Dissertation: Diabetes Patients' Challenges in Healthcare Access
VerifiedAdded on 2023/04/20
|33
|8804
|127
Thesis and Dissertation
AI Summary
This dissertation examines the significant challenges individuals with diabetes encounter when accessing information and medical care. It begins with an introduction to diabetes mellitus, its symptoms, complications, and management strategies. The research question focuses on identifying the main challenges diabetic patients face regarding information and care access. The study aims to determine these challenges and explore patient awareness of diabetes management. The methodology involves a systematic literature review, utilizing electronic databases (MEDLINE, CINAHL, EMBASE) and specific search terms. The inclusion and exclusion criteria are clearly defined, and the review process follows a structured approach. The findings highlight key barriers, including lack of patient knowledge and awareness, insufficient family and peer support, psychosocial issues, and socioeconomic factors. The discussion section analyzes these barriers, emphasizing the need for improved patient education and support. The conclusion underscores the importance of addressing these challenges to enhance the health and well-being of diabetes patients, with implications for future education campaigns and policy development. The dissertation also includes a detailed review of relevant literature, tables outlining inclusion and exclusion criteria, and a personal reflection on the research process.

Running head: DISSERTATION
What are the main challenges do people with diabetes face when accessing information and
medical care?
Name of the Student
Name of the University
Author Note
What are the main challenges do people with diabetes face when accessing information and
medical care?
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1DISSERTATION
Abstract
This dissertation aimed to explore what are the barriers that are faced by individuals with
diabetes, in relation to accessing information and clinical care services. Three electronic
databases MEDLINE, CINAHL, and EMBASE were sued to select 11 primary research
articles, from which four promising themes were identified: (i) lack of knowledge and
awareness among patients, (ii) lack of motivation and support from peers and family, (iii)
psychosocial issues related to diabetes self-management, and (iv) low educational attainment
and poor socioeconomic status of patients. On top of this, the dissertation indicated that there
are several misconceptions and stigma about diabetes in different cultures that hinder the care
seeking process. Thus, the provision of care giving must take into consideration the presence
of adequate awareness on the disease, in addition to the presence of necessary social and
financial support. Finally, the dissertation called for future formulation of education
campaigns and policies that would address the identified barriers and improve health and
wellbeing of diabetes patients.
Keywords: diabetes, barriers, management, access, care
Abstract
This dissertation aimed to explore what are the barriers that are faced by individuals with
diabetes, in relation to accessing information and clinical care services. Three electronic
databases MEDLINE, CINAHL, and EMBASE were sued to select 11 primary research
articles, from which four promising themes were identified: (i) lack of knowledge and
awareness among patients, (ii) lack of motivation and support from peers and family, (iii)
psychosocial issues related to diabetes self-management, and (iv) low educational attainment
and poor socioeconomic status of patients. On top of this, the dissertation indicated that there
are several misconceptions and stigma about diabetes in different cultures that hinder the care
seeking process. Thus, the provision of care giving must take into consideration the presence
of adequate awareness on the disease, in addition to the presence of necessary social and
financial support. Finally, the dissertation called for future formulation of education
campaigns and policies that would address the identified barriers and improve health and
wellbeing of diabetes patients.
