Child Care Facility Under Consideration Case Study 2022
VerifiedAdded on 2022/10/02
|18
|4951
|34
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: Diseases 1
Diseases
by
Course:
Tutor:
University:
Department:
Date:
Diseases
by
Course:
Tutor:
University:
Department:
Date:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Diseases 2
Planning, implementation and evaluation of childhood obesity prevention initiative in
Sydney, Australia
1.0 Demographic characteristics of the specific child-care facility and surrounding
community
The child-care facility under consideration in this study is the Sydney Cove Children’s Centre in
the Sydney central business district. The child-care centre is a long daycare facility that is
conveniently located in the heart of the city and meets the National Quality Standard. The centre
offers all-inclusive, stress-free childcare and early education experience. There is a spacious
outdoor area for effective play-based learning experiences. It also offers a detailed study program
for children aged from birth to 6 years based on the Australian Government’s Early Years
Learning Framework (EYLF) (Australian Department of Education, 2017). The pre-school
program is implemented by experienced and qualified instructors and emphasizes on language,
literacy, numeracy and social skills that prepare the child for future school life.
Sydney Cove Children’s Centre has specific rooms customized to fit the needs of each child and
to offer the best early learning experience to the child. Nursery rooms are for children aged 0 to 2
years and are of three different types. There is the one for younger babies aged 0-15 months and
for senior nursery environments for children aged 15 months -2 years. These rooms offer private
family breastfeeding rooms, safe and secure outdoor play area that is directly linked to the indoor
play space and catering for the small babies. The rooms are also equipped with sound play music
programs in addition to multiple nurturing experiences that are appropriate for each age such as
sensory activities (Sydney Cove Children’s Centre, n.d.)
The junior preschool room is for children aged 2-3 years and provides a large outdoor play space
that inspires children to be interested in physical activities. The preschool room has football,
yoga and Zumba programs and a variety of learning experiences that foster individuality, fun and
Planning, implementation and evaluation of childhood obesity prevention initiative in
Sydney, Australia
1.0 Demographic characteristics of the specific child-care facility and surrounding
community
The child-care facility under consideration in this study is the Sydney Cove Children’s Centre in
the Sydney central business district. The child-care centre is a long daycare facility that is
conveniently located in the heart of the city and meets the National Quality Standard. The centre
offers all-inclusive, stress-free childcare and early education experience. There is a spacious
outdoor area for effective play-based learning experiences. It also offers a detailed study program
for children aged from birth to 6 years based on the Australian Government’s Early Years
Learning Framework (EYLF) (Australian Department of Education, 2017). The pre-school
program is implemented by experienced and qualified instructors and emphasizes on language,
literacy, numeracy and social skills that prepare the child for future school life.
Sydney Cove Children’s Centre has specific rooms customized to fit the needs of each child and
to offer the best early learning experience to the child. Nursery rooms are for children aged 0 to 2
years and are of three different types. There is the one for younger babies aged 0-15 months and
for senior nursery environments for children aged 15 months -2 years. These rooms offer private
family breastfeeding rooms, safe and secure outdoor play area that is directly linked to the indoor
play space and catering for the small babies. The rooms are also equipped with sound play music
programs in addition to multiple nurturing experiences that are appropriate for each age such as
sensory activities (Sydney Cove Children’s Centre, n.d.)
The junior preschool room is for children aged 2-3 years and provides a large outdoor play space
that inspires children to be interested in physical activities. The preschool room has football,
yoga and Zumba programs and a variety of learning experiences that foster individuality, fun and
Diseases 3
inquisitiveness. The centre also offers a preschool room for children aged 3-5 years which offers
a preschool program taught by qualified early childhood instructors with bachelors’ degree and
are aimed at the acquisition of knowledge, social skills and numeracy to prepare the children for
future schooling (Sydney Cove Children’s Centre, n.d.).
Sydney is the most populous and busiest city of Australia occupied by about five million people.
It has a median age of 35 years and each household has approximately 2.7 members. English
speakers are the majority (27%) followed by Australians (25%), Chinese (10.8%) among others
with Korean (1.4%) and Maltese (1.3%) accounting for the least. Therefore, Sydney is a hub of
several migrant communities with the Indigenous community accounting for 1.5% of the total
population (ABS, 2016).
According to the Australian Bureau of Statistics (2016), 52.7% of the population is male and
female are 47.3%. Family statistics show that there are approximately 18,977 families with
approximately 1.5 children in each family with children and 0.2 for all families. There is an
average of 53,316 private residentials with an average people per household of 2. Children aged
0-4 years are approximately 2,983. 35% of the people in Sydney were attending an academic
institution out of which 33.0% were in higher education, 5.8% in primary school and 4.5% in
secondary school. Regarding employment, 60,399 were employees during the 2016 census out of
which 64.7% were in full-time employment, 26.1% were in part-time employment and 5.1%
were unemployed (ABS, 2016).
Based on the above demographic characteristics, Sydney is a very busy city occupied with
families thus necessitating the need for accessible childcare centres such as the Sydney Cove
Children’s Centre. Moreover, city dwellers are a mixture of individuals from different countries
inquisitiveness. The centre also offers a preschool room for children aged 3-5 years which offers
a preschool program taught by qualified early childhood instructors with bachelors’ degree and
are aimed at the acquisition of knowledge, social skills and numeracy to prepare the children for
future schooling (Sydney Cove Children’s Centre, n.d.).
Sydney is the most populous and busiest city of Australia occupied by about five million people.
It has a median age of 35 years and each household has approximately 2.7 members. English
speakers are the majority (27%) followed by Australians (25%), Chinese (10.8%) among others
with Korean (1.4%) and Maltese (1.3%) accounting for the least. Therefore, Sydney is a hub of
several migrant communities with the Indigenous community accounting for 1.5% of the total
population (ABS, 2016).
According to the Australian Bureau of Statistics (2016), 52.7% of the population is male and
female are 47.3%. Family statistics show that there are approximately 18,977 families with
approximately 1.5 children in each family with children and 0.2 for all families. There is an
average of 53,316 private residentials with an average people per household of 2. Children aged
0-4 years are approximately 2,983. 35% of the people in Sydney were attending an academic
institution out of which 33.0% were in higher education, 5.8% in primary school and 4.5% in
secondary school. Regarding employment, 60,399 were employees during the 2016 census out of
which 64.7% were in full-time employment, 26.1% were in part-time employment and 5.1%
were unemployed (ABS, 2016).
