Assignment On Employs A Cross Sectional Study Design
VerifiedAdded on 2022/10/06
|9
|1878
|24
Assignment
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: EPIDEMIOLOGY
EPIDEMIOLOGY
Name of the Student
Name of the University
Author Note
EPIDEMIOLOGY
Name of the Student
Name of the University
Author Note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1EPIDEMIOLOGY
Question 1:
(a) The paper employs a cross-sectional study design. Considering the fact that this is a cross
sectional study design, this paper evaluates the exposure and outcomes of the participants
observed at the same time.
STATA 13.0 (Software for Statistics and Data Sciences) was used to calculate the
sample size. This STATA 13.0 as a data collection tool applied WHO questionnaire for
studying domestic violence in Vietnam (Wassertheil-Smoller & Smoller, 2015).
(b) The main outcomes of this study include organising interview of the participants as well
as identifying the exposure to domestic violence in Vietnam. Mean as well as standard
deviation were calculated. The study had been divided into four different parts. These four
parts were domestic violence, sexual violence, emotional violence and physical violence. The
percentage as well as frequencies of the affected participants were statistically tabulated.
Another significant outcome of this study included a statistical representation of
women to domestic violence in Vietnam. This study is also depicted a significant relation
between domestic violence and low weight neonates (Vachhani et al., 2017).
(c) Considering the fact that this study is a cross-sectional study, it is noteworthy to state that
the risk of selection bias is low. Selection bias is defined as the process of selection of the
group of individuals for a study where significant randomisation at the time of data collection
as well as result interpretation is not performed. Here, out of 24 districts 10 districts were
selected randomly.
Question 1:
(a) The paper employs a cross-sectional study design. Considering the fact that this is a cross
sectional study design, this paper evaluates the exposure and outcomes of the participants
observed at the same time.
STATA 13.0 (Software for Statistics and Data Sciences) was used to calculate the
sample size. This STATA 13.0 as a data collection tool applied WHO questionnaire for
studying domestic violence in Vietnam (Wassertheil-Smoller & Smoller, 2015).
(b) The main outcomes of this study include organising interview of the participants as well
as identifying the exposure to domestic violence in Vietnam. Mean as well as standard
deviation were calculated. The study had been divided into four different parts. These four
parts were domestic violence, sexual violence, emotional violence and physical violence. The
percentage as well as frequencies of the affected participants were statistically tabulated.
