Culture and Language Differences as a Barrier to Quality Care in Saudi Arabia
This assignment requires a research proposal on the significance of interpersonal conflict management in the context of project management students in CQU. The proposal should include a description of the research topic, rationale, research questions, methodology, expected findings, and conclusion.
7 Pages5471 Words452 Views
Added on 2023-06-04
About This Document
This systematic review identifies and summarizes the issues and challenges related to culture and language differences of the health workforce in Saudi Arabia. It highlights the communication barrier between patients and healthcare workers and provides recommendations for improvements.
Culture and Language Differences as a Barrier to Quality Care in Saudi Arabia
This assignment requires a research proposal on the significance of interpersonal conflict management in the context of project management students in CQU. The proposal should include a description of the research topic, rationale, research questions, methodology, expected findings, and conclusion.
Added on 2023-06-04
ShareRelated Documents
Culture and language differences as a barrier to provision
of quality care by the health workforce in Saudi Arabia
Khalid M. Almutairi, MSc, PhD.
425
ABSTRACT
تحديد ودراسة وتلخيص المشاكل والتحديات المتعلقة الأهداف:
بالاختلافات الحضارية واللغوية التي تواجه المرضى والعاملين
الصحيين الأجانب في الملكة العربية السعودية.
وذلك م2014 أُجري هذا المقال المنهجي الشامل في مايو الطريقة:
من أجل تحديد الأبحاث المنشورة التي تناولت هذا الموضوع. لقد
قام مراجعين مستقلين باستشارة مجموعة من الخبراء في الموضوع
ISI Web ofقاعدات بيانات أبحاث إلكترونية ( 4 بالبحث في
)Knowledge, Science Direct, PubMed, Cochrane
وذلك من أجل التدقيق في الأبحاث المنشورة عن الموضوع خلال
. ولقد قمنا بتقييمم2014 م إلى مارس2000 الفترة من يناير
جودة هذه الدراسات من حيث صحة طرق البحث باستخدام
معيار راسيل وجورجي حيث تم تقسيم جودتها إلى ضعيف،
ومتوسط، وقوي.
لقد أشار البحث الالكتروني للأدب العلمي المنشور النتائج:
دراسة ممن تنطبق عليها معايير هذا البحث 12 إلى وجود
المنهجي. وقد كانت قلة معرفة الممرضات غير المسلمات بالحضارة
السعودية، والصعوبات في تحقيق الكفاءة الحضارية، والصدمة
الحضارية من أهم العوامل المؤدية إلى الاختلافات الحضارية.
وشملت مشاكل الاختلافات اللغوية كلا ًمن وضوح لغة العاملين
الصحيين في إعطاء المعلومات، بالإضافة إلى شرح حيثيات الرعاية
الصحية للمرضى بطريقة صحيحة وفعالة.
أشار هذا البحث المنهجي إلى وجود معوقات في التواصل الخاتمة:
بين مقدمي الرعاية الصحية الأجانب والمرضى، وقد تمثل ذلك
في ضعف الكفاءة الحضارية بين هؤلاء الصحيين. وبالرغم من
جهود الحكومة في تقديم البرامج التوعوية لهؤلاء الصحيين، إلا
فنحن بحاجة إلى المزيد من البرامج التعليمية والتوجيهية لهؤلاء
العاملين فيما يتعلق بالحضارة واللغة في الملكة العربية السعودية.
Objectives: To identify, synthesize, and summarize
issues and challenges related to the culture and
language differences of the health workforce in Saudi
Arabia.
Methods: A comprehensive systematic review was
conducted in May 2014 to locate published articles.
Two independent researchers in consultation with
several experts used 4 electronic databases (ISI Web of
Knowledge, Science Direct, PubMed, and Cochrane)
to scrutinize articles published from January 2000 -
March 2014. Each of the studies was given a quality
assessment rating of weak, moderate, or strong, and
was evaluated for methodological soundness using
Russell and Gregory’s criteria.
Results: The online literature search identified
12 studies that met the inclusion criteria. Lack of
knowledge of non-Muslim nurses or culture in Saudi
Arabia, difficulties in achieving cultural competence,
and culture shock were documented as cultural
difference factors. Issues in language difference
include the clarity of language use by health care
providers in giving information and providing
adequate explanation regarding their activities.
