems very depressive and irritable and after that very joyful and euphoric. Nonetheless, she was
cheerful and very enthusiastic like other child and was not shy. In this situation, depressive
episodes have been initiated by an unexpected event. Jessica's father suddenly died in a road
traffic accident, and she could not cope up with the problem. Dualibe & Osorio,2017
recommended in their studies that early emotional trauma is responsible for causing bipolar
disorder among young adults. They reviewed that the patients with BD confronts more emotional
strain than healthy individual and the form of that distress is mainly psychological. From then
she commits some unusual behavior with everyone. She often gets angry, screams at her family,
friends and even school teachers. She finds that in her school no one is interested to talk with her.
Jessica has only one good friend and he also sometimes gets tired of her. As a result she feels
herself lonely, horrible, tearfulness, moodiness. Samalin et al. (2016) reported that patients with
BD experience similar symptoms. She also faces sleeping disturbances like unable to sleep or
feeling sleepy always. According to a claim made by Cretu et al. (2016), the bipolar disorder
patients suffer sleeping instabilities more than that of healthy people. A study shows that
cognitive impairment may be the cause of hampering work performance, may cause person to
become disinterested in work, thus lowering the quality of work done. Bipolar patients in manic
conditions reveal inadequacies in awareness, verbal fluency, memory and recognition (Grunze,
2015). Grunze (2015) further stated that the patients having bipolar depression also lack of
symptoms like ADHD and becomes very challenging to treat in the right direction (Hawi et al.,
2015)
Formulate problems
From the case study, it is known that Jessica, a patient, is a 14 years old girl who has been
suffering from rapid mood swings, disruptive behaviour changes for last 2years. Sometimes she
seems very depressive and irritable and after that very joyful and euphoric. Nonetheless, she was
cheerful and very enthusiastic like other child and was not shy. In this situation, depressive
episodes have been initiated by an unexpected event. Jessica's father suddenly died in a road
traffic accident, and she could not cope up with the problem. Dualibe & Osorio,2017
recommended in their studies that early emotional trauma is responsible for causing bipolar
disorder among young adults. They reviewed that the patients with BD confronts more emotional
strain than healthy individual and the form of that distress is mainly psychological. From then
she commits some unusual behavior with everyone. She often gets angry, screams at her family,
friends and even school teachers. She finds that in her school no one is interested to talk with her.
Jessica has only one good friend and he also sometimes gets tired of her. As a result she feels
herself lonely, horrible, tearfulness, moodiness. Samalin et al. (2016) reported that patients with
BD experience similar symptoms. She also faces sleeping disturbances like unable to sleep or
feeling sleepy always. According to a claim made by Cretu et al. (2016), the bipolar disorder
patients suffer sleeping instabilities more than that of healthy people. A study shows that
cognitive impairment may be the cause of hampering work performance, may cause person to
become disinterested in work, thus lowering the quality of work done. Bipolar patients in manic
conditions reveal inadequacies in awareness, verbal fluency, memory and recognition (Grunze,
2015). Grunze (2015) further stated that the patients having bipolar depression also lack of
6CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
cognitive, behavioral, emotional difficulties, attention, and are diverse from hypomania or
unipolar depression syndrome.
Moreover she is inattentive in her class; could not meet her level as before. Thus, she had
to hold back for a year. She feels hard to share her feelings with her family so she avoids this. In
some cases, when her mother also lost her patience and snapped Jessica, she gets irritated and
locked herself after having arguments. These types of conditions are lookalike with Attention
Deficit Hyperactivity Disorder (ADHD). Studies suggest that there is a high risk of co-
occurrence of the bipolar disease with ADHD (Frias, Palma & Farriols, 2015). Marangoni &
Faedda, 2015 suggested that bipolar and ADHD share some common symptomology that is
challenging to discriminate the two diseases. They also proposed that there are specific
symptoms that help to distinguish the bipolar disorder. The symptoms may appear as destructive
behavior, violence outbursts, anger, sleep difficulties, rapid shifts of moods, fluctuation of self-
esteem.
Jessica's mother also reported that she heard of a great aunt who was manic. There is
evidence of family history having chances these symptoms in Jessica. Sparks et al.,2014
indicated that youth holding family history are increased threat of developing BD. There is
another reason that elicit the bipolar syndrome in women after giving birth to her child. In this
case, early history from Jessica's mother, Mary, reported that Mary had depression for a couple
of months after Jessica was born ( Jones et al.,2014). This clinical symptom revealed that Jessica
has a higher risk of developing the disease. Above all, Jessica also realizes that she is terrible but
does not understand the reason. Jessica regrets and does not want to hurt or upset anyone; still,
Jessica cannot control her anger. Often she reflects herself isolated and has low self-esteem and
accomplishes that she would keep trying better. Some protective factors are present that will help
cognitive, behavioral, emotional difficulties, attention, and are diverse from hypomania or
unipolar depression syndrome.
