Comprehensive Report on Chronic Obstructive Pulmonary Disease (COPD)
VerifiedAdded on 2023/06/05
|14
|3622
|302
Report
AI Summary
This report provides a detailed overview of Chronic Obstructive Pulmonary Disease (COPD). It begins with an introduction to the disease, its impact, and the systems involved. The report then delves into the anatomy and physiology of the respiratory system, explaining how COPD alters normal lung function. It covers the etiology of COPD, highlighting the primary cause of smoking and other contributing factors like exposure to chemicals and genetic predisposition. The report outlines the various signs and symptoms of COPD, including dyspnea, excess mucus production, fatigue, wheezing, and respiratory infections. It also discusses the investigative procedures and tests used for diagnosis, such as spirometry and laboratory tests. Finally, the report explores the treatment and management options, focusing on bronchodilators and their mechanisms of action. Potential complications are also discussed, offering a comprehensive understanding of COPD.

R AD C R C S R C V M AR D S ASUNNING HE : H ONI OB T U TI E PUL ON Y I E E 1
Chronic Obstructive Pulmonary Disease
Name:
Institution:
Tutor:
Date:
Chronic Obstructive Pulmonary Disease
Name:
Institution:
Tutor:
Date:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 2
Chronic Obstructive Pulmonary Disease
INTRODUCTION
Chronic Obstructive Pulmonary Disease is an infection of the lungs that results to
dyspnea. At the moment, the condition does not have any cure but there are only options that
enables management of the condition. It is an umbrella of different conditions such as
emphysema, chronic bronchitis and finally chronic asthma is irreversible .The condition is
characterized by shortness of breath (Dyspnea), repetitive cough that has phlegm or mucus in
most days.
According to statistics, 14.4% of Australians who are above 40 years’ experience
difficulties in airflow of lungs. The figures increase to 29.2% in Australians who are above 75
years old. Out of this figures, 7.5% of those that have COPD in Australia experience advanced
signs and symptoms that affect their daily lives (Barnes, 2016). Several studies have also found
out that among avoidable hospital admission diseases, COPD is ranked second. Recently, there
has been reduced death rates from COPD. However, the condition still contributes largely to the
mortality rates in Australia after cardiovascular disease, stroke and then cancer. There is no
current cure for the condition but is avoidable. In this assignment, the overview of anatomy and
physiology of systems involved in COPD, etiology, signs and symptoms, investigations and
tests, the treatment and management of COPD and potential complications will be discussed.
OVERVIEW OF ANATOMY AND PHYSIOLOGY
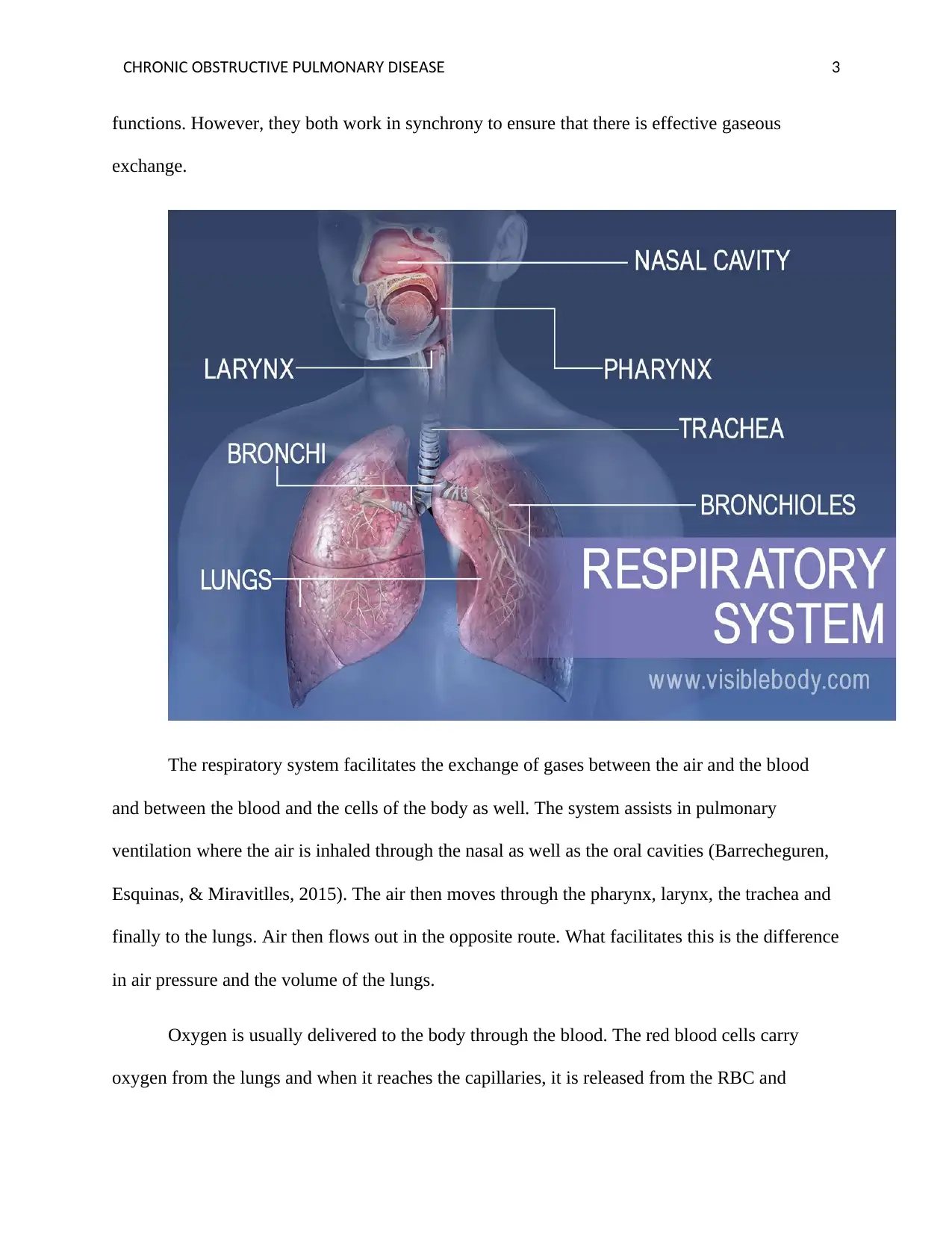
The respiratory system is made up of different structures .They include the nasal cavity,
the larynx, pharynx, trachea, bronchioles, lungs and alveoli. All these structures have different
Chronic Obstructive Pulmonary Disease