Keywords: diabetes, barriers, management, access, care
2DISSERTATION
Table of Contents
Introduction................................................................................................................................3
Background............................................................................................................................3
Research question.......................................................................................................................5
Research aim..............................................................................................................................5
Research objectives....................................................................................................................5
Literature review methodology..................................................................................................6
Purpose statement...................................................................................................................6
Selection criteria.....................................................................................................................7
Search terms...........................................................................................................................7
Relevance assessment............................................................................................................8
Quality appraisal....................................................................................................................9
Results......................................................................................................................................10
Lack of knowledge and awareness among patients.............................................................10
Lack of support and motivation from family and peers.......................................................11
Educational attainment and socioeconomic condition of the patients.................................12
Psychosocial issues related to self-management of diabetes...............................................13
Discussion................................................................................................................................16
Conclusion................................................................................................................................20
Implications..........................................................................................................................21
References................................................................................................................................22
Appendices...............................................................................................................................27
Table of Contents
Introduction................................................................................................................................3
Background............................................................................................................................3
Research question.......................................................................................................................5
Research aim..............................................................................................................................5
Research objectives....................................................................................................................5
Literature review methodology..................................................................................................6
Purpose statement...................................................................................................................6
Selection criteria.....................................................................................................................7
Search terms...........................................................................................................................7
Relevance assessment............................................................................................................8
Quality appraisal....................................................................................................................9
Results......................................................................................................................................10
Lack of knowledge and awareness among patients.............................................................10
Lack of support and motivation from family and peers.......................................................11
Educational attainment and socioeconomic condition of the patients.................................12
Psychosocial issues related to self-management of diabetes...............................................13
Discussion................................................................................................................................16
Conclusion................................................................................................................................20
Implications..........................................................................................................................21
References................................................................................................................................22
Appendices...............................................................................................................................27
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3DISSERTATION
Introduction
Background
Commonly referred to as diabetes, diabetes mellitus is a metabolic disorder that is
characterized by increased blood sugar levels. Some of the common symptoms of diabetes
mellitus include increased thirst, frequent urination, and increase hunger. If not treated
properly, the condition can result in several health complications such as, hyperglycaemic
state, diabetic ketoacidosis, or even death (American Diabetes Association 2014). Other
serious complications comprise of stroke, cardiovascular disease, foot ulcer, chronic kidney
disease, and eye damage. The condition typically arises due to failure of the pancreas in
producing adequate insulin. It also occurs when the cells present in the body are not able to
respond appropriately to the amount of insulin that has been produced from the pancreas.
Three major types of diabetes mellitus are namely, (i) type 1, (ii) type 2, and (iii) gestational
diabetes (Macedo et al., 2014). The principal goal of diabetes management focuses on
restoring carbohydrate metabolism to normal levels. With the aim of accomplishing this goal,
people who suffer from an absolute deficiency of the hormone insulin, require external
insulin replacement therapy that is typically administered through insulin pump or injection.
Exercise and dietary modifications are other management strategies that help in combating
insulin resistance (Holt and Kumar 2015). Secondary goals of diabetes management focus on
preventing or delaying the onset of other co-morbid conditions.
The number of individuals who have been diagnosed with diabetes in the United
Kingdom has increased to 3.5 million in recent years from 1.4 million, as per records of 1996.
Taking into consideration the proportion of people who are likely to be residing with
undiagnosed diabetes in the UK, the number is expected to be as much as 4 million
Introduction
Background
Commonly referred to as diabetes, diabetes mellitus is a metabolic disorder that is
characterized by increased blood sugar levels. Some of the common symptoms of diabetes
mellitus include increased thirst, frequent urination, and increase hunger. If not treated
properly, the condition can result in several health complications such as, hyperglycaemic
state, diabetic ketoacidosis, or even death (American Diabetes Association 2014). Other
serious complications comprise of stroke, cardiovascular disease, foot ulcer, chronic kidney
disease, and eye damage. The condition typically arises due to failure of the pancreas in
producing adequate insulin. It also occurs when the cells present in the body are not able to
respond appropriately to the amount of insulin that has been produced from the pancreas.
Three major types of diabetes mellitus are namely, (i) type 1, (ii) type 2, and (iii) gestational
diabetes (Macedo et al., 2014). The principal goal of diabetes management focuses on
restoring carbohydrate metabolism to normal levels. With the aim of accomplishing this goal,
people who suffer from an absolute deficiency of the hormone insulin, require external
insulin replacement therapy that is typically administered through insulin pump or injection.
Exercise and dietary modifications are other management strategies that help in combating
insulin resistance (Holt and Kumar 2015). Secondary goals of diabetes management focus on
preventing or delaying the onset of other co-morbid conditions.
The number of individuals who have been diagnosed with diabetes in the United
Kingdom has increased to 3.5 million in recent years from 1.4 million, as per records of 1996.