Moreover she is inattentive in her class; could not meet her level as before. Thus, she had
to hold back for a year. She feels hard to share her feelings with her family so she avoids this. In
some cases, when her mother also lost her patience and snapped Jessica, she gets irritated and
locked herself after having arguments. These types of conditions are lookalike with Attention
Deficit Hyperactivity Disorder (ADHD). Studies suggest that there is a high risk of co-
occurrence of the bipolar disease with ADHD (Frias, Palma & Farriols, 2015). Marangoni &
Faedda, 2015 suggested that bipolar and ADHD share some common symptomology that is
challenging to discriminate the two diseases. They also proposed that there are specific
symptoms that help to distinguish the bipolar disorder. The symptoms may appear as destructive
behavior, violence outbursts, anger, sleep difficulties, rapid shifts of moods, fluctuation of self-
esteem.
Jessica's mother also reported that she heard of a great aunt who was manic. There is
evidence of family history having chances these symptoms in Jessica. Sparks et al.,2014
indicated that youth holding family history are increased threat of developing BD. There is
another reason that elicit the bipolar syndrome in women after giving birth to her child. In this
case, early history from Jessica's mother, Mary, reported that Mary had depression for a couple
of months after Jessica was born ( Jones et al.,2014). This clinical symptom revealed that Jessica
has a higher risk of developing the disease. Above all, Jessica also realizes that she is terrible but
does not understand the reason. Jessica regrets and does not want to hurt or upset anyone; still,
Jessica cannot control her anger. Often she reflects herself isolated and has low self-esteem and
accomplishes that she would keep trying better. Some protective factors are present that will help
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
to prevent the illness. These factors include right coping strategies, good interpersonal skill,
peers group, proper social support, effective communication and problem-solving ability that
enable the patient to combat this illness in its elementary phases. Choi et al., 2015 examined a
no. of patients and concluded that the adaptability is related to the bipolar disease. Researchers
showed that low levels of adaptability are associated with high impulsivity and greater risk of
depressive events in the patient with BD. Therefore if the flexibility is improved compared to
impulsivity, then the patient can persist and prevent the disease condition.
Identify interventions
Following the preliminary diagnosis and based on problem formulation, it is analyzed
that the patient had bipolar disorder, specifically cyclothymic disease. Effective treatment
procedures must be drawn up to reduce this syndrome. By analyzing the case study of Jessica,
the one preventive measure that would be best for her is psychotherapy. It is a kind of therapy
where patients undergo a clinical process that can treat people with mental health problems,
cognitive disorders, facing trouble in coping with daily life, the impact of emotional trauma like
death of a closed person and specific symptoms like depression or anxiety. The therapy may
include an individual, family or group sceneries. Mental health professionals like psychologist
and psychiatrists, social workers, mental health nurse select what method suits the patient
according to their illness. Sometimes therapist comprises of different tactics to meet the
individual challenges of patients as the symptoms may vary from person to person. This therapy
is categorized in some specific procedures. They are classified as brief therapy and long term
therapy according to the duration; those therapies that will take lesser number of sessions are
termed as short and vice versa. There are several forms of psychotherapy termed, for example,
Cognitive Behavioral Therapy (CBT), Interpersonal and Social Rhythm Therapy (IPSRT),
to prevent the illness. These factors include right coping strategies, good interpersonal skill,
peers group, proper social support, effective communication and problem-solving ability that
enable the patient to combat this illness in its elementary phases. Choi et al., 2015 examined a
no. of patients and concluded that the adaptability is related to the bipolar disease. Researchers
showed that low levels of adaptability are associated with high impulsivity and greater risk of
depressive events in the patient with BD. Therefore if the flexibility is improved compared to
impulsivity, then the patient can persist and prevent the disease condition.