INTRODUCTION
Chronic Obstructive Pulmonary Disease is an infection of the lungs that results to
dyspnea. At the moment, the condition does not have any cure but there are only options that
enables management of the condition. It is an umbrella of different conditions such as
emphysema, chronic bronchitis and finally chronic asthma is irreversible .The condition is
characterized by shortness of breath (Dyspnea), repetitive cough that has phlegm or mucus in
most days.
According to statistics, 14.4% of Australians who are above 40 years’ experience
difficulties in airflow of lungs. The figures increase to 29.2% in Australians who are above 75
years old. Out of this figures, 7.5% of those that have COPD in Australia experience advanced
signs and symptoms that affect their daily lives (Barnes, 2016). Several studies have also found
out that among avoidable hospital admission diseases, COPD is ranked second. Recently, there
has been reduced death rates from COPD. However, the condition still contributes largely to the
mortality rates in Australia after cardiovascular disease, stroke and then cancer. There is no
current cure for the condition but is avoidable. In this assignment, the overview of anatomy and
physiology of systems involved in COPD, etiology, signs and symptoms, investigations and
tests, the treatment and management of COPD and potential complications will be discussed.
OVERVIEW OF ANATOMY AND PHYSIOLOGY
The respiratory system is made up of different structures .They include the nasal cavity,
the larynx, pharynx, trachea, bronchioles, lungs and alveoli. All these structures have different
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 3
functions. However, they both work in synchrony to ensure that there is effective gaseous
exchange.
The respiratory system facilitates the exchange of gases between the air and the blood
and between the blood and the cells of the body as well. The system assists in pulmonary
ventilation where the air is inhaled through the nasal as well as the oral cavities (Barrecheguren,
Esquinas, & Miravitlles, 2015). The air then moves through the pharynx, larynx, the trachea and
finally to the lungs. Air then flows out in the opposite route. What facilitates this is the difference
in air pressure and the volume of the lungs.
Oxygen is usually delivered to the body through the blood. The red blood cells carry
oxygen from the lungs and when it reaches the capillaries, it is released from the RBC and
functions. However, they both work in synchrony to ensure that there is effective gaseous
exchange.
The respiratory system facilitates the exchange of gases between the air and the blood
and between the blood and the cells of the body as well. The system assists in pulmonary
ventilation where the air is inhaled through the nasal as well as the oral cavities (Barrecheguren,
Esquinas, & Miravitlles, 2015). The air then moves through the pharynx, larynx, the trachea and
finally to the lungs. Air then flows out in the opposite route. What facilitates this is the difference
in air pressure and the volume of the lungs.