Another significant outcome of this study included a statistical representation of
women to domestic violence in Vietnam. This study is also depicted a significant relation
between domestic violence and low weight neonates (Vachhani et al., 2017).
(c) Considering the fact that this study is a cross-sectional study, it is noteworthy to state that
the risk of selection bias is low. Selection bias is defined as the process of selection of the
group of individuals for a study where significant randomisation at the time of data collection
as well as result interpretation is not performed. Here, out of 24 districts 10 districts were
selected randomly.
2EPIDEMIOLOGY
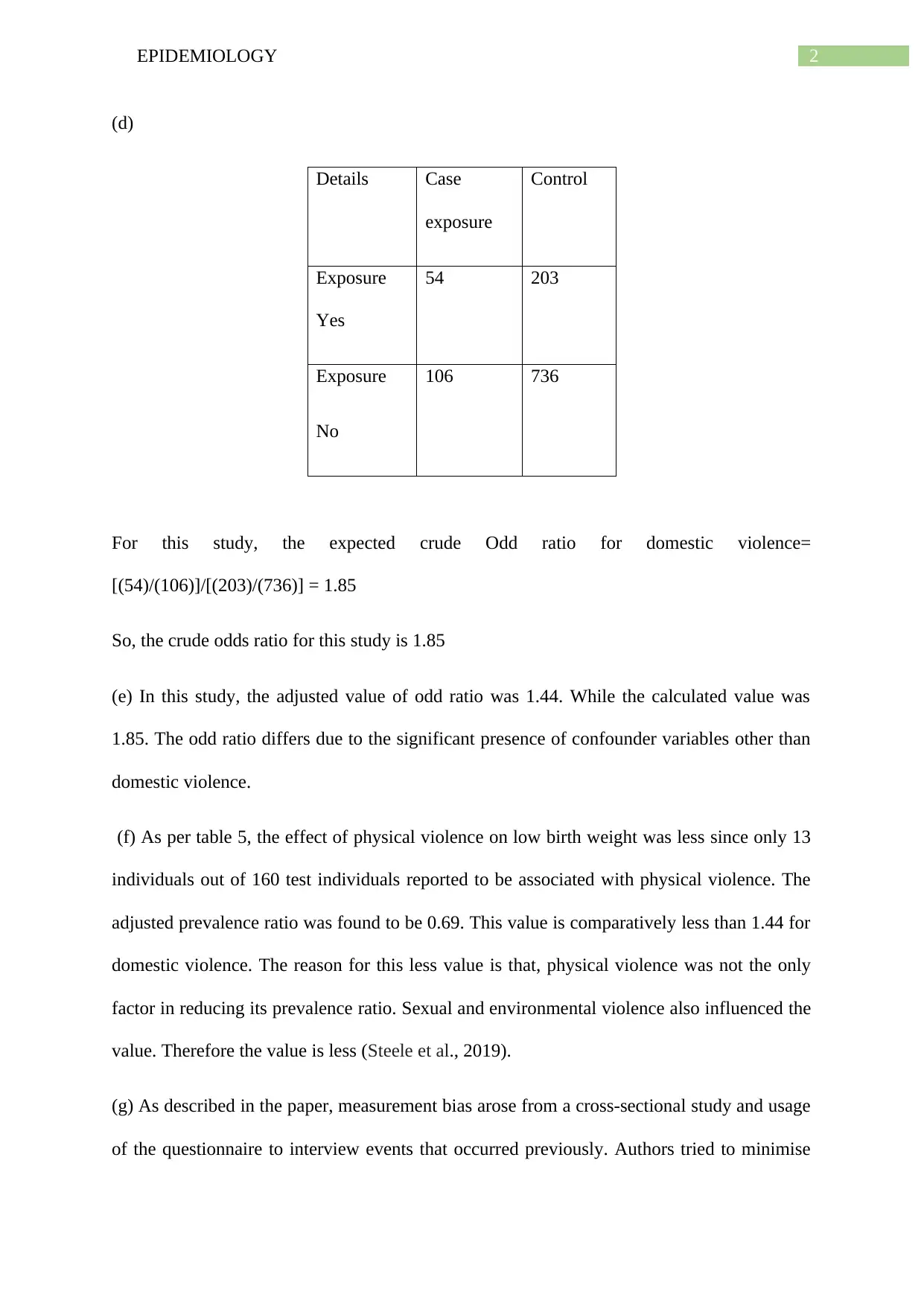
(d)
Details Case
exposure
Control
Exposure
Yes
54 203
Exposure
No
106 736
For this study, the expected crude Odd ratio for domestic violence=
[(54)/(106)]/[(203)/(736)] = 1.85
So, the crude odds ratio for this study is 1.85
(e) In this study, the adjusted value of odd ratio was 1.44. While the calculated value was
1.85. The odd ratio differs due to the significant presence of confounder variables other than
domestic violence.
(f) As per table 5, the effect of physical violence on low birth weight was less since only 13
individuals out of 160 test individuals reported to be associated with physical violence. The
adjusted prevalence ratio was found to be 0.69. This value is comparatively less than 1.44 for
domestic violence. The reason for this less value is that, physical violence was not the only
factor in reducing its prevalence ratio. Sexual and environmental violence also influenced the
value. Therefore the value is less (Steele et al., 2019).
(g) As described in the paper, measurement bias arose from a cross-sectional study and usage
of the questionnaire to interview events that occurred previously. Authors tried to minimise
(d)
Details Case
exposure
Control
Exposure
Yes
54 203
Exposure
No
106 736
For this study, the expected crude Odd ratio for domestic violence=
[(54)/(106)]/[(203)/(736)] = 1.85
So, the crude odds ratio for this study is 1.85
(e) In this study, the adjusted value of odd ratio was 1.44. While the calculated value was
1.85. The odd ratio differs due to the significant presence of confounder variables other than
domestic violence.
(f) As per table 5, the effect of physical violence on low birth weight was less since only 13
individuals out of 160 test individuals reported to be associated with physical violence. The
adjusted prevalence ratio was found to be 0.69. This value is comparatively less than 1.44 for
domestic violence. The reason for this less value is that, physical violence was not the only
factor in reducing its prevalence ratio. Sexual and environmental violence also influenced the
value. Therefore the value is less (Steele et al., 2019).
