Deteriorating Patient Scenario Critique
VerifiedAdded on 2022/08/21
|19
|5069
|51
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Student Name: Shirin Solomonsz
Student Number:11648137
Subject Code: NRS312
Subject Name: Essential Nursing Care: Managing the deteriorating patient
Subject Lecturer: Evan Plowman
Assessment item: 3
Assessment title: Deteriorating Patient Scenario Critique
Due date: 09/04/20
Date of submission: 09/04/20
Word count (excluding in text citations, reference list and appendices): 2126
1
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Student Number:11648137
Subject Code: NRS312
Subject Name: Essential Nursing Care: Managing the deteriorating patient
Subject Lecturer: Evan Plowman
Assessment item: 3
Assessment title: Deteriorating Patient Scenario Critique
Due date: 09/04/20
Date of submission: 09/04/20
Word count (excluding in text citations, reference list and appendices): 2126
1
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Introduction
Identifying and accurately responding to a deteriorating patient is a significant global
priority in nursing and is accomplished by closely supervising variations in the physiological
parameters of a patient, and interpreting the early signs and symptoms of a patient’s health
decline (McGaughey et al., 2017). This scenario involves caring for a deteriorating patient
Mrs Brown who underwent an uneventful total hip replacement (THR) surgery of the left hip.
Post the procedure, Mrs Brown’s health had started to gradually decline over time, which led
to a diagnosis of an acute ischaemic stroke. This assignment will identify the factors involved
in the deterioration of Mrs Brown and discuss the management of her presentation after a
THR.
Question 1: Recognise
Clinical Emergency Response System (CERS) is an umbrella term that refers to the
response of a health facility or service to deteriorating patients, within the provisions of care
delivery (Levett-Jones, 2018, p. 4). CERS are formulated then customized to the needs of the
health service and its resources (Gulacti et al., 2016). The principle components of the CERS
comprise of clinical review procedure, rapid response procedure, essential healthcare
equipment for performing resuscitation, and escalation procedure for transferring patients.
According to the WSLHD CERS framework, there are three levels or three tiers that are
namely, (i) yellow zone breach, (ii) red zone breach that is not life threatening, and (iii) red
zone breach that is life threatening (NSW Government, 2019). While the yellow zone
corresponds to clinical review and encompasses a compulsory bedside review of patient by
the team leader for determination of the necessity of clinical review. The second level
encompasses rapid response and medical officers are required to proceed with immediacy for
completing bedside patient review if they meet these criteria. In the third level, the Advance
2
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Identifying and accurately responding to a deteriorating patient is a significant global
priority in nursing and is accomplished by closely supervising variations in the physiological
parameters of a patient, and interpreting the early signs and symptoms of a patient’s health
decline (McGaughey et al., 2017). This scenario involves caring for a deteriorating patient
Mrs Brown who underwent an uneventful total hip replacement (THR) surgery of the left hip.
Post the procedure, Mrs Brown’s health had started to gradually decline over time, which led
to a diagnosis of an acute ischaemic stroke. This assignment will identify the factors involved
in the deterioration of Mrs Brown and discuss the management of her presentation after a
THR.
Question 1: Recognise
Clinical Emergency Response System (CERS) is an umbrella term that refers to the
response of a health facility or service to deteriorating patients, within the provisions of care
delivery (Levett-Jones, 2018, p. 4). CERS are formulated then customized to the needs of the
health service and its resources (Gulacti et al., 2016). The principle components of the CERS
comprise of clinical review procedure, rapid response procedure, essential healthcare
equipment for performing resuscitation, and escalation procedure for transferring patients.
According to the WSLHD CERS framework, there are three levels or three tiers that are
namely, (i) yellow zone breach, (ii) red zone breach that is not life threatening, and (iii) red
zone breach that is life threatening (NSW Government, 2019). While the yellow zone
corresponds to clinical review and encompasses a compulsory bedside review of patient by
the team leader for determination of the necessity of clinical review. The second level
encompasses rapid response and medical officers are required to proceed with immediacy for
completing bedside patient review if they meet these criteria. In the third level, the Advance
2
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Life Support (ALS) team or code blue team is expected to immediately continue completion
of patient bedside review and provide any intervention to further stop patient deterioration.
There are a range of noticeable physiological irregularities prior to adverse health
events that lead to clinical deterioration of a patient (REF). Following the THR surgery, the
Registered Nurse (RN) was accurate in continuously checking the vital signs of the patient
and also maintained observation charts at regular interval of four hours. During patient
deterioration, observations charts act as the principal tool for information recording
concerning physiological measures and thus are imperative in identification of any health
risks (Christofidis et al., 2016). The RN worked in accordance to the Australian Commission
on Safety and Quality in Health Care that has formulated evidence-based observation chart
for the recognition of clinical deterioration, which in turn prompts instant action in response
to any abnormalities (ACSQHC, 2020). Some common signs that an RN must identify as
clinical deterioration are increased respiratory rate (tachypnoea), retractions, ineffective
breathing, increased heart rate (tachycardia), hyper/hypotention, oliguria and altered
conscious state (Churpek, Adhikari & Edelson, 2016).
The clinical review and rapid response team must have been triggered when Mrs.
Brown’s daughter reported her concerns regarding the health of her mother. (what do you
mean must have been triggered? openeded statement). Just prior to handover, Mrs Brown
reported slight decrease in blood pressure from the previous reading of 121/87 mmHg, when
she had just been transferred to the surgical unit. Complaints of numbness from Mrs Brown at
0045 hours, in addition to an altered GCS are early warning signs of deterioration. Apart
from complaints of headache and increase pain score, there was also an increased blood
pressure, heart rate and respiratory rate, in comparison to the previous instance when the vital
signs had been checked, which would indicate a need for a review of the patients condition.
This was accurately followed since Jeremy immediately called the doctor and asked for a
3
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
of patient bedside review and provide any intervention to further stop patient deterioration.
There are a range of noticeable physiological irregularities prior to adverse health
events that lead to clinical deterioration of a patient (REF). Following the THR surgery, the
Registered Nurse (RN) was accurate in continuously checking the vital signs of the patient
and also maintained observation charts at regular interval of four hours. During patient
deterioration, observations charts act as the principal tool for information recording
concerning physiological measures and thus are imperative in identification of any health
risks (Christofidis et al., 2016). The RN worked in accordance to the Australian Commission
on Safety and Quality in Health Care that has formulated evidence-based observation chart
for the recognition of clinical deterioration, which in turn prompts instant action in response
to any abnormalities (ACSQHC, 2020). Some common signs that an RN must identify as
clinical deterioration are increased respiratory rate (tachypnoea), retractions, ineffective
breathing, increased heart rate (tachycardia), hyper/hypotention, oliguria and altered
conscious state (Churpek, Adhikari & Edelson, 2016).
The clinical review and rapid response team must have been triggered when Mrs.
Brown’s daughter reported her concerns regarding the health of her mother. (what do you
mean must have been triggered? openeded statement). Just prior to handover, Mrs Brown
reported slight decrease in blood pressure from the previous reading of 121/87 mmHg, when
she had just been transferred to the surgical unit. Complaints of numbness from Mrs Brown at
0045 hours, in addition to an altered GCS are early warning signs of deterioration. Apart
from complaints of headache and increase pain score, there was also an increased blood
pressure, heart rate and respiratory rate, in comparison to the previous instance when the vital
signs had been checked, which would indicate a need for a review of the patients condition.
This was accurately followed since Jeremy immediately called the doctor and asked for a
3
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
clinical review. However, there was an indication for clinical review, corresponding to the
yellow zone and soon after, her blood pressure became hypertensive at 220/145 mmHg at
0505 hours. thereafter, a call with the doctor, the only the blood pressure was checked on
hourly basis, and other vital signs were not taken into consideration. This is a major fault on
the part of the RN as a full picture of the patient cannot be achieved if only 1 of the vital
signs are measured (Al-Moteri et al., 2019). Therefore, hourly assessment of respiration rate,
body temperature, and pulse could have provided more information on the likelihood of the
patient to suffer from an ischemic attack.
Question 2: Escalate
Timely escalation for patients who manifest signs and symptoms of clinical
deterioration in healthcare settings is a major challenge encountered by most healthcare
professionals and it encompasses the capability to provide immediate care, following
recognition of adverse signs (Baig et al., 2019). On analysing the case scenario, it can be
suggested that there was considerable delay in escalating the health deterioration of Mrs.
Brown to the rapid response team, which furthered her declining condition. The first occasion
where a concern should have been raised was when Mrs Brown’s daughter voiced her
apprehension and worry about her mother’s health. Despite the fact that the RN informed
about the anxiety of family member of the patient, Jeremy was occupied with administration
of antibiotics to other patients, as a result could not offer adequate time to assess the patient.