Oxygen is usually delivered to the body through the blood. The red blood cells carry
oxygen from the lungs and when it reaches the capillaries, it is released from the RBC and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 4
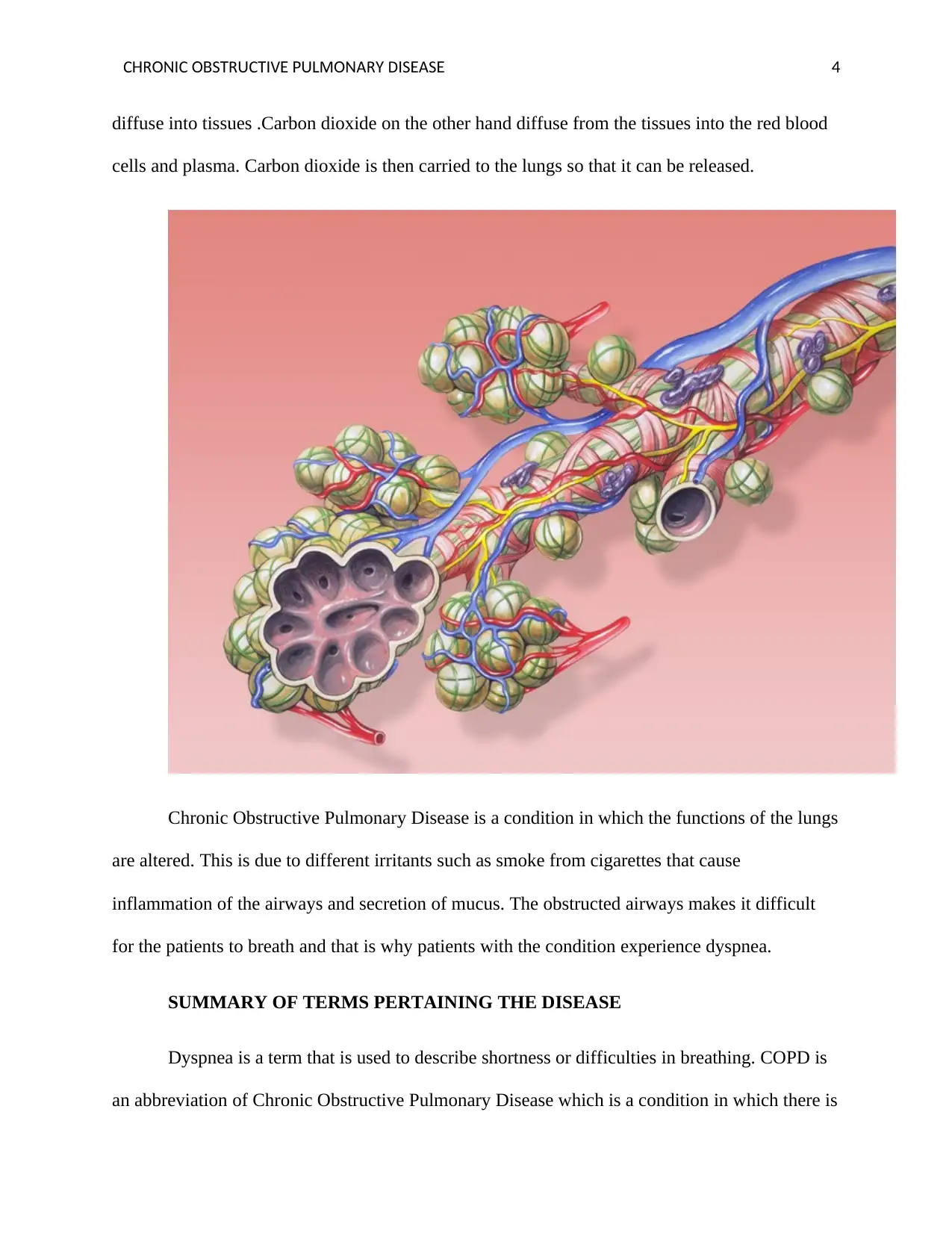
diffuse into tissues .Carbon dioxide on the other hand diffuse from the tissues into the red blood
cells and plasma. Carbon dioxide is then carried to the lungs so that it can be released.
Chronic Obstructive Pulmonary Disease is a condition in which the functions of the lungs
are altered. This is due to different irritants such as smoke from cigarettes that cause
inflammation of the airways and secretion of mucus. The obstructed airways makes it difficult
for the patients to breath and that is why patients with the condition experience dyspnea.
SUMMARY OF TERMS PERTAINING THE DISEASE
Dyspnea is a term that is used to describe shortness or difficulties in breathing. COPD is
an abbreviation of Chronic Obstructive Pulmonary Disease which is a condition in which there is
diffuse into tissues .Carbon dioxide on the other hand diffuse from the tissues into the red blood
cells and plasma. Carbon dioxide is then carried to the lungs so that it can be released.