Based on the above demographic characteristics, Sydney is a very busy city occupied with
families thus necessitating the need for accessible childcare centres such as the Sydney Cove
Children’s Centre. Moreover, city dwellers are a mixture of individuals from different countries
Diseases 4
and cultures. This is important because it determines the language and curriculum to be used in
the childcare centres that doesn’t segregate those from foreign cultures.
1.2 Etiology and epidemiology of overweight and obesity in the target group
1.2.1 Epidemiology
Over 124 million children and teenagers aged 5-19 years worldwide are obese with the incidence
rates (over 20%) being the highest the Caribbean, North Africa, and the Middle East. USA has
the highest prevalence of childhood obesity among the 34 country members of the Organization
for Economic Co-operation and Development with Australia taking the 5th position (Abarca-
Gómez et al., 2017). The incidence of obesity among primary school kids in Australia in 2015
was 22.9%, with obesity accounting for 7.1% (Hardy, King, Espinel, Cosgrove, & Bauman,
2016). The frequency of acute obesity rose in the same age category (Garnett, Baur, Jones, &
Hardy, 2016). The continuous widening gap of socioeconomic imbalances increases the
prevalence rates in children from lower socioeconomic status families (Hardy et al., 2016).
The pervasiveness of obesity and overweight among Indigenous Australian children is much
higher than non-Indigenous children. Research has indicated that Indigenous children residing in
rural parts have minimal incidences of obesity and overweight compared with their counterparts
in the city (Dyer et al., 2016). The incidence of obesity and overweight varies depending on the
race, ethnicity and socioeconomic factors. Childhood obesity is on the rise among different races
in the US (Maahs et al., 2014). It is also more common in populations of low socioeconomic
status. Childhood obesity and overweight is significantly determined by hereditary factors.
Obesity and overweight in a single parent predispose the child to obesity three times and up to
fifteen times if both parents are obese (Jiang, Yang, Guo, & Sun, 2013).
An overwhelming increase in childhood obesity has been observed in school-aged children and
early teenagers aged 6-11 years and 12-19 years respectively between 2009 and 2010 (Ogden,
and cultures. This is important because it determines the language and curriculum to be used in
the childcare centres that doesn’t segregate those from foreign cultures.
1.2 Etiology and epidemiology of overweight and obesity in the target group
1.2.1 Epidemiology
Over 124 million children and teenagers aged 5-19 years worldwide are obese with the incidence
rates (over 20%) being the highest the Caribbean, North Africa, and the Middle East. USA has
the highest prevalence of childhood obesity among the 34 country members of the Organization
for Economic Co-operation and Development with Australia taking the 5th position (Abarca-
Gómez et al., 2017). The incidence of obesity among primary school kids in Australia in 2015
was 22.9%, with obesity accounting for 7.1% (Hardy, King, Espinel, Cosgrove, & Bauman,
2016). The frequency of acute obesity rose in the same age category (Garnett, Baur, Jones, &
Hardy, 2016). The continuous widening gap of socioeconomic imbalances increases the
prevalence rates in children from lower socioeconomic status families (Hardy et al., 2016).
The pervasiveness of obesity and overweight among Indigenous Australian children is much
higher than non-Indigenous children. Research has indicated that Indigenous children residing in
rural parts have minimal incidences of obesity and overweight compared with their counterparts
in the city (Dyer et al., 2016). The incidence of obesity and overweight varies depending on the
race, ethnicity and socioeconomic factors. Childhood obesity is on the rise among different races
in the US (Maahs et al., 2014). It is also more common in populations of low socioeconomic
status. Childhood obesity and overweight is significantly determined by hereditary factors.
Obesity and overweight in a single parent predispose the child to obesity three times and up to
fifteen times if both parents are obese (Jiang, Yang, Guo, & Sun, 2013).
An overwhelming increase in childhood obesity has been observed in school-aged children and
early teenagers aged 6-11 years and 12-19 years respectively between 2009 and 2010 (Ogden,
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Diseases 5
Carroll, Kit, & Flegal, 2012). There is limited research that suggests that the incidence of obesity
and overweight in preschool-aged children has decreased from 13.9% to 8.4% in 2004 and 2011
respectively (Ogden, Carroll, Kit, & Flegal, 2014). Notwithstanding the overall incidence of
obesity and overweight in children in the US, the rate of acute obesity in children of over two
years is still alarming. According to the study by Skinner and Skelton (2014) carried out in 2012,
9.5% of the children were diagnosed with acute obesity (BMI>=120%).
1.2.2 Etiology
Obesity and overweight in children are as a result of an interface among an intricate combination
of aspects that are linked to the setting, heredities and environmental impacts e.g. the
community, institution and the family. The ecological aspects for obesity and overweight in
children are intricate (Mouchacca, Abbott, & Ball, 2013). Studies have shown that emotional and
psychological suffering influence excessive increase in weight in children through maladaptive
managing tactics like consuming food to conquer harmful feelings, control of appetite, and
inflammation (Hemmingsson, 2014; Waters et al., 2011). The dietary conduct in children and the
subsequent increase in the risk of diabetes are linked with dietary patters of the family, and
anxiety (El-Behadli, Sharp, Hughes, Obasi, & Nicklas, 2015). Environmental changes leading to
high food consumption have been associated with risk factors to low energy use such as
inactivity and a lot of time used in phones and television watching. Studies have documented a
link between the time occupied in tv watching in a bedroom of a child and the incidence of
obesity and overweight, (Banfield, Liu, Davis, Chang, & Frazier-Wood, 2016).
The 50% differences in adiposity can be explained by heritable factors. Studies have identified
multiple single-gene flaws associated with obesity. Children diagnosed with genetic syndromes
related to obesity have an initial commencement of obesity and notable features during the
physical assessment that is short stature, retarded development, mental retardation. Mutations in
Carroll, Kit, & Flegal, 2012). There is limited research that suggests that the incidence of obesity
and overweight in preschool-aged children has decreased from 13.9% to 8.4% in 2004 and 2011
respectively (Ogden, Carroll, Kit, & Flegal, 2014). Notwithstanding the overall incidence of
obesity and overweight in children in the US, the rate of acute obesity in children of over two
years is still alarming. According to the study by Skinner and Skelton (2014) carried out in 2012,
9.5% of the children were diagnosed with acute obesity (BMI>=120%).