Nonetheless, there was no delay in patient escalation for clinical review. Upon obesrving
unexpected but steady increase in vital signs like blood pressure, heart rate and respiratory
rate, when compared to the normal values, the doctor was called and the incident was
reported. Hourly pressure checks and recording the vital signs after discussion with the doctor
also ensured that all probable efforts had being taken by Jeremy to put off the onset of any
adverse health event. However, there was a delay in escalation, when in spite of noticing the
4
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
yellow zone and soon after, her blood pressure became hypertensive at 220/145 mmHg at
0505 hours. thereafter, a call with the doctor, the only the blood pressure was checked on
hourly basis, and other vital signs were not taken into consideration. This is a major fault on
the part of the RN as a full picture of the patient cannot be achieved if only 1 of the vital
signs are measured (Al-Moteri et al., 2019). Therefore, hourly assessment of respiration rate,
body temperature, and pulse could have provided more information on the likelihood of the
patient to suffer from an ischemic attack.
Question 2: Escalate
Timely escalation for patients who manifest signs and symptoms of clinical
deterioration in healthcare settings is a major challenge encountered by most healthcare
professionals and it encompasses the capability to provide immediate care, following
recognition of adverse signs (Baig et al., 2019). On analysing the case scenario, it can be
suggested that there was considerable delay in escalating the health deterioration of Mrs.
Brown to the rapid response team, which furthered her declining condition. The first occasion
where a concern should have been raised was when Mrs Brown’s daughter voiced her
apprehension and worry about her mother’s health. Despite the fact that the RN informed
about the anxiety of family member of the patient, Jeremy was occupied with administration
of antibiotics to other patients, as a result could not offer adequate time to assess the patient.
Nonetheless, there was no delay in patient escalation for clinical review. Upon obesrving
unexpected but steady increase in vital signs like blood pressure, heart rate and respiratory
rate, when compared to the normal values, the doctor was called and the incident was
reported. Hourly pressure checks and recording the vital signs after discussion with the doctor
also ensured that all probable efforts had being taken by Jeremy to put off the onset of any
adverse health event. However, there was a delay in escalation, when in spite of noticing the
4
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
the increase in blood pressure to 220/145 mmHg at 0505 hours, no more calls were made to
for the doctor or other healthcare personnel. Moreover, the patient was not continuously
monitored, and the next observation occurred after a gap for 50 minutes. This time in
between the recording of two vital signs was crucial and had the probability of affecting the
patient to an extent that it would be difficult to revive her.
Communication within multidisciplinary healthcare team could have been enhanced
by appropriate usage of the ISBAR (Identify, Situation, Background, and Recommendation)
tool that would enhance safety during transfer of patient clinical information (Kostoff et al.,
2016). Usage of this tool at the time of handover of the patient Mrs Brown would have
guaranteed that the health concerns of the patient or her family members were taken into
consideration, which in turn would have decreased errors in communication. Identification of
clinical alerts such as FYI flags (For Your Information flags) and other indicators also help in
improving communication between team members (Tarango et al., 2018). Taking into
consideration the fact that ineffective communication leads to patient harm, proper linguistic
exchange must have occurred while transferring the responsibilities of Mrs Brown to Jeremy
(Foronda, MacWilliams & McArthur, 2016). Usage of technologies that enhance efficacy of
handover like electronic prescribing systems, electronic medical records, and automated
medical reconciliation could have streamlined access and exchange of information in Mrs
Browns care (Mills, Weidmann& Stewart, 2017). It was necessary to provide adequate
information to Mrs Brown’s daughter about the medical condition and care plan. In addition,
ensuring that there is a responsible provider present who will constantly update information
related to the health status of the patient was imperative. Informing the daughter about the
proposed treatment plan, medications, and other significant variations would have also
enhanced communication and transparency of care (Datta et al., 2017). Inclusion of written
materials that are literacy and language appropriate and in a patient friendly language would
5
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
for the doctor or other healthcare personnel. Moreover, the patient was not continuously
monitored, and the next observation occurred after a gap for 50 minutes. This time in
between the recording of two vital signs was crucial and had the probability of affecting the
patient to an extent that it would be difficult to revive her.
Communication within multidisciplinary healthcare team could have been enhanced
by appropriate usage of the ISBAR (Identify, Situation, Background, and Recommendation)
tool that would enhance safety during transfer of patient clinical information (Kostoff et al.,
2016). Usage of this tool at the time of handover of the patient Mrs Brown would have
guaranteed that the health concerns of the patient or her family members were taken into
consideration, which in turn would have decreased errors in communication. Identification of
clinical alerts such as FYI flags (For Your Information flags) and other indicators also help in
improving communication between team members (Tarango et al., 2018). Taking into
consideration the fact that ineffective communication leads to patient harm, proper linguistic
exchange must have occurred while transferring the responsibilities of Mrs Brown to Jeremy
(Foronda, MacWilliams & McArthur, 2016). Usage of technologies that enhance efficacy of
handover like electronic prescribing systems, electronic medical records, and automated
medical reconciliation could have streamlined access and exchange of information in Mrs
Browns care (Mills, Weidmann& Stewart, 2017). It was necessary to provide adequate
information to Mrs Brown’s daughter about the medical condition and care plan. In addition,
ensuring that there is a responsible provider present who will constantly update information
related to the health status of the patient was imperative. Informing the daughter about the
proposed treatment plan, medications, and other significant variations would have also
enhanced communication and transparency of care (Datta et al., 2017). Inclusion of written
materials that are literacy and language appropriate and in a patient friendly language would
5
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
prevent miscommunication and confusion with medical jargon between the team members
and family, thus improving communication and enhancing patient safety (Schnitzler et al.,
2017). Usage of the ‘teach-back’ method would also have proved effective in
interdisciplinary communication since this method relies on confirming understanding of the
receiver about the information that has been shared (Badaczewski et al., 2017). Furthermore,
scheduling regular meetings with the staff for holding discussions on patient health and
satisfaction would have encouraged open information exchange and collaboration, thereby
facilitating sharing details about the patient and timely delivery of care services
(Cunningham, 2019).
Question 3: Manage
An analysis of the case scenario suggests that the nursing care involved patient-
controlled analgesia (PCA) whereby Mrs. Brown was permitted to administer her own pain
relief medication, through activation of the dosing button of the pump. It is a well-known fact
that PCA helps in rapid alleviation of pain by allowing the patient to adjust medication
dosage and administer own pain relief. However, there is likelihood that the patient might
administer high dosage of the medication, or might even administer narcotics due to their
euphoric effects, despite control of pain symptoms (Ryan et al., 2018). Moreover,
inappropriate programming of the PCA device increases the likelihood of an overdose or
underdose. PCA is not appropriate for patients reporting signs of confusion. It also proves
ineffective for patients who are critically ill. Hence, this was an incorrect nursing care plan.
Furthermore, during telephonic discussion with the doctor, Jeremy asked if he could
administer paracetamol for Mrs Brown pain. Paracetamol is widely used as a pain reliever,
and the common dosage is around one or two 500 mg tablets. Thus, the 1 g dosage that had
been prescribed over telephone was correct (Gaul &Eschalier, 2018). On observing 89%
oxygen saturation, the patient was also administered a Hudson mask at 6L/minute. The major
6
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
and family, thus improving communication and enhancing patient safety (Schnitzler et al.,
2017). Usage of the ‘teach-back’ method would also have proved effective in
interdisciplinary communication since this method relies on confirming understanding of the
receiver about the information that has been shared (Badaczewski et al., 2017). Furthermore,
scheduling regular meetings with the staff for holding discussions on patient health and
satisfaction would have encouraged open information exchange and collaboration, thereby
facilitating sharing details about the patient and timely delivery of care services
(Cunningham, 2019).
Question 3: Manage
An analysis of the case scenario suggests that the nursing care involved patient-
controlled analgesia (PCA) whereby Mrs. Brown was permitted to administer her own pain
relief medication, through activation of the dosing button of the pump. It is a well-known fact
that PCA helps in rapid alleviation of pain by allowing the patient to adjust medication
dosage and administer own pain relief. However, there is likelihood that the patient might
administer high dosage of the medication, or might even administer narcotics due to their
euphoric effects, despite control of pain symptoms (Ryan et al., 2018). Moreover,
inappropriate programming of the PCA device increases the likelihood of an overdose or
underdose. PCA is not appropriate for patients reporting signs of confusion. It also proves
ineffective for patients who are critically ill. Hence, this was an incorrect nursing care plan.
