Effects of Coping Strategies on Anxiety Levels of Nurses during COVID-19 Pandemic
VerifiedAdded on 2023/06/15
|60
|22362
|301
AI Summary
This research aims to investigate the effects of coping strategies on nurses' anxiety levels during the COVID-19 pandemic. The study sample consisted of 404 nurses working in the COVID-19 wards in 10 UK hospitals. The study employed a cross-sectional design and used Brief-COPE and Self-rating Anxiety Scale (SAS) for data collection. The study findings revealed that the nurses' most commonly used coping strategy is problem-focused coping to overcome and bring down their anxiety levels.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
An Investigation of the Effects of Coping Strategies on Anxiety Levels
of Nurses during COVID-19 Pandemic
Abstract
This research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. Anxiety is defined as "a disordered condition" of the body's
emotional sensitivity. During the Coronavirus Disease 2019 (COVID-19) pandemic, nurses in
COVID-19 wards, emergency departments, and fever clinics have served as healthcare system
gatekeepers while risking their own and families’ health and lives. Uncertain situations, working
for long hours, and fear of contracting the disease have increased the nurses' anxiety level. The
nurses serving in the COVID and emergency wards use several coping strategies to overcome
their anxiety. It is vital to understand the correlation between the coping strategies used by the
nurses and their anxiety levels during the COVID-19 pandemic. For this purpose, this study
employed a cross-sectional design and used Brief-COPE and Self-rating Anxiety Scale (SAS) for
data collection. The study sample consisted of 404 nurses working in the COVID-19 wards in 10
UK hospitals. The data was collected online and analysed with the help of SPSS (v. 25) by
running descriptive statistics, Pearson correlation analysis, and Regression analysis for
determining the relationship among the study variables. The study findings revealed that the
nurses' most commonly used coping strategy is problem-focused coping to overcome and bring
down their anxiety levels. Further results showed a positive relationship between the three
sub-scales of managing (problem-focused coping, emotion-focused coping and avoidant coping)
and the nurses’ anxiety levels during the COVID-19 pandemic.
1
of Nurses during COVID-19 Pandemic
Abstract
This research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. Anxiety is defined as "a disordered condition" of the body's
emotional sensitivity. During the Coronavirus Disease 2019 (COVID-19) pandemic, nurses in
COVID-19 wards, emergency departments, and fever clinics have served as healthcare system
gatekeepers while risking their own and families’ health and lives. Uncertain situations, working
for long hours, and fear of contracting the disease have increased the nurses' anxiety level. The
nurses serving in the COVID and emergency wards use several coping strategies to overcome
their anxiety. It is vital to understand the correlation between the coping strategies used by the
nurses and their anxiety levels during the COVID-19 pandemic. For this purpose, this study
employed a cross-sectional design and used Brief-COPE and Self-rating Anxiety Scale (SAS) for
data collection. The study sample consisted of 404 nurses working in the COVID-19 wards in 10
UK hospitals. The data was collected online and analysed with the help of SPSS (v. 25) by
running descriptive statistics, Pearson correlation analysis, and Regression analysis for
determining the relationship among the study variables. The study findings revealed that the
nurses' most commonly used coping strategy is problem-focused coping to overcome and bring
down their anxiety levels. Further results showed a positive relationship between the three
sub-scales of managing (problem-focused coping, emotion-focused coping and avoidant coping)
and the nurses’ anxiety levels during the COVID-19 pandemic.
1
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Contents
Abstract.......................................................................................................................................................1
Chapter One: Introduction...........................................................................................................................4
1.1Introduction and Background ............................................................................................................4
1.2 Rationale of the Research .................................................................................................................8
1.3 Research Aim, Objectives & Question................................................................................................8
1.4 Theoretical Framework......................................................................................................................9
1.5 Study Hypotheses..............................................................................................................................9
1.6 Outline of the Dissertation...............................................................................................................10
Chapter Two: Literature Review................................................................................................................10
2.1 Introduction.....................................................................................................................................11
2.2 Anxiety.............................................................................................................................................11
2.3 Anxiety amongst Healthcare Professionals during COVID-19..........................................................13
2.4 Anxiety Levels of Nurses during COVID-19.......................................................................................16
2.5 Coping Strategies.............................................................................................................................18
2.5.1 Usage of COVID-19 protective measures .................................................................................18
2.5.2 Avoidance coping......................................................................................................................19
2.5.3 Role of social support................................................................................................................20
2.5.4 Faith-based practices................................................................................................................20
2.5.5 Psychological support...............................................................................................................21
2.5.6 Managerial support...................................................................................................................22
2.6 Research Gap...................................................................................................................................22
Chapter Three: Methods...........................................................................................................................23
3.1 Introduction.....................................................................................................................................23
3.2 Study Design....................................................................................................................................24
3.3 Study Participants ...........................................................................................................................24
3.4 Research Tools.................................................................................................................................24
3.4.1Demographic questionnaire......................................................................................................24
3.4.3Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)...........25
3.5 Procedure........................................................................................................................................26
3.6 Data Analysis....................................................................................................................................27
3.7 Ethical Considerations......................................................................................................................27
Chapter Four: Results................................................................................................................................28
4.1 Introduction.....................................................................................................................................28
2
Abstract.......................................................................................................................................................1
Chapter One: Introduction...........................................................................................................................4
1.1Introduction and Background ............................................................................................................4
1.2 Rationale of the Research .................................................................................................................8
1.3 Research Aim, Objectives & Question................................................................................................8
1.4 Theoretical Framework......................................................................................................................9
1.5 Study Hypotheses..............................................................................................................................9
1.6 Outline of the Dissertation...............................................................................................................10
Chapter Two: Literature Review................................................................................................................10
2.1 Introduction.....................................................................................................................................11
2.2 Anxiety.............................................................................................................................................11
2.3 Anxiety amongst Healthcare Professionals during COVID-19..........................................................13
2.4 Anxiety Levels of Nurses during COVID-19.......................................................................................16
2.5 Coping Strategies.............................................................................................................................18
2.5.1 Usage of COVID-19 protective measures .................................................................................18
2.5.2 Avoidance coping......................................................................................................................19
2.5.3 Role of social support................................................................................................................20
2.5.4 Faith-based practices................................................................................................................20
2.5.5 Psychological support...............................................................................................................21
2.5.6 Managerial support...................................................................................................................22
2.6 Research Gap...................................................................................................................................22
Chapter Three: Methods...........................................................................................................................23
3.1 Introduction.....................................................................................................................................23
3.2 Study Design....................................................................................................................................24
3.3 Study Participants ...........................................................................................................................24
3.4 Research Tools.................................................................................................................................24
3.4.1Demographic questionnaire......................................................................................................24
3.4.3Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)...........25
3.5 Procedure........................................................................................................................................26
3.6 Data Analysis....................................................................................................................................27
3.7 Ethical Considerations......................................................................................................................27
Chapter Four: Results................................................................................................................................28
4.1 Introduction.....................................................................................................................................28
2
4.2 Reliability and Validity of the Data...................................................................................................28
4.3 Demographic Results.......................................................................................................................29
4.4 Descriptive Statistics........................................................................................................................30
4.5 Inferential Analysis...........................................................................................................................35
4.5.1 Analysis of correlation between Brief-COPE (Coping Strategies) and SAS (Anxiety levels).......35
Chapter Five: Discussion............................................................................................................................38
5.1 Introduction.....................................................................................................................................38
4.2 Discussion of Findings......................................................................................................................38
Chapter Six: Implications...........................................................................................................................46
6.1 Introduction.....................................................................................................................................46
6.2 Implications.....................................................................................................................................46
6.2.1 Implications for theory..............................................................................................................46
6.2.1 Implications for nursing management......................................................................................47
6.3 Recommendations...........................................................................................................................48
Chapter Seven: Conclusion........................................................................................................................50
7.1 Introduction ....................................................................................................................................50
7.2 Summary of Research......................................................................................................................50
7.3 Limitations and Future Research Suggestions .................................................................................52
References ................................................................................................................................................53
Appendices................................................................................................................................................62
Appendix A............................................................................................................................................62
Demographic questionnaire..................................................................................................................62
Appendix B.................................................................................................................................................65
Zung Self-Rating Anxiety Scale (SAS)..........................................................................................................65
Appendix C.................................................................................................................................................66
Coping Orientation to Problems Experienced Inventory (Brief-Cope).......................................................66
Chapter One: Introduction
3
4.3 Demographic Results.......................................................................................................................29
4.4 Descriptive Statistics........................................................................................................................30
4.5 Inferential Analysis...........................................................................................................................35
4.5.1 Analysis of correlation between Brief-COPE (Coping Strategies) and SAS (Anxiety levels).......35
Chapter Five: Discussion............................................................................................................................38
5.1 Introduction.....................................................................................................................................38
4.2 Discussion of Findings......................................................................................................................38
Chapter Six: Implications...........................................................................................................................46
6.1 Introduction.....................................................................................................................................46
6.2 Implications.....................................................................................................................................46
6.2.1 Implications for theory..............................................................................................................46
6.2.1 Implications for nursing management......................................................................................47
6.3 Recommendations...........................................................................................................................48
Chapter Seven: Conclusion........................................................................................................................50
7.1 Introduction ....................................................................................................................................50
7.2 Summary of Research......................................................................................................................50
7.3 Limitations and Future Research Suggestions .................................................................................52
References ................................................................................................................................................53
Appendices................................................................................................................................................62
Appendix A............................................................................................................................................62
Demographic questionnaire..................................................................................................................62
Appendix B.................................................................................................................................................65
Zung Self-Rating Anxiety Scale (SAS)..........................................................................................................65
Appendix C.................................................................................................................................................66
Coping Orientation to Problems Experienced Inventory (Brief-Cope).......................................................66
Chapter One: Introduction
3
Introduction and Background
The outbreak of COVID-19 in December 2019 has been associated with innumerable challenges,
especially to the healthcare workers, as they occupy the frontline in dealing with COVID-19 pandemics
and are at increased risk of burdens led by COVID-19. Cases of mental health issues among these groups
of individuals are associated with the excessive workload and risk of transmitting the disease during
healthcare pandemics (World Health Organization [WHO] 2020a.) Unpreparedness to handle the surging
cases of the pandemic and emotional distress associated with the fear of infection concerns include the
fact that the disease is highly contagious with a low level of knowledge on the factors surrounding the
infection. The lack of established vaccines or treatments to handle the outbreak has also been another
concern (Pappa et al. 2020) for an extended period before the introduction of vaccines.
The World Health Organisation (WHO, 2020B) reports that nurses are the most prominent health
professionals in the health sector. They play a crucial role in public health emergencies in improving
public health even though COVID-19 has put more burden on health systems, and its impact is beyond
description. Nurses’ contributions and vigilance in health promotion during epidemic outbreaks like
influenza, Ebola, and Zika were seen in the past years. Currently, nurses are at the forefront of caring for
COVID-19 patients in acute care settings (WHO, 2020b.) In addition, they have been engaged together
with the interprofessional sectors, teams, and communities in this global pandemic preparedness and
response (American Academy of Nursing, 2018).
Nurses have proved to be the more excellent asset. In the past decades, nurses have been on the
frontline during major hits of infectious disease outbreaks, including “H1N1, Swine Flu, Severe Acute
Respiratory Syndrome SARS, Middle East Respiratory Syndrome (MERS) and Ebola” (Ruiz-Fernandez et
al., 2020, p. 4321). Similarly, the study done by Jung and Jun (2020) has found that nurses have always
been the front liners and role models in infection control and prevention practices and public health
promotion. It has become apparent that nurses work all around the clock to provide hospital care to the
affected ones. Public health nurses are shifted to acute care settings. They lead a response team,
demonstrating skills and expertise in emergency preparedness, predictive modelling, hospital, and field
operations to deal with the pandemic. However, they are not exempted from experiencing accidental
outcomes such as exposure to outbreaks, occupational stress, lethargy, psychological fatigue, and
trauma (Jung & Jun 2020).
4
The outbreak of COVID-19 in December 2019 has been associated with innumerable challenges,
especially to the healthcare workers, as they occupy the frontline in dealing with COVID-19 pandemics
and are at increased risk of burdens led by COVID-19. Cases of mental health issues among these groups
of individuals are associated with the excessive workload and risk of transmitting the disease during
healthcare pandemics (World Health Organization [WHO] 2020a.) Unpreparedness to handle the surging
cases of the pandemic and emotional distress associated with the fear of infection concerns include the
fact that the disease is highly contagious with a low level of knowledge on the factors surrounding the
infection. The lack of established vaccines or treatments to handle the outbreak has also been another
concern (Pappa et al. 2020) for an extended period before the introduction of vaccines.
The World Health Organisation (WHO, 2020B) reports that nurses are the most prominent health
professionals in the health sector. They play a crucial role in public health emergencies in improving
public health even though COVID-19 has put more burden on health systems, and its impact is beyond
description. Nurses’ contributions and vigilance in health promotion during epidemic outbreaks like
influenza, Ebola, and Zika were seen in the past years. Currently, nurses are at the forefront of caring for
COVID-19 patients in acute care settings (WHO, 2020b.) In addition, they have been engaged together
with the interprofessional sectors, teams, and communities in this global pandemic preparedness and
response (American Academy of Nursing, 2018).
Nurses have proved to be the more excellent asset. In the past decades, nurses have been on the
frontline during major hits of infectious disease outbreaks, including “H1N1, Swine Flu, Severe Acute
Respiratory Syndrome SARS, Middle East Respiratory Syndrome (MERS) and Ebola” (Ruiz-Fernandez et
al., 2020, p. 4321). Similarly, the study done by Jung and Jun (2020) has found that nurses have always
been the front liners and role models in infection control and prevention practices and public health
promotion. It has become apparent that nurses work all around the clock to provide hospital care to the
affected ones. Public health nurses are shifted to acute care settings. They lead a response team,
demonstrating skills and expertise in emergency preparedness, predictive modelling, hospital, and field
operations to deal with the pandemic. However, they are not exempted from experiencing accidental
outcomes such as exposure to outbreaks, occupational stress, lethargy, psychological fatigue, and
trauma (Jung & Jun 2020).
4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
According to the International Council of Nurses (ICN, 2021), 90 million people have been infected with
the disease globally, resulting in 1.9 million deaths worldwide. In Mexico, 21% of nurses have been
infected with COVID-19, whereas 45% were infected with COVID-19 in Iran. Both countries were hardly
hit by COVID-19, shown by the report of ICN (2021). Research has shown that at least 1 in 5 healthcare
workers are showing signs of depression and anxiety, whereas 4 in 10 workers are experiencing
insomnia and a higher rate of anxiety and depression among the female nursing staff and health workers
(Pappa et al., 2020).
According to a systematic literature review conducted by Pappa et al. (2020), “the uneven and increased
distribution of workload, physical exhaustion, lack of personal protective equipment, nosocomial
transmission” as well as “the need to make ethically difficult decisions on the rationing of care” have
posed a tremendous impact on “the physical and mental well-being of nurses” (p. 902). Isolation and
loss of social support, risks of infecting loved ones and relatives as well as rapid changes in the working
environment can further compromise the resilience of nurses leading them to be at a higher risk of
experiencing a variety of psychological effects, including “acute stress disorder, depression, post-
traumatic stress disorder, insomnia, irritability, anger, and emotional exhaustion following disease
outbreak” (Pappa et al., 2020, p. 902).
Ruiz-Fernandez et al. (2020) discovered that “the prevalence of depression (nurses: 30.30 percent vs.
physicians: 25.37 percent) and anxiety (nurses: 25.80 percent vs. doctors: 21.73 percent)” was
substantially greater among nurses in comparison to doctors during the COVID-19 pandemic (p. 4321).
Previous research has indicated that continuous usage of protective equipment, such as “surgical masks,
gloves, goggles, face shields, gowns, and N95 masks”, might result in physical issues like “skin lesions
and de novo PPE-associated headache” (Ruiz-Fernandez et al., 2020, p. 4321). Furthermore, reported
stress symptoms include decreased appetite or dyspepsia, exhaustion, sleeplessness, anxiety, frequent
sobbing, and even suicidal thoughts. It is hardly unexpected that junior and inexperienced nurses suffer
higher stress levels. The psychological crises can and will negatively influence nurses' safety and quality
of life in the long run (Ruiz-Fernandez et al., 2020).
It is essential to understand what the theories and literature say about nurses' experiences during the
crisis. Crisis refers to a decisive stage that bears critical consequences in the future of an individual or a
system. It also refers to an event or a situation perceived as an intolerable difficulty that exceeds
individuals' or people's available resources and coping mechanisms (Yeager & Roberts, 2015). Theories
have been used to explain nurses' and other healthcare professionals’ handling and managing the
5
the disease globally, resulting in 1.9 million deaths worldwide. In Mexico, 21% of nurses have been
infected with COVID-19, whereas 45% were infected with COVID-19 in Iran. Both countries were hardly
hit by COVID-19, shown by the report of ICN (2021). Research has shown that at least 1 in 5 healthcare
workers are showing signs of depression and anxiety, whereas 4 in 10 workers are experiencing
insomnia and a higher rate of anxiety and depression among the female nursing staff and health workers
(Pappa et al., 2020).
According to a systematic literature review conducted by Pappa et al. (2020), “the uneven and increased
distribution of workload, physical exhaustion, lack of personal protective equipment, nosocomial
transmission” as well as “the need to make ethically difficult decisions on the rationing of care” have
posed a tremendous impact on “the physical and mental well-being of nurses” (p. 902). Isolation and
loss of social support, risks of infecting loved ones and relatives as well as rapid changes in the working
environment can further compromise the resilience of nurses leading them to be at a higher risk of
experiencing a variety of psychological effects, including “acute stress disorder, depression, post-
traumatic stress disorder, insomnia, irritability, anger, and emotional exhaustion following disease
outbreak” (Pappa et al., 2020, p. 902).
Ruiz-Fernandez et al. (2020) discovered that “the prevalence of depression (nurses: 30.30 percent vs.
physicians: 25.37 percent) and anxiety (nurses: 25.80 percent vs. doctors: 21.73 percent)” was
substantially greater among nurses in comparison to doctors during the COVID-19 pandemic (p. 4321).
Previous research has indicated that continuous usage of protective equipment, such as “surgical masks,
gloves, goggles, face shields, gowns, and N95 masks”, might result in physical issues like “skin lesions
and de novo PPE-associated headache” (Ruiz-Fernandez et al., 2020, p. 4321). Furthermore, reported
stress symptoms include decreased appetite or dyspepsia, exhaustion, sleeplessness, anxiety, frequent
sobbing, and even suicidal thoughts. It is hardly unexpected that junior and inexperienced nurses suffer
higher stress levels. The psychological crises can and will negatively influence nurses' safety and quality
of life in the long run (Ruiz-Fernandez et al., 2020).
It is essential to understand what the theories and literature say about nurses' experiences during the
crisis. Crisis refers to a decisive stage that bears critical consequences in the future of an individual or a
system. It also refers to an event or a situation perceived as an intolerable difficulty that exceeds
individuals' or people's available resources and coping mechanisms (Yeager & Roberts, 2015). Theories
have been used to explain nurses' and other healthcare professionals’ handling and managing the
5
COVID-19 pandemic. An association between individual psychology and outward expression of behavior
was studied by various psychologists who came up with psychodynamic theories. They believed that
depression and other mental health issues resulted from inwardly directed anger, severe superego
demands, and the loss of self-esteem, among others. The psychodynamic theories handle a variety of
human behaviors and reactions to various issues affecting their day-to-day lives (Marčinko et al., 2020).
The psychodynamic processes are critical in gaining an in-depth understanding necessary for managing
individual and group mental health issues in times of crisis. Psychodynamic theories are being applied to
explain the general population's reaction to the current coronavirus pandemic situation. These include a
clearer understanding of behaviors such as spreading panic, stigmatization, defensive responses, and
socially disruptive behavior in times of such pandemics (Uji, 2020).
Csikszentmihalyi and Seligman (2000) defined positive psychology as a positive subjective experience
that builds positive individual qualities. The four personality traits that contribute to “positive
psychology are subjective well-being, optimism, happiness, and self-determination” (p. 6). These
subjective experiences refer to “what people think and how they feel about their lives to the cognitive
and affective conclusions they reach when they evaluate their existence” (Csikszentmihalyi & Seligman,
2000, p. 6). Positive psychology is different from humanistic psychology in that positive psychology
observes both strength and weakness as authentic and responsive to scientific understanding as
described by (Peterson & Seligman, 2004).
The “need for competence, belongingness, and autonomy” are central to the self-determination theory
and are investigated within the approach. Researchers claim that personal well-being and social
development are greatly optimized (Csikszentmihalyi & Seligman, 2000, p. 6). Optimism is more involved
in cognitive, emotional, and motivational components, according to the article published by Peterson
(2000).
When viewed from the perspective of positive psychology, an optimistic employee has more likelihood
of practicing good habits and work ethics that promote their self-development than a pessimistic one.
Positive psychology is used in preventative and therapeutic strategies that promote positive traits,
creating positive subjective experiences. These experiences can be achieved through resilience. Fear of
uncertainty can lead to anxiety or depression among workers. Positivity builds strength and creates
solutions to the problems by opening the awareness level. Positive psychology helps the healthcare
worker become more resilient and persistent (Csikszentmihalyi & Seligman, 2000).
6
was studied by various psychologists who came up with psychodynamic theories. They believed that
depression and other mental health issues resulted from inwardly directed anger, severe superego
demands, and the loss of self-esteem, among others. The psychodynamic theories handle a variety of
human behaviors and reactions to various issues affecting their day-to-day lives (Marčinko et al., 2020).
The psychodynamic processes are critical in gaining an in-depth understanding necessary for managing
individual and group mental health issues in times of crisis. Psychodynamic theories are being applied to
explain the general population's reaction to the current coronavirus pandemic situation. These include a
clearer understanding of behaviors such as spreading panic, stigmatization, defensive responses, and
socially disruptive behavior in times of such pandemics (Uji, 2020).
Csikszentmihalyi and Seligman (2000) defined positive psychology as a positive subjective experience
that builds positive individual qualities. The four personality traits that contribute to “positive
psychology are subjective well-being, optimism, happiness, and self-determination” (p. 6). These
subjective experiences refer to “what people think and how they feel about their lives to the cognitive
and affective conclusions they reach when they evaluate their existence” (Csikszentmihalyi & Seligman,
2000, p. 6). Positive psychology is different from humanistic psychology in that positive psychology
observes both strength and weakness as authentic and responsive to scientific understanding as
described by (Peterson & Seligman, 2004).
The “need for competence, belongingness, and autonomy” are central to the self-determination theory
and are investigated within the approach. Researchers claim that personal well-being and social
development are greatly optimized (Csikszentmihalyi & Seligman, 2000, p. 6). Optimism is more involved
in cognitive, emotional, and motivational components, according to the article published by Peterson
(2000).
When viewed from the perspective of positive psychology, an optimistic employee has more likelihood
of practicing good habits and work ethics that promote their self-development than a pessimistic one.
Positive psychology is used in preventative and therapeutic strategies that promote positive traits,
creating positive subjective experiences. These experiences can be achieved through resilience. Fear of
uncertainty can lead to anxiety or depression among workers. Positivity builds strength and creates
solutions to the problems by opening the awareness level. Positive psychology helps the healthcare
worker become more resilient and persistent (Csikszentmihalyi & Seligman, 2000).
6

The burdens of the COVID-19 pandemic are likely to have both short- and long-term impacts on
healthcare workers. For safe and continuous patient care, nurses´ health and safety play a crucial role in
controlling any disease outbreak. However, healthcare workers are under tremendous stress and
anxiety during the current pandemic (Cabarkapa et al., 2020). Hence, comprehensive support is needed
for health care workers and nurses during the pandemic crisis.
1.2 Rationale of the Research
Coronavirus disease 2019 (COVID-19) is an ailment caused by coronavirus that causes “severe acute
respiratory syndrome.” COVID-19 is so infectious that by January 2022, it has infected over 298 million
individuals and killed over 5.47 million people worldwide. A significant frequency of a contagious viral
illness will strain any healthcare system and its employees. Healthcare personnel are in danger of
jeopardizing their health, catching the disease, and possibly becoming a source of disease in their
community while performing their professional tasks. The physical hazards are exacerbated by the
concurrent risk of mental health disorders. It is a terrible reality that more than 180,000 healthcare
professionals have died due to the coronavirus globally. Nurses on the front lines of giving life-saving
treatment to COVID-19 patients are at a significantly increased risk of mass traumatization. Their
psychological stress and anxiety are increasingly acknowledged as significant issues. Nurses face
enormous physical and mental stress and anxiety as a result of physical tiredness from “increased
workload,” the danger of transmitting the virus, particularly with an insufficient supply of “personal
protective equipment (PPE),” and the ethical quandary of “triaging patient care.” In response to the
COVID-19, millions of nurses work as COVID-19 front liners. A considerable proportion of nurses are in
psychological turmoil during outbreaks; hence there is an urgent need to establish support mechanisms
and enhance the possible interventions for the holistic well-being of nurses during the pandemic
situation. Therefore, understanding the burdens of COVID-19 and nurses' experiences during the
outbreak is crucial in policy formulation and interventions for maintaining their health and well-being.
1.3 Research Aim, Objectives & Question
The current research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. The aim was met by addressing the following research objectives:
7
healthcare workers. For safe and continuous patient care, nurses´ health and safety play a crucial role in
controlling any disease outbreak. However, healthcare workers are under tremendous stress and
anxiety during the current pandemic (Cabarkapa et al., 2020). Hence, comprehensive support is needed
for health care workers and nurses during the pandemic crisis.
1.2 Rationale of the Research
Coronavirus disease 2019 (COVID-19) is an ailment caused by coronavirus that causes “severe acute
respiratory syndrome.” COVID-19 is so infectious that by January 2022, it has infected over 298 million
individuals and killed over 5.47 million people worldwide. A significant frequency of a contagious viral
illness will strain any healthcare system and its employees. Healthcare personnel are in danger of
jeopardizing their health, catching the disease, and possibly becoming a source of disease in their
community while performing their professional tasks. The physical hazards are exacerbated by the
concurrent risk of mental health disorders. It is a terrible reality that more than 180,000 healthcare
professionals have died due to the coronavirus globally. Nurses on the front lines of giving life-saving
treatment to COVID-19 patients are at a significantly increased risk of mass traumatization. Their
psychological stress and anxiety are increasingly acknowledged as significant issues. Nurses face
enormous physical and mental stress and anxiety as a result of physical tiredness from “increased
workload,” the danger of transmitting the virus, particularly with an insufficient supply of “personal
protective equipment (PPE),” and the ethical quandary of “triaging patient care.” In response to the
COVID-19, millions of nurses work as COVID-19 front liners. A considerable proportion of nurses are in
psychological turmoil during outbreaks; hence there is an urgent need to establish support mechanisms
and enhance the possible interventions for the holistic well-being of nurses during the pandemic
situation. Therefore, understanding the burdens of COVID-19 and nurses' experiences during the
outbreak is crucial in policy formulation and interventions for maintaining their health and well-being.
1.3 Research Aim, Objectives & Question
The current research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. The aim was met by addressing the following research objectives:
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1. To explore the levels of pandemic induced anxiety amongst the nurses
2. To study the strategies adopted by the nurses to cope with the pandemic induced anxiety
3. To determine the correlation between the anxiety levels and coping strategies adopted by the
nurses during the COVID-19 pandemic
This study attempted to answer the following research question “What are the effects of coping
strategies adopted by the nurses on their anxiety levels during the COVID-19 pandemic?”
1.4 Theoretical Framework
The following figure presents the theoretical framework of this study. The correlation between overall
coping strategies (and the three sub-scales of coping strategies) and nurses’ anxiety levels was tested to
determine the effects of the coping strategies used by the nurses on their anxiety levels during the
COVID-19 pandemic. Coping strategies (“problem-focused coping, emotion-focused coping, and
avoidant coping”) were the independent variable, and anxiety levels were the study's dependent
variable.
Figure 1.1 Theoretical framework
1.5 Study Hypotheses
The study attempted to test the following null hypothesis:
H0 = There is no effect of coping strategies on anxiety levels of nurses during the COVID-19 pandemic
The study also tested the following alternate hypotheses
H1= The use of problem-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
H2= The use of emotion-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
8
2. To study the strategies adopted by the nurses to cope with the pandemic induced anxiety
3. To determine the correlation between the anxiety levels and coping strategies adopted by the
nurses during the COVID-19 pandemic
This study attempted to answer the following research question “What are the effects of coping
strategies adopted by the nurses on their anxiety levels during the COVID-19 pandemic?”
1.4 Theoretical Framework
The following figure presents the theoretical framework of this study. The correlation between overall
coping strategies (and the three sub-scales of coping strategies) and nurses’ anxiety levels was tested to
determine the effects of the coping strategies used by the nurses on their anxiety levels during the
COVID-19 pandemic. Coping strategies (“problem-focused coping, emotion-focused coping, and
avoidant coping”) were the independent variable, and anxiety levels were the study's dependent
variable.
Figure 1.1 Theoretical framework
1.5 Study Hypotheses
The study attempted to test the following null hypothesis:
H0 = There is no effect of coping strategies on anxiety levels of nurses during the COVID-19 pandemic
The study also tested the following alternate hypotheses
H1= The use of problem-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
H2= The use of emotion-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
8
H3= The use of avoidant coping has a positive correlation with the anxiety levels of nurses during the
COVID-19 pandemic
The use of (specific) coping strategies will correlate with lowering anxiety levels and vice versa.
1.6 Outline of the Dissertation
Chapter one has provided a background to the study; study rationale; theoretical framework; research
aim, objectives, and question; and an outline of the dissertation. Chapter two consists of a review of the
existing literature on the research problem and ends at identifying a research gap that will be filled by
meeting the objectives of the current study. Chapter three offers an account of the decisions made by
the researcher regarding the way the research was conducted, that is, research methods. The chapter
includes sections on the justification for research design, study population and sample size, research
instrument, an explanation of the research process, and a discussion of ethical aspects and reliability
and validity.
Chapter four presents the results of the study. Chapter five consists of a discussion on the findings of the
study. The implications of the study findings are examined in the context of the discipline in chapter six.
Implications for theory, policy, and practice are addressed, and policy and practice recommendations
are in chapter six. Chapter seven includes a critical examination of the study’s limitations and
suggestions for future research.
Chapter Two: Literature Review
2.1 Introduction
Since this study is concerned with anxiety levels and coping strategies employed by nurses during the
COVID-19 pandemic, this chapter begins with an elucidation of the notion of anxiety. It explores how
this phenomenon affects healthcare professionals during COVID-19 in general. The chapter then heads
on to look at nurses' anxiety levels during COVID-19. Finally, the coping strategies utilized by the nurses
to overcome anxiety are discussed in the light of existing literature on the notion. The chapter ends with
identifying a research gap that will be filled by addressing the objectives of the current study.
9
COVID-19 pandemic
The use of (specific) coping strategies will correlate with lowering anxiety levels and vice versa.
1.6 Outline of the Dissertation
Chapter one has provided a background to the study; study rationale; theoretical framework; research
aim, objectives, and question; and an outline of the dissertation. Chapter two consists of a review of the
existing literature on the research problem and ends at identifying a research gap that will be filled by
meeting the objectives of the current study. Chapter three offers an account of the decisions made by
the researcher regarding the way the research was conducted, that is, research methods. The chapter
includes sections on the justification for research design, study population and sample size, research
instrument, an explanation of the research process, and a discussion of ethical aspects and reliability
and validity.