Identify interventions
Following the preliminary diagnosis and based on problem formulation, it is analyzed
that the patient had bipolar disorder, specifically cyclothymic disease. Effective treatment
procedures must be drawn up to reduce this syndrome. By analyzing the case study of Jessica,
the one preventive measure that would be best for her is psychotherapy. It is a kind of therapy
where patients undergo a clinical process that can treat people with mental health problems,
cognitive disorders, facing trouble in coping with daily life, the impact of emotional trauma like
death of a closed person and specific symptoms like depression or anxiety. The therapy may
include an individual, family or group sceneries. Mental health professionals like psychologist
and psychiatrists, social workers, mental health nurse select what method suits the patient
according to their illness. Sometimes therapist comprises of different tactics to meet the
individual challenges of patients as the symptoms may vary from person to person. This therapy
is categorized in some specific procedures. They are classified as brief therapy and long term
therapy according to the duration; those therapies that will take lesser number of sessions are
termed as short and vice versa. There are several forms of psychotherapy termed, for example,
Cognitive Behavioral Therapy (CBT), Interpersonal and Social Rhythm Therapy (IPSRT),
8CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Dialectical behaviour therapy, Psychodynamic therapy. In this case, IPSRT would be appropriate
for the patient Jessica. IPSRT is an evidence-based procedure that is specially designed to help
the patient with bipolar disorder by enhancing their mood episodes and considering biological
and social rhythms. This IPSRT information panel is planned for providers and customers to
review and know about this therapy thoroughly. This treatment is chosen for the patient Jessica
as she also has symptoms of bipolar disorder. In this treatment process, four stages are followed
to cure the patient. All the steps that are monitored in this procedure follow the appropriate
diagnosis of the disease. In every step, the symptoms are clarified rationally. In the initial stage
of diagnosis, it is focused on history taking that connects with the disturbance in routine bipolar
events and forms justification for providing treatment. In the next step, it is mainly concentrated
on rearranging social rhythms like sleeping cycle, depression and highlights on daily
activities( Rumble, White & Benca., 2015). These symptoms are precisely happening with
Jessica. After that step, those new social rhythms are strengthened, and the techniques of
confidence level are increased that are previously learnt. These symptomatic procedures possess
similarities with the indications of bipolar disorder (Inder et al., 2015)
CBT, a short-term psycho-social process of treatment, is a practical approach to a
problem -solving method. It aims to centre mental health problems and emphasizes to change the
thinking abilities or person's behaviour. It works by changing the individual's approach and their
behaviour by improving emotional misbalance, coping stratagems, changing their thoughts,
confidence level. It is also used to prevent personal life activities such as sleeping disorder, drug
or substance use, anxiety and depression (Niles et al., 2014). CBT functions on persons cognitive
processes. It depends on the combination of two principals; they are behavioural and cognitive
psychotherapy (Jauhar, McKenna & Laws, 2016).
Dialectical behaviour therapy, Psychodynamic therapy. In this case, IPSRT would be appropriate
for the patient Jessica. IPSRT is an evidence-based procedure that is specially designed to help
the patient with bipolar disorder by enhancing their mood episodes and considering biological
and social rhythms. This IPSRT information panel is planned for providers and customers to
review and know about this therapy thoroughly. This treatment is chosen for the patient Jessica
as she also has symptoms of bipolar disorder. In this treatment process, four stages are followed
to cure the patient. All the steps that are monitored in this procedure follow the appropriate
diagnosis of the disease. In every step, the symptoms are clarified rationally. In the initial stage
of diagnosis, it is focused on history taking that connects with the disturbance in routine bipolar
events and forms justification for providing treatment. In the next step, it is mainly concentrated
on rearranging social rhythms like sleeping cycle, depression and highlights on daily
activities( Rumble, White & Benca., 2015). These symptoms are precisely happening with
Jessica. After that step, those new social rhythms are strengthened, and the techniques of
confidence level are increased that are previously learnt. These symptomatic procedures possess
similarities with the indications of bipolar disorder (Inder et al., 2015)
CBT, a short-term psycho-social process of treatment, is a practical approach to a
problem -solving method. It aims to centre mental health problems and emphasizes to change the
thinking abilities or person's behaviour. It works by changing the individual's approach and their
behaviour by improving emotional misbalance, coping stratagems, changing their thoughts,
confidence level. It is also used to prevent personal life activities such as sleeping disorder, drug
or substance use, anxiety and depression (Niles et al., 2014). CBT functions on persons cognitive
processes. It depends on the combination of two principals; they are behavioural and cognitive
psychotherapy (Jauhar, McKenna & Laws, 2016).
9CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Another regimen that should be followed is that medication. Several medicines are
present that are prescribed by health care professionals such as a specialist doctor, nurse, mental
health care co-workers.