Conclusion: The available information provided by
this review study shows that there is a communication
barrier between patients and health care workers
such as healthcare workers demonstrate low cultural
competency. Despite the fact that the government
provides programs for expatriate healthcare workers,
there is a need to further improve educational and
orientation programs regarding the culture and
language in Saudi Arabia.
Saudi Med J 2015; Vol. 36 (4): 425-431
doi: 10.15537/smj.2015.4.10133
From the Department of Community Health Sciences, King Saud
University, Riyadh, Kingdom of Saudi Arabia.
Received 7th September 2014. Accepted 2nd February 2015.
Address correspondence and reprint request to: Dr. Khalid M.
Almutairi, Associate Professor, Department of Community Health
Sciences, King Saud University, Riyadh, Kingdom of Saudi Arabia.
E-mail: assem21@hotmail.com
www.smj.org.sa Saudi Med J 2015; Vol. 36 (4)
OPEN ACCESS
of quality care by the health workforce in Saudi Arabia
Khalid M. Almutairi, MSc, PhD.
425
ABSTRACT
تحديد ودراسة وتلخيص المشاكل والتحديات المتعلقة الأهداف:
بالاختلافات الحضارية واللغوية التي تواجه المرضى والعاملين
الصحيين الأجانب في الملكة العربية السعودية.
وذلك م2014 أُجري هذا المقال المنهجي الشامل في مايو الطريقة:
من أجل تحديد الأبحاث المنشورة التي تناولت هذا الموضوع. لقد
قام مراجعين مستقلين باستشارة مجموعة من الخبراء في الموضوع
ISI Web ofقاعدات بيانات أبحاث إلكترونية ( 4 بالبحث في
)Knowledge, Science Direct, PubMed, Cochrane
وذلك من أجل التدقيق في الأبحاث المنشورة عن الموضوع خلال
. ولقد قمنا بتقييمم2014 م إلى مارس2000 الفترة من يناير
جودة هذه الدراسات من حيث صحة طرق البحث باستخدام
معيار راسيل وجورجي حيث تم تقسيم جودتها إلى ضعيف،
ومتوسط، وقوي.
لقد أشار البحث الالكتروني للأدب العلمي المنشور النتائج:
دراسة ممن تنطبق عليها معايير هذا البحث 12 إلى وجود
المنهجي. وقد كانت قلة معرفة الممرضات غير المسلمات بالحضارة
السعودية، والصعوبات في تحقيق الكفاءة الحضارية، والصدمة
الحضارية من أهم العوامل المؤدية إلى الاختلافات الحضارية.
وشملت مشاكل الاختلافات اللغوية كلا ًمن وضوح لغة العاملين
الصحيين في إعطاء المعلومات، بالإضافة إلى شرح حيثيات الرعاية
الصحية للمرضى بطريقة صحيحة وفعالة.
أشار هذا البحث المنهجي إلى وجود معوقات في التواصل الخاتمة:
بين مقدمي الرعاية الصحية الأجانب والمرضى، وقد تمثل ذلك
في ضعف الكفاءة الحضارية بين هؤلاء الصحيين. وبالرغم من
جهود الحكومة في تقديم البرامج التوعوية لهؤلاء الصحيين، إلا
فنحن بحاجة إلى المزيد من البرامج التعليمية والتوجيهية لهؤلاء
العاملين فيما يتعلق بالحضارة واللغة في الملكة العربية السعودية.
Objectives: To identify, synthesize, and summarize
issues and challenges related to the culture and
language differences of the health workforce in Saudi
Arabia.
Methods: A comprehensive systematic review was
conducted in May 2014 to locate published articles.
Two independent researchers in consultation with
several experts used 4 electronic databases (ISI Web of
Knowledge, Science Direct, PubMed, and Cochrane)
to scrutinize articles published from January 2000 -
March 2014. Each of the studies was given a quality
assessment rating of weak, moderate, or strong, and
was evaluated for methodological soundness using
Russell and Gregory’s criteria.