Furthermore, during telephonic discussion with the doctor, Jeremy asked if he could
administer paracetamol for Mrs Brown pain. Paracetamol is widely used as a pain reliever,
and the common dosage is around one or two 500 mg tablets. Thus, the 1 g dosage that had
been prescribed over telephone was correct (Gaul &Eschalier, 2018). On observing 89%
oxygen saturation, the patient was also administered a Hudson mask at 6L/minute. The major
6
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
drawback was the fact these masks deliver only up to 60% oxygen and might even result in
suffocation under conditions when the gas flow gets interrupted, resulting in creating
breathing problems for the patient (Bashir et al., 2019).
It would have been appropriate to adopt the ABCDE approach at the bedside for
assessing the deteriorating patient. The patient was not assessed for airway patency, which
would have helped in identifying obstructions (Smith & Bowden, 2017). Some signs that
should have been observed are paradoxical chest and abdominal movement, cynosis,
breathing depth and entry of air in the lungs. While determining cardiac output effectiveness,
the capillary refill time was also not noted. Additionally, following the AVPU system would
have facilitated identification of issues related to voice, awake, pain and unresponsiveness
(Akanbi et al., 2017). The healthcare professionals should also have used the early warning
scoring system parameters (EWSS), where a score more than or equivalent to 3 would have
facilitated early identification of the health deterioration (Mestrom et al., 2019).
The primary intervention would include administration of nonsteroidal anti-
inflammatory drugs (NSAID) that would have provided relief from pain by nonselectively
inhibiting the cyclooxygenase enzymes that catalyse prostaglandin and thromboxane
formation (Osafo et al., 2017). For addressing the increased blood pressure, administration of
Angiotensin-converting enzyme (ACE) inhibitors would have widened the blood vessels,
thus increasing the blood pumped by the heart, and decreasing the workload (Messerli et al.,
2018). In addition, fluid resuscitation would have helped in decreasing preload, thus reducing
blood pressure (Vatankhah et al., 2018). For addressing tachypnoea, the patient should have
been placed at Fowler position that would have permitted maximum excursion of her lungs
and chest expansion (Mariani, Hamzah &Solikin, 2018). Usage of an incentive spirometer
would have promoted deep inspiration, and increased oxygenation (McLeod et al., 2018).
Administration of beta-adrenergic agonist would have stimulated relaxation of the smooth
7
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
suffocation under conditions when the gas flow gets interrupted, resulting in creating
breathing problems for the patient (Bashir et al., 2019).
It would have been appropriate to adopt the ABCDE approach at the bedside for
assessing the deteriorating patient. The patient was not assessed for airway patency, which
would have helped in identifying obstructions (Smith & Bowden, 2017). Some signs that
should have been observed are paradoxical chest and abdominal movement, cynosis,
breathing depth and entry of air in the lungs. While determining cardiac output effectiveness,
the capillary refill time was also not noted. Additionally, following the AVPU system would
have facilitated identification of issues related to voice, awake, pain and unresponsiveness
(Akanbi et al., 2017). The healthcare professionals should also have used the early warning
scoring system parameters (EWSS), where a score more than or equivalent to 3 would have
facilitated early identification of the health deterioration (Mestrom et al., 2019).
The primary intervention would include administration of nonsteroidal anti-
inflammatory drugs (NSAID) that would have provided relief from pain by nonselectively
inhibiting the cyclooxygenase enzymes that catalyse prostaglandin and thromboxane
formation (Osafo et al., 2017). For addressing the increased blood pressure, administration of
Angiotensin-converting enzyme (ACE) inhibitors would have widened the blood vessels,
thus increasing the blood pumped by the heart, and decreasing the workload (Messerli et al.,
2018). In addition, fluid resuscitation would have helped in decreasing preload, thus reducing
blood pressure (Vatankhah et al., 2018). For addressing tachypnoea, the patient should have
been placed at Fowler position that would have permitted maximum excursion of her lungs
and chest expansion (Mariani, Hamzah &Solikin, 2018). Usage of an incentive spirometer
would have promoted deep inspiration, and increased oxygenation (McLeod et al., 2018).
Administration of beta-adrenergic agonist would have stimulated relaxation of the smooth
7
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
muscles of the airways, thus leading to bronchodilation and opening the air passages (Hsu &
Bajaj, 2019). There was a need to teach the patient pursed-lip breathing for enhancing
ventilation (Parisien-La Salle et al., 2019). Use of venturi mask for delivering oxygen
concentration would have proven effective since it is a high-flow oxygen therapy equipment
and offers total inspiratory flow (Pennisi et al., 2019). Vasodilator therapy using arteriolar
dilators like hydralazine would have helped in addressing tachycardia, by increasing cardiac
output and reducing the increased peripheral vascular resistance (Maille et al., 2016). Thus,
there was a failure on the part of the healthcare professionals due to which they were unable
to prevent clinical deterioration of the patient.
Conclusion
To conclude, it is imperative for nurses to address the physical ailments of a patient,
in addition to providing care to the emotional needs. Patient deterioration is generally
described as the predictable, evolving and symptomatic procedure of aggravating physiology
of patient, towards critical health condition. The assessment helped to comprehend that the
delay in patient escalation and timely care delivery care were major issues in this case.
Hence, there was a need to immediately seek help from care professionals on observing
abnormal physiological signs in the patient, in addition to timely CERS. A collaborative
approach could have intervened and improved outcomes for Mrs Brown treatment.
8
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Bajaj, 2019). There was a need to teach the patient pursed-lip breathing for enhancing
ventilation (Parisien-La Salle et al., 2019). Use of venturi mask for delivering oxygen
concentration would have proven effective since it is a high-flow oxygen therapy equipment
and offers total inspiratory flow (Pennisi et al., 2019). Vasodilator therapy using arteriolar
dilators like hydralazine would have helped in addressing tachycardia, by increasing cardiac
output and reducing the increased peripheral vascular resistance (Maille et al., 2016). Thus,
there was a failure on the part of the healthcare professionals due to which they were unable
to prevent clinical deterioration of the patient.
Conclusion
To conclude, it is imperative for nurses to address the physical ailments of a patient,
in addition to providing care to the emotional needs. Patient deterioration is generally
described as the predictable, evolving and symptomatic procedure of aggravating physiology
of patient, towards critical health condition. The assessment helped to comprehend that the
delay in patient escalation and timely care delivery care were major issues in this case.
Hence, there was a need to immediately seek help from care professionals on observing
abnormal physiological signs in the patient, in addition to timely CERS. A collaborative
approach could have intervened and improved outcomes for Mrs Brown treatment.
8
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Reference List
Akanbi, O. O., Onilede, D. A., Adeoti, M. L., Olakulehin, O. A., Idowu, N. A., &Olanipekun,
O. O. (2017). Improving Clinicians’ and Nurses’ Response to Abnormal Vital Signs
in Hospital: The Roles of Modified Early Warning Scoring System and Rapid
Response System. Journal of Advances in Medicine and Medical Research, 1-11.
https://doi.org/10.9734/BJMMR/2017/32370
Al-Moteri, M., Plummer, V., Cooper, S., & Symmons, M. (2019). Clinical deterioration of
ward patients in the presence of antecedents: A systematic review and narrative
synthesis. Australian Critical Care, 32(5), 411-420.
https://doi.org/10.1016/j.aucc.2018.06.004
Australian Commission on Safety and Quality in Health Care. (2020). Observation and
Response Charts. https://www.safetyandquality.gov.au/our-work/recognising-and-
responding-deterioration/recognising-and-responding-physiological-deterioration/
guide-implementation-national-consensus-statement/observation-and-response-charts
Badaczewski, A., Bauman, L. J., Blank, A. E., Dreyer, B., Abrams, M. A., Stein, R. E., ... &
Sharif, I. (2017). Relationship between teach-back and patient-centered
communication in primary care pediatric encounters. Patient education and
counseling, 100(7), 1345-1352. https://doi.org/10.1016/j.pec.2017.02.022
Baig, M. M., Afifi, S., GholamHosseini, H., & Ullah, E. (2019). Deterioration to decision: a
comprehensive literature review of rapid response applications for deteriorating
patients in acute care settings. Health and Technology, 1-7.
https://doi.org/10.1007/s12553-019-00403-7
Bashir, T., Srinivas Murki, S. K., Reddy, V. K., &Oleti, T. P. (2019). 'Nasal mask’in
comparison with ‘nasal prongs’ or ‘rotation of nasal mask with nasal prongs’ reduce
9
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Akanbi, O. O., Onilede, D. A., Adeoti, M. L., Olakulehin, O. A., Idowu, N. A., &Olanipekun,
O. O. (2017). Improving Clinicians’ and Nurses’ Response to Abnormal Vital Signs
in Hospital: The Roles of Modified Early Warning Scoring System and Rapid
Response System. Journal of Advances in Medicine and Medical Research, 1-11.