Chronic Obstructive Pulmonary Disease is a condition in which the functions of the lungs
are altered. This is due to different irritants such as smoke from cigarettes that cause
inflammation of the airways and secretion of mucus. The obstructed airways makes it difficult
for the patients to breath and that is why patients with the condition experience dyspnea.
SUMMARY OF TERMS PERTAINING THE DISEASE
Dyspnea is a term that is used to describe shortness or difficulties in breathing. COPD is
an abbreviation of Chronic Obstructive Pulmonary Disease which is a condition in which there is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 5
impairment in gaseous exchange in the lungs .Exacerbations is a term that is used to describe the
worsening of the signs and symptoms or the disease. Wheezing is a term that is used to describe
the sound produced by patients suffering from COPD when they are breathing (Chen, Thomas,
Sadatsafavi, & FitzGerald, 2015). Bronchodilators is a term that is used to describe a group of
drugs that are used in the treatment of COPD. Cor pulmonale is a condition in which the right
ventricles swell as they work hard to pump out blood to the rest of the body.
AETIOLOGY
According to studies, the leading cause of COPD in developed countries like United
States of America and Australia is smoking. Studies have also established that 90% of the people
who are suffering from COPD are either smokers or they are former smokers. Out of those who
smoke, 20-30% end up developing COPD. Majority of the people with COPD are also above 40
years with a history of smoking .This therefore means that the more an individual smokes, the
higher the risks of COPD. Besides the cigarette smoke, others such as cigar smoke, pipe smoke
and the second hand smoke also cause COPD.
One can develop COPD if he/she is exposed to certain chemicals and fumes in the
workplace .Studies have found out that there is a link between long exposure to chemicals,
continuous inhaling of dust and COPD. It has also been established that in developed countries
like Australia, the houses are poorly ventilated and as a result, people inhale fumes from cooking
as well as heating fuel and this increases the risk of COPD(Christenson et al., 2015).COPD has
also been attributed to genetics .Studies have shown that 5% of patients suffering from COPD
have a deficiency in a certain protein known as alpha-1-antitrypsin.This causes the lung to
deteriorate and can also alter the functions of the liver.
impairment in gaseous exchange in the lungs .Exacerbations is a term that is used to describe the
worsening of the signs and symptoms or the disease. Wheezing is a term that is used to describe
the sound produced by patients suffering from COPD when they are breathing (Chen, Thomas,
Sadatsafavi, & FitzGerald, 2015). Bronchodilators is a term that is used to describe a group of
drugs that are used in the treatment of COPD. Cor pulmonale is a condition in which the right
ventricles swell as they work hard to pump out blood to the rest of the body.
AETIOLOGY
According to studies, the leading cause of COPD in developed countries like United
States of America and Australia is smoking. Studies have also established that 90% of the people
who are suffering from COPD are either smokers or they are former smokers. Out of those who
smoke, 20-30% end up developing COPD. Majority of the people with COPD are also above 40
years with a history of smoking .This therefore means that the more an individual smokes, the
higher the risks of COPD. Besides the cigarette smoke, others such as cigar smoke, pipe smoke
and the second hand smoke also cause COPD.
One can develop COPD if he/she is exposed to certain chemicals and fumes in the
workplace .Studies have found out that there is a link between long exposure to chemicals,
continuous inhaling of dust and COPD. It has also been established that in developed countries
like Australia, the houses are poorly ventilated and as a result, people inhale fumes from cooking
as well as heating fuel and this increases the risk of COPD(Christenson et al., 2015).COPD has
also been attributed to genetics .Studies have shown that 5% of patients suffering from COPD
have a deficiency in a certain protein known as alpha-1-antitrypsin.This causes the lung to
deteriorate and can also alter the functions of the liver.
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 6
SIGNS AND SYMPTOMS
There are different signs and symptoms of COPD. One of the most notable sign and
symptom is shortness of breath .This is due to emphysema which is a condition in which there is
destruction of the delicate walls as well as the elastic fibers of the alveoli .The small airways then
collapse when the patient breaths out(Divo et al., 2015). This makes it difficult for the air to flow
into the lungs .Excess mucus in the lungs is another symptom. Patients suffering from COPD
always remove excess mucus especially in the morning. The excess mucus are produced due to
the inflammation of the bronchiole tubules when they are affected by chemical irritants like
smoke from cigarettes.
Patients with COPD always experience fatigue. Since the airways are usually narrowed
and full of secretions like the mucus, the patient’s heart and lungs have to work extra hard to
ensure that the patients is able to undergo gaseous exchange. This aspect of the heart and the
lungs working hard is what makes the patient experience fatigue.