(g) As described in the paper, measurement bias arose from a cross-sectional study and usage
of the questionnaire to interview events that occurred previously. Authors tried to minimise
3EPIDEMIOLOGY
the effect by using close questions stated by WHO’sDV and used well-trained professionals
as interviewers.
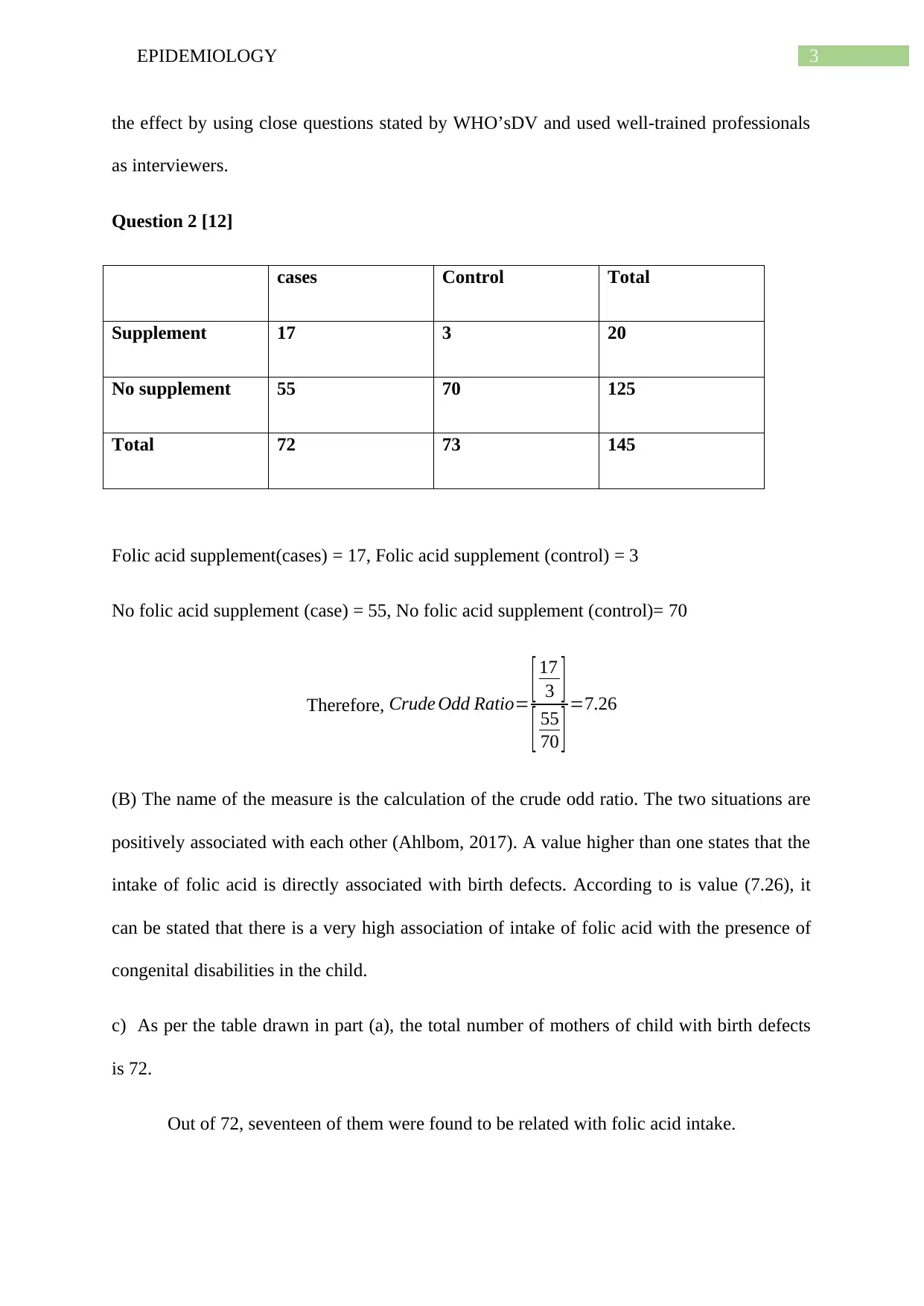
Question 2 [12]
cases Control Total
Supplement 17 3 20
No supplement 55 70 125
Total 72 73 145
Folic acid supplement(cases) = 17, Folic acid supplement (control) = 3
No folic acid supplement (case) = 55, No folic acid supplement (control)= 70
Therefore, Crude Odd Ratio= [ 17
3 ]
[ 55
70 ] =7.26
(B) The name of the measure is the calculation of the crude odd ratio. The two situations are
positively associated with each other (Ahlbom, 2017). A value higher than one states that the
intake of folic acid is directly associated with birth defects. According to is value (7.26), it
can be stated that there is a very high association of intake of folic acid with the presence of
congenital disabilities in the child.