https://doi.org/10.9734/BJMMR/2017/32370
Al-Moteri, M., Plummer, V., Cooper, S., & Symmons, M. (2019). Clinical deterioration of
ward patients in the presence of antecedents: A systematic review and narrative
synthesis. Australian Critical Care, 32(5), 411-420.
https://doi.org/10.1016/j.aucc.2018.06.004
Australian Commission on Safety and Quality in Health Care. (2020). Observation and
Response Charts. https://www.safetyandquality.gov.au/our-work/recognising-and-
responding-deterioration/recognising-and-responding-physiological-deterioration/
guide-implementation-national-consensus-statement/observation-and-response-charts
Badaczewski, A., Bauman, L. J., Blank, A. E., Dreyer, B., Abrams, M. A., Stein, R. E., ... &
Sharif, I. (2017). Relationship between teach-back and patient-centered
communication in primary care pediatric encounters. Patient education and
counseling, 100(7), 1345-1352. https://doi.org/10.1016/j.pec.2017.02.022
Baig, M. M., Afifi, S., GholamHosseini, H., & Ullah, E. (2019). Deterioration to decision: a
comprehensive literature review of rapid response applications for deteriorating
patients in acute care settings. Health and Technology, 1-7.
https://doi.org/10.1007/s12553-019-00403-7
Bashir, T., Srinivas Murki, S. K., Reddy, V. K., &Oleti, T. P. (2019). 'Nasal mask’in
comparison with ‘nasal prongs’ or ‘rotation of nasal mask with nasal prongs’ reduce
9
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
the incidence of nasal injury in preterm neonates supported on nasal continuous
positive airway pressure (nCPAP): A randomized controlled trial. PloS one, 14(1).
10.1371/journal.pone.0211476
Christofidis, M. J., Hill, A., Horswill, M. S., & Watson, M. O. (2016). Observation chart
design features affect the detection of patient deterioration: a systematic experimental
evaluation. Journal of advanced nursing, 72(1), 158-172.
https://doi.org/10.1111/jan.12824
Churpek, M. M., Adhikari, R., & Edelson, D. P. (2016). The value of vital sign trends for
detecting clinical deterioration on the wards. Resuscitation, 102, 1-5.
https://doi.org/10.1016/j.resuscitation.2016.02.005
Cunningham, L. (2019). A Tool Kit for Improving Communication in Your Healthcare
Organization. Frontiers of health services management, 36(1), 3-13.
https://journals.lww.com/frontiersonline/Abstract/2019/09000/A_Tool_Kit_for_Impro
ving_Communication_in_Your.2.aspx
Datta, S. S., Tripathi, L., Varghese, R., Logan, J., Gessler, S., Chatterjee, S., ... & Menon, U.
(2017). Pivotal role of families in doctor–patient communication in oncology: a
qualitative study of patients, their relatives and cancer clinicians. European journal of
cancer care, 26(5), e12543. https://doi.org/10.1111/ecc.12543
Edelson, D. P., Carey, K., Winslow, C. J., &Churpek, M. M. (2018). Less is more: detecting
clinical deterioration in the hospital with machine learning using only age, heart rate
and respiratory rate. In C15. CRITICAL CARE: BIG DATA AND ARTIFICIAL
INTELLIGENCE IN CRITICAL ILLNESS (pp. A4444-A4444). American Thoracic
Society. https://www.atsjournals.org/doi/abs/10.1164/ajrccm-
conference.2018.197.1_MeetingAbstracts.A4444
10
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
positive airway pressure (nCPAP): A randomized controlled trial. PloS one, 14(1).
10.1371/journal.pone.0211476
Christofidis, M. J., Hill, A., Horswill, M. S., & Watson, M. O. (2016). Observation chart
design features affect the detection of patient deterioration: a systematic experimental
evaluation. Journal of advanced nursing, 72(1), 158-172.
https://doi.org/10.1111/jan.12824
Churpek, M. M., Adhikari, R., & Edelson, D. P. (2016). The value of vital sign trends for
detecting clinical deterioration on the wards. Resuscitation, 102, 1-5.
https://doi.org/10.1016/j.resuscitation.2016.02.005
Cunningham, L. (2019). A Tool Kit for Improving Communication in Your Healthcare
Organization. Frontiers of health services management, 36(1), 3-13.
https://journals.lww.com/frontiersonline/Abstract/2019/09000/A_Tool_Kit_for_Impro
ving_Communication_in_Your.2.aspx
Datta, S. S., Tripathi, L., Varghese, R., Logan, J., Gessler, S., Chatterjee, S., ... & Menon, U.
(2017). Pivotal role of families in doctor–patient communication in oncology: a
qualitative study of patients, their relatives and cancer clinicians. European journal of
cancer care, 26(5), e12543. https://doi.org/10.1111/ecc.12543
Edelson, D. P., Carey, K., Winslow, C. J., &Churpek, M. M. (2018). Less is more: detecting
clinical deterioration in the hospital with machine learning using only age, heart rate
and respiratory rate. In C15. CRITICAL CARE: BIG DATA AND ARTIFICIAL
INTELLIGENCE IN CRITICAL ILLNESS (pp. A4444-A4444). American Thoracic
Society. https://www.atsjournals.org/doi/abs/10.1164/ajrccm-
conference.2018.197.1_MeetingAbstracts.A4444
10
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Foronda, C., MacWilliams, B., & McArthur, E. (2016). Interprofessional communication in
healthcare: An integrative review. Nurse education in practice, 19, 36-40.
https://doi.org/10.1016/j.nepr.2016.04.005
Gaul, C., &Eschalier, A. (2018). Dose Can Help to Achieve Effective Pain Relief for Acute
Mild to Moderate Pain with Over-the-Counter Paracetamol. The Open Pain
Journal, 11(1). https://benthamopen.com/ABSTRACT/TOPAINJ-11-12
Gulacti, U., Lok, U., Aydin, I., Gurger, M., Hatipoglu, S., &Polat, H. (2016). Outcomes of in-
hospital cardiopulmonary resuscitation after introduction of medical emergency
team. Kuwait Med J, 48, 127-131.
https://www.researchgate.net/profile/Umut_Gulacti/publication/304952542_Outcome
s_of_in-
hospital_cardiopulmonary_resuscitation_after_introduction_of_medical_emergency_t
eam/links/58ec9b130f7e9b149c088c37/Outcomes-of-in-hospital-cardiopulmonary-
resuscitation-after-introduction-of-medical-emergency-team.pdf
Hsu, E., & Bajaj, T. (2019). Beta 2 Agonists. In StatPearls [Internet]. StatPearls Publishing.
https://www.ncbi.nlm.nih.gov/books/NBK542249/
Jones,T. Clinical Reasoning: Learning to think like a nurse. (pp. 2-13).Melbourne:
Pearson Australia.
Kostoff, M., Burkhardt, C., Winter, A., & Shrader, S. (2016). An interprofessional simulation
using the SBAR communication tool. American journal of pharmaceutical
education, 80(9). https://doi.org/10.5688/ajpe809157
Levett-Jones, T. (2018). Clinical reasoning: what it is and why it matters. In Levett-
11
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
healthcare: An integrative review. Nurse education in practice, 19, 36-40.
https://doi.org/10.1016/j.nepr.2016.04.005
Gaul, C., &Eschalier, A. (2018). Dose Can Help to Achieve Effective Pain Relief for Acute
Mild to Moderate Pain with Over-the-Counter Paracetamol. The Open Pain
Journal, 11(1). https://benthamopen.com/ABSTRACT/TOPAINJ-11-12
Gulacti, U., Lok, U., Aydin, I., Gurger, M., Hatipoglu, S., &Polat, H. (2016). Outcomes of in-
hospital cardiopulmonary resuscitation after introduction of medical emergency
team. Kuwait Med J, 48, 127-131.
https://www.researchgate.net/profile/Umut_Gulacti/publication/304952542_Outcome
s_of_in-
hospital_cardiopulmonary_resuscitation_after_introduction_of_medical_emergency_t
eam/links/58ec9b130f7e9b149c088c37/Outcomes-of-in-hospital-cardiopulmonary-
resuscitation-after-introduction-of-medical-emergency-team.pdf
Hsu, E., & Bajaj, T. (2019). Beta 2 Agonists. In StatPearls [Internet]. StatPearls Publishing.
https://www.ncbi.nlm.nih.gov/books/NBK542249/
Jones,T. Clinical Reasoning: Learning to think like a nurse. (pp. 2-13).Melbourne:
Pearson Australia.