Taking into consideration the proportion of people who are likely to be residing with
undiagnosed diabetes in the UK, the number is expected to be as much as 4 million
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4DISSERTATION
(Diabetes.co.uk 2018). The prevalence of diabetes in the UK is estimated to increase to
roughly 5 million by the year 2025, with prevalence and incidence of type 2 diabetes
increasing at a rapid rate. Hence, recent records suggest that roughly 6% of the entire UK
population, which accounts for one in 16 people, have diabetes which is either diagnosed or
undiagnosed. Higher prevalence of this metabolic syndrome is found in England, followed by
Scotland, Wales, and Northern Ireland. According to reports from the International Diabetes
Federation, the top five nations that have greatest proportion of individuals with diabetes are
namely, China, India, the USA, Brazil, and the Russian Federation, with 109, 69, 29, 14, and
12 million people, respectively (Atlas 2015).
Patient access to appropriate healthcare amenities set the foundation for all client
interactions with the healthcare industry, as defined by Penchansky and Thomas's Theory of
Access (Usher 2015). According to Menke et al. (2015) under circumstances when patients
are not able to access appropriate healthcare services, it becomes impossible to receive
appropriate facilities, build therapeutic relationship with the providers, and accomplish
overall wellness and health. Despite the growing importance of access to healthcare, it has
not yet become a reality for several people residing across the nation. Apart from troubles in
reaching the clinician centres, and appointment availability issues, several challenges are
associated with patient care access, which hinder the process of self-health management.
There is mounting evidence for the fact that problems with the existing medical infrastructure
and socioeconomic status play an important role in preventing hassle free delivery of diabetes
care services (Kivimäki et al. 2015). Failure of the healthcare providers in accurately
monitoring the diabetic patients, and considering them for follow-up also makes the patient
encounter several challenges. Unhealthy food habits, lack of physical exercise, obesity,
urbanisation and population growth are the primary reasons for the ever-increasing
pervasiveness of diabetes. Lack of knowledge among patients about diabetes mellitus also
(Diabetes.co.uk 2018). The prevalence of diabetes in the UK is estimated to increase to
roughly 5 million by the year 2025, with prevalence and incidence of type 2 diabetes
increasing at a rapid rate. Hence, recent records suggest that roughly 6% of the entire UK
population, which accounts for one in 16 people, have diabetes which is either diagnosed or
undiagnosed. Higher prevalence of this metabolic syndrome is found in England, followed by
Scotland, Wales, and Northern Ireland. According to reports from the International Diabetes
Federation, the top five nations that have greatest proportion of individuals with diabetes are
namely, China, India, the USA, Brazil, and the Russian Federation, with 109, 69, 29, 14, and
12 million people, respectively (Atlas 2015).
Patient access to appropriate healthcare amenities set the foundation for all client
interactions with the healthcare industry, as defined by Penchansky and Thomas's Theory of
Access (Usher 2015). According to Menke et al. (2015) under circumstances when patients
are not able to access appropriate healthcare services, it becomes impossible to receive
appropriate facilities, build therapeutic relationship with the providers, and accomplish
overall wellness and health. Despite the growing importance of access to healthcare, it has
not yet become a reality for several people residing across the nation. Apart from troubles in
reaching the clinician centres, and appointment availability issues, several challenges are
associated with patient care access, which hinder the process of self-health management.
There is mounting evidence for the fact that problems with the existing medical infrastructure
and socioeconomic status play an important role in preventing hassle free delivery of diabetes
care services (Kivimäki et al. 2015). Failure of the healthcare providers in accurately
monitoring the diabetic patients, and considering them for follow-up also makes the patient
encounter several challenges. Unhealthy food habits, lack of physical exercise, obesity,
urbanisation and population growth are the primary reasons for the ever-increasing
pervasiveness of diabetes. Lack of knowledge among patients about diabetes mellitus also
5DISSERTATION
hinders their capability to effectively manage the illness (Deepa et al. 2014). Awareness
levels typically increase with education, and patients having greater educational attainment
have better knowledge that the metabolic syndrome is preventable. According to Mumu et al.