c) As per the table drawn in part (a), the total number of mothers of child with birth defects
is 72.
Out of 72, seventeen of them were found to be related with folic acid intake.
the effect by using close questions stated by WHO’sDV and used well-trained professionals
as interviewers.
Question 2 [12]
cases Control Total
Supplement 17 3 20
No supplement 55 70 125
Total 72 73 145
Folic acid supplement(cases) = 17, Folic acid supplement (control) = 3
No folic acid supplement (case) = 55, No folic acid supplement (control)= 70
Therefore, Crude Odd Ratio= [ 17
3 ]
[ 55
70 ] =7.26
(B) The name of the measure is the calculation of the crude odd ratio. The two situations are
positively associated with each other (Ahlbom, 2017). A value higher than one states that the
intake of folic acid is directly associated with birth defects. According to is value (7.26), it
can be stated that there is a very high association of intake of folic acid with the presence of
congenital disabilities in the child.
c) As per the table drawn in part (a), the total number of mothers of child with birth defects
is 72.
Out of 72, seventeen of them were found to be related with folic acid intake.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4EPIDEMIOLOGY
The proportion of people for whom the folic acid intake can be prevented is= ( 17
72 )∗100
The proportion is = 23.61
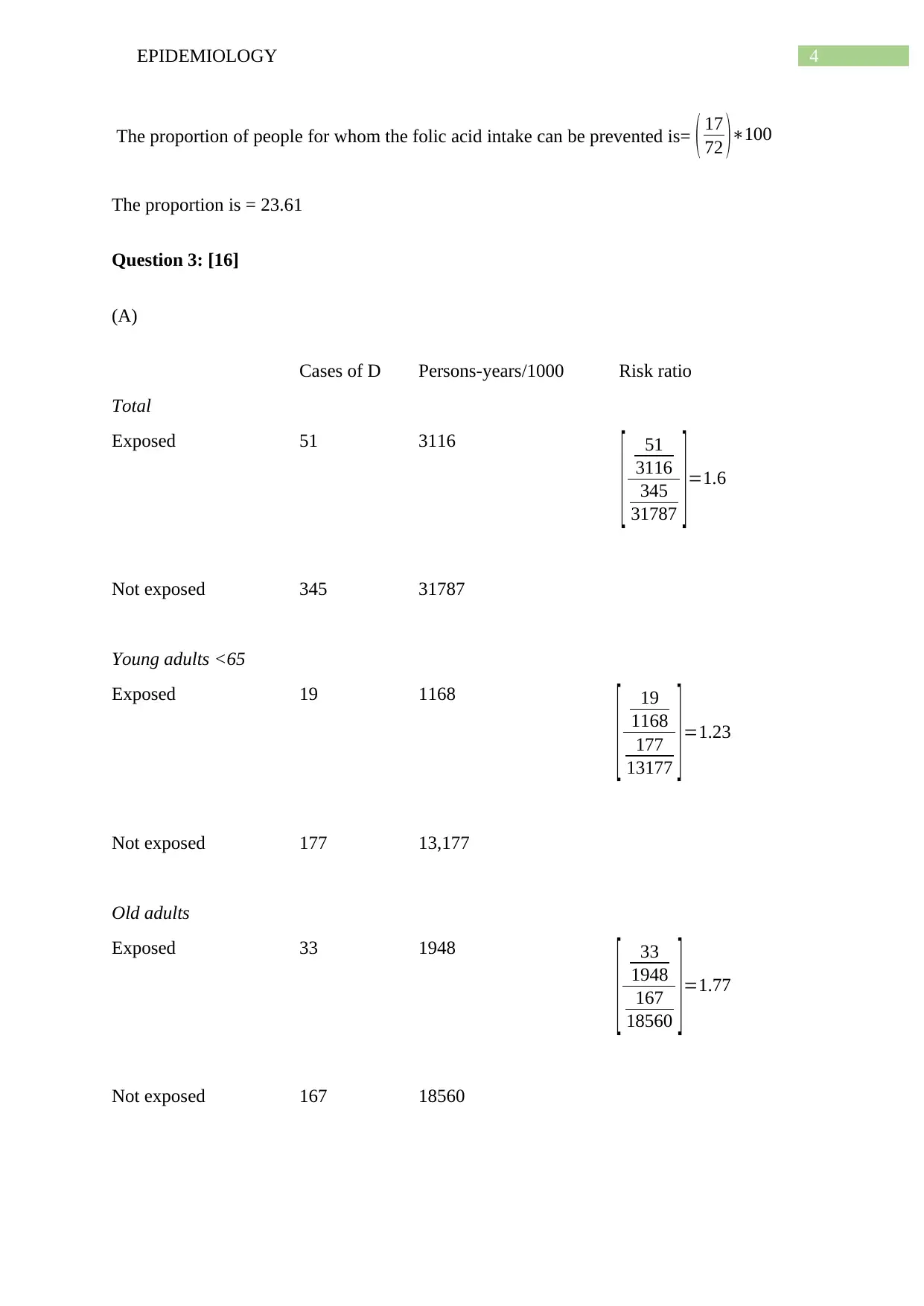
Question 3: [16]
(A)
Cases of D Persons-years/1000 Risk ratio
Total
Exposed 51 3116
[ 51
3116
345
31787 ] =1.6
Not exposed 345 31787
Young adults <65
Exposed 19 1168
[ 19
1168
177
13177 ]=1.23
Not exposed 177 13,177
Old adults
Exposed 33 1948
[ 33
1948
167
18560 ] =1.77
Not exposed 167 18560
The proportion of people for whom the folic acid intake can be prevented is= ( 17
72 )∗100
The proportion is = 23.61
Question 3: [16]
(A)
Cases of D Persons-years/1000 Risk ratio
Total
Exposed 51 3116
[ 51
3116
345
31787 ] =1.6
Not exposed 345 31787
Young adults <65
Exposed 19 1168
[ 19
1168
177
13177 ]=1.23
Not exposed 177 13,177
Old adults
Exposed 33 1948
[ 33
1948
167
18560 ] =1.77
Not exposed 167 18560
5EPIDEMIOLOGY
Table: Incidence of the disease by exposure status, stratified by age group (young /old)