Kostoff, M., Burkhardt, C., Winter, A., & Shrader, S. (2016). An interprofessional simulation
using the SBAR communication tool. American journal of pharmaceutical
education, 80(9). https://doi.org/10.5688/ajpe809157
Levett-Jones, T. (2018). Clinical reasoning: what it is and why it matters. In Levett-
11
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Maille, N., Gokina, N., Mandalà, M., Colton, I., &Osol, G. (2016). Mechanism of
hydralazine-induced relaxation in resistance arteries during pregnancy: hydralazine
induces vasodilation via a prostacyclin pathway. Vascular pharmacology, 78, 36-42.
https://doi.org/10.1016/j.vph.2015.07.009
Mariani, M., Hamzah, H., &Solikin, S. (2018, October). EFFECTIVENESS OF OXYGEN
ACTIVITY THERAPY LOW FLOW SYSTEM BINASAL KANUL WITH SOW
FOWLER POSITION TO REDUCE PAIN IN PATIENTS OF ACUTE CORONER
SIDE IN ULIN RSUD. In International Conference on Heath Care and Management
2018 (Vol. 1, No. 1).
http://ichm2018.stikep-ppnijabar.ac.id/index.php/ichm2018/article/view/41
McGaughey, J., O'Halloran, P., Porter, S., Trinder, J., & Blackwood, B. (2017). Early
warning systems and rapid response to the deteriorating patient in hospital: A realist
evaluation. Journal of advanced nursing, 73(12), 3119-3132.
https://doi.org/10.1111/jan.13367
McLeod, M., Morgan, A., Nordstrand, F., & Williams, S. (2018). Incentive Spirometry: In
post-surgical patients, how effective is the use of incentive spirometers in decreasing
pulmonary complications during hospital
stays?.https://dc.arcabc.ca/islandora/object/dc%3A28253
Messerli, F. H., Bangalore, S., Bavishi, C., &Rimoldi, S. F. (2018). Angiotensin-converting
enzyme inhibitors in hypertension: to use or not to use?. Journal of the American
College of Cardiology, 71(13), 1474-1482.
http://www.onlinejacc.org/content/71/13/1474?
sso=1&sso_redirect_count=3&access_token=&intcmp=trendmd
12
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
hydralazine-induced relaxation in resistance arteries during pregnancy: hydralazine
induces vasodilation via a prostacyclin pathway. Vascular pharmacology, 78, 36-42.
https://doi.org/10.1016/j.vph.2015.07.009
Mariani, M., Hamzah, H., &Solikin, S. (2018, October). EFFECTIVENESS OF OXYGEN
ACTIVITY THERAPY LOW FLOW SYSTEM BINASAL KANUL WITH SOW
FOWLER POSITION TO REDUCE PAIN IN PATIENTS OF ACUTE CORONER
SIDE IN ULIN RSUD. In International Conference on Heath Care and Management
2018 (Vol. 1, No. 1).
http://ichm2018.stikep-ppnijabar.ac.id/index.php/ichm2018/article/view/41
McGaughey, J., O'Halloran, P., Porter, S., Trinder, J., & Blackwood, B. (2017). Early
warning systems and rapid response to the deteriorating patient in hospital: A realist
evaluation. Journal of advanced nursing, 73(12), 3119-3132.
https://doi.org/10.1111/jan.13367
McLeod, M., Morgan, A., Nordstrand, F., & Williams, S. (2018). Incentive Spirometry: In
post-surgical patients, how effective is the use of incentive spirometers in decreasing
pulmonary complications during hospital
stays?.https://dc.arcabc.ca/islandora/object/dc%3A28253
Messerli, F. H., Bangalore, S., Bavishi, C., &Rimoldi, S. F. (2018). Angiotensin-converting
enzyme inhibitors in hypertension: to use or not to use?. Journal of the American
College of Cardiology, 71(13), 1474-1482.
http://www.onlinejacc.org/content/71/13/1474?
sso=1&sso_redirect_count=3&access_token=&intcmp=trendmd
12
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Mestrom, E., De Bie, A., van de Steeg, M., Driessen, M., Atallah, L., Bezemer, R., ... &
Korsten, E. (2019). Implementation of an automated early warning scoring system in
a surgical ward: Practical use and effects on patient outcomes. PloS one, 14(5).
https://journals.plos.org/plosone/article/file?type=printable&id=10.1371/
journal.pone.0213402
Mills, P. R., Weidmann, A. E., & Stewart, D. (2017). Hospital electronic prescribing system
implementation impact on discharge information communication and prescribing
errors: a before and after study. European journal of clinical pharmacology, 73(10),
1279-1286. https://doi.org/10.1007/s00228-017-2274-7
NSW Government. (2019). WSLHD Clinical Emergency Response Systems (CERS)
Framework. http://www.wslhd.health.nsw.gov.au/ArticleDocuments/2876/2019%20O
%20Week%20-%20DETECT%20-%20CERS.pdf.aspx
Osafo, N., Agyare, C., Obiri, D. D., &Antwi, A. O. (2017). Mechanism of action of
nonsteroidal anti-inflammatory drugs. Nonsteroidal Anti-Inflammatory Drugs, 1-15.
https://books.google.co.in/books?
hl=en&lr=&id=_eiPDwAAQBAJ&oi=fnd&pg=PA5&dq=nsaid+mechanism+of+actio
n&ots=Qfx-
RDzhC_&sig=j26AeHq96y_bhUvznHsQULaG6Uk#v=onepage&q=nsaid
%20mechanism%20of%20action&f=false
Parisien-La Salle, S., Rivest, E. A., Boucher, V. G., Lalande-Gauthier, M., Morisset, J.,
Manganas, H., ... & Dubé, B. P. (2019). Effects of pursed lip breathing on exercise
capacity and dyspnea in patients with interstitial lung disease: a randomized,
crossover study. Journal of cardiopulmonary rehabilitation and prevention, 39(2),
112-117.
13
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Korsten, E. (2019). Implementation of an automated early warning scoring system in
a surgical ward: Practical use and effects on patient outcomes. PloS one, 14(5).
https://journals.plos.org/plosone/article/file?type=printable&id=10.1371/
journal.pone.0213402
Mills, P. R., Weidmann, A. E., & Stewart, D. (2017). Hospital electronic prescribing system
implementation impact on discharge information communication and prescribing
errors: a before and after study. European journal of clinical pharmacology, 73(10),
1279-1286. https://doi.org/10.1007/s00228-017-2274-7
NSW Government. (2019). WSLHD Clinical Emergency Response Systems (CERS)
Framework. http://www.wslhd.health.nsw.gov.au/ArticleDocuments/2876/2019%20O
%20Week%20-%20DETECT%20-%20CERS.pdf.aspx
Osafo, N., Agyare, C., Obiri, D. D., &Antwi, A. O. (2017). Mechanism of action of
nonsteroidal anti-inflammatory drugs. Nonsteroidal Anti-Inflammatory Drugs, 1-15.
https://books.google.co.in/books?
hl=en&lr=&id=_eiPDwAAQBAJ&oi=fnd&pg=PA5&dq=nsaid+mechanism+of+actio
n&ots=Qfx-
RDzhC_&sig=j26AeHq96y_bhUvznHsQULaG6Uk#v=onepage&q=nsaid
%20mechanism%20of%20action&f=false
Parisien-La Salle, S., Rivest, E. A., Boucher, V. G., Lalande-Gauthier, M., Morisset, J.,
Manganas, H., ... & Dubé, B. P. (2019). Effects of pursed lip breathing on exercise
capacity and dyspnea in patients with interstitial lung disease: a randomized,
crossover study. Journal of cardiopulmonary rehabilitation and prevention, 39(2),
112-117.
13
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
https://journals.lww.com/jcrjournal/Abstract/2019/03000/Effects_of_Pursed_Lip_Bre
athing_on_Exercise.7.aspx
Pennisi, M. A., Bello, G., Congedo, M. T., Montini, L., Nachira, D., Ferretti, G. M., ...
&Margaritora, S. (2019). Early nasal high-flow versus Venturi mask oxygen therapy
after lung resection: a randomized trial. Critical Care, 23(1), 68.
https://doi.org/10.1186/s13054-019-2361-5
Ryan, S., Wiseman, P., Mannion, S., & O'Sullivan, M. (2018). Acute postoperative
compartment syndrome in a child receiving patient‐controlled analgesia and
peripheral nerve block. Anaesthesia Cases, 6(1), 45-47.
https://doi.org/10.21466/ac.APCSIAC.2018
Schnitzler, L., Smith, S. K., Shepherd, H. L., Shaw, J., Dong, S., Carpenter, D. M., ... &
Dhillon, H. M. (2017). Communication during radiation therapy education sessions:
The role of medical jargon and emotional support in clarifying patient
confusion. Patient education and counseling, 100(1), 112-120.
https://doi.org/10.1016/j.pec.2016.08.006
Smith, D., & Bowden, T. (2017). Using the ABCDE approach to assess the deteriorating
patient. Nursing Standard (2014+), 32(14), 51.
https://search.proquest.com/openview/4ac9f427a1259af55d2eb0de4594a09a/1?pq-
origsite=gscholar&cbl=2042228
Tarango, C., Dahale, D., Dodson, N., Otte, A., &Schoettker, P. J. (2018). Managing
paediatric bleeding disorder patients undergoing surgical procedures: Leveraging the
electronic medical record. Haemophilia, 24(4), e173-e178.
https://doi.org/10.1111/hae.13514
14
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
athing_on_Exercise.7.aspx
Pennisi, M. A., Bello, G., Congedo, M. T., Montini, L., Nachira, D., Ferretti, G. M., ...