Chapter four presents the results of the study. Chapter five consists of a discussion on the findings of the
study. The implications of the study findings are examined in the context of the discipline in chapter six.
Implications for theory, policy, and practice are addressed, and policy and practice recommendations
are in chapter six. Chapter seven includes a critical examination of the study’s limitations and
suggestions for future research.
Chapter Two: Literature Review
2.1 Introduction
Since this study is concerned with anxiety levels and coping strategies employed by nurses during the
COVID-19 pandemic, this chapter begins with an elucidation of the notion of anxiety. It explores how
this phenomenon affects healthcare professionals during COVID-19 in general. The chapter then heads
on to look at nurses' anxiety levels during COVID-19. Finally, the coping strategies utilized by the nurses
to overcome anxiety are discussed in the light of existing literature on the notion. The chapter ends with
identifying a research gap that will be filled by addressing the objectives of the current study.
9

2.2 Anxiety
Anxiety has been defined in a variety of ways, such as “a disturbed state” of the body’s emotional
reactivity (Johnson, 1951), arousal (Skubic, 1986), nervousness (Ekegami, 1970), neuroticism (Kane,
1970; Pikunas, 1969) unrealistic and unpleasant state of body and mind. In medical, terminology anxiety
is defined as “apprehension of danger accompanied by restlessness and feelings of oppression in the
epigastrium” (Crooks & Stein, 1988). A variety of psychological reactions such as increased heart rate,
rapid shallow berating, sweating, muscles tension, and drying of the mouth are associated with anxiety.
Fear and anxiety differ in one crucial respect that is “Fear has an obvious cause, and once that cause is
eliminated, the fear will subside; in contrast, anxiety is less clearly linked to specific events or stimuli.”
Therefore, it tends to be more pervasive and less responsive to environmental changes (Crooks & Stein,
1988).
Fear is usually defined as a rational, emotional reaction to danger or the anticipation of danger or harm
from a real objective stimulus in the external environment. Moreover, the magnitude of fear is directly
proportional to the amount of risk that evokes it that may be unknown to others. Furthermore, the
intensity of anxiety after the danger has been objectively measured. Pressure has a variety of types,
such as “trait anxiety, state anxiety manifest anxiety, chronic anxiety specific anxiety,” etc. Spielberger
(1966) was the first anxiety theorist to differentiate between state anxiety and trait anxiety. Burton
(1976) and Martens (1971) also supported these concepts.
Anxiety can emerge at various times about the presence of a potentially stressful situation. As an
emotional reaction, anxiety is innate and plays a crucial role in shaping human behavior. Lingis (1976)
argues that in all anxious anticipation “there is a sense of void” which produces a sense of vulnerability
(the bases for distress) as well as (a level of exhilaration). Anxiety therefore, is understood not as “a solid
core of substance” but as “a current of forces assembling and dissipating itself”. Anxiety has extremely
wide dimension as is clear from various definitions given, above. Like any other emotion, anxiety is a
psycho-physiological phenomenon on the one end of which lie numerous physiological actions reactions
raising the arousal and activation level of the body and on the other, stands, a feeling tone, a cognitive
state having far reaching consequences and effect on human psyche, seen as a mental label.
10
Anxiety has been defined in a variety of ways, such as “a disturbed state” of the body’s emotional
reactivity (Johnson, 1951), arousal (Skubic, 1986), nervousness (Ekegami, 1970), neuroticism (Kane,
1970; Pikunas, 1969) unrealistic and unpleasant state of body and mind. In medical, terminology anxiety
is defined as “apprehension of danger accompanied by restlessness and feelings of oppression in the
epigastrium” (Crooks & Stein, 1988). A variety of psychological reactions such as increased heart rate,
rapid shallow berating, sweating, muscles tension, and drying of the mouth are associated with anxiety.
Fear and anxiety differ in one crucial respect that is “Fear has an obvious cause, and once that cause is
eliminated, the fear will subside; in contrast, anxiety is less clearly linked to specific events or stimuli.”
Therefore, it tends to be more pervasive and less responsive to environmental changes (Crooks & Stein,
1988).
Fear is usually defined as a rational, emotional reaction to danger or the anticipation of danger or harm
from a real objective stimulus in the external environment. Moreover, the magnitude of fear is directly
proportional to the amount of risk that evokes it that may be unknown to others. Furthermore, the
intensity of anxiety after the danger has been objectively measured. Pressure has a variety of types,
such as “trait anxiety, state anxiety manifest anxiety, chronic anxiety specific anxiety,” etc. Spielberger
(1966) was the first anxiety theorist to differentiate between state anxiety and trait anxiety. Burton
(1976) and Martens (1971) also supported these concepts.
Anxiety can emerge at various times about the presence of a potentially stressful situation. As an
emotional reaction, anxiety is innate and plays a crucial role in shaping human behavior. Lingis (1976)
argues that in all anxious anticipation “there is a sense of void” which produces a sense of vulnerability
(the bases for distress) as well as (a level of exhilaration). Anxiety therefore, is understood not as “a solid
core of substance” but as “a current of forces assembling and dissipating itself”. Anxiety has extremely
wide dimension as is clear from various definitions given, above. Like any other emotion, anxiety is a
psycho-physiological phenomenon on the one end of which lie numerous physiological actions reactions
raising the arousal and activation level of the body and on the other, stands, a feeling tone, a cognitive
state having far reaching consequences and effect on human psyche, seen as a mental label.
10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

Anxiety has often been used as a synonym for activation and arousal. Although this may not be wholly
true, we cannot escape this notion because of the vital physiological changes during anxiety. Anxiety is
documented primarily as a psychological state; it nevertheless has such psychological indices as dry
mouth, clum palms, wet forehand, increased cardio-reaction, reaction faster metabolic activity, etc.
Anxiety affects the psychological and physiological working of organisms in numerous ways. Anxious
people, for example, are considered to have poor attention management. During heightened activity
(including anxiety), attention cannot be focused on a single component of the organism's movement,
which is chaotic and intense. Anxiety typically leads to a narrowing of the field of attention when
significant stimuli are ignored, which influences the individual's judgment. Loss of knowledge appears to
be processed by people experiencing immediate (state) anxiety or whose underlying personality system
is characterized by high levels of trait anxiety (Cratly, 1989).
Anxious people have been observed to be tight or highly strung. As a result, their performance in
activities requiring precise neuromuscular coordination is significantly worse than that of less worried
people and functions in a tension-free state of body and mind. Anxiety, in a nutshell, impairs muscle
function. Cratly (1989) correctly concludes that "anxiety" is not a physical vacuum but a complex of
sentiments, including low self-esteem, helplessness, sadness, or violent thoughts and acts. The chronic
destructive emotion associated with worry and psychological turmoil (an unavoidable effect of high
anxiety syndrome) eventually leads to psycho-somatic diseases. Logically equanimity between activation
arousal and anxiety may be convincing; realistically, it is not because anxiety is a much more complex
phenomenon than the body's general activation arousal physiological state.
Fear of the unknown raises anxiety in those with pre-existing mental health disorders and healthy
people. For example, “the 2001 anthrax letter assaults in the United States” resulted in psychological
illnesses and lowered public impression of infected personnel and responders’ health (North et al.,
2009). According to the Covid-19 mental health repercussions estimates, people’s emotional responses
would most likely consist of doubt and dread. Furthermore, undesirable social behaviors would typically
be motivated by inaccurate perceptions of danger and fear (Shigemura et al., 2020). These experiences
may lead to a wide range of public mental health concerns, such as “distress reactions (such as anger,
insomnia, or fear of illness even in those who have not been exposed), health risk behaviors (such as
social isolation or alcohol and tobacco abuse),” mental health disorders (such as anxiety disorders, post-
traumatic stress disorder, or stress), and lower perceived health (Shigemura et al., 2020).
11
true, we cannot escape this notion because of the vital physiological changes during anxiety. Anxiety is
documented primarily as a psychological state; it nevertheless has such psychological indices as dry
mouth, clum palms, wet forehand, increased cardio-reaction, reaction faster metabolic activity, etc.
Anxiety affects the psychological and physiological working of organisms in numerous ways. Anxious
people, for example, are considered to have poor attention management. During heightened activity
(including anxiety), attention cannot be focused on a single component of the organism's movement,
which is chaotic and intense. Anxiety typically leads to a narrowing of the field of attention when
significant stimuli are ignored, which influences the individual's judgment. Loss of knowledge appears to
be processed by people experiencing immediate (state) anxiety or whose underlying personality system
is characterized by high levels of trait anxiety (Cratly, 1989).
Anxious people have been observed to be tight or highly strung. As a result, their performance in
activities requiring precise neuromuscular coordination is significantly worse than that of less worried
people and functions in a tension-free state of body and mind. Anxiety, in a nutshell, impairs muscle
function. Cratly (1989) correctly concludes that "anxiety" is not a physical vacuum but a complex of
sentiments, including low self-esteem, helplessness, sadness, or violent thoughts and acts. The chronic
destructive emotion associated with worry and psychological turmoil (an unavoidable effect of high
anxiety syndrome) eventually leads to psycho-somatic diseases. Logically equanimity between activation
arousal and anxiety may be convincing; realistically, it is not because anxiety is a much more complex
phenomenon than the body's general activation arousal physiological state.
Fear of the unknown raises anxiety in those with pre-existing mental health disorders and healthy
people. For example, “the 2001 anthrax letter assaults in the United States” resulted in psychological
illnesses and lowered public impression of infected personnel and responders’ health (North et al.,
2009). According to the Covid-19 mental health repercussions estimates, people’s emotional responses
would most likely consist of doubt and dread. Furthermore, undesirable social behaviors would typically
be motivated by inaccurate perceptions of danger and fear (Shigemura et al., 2020). These experiences
may lead to a wide range of public mental health concerns, such as “distress reactions (such as anger,
insomnia, or fear of illness even in those who have not been exposed), health risk behaviors (such as
social isolation or alcohol and tobacco abuse),” mental health disorders (such as anxiety disorders, post-
traumatic stress disorder, or stress), and lower perceived health (Shigemura et al., 2020).
11
2.3 Anxiety amongst Healthcare Professionals during COVID-19
The COVID-19 epidemic in December 2019 has been linked to a slew of issues, particularly for healthcare
personnel. They are on the front lines of dealing with COVID-19 pandemics and are more vulnerable to
COVID-19-related detriments. Cases of mental health issues among these groups of individuals are
associated with the excessive workload during healthcare pandemics (WHO, 2020a). Unpreparedness to
handle the surging cases of the pandemic and emotional distress related to the fear of infection
concerns include the fact that the disease is highly contagious with a low level of knowledge on the
factors surrounding the infection (Pappa et al. 2020).
Disease outbreaks, like the COVID-19 pandemic, are stressful events. Defined as a “state of uneasiness
or apprehension resulting from the anticipation of a real or perceived threatening event or situation”
(Spielberger, 2010, p. 1), during pandemics, anxiety is widespread among healthcare staff who are
directly involved in the care of infected patients. Furthermore, because of their direct interaction with
COVID-19 patients, healthcare providers are more vulnerable to “traumatic events such as patients’
suffering and death” (Pappa et al., 2020), which may exacerbate their anxiety. According to available
data, the prevalence of anxiety among healthcare providers varied from “22.6 to 36.3 percent” (Liu et
al., 2020), which was substantially higher than the general population. Nurses were shown to have the
most significant “anxiety levels and the highest prevalence of anxiety” among HCWs, ranging from “15%
to 92 percent” (Alwani et al., 2020; Luo et al., 2020; Zhu et al., 2020). Anxiety levels were shown to be
high in multiple published research, specifically among female nurses (Alwani et al., 2020; Kaveh et al.,
2020).
During the COVID-19 epidemic, nurses were most concerned about being sick or unwittingly infecting
others (Mo et al., 2020). Other sources of anxiety amongst nurses were identified by Shanafelt et al.
(2020), including “a lack of personal protective equipment (PPE), a fear of harboring the novel
coronavirus at work, a lack of access to COVID-19 testing, a fear of transmitting the virus at work, doubt
that their institution would support them if they became infected, a lack of access to childcare facilities
during the lockdown, a fear of being deployed in an unfamiliar ward or unit, and lack of accurate
information regarding the disease” (p. 2133).
Maintaining a well-engaged nursing staff is critical by implementing steps to decrease nurse anxiety and
its negative implications. Whereas a low level of fear might inspire and elicit enthusiasm in a person,
prolonged anxiety exposure can harm their physiopsychological health and work performance.
12
The COVID-19 epidemic in December 2019 has been linked to a slew of issues, particularly for healthcare
personnel. They are on the front lines of dealing with COVID-19 pandemics and are more vulnerable to
COVID-19-related detriments. Cases of mental health issues among these groups of individuals are
associated with the excessive workload during healthcare pandemics (WHO, 2020a). Unpreparedness to
handle the surging cases of the pandemic and emotional distress related to the fear of infection
concerns include the fact that the disease is highly contagious with a low level of knowledge on the
factors surrounding the infection (Pappa et al. 2020).
Disease outbreaks, like the COVID-19 pandemic, are stressful events. Defined as a “state of uneasiness
or apprehension resulting from the anticipation of a real or perceived threatening event or situation”
(Spielberger, 2010, p. 1), during pandemics, anxiety is widespread among healthcare staff who are
directly involved in the care of infected patients. Furthermore, because of their direct interaction with
COVID-19 patients, healthcare providers are more vulnerable to “traumatic events such as patients’
suffering and death” (Pappa et al., 2020), which may exacerbate their anxiety. According to available
data, the prevalence of anxiety among healthcare providers varied from “22.6 to 36.3 percent” (Liu et
al., 2020), which was substantially higher than the general population. Nurses were shown to have the
most significant “anxiety levels and the highest prevalence of anxiety” among HCWs, ranging from “15%
to 92 percent” (Alwani et al., 2020; Luo et al., 2020; Zhu et al., 2020). Anxiety levels were shown to be
high in multiple published research, specifically among female nurses (Alwani et al., 2020; Kaveh et al.,
2020).
During the COVID-19 epidemic, nurses were most concerned about being sick or unwittingly infecting
others (Mo et al., 2020). Other sources of anxiety amongst nurses were identified by Shanafelt et al.
(2020), including “a lack of personal protective equipment (PPE), a fear of harboring the novel
coronavirus at work, a lack of access to COVID-19 testing, a fear of transmitting the virus at work, doubt
that their institution would support them if they became infected, a lack of access to childcare facilities
during the lockdown, a fear of being deployed in an unfamiliar ward or unit, and lack of accurate
information regarding the disease” (p. 2133).
Maintaining a well-engaged nursing staff is critical by implementing steps to decrease nurse anxiety and
its negative implications. Whereas a low level of fear might inspire and elicit enthusiasm in a person,
prolonged anxiety exposure can harm their physiopsychological health and work performance.
12
According to several types of research, stress has been linked to a lack of appetite, dizziness, sleep
disturbances, and vomiting or nausea (e.g., Lee, 2020). Increased anxiety has also been linked to
impairment in several physical processes, “poor coping techniques (such as increased alcohol or drug
consumption), stress and sadness, and increased suicidal thoughts” (Lee et al., 2020). Moreover,
untreated anxiety can have a long-term impact on a nurse’s “work performance and job satisfaction”
that can lead to frequent absences and ultimate expenses (Labrague et al., 2018a; Lee et al., 2020).
It is critical to assist nurses in their “mental, psychological, and emotional health,” using evidence-based
strategies to successfully manage their worries or anxieties about COVID-19 (Catton, 2020). Nurses have
recognized “personal resilience and social and organizational support as critical variables in coping with
hardship and stress, helping them to preserve their mental and psychological health.” The ability of “a
person to 'bounce back' or recover quickly from a specific event, such as the COVID-19 pandemic”
(Cooper et al., 2020), as well as “support from colleagues, managers, friends, families, and the
organization” (Maben & Bridges, 2020, n.p.), can assist nurses in coping with the pandemic's burden.
However, no research has been done to see if and how coping strategies of problem-focused coping,
emotion-focused coping, and avoidant coping affect nurses’ anxiety levels. As a result, this research
aimed to investigate the causal links between these variables.
Many healthcare professionals are vulnerable to infection and mental health issues during an epidemic
of a new infectious illness (Xiang et al., 2020), as seen by the 2003 SARS outbreak. Nonetheless, given
that the Covid-19 pandemic is a worldwide phenomenon, it appears that paying attention to those
possible mental health issues is even more critical. Given the prevalence of mental health concerns that
arose during the 2003 SARS outbreak, China's National Health Commission issued a notification on
January 26, 2020, outlining the core principles for emergency psychological crisis treatments for the
Covid-19 (National Health Commission of China, 2020). Mental health treatments should be offered not
just for “patients with Covid-19 pneumonitis, close contacts, and suspected instances isolated at home,
but also for health professionals”, according to the notification. In the context of the Covid-19 epidemic,
it is critical to offer precise information to health professionals, including “regular and accurate updates
on the outbreak,” to alleviate their anxiety and concern. It's also critical to give mental health assistance
to medical practitioners (de Medeiros et al., 2020, n.p.).
2.4 Anxiety Levels of Nurses during COVID-19
13
disturbances, and vomiting or nausea (e.g., Lee, 2020). Increased anxiety has also been linked to
impairment in several physical processes, “poor coping techniques (such as increased alcohol or drug
consumption), stress and sadness, and increased suicidal thoughts” (Lee et al., 2020). Moreover,
untreated anxiety can have a long-term impact on a nurse’s “work performance and job satisfaction”
that can lead to frequent absences and ultimate expenses (Labrague et al., 2018a; Lee et al., 2020).
It is critical to assist nurses in their “mental, psychological, and emotional health,” using evidence-based
strategies to successfully manage their worries or anxieties about COVID-19 (Catton, 2020). Nurses have
recognized “personal resilience and social and organizational support as critical variables in coping with
hardship and stress, helping them to preserve their mental and psychological health.” The ability of “a
person to 'bounce back' or recover quickly from a specific event, such as the COVID-19 pandemic”
(Cooper et al., 2020), as well as “support from colleagues, managers, friends, families, and the
organization” (Maben & Bridges, 2020, n.p.), can assist nurses in coping with the pandemic's burden.
However, no research has been done to see if and how coping strategies of problem-focused coping,
emotion-focused coping, and avoidant coping affect nurses’ anxiety levels. As a result, this research
aimed to investigate the causal links between these variables.
Many healthcare professionals are vulnerable to infection and mental health issues during an epidemic
of a new infectious illness (Xiang et al., 2020), as seen by the 2003 SARS outbreak. Nonetheless, given
that the Covid-19 pandemic is a worldwide phenomenon, it appears that paying attention to those
possible mental health issues is even more critical. Given the prevalence of mental health concerns that
arose during the 2003 SARS outbreak, China's National Health Commission issued a notification on
January 26, 2020, outlining the core principles for emergency psychological crisis treatments for the
Covid-19 (National Health Commission of China, 2020). Mental health treatments should be offered not
just for “patients with Covid-19 pneumonitis, close contacts, and suspected instances isolated at home,
but also for health professionals”, according to the notification. In the context of the Covid-19 epidemic,
it is critical to offer precise information to health professionals, including “regular and accurate updates
on the outbreak,” to alleviate their anxiety and concern. It's also critical to give mental health assistance
to medical practitioners (de Medeiros et al., 2020, n.p.).
2.4 Anxiety Levels of Nurses during COVID-19
13
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
According to (World Health Organization, 2020b), nurses are the most prominent health professionals in
the health sector. They play a vital role in public health emergencies in improving public health, even
though COVID-19 has put more burden on health systems, and its impact is beyond description. Nurses'
contributions and vigilance in health promotion during epidemic outbreaks like influenza, Ebola, and
Zika were seen in the past years. Currently, nurses are at the forefront of caring for COVID-19 patients in
acute care settings (World Health Organization, 2020b.) In addition, they are engaged together with the
interprofessional sectors, teams, and communities in this global pandemic preparedness and response
(American Academy of Nursing on Policy, 2018).
The burdens of the COVID-19 pandemic are likely to have both short- and long-term impacts on
healthcare workers, even though these healthcare workers are an essential asset and infrastructure of
the health sector. For safe and continuous patient care, nurses´ health and safety play a crucial role in
controlling any disease outbreak. However, healthcare workers are under tremendous stress and
anxiety during the current pandemic (Cabarkapa et al., 2020). Nurses are at high risk because of their
essential role in COVID-19 preventive and intervention activities, such as preventing, managing, and
isolating the infection. They spend a significant amount of time with patients and are on the frontlines
during this process (Choi et al., 2020; Mo et al., 2020). Nurses who work in direct contact with COVID-19
suspected or confirmed patients are under a lot of stress, even if they take safeguards ahead of time
(Cui et al., 2021). COVID-19 is more likely to infect healthcare professionals, such as nurses, than any
other group (Cui et al., 2021). COVID-19 is causing emotional and mental distress among nurses. Nurses
face not just physiological but also an insurmountable quantity of psychological challenges, resulting in
high levels of anxiety (Choi et al., 2020; Huang & Rong, 2020; Wu et al., 2020). Being vulnerable in the
face of the prospect of not only becoming sick but also infecting their family and others around them
while working in demanding settings under severe psychological stress is one of the most prominent
causes for increasing stress among nurses (Huang & Rong, 2020; Millar, 2020). Exposure to this stressful
circumstance raises the chance of death and can cause significant physical and mental health issues, as
well as behavioral difficulties (Burgdoff et al., 2019; Li et al., 2020; Xiao et al., 2019). This unstable
condition, in which dread and worry reign supreme, has a severe impact on job performance and the
lives of nurses.
According to a systematic literature review conducted by Pappa et al. (2020), “the uneven and increased
distribution of workload, physical exhaustion, lack of personal protective equipment, nosocomial
transmission” as well as “the need to make ethically difficult decisions on the rationing of care” have
14
the health sector. They play a vital role in public health emergencies in improving public health, even
though COVID-19 has put more burden on health systems, and its impact is beyond description. Nurses'
contributions and vigilance in health promotion during epidemic outbreaks like influenza, Ebola, and
Zika were seen in the past years. Currently, nurses are at the forefront of caring for COVID-19 patients in
acute care settings (World Health Organization, 2020b.) In addition, they are engaged together with the
interprofessional sectors, teams, and communities in this global pandemic preparedness and response
(American Academy of Nursing on Policy, 2018).
The burdens of the COVID-19 pandemic are likely to have both short- and long-term impacts on
healthcare workers, even though these healthcare workers are an essential asset and infrastructure of
the health sector. For safe and continuous patient care, nurses´ health and safety play a crucial role in
controlling any disease outbreak. However, healthcare workers are under tremendous stress and
anxiety during the current pandemic (Cabarkapa et al., 2020). Nurses are at high risk because of their
essential role in COVID-19 preventive and intervention activities, such as preventing, managing, and
isolating the infection. They spend a significant amount of time with patients and are on the frontlines
during this process (Choi et al., 2020; Mo et al., 2020). Nurses who work in direct contact with COVID-19
suspected or confirmed patients are under a lot of stress, even if they take safeguards ahead of time
(Cui et al., 2021). COVID-19 is more likely to infect healthcare professionals, such as nurses, than any
other group (Cui et al., 2021). COVID-19 is causing emotional and mental distress among nurses. Nurses
face not just physiological but also an insurmountable quantity of psychological challenges, resulting in
high levels of anxiety (Choi et al., 2020; Huang & Rong, 2020; Wu et al., 2020). Being vulnerable in the
face of the prospect of not only becoming sick but also infecting their family and others around them
while working in demanding settings under severe psychological stress is one of the most prominent
causes for increasing stress among nurses (Huang & Rong, 2020; Millar, 2020). Exposure to this stressful
circumstance raises the chance of death and can cause significant physical and mental health issues, as
well as behavioral difficulties (Burgdoff et al., 2019; Li et al., 2020; Xiao et al., 2019). This unstable
condition, in which dread and worry reign supreme, has a severe impact on job performance and the
lives of nurses.
According to a systematic literature review conducted by Pappa et al. (2020), “the uneven and increased
distribution of workload, physical exhaustion, lack of personal protective equipment, nosocomial
transmission” as well as “the need to make ethically difficult decisions on the rationing of care” have
14
posed a tremendous impact on nurses’ physical and mental well-being (p. 902). Isolation and loss of
social support, as well as the risk of infecting loved ones and relatives, as well as rapid changes in the
working environment, can further weaken nurses' resilience, putting them at risk for a variety of
psychological effects such as acute stress disorder, depression, post-traumatic stress disorder, insomnia,
irritability, anger, and emotional exhaustion in the aftermath of a disease outbreak (Pappa et al., 2020).
Stelnicki et al. (2020) maintain that sudden changes in the nursing environment include concerns
associated with access to personal protective equipment, the risks of being exposed to the disease while
taking care of patients, and the unavailable rapid access to testing characteristics in many nations and
healthcare facilities. Uncertainties with the health care organizations and facilities' ability to take care of
nurses in case they contract the disease have also been a significant source of anxiety among nursing
professionals across the globe. Other causes of stress include the difficulties in the out-of-work lives of
nurses, such as access to childcare following the closure of schools and the increasing family and
personal needs due to increased pressure in the workplace. Nurses have also faced anxiety based on
internal arrangements in the workplace that may call for transfers into unfamiliar working spaces and
fields. It is due to the need to cover up the current gaps in the healthcare system. It is coupled with poor
access to up-to-date communication and information necessary for decision-making during patient care
(Stelnicki et al., 2020).
According to the studies of psychological and mental well-being of healthcare workers, the COVID-19
pandemic has shown an increase in anxiety, depression, and insomnia among nurses. It is associated
with an increased workload as the number of patients significantly rises, the inadequacy of personal
protective equipment, and the need to make ethical decisions despite the present dilemmas in the
workplace. These factors have been cited as typical in contributing to the mental and psychological
health issues facing nurses following the outbreak of the COVID-19 pandemic (Pappa et al., 2020). It is
likely to take a toll on the health and well-being of nurses. Fear and panic among the nursing staff have
posed a significant threat to their personal lives. As they seek to contain the pandemic and offer quality
care for all patients, nurses feel unsafe in the workplace, both physically and psychologically (Ho et al.,
2020). In the course of their duties, nurses are anxious about their own and their families' well-being.
Hence, fear and panic should be considered in nurse’s mental well-being in the management of
healthcare pandemics.
15
social support, as well as the risk of infecting loved ones and relatives, as well as rapid changes in the
working environment, can further weaken nurses' resilience, putting them at risk for a variety of
psychological effects such as acute stress disorder, depression, post-traumatic stress disorder, insomnia,
irritability, anger, and emotional exhaustion in the aftermath of a disease outbreak (Pappa et al., 2020).
Stelnicki et al. (2020) maintain that sudden changes in the nursing environment include concerns
associated with access to personal protective equipment, the risks of being exposed to the disease while
taking care of patients, and the unavailable rapid access to testing characteristics in many nations and
healthcare facilities. Uncertainties with the health care organizations and facilities' ability to take care of
nurses in case they contract the disease have also been a significant source of anxiety among nursing
professionals across the globe. Other causes of stress include the difficulties in the out-of-work lives of
nurses, such as access to childcare following the closure of schools and the increasing family and
personal needs due to increased pressure in the workplace. Nurses have also faced anxiety based on
internal arrangements in the workplace that may call for transfers into unfamiliar working spaces and
fields. It is due to the need to cover up the current gaps in the healthcare system. It is coupled with poor
access to up-to-date communication and information necessary for decision-making during patient care
(Stelnicki et al., 2020).
According to the studies of psychological and mental well-being of healthcare workers, the COVID-19
pandemic has shown an increase in anxiety, depression, and insomnia among nurses. It is associated
with an increased workload as the number of patients significantly rises, the inadequacy of personal
protective equipment, and the need to make ethical decisions despite the present dilemmas in the
workplace. These factors have been cited as typical in contributing to the mental and psychological
health issues facing nurses following the outbreak of the COVID-19 pandemic (Pappa et al., 2020). It is
likely to take a toll on the health and well-being of nurses. Fear and panic among the nursing staff have
posed a significant threat to their personal lives. As they seek to contain the pandemic and offer quality
care for all patients, nurses feel unsafe in the workplace, both physically and psychologically (Ho et al.,
2020). In the course of their duties, nurses are anxious about their own and their families' well-being.
Hence, fear and panic should be considered in nurse’s mental well-being in the management of
healthcare pandemics.
15
2.5 Coping Strategies
The coping strategies as peer the reviewed literature used by nurses to cope with anxiety are: Usage of
COVID-19 protective measures, avoidance coping, the role of social support, faith-based practices,
psychological support, and management support.
2.5.1 Usage of COVID-19 protective measures
The employment of COVID-19 preventive measures was the first topic recognised in the literature as a
tactic nurse used during the COVID-19 pandemic. Protective measures can also be referred to as
preventative measures. The goal of these strategies is to limit the spread of COVID-19. As a result, public
cooperation with these measures is critical to managing the COVID-19 pandemic successfully, as Padidar
et al. (2021) noted. Several researchers discussed COVID-19 preventive methods (e.g., Ali et al., 2020;
Sheroun et al., 2020; Zhang et al., 2020). Sheroun et al. (2020) conducted a cross-sectional online study
on nursing students. They discovered that the individuals were utilizing COVID-19 protective measures
in various ways, including “avoiding public places or events, washing or disinfecting hands more
frequently than usual, and avoiding public transportation such as buses and trains” (p. 285). Cai et al.
(2020) posit that the increased awareness of these preventative measures and a decrease in the number
of reported instances reduces the stress and anxiety of medical personnel such as nurses.
According to research conducted by Shahrour and Dardas (2020), the researchers have stressed the
need for nurse managers to actively safeguard the personal safety of their personnel by collaborating
closely with hospital administration to secure and deliver individual safety measures. Huang et al. (2020)
emphasise that the hospitals must provide “suitable medical protective equipment” and develop a wide
variety of treatments to prevent the transmission of infectious illnesses such as COVID-19 for creating “a
safe environment” in which COVID-19 can not spread. It promotes a positive environment and
safeguards nurses' safety, allowing them to continue giving the best possible patient care to win the
struggle against the COVID-19 epidemic. Contrary to this, Ali et al. (2020) found that “protective
measures” are not widely adopted as coping methods by all nurses. According to the study, only 75% of
participants reported using all stringent preventive measures, for instance, “protective gear, face masks,
and hand washing to lower their risk of infection” (p. 2057). According to Cui et al. (2021), nurses need
to be taught the techniques required to defend themselves against COVID-19. Enough comprehension of
COVID-19 might boost nurses' confidence, and adequate training must be provided (Zhang et al., 2020).
16
The coping strategies as peer the reviewed literature used by nurses to cope with anxiety are: Usage of
COVID-19 protective measures, avoidance coping, the role of social support, faith-based practices,
psychological support, and management support.
2.5.1 Usage of COVID-19 protective measures
The employment of COVID-19 preventive measures was the first topic recognised in the literature as a
tactic nurse used during the COVID-19 pandemic. Protective measures can also be referred to as
preventative measures. The goal of these strategies is to limit the spread of COVID-19. As a result, public
cooperation with these measures is critical to managing the COVID-19 pandemic successfully, as Padidar
et al. (2021) noted. Several researchers discussed COVID-19 preventive methods (e.g., Ali et al., 2020;
Sheroun et al., 2020; Zhang et al., 2020). Sheroun et al. (2020) conducted a cross-sectional online study
on nursing students. They discovered that the individuals were utilizing COVID-19 protective measures
in various ways, including “avoiding public places or events, washing or disinfecting hands more
frequently than usual, and avoiding public transportation such as buses and trains” (p. 285). Cai et al.