1.2.2 Etiology
Obesity and overweight in children are as a result of an interface among an intricate combination
of aspects that are linked to the setting, heredities and environmental impacts e.g. the
community, institution and the family. The ecological aspects for obesity and overweight in
children are intricate (Mouchacca, Abbott, & Ball, 2013). Studies have shown that emotional and
psychological suffering influence excessive increase in weight in children through maladaptive
managing tactics like consuming food to conquer harmful feelings, control of appetite, and
inflammation (Hemmingsson, 2014; Waters et al., 2011). The dietary conduct in children and the
subsequent increase in the risk of diabetes are linked with dietary patters of the family, and
anxiety (El-Behadli, Sharp, Hughes, Obasi, & Nicklas, 2015). Environmental changes leading to
high food consumption have been associated with risk factors to low energy use such as
inactivity and a lot of time used in phones and television watching. Studies have documented a
link between the time occupied in tv watching in a bedroom of a child and the incidence of
obesity and overweight, (Banfield, Liu, Davis, Chang, & Frazier-Wood, 2016).
The 50% differences in adiposity can be explained by heritable factors. Studies have identified
multiple single-gene flaws associated with obesity. Children diagnosed with genetic syndromes
related to obesity have an initial commencement of obesity and notable features during the
physical assessment that is short stature, retarded development, mental retardation. Mutations in
Diseases 6
the melanocortin 4 receptors are the major single-gene flaw that has been recognized in diabetic
children (Fernandez, Klimentidis, Dulin-Keita, & Casazza, 2012). Epigenetic factors are also
influential in the increase of obesity cases. Such aspects can alter the These factors may alter the
interface of the setting, genetic, and diet in fostering obesity (Chang & Neu, 2015). Endocrine
disorders also contribute to the frequency obesity and overweight. However, they are
accountable for only less than 1% of children and teenagers (Kumar, & Kelly, 2017). Majority of
the children diagnosed with the endocrine disease have increased weight gain and poor linear
development, and short stature.
1.3 Justification of stakeholder group selection
The selected intervention for this study is the Nutrition and Physical Activity Self-Assessment
for Child Care (NAP SACC). The potential stakeholders include childcare providers, technical
assistance consultants, early care and education professionals, and parents. Childcare providers
will be critical in the implementation phase of the intervention since it is implemented in a
childcare setting and they will be responsible for the assessment of the overall environment. The
technical assistance consultants will also be critical in the development of an action plan to foster
the area of a target. Moreover, the NPA SACC consultants will also deliver routine education
seminars on childhood obesity, healthy diet for children and physical activity for children. The
NAP SACC technical consultants will also offer continuous technical help through individual
visits and follow-up via telephone. They will also be important in the implementation of
scheduled policy, practice and ecological shifts. Early care and educational professionals are
potential stakeholders because they will also offer advisory services on the legal framework
within which the intervention will be implemented. Furthermore, they will be critical in the
the melanocortin 4 receptors are the major single-gene flaw that has been recognized in diabetic
children (Fernandez, Klimentidis, Dulin-Keita, & Casazza, 2012). Epigenetic factors are also
influential in the increase of obesity cases. Such aspects can alter the These factors may alter the
interface of the setting, genetic, and diet in fostering obesity (Chang & Neu, 2015). Endocrine
disorders also contribute to the frequency obesity and overweight. However, they are
accountable for only less than 1% of children and teenagers (Kumar, & Kelly, 2017). Majority of
the children diagnosed with the endocrine disease have increased weight gain and poor linear
development, and short stature.
1.3 Justification of stakeholder group selection
The selected intervention for this study is the Nutrition and Physical Activity Self-Assessment
for Child Care (NAP SACC). The potential stakeholders include childcare providers, technical
assistance consultants, early care and education professionals, and parents. Childcare providers
will be critical in the implementation phase of the intervention since it is implemented in a
childcare setting and they will be responsible for the assessment of the overall environment. The
technical assistance consultants will also be critical in the development of an action plan to foster
the area of a target. Moreover, the NPA SACC consultants will also deliver routine education
seminars on childhood obesity, healthy diet for children and physical activity for children. The
NAP SACC technical consultants will also offer continuous technical help through individual
visits and follow-up via telephone. They will also be important in the implementation of
scheduled policy, practice and ecological shifts. Early care and educational professionals are
potential stakeholders because they will also offer advisory services on the legal framework
within which the intervention will be implemented. Furthermore, they will be critical in the
Diseases 7
evaluation of adequate physical activity, recommended dietary patterns and recommended BMI
for the children based on their body physiology (Battista et al., 2014).
1.4 Description of the intervention
Nutrition and Physical Activity Self-Assessment for Child Care (NAP SACC) Program
The NAP SACC program is an ecological approach to implement changes in the dietary and
physical activity events, procedures and structural setting of the child-care centers with a
particular focus on attaining a healthy weight for young children. The goal of the program is to
foster appropriated dietary practices and activity among the children in childcare and preschool
environment. The NAP SACC consists of multiple elements such as self-assessment tool,
ongoing education seminars, joint action planning and technical assistance equipment. The
design of the intervention is such that it was to be implemented through an established
organization of public health experts that are licensed nurses and health instructors trained as
NAP SACC consultants (Martin, Martin, Cook, Knaus, & O'Rourke, 2015). The program is
expected to take six months for intervention with the following main steps:
1. Childcare centre directors and major employees complete the individual evaluation tool
to evaluate centre dietary patterns and physical activity procedures, norms and general
setting.
2. The NAP SACC counsellors collaborate with the centre's administration to design an an
implementation guide to advance no less than three areas of target previously identified
through the individual evaluation tool.
3. The NAP SACC counsellors offer five NAP SACC ongoing literacy seminars to centre
employees on i) childhood obesity and overweight, 2) recommended dietary patterns for
evaluation of adequate physical activity, recommended dietary patterns and recommended BMI
for the children based on their body physiology (Battista et al., 2014).