For example, Lithium is that kind of drug that is effective at mood-stabilizing and
preventing the extreme high and low mood swings in bipolar disorder. Episodic blood tests are
analyzed that can affect thyroid and kidney problems. It has some general side effects include
restlessness, dry mouth and digestive malfunction issues. Lithium levels should be evaluated to
ensure the best dosage and toxicity. Anticonvulsants- these medicines are used to treat mania and
for bipolar disorder as well. Valproic acid and carbamazepine are used to prescribe for maniac
patient (Peselow, Clevenge & IsHak 2016). These drugs are more effective than Lithium as these
are better to handle more complex bipolar disorder having rapid cycling and dysphoric mania
(Kessing et al., 2015). In the case of Jessica, she has a similar problem of experiencing
depression and mania simultaneously. Hence the anticonvulsants will be more appropriate for
Jessica. Jessica can be prescribed with antipsychotic drugs that include aripiprazole, olanzapine,
quetiapine that have used as a long term mood stabilizer (Correll et al., 2015). Quetiapine has
other action that serves to lower the bipolar depression. There are other treatments that Jessica
should go through includes person-centred care that is mainly served by the mental-health
practitioner, nurses (Richter et al., 2015). They will help Jessica to come out from her present
situation. Family support is another significant part that plays a pivotal role to recover this type
of mental health patient.
Another regimen that should be followed is that medication. Several medicines are
present that are prescribed by health care professionals such as a specialist doctor, nurse, mental
health care co-workers.
For example, Lithium is that kind of drug that is effective at mood-stabilizing and
preventing the extreme high and low mood swings in bipolar disorder. Episodic blood tests are
analyzed that can affect thyroid and kidney problems. It has some general side effects include
restlessness, dry mouth and digestive malfunction issues. Lithium levels should be evaluated to
ensure the best dosage and toxicity. Anticonvulsants- these medicines are used to treat mania and
for bipolar disorder as well. Valproic acid and carbamazepine are used to prescribe for maniac
patient (Peselow, Clevenge & IsHak 2016). These drugs are more effective than Lithium as these
are better to handle more complex bipolar disorder having rapid cycling and dysphoric mania
(Kessing et al., 2015). In the case of Jessica, she has a similar problem of experiencing
depression and mania simultaneously. Hence the anticonvulsants will be more appropriate for
Jessica. Jessica can be prescribed with antipsychotic drugs that include aripiprazole, olanzapine,
quetiapine that have used as a long term mood stabilizer (Correll et al., 2015). Quetiapine has
other action that serves to lower the bipolar depression. There are other treatments that Jessica
should go through includes person-centred care that is mainly served by the mental-health
practitioner, nurses (Richter et al., 2015). They will help Jessica to come out from her present