(2014) major challenge is also associated with the fact that patients do not have adequate
information about the risk factors that can aggravate their health condition, and result in the
onset of several co-morbidities. One major aspect of diabetes management and care is
satisfactory treatment and timely diagnosis, in the absence of which several co-morbidity and
complications can arise drastically. Access and availability to diabetes drug is another
feature. Not all people who have been affected with this condition are able to access anti-
diabetic pharmaceutical agents. Additional administration of insulin is also delayed in several
patients, until it becomes absolutely necessary to externally administer the hormone, for
keeping a check on the deteriorating HbA1C levels. This calls for the need of conducting a
research in determining the challenges faced.
Research question
What main challenges do people with diabetes face when accessing information and
medical care?
Research aim
To determine the challenges that people suffering from diabetes encounter, while
accessing medical care and health information.
Research objectives
To determine the barriers faced by patients
To explore the awareness of diabetes management and care among patients
hinders their capability to effectively manage the illness (Deepa et al. 2014). Awareness
levels typically increase with education, and patients having greater educational attainment
have better knowledge that the metabolic syndrome is preventable. According to Mumu et al.
(2014) major challenge is also associated with the fact that patients do not have adequate
information about the risk factors that can aggravate their health condition, and result in the
onset of several co-morbidities. One major aspect of diabetes management and care is
satisfactory treatment and timely diagnosis, in the absence of which several co-morbidity and
complications can arise drastically. Access and availability to diabetes drug is another
feature. Not all people who have been affected with this condition are able to access anti-
diabetic pharmaceutical agents. Additional administration of insulin is also delayed in several
patients, until it becomes absolutely necessary to externally administer the hormone, for
keeping a check on the deteriorating HbA1C levels. This calls for the need of conducting a
research in determining the challenges faced.
Research question
What main challenges do people with diabetes face when accessing information and
medical care?
Research aim
To determine the challenges that people suffering from diabetes encounter, while
accessing medical care and health information.
Research objectives
To determine the barriers faced by patients
To explore the awareness of diabetes management and care among patients
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6DISSERTATION
Literature review methodology
Systematic reviews have the potential advantage of providing objective summaries of
information that has already been published in written, about several research topics. This is
particularly valuable in wide research domains, where there exist several publications, each
of which focus on a narrow facet of the phenomenon under investigation. While traditional
reviews encompass publications that discuss and describe the state of science, of a particular
theme on topic from a contextual and theoretical point of view, systematic reviews have the
primary objective of providing a comprehensive overview of research that has been
conducted in that specific domain, until the current date (Peters et al. 2015). Hence, a
systematic review was conducted with the use of rigorous methodological approaches, for
identifying scholarly articles that contain information on the challenges that people face, in
relation to diabetes care and management.
With the aim of conducting a literature review on the aforementioned topic, a three-
stage procedure was formulated that encompassed (i) planning, (ii) conducting, and (iii)
reporting. The planning phase comprised of forming a review panel that consisted of two
independent experts in the particular domain. The structured approach that was followed
while conducting the systematic review was based on the 12-step framework proposed by
Kable, Pich and Maslin-Prothero (2012). A comprehensive documentation of the search
strategy helped in providing a clear explanation for the focus and rationale of the review.
The Framework also provided guidance through the strategy development and helped in
ensuring that no essential aspects were left out.
Literature review methodology
Systematic reviews have the potential advantage of providing objective summaries of
information that has already been published in written, about several research topics. This is
particularly valuable in wide research domains, where there exist several publications, each
of which focus on a narrow facet of the phenomenon under investigation. While traditional
reviews encompass publications that discuss and describe the state of science, of a particular
theme on topic from a contextual and theoretical point of view, systematic reviews have the
primary objective of providing a comprehensive overview of research that has been
conducted in that specific domain, until the current date (Peters et al. 2015). Hence, a
systematic review was conducted with the use of rigorous methodological approaches, for
identifying scholarly articles that contain information on the challenges that people face, in
relation to diabetes care and management.