Wheezing is another significant sign of COPD. People suffering from COPD will always
produce some whistling sounds whenever they force out air through the airways that are
obstructed by excess mucus. This symptom is therefore due to excess mucus that block the
airways as well as the tightening of the muscles of the chest.
Frequent respiratory infections is a clear sign and symptom of COPD. Studies have
shown that patients suffering from COPD have impaired immune systems. The condition also
makes it difficult for the lungs to get rid of different pollutants like dust. The buildup of excess
pollutants and dust makes the patients susceptible to different respiratory infections. The most
common infections include colds, flu and finally pneumonia.
SIGNS AND SYMPTOMS
There are different signs and symptoms of COPD. One of the most notable sign and
symptom is shortness of breath .This is due to emphysema which is a condition in which there is
destruction of the delicate walls as well as the elastic fibers of the alveoli .The small airways then
collapse when the patient breaths out(Divo et al., 2015). This makes it difficult for the air to flow
into the lungs .Excess mucus in the lungs is another symptom. Patients suffering from COPD
always remove excess mucus especially in the morning. The excess mucus are produced due to
the inflammation of the bronchiole tubules when they are affected by chemical irritants like
smoke from cigarettes.
Patients with COPD always experience fatigue. Since the airways are usually narrowed
and full of secretions like the mucus, the patient’s heart and lungs have to work extra hard to
ensure that the patients is able to undergo gaseous exchange. This aspect of the heart and the
lungs working hard is what makes the patient experience fatigue.
Wheezing is another significant sign of COPD. People suffering from COPD will always
produce some whistling sounds whenever they force out air through the airways that are
obstructed by excess mucus. This symptom is therefore due to excess mucus that block the
airways as well as the tightening of the muscles of the chest.
Frequent respiratory infections is a clear sign and symptom of COPD. Studies have
shown that patients suffering from COPD have impaired immune systems. The condition also
makes it difficult for the lungs to get rid of different pollutants like dust. The buildup of excess
pollutants and dust makes the patients susceptible to different respiratory infections. The most
common infections include colds, flu and finally pneumonia.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 7
Weight loss is common among patients with COPD. This is because they need more
energy to breathe effectively and this uses a lot of calories in the body .In most cases, the calories
used are not proportional to the ones being used up and this leads to weight loss. Swollen feet
and ankles is also a common sign and symptom of COPD.COPD causes severe damage to the
lungs and this means that the heart has to work extra hard to supply blood to the damaged lungs
(Lange et al., 2015). This eventually leads to congestive heart failure that is shown by the
swollen feet and ankles. Headaches and fever are also common. This is due to the high level of
carbon dioxide in the blood. This signs and symptoms can also occur when the level of oxygen is
low since there is impaired gaseous exchange.
INVESTIGATIONS AND TESTS
There are different investigative procedures, clinical tests and laboratory tests that are
used to investigate COPD. There are cases where the condition has been misdiagnosed. Some
patients who quit smoking are often told that they are suffering from COPD when they are just
experiencing deconditioning or another condition of the lungs. Other people who have the
disease might also not be diagnosed until the symptoms gets worse and this hampers the
interventions. For effective diagnosis, the doctor needs to review the signs and symptoms and
then make an inquiry of history of health and exposure to lung irritants more so smoking. There
are several tests that can be done.
The lung (pulmonary) function test is one of them. The aim of this test is to determine the
quantity of air that the patient can inhale and exhale .It also checks if the lungs are taking enough
oxygen to the blood r]of the patient .The most common lung function test is spirometry
(McCarthy et al., 2015). The doctor usually instruct the patient to blow into a tube that is
connected to an equipment known as spirometer. The spirometer could then indicate the quantity
Weight loss is common among patients with COPD. This is because they need more
energy to breathe effectively and this uses a lot of calories in the body .In most cases, the calories
used are not proportional to the ones being used up and this leads to weight loss. Swollen feet
and ankles is also a common sign and symptom of COPD.COPD causes severe damage to the
lungs and this means that the heart has to work extra hard to supply blood to the damaged lungs
(Lange et al., 2015). This eventually leads to congestive heart failure that is shown by the
swollen feet and ankles. Headaches and fever are also common. This is due to the high level of
carbon dioxide in the blood. This signs and symptoms can also occur when the level of oxygen is
low since there is impaired gaseous exchange.
INVESTIGATIONS AND TESTS
There are different investigative procedures, clinical tests and laboratory tests that are
used to investigate COPD. There are cases where the condition has been misdiagnosed. Some
patients who quit smoking are often told that they are suffering from COPD when they are just
experiencing deconditioning or another condition of the lungs. Other people who have the
disease might also not be diagnosed until the symptoms gets worse and this hampers the
interventions. For effective diagnosis, the doctor needs to review the signs and symptoms and
then make an inquiry of history of health and exposure to lung irritants more so smoking. There
are several tests that can be done.