1.4 Description of the intervention
Nutrition and Physical Activity Self-Assessment for Child Care (NAP SACC) Program
The NAP SACC program is an ecological approach to implement changes in the dietary and
physical activity events, procedures and structural setting of the child-care centers with a
particular focus on attaining a healthy weight for young children. The goal of the program is to
foster appropriated dietary practices and activity among the children in childcare and preschool
environment. The NAP SACC consists of multiple elements such as self-assessment tool,
ongoing education seminars, joint action planning and technical assistance equipment. The
design of the intervention is such that it was to be implemented through an established
organization of public health experts that are licensed nurses and health instructors trained as
NAP SACC consultants (Martin, Martin, Cook, Knaus, & O'Rourke, 2015). The program is
expected to take six months for intervention with the following main steps:
1. Childcare centre directors and major employees complete the individual evaluation tool
to evaluate centre dietary patterns and physical activity procedures, norms and general
setting.
2. The NAP SACC counsellors collaborate with the centre's administration to design an an
implementation guide to advance no less than three areas of target previously identified
through the individual evaluation tool.
3. The NAP SACC counsellors offer five NAP SACC ongoing literacy seminars to centre
employees on i) childhood obesity and overweight, 2) recommended dietary patterns for
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diseases 8
children 3) active lifestyle, 4) individual welfare of employees , and 5) incorporating
families
4. NAP SACC counsellors offer continuous technical aid, through personal visits and via
mobile follow-up, to promote the actualization of an established procedure, exercise, and
ecological variations
5. The centres then complete a follow-up individual evaluation tool to assess the changes
previously implemented over 6 months.
(Martin et al., 2015)
1.4.1 Development of the individual evaluation tool and seminars
A self-assessment instrument is important in improving childcare settings more than other
existing rating scales for childcare quality. Moreover, the individual evaluation tool will be
important in focusing on the areas of interest and provide more workable advancements through
willful involvement and self-initiated change. Moreover, centre-directed evaluation permits a
childcare environment to assess their dietary pattern and physical activity settings without
consequences from the governing agencies. Furthermore, the tool is fast and easy, and it is made
to permit the childcare centre administrator to respond to queries with the help of the major
employee. The initial evaluation will consist of 44 questions obtained from 9 nutrition and 6
physical activity areas with previous evidence-based or professional-based association to
childhood obesity (Blaine et al., 2015).
1.4.2 Barriers to implementation
The implementation of the NAP SACC program is likely to be affected by several barriers. One
of the potential barriers to its implementation is the reliance on NAP SACC consultants to recruit
early care and education program administrators and to help them with implementation. The
provision of the local technical assistance is a significant implementation strategy but the un-
children 3) active lifestyle, 4) individual welfare of employees , and 5) incorporating
families
4. NAP SACC counsellors offer continuous technical aid, through personal visits and via
mobile follow-up, to promote the actualization of an established procedure, exercise, and
ecological variations
5. The centres then complete a follow-up individual evaluation tool to assess the changes
previously implemented over 6 months.
(Martin et al., 2015)
1.4.1 Development of the individual evaluation tool and seminars
A self-assessment instrument is important in improving childcare settings more than other
existing rating scales for childcare quality. Moreover, the individual evaluation tool will be
important in focusing on the areas of interest and provide more workable advancements through
willful involvement and self-initiated change. Moreover, centre-directed evaluation permits a
childcare environment to assess their dietary pattern and physical activity settings without
consequences from the governing agencies. Furthermore, the tool is fast and easy, and it is made
to permit the childcare centre administrator to respond to queries with the help of the major
employee. The initial evaluation will consist of 44 questions obtained from 9 nutrition and 6
physical activity areas with previous evidence-based or professional-based association to
childhood obesity (Blaine et al., 2015).
1.4.2 Barriers to implementation
The implementation of the NAP SACC program is likely to be affected by several barriers. One
of the potential barriers to its implementation is the reliance on NAP SACC consultants to recruit
early care and education program administrators and to help them with implementation. The
provision of the local technical assistance is a significant implementation strategy but the un-
Diseases 9
availability of consultants, the necessity for distinct training, and the insufficient funds for
consultant time implies that NAP SACC program will not be available most of the times or could
only be promoted in a few early cares and education programs, Evers, Davis, Maalouf, & Griffin,
2014).
Another potential barrier is the possibility of slow internet service which is common in rural
areas in which the childcare centres are found. This is also associated with computer illiteracy.
The program requires internet connectivity and computer literacy without which it would be
impossible to implement it. This will necessitate the need for computer training, thus increasing
the cost of implementation. Studies on the effectiveness of the NAP SACC program have
generally received limited attention to date (Ward, Vaughn, Mazzucca, & Burney, 2017)
especially in programs associated with child nutrition. Some early care and education (ECE)
technical assistance agencies are likely to be reluctant to the use of online tools with ECE
programs due to their perception of the limited computer knowledge and internet skills among
ECE providers.
1.5 Outline of the communication strategy
The communication strategy for NAP SACC intervention program will include 7 steps namely
identification of stakeholders, identification of stakeholder prospects, identify the
communication appropriate for communicating stakeholder expectations, identify time-frame or
frequency of communication, determine the preferred communication channel of the stakeholder,
assign communication duties and document items.
1. Identification of stakeholders: The potential stakeholders for the intervention include
parents, director and staff of childcare centre, early care and education professionals.
availability of consultants, the necessity for distinct training, and the insufficient funds for
consultant time implies that NAP SACC program will not be available most of the times or could
only be promoted in a few early cares and education programs, Evers, Davis, Maalouf, & Griffin,
2014).
Another potential barrier is the possibility of slow internet service which is common in rural
areas in which the childcare centres are found. This is also associated with computer illiteracy.
The program requires internet connectivity and computer literacy without which it would be
impossible to implement it. This will necessitate the need for computer training, thus increasing
the cost of implementation. Studies on the effectiveness of the NAP SACC program have
generally received limited attention to date (Ward, Vaughn, Mazzucca, & Burney, 2017)
especially in programs associated with child nutrition. Some early care and education (ECE)
technical assistance agencies are likely to be reluctant to the use of online tools with ECE
programs due to their perception of the limited computer knowledge and internet skills among
ECE providers.
1.5 Outline of the communication strategy
The communication strategy for NAP SACC intervention program will include 7 steps namely
identification of stakeholders, identification of stakeholder prospects, identify the
communication appropriate for communicating stakeholder expectations, identify time-frame or
frequency of communication, determine the preferred communication channel of the stakeholder,
assign communication duties and document items.
1. Identification of stakeholders: The potential stakeholders for the intervention include
parents, director and staff of childcare centre, early care and education professionals.