With the aim of conducting a literature review on the aforementioned topic, a three-
stage procedure was formulated that encompassed (i) planning, (ii) conducting, and (iii)
reporting. The planning phase comprised of forming a review panel that consisted of two
independent experts in the particular domain. The structured approach that was followed
while conducting the systematic review was based on the 12-step framework proposed by
Kable, Pich and Maslin-Prothero (2012). A comprehensive documentation of the search
strategy helped in providing a clear explanation for the focus and rationale of the review.
The Framework also provided guidance through the strategy development and helped in
ensuring that no essential aspects were left out.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7DISSERTATION
Purpose statement
The purpose was formulated under the guidance of the project supervisor. The
purpose was stipulated as exploring the challenges that People suffering from diabetes have
to encounter while accessing information and medical care.
Selection criteria
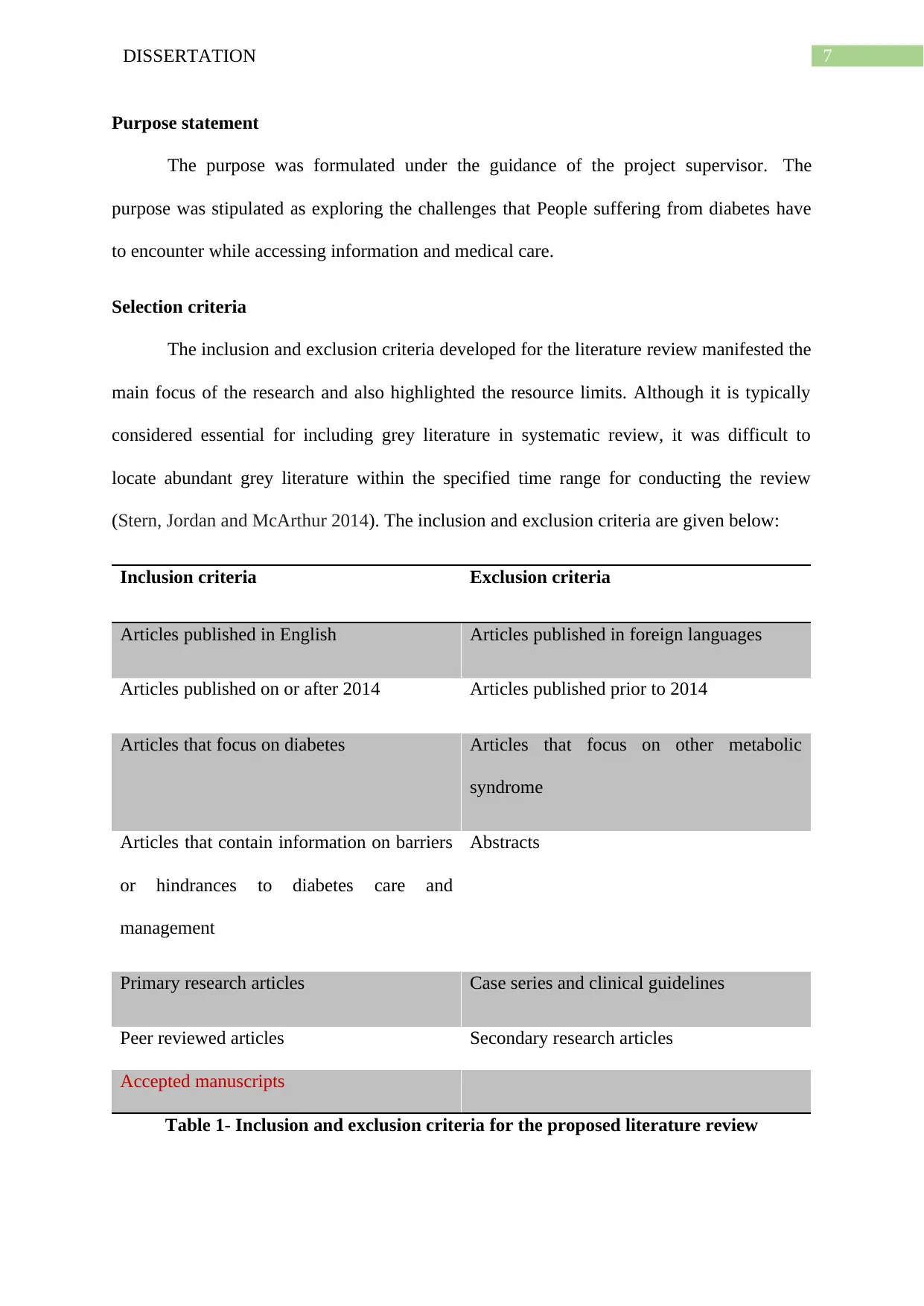
The inclusion and exclusion criteria developed for the literature review manifested the
main focus of the research and also highlighted the resource limits. Although it is typically
considered essential for including grey literature in systematic review, it was difficult to
locate abundant grey literature within the specified time range for conducting the review
(Stern, Jordan and McArthur 2014). The inclusion and exclusion criteria are given below:
Inclusion criteria Exclusion criteria
Articles published in English Articles published in foreign languages
Articles published on or after 2014 Articles published prior to 2014
Articles that focus on diabetes Articles that focus on other metabolic
syndrome
Articles that contain information on barriers
or hindrances to diabetes care and
management
Abstracts
Primary research articles Case series and clinical guidelines
Peer reviewed articles Secondary research articles
Accepted manuscripts
Table 1- Inclusion and exclusion criteria for the proposed literature review
Purpose statement
The purpose was formulated under the guidance of the project supervisor. The
purpose was stipulated as exploring the challenges that People suffering from diabetes have