The lung (pulmonary) function test is one of them. The aim of this test is to determine the
quantity of air that the patient can inhale and exhale .It also checks if the lungs are taking enough
oxygen to the blood r]of the patient .The most common lung function test is spirometry
(McCarthy et al., 2015). The doctor usually instruct the patient to blow into a tube that is
connected to an equipment known as spirometer. The spirometer could then indicate the quantity
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 8
of air that the lungs can sustain and the speed at which the patient can blow air out of the
lungs .The advantage with the lung function test using a spirometer is that it has the ability to
detect COPD even before the signs and symptoms can be experienced. The test can also be used
to track on how the disease progress and it can also be used to evaluate if the medication is
working or not .It also measures the effects of the bronchodilators. Other tests under the lung
function tests include measurement of the lung volumes, diffusing capacity and finally the pulse
oximetry.
Laboratory tests are also investigative tests that can be used in COPD. However, the
laboratory tests are not used to diagnose COPD .It is only used to establish the cause of the
symptoms or rule out the disease. An example of a laboratory test is the one that tests for the
genetic disorder alpha-1-antitrypsin (AAt) deficiency which is known to be one of the conditions
that contribute to COPD .The test is done when an individual has a family history of COPD and
developed the condition below 45 years.
TREATMENT AND MANAGEMENT
Description
There are different options that can be used to treat COPD. The most common group of
drugs used however the bronchodilators are. The bronchodilators are a broad group which can be
divided further into the long acting and the short acting bronchodilators .The difference between
the two is that the short acting bronchodilators provide a swift or quick response to relieve acute
bronchoconstriction while the long acting bronchodilators assist in preventing the symptoms.
Uses
of air that the lungs can sustain and the speed at which the patient can blow air out of the
lungs .The advantage with the lung function test using a spirometer is that it has the ability to
detect COPD even before the signs and symptoms can be experienced. The test can also be used
to track on how the disease progress and it can also be used to evaluate if the medication is
working or not .It also measures the effects of the bronchodilators. Other tests under the lung
function tests include measurement of the lung volumes, diffusing capacity and finally the pulse
oximetry.
Laboratory tests are also investigative tests that can be used in COPD. However, the
laboratory tests are not used to diagnose COPD .It is only used to establish the cause of the
symptoms or rule out the disease. An example of a laboratory test is the one that tests for the
genetic disorder alpha-1-antitrypsin (AAt) deficiency which is known to be one of the conditions
that contribute to COPD .The test is done when an individual has a family history of COPD and
developed the condition below 45 years.
TREATMENT AND MANAGEMENT
Description
There are different options that can be used to treat COPD. The most common group of
drugs used however the bronchodilators are. The bronchodilators are a broad group which can be
divided further into the long acting and the short acting bronchodilators .The difference between
the two is that the short acting bronchodilators provide a swift or quick response to relieve acute
bronchoconstriction while the long acting bronchodilators assist in preventing the symptoms.
Uses
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 9
The indications or the uses of the bronchodilators generally depend on the extent or the
severity of the disease .In case the disease is still at its acute stage, then the short acting
bronchodilators are prescribed. Examples of the short acting bronchodilators include albuterol,
levalbuterol and ipratropium. The long acting bronchodilators are on the other hand used when
the condition is very severe and they are used to control the symptoms (Pascoe, Locantore,
Dransfield, Barnes, & Pavord, 2015). They are also used to prevent bronchoconstriction. They
also take long before they start acting. They are also used to relieve airways constriction for a
period of up to 12 hours. They are administered two times a day together with another anti-
inflammatory medication so that they can open the airways thus preventing the symptoms of
asthma especially at night. Examples of the long acting bronchodilators are salmeterol and the
formoterol.
Mechanism of action
The mechanism of action of these drugs is that they dilate the bronchi of the patient as
well as the bronchioles and therefore reduce resistance of the respiratory airways and this
increases the amount of air that flows into the lungs. These group of drugs maybe endogenous
which means they can originate from the body or they can be administered in the form of
medications.
Contraindications
There are different contraindications that should be considered when using the
bronchodilators .Patients who are hypersensitive, have cardiac arrhythmias that is associated
with tachycardia, organic brain damage, cerebral arteriosclerosis and narrow angle glaucoma are
usually contraindicated against the sympathomimetic bronchodilators (Postma, Bush, & Van den
The indications or the uses of the bronchodilators generally depend on the extent or the
severity of the disease .In case the disease is still at its acute stage, then the short acting
bronchodilators are prescribed. Examples of the short acting bronchodilators include albuterol,
levalbuterol and ipratropium. The long acting bronchodilators are on the other hand used when
the condition is very severe and they are used to control the symptoms (Pascoe, Locantore,
Dransfield, Barnes, & Pavord, 2015). They are also used to prevent bronchoconstriction. They
also take long before they start acting. They are also used to relieve airways constriction for a
period of up to 12 hours. They are administered two times a day together with another anti-
inflammatory medication so that they can open the airways thus preventing the symptoms of
asthma especially at night. Examples of the long acting bronchodilators are salmeterol and the
formoterol.