Results: The online literature search identified
12 studies that met the inclusion criteria. Lack of
knowledge of non-Muslim nurses or culture in Saudi
Arabia, difficulties in achieving cultural competence,
and culture shock were documented as cultural
difference factors. Issues in language difference
include the clarity of language use by health care
providers in giving information and providing
adequate explanation regarding their activities.
Conclusion: The available information provided by
this review study shows that there is a communication
barrier between patients and health care workers
such as healthcare workers demonstrate low cultural
competency. Despite the fact that the government
provides programs for expatriate healthcare workers,
there is a need to further improve educational and
orientation programs regarding the culture and
language in Saudi Arabia.
Saudi Med J 2015; Vol. 36 (4): 425-431
doi: 10.15537/smj.2015.4.10133
From the Department of Community Health Sciences, King Saud
University, Riyadh, Kingdom of Saudi Arabia.
Received 7th September 2014. Accepted 2nd February 2015.
Address correspondence and reprint request to: Dr. Khalid M.
Almutairi, Associate Professor, Department of Community Health
Sciences, King Saud University, Riyadh, Kingdom of Saudi Arabia.
E-mail: assem21@hotmail.com
www.smj.org.sa Saudi Med J 2015; Vol. 36 (4)
OPEN ACCESS
426
Culture and language differences ... Almutairi
Saudi Med J 2015; Vol. 36 (4) www.smj.org.sa
Effective communication with patients and health
care workers is a key process in safe and quality
health care.1 Patient and clinician relationships rely on
good communication, resulting in improved patient
satisfaction, adherence to medical recommendations,
and better healthcare outcomes.2 Effective patient and
clinician interaction starts from the patient inquiry
regarding symptoms of the disease, to discussing the
treatment, and management plan of the clinician.2
According to Stewart,3 many healthcare professionals
believe that communication is more effective when it
is responsive to patient needs, values, and preferences.
Factors that influence this communication include
cultural differences, low health literacy, and language
differences.1 Cultural misunderstanding between
patients and predominantly expatriate health care
providers is another factor contributing to patient
dissatisfaction and poor quality of care. The cultural
setting of Saudi Arabia is a unique blend of Arabic
with an Islamic influence.4 The beliefs and attitudes
of Saudi people are characterized by the Arabic tribal
traditions and customs, and the Islamic worldview.4,5
The uniqueness of Saudi culture, coupled with the
large number of expatriate health professionals who
have a limited knowledge of Saudi culture, aggravate
the problem of providing high quality of care and
may cause potential cultural conflicts, which may lead
to patient dissatisfaction. According to the Ministry
of Health (MOH), most healthcare workers in Saudi
Arabia such as nurses are expatriates from countries like
India, the Philippines, Malaysia, Australia, America,
the United Kingdom, South Africa, and other Middle
Eastern countries with different cultural backgrounds.6-9
Not only do cultural backgrounds differ among these
healthcare workers, language differences also serve as
a barrier to effective communication. This language
barrier is often not immediately an issue because of their
proficiency in English. However, the Arabic language
is the primary language in Saudi Arabia and not all
patients understand or are proficient in the English
language.10 With the increasing number of expatriates’
healthcare workers, effective communication may not
occur and the quality of patients’ healthcare as well as
their safety will be at risk. Therefore, we aim to perform a
systematic review to identify, synthesize, and summarize
the issues and challenges of effective communication
between patients and health workers, and to provide
recommendations for improvements.
Methods. A comprehensive systematic review was
conducted in May 2014. We extensively searched
electronic databases (ISI Web of Knowledge, Science
Direct, PubMed and Cochrane) dating from January
2000 through March 2014. The search terms used were
cultural difference, language difference, barriers, health
care workers, health workforce, and Saudi Arabia.
Grey literature was performed (King Saud University -
Central Library) using electronic database and reference
list of included articles were scanned for further studies.