to encounter while accessing information and medical care.
Selection criteria
The inclusion and exclusion criteria developed for the literature review manifested the
main focus of the research and also highlighted the resource limits. Although it is typically
considered essential for including grey literature in systematic review, it was difficult to
locate abundant grey literature within the specified time range for conducting the review
(Stern, Jordan and McArthur 2014). The inclusion and exclusion criteria are given below:
Inclusion criteria Exclusion criteria
Articles published in English Articles published in foreign languages
Articles published on or after 2014 Articles published prior to 2014
Articles that focus on diabetes Articles that focus on other metabolic
syndrome
Articles that contain information on barriers
or hindrances to diabetes care and
management
Abstracts
Primary research articles Case series and clinical guidelines
Peer reviewed articles Secondary research articles
Accepted manuscripts
Table 1- Inclusion and exclusion criteria for the proposed literature review
8DISSERTATION
Search terms
The second stage of conducting the literature review comprised of formulation of
search terms, on the basis of discussions and scoping studies within the panel. While
developing suitable search terms that would help in extraction of literature that were pertinent
to the research question, the 2009 guideline by the Centre for Reviews and Dissemination’s
(CRD) was taken into consideration, which provided the suggestion for consulting the
principal research question (Zeng et al. 2015). As per the guideline, abbreviations, spelling
variance, and synonyms were considered. MEDLINE, CINAHL, and EMBASE electronic
databases were extensively searched for retrieving articles.
The reference lists of the articles were also manually searched, thus utilizing the
procedure of snowballing. Hand searching the bibliography of the articles and consulting the
citation analysis, helped in discovering studies that were relatable to the review. The search
terms used were “diabetes”, “care”, “management”, “barriers”, “challenges”, “hindrances”,
“people”, “access”, “information”, and “patients” that were combined with boolean operators
AND, NOT and OR (McGowan et al. 2016).