situation. Family support is another significant part that plays a pivotal role to recover this type
of mental health patient.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
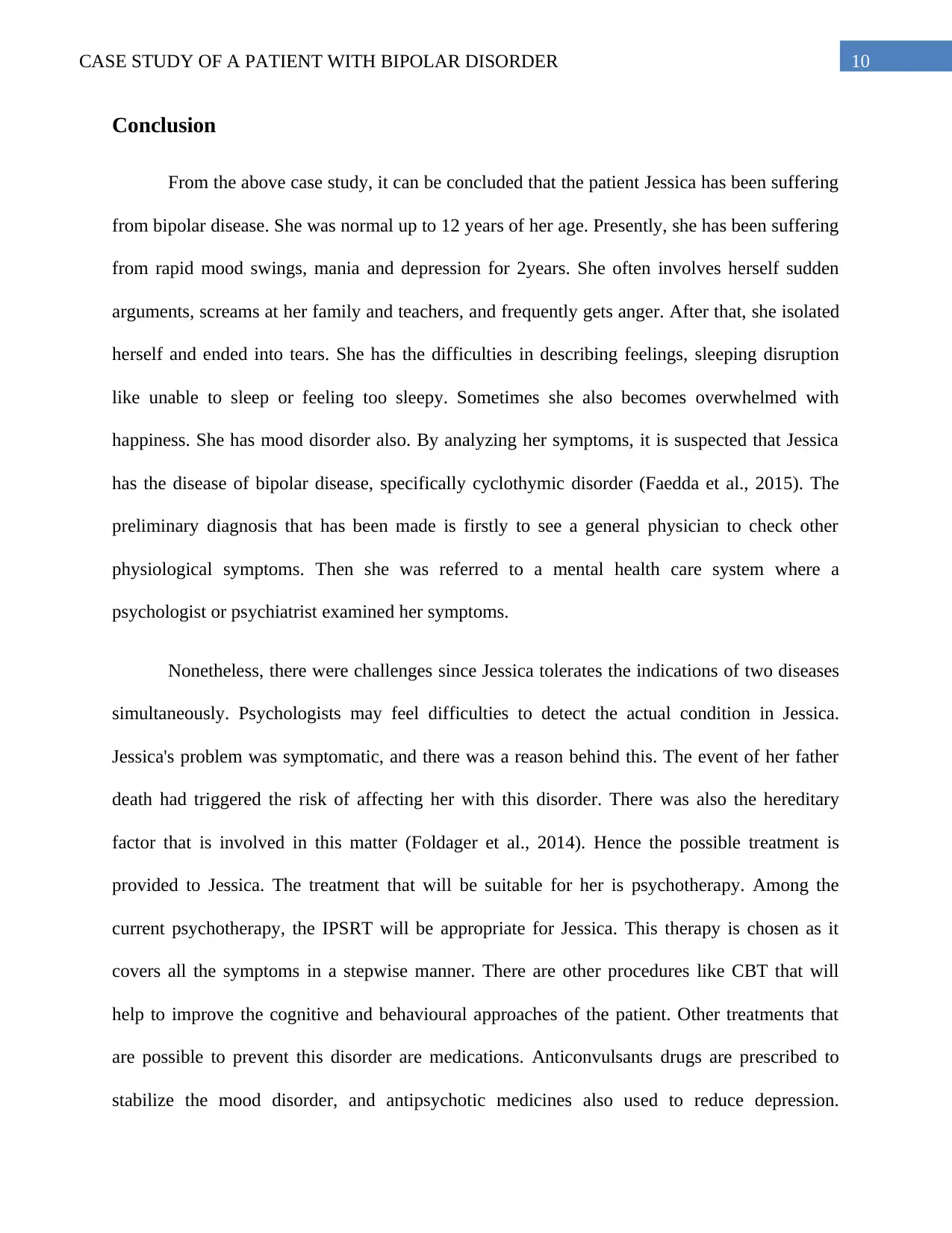
Conclusion
From the above case study, it can be concluded that the patient Jessica has been suffering
from bipolar disease. She was normal up to 12 years of her age. Presently, she has been suffering
from rapid mood swings, mania and depression for 2years. She often involves herself sudden
arguments, screams at her family and teachers, and frequently gets anger. After that, she isolated
herself and ended into tears. She has the difficulties in describing feelings, sleeping disruption
like unable to sleep or feeling too sleepy. Sometimes she also becomes overwhelmed with
happiness. She has mood disorder also. By analyzing her symptoms, it is suspected that Jessica
has the disease of bipolar disease, specifically cyclothymic disorder (Faedda et al., 2015). The
preliminary diagnosis that has been made is firstly to see a general physician to check other
physiological symptoms. Then she was referred to a mental health care system where a
psychologist or psychiatrist examined her symptoms.
Nonetheless, there were challenges since Jessica tolerates the indications of two diseases
simultaneously. Psychologists may feel difficulties to detect the actual condition in Jessica.
Jessica's problem was symptomatic, and there was a reason behind this. The event of her father
death had triggered the risk of affecting her with this disorder. There was also the hereditary
factor that is involved in this matter (Foldager et al., 2014). Hence the possible treatment is
provided to Jessica. The treatment that will be suitable for her is psychotherapy. Among the
current psychotherapy, the IPSRT will be appropriate for Jessica. This therapy is chosen as it
covers all the symptoms in a stepwise manner. There are other procedures like CBT that will
help to improve the cognitive and behavioural approaches of the patient. Other treatments that
are possible to prevent this disorder are medications. Anticonvulsants drugs are prescribed to
stabilize the mood disorder, and antipsychotic medicines also used to reduce depression.
Conclusion
From the above case study, it can be concluded that the patient Jessica has been suffering
from bipolar disease. She was normal up to 12 years of her age. Presently, she has been suffering
from rapid mood swings, mania and depression for 2years. She often involves herself sudden
arguments, screams at her family and teachers, and frequently gets anger. After that, she isolated
herself and ended into tears. She has the difficulties in describing feelings, sleeping disruption
like unable to sleep or feeling too sleepy. Sometimes she also becomes overwhelmed with
happiness. She has mood disorder also. By analyzing her symptoms, it is suspected that Jessica
has the disease of bipolar disease, specifically cyclothymic disorder (Faedda et al., 2015). The
preliminary diagnosis that has been made is firstly to see a general physician to check other
physiological symptoms. Then she was referred to a mental health care system where a
psychologist or psychiatrist examined her symptoms.