Mechanism of action
The mechanism of action of these drugs is that they dilate the bronchi of the patient as
well as the bronchioles and therefore reduce resistance of the respiratory airways and this
increases the amount of air that flows into the lungs. These group of drugs maybe endogenous
which means they can originate from the body or they can be administered in the form of
medications.
Contraindications
There are different contraindications that should be considered when using the
bronchodilators .Patients who are hypersensitive, have cardiac arrhythmias that is associated
with tachycardia, organic brain damage, cerebral arteriosclerosis and narrow angle glaucoma are
usually contraindicated against the sympathomimetic bronchodilators (Postma, Bush, & Van den
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 10
Berge, 2015). During acute bronchospasm, salmeterol is usually contraindicated .The
sympathomimetic drugs should not be used with oxytocic drugs concurrently since they lead to
hypotension .In patients who are pregnant, have hypertension, cardiac dysfunction,
hyperthyroidism, glaucoma, diabetes and history of seizures, the sympathomimetic
bronchodilators should not be used .If they are used, the doctor ought to be very cautious.
Sympathomimetic should also not be administered together with adrenergic blockers since they
can inhibit cardiac Broncho dilating as well as the vasodilating action of the sympathomimetic
drug. There would also be an increased cardio toxicity if sympathomimetic drugs are used with
theophylline and the doctor should therefore be very careful.
Adverse reaction/side effects
These drugs are associated with many adverse reactions or the side effects. The side
effects of the beta-2-agonists such as the salbutamol include trembling especially the hands,
nervous tension ,headaches and sudden palpitations. It is also associated with muscle cramps.
These side effects however improve and can disappear after using the drugs for some days or
weeks. Serious side effects include paradoxical bronchospasm or the constrictions of the airways.
High doses of the drugs can also lead to heart attacks and low level of potassium otherwise
described as hypokalemia (Woodruff, Agusti, Roche, Singh, & Martinez, 2015). The side effects
of using anticholinergics on the other hand include dry mouth, constipation, headaches. Other
minor side effects include nausea, heartburns and dysphagia .When a patient is using an inhaler,
glaucoma may get worse especially if the drugs get into the eyes. Finally, theophylline can lead
to severe side effects if it builds up in the body. Old people are the ones at risk since their livers
might fail to clear the drug in the blood. The main side effects include tachycardia, arrhythmia,
headaches and insomnia.
Berge, 2015). During acute bronchospasm, salmeterol is usually contraindicated .The
sympathomimetic drugs should not be used with oxytocic drugs concurrently since they lead to
hypotension .In patients who are pregnant, have hypertension, cardiac dysfunction,
hyperthyroidism, glaucoma, diabetes and history of seizures, the sympathomimetic
bronchodilators should not be used .If they are used, the doctor ought to be very cautious.
Sympathomimetic should also not be administered together with adrenergic blockers since they
can inhibit cardiac Broncho dilating as well as the vasodilating action of the sympathomimetic
drug. There would also be an increased cardio toxicity if sympathomimetic drugs are used with
theophylline and the doctor should therefore be very careful.
Adverse reaction/side effects
These drugs are associated with many adverse reactions or the side effects. The side
effects of the beta-2-agonists such as the salbutamol include trembling especially the hands,
nervous tension ,headaches and sudden palpitations. It is also associated with muscle cramps.
These side effects however improve and can disappear after using the drugs for some days or
weeks. Serious side effects include paradoxical bronchospasm or the constrictions of the airways.
High doses of the drugs can also lead to heart attacks and low level of potassium otherwise
described as hypokalemia (Woodruff, Agusti, Roche, Singh, & Martinez, 2015). The side effects
of using anticholinergics on the other hand include dry mouth, constipation, headaches. Other
minor side effects include nausea, heartburns and dysphagia .When a patient is using an inhaler,
glaucoma may get worse especially if the drugs get into the eyes. Finally, theophylline can lead
to severe side effects if it builds up in the body. Old people are the ones at risk since their livers
might fail to clear the drug in the blood. The main side effects include tachycardia, arrhythmia,
headaches and insomnia.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 11
POTENTIAL COMPLICATIONS
Chronic obstructive pulmonary Disease is associated with different complications .Cor
Pulmonale is an example of the complications. This is a condition in which there is edema or
swelling of the lower extremities. Since there is poor exchange in COPD, there is less oxygen in
blood and this leads to constriction of blood vessels .Majority of the capillaries that surround the
alveoli are in return destroyed and this therefore makes the heart to work hard to pump blood in
the few and constricted blood vessels .Due to this effort, the right hand side of the heart enlarge
and the walls thicken and finally the chamber loses its ability to contract efficiently. This is what
brings about pulmonary hypertension and right sided heart failure that is known as cor
pulmonale.