(2020) posit that the increased awareness of these preventative measures and a decrease in the number
of reported instances reduces the stress and anxiety of medical personnel such as nurses.
According to research conducted by Shahrour and Dardas (2020), the researchers have stressed the
need for nurse managers to actively safeguard the personal safety of their personnel by collaborating
closely with hospital administration to secure and deliver individual safety measures. Huang et al. (2020)
emphasise that the hospitals must provide “suitable medical protective equipment” and develop a wide
variety of treatments to prevent the transmission of infectious illnesses such as COVID-19 for creating “a
safe environment” in which COVID-19 can not spread. It promotes a positive environment and
safeguards nurses' safety, allowing them to continue giving the best possible patient care to win the
struggle against the COVID-19 epidemic. Contrary to this, Ali et al. (2020) found that “protective
measures” are not widely adopted as coping methods by all nurses. According to the study, only 75% of
participants reported using all stringent preventive measures, for instance, “protective gear, face masks,
and hand washing to lower their risk of infection” (p. 2057). According to Cui et al. (2021), nurses need
to be taught the techniques required to defend themselves against COVID-19. Enough comprehension of
COVID-19 might boost nurses' confidence, and adequate training must be provided (Zhang et al., 2020).
16
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
2.5.2 Avoidance coping
The avoidance technique was highlighted as a second theme in the literature as a method nurses utilize
in the wake of the COVID-19 epidemic. Avoidance in this context is referred to as “the act or habit of
withdrawing from or avoiding anything undesirable.” Only two reviewed papers mentioned nurses using
an avoidance strategy during the COVID-19 epidemic (Ali et al., 2020; Sheroun et al., 2020). Ali et al.
(2020) discovered that the majority of participants in an Alabama research reported: “avoiding media
coverage providing updates on COVID-19 infection and death rates” (p. 2057). However, according to Ali
et al. (2020), relying on an “avoidance strategy for nurses” may severely “limit their access to current
risk information, which may include improved research or more preventative measures” (p. 2057).
According to Sheroun et al. (2020), Erroneous news stories have also contributed to worry and panic.
2.5.3 Role of social support
Social support was recognised as a third topic in the literature reviewed by the researcher as a tactic
adopted by nurses during the COVID-19 epidemic. Social support is one of the most efficient ways for
people to cope with stressful circumstances, and according to Kim et al. (2008), it can come from a
spouse, family, friends, coworkers, or community members. Babore et al. (2020) conducted a prior study
on social support saw it as a “functional” method for dealing with difficult situations. Ali et al. (2020), Cai
et al. (2020), Gunawan et al. (2021), Shaohua et al. (2020), and Zhang et al. (2020) are five papers that
cited “social support “as a method employed by nurses for coping with the stress and anxiety during the
COVID-19 pandemic.
According to Gunawan et al. (2021), there is a need to provide support to the nurses at all times for
them to be satisfied with their work. Nurses’ stress reactions can be considerably decreased with social
backing (Shaohua et al., 2020). During the difficult stages of COVID-19, nurses, for example, place a
significant priority on family support (Cai et al., 2020; Zhang et al., 2020). Nurses are especially urged to
video connect with a loved one or get individual counseling at least once throughout their shift, as Ali et
al. (2020) reported.
2.5.4 Faith-based practices
Faith-based practices were recognised as a fourth theme in the reviewed literature as a tactic employed
by nurses during the COVID-19 epidemic. Only two of the nine publications included in the literature
17
The avoidance technique was highlighted as a second theme in the literature as a method nurses utilize
in the wake of the COVID-19 epidemic. Avoidance in this context is referred to as “the act or habit of
withdrawing from or avoiding anything undesirable.” Only two reviewed papers mentioned nurses using
an avoidance strategy during the COVID-19 epidemic (Ali et al., 2020; Sheroun et al., 2020). Ali et al.
(2020) discovered that the majority of participants in an Alabama research reported: “avoiding media
coverage providing updates on COVID-19 infection and death rates” (p. 2057). However, according to Ali
et al. (2020), relying on an “avoidance strategy for nurses” may severely “limit their access to current
risk information, which may include improved research or more preventative measures” (p. 2057).
According to Sheroun et al. (2020), Erroneous news stories have also contributed to worry and panic.
2.5.3 Role of social support
Social support was recognised as a third topic in the literature reviewed by the researcher as a tactic
adopted by nurses during the COVID-19 epidemic. Social support is one of the most efficient ways for
people to cope with stressful circumstances, and according to Kim et al. (2008), it can come from a
spouse, family, friends, coworkers, or community members. Babore et al. (2020) conducted a prior study
on social support saw it as a “functional” method for dealing with difficult situations. Ali et al. (2020), Cai
et al. (2020), Gunawan et al. (2021), Shaohua et al. (2020), and Zhang et al. (2020) are five papers that
cited “social support “as a method employed by nurses for coping with the stress and anxiety during the
COVID-19 pandemic.
According to Gunawan et al. (2021), there is a need to provide support to the nurses at all times for
them to be satisfied with their work. Nurses’ stress reactions can be considerably decreased with social
backing (Shaohua et al., 2020). During the difficult stages of COVID-19, nurses, for example, place a
significant priority on family support (Cai et al., 2020; Zhang et al., 2020). Nurses are especially urged to
video connect with a loved one or get individual counseling at least once throughout their shift, as Ali et
al. (2020) reported.
2.5.4 Faith-based practices
Faith-based practices were recognised as a fourth theme in the reviewed literature as a tactic employed
by nurses during the COVID-19 epidemic. Only two of the nine publications included in the literature
17
review for this study highlighted faith-based practices as a technique used by nurses during the COVID-
19 outbreak (e.g., Munawar & Choudhry, 2020; Savitsky et al., 2020). To cope with the COVID-19
epidemic, “faith-based behaviors and belief systems are thought to play an important part in the lives of
health workers such as nurses” (Munawar & Choudhry, 2020, p. 289).
Coping is thought to be crucial in deciding “whether a stressful situation results in adaptive or
maladaptive effects” (Dardas & Ahmad, 2015, p. 7). Contrarily, Savitsky et al. (2020, p. 102809)
discovered that “the anxiety level of religious student nurses may increase” since living a religious
lifestyle was substantially hindered throughout the COVID-19 period due to strict limitations against
worshipping in “a mosque or synagogue and using a Mikveh (Jewish ritual bath).” The findings of the
existing studies indicate the gap that needs to be filled to aid nurses in maintaining their religious
practices and lifestyle throughout the COVID-19 epidemic.
2.5.5 Psychological support
Psychological support was highlighted as the sixth topic in the reviewed literature as a tactic utilized by
nurses during the COVID-19 epidemic. Psychological assistance alleviates emotional distress, allowing
beneficiaries to “rely on their resources sooner and cope more successfully with the challenges they
experience on the road to recovery” (International Federation of Red Cross and Red Crescent Societies,
2003, n.p.).
It is highlighted by Cole et al. (2020) that psychological assistance should try to treat “mental health
issues”s that have arisen as a result of trauma or other stressful events on the frontlines. Only four
papers addressed nurses using psychological assistance as a coping technique for the COVID-19
epidemic (e.g., Huang et al., 2020; Sheroun et al., 2020; Zhang et al., 2020). It was evidenced by Huang
et al. (2020) that hospitals in Anhui Province, China, “focus on providing psychological support to nurses
as well as training in coping skills” (n.p.). According to research conducted by Zhang et al. (2020), there is
a need to provide continual attention and psychological support on a timely basis. Management and
organizations that satisfy the demands of nurses, according to these writers, should give psychological
assistance. Sheroun et al. (2020) emphasized that offering psychological support and confidence to
nursing students helps them overcome stress, cope with the lockout, and do better in their studies.
According to Shaohua et al. (2020), hospital management must also “identify and address the root
causes of the nurses' psychological difficulties as soon as possible” (n.p.). Shaohua et al. (2020) further
stress that hospital administrators should encourage nurses to use good coping mechanisms and social
18
19 outbreak (e.g., Munawar & Choudhry, 2020; Savitsky et al., 2020). To cope with the COVID-19
epidemic, “faith-based behaviors and belief systems are thought to play an important part in the lives of
health workers such as nurses” (Munawar & Choudhry, 2020, p. 289).
Coping is thought to be crucial in deciding “whether a stressful situation results in adaptive or
maladaptive effects” (Dardas & Ahmad, 2015, p. 7). Contrarily, Savitsky et al. (2020, p. 102809)
discovered that “the anxiety level of religious student nurses may increase” since living a religious
lifestyle was substantially hindered throughout the COVID-19 period due to strict limitations against
worshipping in “a mosque or synagogue and using a Mikveh (Jewish ritual bath).” The findings of the
existing studies indicate the gap that needs to be filled to aid nurses in maintaining their religious
practices and lifestyle throughout the COVID-19 epidemic.
2.5.5 Psychological support
Psychological support was highlighted as the sixth topic in the reviewed literature as a tactic utilized by
nurses during the COVID-19 epidemic. Psychological assistance alleviates emotional distress, allowing
beneficiaries to “rely on their resources sooner and cope more successfully with the challenges they
experience on the road to recovery” (International Federation of Red Cross and Red Crescent Societies,
2003, n.p.).
It is highlighted by Cole et al. (2020) that psychological assistance should try to treat “mental health
issues”s that have arisen as a result of trauma or other stressful events on the frontlines. Only four
papers addressed nurses using psychological assistance as a coping technique for the COVID-19
epidemic (e.g., Huang et al., 2020; Sheroun et al., 2020; Zhang et al., 2020). It was evidenced by Huang
et al. (2020) that hospitals in Anhui Province, China, “focus on providing psychological support to nurses
as well as training in coping skills” (n.p.). According to research conducted by Zhang et al. (2020), there is
a need to provide continual attention and psychological support on a timely basis. Management and
organizations that satisfy the demands of nurses, according to these writers, should give psychological
assistance. Sheroun et al. (2020) emphasized that offering psychological support and confidence to
nursing students helps them overcome stress, cope with the lockout, and do better in their studies.
According to Shaohua et al. (2020), hospital management must also “identify and address the root
causes of the nurses' psychological difficulties as soon as possible” (n.p.). Shaohua et al. (2020) further
stress that hospital administrators should encourage nurses to use good coping mechanisms and social
18
support to lower harmful psychological levels. It demonstrates another gap that there is a need to carry
out further research on how various nurse groups are coping with anxiety and stress during the COVID-
19 pandemic.
2.5.6 Managerial support
The sixth and final topic highlighted as a method nurses adopt during the COVID-19 epidemic in the
reviewed literature is management assistance. Managers hold a crucial role in meeting the demands of
their staff. Only three studies have discussed management support as a nursing strategy during the
COVID-19 epidemic (Ali et al., 2020; Shaohua et al., 2020). According to the study conducted by Shaohua
et al. (2020), “management should pay close attention to nurses' job pressure and mental health in
combating COVID-19”. The researchers (Shaohua et al., 2020) also stress the need for management to
identify and address the root causes of the nurses' psychological difficulties as soon as possible.
Furthermore, hospital administrators should also encourage nurses to use good coping mechanisms and
social support to lower harmful psychological levels, as noted by Shaohua et al. (2020). Ali et al. (2020)
evidenced that “the role of hospital administration offered psychological support as a critical aspect in
nurses' capacity to overcome COVID-19 problems”. Shahrour and Dardas (2020) argue that nurse
managers may take the lead in adopting “stress-reduction methods for nurses by giving consecutive rest
days, rotating challenging patient assignments, coordinating support services, and being available to the
nursing staff” (p. 2134).
2.6 Research Gap
The review of the existing literature revealed that a few current studies had been conducted to
investigate the relationship between nurses’ stress, depression, and anxiety during the COVID-19
pandemic and the coping strategies to overcome these conditions. However, no study has been
conducted to date to investigate the effects of coping strategies on nurses' anxiety levels in the UK
during the COVID-19 pandemic. The findings of this study hope to fill this research gap.
19
out further research on how various nurse groups are coping with anxiety and stress during the COVID-
19 pandemic.
2.5.6 Managerial support
The sixth and final topic highlighted as a method nurses adopt during the COVID-19 epidemic in the
reviewed literature is management assistance. Managers hold a crucial role in meeting the demands of
their staff. Only three studies have discussed management support as a nursing strategy during the
COVID-19 epidemic (Ali et al., 2020; Shaohua et al., 2020). According to the study conducted by Shaohua
et al. (2020), “management should pay close attention to nurses' job pressure and mental health in
combating COVID-19”. The researchers (Shaohua et al., 2020) also stress the need for management to
identify and address the root causes of the nurses' psychological difficulties as soon as possible.
Furthermore, hospital administrators should also encourage nurses to use good coping mechanisms and
social support to lower harmful psychological levels, as noted by Shaohua et al. (2020). Ali et al. (2020)
evidenced that “the role of hospital administration offered psychological support as a critical aspect in
nurses' capacity to overcome COVID-19 problems”. Shahrour and Dardas (2020) argue that nurse
managers may take the lead in adopting “stress-reduction methods for nurses by giving consecutive rest
days, rotating challenging patient assignments, coordinating support services, and being available to the
nursing staff” (p. 2134).
2.6 Research Gap
The review of the existing literature revealed that a few current studies had been conducted to
investigate the relationship between nurses’ stress, depression, and anxiety during the COVID-19
pandemic and the coping strategies to overcome these conditions. However, no study has been
conducted to date to investigate the effects of coping strategies on nurses' anxiety levels in the UK
during the COVID-19 pandemic. The findings of this study hope to fill this research gap.
19
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Chapter Three: Methods
3.1 Introduction
The present study is a quantitative research that investigates the effects of coping strategies used by
nurses on their anxiety levels during the COVID-19 pandemic. This chapter presents the methodological
framework adopted in the current study. The chapter comprises sections on research design, study
population, sample, and research process. Further, it sheds light on the tools used in this study to
achieve the objectives. In addition, this chapter explains the population selected for the study, the
sampling technique used to collect data, and data collection and analysis procedures. Lastly, it talks
about the ethical principles and considerations taken care of in this study.
3.2 Study Design
This study was quantitative. The researcher used a cross-sectional design that aimed to explore the
effects of coping strategies on nurses' anxiety levels during the COVID-19 pandemic. The basic rationale
for this design is to “collecting data to test hypotheses or to answer questions about people’s opinions
on some topic or issue” (Gay et al., 2012, p. 118). Online questionnaires were sent to the respondents.
3.3 Study Participants
The online questionnaires were sent to 500 nurses as the initial aim was to collect information from 500
nurses. The study population comprised nurses working in the COVID-19 wards in 10 UK hospitals. A
participation code was used to identify participants. However, 96 respondents did not correctly
complete the surveys and left certain areas blank, so these had to be eliminated, leaving the researcher
with 404 filled and finished questionnaires.
3.4 Research Tools
The following tools were used to measure the variables and establish a link between them in this study:
1. Demographic questionnaire
20
3.1 Introduction
The present study is a quantitative research that investigates the effects of coping strategies used by
nurses on their anxiety levels during the COVID-19 pandemic. This chapter presents the methodological
framework adopted in the current study. The chapter comprises sections on research design, study
population, sample, and research process. Further, it sheds light on the tools used in this study to
achieve the objectives. In addition, this chapter explains the population selected for the study, the
sampling technique used to collect data, and data collection and analysis procedures. Lastly, it talks
about the ethical principles and considerations taken care of in this study.
3.2 Study Design
This study was quantitative. The researcher used a cross-sectional design that aimed to explore the
effects of coping strategies on nurses' anxiety levels during the COVID-19 pandemic. The basic rationale
for this design is to “collecting data to test hypotheses or to answer questions about people’s opinions
on some topic or issue” (Gay et al., 2012, p. 118). Online questionnaires were sent to the respondents.
3.3 Study Participants
The online questionnaires were sent to 500 nurses as the initial aim was to collect information from 500
nurses. The study population comprised nurses working in the COVID-19 wards in 10 UK hospitals. A
participation code was used to identify participants. However, 96 respondents did not correctly
complete the surveys and left certain areas blank, so these had to be eliminated, leaving the researcher
with 404 filled and finished questionnaires.
3.4 Research Tools
The following tools were used to measure the variables and establish a link between them in this study:
1. Demographic questionnaire
20
2. The Self-Rating Anxiety Scale (SAS) (Zung, 1971)
3. Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)
Higher scores reflect higher construct values for each questionnaire measure.
Demographic questionnaire
The researcher created this questionnaire to collect information on the study respondents' backgrounds.
It gathered information on the nurses' demographic, social, and job-related aspects. The questionnaire
consisted of six items concerning the respondents’ age, gender, marital status, having children, work
experience in years, and working position (See Appendix A).
3.4.1 The Self-Rating Anxiety Scale (SAS) (Zung, 1971)
The SAS (See Appendix B), developed by ZUNG in 1971, assesses degrees of anxiety. The scale has “20
items and a 4-point scoring method” to determine “the frequency of symptoms (1 = no or little time,
two = a small part of the time, three = a considerable amount of time, and four = most or all of the
time)”. Out of these items, 15 employ negative language (e.g., "I feel more worried and anxious than
usual"; "I feel terrified for no reason") and are rated on a scale of “1 to 4”. The last five items are graded
in reverse and utilize positive language (e.g., "I feel calm and sit still easily"; "I can breathe in and out
effortlessly"). The raw score is calculated by “adding the scores of all items,” The standard score is
calculated by “multiplying the raw score by 1.25”. The higher the standard SAS score, the greater the
amount of anxiety.
Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)
"Coping" is defined broadly as an endeavor to reduce the suffering caused by unfavorable life situations.
The Brief-COPE (See Appendix C) is “a 28-item self-report questionnaire” designed to assess “successful
and inefficient coping strategies in the face of a stressful life event.” The Brief-Cope was created by Dias
et al. (2012) as a condensed “version of the original 60-item COPE scale” created by Carver et al. (1989),
which was theoretically drawn from several coping theories. Scores for three overarching coping
methods are reported as “average scores (sum of item scores divided by several items), reflecting the
extent to which the respondent has used that coping style.”
“1= I haven’t been doing this at all
2= A little bit
3= A medium amount
21
3. Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)
Higher scores reflect higher construct values for each questionnaire measure.
Demographic questionnaire
The researcher created this questionnaire to collect information on the study respondents' backgrounds.
It gathered information on the nurses' demographic, social, and job-related aspects. The questionnaire
consisted of six items concerning the respondents’ age, gender, marital status, having children, work
experience in years, and working position (See Appendix A).
3.4.1 The Self-Rating Anxiety Scale (SAS) (Zung, 1971)
The SAS (See Appendix B), developed by ZUNG in 1971, assesses degrees of anxiety. The scale has “20
items and a 4-point scoring method” to determine “the frequency of symptoms (1 = no or little time,
two = a small part of the time, three = a considerable amount of time, and four = most or all of the
time)”. Out of these items, 15 employ negative language (e.g., "I feel more worried and anxious than
usual"; "I feel terrified for no reason") and are rated on a scale of “1 to 4”. The last five items are graded
in reverse and utilize positive language (e.g., "I feel calm and sit still easily"; "I can breathe in and out
effortlessly"). The raw score is calculated by “adding the scores of all items,” The standard score is
calculated by “multiplying the raw score by 1.25”. The higher the standard SAS score, the greater the
amount of anxiety.
Coping Orientation to Problems Experienced Inventory (Brief-Cope) (Dias et al., 2012)
"Coping" is defined broadly as an endeavor to reduce the suffering caused by unfavorable life situations.
The Brief-COPE (See Appendix C) is “a 28-item self-report questionnaire” designed to assess “successful
and inefficient coping strategies in the face of a stressful life event.” The Brief-Cope was created by Dias
et al. (2012) as a condensed “version of the original 60-item COPE scale” created by Carver et al. (1989),
which was theoretically drawn from several coping theories. Scores for three overarching coping
methods are reported as “average scores (sum of item scores divided by several items), reflecting the
extent to which the respondent has used that coping style.”
“1= I haven’t been doing this at all
2= A little bit
3= A medium amount
21
4= I’ve been doing this a lot.”
With scores on the following three subscales, the scale can indicate a person's following three principal
coping styles:
“Problem-Focussed Coping
Emotion-Focussed Coping
Avoidant Coping”
The three overarching coping styles are elucidated below:
Problem-Focused Coping: “(Items 2, 7, 10, 12, 14, 17, 23, 25)”
“A high score” suggests that coping mechanisms are being used to change stressful circumstances. It is
characterized by active coping, informational assistance, planning, and positive reframing. “High scores”
indicate psychological strength, tenacity, and a practical approach to problem resolution, in addition to a
penchant for positive outcomes.
Emotion-Focused Coping: “(Items 5, 9, 13, 15, 18, 20, 21, 22, 24, 26, 27, 28)”
Venting, emotional support, comedy, acceptance, self-blame, and religion are all characteristics of
emotion-focused coping. “A high score implies coping techniques to regulate emotions related to the
stressful circumstance.” High or low scores are not universally connected with psychological wellness or
ill health, but they can be used to generate a more comprehensive assessment of the respondent's
coping methods.
Avoidant Coping: “(Items 1, 3, 4, 6, 8, 11, 16, 19)”
Self-distraction, denial, drug abuse, and behavioral disengagement are all avoidant coping. “A high score
indicates that physical or cognitive attempts were made to disconnect from the stressor.” Low scores
are usually a sign of avoidant coping.
3.5 Procedure
The link to the online questionnaire was sent via email to the nursing officers at the ten selected
hospitals. The criteria for inclusion in the study were hospitals designated for treating COVID-19
patients, which permitted participation in the study. The nursing officers then invited eligible nurses of
22
With scores on the following three subscales, the scale can indicate a person's following three principal
coping styles:
“Problem-Focussed Coping
Emotion-Focussed Coping
Avoidant Coping”
The three overarching coping styles are elucidated below:
Problem-Focused Coping: “(Items 2, 7, 10, 12, 14, 17, 23, 25)”
“A high score” suggests that coping mechanisms are being used to change stressful circumstances. It is
characterized by active coping, informational assistance, planning, and positive reframing. “High scores”
indicate psychological strength, tenacity, and a practical approach to problem resolution, in addition to a
penchant for positive outcomes.
Emotion-Focused Coping: “(Items 5, 9, 13, 15, 18, 20, 21, 22, 24, 26, 27, 28)”
Venting, emotional support, comedy, acceptance, self-blame, and religion are all characteristics of
emotion-focused coping. “A high score implies coping techniques to regulate emotions related to the
stressful circumstance.” High or low scores are not universally connected with psychological wellness or
ill health, but they can be used to generate a more comprehensive assessment of the respondent's
coping methods.
Avoidant Coping: “(Items 1, 3, 4, 6, 8, 11, 16, 19)”
Self-distraction, denial, drug abuse, and behavioral disengagement are all avoidant coping. “A high score
indicates that physical or cognitive attempts were made to disconnect from the stressor.” Low scores
are usually a sign of avoidant coping.
3.5 Procedure
The link to the online questionnaire was sent via email to the nursing officers at the ten selected
hospitals. The criteria for inclusion in the study were hospitals designated for treating COVID-19
patients, which permitted participation in the study. The nursing officers then invited eligible nurses of
22
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
involvement in the study by sending them an email linked to the questionnaires. They were provided
clear and extensive explanations in the email regarding the goal, projected time necessary to fill and
complete the online questionnaires, confidentiality, and the opportunity to refuse to participate in the
study or to withdraw at any time without providing any reason. After getting ethical permission from the
University of Wolverhampton, data collection commenced. Participation was entirely optional and
voluntary. Participants' electronic permission (See Appendix A) was gained by asking them to click on
the "agree" button. The responses were confidential since they were not asked to share their names,
email addresses, and hospital names.
3.6 Data Analysis
SPSS version 25.0 was used to analyze the data (IBM Corp., Armonk, NY, USA). The nurses' demographic,
social, and job-related variables and their reported degree of anxiety and coping mechanisms were
summarized and described using descriptive statistics. The link between coping techniques and
perceived anxiety levels was measured, and hypotheses were tested using Pearson’s correlation. The
correlation between coping strategies and reported anxiety levels was assessed using regression
analysis. Asymptotic values of 0.01 and 0.05 were considered significant.
3.7 Ethical Considerations
The researcher was responsible for adhering to ethical norms during data collection and reporting the
study's findings. The following ethical principles were taken care of:
The researcher obtained prior permission from the ethics committee of the university to
conduct the research and collect data from a human population and sample
The researcher briefed the participants on the aims and objectives of the current study through
an online information sheet
The researcher obtained the participants’ consent for participation in the study before data
collection on online consent forms
The study participants had the right to withdraw from participation in the study at any stage
without explaining the reason
23
clear and extensive explanations in the email regarding the goal, projected time necessary to fill and
complete the online questionnaires, confidentiality, and the opportunity to refuse to participate in the
study or to withdraw at any time without providing any reason. After getting ethical permission from the
University of Wolverhampton, data collection commenced. Participation was entirely optional and
voluntary. Participants' electronic permission (See Appendix A) was gained by asking them to click on
the "agree" button. The responses were confidential since they were not asked to share their names,
email addresses, and hospital names.
3.6 Data Analysis
SPSS version 25.0 was used to analyze the data (IBM Corp., Armonk, NY, USA). The nurses' demographic,
social, and job-related variables and their reported degree of anxiety and coping mechanisms were
summarized and described using descriptive statistics. The link between coping techniques and
perceived anxiety levels was measured, and hypotheses were tested using Pearson’s correlation. The
correlation between coping strategies and reported anxiety levels was assessed using regression
analysis. Asymptotic values of 0.01 and 0.05 were considered significant.
3.7 Ethical Considerations
The researcher was responsible for adhering to ethical norms during data collection and reporting the
study's findings. The following ethical principles were taken care of:
The researcher obtained prior permission from the ethics committee of the university to
conduct the research and collect data from a human population and sample
The researcher briefed the participants on the aims and objectives of the current study through
an online information sheet
The researcher obtained the participants’ consent for participation in the study before data
collection on online consent forms
The study participants had the right to withdraw from participation in the study at any stage
without explaining the reason
23
The researcher took measures to maintain the privacy and confidentiality of the study
participants
Chapter Four: Results
4.1 Introduction
The current research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. The data were analysed with the IBM statistical program for social
sciences (SPSS) version 25. For each scale, descriptive statistics and reliability analysis were provided.
For evaluating the study hypotheses, correlation analysis and regression analysis were used to measure
the associations between the study variables, independent coping strategies, and dependent variables
of anxiety levels. Three sub-scales that is problem-focused coping, emotion-focused coping, and
avoidant coping, were measured under the independent variable of coping strategies. The
asymptomatic value was estimated at two levels of significance, p≤0.01 and p≤0.05. This signifies that
“the probability of distribution of values occurring by chance is less than .01 or 1 in 100, and less
than .05 or 5 in 100” (Greasley, 2008, p. 671).
4.2 Reliability and Validity of the Data
Since the two scales used for this study are already established hierarchies, there was no need to test
their reliability. However, validity was confirmed in this study. The external reality, according to Cohen
et al. (2000, p. 107), is "the degree to which the results may be generalized [sic] to the wider
population.” External validity is associated with “generalizability.” It was kept by ensuring that the
sample size (n=404) was large enough to produce statistically significant findings. However, it was not
practicable to include all of the nurses in the United Kingdom. As a result, the sample was limited to
nurses from ten hospitals in the United Kingdom. It made it difficult to generalize the study's findings to
a more extensive selection of nurses working in the COVID wards in the UK.
Internal validity, in contrast, is "concerned with the extent to which explanations can be sustained by
the data" (Cohen et al., 2000, p 107). It was achieved by gathering data from three self-reporting
surveys, in which respondents filled out the questionnaires independently and gave the information on
24
participants
Chapter Four: Results
4.1 Introduction
The current research aimed to investigate the effects of coping strategies on nurses' anxiety levels
during the COVID-19 pandemic. The data were analysed with the IBM statistical program for social
sciences (SPSS) version 25. For each scale, descriptive statistics and reliability analysis were provided.
For evaluating the study hypotheses, correlation analysis and regression analysis were used to measure
the associations between the study variables, independent coping strategies, and dependent variables
of anxiety levels. Three sub-scales that is problem-focused coping, emotion-focused coping, and
avoidant coping, were measured under the independent variable of coping strategies. The
asymptomatic value was estimated at two levels of significance, p≤0.01 and p≤0.05. This signifies that
“the probability of distribution of values occurring by chance is less than .01 or 1 in 100, and less
than .05 or 5 in 100” (Greasley, 2008, p. 671).
4.2 Reliability and Validity of the Data
Since the two scales used for this study are already established hierarchies, there was no need to test
their reliability. However, validity was confirmed in this study. The external reality, according to Cohen
et al. (2000, p. 107), is "the degree to which the results may be generalized [sic] to the wider
population.” External validity is associated with “generalizability.” It was kept by ensuring that the
sample size (n=404) was large enough to produce statistically significant findings. However, it was not
practicable to include all of the nurses in the United Kingdom. As a result, the sample was limited to
nurses from ten hospitals in the United Kingdom. It made it difficult to generalize the study's findings to
a more extensive selection of nurses working in the COVID wards in the UK.
Internal validity, in contrast, is "concerned with the extent to which explanations can be sustained by
the data" (Cohen et al., 2000, p 107). It was achieved by gathering data from three self-reporting
surveys, in which respondents filled out the questionnaires independently and gave the information on
24
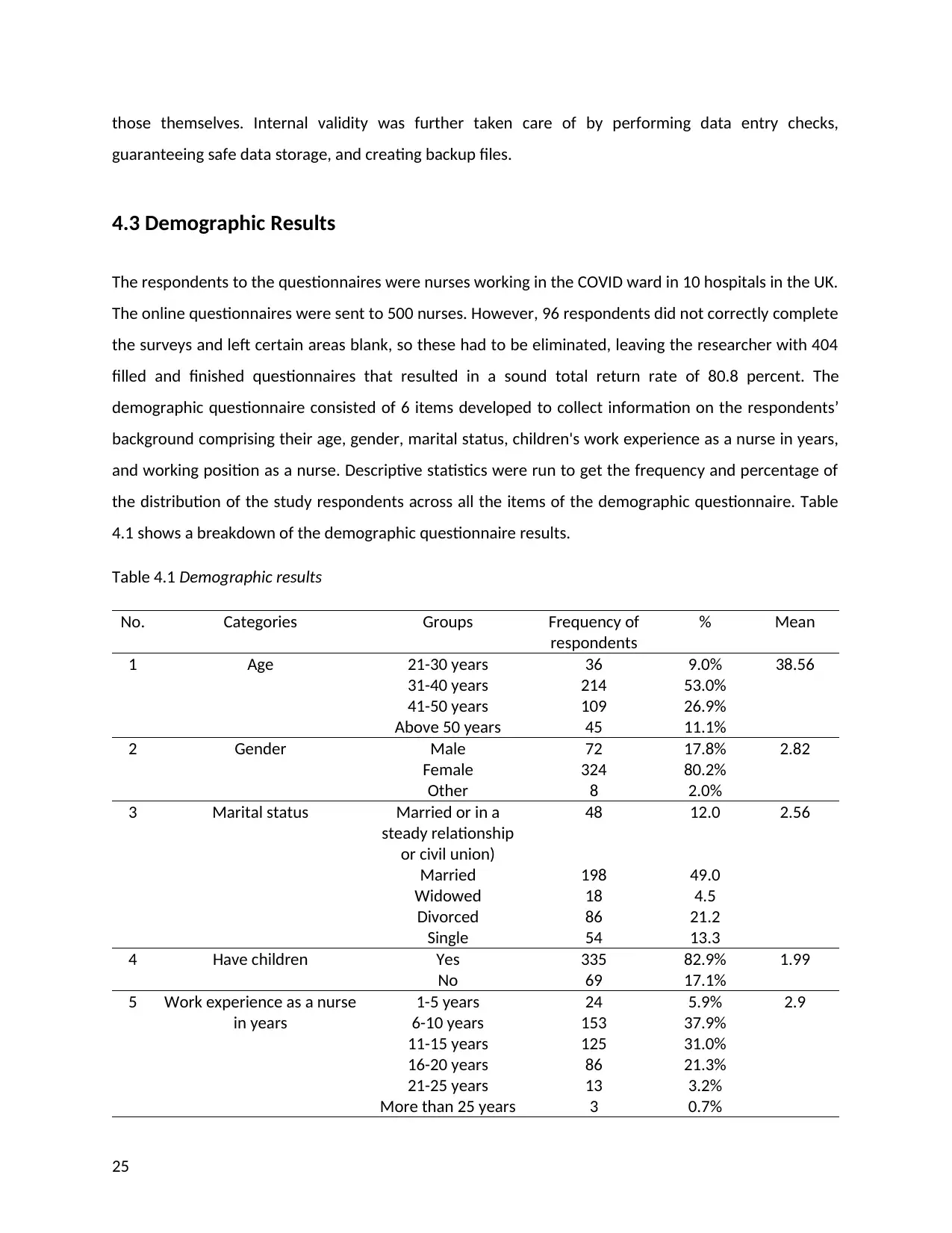
those themselves. Internal validity was further taken care of by performing data entry checks,
guaranteeing safe data storage, and creating backup files.