The electronic search was completed in consultation
with several experts and supplemented by several
databases. We included studies if they met the following
criteria: (1) focus on issues or areas of concern as they
relate to cultural and language differences; (2) focus on
barriers in quality of care of the health workforce in
Saudi Arabia; and (3) studies carried out with different
designs and method of analysis - case-control studies or
cross-sectional studies and review studies. Following the
literature search, titles and abstracts were independently
assessed by 2 researchers for inclusion criteria. Studies
not carried out in Saudi Arabia were excluded in this
phase. After the preliminary screening, the included
studies were analyzed and reviewed by a specialist for
significance and potential duplication. Details of the
author of the study, location of the study, sample, and
major findings were extracted from each study that met
the inclusion criteria.
Quality appraisal and synthesis of included studies.
After the extraction of all included studies, each study
was critically appraised by a specialist using the health
evidence.org tool for reviews.11 Meta-analysis was
not conducted due to different study designs of the
included studies. Each of the studies was appraised and
was evaluated for methodological soundness using the
Russell and Gregory’s criteria.12 Evaluation was based
on whether the article answered each of the following
questions: 1) Is the research question clear and
adequately substantiated? 2) Is the design appropriate
for the research question? 3) Was the sampling method
appropriate for the research question and design? 4)
Was data collected and managed systematically? 5) Was
the data analyzed appropriately? A quality score was
Disclosure. Author has no conflict of interests, and the
work was not supported or funded by any drug company.
The author would like to extend his sincere appreciation
to the Deanship of Scientific Research at King Saud
University for funding this research (RG# 1435-024).
Culture and language differences ... Almutairi
Saudi Med J 2015; Vol. 36 (4) www.smj.org.sa
Effective communication with patients and health
care workers is a key process in safe and quality
health care.1 Patient and clinician relationships rely on
good communication, resulting in improved patient
satisfaction, adherence to medical recommendations,
and better healthcare outcomes.2 Effective patient and
clinician interaction starts from the patient inquiry
regarding symptoms of the disease, to discussing the
treatment, and management plan of the clinician.2
According to Stewart,3 many healthcare professionals
believe that communication is more effective when it
is responsive to patient needs, values, and preferences.
Factors that influence this communication include
cultural differences, low health literacy, and language
differences.1 Cultural misunderstanding between
patients and predominantly expatriate health care
providers is another factor contributing to patient
dissatisfaction and poor quality of care. The cultural
setting of Saudi Arabia is a unique blend of Arabic
with an Islamic influence.4 The beliefs and attitudes
of Saudi people are characterized by the Arabic tribal
traditions and customs, and the Islamic worldview.4,5
The uniqueness of Saudi culture, coupled with the
large number of expatriate health professionals who
have a limited knowledge of Saudi culture, aggravate
the problem of providing high quality of care and
may cause potential cultural conflicts, which may lead
to patient dissatisfaction. According to the Ministry
of Health (MOH), most healthcare workers in Saudi
Arabia such as nurses are expatriates from countries like
India, the Philippines, Malaysia, Australia, America,
the United Kingdom, South Africa, and other Middle
Eastern countries with different cultural backgrounds.6-9
Not only do cultural backgrounds differ among these
healthcare workers, language differences also serve as
a barrier to effective communication. This language
barrier is often not immediately an issue because of their
proficiency in English. However, the Arabic language
is the primary language in Saudi Arabia and not all
patients understand or are proficient in the English
language.10 With the increasing number of expatriates’
healthcare workers, effective communication may not
occur and the quality of patients’ healthcare as well as
their safety will be at risk. Therefore, we aim to perform a
systematic review to identify, synthesize, and summarize
the issues and challenges of effective communication
between patients and health workers, and to provide
recommendations for improvements.
Methods. A comprehensive systematic review was
conducted in May 2014. We extensively searched
electronic databases (ISI Web of Knowledge, Science
Direct, PubMed and Cochrane) dating from January
2000 through March 2014. The search terms used were
cultural difference, language difference, barriers, health
care workers, health workforce, and Saudi Arabia.
Grey literature was performed (King Saud University -
Central Library) using electronic database and reference
list of included articles were scanned for further studies.