&Margaritora, S. (2019). Early nasal high-flow versus Venturi mask oxygen therapy
after lung resection: a randomized trial. Critical Care, 23(1), 68.
https://doi.org/10.1186/s13054-019-2361-5
Ryan, S., Wiseman, P., Mannion, S., & O'Sullivan, M. (2018). Acute postoperative
compartment syndrome in a child receiving patient‐controlled analgesia and
peripheral nerve block. Anaesthesia Cases, 6(1), 45-47.
https://doi.org/10.21466/ac.APCSIAC.2018
Schnitzler, L., Smith, S. K., Shepherd, H. L., Shaw, J., Dong, S., Carpenter, D. M., ... &
Dhillon, H. M. (2017). Communication during radiation therapy education sessions:
The role of medical jargon and emotional support in clarifying patient
confusion. Patient education and counseling, 100(1), 112-120.
https://doi.org/10.1016/j.pec.2016.08.006
Smith, D., & Bowden, T. (2017). Using the ABCDE approach to assess the deteriorating
patient. Nursing Standard (2014+), 32(14), 51.
https://search.proquest.com/openview/4ac9f427a1259af55d2eb0de4594a09a/1?pq-
origsite=gscholar&cbl=2042228
Tarango, C., Dahale, D., Dodson, N., Otte, A., &Schoettker, P. J. (2018). Managing
paediatric bleeding disorder patients undergoing surgical procedures: Leveraging the
electronic medical record. Haemophilia, 24(4), e173-e178.
https://doi.org/10.1111/hae.13514
14
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Vatankhah, S., Sheikhi, R. A., Heidari, M., & Moradimajd, P. (2018). The relationship
between fluid resuscitation and intra-abdominal hypertension in patients with blunt
abdominal trauma. International journal of critical illness and injury science, 8(3),
149. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6116304/
15
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
between fluid resuscitation and intra-abdominal hypertension in patients with blunt
abdominal trauma. International journal of critical illness and injury science, 8(3),
149. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6116304/
15
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Appendix A: ISBAR Clinical Handover Table
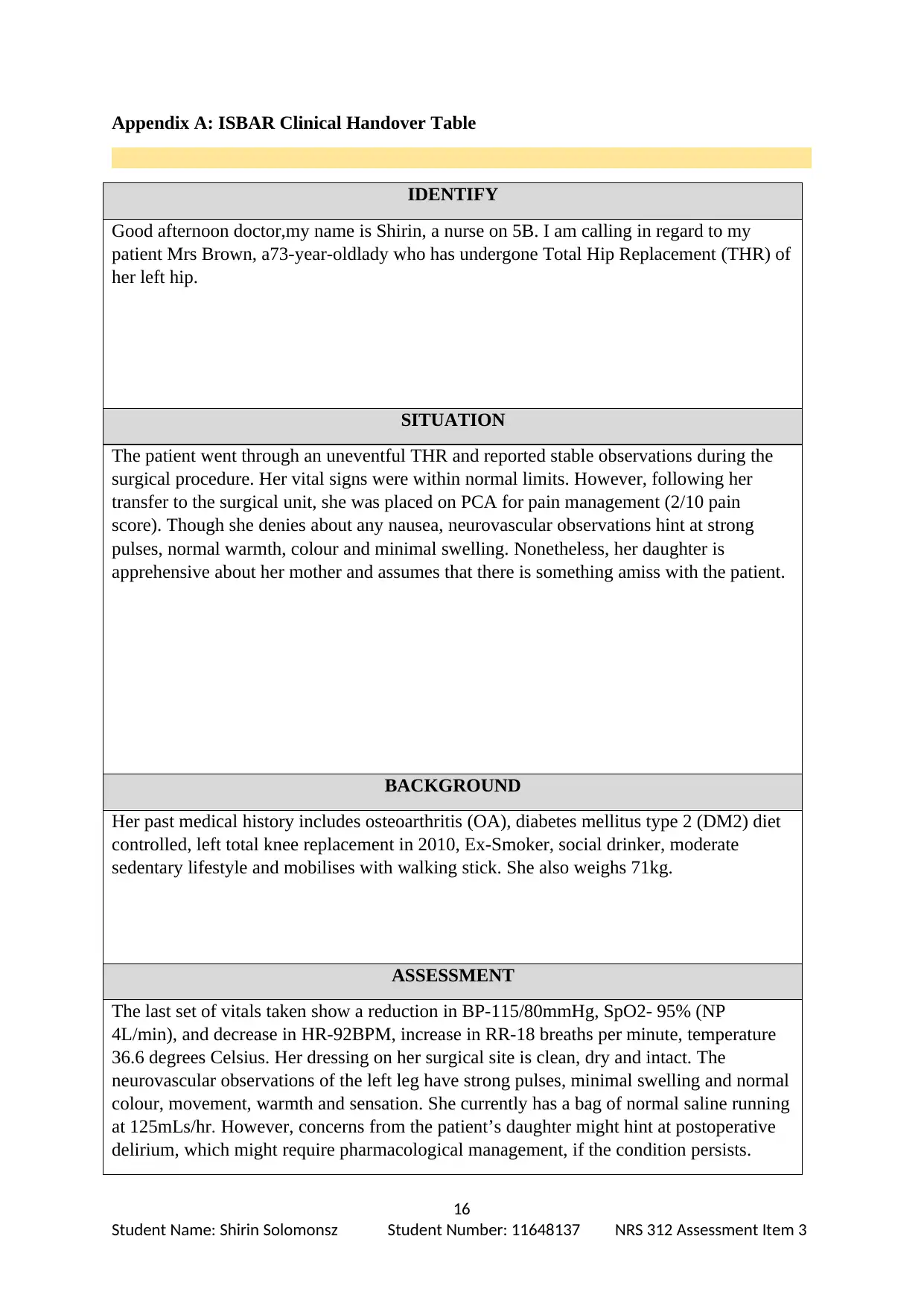
IDENTIFY
Good afternoon doctor,my name is Shirin, a nurse on 5B. I am calling in regard to my
patient Mrs Brown, a73-year-oldlady who has undergone Total Hip Replacement (THR) of
her left hip.
SITUATION
The patient went through an uneventful THR and reported stable observations during the
surgical procedure. Her vital signs were within normal limits. However, following her
transfer to the surgical unit, she was placed on PCA for pain management (2/10 pain
score). Though she denies about any nausea, neurovascular observations hint at strong
pulses, normal warmth, colour and minimal swelling. Nonetheless, her daughter is
apprehensive about her mother and assumes that there is something amiss with the patient.
BACKGROUND
Her past medical history includes osteoarthritis (OA), diabetes mellitus type 2 (DM2) diet
controlled, left total knee replacement in 2010, Ex-Smoker, social drinker, moderate
sedentary lifestyle and mobilises with walking stick. She also weighs 71kg.
ASSESSMENT
The last set of vitals taken show a reduction in BP-115/80mmHg, SpO2- 95% (NP
4L/min), and decrease in HR-92BPM, increase in RR-18 breaths per minute, temperature
36.6 degrees Celsius. Her dressing on her surgical site is clean, dry and intact. The
neurovascular observations of the left leg have strong pulses, minimal swelling and normal
colour, movement, warmth and sensation. She currently has a bag of normal saline running
at 125mLs/hr. However, concerns from the patient’s daughter might hint at postoperative
delirium, which might require pharmacological management, if the condition persists.
16
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
IDENTIFY
Good afternoon doctor,my name is Shirin, a nurse on 5B. I am calling in regard to my
patient Mrs Brown, a73-year-oldlady who has undergone Total Hip Replacement (THR) of
her left hip.
SITUATION
The patient went through an uneventful THR and reported stable observations during the
surgical procedure. Her vital signs were within normal limits. However, following her
transfer to the surgical unit, she was placed on PCA for pain management (2/10 pain
score). Though she denies about any nausea, neurovascular observations hint at strong
pulses, normal warmth, colour and minimal swelling. Nonetheless, her daughter is
apprehensive about her mother and assumes that there is something amiss with the patient.