4.3 Demographic Results
The respondents to the questionnaires were nurses working in the COVID ward in 10 hospitals in the UK.
The online questionnaires were sent to 500 nurses. However, 96 respondents did not correctly complete
the surveys and left certain areas blank, so these had to be eliminated, leaving the researcher with 404
filled and finished questionnaires that resulted in a sound total return rate of 80.8 percent. The
demographic questionnaire consisted of 6 items developed to collect information on the respondents’
background comprising their age, gender, marital status, children's work experience as a nurse in years,
and working position as a nurse. Descriptive statistics were run to get the frequency and percentage of
the distribution of the study respondents across all the items of the demographic questionnaire. Table
4.1 shows a breakdown of the demographic questionnaire results.
Table 4.1 Demographic results
No. Categories Groups Frequency of
respondents
% Mean
1 Age 21-30 years
31-40 years
41-50 years
Above 50 years
36
214
109
45
9.0%
53.0%
26.9%
11.1%
38.56
2 Gender Male
Female
Other
72
324
8
17.8%
80.2%
2.0%
2.82
3 Marital status Married or in a
steady relationship
or civil union)
Married
Widowed
Divorced
Single
48
198
18
86
54
12.0
49.0
4.5
21.2
13.3
2.56
4 Have children Yes
No
335
69
82.9%
17.1%
1.99
5 Work experience as a nurse
in years
1-5 years
6-10 years
11-15 years
16-20 years
21-25 years
More than 25 years
24
153
125
86
13
3
5.9%
37.9%
31.0%
21.3%
3.2%
0.7%
2.9
25
guaranteeing safe data storage, and creating backup files.
4.3 Demographic Results
The respondents to the questionnaires were nurses working in the COVID ward in 10 hospitals in the UK.
The online questionnaires were sent to 500 nurses. However, 96 respondents did not correctly complete
the surveys and left certain areas blank, so these had to be eliminated, leaving the researcher with 404
filled and finished questionnaires that resulted in a sound total return rate of 80.8 percent. The
demographic questionnaire consisted of 6 items developed to collect information on the respondents’
background comprising their age, gender, marital status, children's work experience as a nurse in years,
and working position as a nurse. Descriptive statistics were run to get the frequency and percentage of
the distribution of the study respondents across all the items of the demographic questionnaire. Table
4.1 shows a breakdown of the demographic questionnaire results.
Table 4.1 Demographic results
No. Categories Groups Frequency of
respondents
% Mean
1 Age 21-30 years
31-40 years
41-50 years
Above 50 years
36
214
109
45
9.0%
53.0%
26.9%
11.1%
38.56
2 Gender Male
Female
Other
72
324
8
17.8%
80.2%
2.0%
2.82
3 Marital status Married or in a
steady relationship
or civil union)
Married
Widowed
Divorced
Single
48
198
18
86
54
12.0
49.0
4.5
21.2
13.3
2.56
4 Have children Yes
No
335
69
82.9%
17.1%
1.99
5 Work experience as a nurse
in years
1-5 years
6-10 years
11-15 years
16-20 years
21-25 years
More than 25 years
24
153
125
86
13
3
5.9%
37.9%
31.0%
21.3%
3.2%
0.7%
2.9
25
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
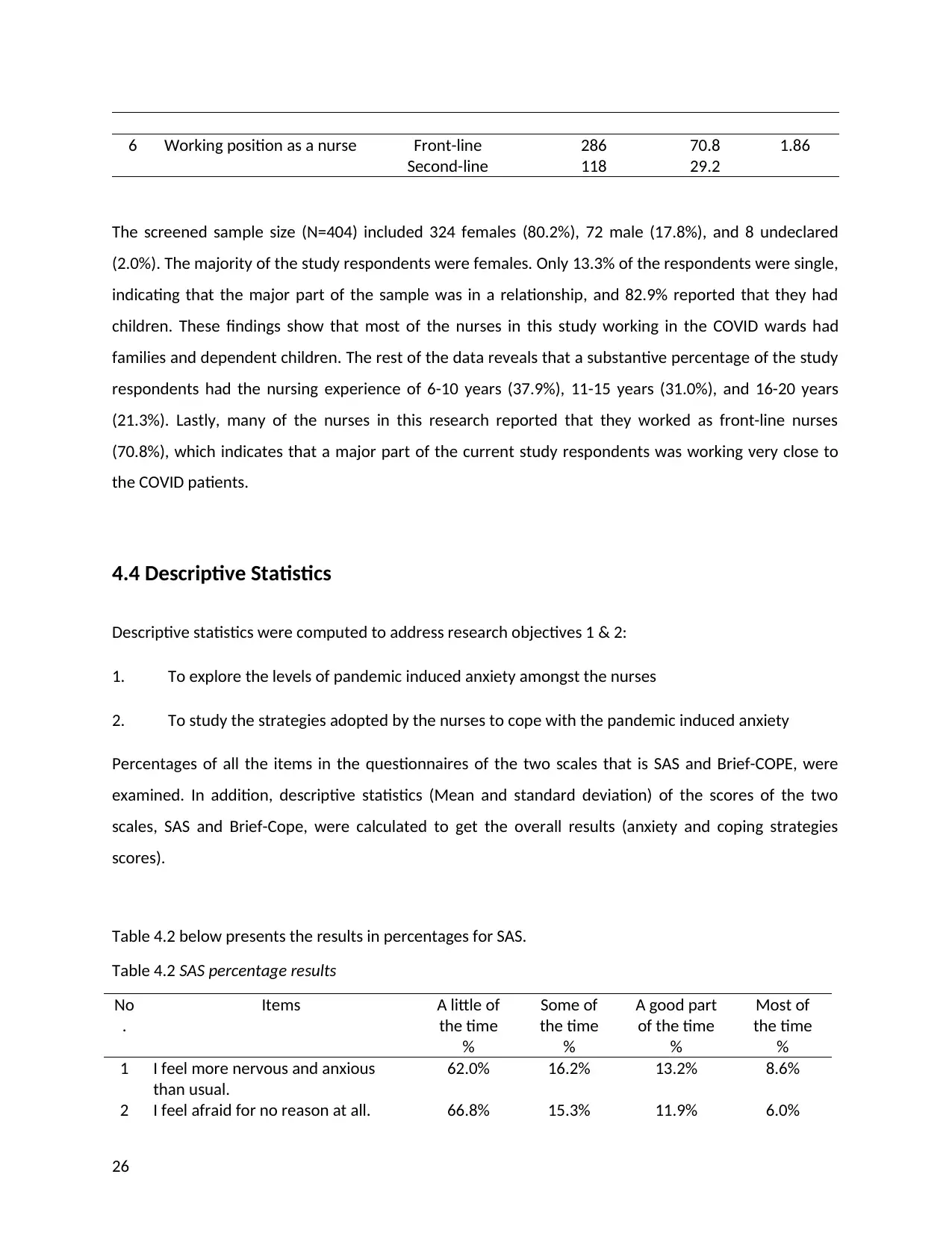
6 Working position as a nurse Front-line
Second-line
286
118
70.8
29.2
1.86
The screened sample size (N=404) included 324 females (80.2%), 72 male (17.8%), and 8 undeclared
(2.0%). The majority of the study respondents were females. Only 13.3% of the respondents were single,
indicating that the major part of the sample was in a relationship, and 82.9% reported that they had
children. These findings show that most of the nurses in this study working in the COVID wards had
families and dependent children. The rest of the data reveals that a substantive percentage of the study
respondents had the nursing experience of 6-10 years (37.9%), 11-15 years (31.0%), and 16-20 years
(21.3%). Lastly, many of the nurses in this research reported that they worked as front-line nurses
(70.8%), which indicates that a major part of the current study respondents was working very close to
the COVID patients.
4.4 Descriptive Statistics
Descriptive statistics were computed to address research objectives 1 & 2:
1. To explore the levels of pandemic induced anxiety amongst the nurses
2. To study the strategies adopted by the nurses to cope with the pandemic induced anxiety
Percentages of all the items in the questionnaires of the two scales that is SAS and Brief-COPE, were
examined. In addition, descriptive statistics (Mean and standard deviation) of the scores of the two
scales, SAS and Brief-Cope, were calculated to get the overall results (anxiety and coping strategies
scores).
Table 4.2 below presents the results in percentages for SAS.
Table 4.2 SAS percentage results
No
.
Items A little of
the time
%
Some of
the time
%
A good part
of the time
%
Most of
the time
%
1 I feel more nervous and anxious
than usual.
62.0% 16.2% 13.2% 8.6%
2 I feel afraid for no reason at all. 66.8% 15.3% 11.9% 6.0%
26
Second-line
286
118
70.8
29.2
1.86
The screened sample size (N=404) included 324 females (80.2%), 72 male (17.8%), and 8 undeclared
(2.0%). The majority of the study respondents were females. Only 13.3% of the respondents were single,
indicating that the major part of the sample was in a relationship, and 82.9% reported that they had
children. These findings show that most of the nurses in this study working in the COVID wards had
families and dependent children. The rest of the data reveals that a substantive percentage of the study
respondents had the nursing experience of 6-10 years (37.9%), 11-15 years (31.0%), and 16-20 years
(21.3%). Lastly, many of the nurses in this research reported that they worked as front-line nurses
(70.8%), which indicates that a major part of the current study respondents was working very close to
the COVID patients.
4.4 Descriptive Statistics
Descriptive statistics were computed to address research objectives 1 & 2:
1. To explore the levels of pandemic induced anxiety amongst the nurses
2. To study the strategies adopted by the nurses to cope with the pandemic induced anxiety
Percentages of all the items in the questionnaires of the two scales that is SAS and Brief-COPE, were
examined. In addition, descriptive statistics (Mean and standard deviation) of the scores of the two
scales, SAS and Brief-Cope, were calculated to get the overall results (anxiety and coping strategies
scores).
Table 4.2 below presents the results in percentages for SAS.
Table 4.2 SAS percentage results
No
.
Items A little of
the time
%
Some of
the time
%
A good part
of the time
%
Most of
the time
%
1 I feel more nervous and anxious
than usual.
62.0% 16.2% 13.2% 8.6%
2 I feel afraid for no reason at all. 66.8% 15.3% 11.9% 6.0%
26
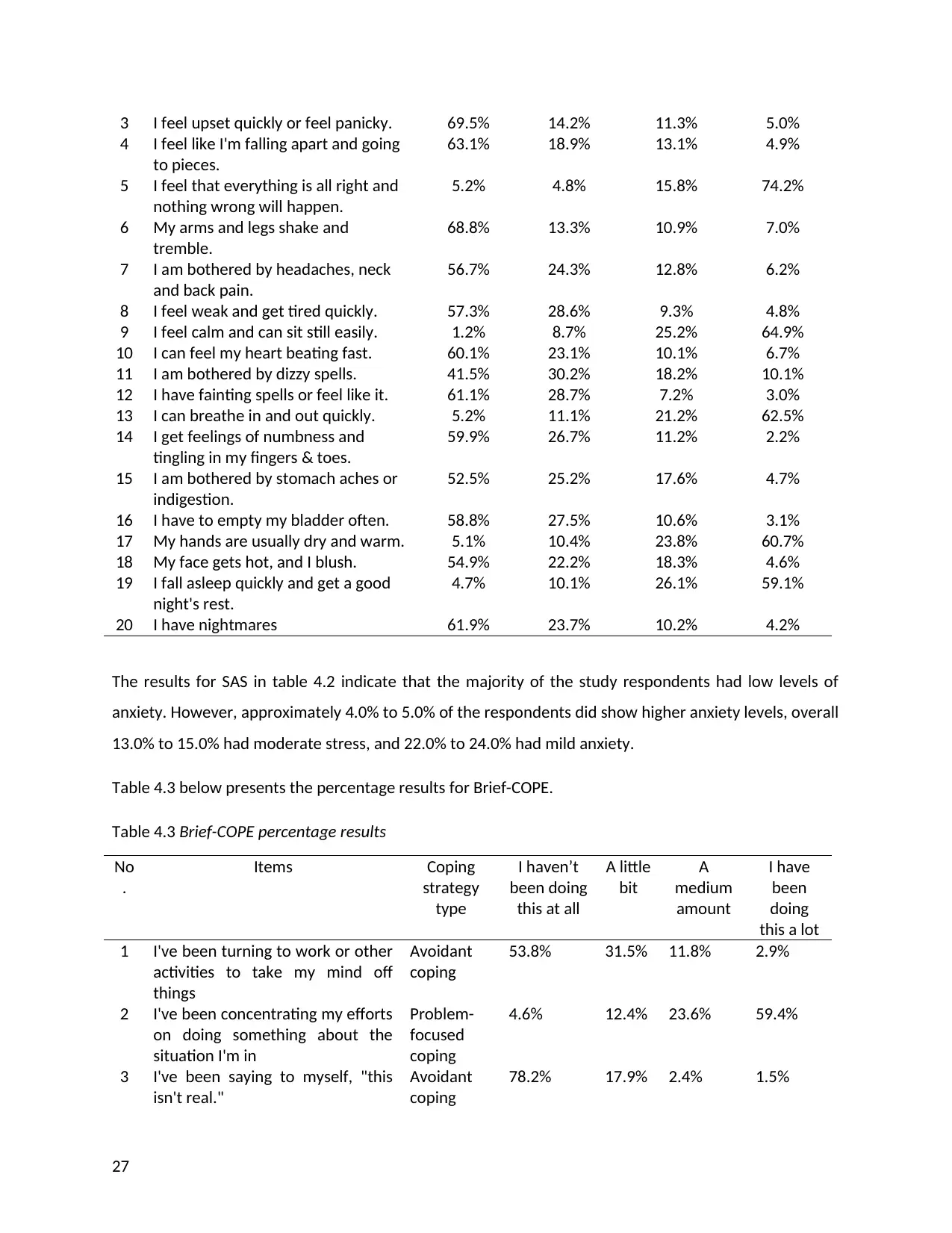
3 I feel upset quickly or feel panicky. 69.5% 14.2% 11.3% 5.0%
4 I feel like I'm falling apart and going
to pieces.
63.1% 18.9% 13.1% 4.9%
5 I feel that everything is all right and
nothing wrong will happen.
5.2% 4.8% 15.8% 74.2%
6 My arms and legs shake and
tremble.
68.8% 13.3% 10.9% 7.0%
7 I am bothered by headaches, neck
and back pain.
56.7% 24.3% 12.8% 6.2%
8 I feel weak and get tired quickly. 57.3% 28.6% 9.3% 4.8%
9 I feel calm and can sit still easily. 1.2% 8.7% 25.2% 64.9%
10 I can feel my heart beating fast. 60.1% 23.1% 10.1% 6.7%
11 I am bothered by dizzy spells. 41.5% 30.2% 18.2% 10.1%
12 I have fainting spells or feel like it. 61.1% 28.7% 7.2% 3.0%
13 I can breathe in and out quickly. 5.2% 11.1% 21.2% 62.5%
14 I get feelings of numbness and
tingling in my fingers & toes.
59.9% 26.7% 11.2% 2.2%
15 I am bothered by stomach aches or
indigestion.
52.5% 25.2% 17.6% 4.7%
16 I have to empty my bladder often. 58.8% 27.5% 10.6% 3.1%
17 My hands are usually dry and warm. 5.1% 10.4% 23.8% 60.7%
18 My face gets hot, and I blush. 54.9% 22.2% 18.3% 4.6%
19 I fall asleep quickly and get a good
night's rest.
4.7% 10.1% 26.1% 59.1%
20 I have nightmares 61.9% 23.7% 10.2% 4.2%
The results for SAS in table 4.2 indicate that the majority of the study respondents had low levels of
anxiety. However, approximately 4.0% to 5.0% of the respondents did show higher anxiety levels, overall
13.0% to 15.0% had moderate stress, and 22.0% to 24.0% had mild anxiety.
Table 4.3 below presents the percentage results for Brief-COPE.
Table 4.3 Brief-COPE percentage results
No
.
Items Coping
strategy
type
I haven’t
been doing
this at all
A little
bit
A
medium
amount
I have
been
doing
this a lot
1 I've been turning to work or other
activities to take my mind off
things
Avoidant
coping
53.8% 31.5% 11.8% 2.9%
2 I've been concentrating my efforts
on doing something about the
situation I'm in
Problem-
focused
coping
4.6% 12.4% 23.6% 59.4%
3 I've been saying to myself, "this
isn't real."
Avoidant
coping
78.2% 17.9% 2.4% 1.5%
27
4 I feel like I'm falling apart and going
to pieces.
63.1% 18.9% 13.1% 4.9%
5 I feel that everything is all right and
nothing wrong will happen.
5.2% 4.8% 15.8% 74.2%
6 My arms and legs shake and
tremble.
68.8% 13.3% 10.9% 7.0%
7 I am bothered by headaches, neck
and back pain.
56.7% 24.3% 12.8% 6.2%
8 I feel weak and get tired quickly. 57.3% 28.6% 9.3% 4.8%
9 I feel calm and can sit still easily. 1.2% 8.7% 25.2% 64.9%
10 I can feel my heart beating fast. 60.1% 23.1% 10.1% 6.7%
11 I am bothered by dizzy spells. 41.5% 30.2% 18.2% 10.1%
12 I have fainting spells or feel like it. 61.1% 28.7% 7.2% 3.0%
13 I can breathe in and out quickly. 5.2% 11.1% 21.2% 62.5%
14 I get feelings of numbness and
tingling in my fingers & toes.
59.9% 26.7% 11.2% 2.2%
15 I am bothered by stomach aches or
indigestion.
52.5% 25.2% 17.6% 4.7%
16 I have to empty my bladder often. 58.8% 27.5% 10.6% 3.1%
17 My hands are usually dry and warm. 5.1% 10.4% 23.8% 60.7%
18 My face gets hot, and I blush. 54.9% 22.2% 18.3% 4.6%
19 I fall asleep quickly and get a good
night's rest.
4.7% 10.1% 26.1% 59.1%
20 I have nightmares 61.9% 23.7% 10.2% 4.2%
The results for SAS in table 4.2 indicate that the majority of the study respondents had low levels of
anxiety. However, approximately 4.0% to 5.0% of the respondents did show higher anxiety levels, overall
13.0% to 15.0% had moderate stress, and 22.0% to 24.0% had mild anxiety.
Table 4.3 below presents the percentage results for Brief-COPE.
Table 4.3 Brief-COPE percentage results
No
.
Items Coping
strategy
type
I haven’t
been doing
this at all
A little
bit
A
medium
amount
I have
been
doing
this a lot
1 I've been turning to work or other
activities to take my mind off
things
Avoidant
coping
53.8% 31.5% 11.8% 2.9%
2 I've been concentrating my efforts
on doing something about the
situation I'm in
Problem-
focused
coping
4.6% 12.4% 23.6% 59.4%
3 I've been saying to myself, "this
isn't real."
Avoidant
coping
78.2% 17.9% 2.4% 1.5%
27
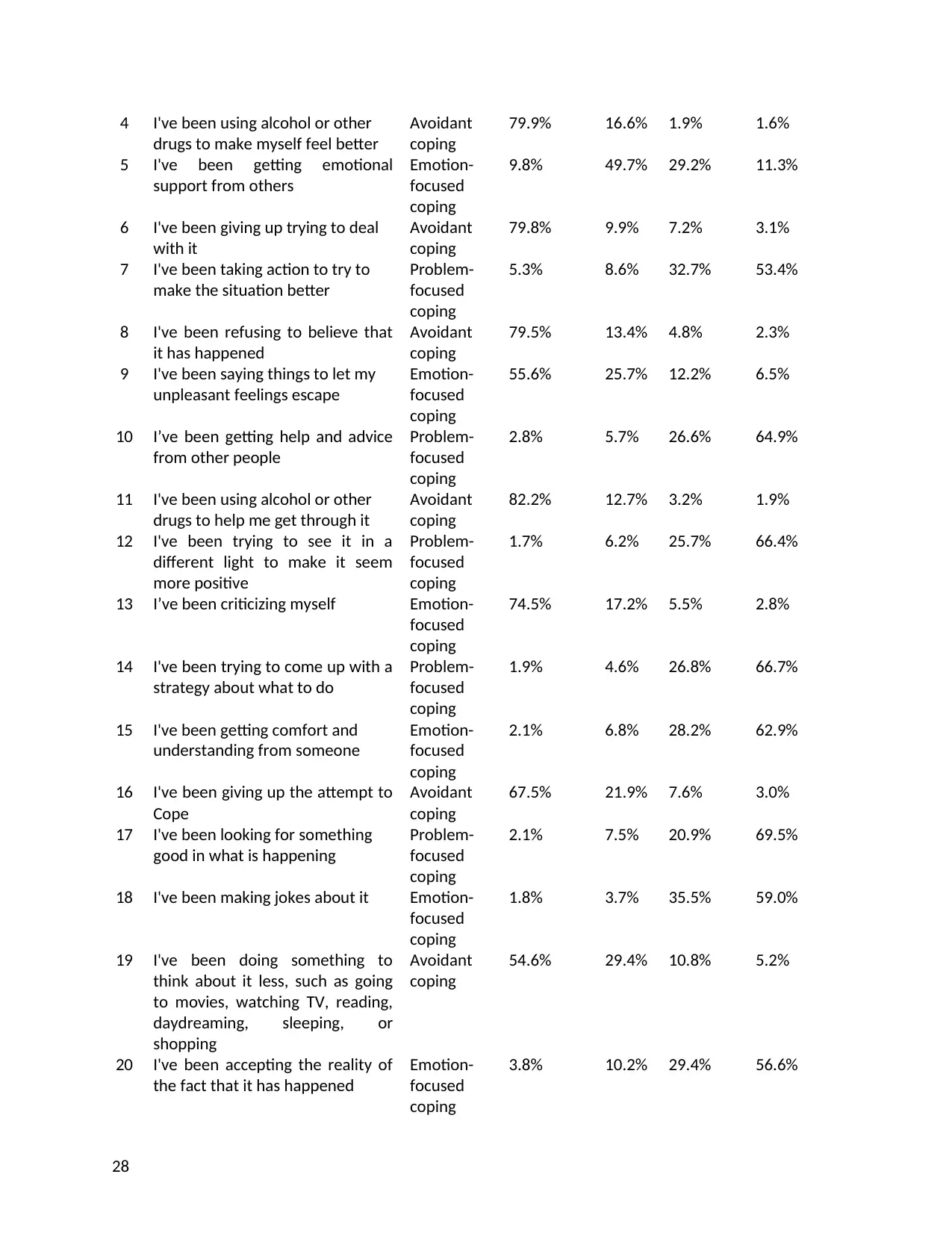
4 I've been using alcohol or other
drugs to make myself feel better
Avoidant
coping
79.9% 16.6% 1.9% 1.6%
5 I've been getting emotional
support from others
Emotion-
focused
coping
9.8% 49.7% 29.2% 11.3%
6 I've been giving up trying to deal
with it
Avoidant
coping
79.8% 9.9% 7.2% 3.1%
7 I've been taking action to try to
make the situation better
Problem-
focused
coping
5.3% 8.6% 32.7% 53.4%
8 I've been refusing to believe that
it has happened
Avoidant
coping
79.5% 13.4% 4.8% 2.3%
9 I've been saying things to let my
unpleasant feelings escape
Emotion-
focused
coping
55.6% 25.7% 12.2% 6.5%
10 I’ve been getting help and advice
from other people
Problem-
focused
coping
2.8% 5.7% 26.6% 64.9%
11 I've been using alcohol or other
drugs to help me get through it
Avoidant
coping
82.2% 12.7% 3.2% 1.9%
12 I've been trying to see it in a
different light to make it seem
more positive
Problem-
focused
coping
1.7% 6.2% 25.7% 66.4%
13 I’ve been criticizing myself Emotion-
focused
coping
74.5% 17.2% 5.5% 2.8%
14 I've been trying to come up with a
strategy about what to do
Problem-
focused
coping
1.9% 4.6% 26.8% 66.7%
15 I've been getting comfort and
understanding from someone
Emotion-
focused
coping
2.1% 6.8% 28.2% 62.9%
16 I've been giving up the attempt to
Cope
Avoidant
coping
67.5% 21.9% 7.6% 3.0%
17 I've been looking for something
good in what is happening
Problem-
focused
coping
2.1% 7.5% 20.9% 69.5%
18 I've been making jokes about it Emotion-
focused
coping
1.8% 3.7% 35.5% 59.0%
19 I've been doing something to
think about it less, such as going
to movies, watching TV, reading,
daydreaming, sleeping, or
shopping
Avoidant
coping
54.6% 29.4% 10.8% 5.2%
20 I've been accepting the reality of
the fact that it has happened
Emotion-
focused
coping
3.8% 10.2% 29.4% 56.6%
28
drugs to make myself feel better
Avoidant
coping
79.9% 16.6% 1.9% 1.6%
5 I've been getting emotional
support from others
Emotion-
focused
coping
9.8% 49.7% 29.2% 11.3%
6 I've been giving up trying to deal
with it
Avoidant
coping
79.8% 9.9% 7.2% 3.1%
7 I've been taking action to try to
make the situation better
Problem-
focused
coping
5.3% 8.6% 32.7% 53.4%
8 I've been refusing to believe that
it has happened
Avoidant
coping
79.5% 13.4% 4.8% 2.3%
9 I've been saying things to let my
unpleasant feelings escape
Emotion-
focused
coping
55.6% 25.7% 12.2% 6.5%
10 I’ve been getting help and advice
from other people
Problem-
focused
coping
2.8% 5.7% 26.6% 64.9%
11 I've been using alcohol or other
drugs to help me get through it
Avoidant
coping
82.2% 12.7% 3.2% 1.9%
12 I've been trying to see it in a
different light to make it seem
more positive
Problem-
focused
coping
1.7% 6.2% 25.7% 66.4%
13 I’ve been criticizing myself Emotion-
focused
coping
74.5% 17.2% 5.5% 2.8%
14 I've been trying to come up with a
strategy about what to do
Problem-
focused
coping
1.9% 4.6% 26.8% 66.7%
15 I've been getting comfort and
understanding from someone
Emotion-
focused
coping
2.1% 6.8% 28.2% 62.9%
16 I've been giving up the attempt to
Cope
Avoidant
coping
67.5% 21.9% 7.6% 3.0%
17 I've been looking for something
good in what is happening
Problem-
focused
coping
2.1% 7.5% 20.9% 69.5%
18 I've been making jokes about it Emotion-
focused
coping
1.8% 3.7% 35.5% 59.0%
19 I've been doing something to
think about it less, such as going
to movies, watching TV, reading,
daydreaming, sleeping, or
shopping
Avoidant
coping
54.6% 29.4% 10.8% 5.2%
20 I've been accepting the reality of
the fact that it has happened
Emotion-
focused
coping
3.8% 10.2% 29.4% 56.6%
28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
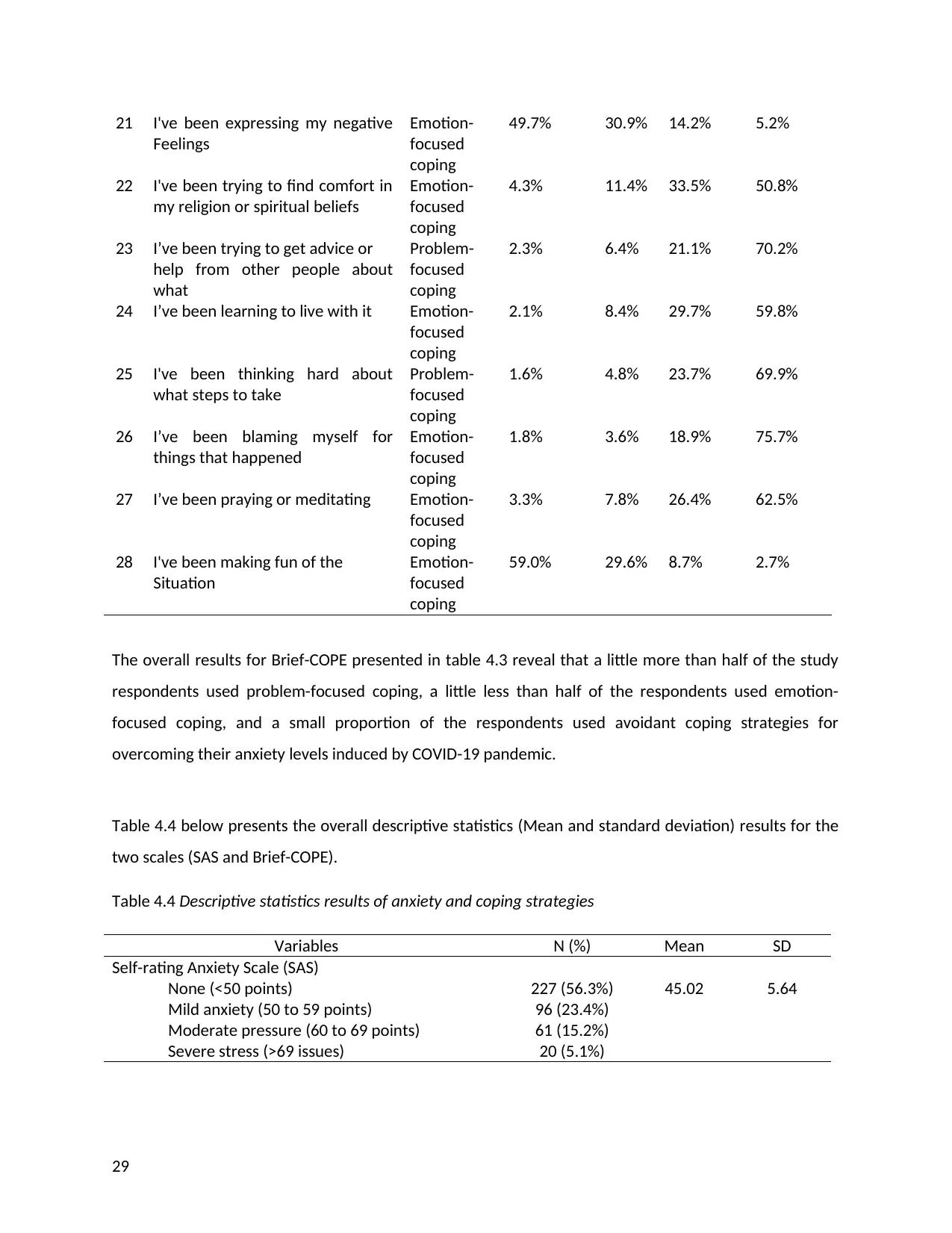
21 I've been expressing my negative
Feelings
Emotion-
focused
coping
49.7% 30.9% 14.2% 5.2%
22 I've been trying to find comfort in
my religion or spiritual beliefs
Emotion-
focused
coping
4.3% 11.4% 33.5% 50.8%
23 I’ve been trying to get advice or
help from other people about
what
Problem-
focused
coping
2.3% 6.4% 21.1% 70.2%
24 I’ve been learning to live with it Emotion-
focused
coping
2.1% 8.4% 29.7% 59.8%
25 I've been thinking hard about
what steps to take
Problem-
focused
coping
1.6% 4.8% 23.7% 69.9%
26 I’ve been blaming myself for
things that happened
Emotion-
focused
coping
1.8% 3.6% 18.9% 75.7%
27 I’ve been praying or meditating Emotion-
focused
coping
3.3% 7.8% 26.4% 62.5%
28 I've been making fun of the
Situation
Emotion-
focused
coping
59.0% 29.6% 8.7% 2.7%
The overall results for Brief-COPE presented in table 4.3 reveal that a little more than half of the study
respondents used problem-focused coping, a little less than half of the respondents used emotion-
focused coping, and a small proportion of the respondents used avoidant coping strategies for
overcoming their anxiety levels induced by COVID-19 pandemic.