Diseases 10
2. Identification of stakeholder prospects: the possible expectations of the potential
stakeholders include healthy eating, physical activity and reduced sedentary behaviour, program
recognition, implementation of nutritional guidelines, healthy weight and improved quality of
life.
3. Determining appropriate communication messages to the stakeholders: the messages for
each intervention level will be communicated separately depending on the assessment of the
indicators. For instance, at the individual assessment level, the reports will consist of the need
and willingness of the centre to adopt the proposed changes.
4. Time-frame or frequency of communication: the intervention will take 6 months but
communication for each level of implementation will be made to the relevant stakeholders after 2
months. This is to ensure that the relevant parties of interest are updated on the progress of the
implementation
5. Communication Channel: the major channels of communication will include emails and any
preferred social media platform by the stakeholder
6. Communication responsibility: a designated secretary will be responsible for all
communications
7. Documentation: All communications and partial or complete reports will be documented in
the acceptable formats and templates
1.6 Outline of the evaluation framework
The Supplemental Nutrition Assistance Program Education (SNAP-ED) Evaluation Framework
will be used in evaluating the implementation of the NAP SACC intervention program. The
SNAP-ED framework utilizes the social-ecological model to the nutrition, physical activity and
prevention of obesity. The Framework has three levels of evaluation namely individual,
2. Identification of stakeholder prospects: the possible expectations of the potential
stakeholders include healthy eating, physical activity and reduced sedentary behaviour, program
recognition, implementation of nutritional guidelines, healthy weight and improved quality of
life.
3. Determining appropriate communication messages to the stakeholders: the messages for
each intervention level will be communicated separately depending on the assessment of the
indicators. For instance, at the individual assessment level, the reports will consist of the need
and willingness of the centre to adopt the proposed changes.
4. Time-frame or frequency of communication: the intervention will take 6 months but
communication for each level of implementation will be made to the relevant stakeholders after 2
months. This is to ensure that the relevant parties of interest are updated on the progress of the
implementation
5. Communication Channel: the major channels of communication will include emails and any
preferred social media platform by the stakeholder
6. Communication responsibility: a designated secretary will be responsible for all
communications
7. Documentation: All communications and partial or complete reports will be documented in
the acceptable formats and templates
1.6 Outline of the evaluation framework
The Supplemental Nutrition Assistance Program Education (SNAP-ED) Evaluation Framework
will be used in evaluating the implementation of the NAP SACC intervention program. The
SNAP-ED framework utilizes the social-ecological model to the nutrition, physical activity and
prevention of obesity. The Framework has three levels of evaluation namely individual,
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Diseases 11
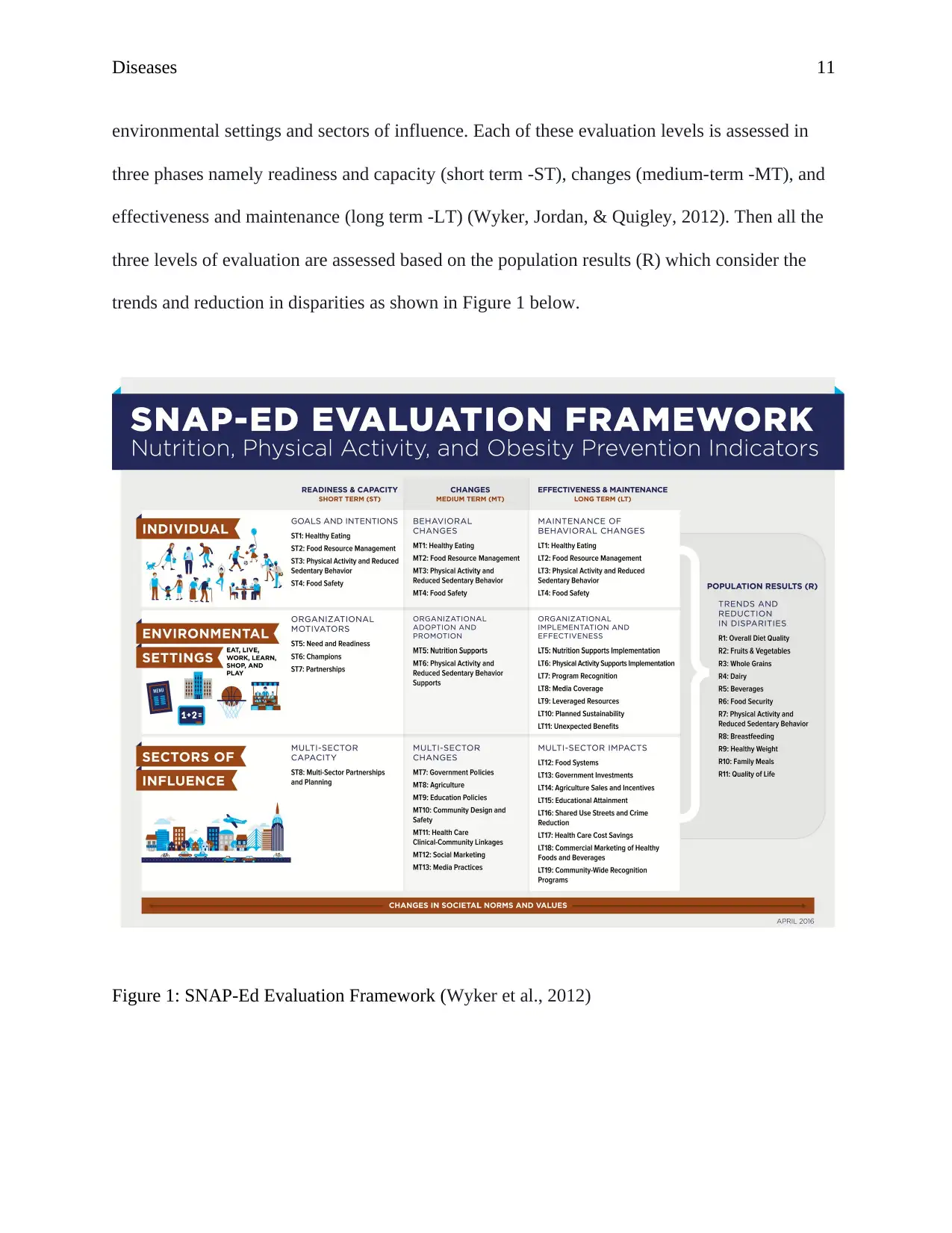
environmental settings and sectors of influence. Each of these evaluation levels is assessed in
three phases namely readiness and capacity (short term -ST), changes (medium-term -MT), and
effectiveness and maintenance (long term -LT) (Wyker, Jordan, & Quigley, 2012). Then all the
three levels of evaluation are assessed based on the population results (R) which consider the
trends and reduction in disparities as shown in Figure 1 below.