Relevance assessment
Followed by retrieval of several articles from the electronic databases, bibliography
search and citation analysis, the PRISMA (Preferred Reporting Items for Systematic Reviews
and Meta-Analyses) was used for determining relevance of the retrieved scholarly literature,
at the end of search process (Moher et al. 2015). The articles were evaluated in a three-stage
process by assessing them against the criteria. Initially all the titles of the obtained hits were
evaluated, which had the potential advantage of the fact that the literature, which did not meet
the rational of the intended research, could be eliminated within a comparatively short period
of time. Under circumstances when the article title had limited information for judging its
relevance, it was included within the list. All the steps were conducted separately by two
Search terms
The second stage of conducting the literature review comprised of formulation of
search terms, on the basis of discussions and scoping studies within the panel. While
developing suitable search terms that would help in extraction of literature that were pertinent
to the research question, the 2009 guideline by the Centre for Reviews and Dissemination’s
(CRD) was taken into consideration, which provided the suggestion for consulting the
principal research question (Zeng et al. 2015). As per the guideline, abbreviations, spelling
variance, and synonyms were considered. MEDLINE, CINAHL, and EMBASE electronic
databases were extensively searched for retrieving articles.
The reference lists of the articles were also manually searched, thus utilizing the
procedure of snowballing. Hand searching the bibliography of the articles and consulting the
citation analysis, helped in discovering studies that were relatable to the review. The search
terms used were “diabetes”, “care”, “management”, “barriers”, “challenges”, “hindrances”,
“people”, “access”, “information”, and “patients” that were combined with boolean operators
AND, NOT and OR (McGowan et al. 2016).
Relevance assessment
Followed by retrieval of several articles from the electronic databases, bibliography
search and citation analysis, the PRISMA (Preferred Reporting Items for Systematic Reviews
and Meta-Analyses) was used for determining relevance of the retrieved scholarly literature,
at the end of search process (Moher et al. 2015). The articles were evaluated in a three-stage
process by assessing them against the criteria. Initially all the titles of the obtained hits were
evaluated, which had the potential advantage of the fact that the literature, which did not meet
the rational of the intended research, could be eliminated within a comparatively short period
of time. Under circumstances when the article title had limited information for judging its
relevance, it was included within the list. All the steps were conducted separately by two
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9DISSERTATION
individual researchers, following which disagreements were resolved by participating in
group discussions that resulted in refinement of the search criteria (Booth 2016). The initial
hits of 103 articles were decreased to 58.
The second screening step comprised of reading and assessing the abstract of all 58
articles against the formulated criteria and duplicate removal. Complete articles with less
informative abstracts were also added to the list. At the end of the second screening phase,
roughly 24 scholarly literatures remained. The third screening phase was conducted by
determining the full text eligibility of the articles. This resulted in exclusion of 13 articles
from the analysis in the final step, thereby leading to a final batch of 11 articles that were
included in this review. Resource and time limitation of the systematic review did not permit
for complete inclusion of other researches for assessing representativeness of the included
articles. This makes the systematic review slightly vulnerable of being subjectively biased,
thus not completely providing a representative overview of the contemporary status of
investigation. While a complete representative review is typically needed and aspired by
science, this paper will provide other researchers the foundation for imitating the research
procedure, and assessing its findings. My personal values initially influenced the decision of
formulating search terms since I wanted to focus on barriers that are generally faced by
people with diabetes in the UK. However, a discussion with my supervisor helped me
understand that restricting the review population to the UK would prevent generalizability of
our findings and would also decrease representativeness of the results we obtained. Appendix
A contains the PRISMA flowchart.
Quality appraisal
At the end of determining the relevance of the included article, all 11 literatures were
thoroughly analysed and appraised, for ensuring reliability of the information reported in
individual researchers, following which disagreements were resolved by participating in
group discussions that resulted in refinement of the search criteria (Booth 2016). The initial
hits of 103 articles were decreased to 58.