Table 4.4 below presents the overall descriptive statistics (Mean and standard deviation) results for the
two scales (SAS and Brief-COPE).
Table 4.4 Descriptive statistics results of anxiety and coping strategies
Variables N (%) Mean SD
Self-rating Anxiety Scale (SAS)
None (<50 points)
Mild anxiety (50 to 59 points)
Moderate pressure (60 to 69 points)
Severe stress (>69 issues)
227 (56.3%)
96 (23.4%)
61 (15.2%)
20 (5.1%)
45.02 5.64
29
Feelings
Emotion-
focused
coping
49.7% 30.9% 14.2% 5.2%
22 I've been trying to find comfort in
my religion or spiritual beliefs
Emotion-
focused
coping
4.3% 11.4% 33.5% 50.8%
23 I’ve been trying to get advice or
help from other people about
what
Problem-
focused
coping
2.3% 6.4% 21.1% 70.2%
24 I’ve been learning to live with it Emotion-
focused
coping
2.1% 8.4% 29.7% 59.8%
25 I've been thinking hard about
what steps to take
Problem-
focused
coping
1.6% 4.8% 23.7% 69.9%
26 I’ve been blaming myself for
things that happened
Emotion-
focused
coping
1.8% 3.6% 18.9% 75.7%
27 I’ve been praying or meditating Emotion-
focused
coping
3.3% 7.8% 26.4% 62.5%
28 I've been making fun of the
Situation
Emotion-
focused
coping
59.0% 29.6% 8.7% 2.7%
The overall results for Brief-COPE presented in table 4.3 reveal that a little more than half of the study
respondents used problem-focused coping, a little less than half of the respondents used emotion-
focused coping, and a small proportion of the respondents used avoidant coping strategies for
overcoming their anxiety levels induced by COVID-19 pandemic.
Table 4.4 below presents the overall descriptive statistics (Mean and standard deviation) results for the
two scales (SAS and Brief-COPE).
Table 4.4 Descriptive statistics results of anxiety and coping strategies
Variables N (%) Mean SD
Self-rating Anxiety Scale (SAS)
None (<50 points)
Mild anxiety (50 to 59 points)
Moderate pressure (60 to 69 points)
Severe stress (>69 issues)
227 (56.3%)
96 (23.4%)
61 (15.2%)
20 (5.1%)
45.02 5.64
29
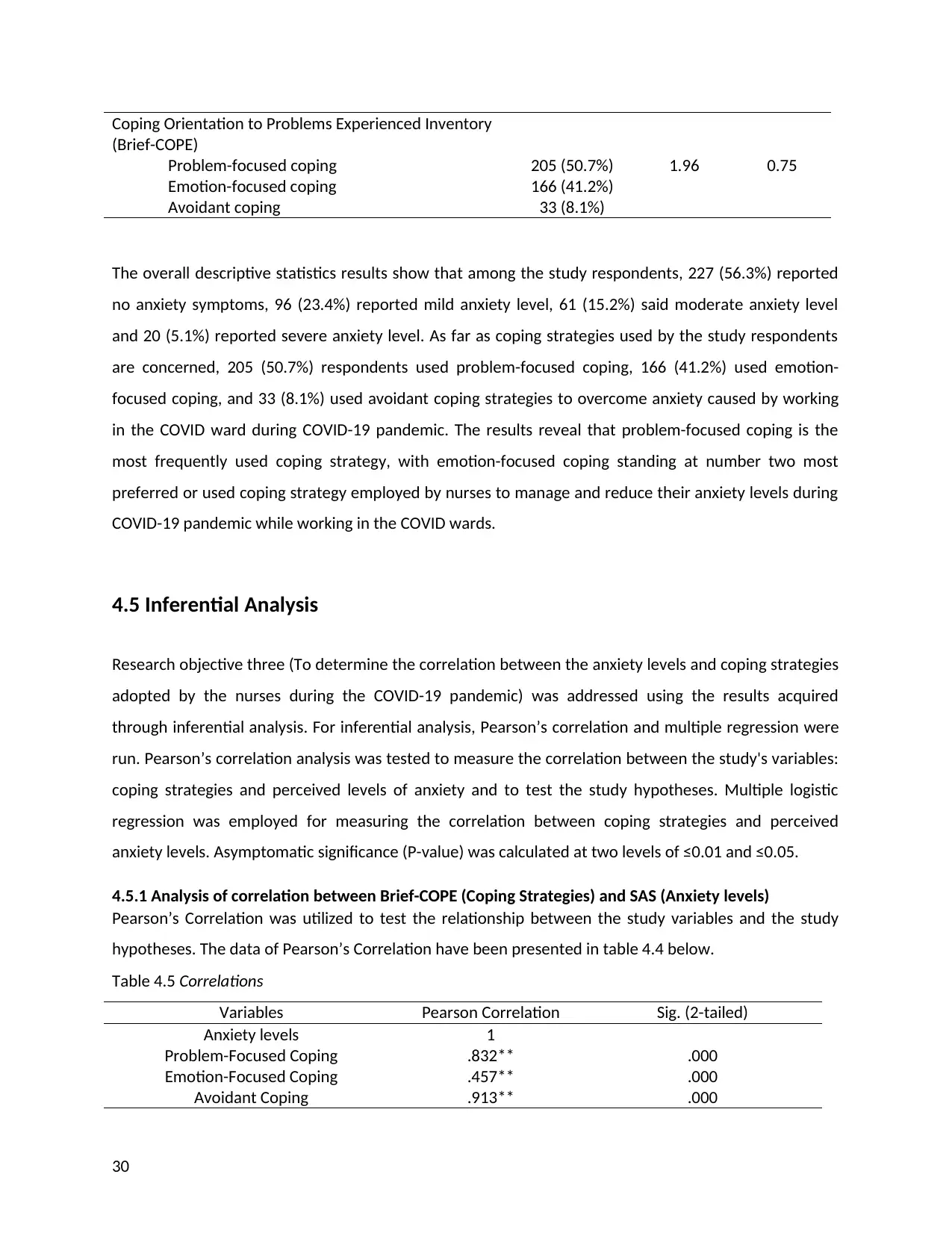
Coping Orientation to Problems Experienced Inventory
(Brief-COPE)
Problem-focused coping
Emotion-focused coping
Avoidant coping
205 (50.7%)
166 (41.2%)
33 (8.1%)
1.96 0.75
The overall descriptive statistics results show that among the study respondents, 227 (56.3%) reported
no anxiety symptoms, 96 (23.4%) reported mild anxiety level, 61 (15.2%) said moderate anxiety level
and 20 (5.1%) reported severe anxiety level. As far as coping strategies used by the study respondents
are concerned, 205 (50.7%) respondents used problem-focused coping, 166 (41.2%) used emotion-
focused coping, and 33 (8.1%) used avoidant coping strategies to overcome anxiety caused by working
in the COVID ward during COVID-19 pandemic. The results reveal that problem-focused coping is the
most frequently used coping strategy, with emotion-focused coping standing at number two most
preferred or used coping strategy employed by nurses to manage and reduce their anxiety levels during
COVID-19 pandemic while working in the COVID wards.
4.5 Inferential Analysis
Research objective three (To determine the correlation between the anxiety levels and coping strategies
adopted by the nurses during the COVID-19 pandemic) was addressed using the results acquired
through inferential analysis. For inferential analysis, Pearson’s correlation and multiple regression were
run. Pearson’s correlation analysis was tested to measure the correlation between the study's variables:
coping strategies and perceived levels of anxiety and to test the study hypotheses. Multiple logistic
regression was employed for measuring the correlation between coping strategies and perceived
anxiety levels. Asymptomatic significance (P-value) was calculated at two levels of ≤0.01 and ≤0.05.
4.5.1 Analysis of correlation between Brief-COPE (Coping Strategies) and SAS (Anxiety levels)
Pearson’s Correlation was utilized to test the relationship between the study variables and the study
hypotheses. The data of Pearson’s Correlation have been presented in table 4.4 below.
Table 4.5 Correlations
Variables Pearson Correlation Sig. (2-tailed)
Anxiety levels 1
Problem-Focused Coping .832** .000
Emotion-Focused Coping .457** .000
Avoidant Coping .913** .000
30
(Brief-COPE)
Problem-focused coping
Emotion-focused coping
Avoidant coping
205 (50.7%)
166 (41.2%)
33 (8.1%)
1.96 0.75
The overall descriptive statistics results show that among the study respondents, 227 (56.3%) reported
no anxiety symptoms, 96 (23.4%) reported mild anxiety level, 61 (15.2%) said moderate anxiety level
and 20 (5.1%) reported severe anxiety level. As far as coping strategies used by the study respondents
are concerned, 205 (50.7%) respondents used problem-focused coping, 166 (41.2%) used emotion-
focused coping, and 33 (8.1%) used avoidant coping strategies to overcome anxiety caused by working
in the COVID ward during COVID-19 pandemic. The results reveal that problem-focused coping is the
most frequently used coping strategy, with emotion-focused coping standing at number two most
preferred or used coping strategy employed by nurses to manage and reduce their anxiety levels during
COVID-19 pandemic while working in the COVID wards.
4.5 Inferential Analysis
Research objective three (To determine the correlation between the anxiety levels and coping strategies
adopted by the nurses during the COVID-19 pandemic) was addressed using the results acquired
through inferential analysis. For inferential analysis, Pearson’s correlation and multiple regression were
run. Pearson’s correlation analysis was tested to measure the correlation between the study's variables:
coping strategies and perceived levels of anxiety and to test the study hypotheses. Multiple logistic
regression was employed for measuring the correlation between coping strategies and perceived
anxiety levels. Asymptomatic significance (P-value) was calculated at two levels of ≤0.01 and ≤0.05.
4.5.1 Analysis of correlation between Brief-COPE (Coping Strategies) and SAS (Anxiety levels)
Pearson’s Correlation was utilized to test the relationship between the study variables and the study
hypotheses. The data of Pearson’s Correlation have been presented in table 4.4 below.
Table 4.5 Correlations
Variables Pearson Correlation Sig. (2-tailed)
Anxiety levels 1
Problem-Focused Coping .832** .000
Emotion-Focused Coping .457** .000
Avoidant Coping .913** .000
30
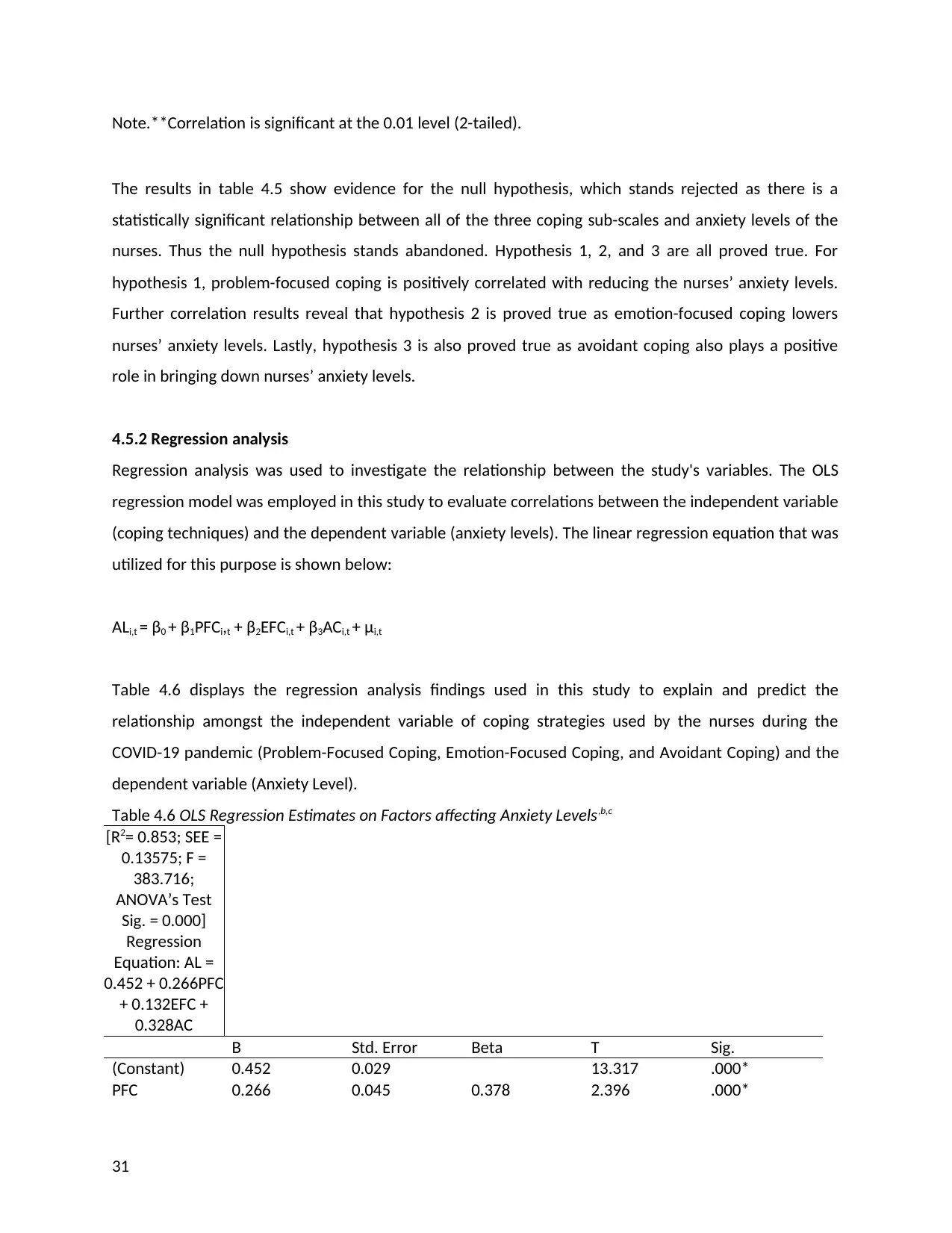
Note.**Correlation is significant at the 0.01 level (2-tailed).
The results in table 4.5 show evidence for the null hypothesis, which stands rejected as there is a
statistically significant relationship between all of the three coping sub-scales and anxiety levels of the
nurses. Thus the null hypothesis stands abandoned. Hypothesis 1, 2, and 3 are all proved true. For
hypothesis 1, problem-focused coping is positively correlated with reducing the nurses’ anxiety levels.
Further correlation results reveal that hypothesis 2 is proved true as emotion-focused coping lowers
nurses’ anxiety levels. Lastly, hypothesis 3 is also proved true as avoidant coping also plays a positive
role in bringing down nurses’ anxiety levels.
4.5.2 Regression analysis
Regression analysis was used to investigate the relationship between the study's variables. The OLS
regression model was employed in this study to evaluate correlations between the independent variable
(coping techniques) and the dependent variable (anxiety levels). The linear regression equation that was
utilized for this purpose is shown below:
ALi,t = β0 + β1PFCi,t + β2EFCi,t + β3ACi,t + μi,t
Table 4.6 displays the regression analysis findings used in this study to explain and predict the
relationship amongst the independent variable of coping strategies used by the nurses during the
COVID-19 pandemic (Problem-Focused Coping, Emotion-Focused Coping, and Avoidant Coping) and the
dependent variable (Anxiety Level).
Table 4.6 OLS Regression Estimates on Factors affecting Anxiety Levels,b,c
[R2= 0.853; SEE =
0.13575; F =
383.716;
ANOVA’s Test
Sig. = 0.000]
Regression
Equation: AL =
0.452 + 0.266PFC
+ 0.132EFC +
0.328AC
B Std. Error Beta T Sig.
(Constant) 0.452 0.029 13.317 .000*
PFC 0.266 0.045 0.378 2.396 .000*
31
The results in table 4.5 show evidence for the null hypothesis, which stands rejected as there is a
statistically significant relationship between all of the three coping sub-scales and anxiety levels of the
nurses. Thus the null hypothesis stands abandoned. Hypothesis 1, 2, and 3 are all proved true. For
hypothesis 1, problem-focused coping is positively correlated with reducing the nurses’ anxiety levels.
Further correlation results reveal that hypothesis 2 is proved true as emotion-focused coping lowers
nurses’ anxiety levels. Lastly, hypothesis 3 is also proved true as avoidant coping also plays a positive
role in bringing down nurses’ anxiety levels.
4.5.2 Regression analysis
Regression analysis was used to investigate the relationship between the study's variables. The OLS
regression model was employed in this study to evaluate correlations between the independent variable
(coping techniques) and the dependent variable (anxiety levels). The linear regression equation that was
utilized for this purpose is shown below:
ALi,t = β0 + β1PFCi,t + β2EFCi,t + β3ACi,t + μi,t
Table 4.6 displays the regression analysis findings used in this study to explain and predict the
relationship amongst the independent variable of coping strategies used by the nurses during the
COVID-19 pandemic (Problem-Focused Coping, Emotion-Focused Coping, and Avoidant Coping) and the
dependent variable (Anxiety Level).
Table 4.6 OLS Regression Estimates on Factors affecting Anxiety Levels,b,c
[R2= 0.853; SEE =
0.13575; F =
383.716;
ANOVA’s Test
Sig. = 0.000]
Regression
Equation: AL =
0.452 + 0.266PFC
+ 0.132EFC +
0.328AC
B Std. Error Beta T Sig.
(Constant) 0.452 0.029 13.317 .000*
PFC 0.266 0.045 0.378 2.396 .000*
31
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
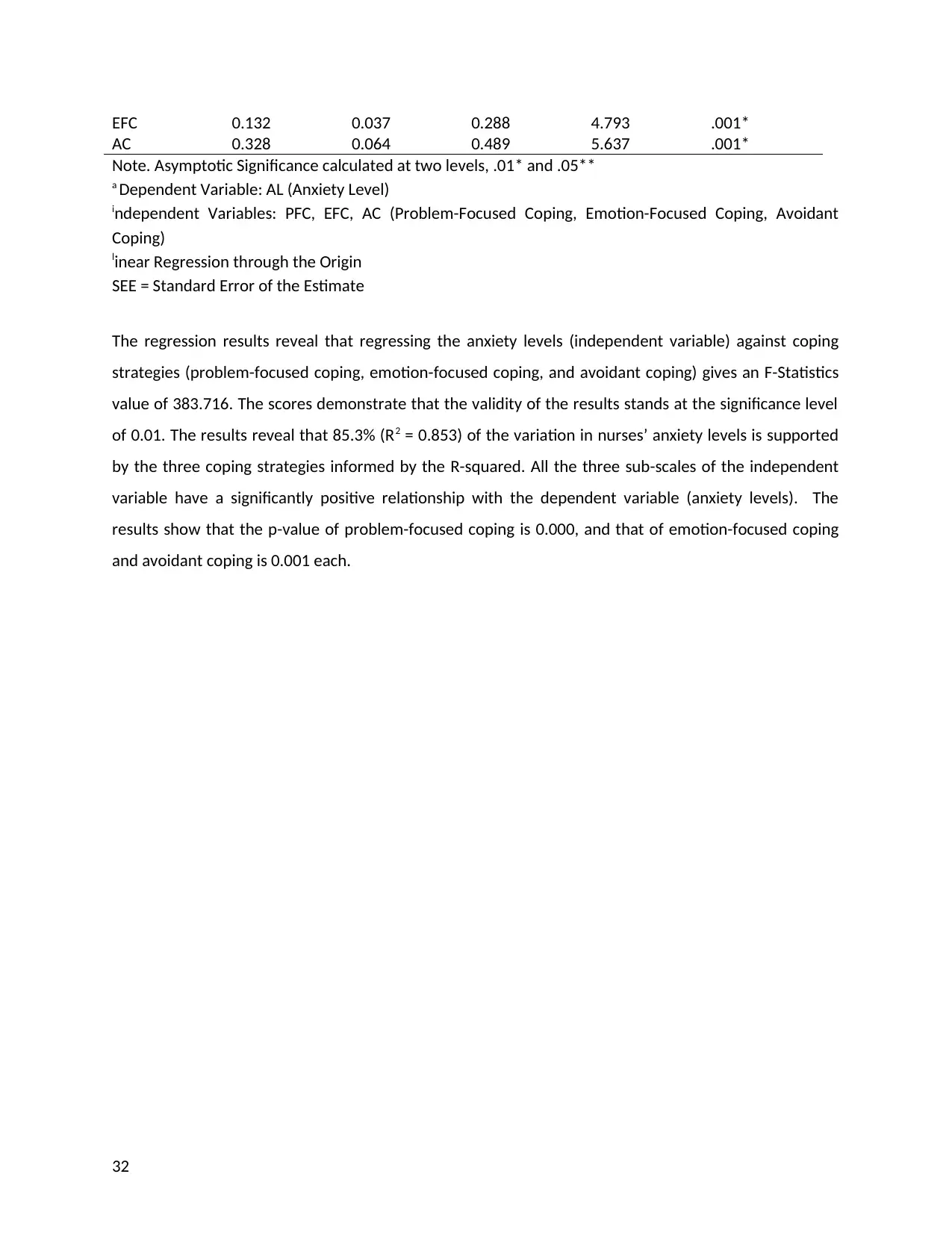
EFC 0.132 0.037 0.288 4.793 .001*
AC 0.328 0.064 0.489 5.637 .001*
Note. Asymptotic Significance calculated at two levels, .01* and .05**
a Dependent Variable: AL (Anxiety Level)
independent Variables: PFC, EFC, AC (Problem-Focused Coping, Emotion-Focused Coping, Avoidant
Coping)
linear Regression through the Origin
SEE = Standard Error of the Estimate
The regression results reveal that regressing the anxiety levels (independent variable) against coping
strategies (problem-focused coping, emotion-focused coping, and avoidant coping) gives an F-Statistics
value of 383.716. The scores demonstrate that the validity of the results stands at the significance level
of 0.01. The results reveal that 85.3% (R2 = 0.853) of the variation in nurses’ anxiety levels is supported
by the three coping strategies informed by the R-squared. All the three sub-scales of the independent
variable have a significantly positive relationship with the dependent variable (anxiety levels). The
results show that the p-value of problem-focused coping is 0.000, and that of emotion-focused coping
and avoidant coping is 0.001 each.
32
AC 0.328 0.064 0.489 5.637 .001*
Note. Asymptotic Significance calculated at two levels, .01* and .05**
a Dependent Variable: AL (Anxiety Level)
independent Variables: PFC, EFC, AC (Problem-Focused Coping, Emotion-Focused Coping, Avoidant
Coping)
linear Regression through the Origin
SEE = Standard Error of the Estimate
The regression results reveal that regressing the anxiety levels (independent variable) against coping
strategies (problem-focused coping, emotion-focused coping, and avoidant coping) gives an F-Statistics
value of 383.716. The scores demonstrate that the validity of the results stands at the significance level
of 0.01. The results reveal that 85.3% (R2 = 0.853) of the variation in nurses’ anxiety levels is supported
by the three coping strategies informed by the R-squared. All the three sub-scales of the independent
variable have a significantly positive relationship with the dependent variable (anxiety levels). The
results show that the p-value of problem-focused coping is 0.000, and that of emotion-focused coping
and avoidant coping is 0.001 each.
32
Chapter Five: Discussion
5.1 Introduction
The current study aimed to investigate the effects of coping strategies on nurses' anxiety levels during
the COVID-19 pandemic. The study attempted to test the following null hypothesis and three alternate
hypotheses:
H0 = There is no effect of coping strategies on anxiety levels of nurses during the COVID-19 pandemic
H1= The use of problem-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
H2= The emotion-focused coping has a positive correlation with the anxiety levels of nurses during the
COVID-19 pandemic
H3= The avoidant coping has a positive correlation with the anxiety levels of nurses during the COVID-19
pandemic
The study used a cross-sectional design. The data was collected from 404 nurses working in COVID
wards in 10 UK hospitals through a demographic questionnaire and two established scales of SAS and
Brief-COPE. The data were analysed through SPSS (v. 25) by running descriptive statistics, Pearson’s
correlation analysis and regression analysis to test the relationships between the study variables and
test the study hypotheses.
4.2 Discussion of Findings
The key finding of the study about the main aim reveals a positive effect of coping strategies used by the
nurses on their anxiety levels while they work in the COVID wards during the COVID-19 pandemic.
33
5.1 Introduction
The current study aimed to investigate the effects of coping strategies on nurses' anxiety levels during
the COVID-19 pandemic. The study attempted to test the following null hypothesis and three alternate
hypotheses:
H0 = There is no effect of coping strategies on anxiety levels of nurses during the COVID-19 pandemic
H1= The use of problem-focused coping has a positive correlation with the anxiety levels of nurses during
the COVID-19 pandemic
H2= The emotion-focused coping has a positive correlation with the anxiety levels of nurses during the
COVID-19 pandemic
H3= The avoidant coping has a positive correlation with the anxiety levels of nurses during the COVID-19
pandemic
The study used a cross-sectional design. The data was collected from 404 nurses working in COVID
wards in 10 UK hospitals through a demographic questionnaire and two established scales of SAS and
Brief-COPE. The data were analysed through SPSS (v. 25) by running descriptive statistics, Pearson’s
correlation analysis and regression analysis to test the relationships between the study variables and
test the study hypotheses.
4.2 Discussion of Findings
The key finding of the study about the main aim reveals a positive effect of coping strategies used by the
nurses on their anxiety levels while they work in the COVID wards during the COVID-19 pandemic.
33
Problem-focused coping proved to be the most used coping strategy by the study respondents for
overcoming their anxiety levels. When the controllability of the stressful event matches the choice of
the approach, the coping method is said to be adaptive, as suggested by Simione et al. (2020.) Coping, in
general, refers to the adaptive mechanisms used to alleviate stress. Coping is a sequence of cognitive
and behavioral efforts for managing specific internal or external difficulties that put individual resources
to the test or exceed personal resources.
Coping with COVID-19 required a layered response from organizations and individuals. From the
findings, it is evident that nurses prioritized taking care of themselves by adopting problem-focused and
emotion-focused coping strategies. This enabled them to identify challenges and adopt intervention
strategies to enhance the quality of care provision and well-being as healthcare providers and frontline
healthcare workers. Similar findings were also supported in Huang et al. (2020) published in an article.
Furthermore, these nurses collaborated with other healthcare providers, such as managers and other
professionals involved in delivering care. According to the study's conclusions, nurses still need to
prioritize their well-being in the face of pandemics like COVID-19. They must attend to their physical
demands and necessities, such as rest, sleep, and adequate breaks. Through a comprehensive coping
approach, hospitals need to implement appropriate measures to assist nurses in reducing their anxiety,
worries, stress, fear, despair, and panic. It can be done by using problem-focused and emotion-focused
coping strategies, which were found to assist nurses in the current study in focusing on their current
emotions and overall well-being during the COVID-19 pandemic.
The current study observations converged on what was known in the literature on nurses’ experiences
during a worldwide epidemic. As a result, it is crucial in shaping support strategies to maximize the
nursing staff in the hospitals during and after the latest COVID-19 pandemic. In recent decades, many
infectious disease outbreaks have occurred, including SARS in 2003, H1N1 in 2009, Ebola, Zika, and
MERS in 2014 and 2016 (Morens & Fauci, 2020). During these illness epidemics, nurses who cared for
infected patients faced significant physical, mental, and social difficulties (Zhang et al., 2020). A host of
studies on healthcare professionals and COVID-19 have revealed that nurses work in an exceedingly
stressful setting. COVID-19’s unknown nature and ambiguity have exacerbated the load and increased
stress among nurses tackling the outbreak, thus creating anxiety amongst them. According to the
present study findings, familiar individual coping strategies used by the nurse participants to cope with
COVID-19 burdens were collegial support, humor, optimism, a sense of being in a similar situation, a
sense of positivity amid the COVID-19 crisis, and a problem-solving stance. To deal with the current
34
overcoming their anxiety levels. When the controllability of the stressful event matches the choice of
the approach, the coping method is said to be adaptive, as suggested by Simione et al. (2020.) Coping, in
general, refers to the adaptive mechanisms used to alleviate stress. Coping is a sequence of cognitive
and behavioral efforts for managing specific internal or external difficulties that put individual resources
to the test or exceed personal resources.
Coping with COVID-19 required a layered response from organizations and individuals. From the
findings, it is evident that nurses prioritized taking care of themselves by adopting problem-focused and
emotion-focused coping strategies. This enabled them to identify challenges and adopt intervention
strategies to enhance the quality of care provision and well-being as healthcare providers and frontline
healthcare workers. Similar findings were also supported in Huang et al. (2020) published in an article.
Furthermore, these nurses collaborated with other healthcare providers, such as managers and other
professionals involved in delivering care. According to the study's conclusions, nurses still need to
prioritize their well-being in the face of pandemics like COVID-19. They must attend to their physical
demands and necessities, such as rest, sleep, and adequate breaks. Through a comprehensive coping
approach, hospitals need to implement appropriate measures to assist nurses in reducing their anxiety,
worries, stress, fear, despair, and panic. It can be done by using problem-focused and emotion-focused
coping strategies, which were found to assist nurses in the current study in focusing on their current
emotions and overall well-being during the COVID-19 pandemic.
The current study observations converged on what was known in the literature on nurses’ experiences
during a worldwide epidemic. As a result, it is crucial in shaping support strategies to maximize the
nursing staff in the hospitals during and after the latest COVID-19 pandemic. In recent decades, many
infectious disease outbreaks have occurred, including SARS in 2003, H1N1 in 2009, Ebola, Zika, and
MERS in 2014 and 2016 (Morens & Fauci, 2020). During these illness epidemics, nurses who cared for
infected patients faced significant physical, mental, and social difficulties (Zhang et al., 2020). A host of
studies on healthcare professionals and COVID-19 have revealed that nurses work in an exceedingly
stressful setting. COVID-19’s unknown nature and ambiguity have exacerbated the load and increased
stress among nurses tackling the outbreak, thus creating anxiety amongst them. According to the
present study findings, familiar individual coping strategies used by the nurse participants to cope with
COVID-19 burdens were collegial support, humor, optimism, a sense of being in a similar situation, a
sense of positivity amid the COVID-19 crisis, and a problem-solving stance. To deal with the current
34
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
situation, nurses are expected to get assistance from hospital administrators, enough material supplies,
government funding, clear instructions on care protocols, and adequate knowledge of COVID-19 illness.