BACKGROUND
Her past medical history includes osteoarthritis (OA), diabetes mellitus type 2 (DM2) diet
controlled, left total knee replacement in 2010, Ex-Smoker, social drinker, moderate
sedentary lifestyle and mobilises with walking stick. She also weighs 71kg.
ASSESSMENT
The last set of vitals taken show a reduction in BP-115/80mmHg, SpO2- 95% (NP
4L/min), and decrease in HR-92BPM, increase in RR-18 breaths per minute, temperature
36.6 degrees Celsius. Her dressing on her surgical site is clean, dry and intact. The
neurovascular observations of the left leg have strong pulses, minimal swelling and normal
colour, movement, warmth and sensation. She currently has a bag of normal saline running
at 125mLs/hr. However, concerns from the patient’s daughter might hint at postoperative
delirium, which might require pharmacological management, if the condition persists.
16
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
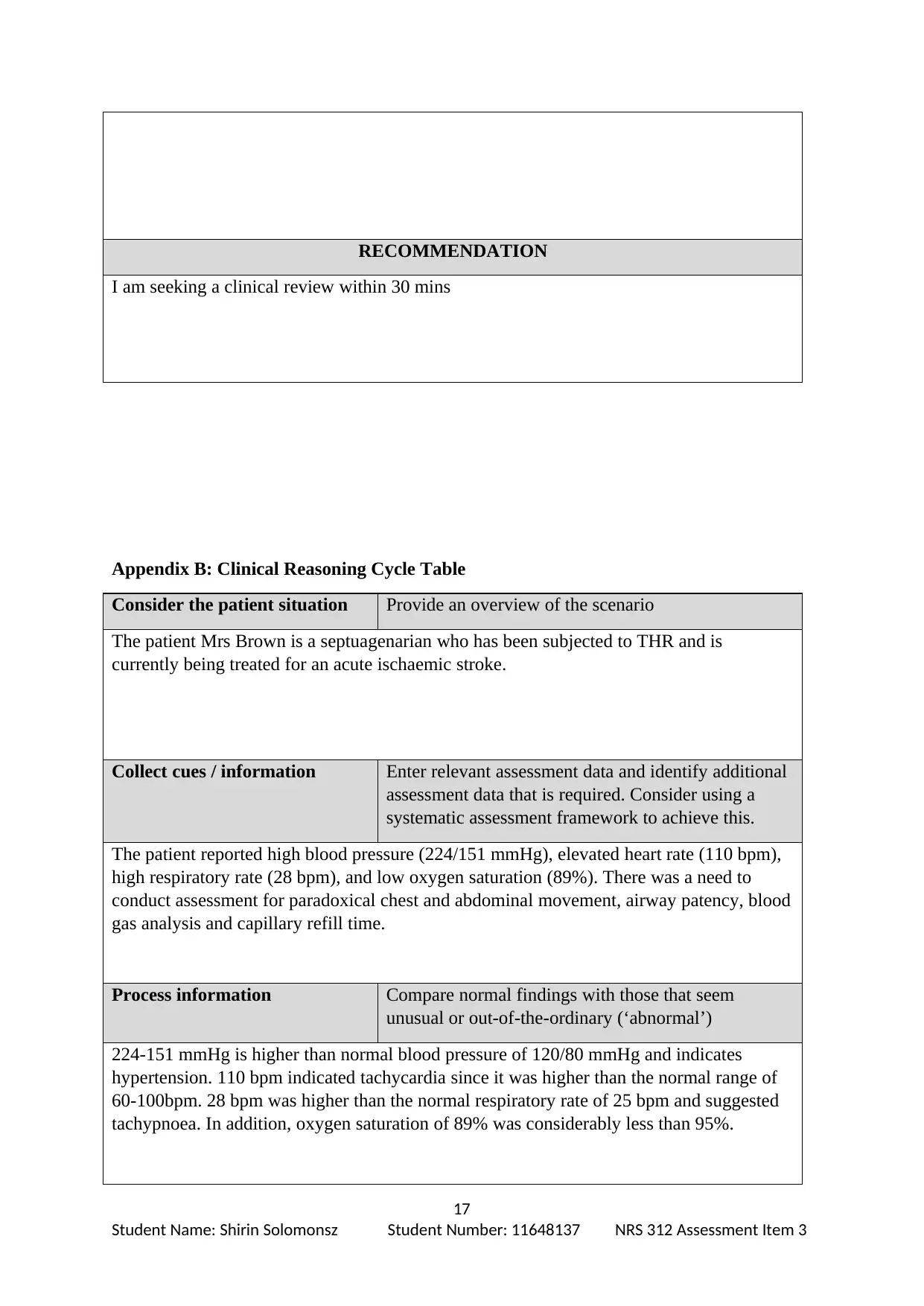
RECOMMENDATION
I am seeking a clinical review within 30 mins
Appendix B: Clinical Reasoning Cycle Table
Consider the patient situation Provide an overview of the scenario
The patient Mrs Brown is a septuagenarian who has been subjected to THR and is
currently being treated for an acute ischaemic stroke.
Collect cues / information Enter relevant assessment data and identify additional
assessment data that is required. Consider using a
systematic assessment framework to achieve this.
The patient reported high blood pressure (224/151 mmHg), elevated heart rate (110 bpm),
high respiratory rate (28 bpm), and low oxygen saturation (89%). There was a need to
conduct assessment for paradoxical chest and abdominal movement, airway patency, blood
gas analysis and capillary refill time.
Process information Compare normal findings with those that seem
unusual or out-of-the-ordinary (‘abnormal’)
224-151 mmHg is higher than normal blood pressure of 120/80 mmHg and indicates
hypertension. 110 bpm indicated tachycardia since it was higher than the normal range of
60-100bpm. 28 bpm was higher than the normal respiratory rate of 25 bpm and suggested
tachypnoea. In addition, oxygen saturation of 89% was considerably less than 95%.
17
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
I am seeking a clinical review within 30 mins
Appendix B: Clinical Reasoning Cycle Table
Consider the patient situation Provide an overview of the scenario
The patient Mrs Brown is a septuagenarian who has been subjected to THR and is
currently being treated for an acute ischaemic stroke.
Collect cues / information Enter relevant assessment data and identify additional
assessment data that is required. Consider using a
systematic assessment framework to achieve this.
The patient reported high blood pressure (224/151 mmHg), elevated heart rate (110 bpm),
high respiratory rate (28 bpm), and low oxygen saturation (89%). There was a need to
conduct assessment for paradoxical chest and abdominal movement, airway patency, blood
gas analysis and capillary refill time.
Process information Compare normal findings with those that seem
unusual or out-of-the-ordinary (‘abnormal’)
224-151 mmHg is higher than normal blood pressure of 120/80 mmHg and indicates
hypertension. 110 bpm indicated tachycardia since it was higher than the normal range of
60-100bpm. 28 bpm was higher than the normal respiratory rate of 25 bpm and suggested
tachypnoea. In addition, oxygen saturation of 89% was considerably less than 95%.