The electronic search was completed in consultation
with several experts and supplemented by several
databases. We included studies if they met the following
criteria: (1) focus on issues or areas of concern as they
relate to cultural and language differences; (2) focus on
barriers in quality of care of the health workforce in
Saudi Arabia; and (3) studies carried out with different
designs and method of analysis - case-control studies or
cross-sectional studies and review studies. Following the
literature search, titles and abstracts were independently
assessed by 2 researchers for inclusion criteria. Studies
not carried out in Saudi Arabia were excluded in this
phase. After the preliminary screening, the included
studies were analyzed and reviewed by a specialist for
significance and potential duplication. Details of the
author of the study, location of the study, sample, and
major findings were extracted from each study that met
the inclusion criteria.
Quality appraisal and synthesis of included studies.
After the extraction of all included studies, each study
was critically appraised by a specialist using the health
evidence.org tool for reviews.11 Meta-analysis was
not conducted due to different study designs of the
included studies. Each of the studies was appraised and
was evaluated for methodological soundness using the
Russell and Gregory’s criteria.12 Evaluation was based
on whether the article answered each of the following
questions: 1) Is the research question clear and
adequately substantiated? 2) Is the design appropriate
for the research question? 3) Was the sampling method
appropriate for the research question and design? 4)
Was data collected and managed systematically? 5) Was
the data analyzed appropriately? A quality score was
Disclosure. Author has no conflict of interests, and the
work was not supported or funded by any drug company.
The author would like to extend his sincere appreciation
to the Deanship of Scientific Research at King Saud
University for funding this research (RG# 1435-024).

427www.smj.org.sa Saudi Med J 2015; Vol. 36 (4)
Culture and language differences ... Almutairi
applied to each study using these guidelines. Each study
was given a quality score ranging from 0 to 5, where 5
is the highest, based on whether they met each of the
guidelines.
Results. The online literature search yielded 79
results, and 10 references were pre-selected from
searching the grey literature and reference list of included
articles because they aligned with study objectives. In
total, 39 studies passed the preliminary screening and
went for more detailed evaluation. After an extensive
evaluation, only 12 studies met the inclusion criteria.
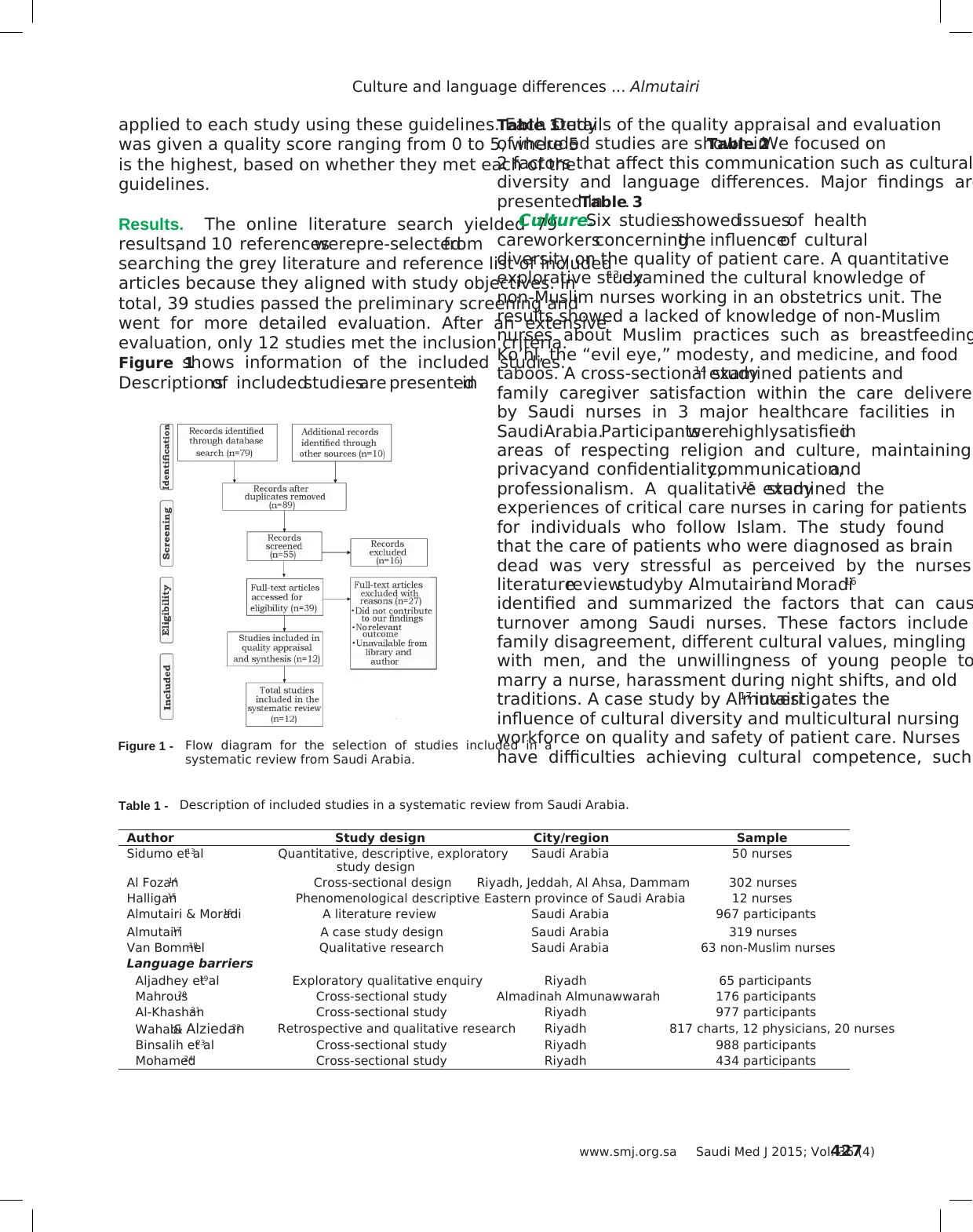
Figure 1 shows information of the included studies.
Descriptions of included studies are presented in
Figure 1 - Flow diagram for the selection of studies included in a
systematic review from Saudi Arabia.