End stage lung disease is a serious complication of COPD. Chronic Obstructive
Pulmonary Disease is characterized by the slow decline in the lung function as well as increased
levels of carbon dioxide in blood. The elevated levels of carbon dioxide leads to a narcotic effect
in the patient who end up losing consciousness and eventually stops breathing.
Pneumonia, polycythemia and pneumothorax are other complications that are associated
with COPD. Since patients with COPD have impaired immune systems, it makes the patient
susceptible to bacterial infection especially the streptococcus pneumoniae that leads to
pneumonia .Since there is impaired lung function in patients with COPD, the level of oxygen in
blood reduce. This therefore needs the body to adjust and produce more oxygen carrying red
blood cells. This condition is known as polycythemia. COPD leads to a weakened lung structure.
POTENTIAL COMPLICATIONS
Chronic obstructive pulmonary Disease is associated with different complications .Cor
Pulmonale is an example of the complications. This is a condition in which there is edema or
swelling of the lower extremities. Since there is poor exchange in COPD, there is less oxygen in
blood and this leads to constriction of blood vessels .Majority of the capillaries that surround the
alveoli are in return destroyed and this therefore makes the heart to work hard to pump blood in
the few and constricted blood vessels .Due to this effort, the right hand side of the heart enlarge
and the walls thicken and finally the chamber loses its ability to contract efficiently. This is what
brings about pulmonary hypertension and right sided heart failure that is known as cor
pulmonale.
End stage lung disease is a serious complication of COPD. Chronic Obstructive
Pulmonary Disease is characterized by the slow decline in the lung function as well as increased
levels of carbon dioxide in blood. The elevated levels of carbon dioxide leads to a narcotic effect
in the patient who end up losing consciousness and eventually stops breathing.
Pneumonia, polycythemia and pneumothorax are other complications that are associated
with COPD. Since patients with COPD have impaired immune systems, it makes the patient
susceptible to bacterial infection especially the streptococcus pneumoniae that leads to
pneumonia .Since there is impaired lung function in patients with COPD, the level of oxygen in
blood reduce. This therefore needs the body to adjust and produce more oxygen carrying red
blood cells. This condition is known as polycythemia. COPD leads to a weakened lung structure.
C R C S R C V M AR D S ASH ONI OB T U TI E PUL ON Y I E E 12
This therefore makes the lungs to develop holes as air tries to escape into the chest wall. This
condition in which there are holes in the lungs is known as pneumothorax.
CONCLUSION
Chronic Obstructive Pulmonary Disease is a condition in which patients experience
difficulties in breathing .It is caused by substances that can irritate the lungs such as smoke from
cigarettes and the dust as well as some chemicals. This chemicals cause inflammation of the
airways and increased production of mucus that block the airways and that is why patients
suffering from COPD experience difficulties in breathing.14.4% of Australians who are above 40
years are suffering from COPD .Some of the signs and symptoms for the condition include
wheezing sounds, shortness of breath and fatigue. Diagnosis of COPD involve the lung function
test that is done using a spirometer and different laboratory tests. The treatment includes the use
of bronchodilators that cause dilation of airways and improves the breathing pattern of the
patient. COPD is the third leading cause of mortalities in Australia and therefore should be
strategies to reduce its prevalence
This therefore makes the lungs to develop holes as air tries to escape into the chest wall. This
condition in which there are holes in the lungs is known as pneumothorax.
CONCLUSION
Chronic Obstructive Pulmonary Disease is a condition in which patients experience
difficulties in breathing .It is caused by substances that can irritate the lungs such as smoke from
cigarettes and the dust as well as some chemicals. This chemicals cause inflammation of the
airways and increased production of mucus that block the airways and that is why patients
suffering from COPD experience difficulties in breathing.14.4% of Australians who are above 40
years are suffering from COPD .Some of the signs and symptoms for the condition include
wheezing sounds, shortness of breath and fatigue. Diagnosis of COPD involve the lung function
test that is done using a spirometer and different laboratory tests. The treatment includes the use
of bronchodilators that cause dilation of airways and improves the breathing pattern of the
patient. COPD is the third leading cause of mortalities in Australia and therefore should be
strategies to reduce its prevalence
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.