From the above table it can be concluded that the association of exposure to this particular
disease is 1.6. However, it has been observed that when young adults were taken, the crude
association rate reduced to 1.23. In case of old adults, it increased to 1.77. So, these two
variables are referred as confounders which affects the original value (1.6).
(B) The adjusted risk ratio was found 1.51. While the calculated risk ratio was equal to 1.6,
the age variable can be assessed as a confounder variable. This value significantly deviates
from the original value. The value of this variable influences both the rare exposure and the
disease. The significant correlation between them can never be calculated.
(C) Attributable risk is referred as the difference between the probability of the predisposition
of the disease in people exposed to it and the probability of the predisposition of the disease
in the unexposed ones.
As per the above table, the following risk ratios can be calculated:
The risk ratio associated with exposed older people = 33
1948 =0.017
The risk ratio associated with unexposed older people = 167
18560 =0.009
Therefore, the attributable risk ratio is = ( 0.017−0.009 )∗100
¿ 0.8 %
Hence, the attributable risk of exposure for older people was 0.8%.
Table: Incidence of the disease by exposure status, stratified by age group (young /old)
From the above table it can be concluded that the association of exposure to this particular
disease is 1.6. However, it has been observed that when young adults were taken, the crude
association rate reduced to 1.23. In case of old adults, it increased to 1.77. So, these two
variables are referred as confounders which affects the original value (1.6).
(B) The adjusted risk ratio was found 1.51. While the calculated risk ratio was equal to 1.6,
the age variable can be assessed as a confounder variable. This value significantly deviates
from the original value. The value of this variable influences both the rare exposure and the
disease. The significant correlation between them can never be calculated.
(C) Attributable risk is referred as the difference between the probability of the predisposition
of the disease in people exposed to it and the probability of the predisposition of the disease
in the unexposed ones.