Table 1 - Description of included studies in a systematic review from Saudi Arabia.
Author Study design City/region Sample
Sidumo et al13 Quantitative, descriptive, exploratory
study design
Saudi Arabia 50 nurses
Al Fozan14 Cross-sectional design Riyadh, Jeddah, Al Ahsa, Dammam 302 nurses
Halligan15 Phenomenological descriptive Eastern province of Saudi Arabia 12 nurses
Almutairi & Moradi16 A literature review Saudi Arabia 967 participants
Almutairi17 A case study design Saudi Arabia 319 nurses
Van Bommel18 Qualitative research Saudi Arabia 63 non-Muslim nurses
Language barriers
Aljadhey et al19 Exploratory qualitative enquiry Riyadh 65 participants
Mahrous20 Cross-sectional study Almadinah Almunawwarah 176 participants
Al-Khashan21 Cross-sectional study Riyadh 977 participants
Wahabi & Alziedan22 Retrospective and qualitative research Riyadh 817 charts, 12 physicians, 20 nurses
Binsalih et al23 Cross-sectional study Riyadh 988 participants
Mohamed24 Cross-sectional study Riyadh 434 participants
Table 1. Details of the quality appraisal and evaluation
of included studies are shown in Table 2. We focused on
2 factors that affect this communication such as cultural
diversity and language differences. Major findings are
presented in Table 3.
Culture. Six studies showed issues of health
care workers concerning the influence of cultural
diversity on the quality of patient care. A quantitative
explorative study13 examined the cultural knowledge of
non-Muslim nurses working in an obstetrics unit. The
results showed a lacked of knowledge of non-Muslim
nurses about Muslim practices such as breastfeeding,
Ko’hl, the “evil eye,” modesty, and medicine, and food
taboos. A cross-sectional study14 examined patients and
family caregiver satisfaction within the care delivered
by Saudi nurses in 3 major healthcare facilities in
Saudi Arabia. Participants were highly satisfied in
areas of respecting religion and culture, maintaining
privacy and confidentiality, communication, and
professionalism. A qualitative study15 examined the
experiences of critical care nurses in caring for patients
for individuals who follow Islam. The study found
that the care of patients who were diagnosed as brain
dead was very stressful as perceived by the nurses. A
literature review study by Almutairi and Moradi16
identified and summarized the factors that can cause
turnover among Saudi nurses. These factors include
family disagreement, different cultural values, mingling
with men, and the unwillingness of young people to
marry a nurse, harassment during night shifts, and old
traditions. A case study by Almutairi17 investigates the
influence of cultural diversity and multicultural nursing
workforce on quality and safety of patient care. Nurses
have difficulties achieving cultural competence, such
Culture and language differences ... Almutairi
applied to each study using these guidelines. Each study
was given a quality score ranging from 0 to 5, where 5
is the highest, based on whether they met each of the
guidelines.