Figure 1: SNAP-Ed Evaluation Framework (Wyker et al., 2012)
environmental settings and sectors of influence. Each of these evaluation levels is assessed in
three phases namely readiness and capacity (short term -ST), changes (medium-term -MT), and
effectiveness and maintenance (long term -LT) (Wyker, Jordan, & Quigley, 2012). Then all the
three levels of evaluation are assessed based on the population results (R) which consider the
trends and reduction in disparities as shown in Figure 1 below.
Figure 1: SNAP-Ed Evaluation Framework (Wyker et al., 2012)
Diseases 12
Individual-level
The SNAP-ED framework aims at determining the degree to which the intervention improves
and maintains healthy eating and physical activity behaviours of the participants. The short-term
indicators are the initial steps towards behaviour change, for example, the participants’ goals and
motives regarding nutrition and physical activity. Behaviour change in the medium term is
determined using multiple parameters such as healthy eating, decrease in sedentary behaviour,
physical activity and the management of food resources- based on the area of focus of the
intervention. For pre-school children, the study will use the Visually-Enhanced Food Behavior
Checklist before and after implementation. The long-term indicators evaluate the sustainability
of the observed and recorded behaviour changes within 6 months after the successful completion
of the program (Ward, Vaughn, Mazzucca, & Burney, 2017).
Environmental level
This evaluation level aims at determining the degree to which the intervention create and
maintain access and plea for healthy eating and physical activity options in the environment
where the participants eat, learn, play, and reside. The short-term indicators include the need and
readiness of the childcare centre in addition to the readiness of the employees to accept and
embrace changes. Medium-term indicators assess the childcare centres adoption of policies,
systems, and environments (PSEs) for instance, integrating physical activity breaks during the
routine class sessions in addition to the number of learners reached by the changes. Long-term
indicators assess the implementation and if the significant elements for successful results are
present such as parent involvement and training. Studies in the effectiveness of SNAP-ED
Individual-level
The SNAP-ED framework aims at determining the degree to which the intervention improves
and maintains healthy eating and physical activity behaviours of the participants. The short-term
indicators are the initial steps towards behaviour change, for example, the participants’ goals and
motives regarding nutrition and physical activity. Behaviour change in the medium term is
determined using multiple parameters such as healthy eating, decrease in sedentary behaviour,
physical activity and the management of food resources- based on the area of focus of the
intervention. For pre-school children, the study will use the Visually-Enhanced Food Behavior
Checklist before and after implementation. The long-term indicators evaluate the sustainability
of the observed and recorded behaviour changes within 6 months after the successful completion
of the program (Ward, Vaughn, Mazzucca, & Burney, 2017).
Environmental level
This evaluation level aims at determining the degree to which the intervention create and
maintain access and plea for healthy eating and physical activity options in the environment
where the participants eat, learn, play, and reside. The short-term indicators include the need and
readiness of the childcare centre in addition to the readiness of the employees to accept and
embrace changes. Medium-term indicators assess the childcare centres adoption of policies,
systems, and environments (PSEs) for instance, integrating physical activity breaks during the
routine class sessions in addition to the number of learners reached by the changes. Long-term
indicators assess the implementation and if the significant elements for successful results are
present such as parent involvement and training. Studies in the effectiveness of SNAP-ED

Diseases 13
interventions in cities reported improvement in physical activity scores of the school-going
children (Mehtälä, Sääkslahti, Inkinen, & Poskiparta, 2014).
Sectors of influence
The sector of influence level of assessment evaluates the degree to which the intervention
collaborates with other stakeholders both in the private and public sector to mutually impact long
term healthy eating and physical activity level in the most vulnerable communities. An intricate
of factors that lead to chronic diseases for instance food insecurity and overweight among others
require a wider frame. The short-term indicator aims at assessing the quality of multi-sector
collaborations that are dealing with changes in nutrition or physical activity. The intervention is
assessed on the nature of partners such as agriculture, media, food industry among others to
increase accessibility to healthy foods and establish settings that are favourable to active lives
(Ward et al., 2017).
Population results
The assessment of the population results is aimed at determining the degree to which the
intervention helps attain the standard recommendations by the Dietary Guidelines for Americans
(DGA) and the World Health Organization. The population results are measured based on the
trends and reduction in disparities. The specific parameters used include overall diet quality,
whole grains, healthy weight, food security, physical activity and reduced sedentary lifestyle
among others (Ward et al., 2017).
interventions in cities reported improvement in physical activity scores of the school-going
children (Mehtälä, Sääkslahti, Inkinen, & Poskiparta, 2014).
Sectors of influence
The sector of influence level of assessment evaluates the degree to which the intervention
collaborates with other stakeholders both in the private and public sector to mutually impact long
term healthy eating and physical activity level in the most vulnerable communities. An intricate
of factors that lead to chronic diseases for instance food insecurity and overweight among others
require a wider frame. The short-term indicator aims at assessing the quality of multi-sector
collaborations that are dealing with changes in nutrition or physical activity. The intervention is
assessed on the nature of partners such as agriculture, media, food industry among others to
increase accessibility to healthy foods and establish settings that are favourable to active lives
(Ward et al., 2017).
Population results
The assessment of the population results is aimed at determining the degree to which the
intervention helps attain the standard recommendations by the Dietary Guidelines for Americans
(DGA) and the World Health Organization. The population results are measured based on the
trends and reduction in disparities. The specific parameters used include overall diet quality,
whole grains, healthy weight, food security, physical activity and reduced sedentary lifestyle
among others (Ward et al., 2017).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Diseases 14
References
Abarca-Gómez, L., Abdeen, Z. A., Hamid, Z. A., Abu-Rmeileh, N. M., Acosta-Cazares, B.,
Acuin, C., ... & Agyemang, C. (2017). Worldwide trends in body-mass index,
underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416
population-based measurement studies in 128· 9 million children, adolescents, and
adults. The Lancet, 390(10113), 2627-2642.