Nonetheless, there were challenges since Jessica tolerates the indications of two diseases
simultaneously. Psychologists may feel difficulties to detect the actual condition in Jessica.
Jessica's problem was symptomatic, and there was a reason behind this. The event of her father
death had triggered the risk of affecting her with this disorder. There was also the hereditary
factor that is involved in this matter (Foldager et al., 2014). Hence the possible treatment is
provided to Jessica. The treatment that will be suitable for her is psychotherapy. Among the
current psychotherapy, the IPSRT will be appropriate for Jessica. This therapy is chosen as it
covers all the symptoms in a stepwise manner. There are other procedures like CBT that will
help to improve the cognitive and behavioural approaches of the patient. Other treatments that
are possible to prevent this disorder are medications. Anticonvulsants drugs are prescribed to
stabilize the mood disorder, and antipsychotic medicines also used to reduce depression.

11CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Moreover, person-centred care and family support are the major factors that support to handle
this kind of patient.
Moreover, person-centred care and family support are the major factors that support to handle
this kind of patient.
12CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
References
Choi, J. W., Cha, B., Jang, J., Park, C. S., Kim, B. J., Lee, C. S., & Lee, S. J. (2015). Resilience
and impulsivity in euthymic patients with bipolar disorder. Journal of affective
disorders, 170, 172-177.
Correll, C. U., Detraux, J., De Lepeleire, J., & De Hert, M. (2015). Effects of antipsychotics,
antidepressants and mood stabilizers on risk for physical diseases in people with
schizophrenia, depression and bipolar disorder. World psychiatry, 14(2), 119-136.
Cretu, J. B., Culver, J. L., Goffin, K. C., Shah, S., & Ketter, T. A. (2016). Sleep, residual mood
symptoms, and time to relapse in recovered patients with bipolar disorder. Journal of
affective disorders, 190, 162-166.
Dualibe, A. L., & Osório, F. L. (2017). Bipolar disorder and early emotional trauma: a critical
literature review on indicators of prevalence rates and clinical outcomes. Harvard review
of psychiatry, 25(5), 198-208.
Duffy, A., Jones, S., Goodday, S., & Bentall, R. (2016). Candidate risks indicators for bipolar
disorder: early intervention opportunities in high-risk youth. International Journal of
Neuropsychopharmacology, 19(1).
Faedda, G. L., Marangoni, C., Serra, G., Salvatore, P., Sani, G., Vázquez, G. H., ... &
Koukopoulos, A. (2015). Precursors of bipolar disorders: a systematic literature review of
prospective studies. J Clin Psychiatry, 76(5), 614-624.
References
Choi, J. W., Cha, B., Jang, J., Park, C. S., Kim, B. J., Lee, C. S., & Lee, S. J. (2015). Resilience
and impulsivity in euthymic patients with bipolar disorder. Journal of affective
disorders, 170, 172-177.
Correll, C. U., Detraux, J., De Lepeleire, J., & De Hert, M. (2015). Effects of antipsychotics,
antidepressants and mood stabilizers on risk for physical diseases in people with
schizophrenia, depression and bipolar disorder. World psychiatry, 14(2), 119-136.
Cretu, J. B., Culver, J. L., Goffin, K. C., Shah, S., & Ketter, T. A. (2016). Sleep, residual mood
symptoms, and time to relapse in recovered patients with bipolar disorder. Journal of
affective disorders, 190, 162-166.
Dualibe, A. L., & Osório, F. L. (2017). Bipolar disorder and early emotional trauma: a critical
literature review on indicators of prevalence rates and clinical outcomes. Harvard review
of psychiatry, 25(5), 198-208.
Duffy, A., Jones, S., Goodday, S., & Bentall, R. (2016). Candidate risks indicators for bipolar
disorder: early intervention opportunities in high-risk youth. International Journal of
Neuropsychopharmacology, 19(1).
Faedda, G. L., Marangoni, C., Serra, G., Salvatore, P., Sani, G., Vázquez, G. H., ... &
Koukopoulos, A. (2015). Precursors of bipolar disorders: a systematic literature review of
prospective studies. J Clin Psychiatry, 76(5), 614-624.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Foldager, L., Köhler, O., Steffensen, R., Thiel, S., Kristensen, A. S., Jensenius, J. C., & Mors, O.
(2014). Bipolar and panic disorders may be associated with hereditary defects in the
innate immune system. Journal of affective disorders, 164, 148-154.