Results. The online literature search yielded 79
results, and 10 references were pre-selected from
searching the grey literature and reference list of included
articles because they aligned with study objectives. In
total, 39 studies passed the preliminary screening and
went for more detailed evaluation. After an extensive
evaluation, only 12 studies met the inclusion criteria.
Figure 1 shows information of the included studies.
Descriptions of included studies are presented in
Figure 1 - Flow diagram for the selection of studies included in a
systematic review from Saudi Arabia.
Table 1 - Description of included studies in a systematic review from Saudi Arabia.
Author Study design City/region Sample
Sidumo et al13 Quantitative, descriptive, exploratory
study design
Saudi Arabia 50 nurses
Al Fozan14 Cross-sectional design Riyadh, Jeddah, Al Ahsa, Dammam 302 nurses
Halligan15 Phenomenological descriptive Eastern province of Saudi Arabia 12 nurses
Almutairi & Moradi16 A literature review Saudi Arabia 967 participants
Almutairi17 A case study design Saudi Arabia 319 nurses
Van Bommel18 Qualitative research Saudi Arabia 63 non-Muslim nurses
Language barriers
Aljadhey et al19 Exploratory qualitative enquiry Riyadh 65 participants
Mahrous20 Cross-sectional study Almadinah Almunawwarah 176 participants
Al-Khashan21 Cross-sectional study Riyadh 977 participants
Wahabi & Alziedan22 Retrospective and qualitative research Riyadh 817 charts, 12 physicians, 20 nurses
Binsalih et al23 Cross-sectional study Riyadh 988 participants
Mohamed24 Cross-sectional study Riyadh 434 participants
Table 1. Details of the quality appraisal and evaluation
of included studies are shown in Table 2. We focused on
2 factors that affect this communication such as cultural
diversity and language differences. Major findings are
presented in Table 3.
Culture. Six studies showed issues of health
care workers concerning the influence of cultural
diversity on the quality of patient care. A quantitative
explorative study13 examined the cultural knowledge of
non-Muslim nurses working in an obstetrics unit. The
results showed a lacked of knowledge of non-Muslim
nurses about Muslim practices such as breastfeeding,
Ko’hl, the “evil eye,” modesty, and medicine, and food
taboos. A cross-sectional study14 examined patients and
family caregiver satisfaction within the care delivered
by Saudi nurses in 3 major healthcare facilities in
Saudi Arabia. Participants were highly satisfied in
areas of respecting religion and culture, maintaining
privacy and confidentiality, communication, and
professionalism. A qualitative study15 examined the
experiences of critical care nurses in caring for patients
for individuals who follow Islam. The study found
that the care of patients who were diagnosed as brain
dead was very stressful as perceived by the nurses. A
literature review study by Almutairi and Moradi16
identified and summarized the factors that can cause
turnover among Saudi nurses. These factors include
family disagreement, different cultural values, mingling
with men, and the unwillingness of young people to
marry a nurse, harassment during night shifts, and old
traditions. A case study by Almutairi17 investigates the
influence of cultural diversity and multicultural nursing
workforce on quality and safety of patient care. Nurses
have difficulties achieving cultural competence, such
End of preview
Want to access all the pages? Upload your documents or become a member.
Related Documents
Literature Review: Table of Evidence on Cultural Barriers in Healthcare for Indigenous Australianslg...
|9
|1925
|353
NUR 4029 - Nursing Assignment | Patient Safetylg...
|7
|1754
|268
Musculoskeletal Problems in Healthcare Professionalslg...
|15
|3601
|20