Australian Bureau of Statistics (ABS). (2016). 2016 Census QuickStats. Retrieved from
https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/
quickstat/SED10080
Australian Department of Education. (2017). Early Years Learning Framework. Retrieved from
https://www.education.gov.au/early-years-learning-framework-0
Banfield, E. C., Liu, Y., Davis, J. S., Chang, S., & Frazier-Wood, A. C. (2016). Poor adherence
to US dietary guidelines for children and adolescents in the national health and nutrition
examination survey population. Journal of the Academy of Nutrition and
Dietetics, 116(1), 21-27.
Battista, R. A., Oakley, H., Weddell, M. S., Mudd, L. M., Greene, J. B., & West, S. T. (2014).
Improving the physical activity and nutrition environment through self-assessment (NAP
SACC) in rural area child care centers in North Carolina. Preventive medicine, 67, S10-
S16.
Blaine, R. E., Davison, K. K., Hesketh, K., Taveras, E. M., Gillman, M. W., & Benjamin Neelon,
References
Abarca-Gómez, L., Abdeen, Z. A., Hamid, Z. A., Abu-Rmeileh, N. M., Acosta-Cazares, B.,
Acuin, C., ... & Agyemang, C. (2017). Worldwide trends in body-mass index,
underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416
population-based measurement studies in 128· 9 million children, adolescents, and
adults. The Lancet, 390(10113), 2627-2642.
Australian Bureau of Statistics (ABS). (2016). 2016 Census QuickStats. Retrieved from
https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/
quickstat/SED10080
Australian Department of Education. (2017). Early Years Learning Framework. Retrieved from
https://www.education.gov.au/early-years-learning-framework-0
Banfield, E. C., Liu, Y., Davis, J. S., Chang, S., & Frazier-Wood, A. C. (2016). Poor adherence
to US dietary guidelines for children and adolescents in the national health and nutrition
examination survey population. Journal of the Academy of Nutrition and
Dietetics, 116(1), 21-27.
Battista, R. A., Oakley, H., Weddell, M. S., Mudd, L. M., Greene, J. B., & West, S. T. (2014).
Improving the physical activity and nutrition environment through self-assessment (NAP
SACC) in rural area child care centers in North Carolina. Preventive medicine, 67, S10-
S16.
Blaine, R. E., Davison, K. K., Hesketh, K., Taveras, E. M., Gillman, M. W., & Benjamin Neelon,
Diseases 15
S. E. (2015). Child care provider adherence to infant and toddler feeding
recommendations: findings from the Baby Nutrition and Physical Activity Self-
Assessment for Child Care (Baby NAP SACC) Study. Childhood obesity, 11(3), 304-
313.
Chang, L., & Neu, J. (2015). Early factors leading to later obesity: interactions of the
microbiome, epigenome, and nutrition. Current problems in pediatric and adolescent
health care, 45(5), 134-142.
Dyer, S. M., Gomersall, J. S., Smithers, L. G., Davy, C., Coleman, D. T., & Street, J. M. (2017).
Prevalence and characteristics of overweight and obesity in indigenous Australian
children: a systematic review. Critical reviews in food science and nutrition, 57(7), 1365-
1376.
El-Behadli, A. F., Sharp, C., Hughes, S. O., Obasi, E. M., & Nicklas, T. A. (2015). Maternal
depression, stress and feeding styles: towards a framework for theory and research in
child obesity. British journal of nutrition, 113(S1), S55-S71.
Fernandez, J. R., Klimentidis, Y. C., Dulin-Keita, A., & Casazza, K. (2012). Genetic influences
in childhood obesity: recent progress and recommendations for experimental
designs. International Journal of Obesity, 479.
Garnett, S. P., Baur, L. A., Jones, A. M., & Hardy, L. L. (2016). Trends in the prevalence of
morbid and severe obesity in Australian children aged 7-15 years, 1985-2012. PloS
one, 11(5), e0154879.
S. E. (2015). Child care provider adherence to infant and toddler feeding
recommendations: findings from the Baby Nutrition and Physical Activity Self-
Assessment for Child Care (Baby NAP SACC) Study. Childhood obesity, 11(3), 304-
313.
Chang, L., & Neu, J. (2015). Early factors leading to later obesity: interactions of the
microbiome, epigenome, and nutrition. Current problems in pediatric and adolescent
health care, 45(5), 134-142.
Dyer, S. M., Gomersall, J. S., Smithers, L. G., Davy, C., Coleman, D. T., & Street, J. M. (2017).
Prevalence and characteristics of overweight and obesity in indigenous Australian
children: a systematic review. Critical reviews in food science and nutrition, 57(7), 1365-
1376.
El-Behadli, A. F., Sharp, C., Hughes, S. O., Obasi, E. M., & Nicklas, T. A. (2015). Maternal
depression, stress and feeding styles: towards a framework for theory and research in
child obesity. British journal of nutrition, 113(S1), S55-S71.
Fernandez, J. R., Klimentidis, Y. C., Dulin-Keita, A., & Casazza, K. (2012). Genetic influences
in childhood obesity: recent progress and recommendations for experimental
designs. International Journal of Obesity, 479.
Garnett, S. P., Baur, L. A., Jones, A. M., & Hardy, L. L. (2016). Trends in the prevalence of
morbid and severe obesity in Australian children aged 7-15 years, 1985-2012. PloS
one, 11(5), e0154879.
Diseases 16
Hardy, L. L., King, L., Espinel, P., Cosgrove, C., & Bauman, A. (2016). NSW schools physical
activity and nutrition survey (SPANS) 2010: Full Report. 2011. Sydney: NSW Ministry of
Health, 1-387.
Hemmingsson, E. (2014). A new model of the role of psychological and emotional distress in
promoting obesity: conceptual review with implications for treatment and
prevention. Obesity Reviews, 15(9), 769-779.
Jiang, M. H., Yang, Y., Guo, X. F., & Sun, Y. X. (2013). Association between child and
adolescent obesity and parental weight status: a cross-sectional study from rural North
China. Journal of International Medical Research, 41(4), 1326-1332.
Kumar, S., & Kelly, A. S. (2017, February). Review of childhood obesity: from epidemiology,
etiology, and comorbidities to clinical assessment and treatment. In Mayo Clinic
Proceedings (Vol. 92, No. 2, pp. 251-265). Elsevier.