17
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
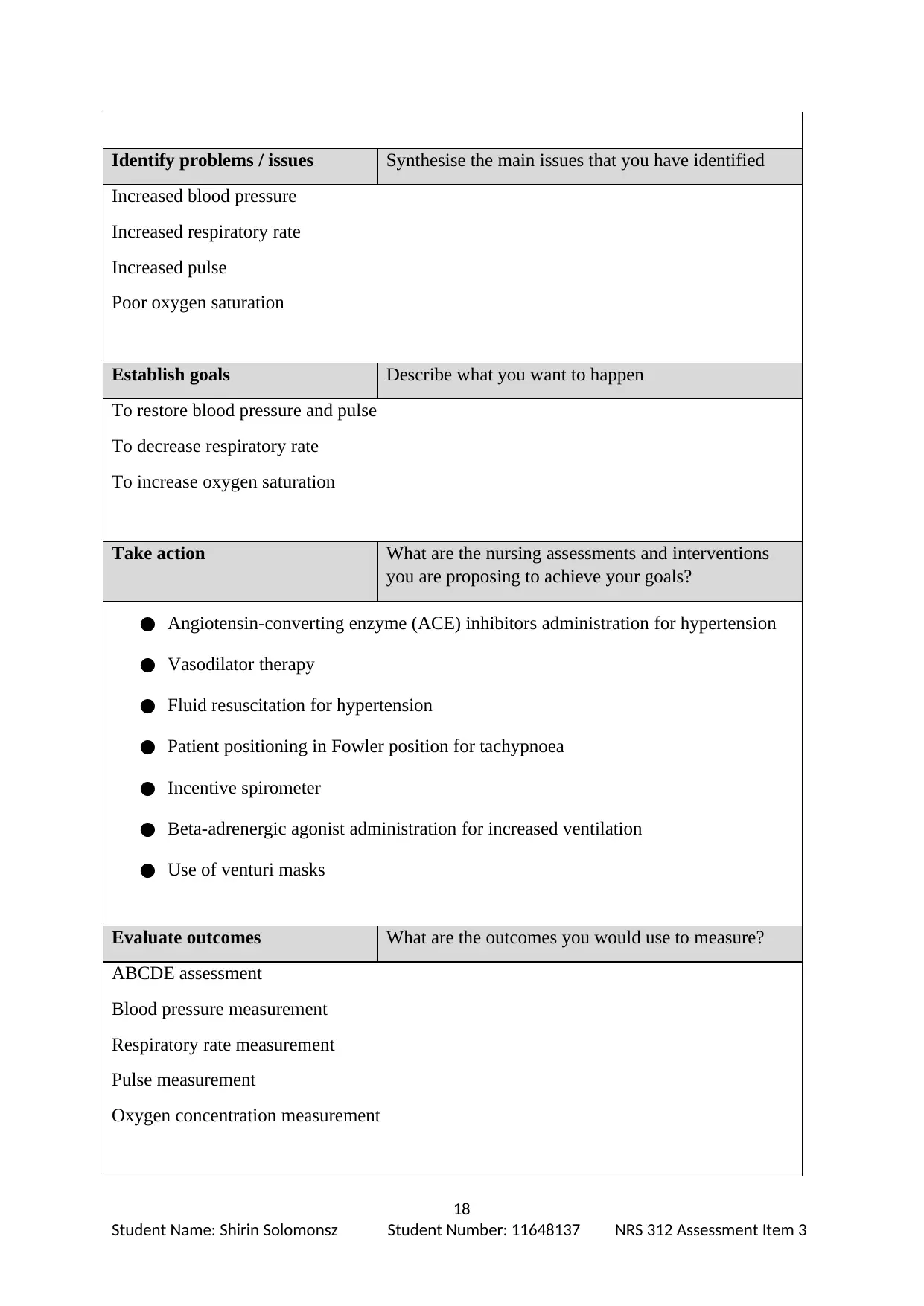
Identify problems / issues Synthesise the main issues that you have identified
Increased blood pressure
Increased respiratory rate
Increased pulse
Poor oxygen saturation
Establish goals Describe what you want to happen
To restore blood pressure and pulse
To decrease respiratory rate
To increase oxygen saturation
Take action What are the nursing assessments and interventions
you are proposing to achieve your goals?
● Angiotensin-converting enzyme (ACE) inhibitors administration for hypertension
● Vasodilator therapy
● Fluid resuscitation for hypertension
● Patient positioning in Fowler position for tachypnoea
● Incentive spirometer
● Beta-adrenergic agonist administration for increased ventilation
● Use of venturi masks
Evaluate outcomes What are the outcomes you would use to measure?
ABCDE assessment
Blood pressure measurement
Respiratory rate measurement
Pulse measurement
Oxygen concentration measurement
18
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
Increased blood pressure
Increased respiratory rate
Increased pulse
Poor oxygen saturation
Establish goals Describe what you want to happen
To restore blood pressure and pulse
To decrease respiratory rate
To increase oxygen saturation
Take action What are the nursing assessments and interventions
you are proposing to achieve your goals?
● Angiotensin-converting enzyme (ACE) inhibitors administration for hypertension
● Vasodilator therapy
● Fluid resuscitation for hypertension
● Patient positioning in Fowler position for tachypnoea
● Incentive spirometer
● Beta-adrenergic agonist administration for increased ventilation
● Use of venturi masks
Evaluate outcomes What are the outcomes you would use to measure?
ABCDE assessment
Blood pressure measurement
Respiratory rate measurement
Pulse measurement
Oxygen concentration measurement
18
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
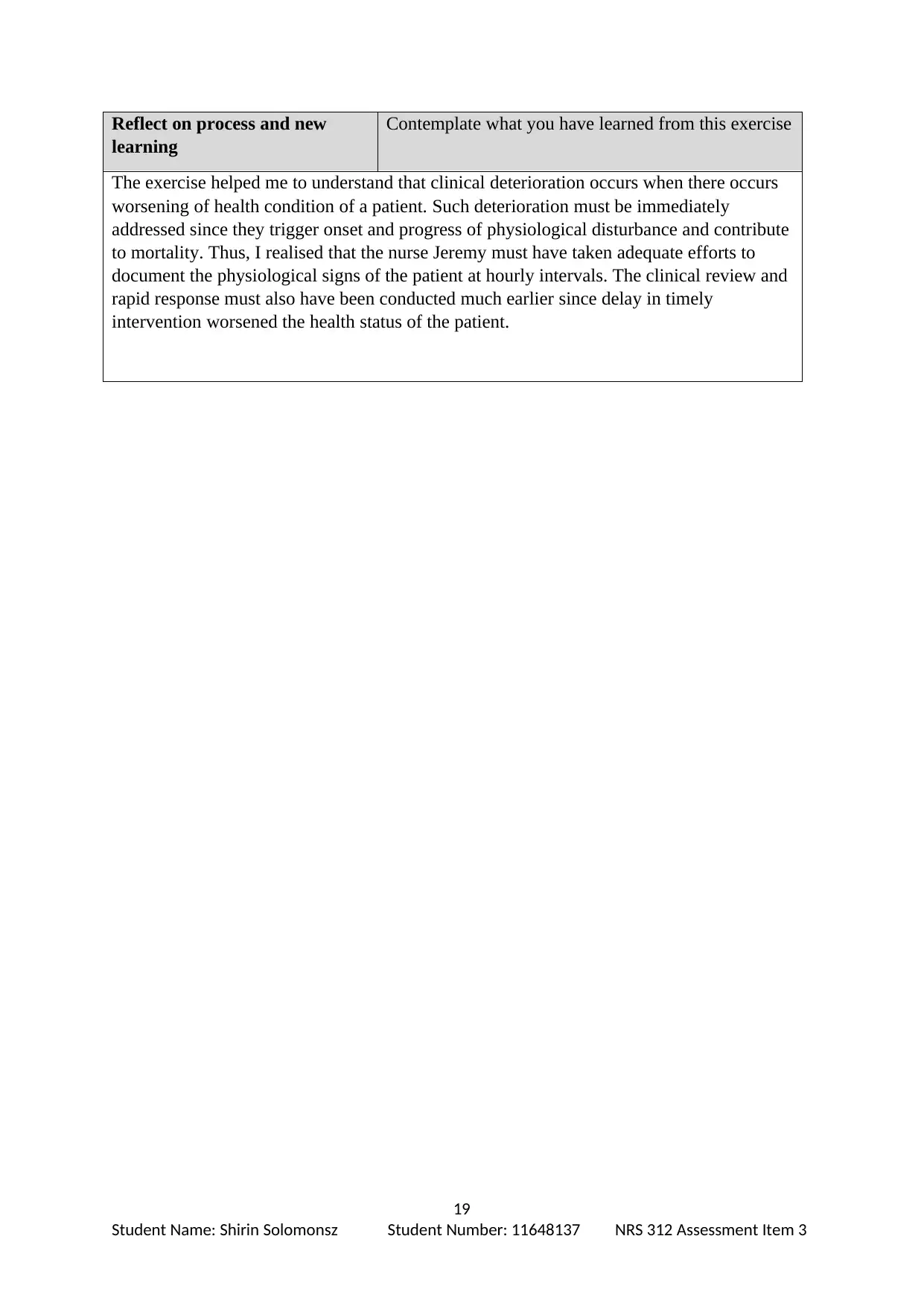
Reflect on process and new
learning
Contemplate what you have learned from this exercise
The exercise helped me to understand that clinical deterioration occurs when there occurs
worsening of health condition of a patient. Such deterioration must be immediately
addressed since they trigger onset and progress of physiological disturbance and contribute
to mortality. Thus, I realised that the nurse Jeremy must have taken adequate efforts to
document the physiological signs of the patient at hourly intervals. The clinical review and
rapid response must also have been conducted much earlier since delay in timely
intervention worsened the health status of the patient.
19
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
learning
Contemplate what you have learned from this exercise
The exercise helped me to understand that clinical deterioration occurs when there occurs
worsening of health condition of a patient. Such deterioration must be immediately
addressed since they trigger onset and progress of physiological disturbance and contribute
to mortality. Thus, I realised that the nurse Jeremy must have taken adequate efforts to
document the physiological signs of the patient at hourly intervals. The clinical review and
rapid response must also have been conducted much earlier since delay in timely
intervention worsened the health status of the patient.
19
Student Name: Shirin Solomonsz Student Number: 11648137 NRS 312 Assessment Item 3
1 out of 19
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.