Individual coping methods were actively used by the majority of the nurses in this study. However,
moral support methods such as managerial assistance, material support, and allowances are required to
support nurses’ emotional, physical, and social well-being. Other coping mechanisms that need to be
provided include the assistance of team leaders and an appropriate amount of supplies. Furthermore,
several nurses should also be given incentives, bonuses, hazard pay, and food supplies to acknowledging
their efforts during the pandemic.
Managerial assistance has been deemed crucial for the supply of resources required for improving
patient care effectiveness and lowering stress and burnout among nurses in the existing literature. Their
vital contributions in assisting nurses in dealing with the COVID-19 pandemic have resulted in resource
optimisation for improved treatment of COVID-19 patients on the ward. Other studies have reported
that the coping strategies nurses used to overcome COVID-19 stress included following “preventive
measures, actively learning about new diseases, learning professional knowledge, adjusting attitude and
facing the COVID-19 epidemic positively, and staying in touch with friends and families” (Zhang et al.,
2020, p. 1154) as also evidenced in this study. Watson (2021) suggests that team support may be
improved by valuing uniqueness, offering acknowledgment, and looking for chances to reframe
negativity and promote each other’s well-being. Nurses feel comfortable, appreciated, and welcomed
due to the team's assistance. Their actions during a crisis put them at grave risk, but they accepted the
load with a stronger feeling of duty and responsibility, as well as mutual trust among their colleagues.
Nurses play a crucial role in supporting team members' communication and teamwork. When the duties
of the individual nurses and team are established, mutual trust and a respectful atmosphere can be
formed, and effective communication may be maintained. Cheerful humor among coworkers helps to
build a sense of belonging. Compared to hostile humor, positive humor is full of hope, fun, and self-
improvement. Humor that is light and gentle reduces anxiety and enhances emotional and psychological
well-being. As a result, prior studies have seen cheerful humor as a more effective stress reliever among
these nurses. It provided a therapeutic benefit by allowing nurses to vent their frustrations, perhaps
reducing burnout. In this study, nurse participants used humor coping strategy as another unique coping
technique that provided a creative approach for dealing with stressful situations by helping them enjoy
the humorous aspects of their daily work even while they were going through a challenging moment.
The findings also revealed the nurse participants' optimism and resilience helped them cope with the
35
government funding, clear instructions on care protocols, and adequate knowledge of COVID-19 illness.
Individual coping methods were actively used by the majority of the nurses in this study. However,
moral support methods such as managerial assistance, material support, and allowances are required to
support nurses’ emotional, physical, and social well-being. Other coping mechanisms that need to be
provided include the assistance of team leaders and an appropriate amount of supplies. Furthermore,
several nurses should also be given incentives, bonuses, hazard pay, and food supplies to acknowledging
their efforts during the pandemic.
Managerial assistance has been deemed crucial for the supply of resources required for improving
patient care effectiveness and lowering stress and burnout among nurses in the existing literature. Their
vital contributions in assisting nurses in dealing with the COVID-19 pandemic have resulted in resource
optimisation for improved treatment of COVID-19 patients on the ward. Other studies have reported
that the coping strategies nurses used to overcome COVID-19 stress included following “preventive
measures, actively learning about new diseases, learning professional knowledge, adjusting attitude and
facing the COVID-19 epidemic positively, and staying in touch with friends and families” (Zhang et al.,
2020, p. 1154) as also evidenced in this study. Watson (2021) suggests that team support may be
improved by valuing uniqueness, offering acknowledgment, and looking for chances to reframe
negativity and promote each other’s well-being. Nurses feel comfortable, appreciated, and welcomed
due to the team's assistance. Their actions during a crisis put them at grave risk, but they accepted the
load with a stronger feeling of duty and responsibility, as well as mutual trust among their colleagues.
Nurses play a crucial role in supporting team members' communication and teamwork. When the duties
of the individual nurses and team are established, mutual trust and a respectful atmosphere can be
formed, and effective communication may be maintained. Cheerful humor among coworkers helps to
build a sense of belonging. Compared to hostile humor, positive humor is full of hope, fun, and self-
improvement. Humor that is light and gentle reduces anxiety and enhances emotional and psychological
well-being. As a result, prior studies have seen cheerful humor as a more effective stress reliever among
these nurses. It provided a therapeutic benefit by allowing nurses to vent their frustrations, perhaps
reducing burnout. In this study, nurse participants used humor coping strategy as another unique coping
technique that provided a creative approach for dealing with stressful situations by helping them enjoy
the humorous aspects of their daily work even while they were going through a challenging moment.
The findings also revealed the nurse participants' optimism and resilience helped them cope with the
35
anxiety and be resilient (LoGiudice & Bartos 2021). The notion of resilience in the workplace has shown
that it effectively safeguards individuals from job stress and anxiety.
The reaction happens at various life periods and depends on the circumstances (Cusack et al. 2016). To
cope with difficult situations, demonstrate resilience, there is a need to consider both positive
adaptation and adversity. This study focuses on nurses' intrinsic capacity to handle professional anxiety
and a process of positive coping and adaptation based on adversity. It suggests that adversity is the
primary cause of resilience, while beneficial adaptations are the main result. In terms of strength as a
quality, it symbolizes the attributes that allow individuals to adapt to various situations in their daily
lives. It is related to people's capacity to have good protective traits, including hardiness, positive
emotions, extraversion, self-esteem, self-efficacy, and positive affect, as evidenced by Fletcher & Sarkar
(2013).
The outcomes of this study revealed that nurses were participating and interacting in numerous
protective mechanisms at multiple levels, including support from management, coworkers, and practical
coping skills among people. They discovered problem-based, optimism, and emotion-based coping.
Amid a health crisis, a sense of oneness may promote resilience. Prior research also found resilience to
mediate between coping and subjective well-being (Ziarko et al., 2020; Lorente et al., 2021). Individual
coping techniques and self-care behaviors were utilized to explain pliability by the nurses in this study.
According to the European Centre for Disease Control and Prevention’s technical report (2021),
adequate resources and procedures should be in place to address: (1) infection prevention and control
measures (IPC), supplies of PPE, and training; (2) COVID-19 surveillance; (3) testing and monitoring of
COVID-19 for early outbreak detection and control; and (4) access to psychosocial care and visitor
restrictions in the health care facility. The present study's findings also indicated that the delivery of
safe, efficient, and high-quality health care was highly reliant on effective IPC widespread measures in
the hospitals. According to the statistics, IPC measures in the psychogeriatric ward comprised
administrative processes, physical distance, hand washing, and correct use of personal protective
equipment (PPE). Patient visits were restricted in the controls for the time being to minimize any COVID-
19 transmissions from patient family and visitors. They were only permitted when there was an urgent
crisis, and they were instructed to exercise physical distance, hand cleanliness, and wear facemasks if
physical distancing was not possible. As these nurses were given sufficient training and PPE, there was
good adherence to infection prevention measures in the unit.
36
that it effectively safeguards individuals from job stress and anxiety.
The reaction happens at various life periods and depends on the circumstances (Cusack et al. 2016). To
cope with difficult situations, demonstrate resilience, there is a need to consider both positive
adaptation and adversity. This study focuses on nurses' intrinsic capacity to handle professional anxiety
and a process of positive coping and adaptation based on adversity. It suggests that adversity is the
primary cause of resilience, while beneficial adaptations are the main result. In terms of strength as a
quality, it symbolizes the attributes that allow individuals to adapt to various situations in their daily
lives. It is related to people's capacity to have good protective traits, including hardiness, positive
emotions, extraversion, self-esteem, self-efficacy, and positive affect, as evidenced by Fletcher & Sarkar
(2013).
The outcomes of this study revealed that nurses were participating and interacting in numerous
protective mechanisms at multiple levels, including support from management, coworkers, and practical
coping skills among people. They discovered problem-based, optimism, and emotion-based coping.
Amid a health crisis, a sense of oneness may promote resilience. Prior research also found resilience to
mediate between coping and subjective well-being (Ziarko et al., 2020; Lorente et al., 2021). Individual
coping techniques and self-care behaviors were utilized to explain pliability by the nurses in this study.
According to the European Centre for Disease Control and Prevention’s technical report (2021),
adequate resources and procedures should be in place to address: (1) infection prevention and control
measures (IPC), supplies of PPE, and training; (2) COVID-19 surveillance; (3) testing and monitoring of
COVID-19 for early outbreak detection and control; and (4) access to psychosocial care and visitor
restrictions in the health care facility. The present study's findings also indicated that the delivery of
safe, efficient, and high-quality health care was highly reliant on effective IPC widespread measures in
the hospitals. According to the statistics, IPC measures in the psychogeriatric ward comprised
administrative processes, physical distance, hand washing, and correct use of personal protective
equipment (PPE). Patient visits were restricted in the controls for the time being to minimize any COVID-
19 transmissions from patient family and visitors. They were only permitted when there was an urgent
crisis, and they were instructed to exercise physical distance, hand cleanliness, and wear facemasks if
physical distancing was not possible. As these nurses were given sufficient training and PPE, there was
good adherence to infection prevention measures in the unit.
36
Further measures included making appropriate logistic supplies available in the ward. All these helped
the nurses have a problem-focused coping attitude towards the pandemic situation. During the
significant influence of COVID-19 on global perspectives, these administrative initiatives reduced
breakout rates by limiting illness transmission among coworkers inside the psychogeriatric unit. These
suggestions were also viewed as organizational methods to improve nurses' well-being and avoid
nosocomial infections, thus making them feel safe and reducing their anxiety.
The COVID-19 illness has been around for about two years and has had a significant influence on the
healthcare sector and other sectors of society. Nurses all across the world are carrying a tremendous
emotional weight. As the epidemic persists, nurses’ physical and emotional well-being is at an all-time
low. According to ICN (2021), the total number of documented COVID-19 fatalities among nurses in 59
countries is 2,266. Nurses are the most numerous workers in the healthcare industry worldwide (WHO
2020b). Nurses’ emotional anguish has frequently been shown as sadness and anxiety among frontline
healthcare professionals. Being in the vanguard of the fight against the pandemic has presented its own
set of obstacles for nursing personnel across diverse hospital settings. It puts them at a higher risk of
emotional anguish than other healthcare team members. Nurses have been subjected to worry, stress,
and anxiety due to the concern of getting COVID-19 and passing it to their families and other persons
deemed more sensitive to the diseases (Sethi et al., 2020). Exposure to the disease alters nurses’
behaviors and judgments depending on the disease’s linked vulnerabilities and consequences. Nurses’
emotional loads are also related to the treatment they receive from public members since they are
perceived to be at more risk than the general population. Some nurses experience social isolation and
stigma in society, while others avoid association with them.
The lack of an authorized treatment or vaccination for the disease for an extended period has also been
linked to depression, dread, and anxiety. The virus’s shifting and mutation expose more significant
concerns about treating it. Because of the uncertainty associated with the illnesses, nurses have
reported an upsurge in mental health concerns (Ornell et al., 2020). The increased workload compounds
the worry of getting the virus in healthcare settings and the necessity to cater to unfavorable nursing
demands while unsure of the best treatment method. Inadequate protection for nurses from catching
the illness has been linked to a lack of healthcare resources. It is prevalent, particularly in developing
nations where the healthcare system has been overburdened due to the increased patient population.
As a result, nurses have noted a lack of proper personal protective equipment, exposing them to
increased chances of getting the virus. It has hurt the nurses’ mental health and overall well-being.
37
the nurses have a problem-focused coping attitude towards the pandemic situation. During the
significant influence of COVID-19 on global perspectives, these administrative initiatives reduced
breakout rates by limiting illness transmission among coworkers inside the psychogeriatric unit. These
suggestions were also viewed as organizational methods to improve nurses' well-being and avoid
nosocomial infections, thus making them feel safe and reducing their anxiety.
The COVID-19 illness has been around for about two years and has had a significant influence on the
healthcare sector and other sectors of society. Nurses all across the world are carrying a tremendous
emotional weight. As the epidemic persists, nurses’ physical and emotional well-being is at an all-time
low. According to ICN (2021), the total number of documented COVID-19 fatalities among nurses in 59
countries is 2,266. Nurses are the most numerous workers in the healthcare industry worldwide (WHO
2020b). Nurses’ emotional anguish has frequently been shown as sadness and anxiety among frontline
healthcare professionals. Being in the vanguard of the fight against the pandemic has presented its own
set of obstacles for nursing personnel across diverse hospital settings. It puts them at a higher risk of
emotional anguish than other healthcare team members. Nurses have been subjected to worry, stress,
and anxiety due to the concern of getting COVID-19 and passing it to their families and other persons
deemed more sensitive to the diseases (Sethi et al., 2020). Exposure to the disease alters nurses’
behaviors and judgments depending on the disease’s linked vulnerabilities and consequences. Nurses’
emotional loads are also related to the treatment they receive from public members since they are
perceived to be at more risk than the general population. Some nurses experience social isolation and
stigma in society, while others avoid association with them.
The lack of an authorized treatment or vaccination for the disease for an extended period has also been
linked to depression, dread, and anxiety. The virus’s shifting and mutation expose more significant
concerns about treating it. Because of the uncertainty associated with the illnesses, nurses have
reported an upsurge in mental health concerns (Ornell et al., 2020). The increased workload compounds
the worry of getting the virus in healthcare settings and the necessity to cater to unfavorable nursing
demands while unsure of the best treatment method. Inadequate protection for nurses from catching
the illness has been linked to a lack of healthcare resources. It is prevalent, particularly in developing
nations where the healthcare system has been overburdened due to the increased patient population.
As a result, nurses have noted a lack of proper personal protective equipment, exposing them to
increased chances of getting the virus. It has hurt the nurses’ mental health and overall well-being.
37
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
The majority of the nurses experienced fear, and fear is one of the elements impacting nurses during a
crisis. It produces dread and terror, a significant factor in nurses’ mental health when dealing with
healthcare pandemics. According to Ho et al. (2020), anxiety and panic among nursing staff emerge due
to the threat to their personal life and concerns about how they are required to handle professionally as
a load of COVID-19 patients increases. Nurses are concerned about their own and their families well-
being while on the job. Nurses feel insecure at work and fearful of exposing their families after being
exposed to the highly contagious disease as they struggle to manage the epidemic and provide quality
treatment to all patients.
Furthermore, most participants indicated the worry of being ill and transferring disease to close and
loved ones like a professional stressor. However, most participants stated that the fear of infecting
others was still the most prevalent among them. The study also discovered that several nurse
participants working in the psychogeriatric department experienced significant emotional weariness and
burnout symptoms while caring for COVID-19 patients.
As a physical indication of burnout, the nurse participants experienced anxiety, weariness, decreased
satisfaction, and poor job performance. These findings are consistent with previous research (Khasne et
al., 2020). According to the results, the participants were scared and frightened by the severity of the
sickness. These nurses were shown to have a greater level of perceived threat. The nursing workforce
has been under severe strain since the start of the COVID-19 epidemic, as evidenced by the publications
of WHO (2020b). Millions of nurses worldwide have reported fear of uncertainty, helplessness, and the
prospect of illness severity, as well as worry of contracting the disease and infecting others. These
substantial sensations are crucial in the midst of a healthcare crisis and have played an essential role in
depleting the study’s nurse participants' emotional power to fulfill the demands made by the pandemic
catastrophe.
During the current COVID-19 epidemic, nurse participants watched coworkers become infected with the
disease, which was the most unpleasant event for nurses, instilling worry about their vulnerability. It has
put them under additional mental strain. These findings were consistent with prior results from the
2009 H1N1 epidemic (Morens et al., 2020). Lasalvia et al. (2021) describe emotional exhaustion as
related to an individual’s anxiety experiences linked to a reduction in mental and physical resources.
From this study, during the COVID-19 pandemic in the COVID ward, nurses had mixed negative emotions
of excitement, doubt, and helplessness. The heightened emotional burdens experienced by nurses of
38
crisis. It produces dread and terror, a significant factor in nurses’ mental health when dealing with
healthcare pandemics. According to Ho et al. (2020), anxiety and panic among nursing staff emerge due
to the threat to their personal life and concerns about how they are required to handle professionally as
a load of COVID-19 patients increases. Nurses are concerned about their own and their families well-
being while on the job. Nurses feel insecure at work and fearful of exposing their families after being
exposed to the highly contagious disease as they struggle to manage the epidemic and provide quality
treatment to all patients.
Furthermore, most participants indicated the worry of being ill and transferring disease to close and
loved ones like a professional stressor. However, most participants stated that the fear of infecting
others was still the most prevalent among them. The study also discovered that several nurse
participants working in the psychogeriatric department experienced significant emotional weariness and
burnout symptoms while caring for COVID-19 patients.
As a physical indication of burnout, the nurse participants experienced anxiety, weariness, decreased
satisfaction, and poor job performance. These findings are consistent with previous research (Khasne et
al., 2020). According to the results, the participants were scared and frightened by the severity of the
sickness. These nurses were shown to have a greater level of perceived threat. The nursing workforce
has been under severe strain since the start of the COVID-19 epidemic, as evidenced by the publications
of WHO (2020b). Millions of nurses worldwide have reported fear of uncertainty, helplessness, and the
prospect of illness severity, as well as worry of contracting the disease and infecting others. These
substantial sensations are crucial in the midst of a healthcare crisis and have played an essential role in
depleting the study’s nurse participants' emotional power to fulfill the demands made by the pandemic
catastrophe.
During the current COVID-19 epidemic, nurse participants watched coworkers become infected with the
disease, which was the most unpleasant event for nurses, instilling worry about their vulnerability. It has
put them under additional mental strain. These findings were consistent with prior results from the
2009 H1N1 epidemic (Morens et al., 2020). Lasalvia et al. (2021) describe emotional exhaustion as
related to an individual’s anxiety experiences linked to a reduction in mental and physical resources.
From this study, during the COVID-19 pandemic in the COVID ward, nurses had mixed negative emotions
of excitement, doubt, and helplessness. The heightened emotional burdens experienced by nurses of
38
the COVID ward had similar results in a cross-sectional study conducted in a tertiary hospital of a highly
burdened area of COVID-19 in northeast Italy by Lasalvia et al. (2021).
The findings from the present study have depicted the workplace and COVID-19 induced anxiety among
the nurse participants. The emotional exhaustion due to continuous exposure to long working hours,
health threats, poor crisis communication in the organization, and lack of knowledge of COVID-19
pandemic may have led to formation of negative emotions (Lapum et al., 2021). Other emotional
burdens included feelings of remorse and self-blame being COVID-19 situations for longer times without
control over it. On the other hand, nurses were afraid and guilty that they might infect their families and
loved ones. It could further lead to lower personal accomplishment and detachment from work due to
the lack of energy. The nurses also experienced low professional efficacy and lack of productivity due to
emotional distress; however, nurses reported a strong sense of responsibility that came along with the
nursing profession in the current study findings. Their emotional experiences reaffirmed their dedication
to the nursing job they do.
The findings from this study have highlighted the importance of supporting and enhancing nurse’s
emotional well-being during an event of health care crisis to help them avoid getting anxiety attacks.
Nurse participants in this study shared their feeling of fear, isolation, anger, frustrations as they
reflected on how their unrelenting thoughts of catching the virus and infecting others worried them. The
emotional toll of all these events left many nurses exhausted, but seeing their patients struggle in
isolation motivated nurses to stay and work in solidarity and care for patients with greater empathy and
compassion.
39
burdened area of COVID-19 in northeast Italy by Lasalvia et al. (2021).
The findings from the present study have depicted the workplace and COVID-19 induced anxiety among
the nurse participants. The emotional exhaustion due to continuous exposure to long working hours,
health threats, poor crisis communication in the organization, and lack of knowledge of COVID-19
pandemic may have led to formation of negative emotions (Lapum et al., 2021). Other emotional
burdens included feelings of remorse and self-blame being COVID-19 situations for longer times without
control over it. On the other hand, nurses were afraid and guilty that they might infect their families and
loved ones. It could further lead to lower personal accomplishment and detachment from work due to
the lack of energy. The nurses also experienced low professional efficacy and lack of productivity due to
emotional distress; however, nurses reported a strong sense of responsibility that came along with the
nursing profession in the current study findings. Their emotional experiences reaffirmed their dedication
to the nursing job they do.
The findings from this study have highlighted the importance of supporting and enhancing nurse’s
emotional well-being during an event of health care crisis to help them avoid getting anxiety attacks.
Nurse participants in this study shared their feeling of fear, isolation, anger, frustrations as they
reflected on how their unrelenting thoughts of catching the virus and infecting others worried them. The
emotional toll of all these events left many nurses exhausted, but seeing their patients struggle in
isolation motivated nurses to stay and work in solidarity and care for patients with greater empathy and
compassion.
39
Chapter Six: Implications
6.1 Introduction
The current study findings hold implications for theory and policy. This chapter offers an insight into
these implications and comprises sections on impact and recommendations for policy and practice
presented in the light of the current study findings.
6.2 Implications
The study findings held implications for theory and nurse management, presented in the following
sections.
6.2.1 Implications for theory
The current study findings contribute significantly to the existing theoretical knowledge on the role and
effect of coping strategies on nurses’ anxiety levels during the COVID-19 pandemic. It is the first study
conducted to test the correlation between the coping strategies of problem-focused coping, emotion-
focused coping, avoidant coping, and nurses’ anxiety levels. The results also show the interrelationship
between the variables considered in the present study. The current findings demonstrated that
problem-focused coping strategies are the ones used by the majority of the nurses, with emotion-
focused coping strategies preferred on the second number. It was also found that these coping
strategies help nurses avoid and overcome anxiety, as the majority of the nurses in this study either did
not suffer from anxiety or had lower stress levels. This finding proves the positive effect of coping
strategies on nurses' anxiety levels during the COVID-19 pandemic.
The current study's findings have significant theoretical implications and prepare the ground for further
investigation into the practical aspects of coping strategies and their role in managing anxiety and
keeping the nurses’ psychological health sound. The findings can aid in the development of solutions to
40
6.1 Introduction
The current study findings hold implications for theory and policy. This chapter offers an insight into
these implications and comprises sections on impact and recommendations for policy and practice
presented in the light of the current study findings.
6.2 Implications
The study findings held implications for theory and nurse management, presented in the following
sections.
6.2.1 Implications for theory
The current study findings contribute significantly to the existing theoretical knowledge on the role and
effect of coping strategies on nurses’ anxiety levels during the COVID-19 pandemic. It is the first study
conducted to test the correlation between the coping strategies of problem-focused coping, emotion-
focused coping, avoidant coping, and nurses’ anxiety levels. The results also show the interrelationship
between the variables considered in the present study. The current findings demonstrated that
problem-focused coping strategies are the ones used by the majority of the nurses, with emotion-
focused coping strategies preferred on the second number. It was also found that these coping
strategies help nurses avoid and overcome anxiety, as the majority of the nurses in this study either did
not suffer from anxiety or had lower stress levels. This finding proves the positive effect of coping
strategies on nurses' anxiety levels during the COVID-19 pandemic.
The current study's findings have significant theoretical implications and prepare the ground for further
investigation into the practical aspects of coping strategies and their role in managing anxiety and
keeping the nurses’ psychological health sound. The findings can aid in the development of solutions to
40
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
assist people in general and nurses in particular who are suffering from the concerns above, which are
hurting their psychological well-being and overall attitude toward life, work, and day-to-day matters.
6.2.1 Implications for nursing management
Because excessive COVID-19 anxiety can negatively impact nurses’ well-being and mental health,
healthcare administrators should prioritize providing necessary emotional and psychological support
and implementing evidence-based methods to enhance nurses' mental health during the COVID-19
pandemic. It can be achieved by providing nurses with access to psychological or psychotherapy
treatment and tools and resources to promote their mental health. Furthermore, anxiety is frequently
created by a shortage of precise knowledge about the condition, which may be alleviated by bestowing
nurses with current and up-to-date information about the disease. Further assistance can be granted by
promoting self-care among nurses, for example, by providing “shorter or flexible duty hours, enough
breaks, and time scheduling.” These arrangements can help lessen the negative effect of the pandemic
and minimize anxiety amongst nurses.
Hospitals can improve stability among nursing staff by promoting suitable coping methods and
bolstering nurses’ self-efficacy. There is a need to prioritize personal building resilience among frontline
nurses since it was related to decreased COVID-19 anxiety. Previous research has evidenced that work-
based educational interventions can help nurses develop and maintain emotional stability, which is
important when dealing with stressful work events and adversity at the workplace, such as pandemics or
disease outbreaks. Social support, such as that provided by families, friends, and colleagues, may help
nurses feel more secure and lessen their worries during a pandemic.
Nurses’ psychological well-being and mental health will be promoted, and their morale will be boosted
by sharing work experiences, listening to their problems, and providing them empathic support.
Organizational support, such as providing a safe work environment and complete and quality PPE and
supplies for preventing infection, providing timely and correct disease information, and implementing
relevant COVID-19 training, is critical to supporting nurses in their nursing practices and protecting both
their mental and physical health.
6.3 Recommendations
41
hurting their psychological well-being and overall attitude toward life, work, and day-to-day matters.
6.2.1 Implications for nursing management
Because excessive COVID-19 anxiety can negatively impact nurses’ well-being and mental health,
healthcare administrators should prioritize providing necessary emotional and psychological support
and implementing evidence-based methods to enhance nurses' mental health during the COVID-19
pandemic. It can be achieved by providing nurses with access to psychological or psychotherapy
treatment and tools and resources to promote their mental health. Furthermore, anxiety is frequently
created by a shortage of precise knowledge about the condition, which may be alleviated by bestowing
nurses with current and up-to-date information about the disease. Further assistance can be granted by
promoting self-care among nurses, for example, by providing “shorter or flexible duty hours, enough
breaks, and time scheduling.” These arrangements can help lessen the negative effect of the pandemic
and minimize anxiety amongst nurses.
Hospitals can improve stability among nursing staff by promoting suitable coping methods and
bolstering nurses’ self-efficacy. There is a need to prioritize personal building resilience among frontline
nurses since it was related to decreased COVID-19 anxiety. Previous research has evidenced that work-
based educational interventions can help nurses develop and maintain emotional stability, which is
important when dealing with stressful work events and adversity at the workplace, such as pandemics or
disease outbreaks. Social support, such as that provided by families, friends, and colleagues, may help
nurses feel more secure and lessen their worries during a pandemic.
Nurses’ psychological well-being and mental health will be promoted, and their morale will be boosted
by sharing work experiences, listening to their problems, and providing them empathic support.
Organizational support, such as providing a safe work environment and complete and quality PPE and
supplies for preventing infection, providing timely and correct disease information, and implementing
relevant COVID-19 training, is critical to supporting nurses in their nursing practices and protecting both
their mental and physical health.
6.3 Recommendations
41
There is a need to carry out more research on nurses' coping techniques during the COVID-19 pandemic.
These investigations should use a variety of approaches, including quantitative, qualitative, and mixed
methods. It is also necessary to investigate the effects of various coping mechanisms on anxiety levels or
other outcomes. During COVID-19, nurses in hospitals and clinics should be taught appropriate stress,
anxiety, and burnout coping mechanisms. Government, hospital, and clinic administration should assist
nurses in dealing with anxiety during COVID-19.
During a pandemic, nurses' professional dedication can be increased by taking proper actions to limit
their infection risk. Nurses caring for COVID-19 patients should emphasize their workload, performance,
and frustration to stimulate their job dedication. The following are some more recommendations
regarding nurse managers and hospital administration: nurse managers in the ward should be evident
and approachable, transparent and regular communication with the staff is essential to acknowledge
them, nurse managers and leaders are expected to be honest and approachable, staff well-being should
be a priority, mandating and monitoring work breaks, encouraging opportunities for the staff to support
each other, and employee incentives, bonuses, and hazard allowances be provided.
The study's overarching recommendation is for organizational leaders and hospital management to give
tools to nurses ahead of time to boost their mental and emotional well-being. The organization should
use the lessons learned throughout the crisis, taking into account nurses' occupational safety, physical,
social, and emotional well-being. Managers should appreciate nurses’ dedication and dedicate more
attention to infection prevention and physical pain induced by PPE in order to improve nurses’
professional safety. Managers should be truthful in communicating the facts, creating coping methods,
and raising awareness of possible mental health concerns. Nonetheless, they should actively check if
their employees' critical safety needs are being met and all deficiencies, such as PPE, staff illness, testing,
and other issues of concern to employees, are being addressed. They should also develop long-term
healing programs for their employees. Furthermore, hospital administrations and organizations should
provide comprehensive assistance to reduce the costs associated with COVID-19 and increase the well-
being of nurses working in COVID-19 environments. Finally, a thorough grasp of COVID-19 might boost
nurses’ morale by ensuring proper crisis response assistance.
42
These investigations should use a variety of approaches, including quantitative, qualitative, and mixed
methods. It is also necessary to investigate the effects of various coping mechanisms on anxiety levels or
other outcomes. During COVID-19, nurses in hospitals and clinics should be taught appropriate stress,
anxiety, and burnout coping mechanisms. Government, hospital, and clinic administration should assist
nurses in dealing with anxiety during COVID-19.
During a pandemic, nurses' professional dedication can be increased by taking proper actions to limit
their infection risk. Nurses caring for COVID-19 patients should emphasize their workload, performance,
and frustration to stimulate their job dedication. The following are some more recommendations
regarding nurse managers and hospital administration: nurse managers in the ward should be evident
and approachable, transparent and regular communication with the staff is essential to acknowledge
them, nurse managers and leaders are expected to be honest and approachable, staff well-being should
be a priority, mandating and monitoring work breaks, encouraging opportunities for the staff to support
each other, and employee incentives, bonuses, and hazard allowances be provided.
The study's overarching recommendation is for organizational leaders and hospital management to give
tools to nurses ahead of time to boost their mental and emotional well-being. The organization should
use the lessons learned throughout the crisis, taking into account nurses' occupational safety, physical,
social, and emotional well-being. Managers should appreciate nurses’ dedication and dedicate more
attention to infection prevention and physical pain induced by PPE in order to improve nurses’
professional safety. Managers should be truthful in communicating the facts, creating coping methods,
and raising awareness of possible mental health concerns. Nonetheless, they should actively check if
their employees' critical safety needs are being met and all deficiencies, such as PPE, staff illness, testing,
and other issues of concern to employees, are being addressed. They should also develop long-term
healing programs for their employees. Furthermore, hospital administrations and organizations should
provide comprehensive assistance to reduce the costs associated with COVID-19 and increase the well-
being of nurses working in COVID-19 environments. Finally, a thorough grasp of COVID-19 might boost
nurses’ morale by ensuring proper crisis response assistance.
42
Chapter Seven: Conclusion
7.1 Introduction
This chapter concludes this study and consists of the research summary, limitations of the research, and
recommendations for future research.
7.2 Summary of Research
43
7.1 Introduction
This chapter concludes this study and consists of the research summary, limitations of the research, and
recommendations for future research.