Frías, Á., Palma, C., & Farriols, N. (2015). Comorbidity in pediatric bipolar disorder:
prevalence, clinical impact, etiology and treatment. Journal of affective disorders, 174,
378-389.
Grunze, H. (2015). Bipolar disorder. In Neurobiology of brain disorders (pp. 655-673).
Academic Press.
Hawi, Z., Cummins, T. D. R., Tong, J., Johnson, B., Lau, R., Samarrai, W., & Bellgrove, M. A.
(2015). The molecular genetic architecture of attention deficit hyperactivity
disorder. Molecular psychiatry, 20(3), 289-297.
Inder, M. L., Crowe, M. T., Luty, S. E., Carter, J. D., Moor, S., Frampton, C. M., & Joyce, P. R.
(2015). Randomized, controlled trial of Interpersonal and Social Rhythm Therapy for
young people with bipolar disorder. Bipolar disorders, 17(2), 128-138.
Jauhar, S., McKenna, P. J., & Laws, K. R. (2016). NICE guidance on psychological treatments
for bipolar disorder: searching for the evidence. The Lancet Psychiatry, 3(4), 386-388.
Jones, I., Chandra, P. S., Dazzan, P., & Howard, L. M. (2014). Bipolar disorder, affective
psychosis, and schizophrenia in pregnancy and the post-partum period. The
Lancet, 384(9956), 1789-1799.
Foldager, L., Köhler, O., Steffensen, R., Thiel, S., Kristensen, A. S., Jensenius, J. C., & Mors, O.
(2014). Bipolar and panic disorders may be associated with hereditary defects in the
innate immune system. Journal of affective disorders, 164, 148-154.
Frías, Á., Palma, C., & Farriols, N. (2015). Comorbidity in pediatric bipolar disorder:
prevalence, clinical impact, etiology and treatment. Journal of affective disorders, 174,
378-389.
Grunze, H. (2015). Bipolar disorder. In Neurobiology of brain disorders (pp. 655-673).
Academic Press.
Hawi, Z., Cummins, T. D. R., Tong, J., Johnson, B., Lau, R., Samarrai, W., & Bellgrove, M. A.
(2015). The molecular genetic architecture of attention deficit hyperactivity
disorder. Molecular psychiatry, 20(3), 289-297.
Inder, M. L., Crowe, M. T., Luty, S. E., Carter, J. D., Moor, S., Frampton, C. M., & Joyce, P. R.
(2015). Randomized, controlled trial of Interpersonal and Social Rhythm Therapy for
young people with bipolar disorder. Bipolar disorders, 17(2), 128-138.
Jauhar, S., McKenna, P. J., & Laws, K. R. (2016). NICE guidance on psychological treatments
for bipolar disorder: searching for the evidence. The Lancet Psychiatry, 3(4), 386-388.
Jones, I., Chandra, P. S., Dazzan, P., & Howard, L. M. (2014). Bipolar disorder, affective
psychosis, and schizophrenia in pregnancy and the post-partum period. The
Lancet, 384(9956), 1789-1799.
14CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Kessing, L. V., Gerds, T. A., Feldt-Rasmussen, B., Andersen, P. K., & Licht, R. W. (2015). Use
of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide
population-based study. JAMA psychiatry, 72(12), 1182-1191.
Koenders, M. A., De Kleijn, R., Giltay, E. J., Elzinga, B. M., Spinhoven, P., & Spijker, A. T.
(2015). A network approach to bipolar symptomatology in patients with different course
types. PLoS One, 10(10).
Kupfer, D. J., Frank, E., & Ritchey, F. C. (2015). Staging bipolar disorder: what data and what
models are needed?. The Lancet Psychiatry, 2(6), 564-570.
Marangoni, C., De Chiara, L., & Faedda, G. L. (2015). Bipolar disorder and ADHD: comorbidity
and diagnostic distinctions. Current psychiatry reports, 17(8), 67.
McIntyre, R. S., Soczynska, J. K., Cha, D. S., Woldeyohannes, H. O., Dale, R. S., Alsuwaidan,
M. T., ... & Kennedy, S. H. (2015). The prevalence and illness characteristics of DSM-5-
defined “mixed feature specifier” in adults with major depressive disorder and bipolar
disorder: results from the International Mood Disorders Collaborative Project. Journal of
affective disorders, 172, 259-264.
Niles, A. N., Burklund, L. J., Arch, J. J., Lieberman, M. D., Saxbe, D., & Craske, M. G. (2014).