Lyn, R., Evers, S., Davis, J., Maalouf, J., & Griffin, M. (2014). Barriers and supports to
implementing a nutrition and physical activity intervention in child care: directors'
perspectives. Journal of nutrition education and behavior, 46(3), 171-180.
Maahs, D. M., Daniels, S. R., De Ferranti, S. D., Dichek, H. L., Flynn, J., Goldstein, B. I., ... &
Quinn, L. (2014). Cardiovascular disease risk factors in youth with diabetes mellitus: a
scientific statement from the American Heart Association. Circulation, 130(17), 1532-
1558.
Martin, S. L., Martin, M. W., Cook, B., Knaus, R., & O'Rourke, K. (2015). Notes from the field:
Hardy, L. L., King, L., Espinel, P., Cosgrove, C., & Bauman, A. (2016). NSW schools physical
activity and nutrition survey (SPANS) 2010: Full Report. 2011. Sydney: NSW Ministry of
Health, 1-387.
Hemmingsson, E. (2014). A new model of the role of psychological and emotional distress in
promoting obesity: conceptual review with implications for treatment and
prevention. Obesity Reviews, 15(9), 769-779.
Jiang, M. H., Yang, Y., Guo, X. F., & Sun, Y. X. (2013). Association between child and
adolescent obesity and parental weight status: a cross-sectional study from rural North
China. Journal of International Medical Research, 41(4), 1326-1332.
Kumar, S., & Kelly, A. S. (2017, February). Review of childhood obesity: from epidemiology,
etiology, and comorbidities to clinical assessment and treatment. In Mayo Clinic
Proceedings (Vol. 92, No. 2, pp. 251-265). Elsevier.
Lyn, R., Evers, S., Davis, J., Maalouf, J., & Griffin, M. (2014). Barriers and supports to
implementing a nutrition and physical activity intervention in child care: directors'
perspectives. Journal of nutrition education and behavior, 46(3), 171-180.
Maahs, D. M., Daniels, S. R., De Ferranti, S. D., Dichek, H. L., Flynn, J., Goldstein, B. I., ... &
Quinn, L. (2014). Cardiovascular disease risk factors in youth with diabetes mellitus: a
scientific statement from the American Heart Association. Circulation, 130(17), 1532-
1558.
Martin, S. L., Martin, M. W., Cook, B., Knaus, R., & O'Rourke, K. (2015). Notes from the field:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Diseases 17
the evaluation of Maine nutrition and physical activity self-assessment for child care
(NAPSACC) experience. Evaluation & the health professions, 38(1), 140-145.
Mehtälä, M. A. K., Sääkslahti, A. K., Inkinen, M. E., & Poskiparta, M. E. H. (2014). A socio-
ecological approach to physical activity interventions in childcare: a systematic
review. International Journal of Behavioral Nutrition and Physical Activity, 11(1), 22.
Mouchacca, J., Abbott, G. R., & Ball, K. (2013). Associations between psychological stress,
eating, physical activity, sedentary behaviours and body weight among women: a
longitudinal study. BMC public health, 13(1), 828.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2012). Prevalence of obesity and
trends in body mass index among US children and adolescents, 1999-2010. Jama, 307(5),
483-490.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2014). Prevalence of childhood and
adult obesity in the United States, 2011-2012. Jama, 311(8), 806-814.
Skinner, A. C., & Skelton, J. A. (2014). Prevalence and trends in obesity and severe obesity
among children in the United States, 1999-2012. JAMA pediatrics, 168(6), 561-566.
Sydney Cove Children’s Centres .(n.d.). About Us. Retrieved from
https://www.earlylearningservices.com.au/centres/childcare-sydney/
Ward, D. S., Vaughn, A. E., Mazzucca, S., & Burney, R. (2017). Translating a child care based
the evaluation of Maine nutrition and physical activity self-assessment for child care
(NAPSACC) experience. Evaluation & the health professions, 38(1), 140-145.
Mehtälä, M. A. K., Sääkslahti, A. K., Inkinen, M. E., & Poskiparta, M. E. H. (2014). A socio-
ecological approach to physical activity interventions in childcare: a systematic
review. International Journal of Behavioral Nutrition and Physical Activity, 11(1), 22.
Mouchacca, J., Abbott, G. R., & Ball, K. (2013). Associations between psychological stress,
eating, physical activity, sedentary behaviours and body weight among women: a
longitudinal study. BMC public health, 13(1), 828.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2012). Prevalence of obesity and
trends in body mass index among US children and adolescents, 1999-2010. Jama, 307(5),
483-490.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2014). Prevalence of childhood and
adult obesity in the United States, 2011-2012. Jama, 311(8), 806-814.
Skinner, A. C., & Skelton, J. A. (2014). Prevalence and trends in obesity and severe obesity
among children in the United States, 1999-2012. JAMA pediatrics, 168(6), 561-566.
Sydney Cove Children’s Centres .(n.d.). About Us. Retrieved from
https://www.earlylearningservices.com.au/centres/childcare-sydney/
Ward, D. S., Vaughn, A. E., Mazzucca, S., & Burney, R. (2017). Translating a child care based
Diseases 18
intervention for online delivery: development and randomized pilot study of Go
NAPSACC. BMC public health, 17(1), 891.
Waters, E., de Silva‐Sanigorski, A., Burford, B. J., Brown, T., Campbell, K. J., Gao, Y., ... &
Summerbell, C. D. (2011). Interventions for preventing obesity in children. Cochrane
database of systematic reviews, (12).
Wyker, B. A., Jordan, P., & Quigley, D. L. (2012). Evaluation of supplemental nutrition
assistance program education: application of behavioral theory and survey
validation. Journal of nutrition education and behavior, 44(4), 360-364.
intervention for online delivery: development and randomized pilot study of Go
NAPSACC. BMC public health, 17(1), 891.
Waters, E., de Silva‐Sanigorski, A., Burford, B. J., Brown, T., Campbell, K. J., Gao, Y., ... &
Summerbell, C. D. (2011). Interventions for preventing obesity in children. Cochrane
database of systematic reviews, (12).
Wyker, B. A., Jordan, P., & Quigley, D. L. (2012). Evaluation of supplemental nutrition
assistance program education: application of behavioral theory and survey
validation. Journal of nutrition education and behavior, 44(4), 360-364.
1 out of 18






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.