7.2 Summary of Research
43
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
This study aimed to investigate the effects of coping strategies on nurses' anxiety levels during the
COVID-19 pandemic. Three sub-categories of coping strategies of problem-focused coping, emotion-
focused coping, and avoidant coping were tested for correlation with anxiety levels. The study used a
cross-sectional design. The data was collected through three questionnaires: Demographic survey, SAS,
and Brief-COPE, in which participants were 404 nurses working in the COVID wards in 10 hospitals in the
UK. The questionnaires were dispensed online, and the data were analysed with the help of SPSS (v. 25).
Descriptive statistics, Pearson’s correlation, and regression analysis were computed for data analysis,
test the correlations between the study variables, and test the hypotheses. The null hypothesis was
rejected in light of the study findings, and all of the three alternate theories proved true. The results
revealed that the coping strategies used by the nurses had a significant effect on their anxiety levels.
Moreover, all three coping strategies of problem-focused, emotion-focused, and avoidant coping
affected and helped lower the nurses' anxiety levels.
Furthermore, problem-focused coping was the most frequently used set of coping strategies by the
nurses in the current study, and emotion-focused managing was the second most commonly used set of
coping strategies. It was also found that although the majority of the nurses in this study did not suffer
from anxiety, this can be attributed to the use of problem-focused and emotion-focused coping
strategies. It was also found that a large proportion of nurses had lower levels of anxiety, and some of
the nurses had mild, medium, and higher levels of stress.
In light of the present study findings, it is concluded that COVID-19’s development and dissemination
have had an impact on the nurses' psychological, emotional and physical health and well-being. The
results have implications for nurses' emotional, physical, and social well-being. The worsening health of
nurses and organizational obstacles in pandemic management were identified as significant components
in the pandemic’s successful handling. During the COVID-19 healthcare crisis, it is critical to appreciate
the importance of nurses and their key responsibilities in supporting patients’ well-being because they
are constantly on the frontlines during this and other crises. The organization should provide genuine
assistance to enable them to develop tenacity and strong resilience in the nursing staff, particularly
during times of crisis like COVID-19.
To avoid nurse shortfall in the future, the healthcare industry should establish methods to meet their
social and physical requirements, alleviate mental health concerns and behavior, and evaluate potential
treatments for holistic well-being during and after a crisis. The short- and long-term impacts of
pandemics such as COVID-19 should be explored in the future through prospective research. Under all
44
COVID-19 pandemic. Three sub-categories of coping strategies of problem-focused coping, emotion-
focused coping, and avoidant coping were tested for correlation with anxiety levels. The study used a
cross-sectional design. The data was collected through three questionnaires: Demographic survey, SAS,
and Brief-COPE, in which participants were 404 nurses working in the COVID wards in 10 hospitals in the
UK. The questionnaires were dispensed online, and the data were analysed with the help of SPSS (v. 25).
Descriptive statistics, Pearson’s correlation, and regression analysis were computed for data analysis,
test the correlations between the study variables, and test the hypotheses. The null hypothesis was
rejected in light of the study findings, and all of the three alternate theories proved true. The results
revealed that the coping strategies used by the nurses had a significant effect on their anxiety levels.
Moreover, all three coping strategies of problem-focused, emotion-focused, and avoidant coping
affected and helped lower the nurses' anxiety levels.
Furthermore, problem-focused coping was the most frequently used set of coping strategies by the
nurses in the current study, and emotion-focused managing was the second most commonly used set of
coping strategies. It was also found that although the majority of the nurses in this study did not suffer
from anxiety, this can be attributed to the use of problem-focused and emotion-focused coping
strategies. It was also found that a large proportion of nurses had lower levels of anxiety, and some of
the nurses had mild, medium, and higher levels of stress.
In light of the present study findings, it is concluded that COVID-19’s development and dissemination
have had an impact on the nurses' psychological, emotional and physical health and well-being. The
results have implications for nurses' emotional, physical, and social well-being. The worsening health of
nurses and organizational obstacles in pandemic management were identified as significant components
in the pandemic’s successful handling. During the COVID-19 healthcare crisis, it is critical to appreciate
the importance of nurses and their key responsibilities in supporting patients’ well-being because they
are constantly on the frontlines during this and other crises. The organization should provide genuine
assistance to enable them to develop tenacity and strong resilience in the nursing staff, particularly
during times of crisis like COVID-19.
To avoid nurse shortfall in the future, the healthcare industry should establish methods to meet their
social and physical requirements, alleviate mental health concerns and behavior, and evaluate potential
treatments for holistic well-being during and after a crisis. The short- and long-term impacts of
pandemics such as COVID-19 should be explored in the future through prospective research. Under all
44
conditions, nurses’ mental health is a crucial component of occupational safety and health. It is even
more critical to provide more excellent assistance for nurses dealing with anxiety during a pandemic like
the current COVID-19 issue. The study's findings illuminate the mental health and coping mechanisms of
nurses in the UK who are actively involved in taking care of patients with suspected or confirmed COVID-
19. It would be highly beneficial in teaching nursing administrators how to provide mental health
services for nurses both during and after the worldwide COVID-19 epidemic.
Since the present study was the first study on the research problem, it is essential to examine the aspect
of anxiety and coping strategies in future studies aimed at healthcare provider populations. There is a
need to introduce intervention plans in hospitals for healthcare providers who require them. There is
also the need to create programs for healthcare staff's preventative and psychological treatment.
7.3 Limitations and Future Research Suggestions
This study has certain limitations that should be addressed in future research and considered when
interpreting the findings. First, because this study used a cross-sectional design, the researcher couldn't
identify causal links between the studied variables. Secondly, the present study used a convenience
sample, which may have reduced the generalisability of the results. Some parameters (such as gender
and occupation) may have been oversampled and so are not representative of the UK healthcare
professionals population. As a result, several features of the respondents (for example, profession type)
may have an impact on the results produced. In reality, data collected via an online survey did not allow
for the assessment of preexisting mental problems. There is a need to carry out longitudinal studies like
these that can help shed further light on the long-term effects of coping strategies on nurses’ anxiety
levels and other components on the development of depression, anxiety, and stress among healthcare
workers exposed to the COVID-19 epidemic.
Nonetheless, during the COVID-19 shutdown and social distancing restrictions, the researcher had to
collect data through an online survey only and could not conduct face-to-face interviews, which
constrained the chances of getting an in-depth understanding of the phenomenon under study. The
third limitation was the use of self-report anxiety and coping strategies measures. Although the SAS and
Brief-COPE are trustworthy and extensively used tests, social desirability may influence findings. These
scales are scenario-based indices that do not need responders to know their abilities fully. It should be
45
more critical to provide more excellent assistance for nurses dealing with anxiety during a pandemic like
the current COVID-19 issue. The study's findings illuminate the mental health and coping mechanisms of
nurses in the UK who are actively involved in taking care of patients with suspected or confirmed COVID-
19. It would be highly beneficial in teaching nursing administrators how to provide mental health
services for nurses both during and after the worldwide COVID-19 epidemic.
Since the present study was the first study on the research problem, it is essential to examine the aspect
of anxiety and coping strategies in future studies aimed at healthcare provider populations. There is a
need to introduce intervention plans in hospitals for healthcare providers who require them. There is
also the need to create programs for healthcare staff's preventative and psychological treatment.
7.3 Limitations and Future Research Suggestions
This study has certain limitations that should be addressed in future research and considered when
interpreting the findings. First, because this study used a cross-sectional design, the researcher couldn't
identify causal links between the studied variables. Secondly, the present study used a convenience
sample, which may have reduced the generalisability of the results. Some parameters (such as gender
and occupation) may have been oversampled and so are not representative of the UK healthcare
professionals population. As a result, several features of the respondents (for example, profession type)
may have an impact on the results produced. In reality, data collected via an online survey did not allow
for the assessment of preexisting mental problems. There is a need to carry out longitudinal studies like
these that can help shed further light on the long-term effects of coping strategies on nurses’ anxiety
levels and other components on the development of depression, anxiety, and stress among healthcare
workers exposed to the COVID-19 epidemic.
Nonetheless, during the COVID-19 shutdown and social distancing restrictions, the researcher had to
collect data through an online survey only and could not conduct face-to-face interviews, which
constrained the chances of getting an in-depth understanding of the phenomenon under study. The
third limitation was the use of self-report anxiety and coping strategies measures. Although the SAS and
Brief-COPE are trustworthy and extensively used tests, social desirability may influence findings. These
scales are scenario-based indices that do not need responders to know their abilities fully. It should be
45
highlighted that the use of self-report measures and data collection via an online survey provided the
researcher with information on anxiety levels and coping strategies as stated by research participants.
However, it is not viable to specify psychiatric diagnoses that need additional sources of evidence, such
as clinical judgment, in any circumstance. Future studies need to consider all these and use other data
collection methods to get a more holistic picture of the effect of coping strategies on nurses’ anxiety
levels in other crises and the COVID-19 pandemic.
References
Ali, H., Astin Cole, A.A., & Sa’d Hamasha, G.P. (2020). Major stressors and coping strategies of frontline
nursing staff during the outbreak of coronavirus disease 2020 (COVID-19) in Alabama. Journal of
Multidisciplinary Healthcare 13, 2057. https://doi.org/10.2147/JMDH.S285933
Alwani, S. S., Majeed, M. M., Ramzan, Z., Rauf, S., Syed, M. S., Shah, S. H., ... & Hamirani, F. (2020).
Evaluation of Knowledge, Practices, Attitude, and Anxiety of Nurses towards COVID-19 during
the Current Outbreak in Karachi, Pakistan. Pakistan Journal of Public Health, 10(2), 82-90.
https://doi.org/10.1101/2020.06.05.20123703
American Academy of Nursing (2018). 2018 Policy News. Retrieved from
https://www.aannet.org/news/policy-news/policy-advocacy-2018-news
Atmaca, Ç.T. (2016). Anxiety Levels of Nurses and Doctors Working in the Emergency Room before and
after Seizure [Master thesis]. Samsun, Turkey: Ondokuz Mayıs University Institute of Health
Sciences.
Babore, A., Lombardi, L., Viceconti, M. L., Pignataro, S., Marino, V., Crudele, M., ... & Trumello, C. (2020).
Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies
among healthcare professionals. Psychiatry Research, 293, 113366.
https://doi.org/10.1016/j.psychres.2020.113366
Burgdorf, K. S., Trabjerg, B. B., Pedersen, M. G., Nissen, J., Banasik, K., Pedersen, O. B., ... & Ullum, H.
(2019). Large-scale study of Toxoplasma and Cytomegalovirus shows an association between
infection and serious psychiatric disorders. Brain, behavior, and immunity, 79, 152-158.
https://doi.org/10.1016/j.bbi.2019.01.026
46
researcher with information on anxiety levels and coping strategies as stated by research participants.
However, it is not viable to specify psychiatric diagnoses that need additional sources of evidence, such
as clinical judgment, in any circumstance. Future studies need to consider all these and use other data
collection methods to get a more holistic picture of the effect of coping strategies on nurses’ anxiety
levels in other crises and the COVID-19 pandemic.
References
Ali, H., Astin Cole, A.A., & Sa’d Hamasha, G.P. (2020). Major stressors and coping strategies of frontline
nursing staff during the outbreak of coronavirus disease 2020 (COVID-19) in Alabama. Journal of
Multidisciplinary Healthcare 13, 2057. https://doi.org/10.2147/JMDH.S285933
Alwani, S. S., Majeed, M. M., Ramzan, Z., Rauf, S., Syed, M. S., Shah, S. H., ... & Hamirani, F. (2020).
Evaluation of Knowledge, Practices, Attitude, and Anxiety of Nurses towards COVID-19 during
the Current Outbreak in Karachi, Pakistan. Pakistan Journal of Public Health, 10(2), 82-90.
https://doi.org/10.1101/2020.06.05.20123703
American Academy of Nursing (2018). 2018 Policy News. Retrieved from
https://www.aannet.org/news/policy-news/policy-advocacy-2018-news
Atmaca, Ç.T. (2016). Anxiety Levels of Nurses and Doctors Working in the Emergency Room before and
after Seizure [Master thesis]. Samsun, Turkey: Ondokuz Mayıs University Institute of Health
Sciences.
Babore, A., Lombardi, L., Viceconti, M. L., Pignataro, S., Marino, V., Crudele, M., ... & Trumello, C. (2020).
Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies
among healthcare professionals. Psychiatry Research, 293, 113366.
https://doi.org/10.1016/j.psychres.2020.113366
Burgdorf, K. S., Trabjerg, B. B., Pedersen, M. G., Nissen, J., Banasik, K., Pedersen, O. B., ... & Ullum, H.
(2019). Large-scale study of Toxoplasma and Cytomegalovirus shows an association between
infection and serious psychiatric disorders. Brain, behavior, and immunity, 79, 152-158.
https://doi.org/10.1016/j.bbi.2019.01.026
46
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Cabarkapa, S., Nadjidai, S. E., Murgier, J., & Ng, C. H. (2020). The psychological impact of COVID-19 and
other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic
review. Brain, behavior, & immunity-health, 100144.
Cai, H., Tu, B., Ma, J., Chen, L., Fu, L., Jiang, Y., & Zhuang, Q. (2020). Psychological impact and coping
strategies of frontline medical staff in Hunan between January and March 2020 during the
outbreak of coronavirus disease 2019 (COVID-19) in Hubei, China. Medical Science Monitor.
International Medical Journal of Experimental and Clinical Research, 26, e924171-1.
Catton, H. (2020). Global challenges in health and health care for nurses and midwives everywhere.
International Nursing Review, 67(1), 4-6.
Choi, K.R., Jeffers, K.S., & Logsdon, M.C. (2020). Nursing and the novel coronavirus: risks and
responsibilities in a global outbreak. J Adv Nurs., 76, 1486 1487.‐
https://doi.org/10.1111/jan.14369
Cohen, L., Manion, L., & Morrison, K. (2002). Research methods in education. Routledge.
Cole, C. L., Waterman, S., Stott, J., Saunders, R., Buckman, J. E. J., Pilling, S., & Wheatley, J. (2020).
Adapting IAPT services to support frontline NHS staff during the Covid-19 pandemic: the
Homerton Covid Psychological Support (HCPS) pathway. The Cognitive Behaviour Therapist, 13.
https://doi.org/10.1017/S1754470X20000148
Cooper, A. L., Brown, J. A., Rees, C. S., & Leslie, G. D. (2020). Nurse resilience: A concept
analysis. International journal of mental health nursing, 29(4), 553-575.
Crooks, R. L., & Stein, J. (1988). Psychology: Science, behavior and life. Holt, Rinehart & Winston Inc.
Csikszentmihalyi, M., & Seligman, M. (2000). Positive psychology. American Psychologist, 55(1), 5-14.
Cui, S., Jiang, Y., Shi, Q., Zhang, L., Kong, D., Qian, M., & Chu, J. (2021). Impact of COVID-19 on anxiety,
stress, and coping styles in nurses in emergency departments and fever Clinics: A cross-sectional
survey. Risk management and healthcare policy, 14, 585.
https://doi.org/10.2147/RMHP.S289782
Cusack, K., Jonas, D. E., Forneris, C. A., Wines, C., Sonis, J., Middleton, J. C., ... & Gaynes, B. N. (2016).
Psychological treatments for adults with posttraumatic stress disorder: A systematic review and
meta-analysis. Clinical psychology review, 43, 128-141.
47
other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic
review. Brain, behavior, & immunity-health, 100144.
Cai, H., Tu, B., Ma, J., Chen, L., Fu, L., Jiang, Y., & Zhuang, Q. (2020). Psychological impact and coping
strategies of frontline medical staff in Hunan between January and March 2020 during the
outbreak of coronavirus disease 2019 (COVID-19) in Hubei, China. Medical Science Monitor.
International Medical Journal of Experimental and Clinical Research, 26, e924171-1.
Catton, H. (2020). Global challenges in health and health care for nurses and midwives everywhere.
International Nursing Review, 67(1), 4-6.
Choi, K.R., Jeffers, K.S., & Logsdon, M.C. (2020). Nursing and the novel coronavirus: risks and
responsibilities in a global outbreak. J Adv Nurs., 76, 1486 1487.‐
https://doi.org/10.1111/jan.14369
Cohen, L., Manion, L., & Morrison, K. (2002). Research methods in education. Routledge.
Cole, C. L., Waterman, S., Stott, J., Saunders, R., Buckman, J. E. J., Pilling, S., & Wheatley, J. (2020).
Adapting IAPT services to support frontline NHS staff during the Covid-19 pandemic: the
Homerton Covid Psychological Support (HCPS) pathway. The Cognitive Behaviour Therapist, 13.
https://doi.org/10.1017/S1754470X20000148
Cooper, A. L., Brown, J. A., Rees, C. S., & Leslie, G. D. (2020). Nurse resilience: A concept
analysis. International journal of mental health nursing, 29(4), 553-575.
Crooks, R. L., & Stein, J. (1988). Psychology: Science, behavior and life. Holt, Rinehart & Winston Inc.
Csikszentmihalyi, M., & Seligman, M. (2000). Positive psychology. American Psychologist, 55(1), 5-14.
Cui, S., Jiang, Y., Shi, Q., Zhang, L., Kong, D., Qian, M., & Chu, J. (2021). Impact of COVID-19 on anxiety,
stress, and coping styles in nurses in emergency departments and fever Clinics: A cross-sectional
survey. Risk management and healthcare policy, 14, 585.
https://doi.org/10.2147/RMHP.S289782
Cusack, K., Jonas, D. E., Forneris, C. A., Wines, C., Sonis, J., Middleton, J. C., ... & Gaynes, B. N. (2016).
Psychological treatments for adults with posttraumatic stress disorder: A systematic review and
meta-analysis. Clinical psychology review, 43, 128-141.
47
Dardas, L.A., & Ahmad, M.M. (2015). Coping strategies as mediators and moderators between stress and
quality of life among parents of children with autistic disorder. Stress and Health, 31(1), 5–12.
https://doi.org/10.1002/smi.2513
Davey, Z., Jackson, D., & Henshall, C. (2020). The value of nurse mentoring relationships: Lessons learnt
from a work‐based resilience enhancement programme for nurses working in the forensic
setting. International journal of mental health nursing, 29(5), 992-1001.
de Medeiros Carvalho, P. M., Moreira, M. M., de Oliveira, M. N. A., Landim, J. M. M., & Neto, M. L. R.
(2020). The psychiatric impact of the novel coronavirus outbreak. Psychiatry research, 286,
112902.
European Centre for Disease Prevention and Control (2021). COVID-19 Pandemic. Retrieved from
https://www.ecdc.europa.eu/en
Fletcher, D., & Sarkar, M. (2013). Psychological resilience. European psychologist.
Gay, L. R., Mills, G. E., & Airasian, P. (2012). Educational Research Competencies for Analysis and
Applications (10 th ed.). London: Pearson Education.
Greasley, A. (2008). Using simulation for facility design: A case study. Simulation Modelling Practice and
Theory, 16(6), 670-677.
Gunawan, J., Aungsuroch, Y., Marzilli, C., Fisher, M.L. & Sukarna, A. (2021). A phenomenological study of
the lived experience of nurses in the battle of COVID-19. Nursing outlook, 69, 652–659.
Henshall, C., Davey, Z., & Jackson, D. (2020). The implementation and evaluation of a resilience
enhancement programme for nurses working in the forensic setting. International Journal of
Mental Health Nursing, 29(3), 508–520
Ho, C. S., Chee, C. Y., & Ho, R. C. (2020). Mental health strategies to combat the psychological impact of
COVID-19 beyond paranoia and panic. Ann Acad Med Singapore, 49(1), 1-3.
Huang, L., Lei, W., Xu, F., Liu, H., & Yu, L. (2020). Emotional responses and coping strategies in nurses
and nursing students during Covid-19 outbreak: A comparative study. PLoS One, 15(8),
e0237303. https://doi.org/10.1371/journal.pone.0237303
Hudgins, T.A. (2016). Resilience, job satisfaction and anticipated turnover in nurse leaders. J Nurs
Manag., 24(1), E62-9. doi: 10.1111/jonm.12289.
48
quality of life among parents of children with autistic disorder. Stress and Health, 31(1), 5–12.
https://doi.org/10.1002/smi.2513
Davey, Z., Jackson, D., & Henshall, C. (2020). The value of nurse mentoring relationships: Lessons learnt
from a work‐based resilience enhancement programme for nurses working in the forensic
setting. International journal of mental health nursing, 29(5), 992-1001.
de Medeiros Carvalho, P. M., Moreira, M. M., de Oliveira, M. N. A., Landim, J. M. M., & Neto, M. L. R.
(2020). The psychiatric impact of the novel coronavirus outbreak. Psychiatry research, 286,
112902.
European Centre for Disease Prevention and Control (2021). COVID-19 Pandemic. Retrieved from
https://www.ecdc.europa.eu/en
Fletcher, D., & Sarkar, M. (2013). Psychological resilience. European psychologist.
Gay, L. R., Mills, G. E., & Airasian, P. (2012). Educational Research Competencies for Analysis and
Applications (10 th ed.). London: Pearson Education.
Greasley, A. (2008). Using simulation for facility design: A case study. Simulation Modelling Practice and
Theory, 16(6), 670-677.
Gunawan, J., Aungsuroch, Y., Marzilli, C., Fisher, M.L. & Sukarna, A. (2021). A phenomenological study of
the lived experience of nurses in the battle of COVID-19. Nursing outlook, 69, 652–659.
Henshall, C., Davey, Z., & Jackson, D. (2020). The implementation and evaluation of a resilience
enhancement programme for nurses working in the forensic setting. International Journal of
Mental Health Nursing, 29(3), 508–520
Ho, C. S., Chee, C. Y., & Ho, R. C. (2020). Mental health strategies to combat the psychological impact of
COVID-19 beyond paranoia and panic. Ann Acad Med Singapore, 49(1), 1-3.
Huang, L., Lei, W., Xu, F., Liu, H., & Yu, L. (2020). Emotional responses and coping strategies in nurses
and nursing students during Covid-19 outbreak: A comparative study. PLoS One, 15(8),
e0237303. https://doi.org/10.1371/journal.pone.0237303
Hudgins, T.A. (2016). Resilience, job satisfaction and anticipated turnover in nurse leaders. J Nurs
Manag., 24(1), E62-9. doi: 10.1111/jonm.12289.
48
International Council of Nurses. The COVID-19 Effect: World’s Nurses Facing Mass Trauma, an
Immediate Danger to the Profession and Future of our Health Systems. Retrieved from
https://www.icn.ch/news/COVID-19-effect-worlds-nursesfacing-mass-trauma-immediate-
danger-profession-and-future-our
Johnson, B. I. (1951). Paradoxical embolism. Journal of clinical pathology, 4(3), 316.
Jung, S. J., & Jun, J. Y. (2020). Mental health and psychological intervention amid COVID-19 outbreak:
perspectives from South Korea. Yonsei Medical Journal, 61(4), 271-272.
Kaveh, M., Hajaliakbari, V., Davari-Tanha, F., Varaei, S., Ghajarzadeh, M., Feizabad, E., ... & Kaveh, Z.
(2022). Anxiety Levels Among Female Iranian Health Care Workers During the COVID-19 Surge: A
Cross-sectional Study. Journal of Obstetrics, Gynecology and Cancer Research (JOGCR), 7(2), 69-
76. https://doi.org/10.1101/2020.05.02.20089045
K ester, K., & Wei, H. (2018). Building nurse resilience. Nursing Management, 49(6), 42-45. 10.1097/01.
Khasne, R. W., Dhakulkar, B. S., Mahajan, H. C., & Kulkarni, A. P. (2020). Burnout among healthcare
workers during COVID-19 pandemic in India: results of a questionnaire-based survey. Indian
Journal of Critical Care Medicine: Peer-reviewed, Official Publication of Indian Society of Critical
Care Medicine, 24(8), 664.
Kim, H.S., Sherman, D.K., & Taylor, S.E. (2008). Culture and social support. American psychologist, 63(6),
518–526. https://doi.org/10.1037/0003-066X
Koh D. (2020). Occupational risks for COVID 19 infection.‐ Occup Med (Lond)., 70, 3 5.‐
https://doi.org/10.1093/occmed/kqaa036
Labrague, L. J., & McEnroe Petitte, D. M. (2018). Job stress in new nurses during the transition period: an
integrative review. International Nursing Review, 65(4), 491-504.
Lapum, J., Nguyen, M., Fredericks, S., Lai, S., & McShane, J. (2021). “Goodbye … Through a Glass Door”:
Emotional Experiences of Working in COVID-19 Acute Care Hospital Environments. Canadian
Journal of Nursing Research, 53(1), 5-15. doi:10.1177/0844562120982420
Lasalvia, A., Amaddeo, F., Porru, S., Carta, A., Tardivo, S., Bovo, C., Ruggeri, M., & Bonetto, C. (2021).
Levels of burn-out among healthcare workers during the COVID-19 pandemic and their
49
Immediate Danger to the Profession and Future of our Health Systems. Retrieved from
https://www.icn.ch/news/COVID-19-effect-worlds-nursesfacing-mass-trauma-immediate-
danger-profession-and-future-our
Johnson, B. I. (1951). Paradoxical embolism. Journal of clinical pathology, 4(3), 316.
Jung, S. J., & Jun, J. Y. (2020). Mental health and psychological intervention amid COVID-19 outbreak:
perspectives from South Korea. Yonsei Medical Journal, 61(4), 271-272.
Kaveh, M., Hajaliakbari, V., Davari-Tanha, F., Varaei, S., Ghajarzadeh, M., Feizabad, E., ... & Kaveh, Z.
(2022). Anxiety Levels Among Female Iranian Health Care Workers During the COVID-19 Surge: A
Cross-sectional Study. Journal of Obstetrics, Gynecology and Cancer Research (JOGCR), 7(2), 69-
76. https://doi.org/10.1101/2020.05.02.20089045
K ester, K., & Wei, H. (2018). Building nurse resilience. Nursing Management, 49(6), 42-45. 10.1097/01.
Khasne, R. W., Dhakulkar, B. S., Mahajan, H. C., & Kulkarni, A. P. (2020). Burnout among healthcare
workers during COVID-19 pandemic in India: results of a questionnaire-based survey. Indian
Journal of Critical Care Medicine: Peer-reviewed, Official Publication of Indian Society of Critical
Care Medicine, 24(8), 664.
Kim, H.S., Sherman, D.K., & Taylor, S.E. (2008). Culture and social support. American psychologist, 63(6),
518–526. https://doi.org/10.1037/0003-066X
Koh D. (2020). Occupational risks for COVID 19 infection.‐ Occup Med (Lond)., 70, 3 5.‐
https://doi.org/10.1093/occmed/kqaa036
Labrague, L. J., & McEnroe Petitte, D. M. (2018). Job stress in new nurses during the transition period: an
integrative review. International Nursing Review, 65(4), 491-504.
Lapum, J., Nguyen, M., Fredericks, S., Lai, S., & McShane, J. (2021). “Goodbye … Through a Glass Door”:
Emotional Experiences of Working in COVID-19 Acute Care Hospital Environments. Canadian
Journal of Nursing Research, 53(1), 5-15. doi:10.1177/0844562120982420
Lasalvia, A., Amaddeo, F., Porru, S., Carta, A., Tardivo, S., Bovo, C., Ruggeri, M., & Bonetto, C. (2021).
Levels of burn-out among healthcare workers during the COVID-19 pandemic and their
49
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
associated factors: a cross-sectional study in a tertiary hospital of a highly burdened area of
north-east Italy. BMJ Open, 11(1):e045127. doi: 10.1136/bmjopen-2020-045127.
Lee, S. A. (2020). Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety.
Death Studies, 44(7), 393-401.
Lee, S. A., Mathis, A. A., Jobe, M. C., & Pappalardo, E. A. (2020). Clinically significant fear and anxiety of
COVID-19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Research,
113112.
Li, Z., Ge, J., Yang, M., Feng, J., Qiao, M., Jiang, R., ... & Yang, C. (2020). Vicarious traumatization in the
general public, members, and non-members of medical teams aiding in COVID-19 control. Brain,
behavior, and immunity, 88, 916-919. Retrieved from https://doi.org/10.1016/j.bbi.2020.03.007
Liu, Y., Gayle, A. A., Wilder-Smith, A., & Rocklöv, J. (2020). The reproductive number of COVID-19 is
higher compared to SARS coronavirus. Journal of Travel Medicine, 27(2), 1-4.
LoGiudice, J. A., & Bartos, S. (2021). Experiences of nurses during the COVID-19 pandemic: A mixed-
methods study. AACN Advanced Critical Care, 32(1), 14-26.
Lorente, L., Vera, M., & Peiró, T. (2021). Nurses´ stressors and psychological distress during the COVID-
19 pandemic: The mediating role of coping and resilience. J Adv Nurs., 77(3), 1335-1344. doi:
10.1111/jan.14695
Luo, M., Guo, L., Yu, M., & Wang, H. (2020). The Psychological and Mental Impact of Coronavirus Disease
2019 (COVID-19) on Medical Staff and General Public–A Systematic Review and Meta-analysis.
Psychiatry Research, 113190.
Maben, J., & Bridges, J. (2020). Covid‐19: Supporting nurses’ psychological and mental health. Journal of
clinical nursing, Accepted-Article. https://doi.org/10.1111/jocn.15307
Marčinko, D., Jakovljević, M., Jakšić, N., Bjedov, S., & Mindoljević Drakulić, A. (2020). The importance of
psychodynamic approach during COVID-19 pandemic. Psychiatria Danubina, 32(1), 15-21.
McDonald, G., Jackson, D., Wilkes, L., & Vickers, M. (2013). Personal resilience in nurses and midwives:
effects of a work-based educational intervention. Contemporary Nurse, 45(1), 134–143.
Millar R.C. (2020). Nursing a patient with Covid 19 infection.‐ Tasman Med J., 1(1), 4 8.‐
50
north-east Italy. BMJ Open, 11(1):e045127. doi: 10.1136/bmjopen-2020-045127.
Lee, S. A. (2020). Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety.
Death Studies, 44(7), 393-401.
Lee, S. A., Mathis, A. A., Jobe, M. C., & Pappalardo, E. A. (2020). Clinically significant fear and anxiety of
COVID-19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Research,
113112.
Li, Z., Ge, J., Yang, M., Feng, J., Qiao, M., Jiang, R., ... & Yang, C. (2020). Vicarious traumatization in the
general public, members, and non-members of medical teams aiding in COVID-19 control. Brain,
behavior, and immunity, 88, 916-919. Retrieved from https://doi.org/10.1016/j.bbi.2020.03.007
Liu, Y., Gayle, A. A., Wilder-Smith, A., & Rocklöv, J. (2020). The reproductive number of COVID-19 is
higher compared to SARS coronavirus. Journal of Travel Medicine, 27(2), 1-4.
LoGiudice, J. A., & Bartos, S. (2021). Experiences of nurses during the COVID-19 pandemic: A mixed-
methods study. AACN Advanced Critical Care, 32(1), 14-26.
Lorente, L., Vera, M., & Peiró, T. (2021). Nurses´ stressors and psychological distress during the COVID-
19 pandemic: The mediating role of coping and resilience. J Adv Nurs., 77(3), 1335-1344. doi:
10.1111/jan.14695
Luo, M., Guo, L., Yu, M., & Wang, H. (2020). The Psychological and Mental Impact of Coronavirus Disease
2019 (COVID-19) on Medical Staff and General Public–A Systematic Review and Meta-analysis.
Psychiatry Research, 113190.