Cognitive mediators of treatment for social anxiety disorder: Comparing acceptance and
commitment therapy and cognitive-behavioral therapy. Behavior therapy, 45(5), 664-677.
Peselow, E. D., Clevenger, S., & IsHak, W. W. (2016). Prophylactic efficacy of lithium, valproic
acid, and carbamazepine in the maintenance phase of bipolar disorder: a naturalistic
study. International clinical psychopharmacology, 31(4), 218-223.
Kessing, L. V., Gerds, T. A., Feldt-Rasmussen, B., Andersen, P. K., & Licht, R. W. (2015). Use
of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide
population-based study. JAMA psychiatry, 72(12), 1182-1191.
Koenders, M. A., De Kleijn, R., Giltay, E. J., Elzinga, B. M., Spinhoven, P., & Spijker, A. T.
(2015). A network approach to bipolar symptomatology in patients with different course
types. PLoS One, 10(10).
Kupfer, D. J., Frank, E., & Ritchey, F. C. (2015). Staging bipolar disorder: what data and what
models are needed?. The Lancet Psychiatry, 2(6), 564-570.
Marangoni, C., De Chiara, L., & Faedda, G. L. (2015). Bipolar disorder and ADHD: comorbidity
and diagnostic distinctions. Current psychiatry reports, 17(8), 67.
McIntyre, R. S., Soczynska, J. K., Cha, D. S., Woldeyohannes, H. O., Dale, R. S., Alsuwaidan,
M. T., ... & Kennedy, S. H. (2015). The prevalence and illness characteristics of DSM-5-
defined “mixed feature specifier” in adults with major depressive disorder and bipolar
disorder: results from the International Mood Disorders Collaborative Project. Journal of
affective disorders, 172, 259-264.
Niles, A. N., Burklund, L. J., Arch, J. J., Lieberman, M. D., Saxbe, D., & Craske, M. G. (2014).
Cognitive mediators of treatment for social anxiety disorder: Comparing acceptance and
commitment therapy and cognitive-behavioral therapy. Behavior therapy, 45(5), 664-677.
Peselow, E. D., Clevenger, S., & IsHak, W. W. (2016). Prophylactic efficacy of lithium, valproic
acid, and carbamazepine in the maintenance phase of bipolar disorder: a naturalistic
study. International clinical psychopharmacology, 31(4), 218-223.
15CASE STUDY OF A PATIENT WITH BIPOLAR DISORDER
Richter, C., Berg, A., Fleischer, S., Köpke, S., Balzer, K., Fick, E. M., ... & Icks, A. (2015).
Effect of person-centred care on antipsychotic drug use in nursing homes (EPCentCare):
study protocol for a cluster-randomised controlled trial. Implementation Science, 10(1),
82.
Rumble, M. E., White, K. H., & Benca, R. M. (2015). Sleep disturbances in mood
disorders. Psychiatric Clinics, 38(4), 743-759.
Samalin, L., de Chazeron, I., Vieta, E., Bellivier, F., & Llorca, P. M. (2016). Residual symptoms
and specific functional impairments in euthymic patients with bipolar disorder. Bipolar
disorders, 18(2), 164-173.
Sparks, G. M., Axelson, D. A., Yu, H., Ha, W., Ballester, J., Diler, R. S., ... & Monk, K. (2014).
Disruptive mood dysregulation disorder and chronic irritability in youth at familial risk
for bipolar disorder. Journal of the American Academy of Child & Adolescent
Psychiatry, 53(4), 408-416.
Richter, C., Berg, A., Fleischer, S., Köpke, S., Balzer, K., Fick, E. M., ... & Icks, A. (2015).
Effect of person-centred care on antipsychotic drug use in nursing homes (EPCentCare):
study protocol for a cluster-randomised controlled trial. Implementation Science, 10(1),
82.
Rumble, M. E., White, K. H., & Benca, R. M. (2015). Sleep disturbances in mood
disorders. Psychiatric Clinics, 38(4), 743-759.
Samalin, L., de Chazeron, I., Vieta, E., Bellivier, F., & Llorca, P. M. (2016). Residual symptoms
and specific functional impairments in euthymic patients with bipolar disorder. Bipolar
disorders, 18(2), 164-173.
Sparks, G. M., Axelson, D. A., Yu, H., Ha, W., Ballester, J., Diler, R. S., ... & Monk, K. (2014).
Disruptive mood dysregulation disorder and chronic irritability in youth at familial risk
for bipolar disorder. Journal of the American Academy of Child & Adolescent
Psychiatry, 53(4), 408-416.
1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.