The second screening step comprised of reading and assessing the abstract of all 58
articles against the formulated criteria and duplicate removal. Complete articles with less
informative abstracts were also added to the list. At the end of the second screening phase,
roughly 24 scholarly literatures remained. The third screening phase was conducted by
determining the full text eligibility of the articles. This resulted in exclusion of 13 articles
from the analysis in the final step, thereby leading to a final batch of 11 articles that were
included in this review. Resource and time limitation of the systematic review did not permit
for complete inclusion of other researches for assessing representativeness of the included
articles. This makes the systematic review slightly vulnerable of being subjectively biased,
thus not completely providing a representative overview of the contemporary status of
investigation. While a complete representative review is typically needed and aspired by
science, this paper will provide other researchers the foundation for imitating the research
procedure, and assessing its findings. My personal values initially influenced the decision of
formulating search terms since I wanted to focus on barriers that are generally faced by
people with diabetes in the UK. However, a discussion with my supervisor helped me
understand that restricting the review population to the UK would prevent generalizability of
our findings and would also decrease representativeness of the results we obtained. Appendix
A contains the PRISMA flowchart.
Quality appraisal
At the end of determining the relevance of the included article, all 11 literatures were
thoroughly analysed and appraised, for ensuring reliability of the information reported in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10DISSERTATION
them. Their internal and external validity, findings, and relevance to the current research were
also determined.
them. Their internal and external validity, findings, and relevance to the current research were
also determined.
11DISSERTATION
Results
The 11 studies that were included in the qualitative data synthesis resulted in the
identification of four major themes. Of the 11 studies that were included, three were
quantitative and focused on questionnaires and surveys as the data collection tools, following
which the responses of the patients were statistically represented. The rest eight studies were
based on qualitative research design and included surveys, focus groups, semi-structured
interviews or a combination of both. The most frequently occurring and noticeable themes
comprised of (i) lack of knowledge and awareness of diabetes management and care services,
(ii) lack of support and motivation from family and peers, (iii) psychosocial issues associated
with self-management of diabetes, and (iv) poor socioeconomic status and educational
attainment of the patients.
Lack of knowledge and awareness among patients
Sufficient knowledge was also associated with accurate medication taking, exercise,
diet, foot care and blood glucose monitoring. Booth et al. (2013) and Hu et al. (2013) stressed
on the fact that low levels of understanding among diabetes patients and their family
members often resulted in their failure in realising the management steps that they should
adopt. Additionally, vast amount of information on diabetes care also confused the patients in
adequately seeking care services and maintaining blood glucose levels. This was in
accordance to the findings presented by Sina, Graffy and Simmons (2018) who suggested that
patients often have inadequate knowledge about diabetes management and its allied care
services. On conducting a statistical analysis they reported that 408 and 340 patients with no
reported diabetes complications cited lack of awareness on diabetes and diabetes service as
the major barrier to proper healthcare, respectively. In addition, 355 people who reported
diabetes complications also identified poor diabetes knowledge as a major barrier in self-care
and management.
Results
The 11 studies that were included in the qualitative data synthesis resulted in the
identification of four major themes. Of the 11 studies that were included, three were
quantitative and focused on questionnaires and surveys as the data collection tools, following
which the responses of the patients were statistically represented. The rest eight studies were
based on qualitative research design and included surveys, focus groups, semi-structured
interviews or a combination of both. The most frequently occurring and noticeable themes
comprised of (i) lack of knowledge and awareness of diabetes management and care services,
(ii) lack of support and motivation from family and peers, (iii) psychosocial issues associated
with self-management of diabetes, and (iv) poor socioeconomic status and educational
attainment of the patients.
Lack of knowledge and awareness among patients
Sufficient knowledge was also associated with accurate medication taking, exercise,
diet, foot care and blood glucose monitoring. Booth et al. (2013) and Hu et al. (2013) stressed
on the fact that low levels of understanding among diabetes patients and their family
members often resulted in their failure in realising the management steps that they should
adopt. Additionally, vast amount of information on diabetes care also confused the patients in
adequately seeking care services and maintaining blood glucose levels. This was in
accordance to the findings presented by Sina, Graffy and Simmons (2018) who suggested that
patients often have inadequate knowledge about diabetes management and its allied care
services. On conducting a statistical analysis they reported that 408 and 340 patients with no
reported diabetes complications cited lack of awareness on diabetes and diabetes service as
the major barrier to proper healthcare, respectively. In addition, 355 people who reported
diabetes complications also identified poor diabetes knowledge as a major barrier in self-care
and management.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 33
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.