Maben, J., & Bridges, J. (2020). Covid‐19: Supporting nurses’ psychological and mental health. Journal of
clinical nursing, Accepted-Article. https://doi.org/10.1111/jocn.15307
Marčinko, D., Jakovljević, M., Jakšić, N., Bjedov, S., & Mindoljević Drakulić, A. (2020). The importance of
psychodynamic approach during COVID-19 pandemic. Psychiatria Danubina, 32(1), 15-21.
McDonald, G., Jackson, D., Wilkes, L., & Vickers, M. (2013). Personal resilience in nurses and midwives:
effects of a work-based educational intervention. Contemporary Nurse, 45(1), 134–143.
Millar R.C. (2020). Nursing a patient with Covid 19 infection.‐ Tasman Med J., 1(1), 4 8.‐
50
Mo, Y., Deng, L., Zhang, L., Lang, Q., Liao, C., Wang, N., ... & Huang, H. (2020). Work stress among
Chinese nurses to support Wuhan in fighting against COVID‐19 epidemic. Journal of nursing
management, 28(5), 1002-1009. https://doi.org/10.1111/jonm.13014
Morens, D. M., & Fauci, A. S. (2020). Emerging Pandemic Diseases: How We Got to COVID-
19. Cell, 182(5), 1077–1092. https://doi.org/10.1016/j.cell.2020.08.021
Morens, D. M., Daszak, P., & Taubenberger, J. K. (2020). Escaping Pandora’s box—another novel
coronavirus. New England Journal of Medicine, 382(14), 1293-1295.
Munawar, K., & Choudhry, F.R. (2020). Exploring stress coping strategies of frontline emergency health
workers dealing Covid-19 in Pakistan: A qualitative inquiry. American Journal of Infection
Control, 49(3), 286–292. https://doi.org/10.1016/j.ajic.2020.06.214
National Health Commission of China (2020). Principles for emergency psychological crisis intervention
for the new coronavirus pneumonia. Available at:
http://www.nhc.gov.cn/jkj/s3577/202001/6adc08b966594253b2b791be5c3b9467.shtml
North, C. S., Pfefferbaum, B., Vythilingam, M., Martin, G. J., Schorr, J. K., Boudreaux, A. S., ... & Hong, B.
A. (2009). Exposure to bioterrorism and mental health response among staff on Capitol
Hill. Biosecurity and bioterrorism: biodefense strategy, practice, and science, 7(4), 379-388.
NovoPsych (2021). Coping Orientation to Problems Experienced Inventory (Brief-COPE). Retrieved from
https://novopsych.com.au/wp-content/uploads/2018/10/brief-cope_PDF-assessment-
scoring.pdf
Ornell, F., Schuch, J.B., Sordi, A.O., & Kessler, F.H.P. (2020). "Pandemic fear" and COVID-19: mental
health burden and strategies. Braz J Psychiatry, 42(3), 232-235. doi: 10.1590/1516-4446-2020-
0008.
Padida,r, S., Liao, S.M., Magagula, S., Mahlaba, T.A.A., Nhlabatsi, N.M., & Lukas, S. (2021). Assessment of
early COVID-19 compliance to and challenges with public health and social prevention measures
in the Kingdom of Eswatini, using an online survey. Plos one 16(6), e0253954.
https://doi.org/10.1371/journal.pone.0253954
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., & Katsaounou, P. (2020). Prevalence
of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic:
51
Chinese nurses to support Wuhan in fighting against COVID‐19 epidemic. Journal of nursing
management, 28(5), 1002-1009. https://doi.org/10.1111/jonm.13014
Morens, D. M., & Fauci, A. S. (2020). Emerging Pandemic Diseases: How We Got to COVID-
19. Cell, 182(5), 1077–1092. https://doi.org/10.1016/j.cell.2020.08.021
Morens, D. M., Daszak, P., & Taubenberger, J. K. (2020). Escaping Pandora’s box—another novel
coronavirus. New England Journal of Medicine, 382(14), 1293-1295.
Munawar, K., & Choudhry, F.R. (2020). Exploring stress coping strategies of frontline emergency health
workers dealing Covid-19 in Pakistan: A qualitative inquiry. American Journal of Infection
Control, 49(3), 286–292. https://doi.org/10.1016/j.ajic.2020.06.214
National Health Commission of China (2020). Principles for emergency psychological crisis intervention
for the new coronavirus pneumonia. Available at:
http://www.nhc.gov.cn/jkj/s3577/202001/6adc08b966594253b2b791be5c3b9467.shtml
North, C. S., Pfefferbaum, B., Vythilingam, M., Martin, G. J., Schorr, J. K., Boudreaux, A. S., ... & Hong, B.
A. (2009). Exposure to bioterrorism and mental health response among staff on Capitol
Hill. Biosecurity and bioterrorism: biodefense strategy, practice, and science, 7(4), 379-388.
NovoPsych (2021). Coping Orientation to Problems Experienced Inventory (Brief-COPE). Retrieved from
https://novopsych.com.au/wp-content/uploads/2018/10/brief-cope_PDF-assessment-
scoring.pdf
Ornell, F., Schuch, J.B., Sordi, A.O., & Kessler, F.H.P. (2020). "Pandemic fear" and COVID-19: mental
health burden and strategies. Braz J Psychiatry, 42(3), 232-235. doi: 10.1590/1516-4446-2020-
0008.
Padida,r, S., Liao, S.M., Magagula, S., Mahlaba, T.A.A., Nhlabatsi, N.M., & Lukas, S. (2021). Assessment of
early COVID-19 compliance to and challenges with public health and social prevention measures
in the Kingdom of Eswatini, using an online survey. Plos one 16(6), e0253954.
https://doi.org/10.1371/journal.pone.0253954
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., & Katsaounou, P. (2020). Prevalence
of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic:
51
A systematic review and meta-analysis. Brain, behavior, and immunity, 88, 901-907.
https://doi.org/10.1016/j.bbi.2020.05.026
Peterson, C. (2000). The future of optimism. American psychologist, 55(1), 44.
Peterson, C., & Seligman, M. E. (2004). Character strengths and virtues: A handbook and
classification (Vol. 1). Oxford University Press.
Rimmer, A. (2020). Covid 19: give NHS staff rest spaces and free parking not thank yous, says doctor.‐
BMJ, 368, 1171. https://doi.org/10.1136/bmj.m1171
Ruiz‐Fernández, M. D., Ramos‐Pichardo, J. D., Ibáñez‐Masero, O., Cabrera‐Troya, J., Carmona‐Rega, M.
I., & Ortega‐Galán, Á. M. (2020). Compassion fatigue, burnout, compassion satisfaction and
perceived stress in healthcare professionals during the COVID‐19 health crisis in Spain. Journal
of clinical nursing, 29(21-22), 4321-4330.
Savitsky, B., Findling, Y., Ereli, A, & Hendel, T. (2020). Anxiety and coping strategies among nursing
students during the covid-19 pandemic. Nurse Education in Practice 46, 102809.
https://doi.org/10.1016/j.nepr.2020.102809
Sethi, B.A., Sethi, A., Ali, S., & Aamir, H.S. (2020). Impact of Coronavirus disease (COVID-19) pandemic on
health professionals. Pak J Med Sci., 36(COVID19-S4):COVID19-S6-S11. doi:
https://doi.org/10.12669/pjms
Shahrour, G., & Dardas, L.A. (2020). Acute stress disorder, coping self efficacy and subsequent‐
psychological distress among nurses amid COVID 19.‐ Journal of Nursing Management, 28(7),
1686–1695. https://doi.org/10.1111/jonm.13124
Shanafelt, T., Ripp, J., & Trockel, M. (2020). Understanding and addressing sources of anxiety among
health care professionals during the COVID-19 pandemic. Jama, 323(21), 2133-2134.
Shaohua, H., Dai, Q., Wang, T., Zhang, Q., Li, C., & He, H. (2021). Relationship between work stressors
and mental health in frontline nurses exposed to COVID-19: A structural equation model
analysis. Annales Médico-Psychologiques, Revue Psychiatrique, 30(54), 1–14.
Sheroun, D., Wankhar, D., Devrani, A., Lissamma, P.V., & Chatterjee, K. (2020). A study to assess the
perceived stress and coping strategies among BSc nursing students of selected colleges in Pune
52
https://doi.org/10.1016/j.bbi.2020.05.026
Peterson, C. (2000). The future of optimism. American psychologist, 55(1), 44.
Peterson, C., & Seligman, M. E. (2004). Character strengths and virtues: A handbook and
classification (Vol. 1). Oxford University Press.
Rimmer, A. (2020). Covid 19: give NHS staff rest spaces and free parking not thank yous, says doctor.‐
BMJ, 368, 1171. https://doi.org/10.1136/bmj.m1171
Ruiz‐Fernández, M. D., Ramos‐Pichardo, J. D., Ibáñez‐Masero, O., Cabrera‐Troya, J., Carmona‐Rega, M.
I., & Ortega‐Galán, Á. M. (2020). Compassion fatigue, burnout, compassion satisfaction and
perceived stress in healthcare professionals during the COVID‐19 health crisis in Spain. Journal
of clinical nursing, 29(21-22), 4321-4330.
Savitsky, B., Findling, Y., Ereli, A, & Hendel, T. (2020). Anxiety and coping strategies among nursing
students during the covid-19 pandemic. Nurse Education in Practice 46, 102809.
https://doi.org/10.1016/j.nepr.2020.102809
Sethi, B.A., Sethi, A., Ali, S., & Aamir, H.S. (2020). Impact of Coronavirus disease (COVID-19) pandemic on
health professionals. Pak J Med Sci., 36(COVID19-S4):COVID19-S6-S11. doi:
https://doi.org/10.12669/pjms
Shahrour, G., & Dardas, L.A. (2020). Acute stress disorder, coping self efficacy and subsequent‐
psychological distress among nurses amid COVID 19.‐ Journal of Nursing Management, 28(7),
1686–1695. https://doi.org/10.1111/jonm.13124
Shanafelt, T., Ripp, J., & Trockel, M. (2020). Understanding and addressing sources of anxiety among
health care professionals during the COVID-19 pandemic. Jama, 323(21), 2133-2134.
Shaohua, H., Dai, Q., Wang, T., Zhang, Q., Li, C., & He, H. (2021). Relationship between work stressors
and mental health in frontline nurses exposed to COVID-19: A structural equation model
analysis. Annales Médico-Psychologiques, Revue Psychiatrique, 30(54), 1–14.
Sheroun, D., Wankhar, D., Devrani, A., Lissamma, P.V., & Chatterjee, K. (2020). A study to assess the
perceived stress and coping strategies among BSc nursing students of selected colleges in Pune
52
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
during COVID-19 pandemic lockdown. International Journal of Science and Healthcare Research,
5(2), 280–288.
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., & Benedek, D. M. (2020). Public responses
to the novel 2019 coronavirus (2019‐nCoV) in Japan: Mental health consequences and target
populations. Psychiatry and clinical neurosciences, 74(4), 281.
Simione, L., Vagni, M., Gnagnarella, C., Bersani, G., & Pajardi, D. (2021). Mistrust and beliefs in
conspiracy theories differently mediate the effects of psychological factors on propensity for
COVID-19 vaccine. Frontiers in psychology, 12.
Spielberger, C. D. (2010). State Trait anxiety inventory. The Corsini Encyclopedia of Psychology, 1-1.
Uji, M. (2020). Discussing the impact of COVID-19 on mental health from a psychological
perspective. Psychology, 11(7), 1005-1008.
Watson, M. (2021). Psychological Distress During the COVID-19 Pandemic in Nursing Students: A Mixed
Methods Study.
Wei, H., Roberts, P., Strickler, J., & Corbett, R. W. (2019). Nurse leaders’ strategies to foster nurse
resilience. Journal of Nursing Management, 27, 681-687.
WHO (2019). Coronavirus disease (COVID-19) pandemic. Retrieved from
https://www.who.int/emergencies/diseases/novel-coronavirus-2019
World Health Organization (2016). Global Strategic Directions for Strengthening Nursing and Midwifery
2016–2020. Geneva: World Health Organization.
Wu, Y., Wang, J., Luo, C., Hu, S., Lin, X., Anderson, A. E., ... & Qian, Y. (2020). A comparison of burnout
frequency among oncology physicians and nurses working on the frontline and usual wards
during the COVID-19 epidemic in Wuhan, China. Journal of pain and symptom
management, 60(1), e60-e65. https://doi.org/10.1016/j.jpainsymman.2020.04.008
Xiang, Y. T., Yang, Y., Li, W., Zhang, L., Zhang, Q., Cheung, T., & Ng, C. H. (2020). Timely mental health
care for the 2019 novel coronavirus outbreak is urgently needed. The lancet psychiatry, 7(3),
228-229.
53
5(2), 280–288.
Shigemura, J., Ursano, R. J., Morganstein, J. C., Kurosawa, M., & Benedek, D. M. (2020). Public responses
to the novel 2019 coronavirus (2019‐nCoV) in Japan: Mental health consequences and target
populations. Psychiatry and clinical neurosciences, 74(4), 281.
Simione, L., Vagni, M., Gnagnarella, C., Bersani, G., & Pajardi, D. (2021). Mistrust and beliefs in
conspiracy theories differently mediate the effects of psychological factors on propensity for
COVID-19 vaccine. Frontiers in psychology, 12.
Spielberger, C. D. (2010). State Trait anxiety inventory. The Corsini Encyclopedia of Psychology, 1-1.
Uji, M. (2020). Discussing the impact of COVID-19 on mental health from a psychological
perspective. Psychology, 11(7), 1005-1008.
Watson, M. (2021). Psychological Distress During the COVID-19 Pandemic in Nursing Students: A Mixed
Methods Study.
Wei, H., Roberts, P., Strickler, J., & Corbett, R. W. (2019). Nurse leaders’ strategies to foster nurse
resilience. Journal of Nursing Management, 27, 681-687.
WHO (2019). Coronavirus disease (COVID-19) pandemic. Retrieved from
https://www.who.int/emergencies/diseases/novel-coronavirus-2019
World Health Organization (2016). Global Strategic Directions for Strengthening Nursing and Midwifery
2016–2020. Geneva: World Health Organization.
Wu, Y., Wang, J., Luo, C., Hu, S., Lin, X., Anderson, A. E., ... & Qian, Y. (2020). A comparison of burnout
frequency among oncology physicians and nurses working on the frontline and usual wards
during the COVID-19 epidemic in Wuhan, China. Journal of pain and symptom
management, 60(1), e60-e65. https://doi.org/10.1016/j.jpainsymman.2020.04.008
Xiang, Y. T., Yang, Y., Li, W., Zhang, L., Zhang, Q., Cheung, T., & Ng, C. H. (2020). Timely mental health
care for the 2019 novel coronavirus outbreak is urgently needed. The lancet psychiatry, 7(3),
228-229.
53
Xiao, H., Zhang, Y., Kong, D., Li, S., & Yang, N. (2020). Social capital and sleep quality in individuals who
self isolated for 14 days during the coronavirus disease 2019 (COVID 19) outbreak in January‐ ‐
2020 in China. Med Sci Monit., 26, e923921. https://doi.org/10.12659/MSM.923921
Yeager, K., & Roberts, A. (Eds.). (2015). Crisis intervention handbook: Assessment, treatment, and
research. Oxford University Press.
Zhang, Y., Wang, C., Pan, W., Zheng, J., Gao, J., Huang, X., ... & Zhu, C. (2020). Stress, burnout, and coping
strategies of frontline nurses during the COVID-19 epidemic in Wuhan and Shanghai,
China. Frontiers in psychiatry, 11, 1154. https://doi.org/10.3389/fpsyt.2020.565520
Zhu, J., Sun, L., Zhang, L., Wang, H., Fan, A., Yang, B., ... & Xiao, S. (2020). Prevalence and Influencing
Factors of Anxiety and Depression Symptoms in the First-Line Medical Staff Fighting Against
COVID-19 in Gansu. Frontiers in Psychiatry https://dx.doi.org/10.3389%2Ffpsyt.2020.00386
Ziarko, M., Mojs, E., Sikorska, D., & Samborski, W. (2020). Coping and Life Satisfaction: Mediating Role of
Ego-Resiliency in Patients with Rheumatoid Arthritis. Med Princ Pract., 29, 160-165. doi:
10.1159/000503708
Zung, W.K. (1971). Zung Self-Rating Anxiety Scale. Retrieved from
https://www.mnsu.edu/comdis/isad16/papers/therapy16/sugarmanzunganxiety.pdf
Appendices
Appendix A
Demographic questionnaire
Choose your answer to each question and put a tick in the box before the solution you choose. Please
tick only ONE answer for each question unless asked otherwise. Choose your response to each question
54
self isolated for 14 days during the coronavirus disease 2019 (COVID 19) outbreak in January‐ ‐
2020 in China. Med Sci Monit., 26, e923921. https://doi.org/10.12659/MSM.923921
Yeager, K., & Roberts, A. (Eds.). (2015). Crisis intervention handbook: Assessment, treatment, and
research. Oxford University Press.
Zhang, Y., Wang, C., Pan, W., Zheng, J., Gao, J., Huang, X., ... & Zhu, C. (2020). Stress, burnout, and coping
strategies of frontline nurses during the COVID-19 epidemic in Wuhan and Shanghai,
China. Frontiers in psychiatry, 11, 1154. https://doi.org/10.3389/fpsyt.2020.565520
Zhu, J., Sun, L., Zhang, L., Wang, H., Fan, A., Yang, B., ... & Xiao, S. (2020). Prevalence and Influencing
Factors of Anxiety and Depression Symptoms in the First-Line Medical Staff Fighting Against
COVID-19 in Gansu. Frontiers in Psychiatry https://dx.doi.org/10.3389%2Ffpsyt.2020.00386
Ziarko, M., Mojs, E., Sikorska, D., & Samborski, W. (2020). Coping and Life Satisfaction: Mediating Role of
Ego-Resiliency in Patients with Rheumatoid Arthritis. Med Princ Pract., 29, 160-165. doi:
10.1159/000503708
Zung, W.K. (1971). Zung Self-Rating Anxiety Scale. Retrieved from
https://www.mnsu.edu/comdis/isad16/papers/therapy16/sugarmanzunganxiety.pdf
Appendices
Appendix A
Demographic questionnaire
Choose your answer to each question and put a tick in the box before the solution you choose. Please
tick only ONE answer for each question unless asked otherwise. Choose your response to each question
54
and place a checkmark in the box next to it. Unless otherwise instructed, please choose ONLY ONE
ANSWER FOR EACH QUESTION.
1. What is your age group:
o 20-30 years
o 31-40 years
o 40-50 years
o Above 50 years
2. Please select your gender:
o Male
o Female
o Other
3. What is your marital status?
o Married or in a steady relationship
o Married
o Widowed
o Divorced
o Single
4. Have children
o Yes
o No
5. What is your work experience as a nurse in years?
55
ANSWER FOR EACH QUESTION.
1. What is your age group:
o 20-30 years
o 31-40 years
o 40-50 years
o Above 50 years
2. Please select your gender:
o Male
o Female
o Other
3. What is your marital status?
o Married or in a steady relationship
o Married
o Widowed
o Divorced
o Single
4. Have children
o Yes
o No
5. What is your work experience as a nurse in years?
55
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
o 1-5 years
o 6-10 years
o 11-15 years
o 16-20 years
o 20-25 years
o More than 25 years
6. What is your working position as a nurse?
o Front-line
o Second-line
56
o 6-10 years
o 11-15 years
o 16-20 years
o 20-25 years
o More than 25 years
6. What is your working position as a nurse?
o Front-line
o Second-line
56
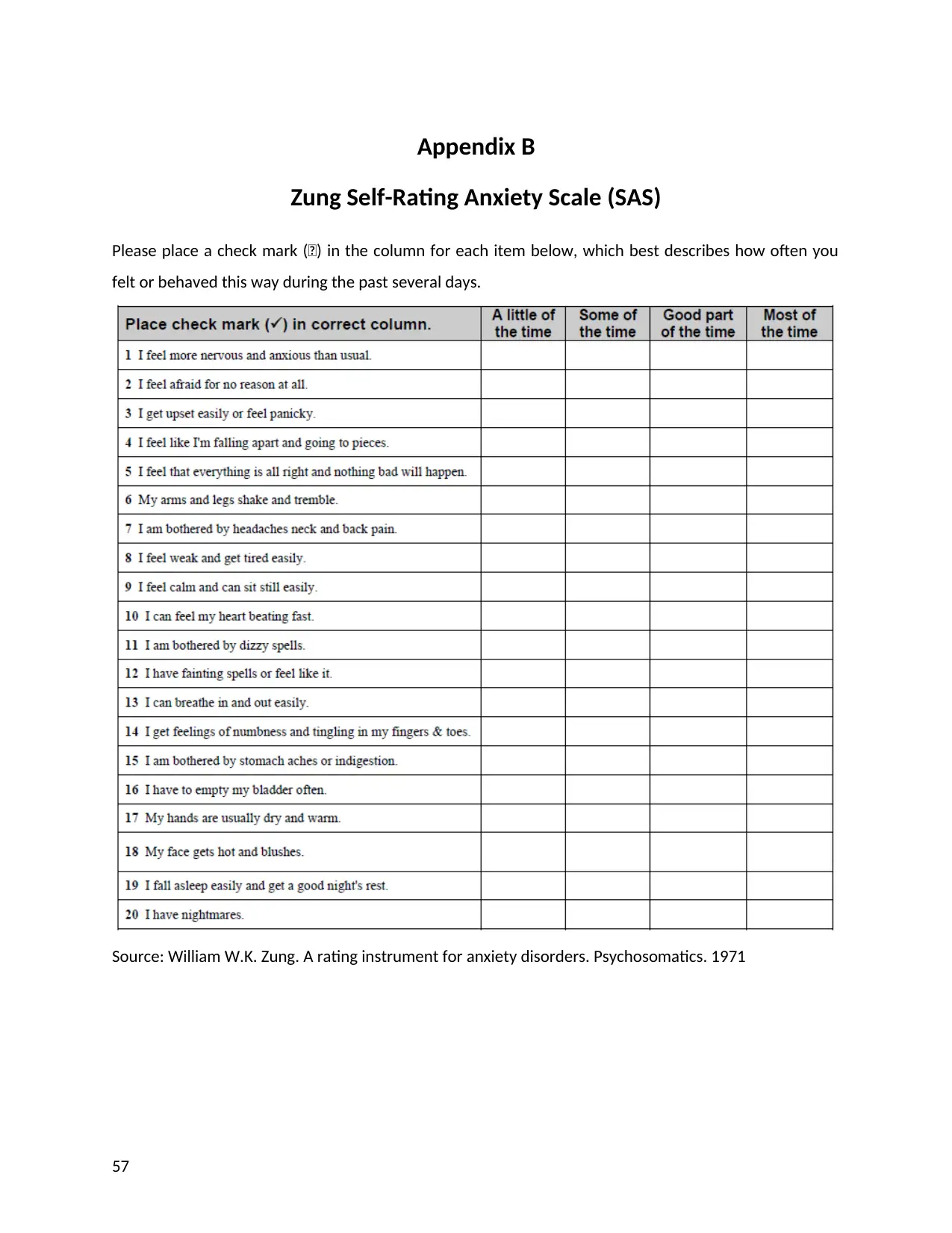
Appendix B
Zung Self-Rating Anxiety Scale (SAS)
Please place a check mark () in the column for each item below, which best describes how often you
felt or behaved this way during the past several days.
Source: William W.K. Zung. A rating instrument for anxiety disorders. Psychosomatics. 1971
57
Zung Self-Rating Anxiety Scale (SAS)
Please place a check mark () in the column for each item below, which best describes how often you
felt or behaved this way during the past several days.
Source: William W.K. Zung. A rating instrument for anxiety disorders. Psychosomatics. 1971
57
Appendix C
Coping Orientation to Problems Experienced Inventory (Brief-Cope)
Instructions:
The following questions ask how you have sought to cope with hardship in your life. Read the
statements and indicate how much you have used each coping style.
58
Coping Orientation to Problems Experienced Inventory (Brief-Cope)
Instructions:
The following questions ask how you have sought to cope with hardship in your life. Read the
statements and indicate how much you have used each coping style.
58
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
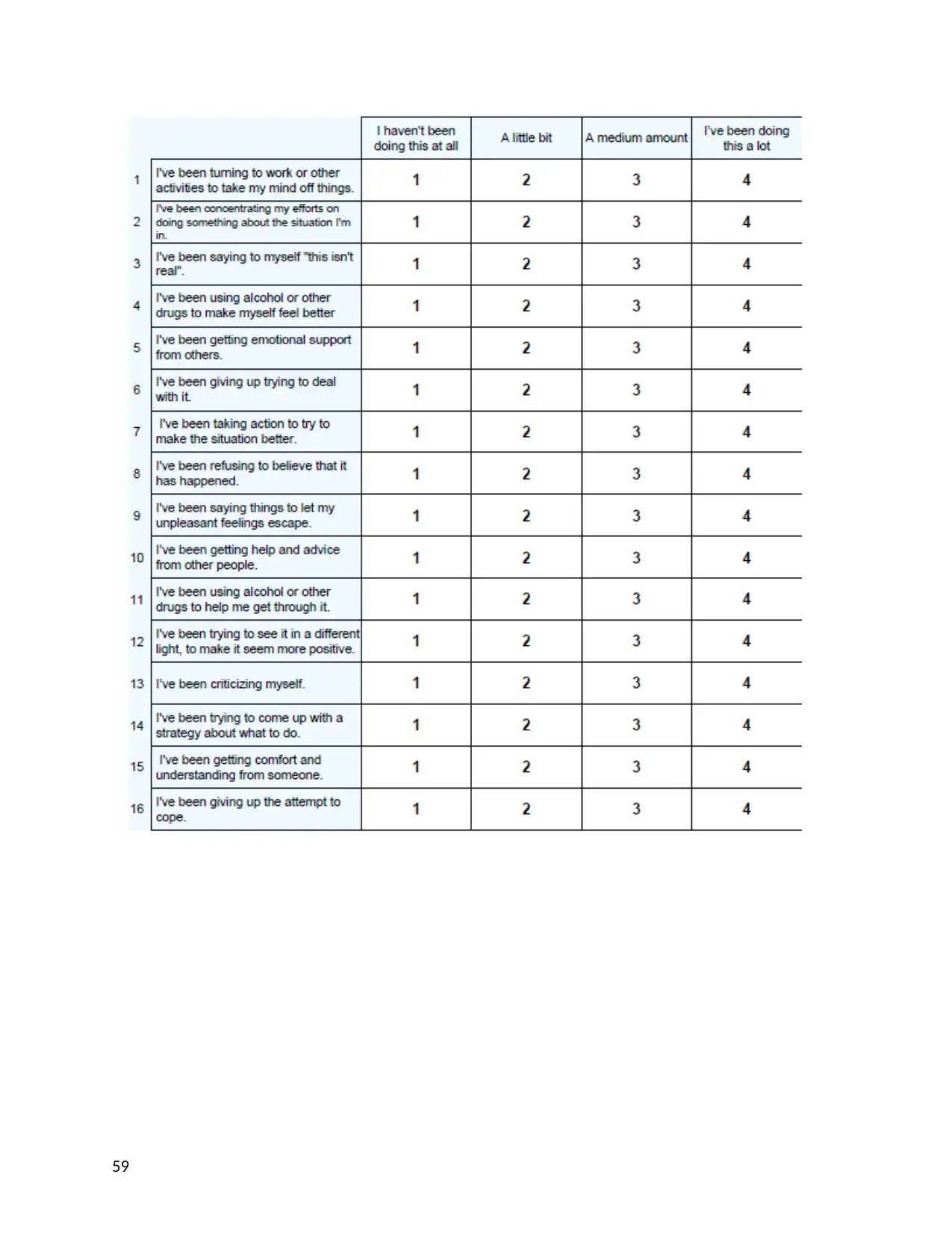
59
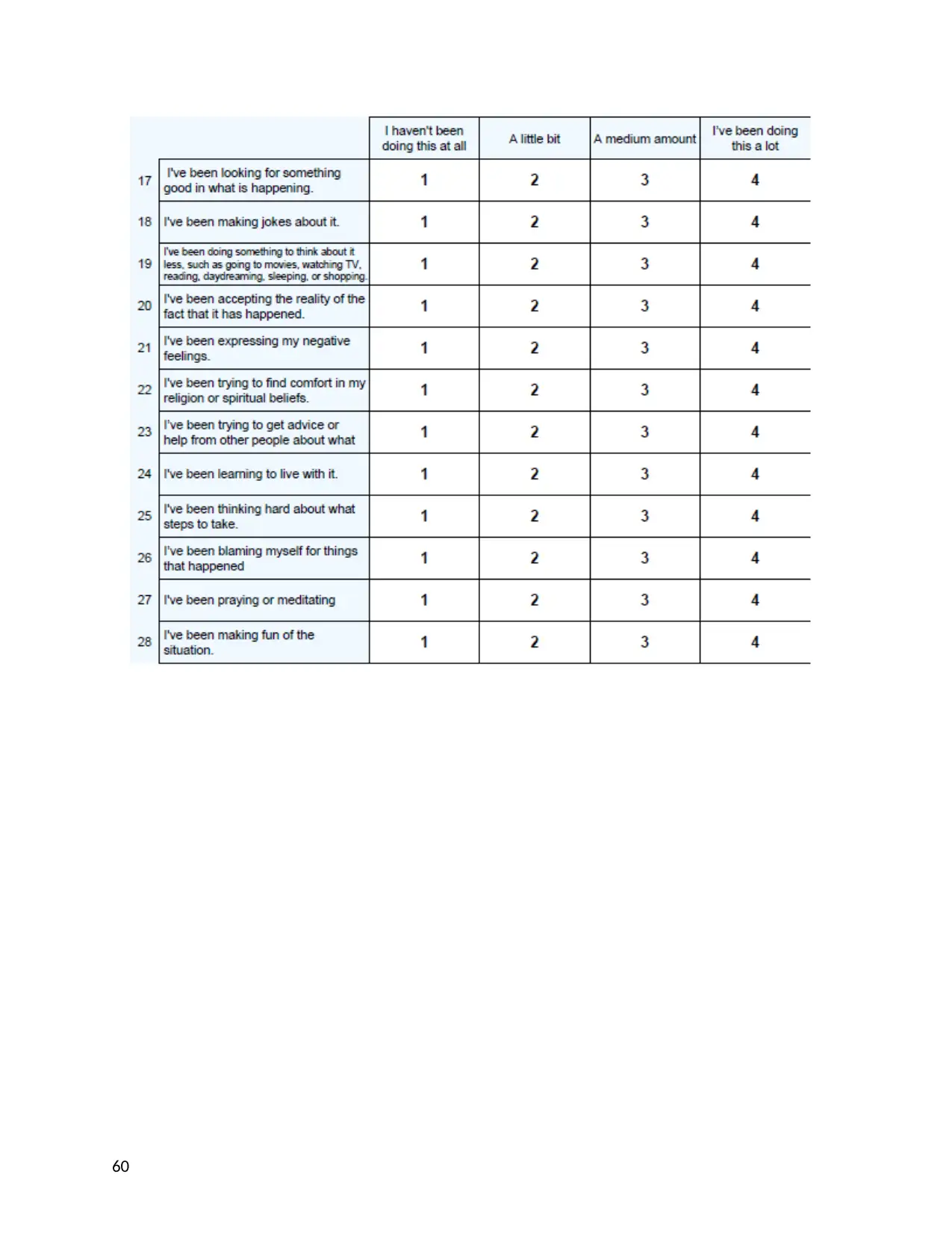
60
1 out of 60
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.