As per the above table, the following risk ratios can be calculated:
The risk ratio associated with exposed older people = 33
1948 =0.017
The risk ratio associated with unexposed older people = 167
18560 =0.009
Therefore, the attributable risk ratio is = ( 0.017−0.009 )∗100
¿ 0.8 %
Hence, the attributable risk of exposure for older people was 0.8%.
6EPIDEMIOLOGY
(D) From the result of the above calculation 3(c), it has been observed that the attributable
risk of exposure for older adults is 0.8%. According to this calculation, the risk of exposures
for older adults is always significantly higher than the young adult. These results proved that
old age people were more exposed to the disease than the younger adults (Rao, 2016).
Question 4 [12]
(A) In the field of epidemiology, biases is referred as a systematic fault that finally concludes
the wrong estimation of an accurate value of a specific exposure. As per the statement in the
article “In a survey of the prevalence of overweight and obese participants were measure
once for their weight and once for their height in the same lab”. Generally there are two types
of biases, Information bias and Selection bias. Here, the bias type is basically an information
bias. The bias is generally regarded as informational as both height and weight are not taken
at the same time. These two variables were used differently for calculating the prevalence of
obesity as well as overweight among people in the experimental lab. Hence, there can be a
statistical error as both height and weight were collected separately. Thus, the height of an
individual can easily be merged with the weight of another person at the time of tabulation
(March et al., 2018).
(B) As per the second statement “In another survey to estimate the prevalence of overweight
and obesity participants were asked to report on their weight and height from their head",
here, this is also an information bias. This bias is said to be information bias as the data were
collected from verbal communication with the individuals participating in the survey.
However, this biasness can also provide the wrong height and weights of themselves and thus
resulting in information bias (Ananth & Schisterman, 2017). This biasness can be referred as
a recall bias as people have to correctly recall what they heard in the past and accurately
(D) From the result of the above calculation 3(c), it has been observed that the attributable
risk of exposure for older adults is 0.8%. According to this calculation, the risk of exposures
for older adults is always significantly higher than the young adult. These results proved that
old age people were more exposed to the disease than the younger adults (Rao, 2016).
Question 4 [12]
(A) In the field of epidemiology, biases is referred as a systematic fault that finally concludes
the wrong estimation of an accurate value of a specific exposure. As per the statement in the
article “In a survey of the prevalence of overweight and obese participants were measure
once for their weight and once for their height in the same lab”. Generally there are two types
of biases, Information bias and Selection bias. Here, the bias type is basically an information
bias. The bias is generally regarded as informational as both height and weight are not taken
at the same time. These two variables were used differently for calculating the prevalence of
obesity as well as overweight among people in the experimental lab. Hence, there can be a
statistical error as both height and weight were collected separately. Thus, the height of an
individual can easily be merged with the weight of another person at the time of tabulation
(March et al., 2018).
(B) As per the second statement “In another survey to estimate the prevalence of overweight
and obesity participants were asked to report on their weight and height from their head",
here, this is also an information bias. This bias is said to be information bias as the data were
collected from verbal communication with the individuals participating in the survey.
However, this biasness can also provide the wrong height and weights of themselves and thus
resulting in information bias (Ananth & Schisterman, 2017). This biasness can be referred as
a recall bias as people have to correctly recall what they heard in the past and accurately
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7EPIDEMIOLOGY
report the values for the study. Hence, there is always a probability for forgetting the original
values and incorporation of new values.
(C) The above-stated problem in the case of women underestimating their weights and men
reporting their weights accurately occurs due to differential misclassification. This condition
occurs when the exposure becomes unequal between the candidates used in the study
(Ahlbom, 2017). The problem also arises when the misclassification of the case is not equal
in the case of exposed and unexposed subjects. Here, women can be stated to be more
concerned about having less weight, and thus, they underestimate the weight and states than
their original weights. However, men provide accurate weights and thus the differential
misclassification is seen in this case.
report the values for the study. Hence, there is always a probability for forgetting the original
values and incorporation of new values.
(C) The above-stated problem in the case of women underestimating their weights and men
reporting their weights accurately occurs due to differential misclassification. This condition
occurs when the exposure becomes unequal between the candidates used in the study
(Ahlbom, 2017). The problem also arises when the misclassification of the case is not equal
in the case of exposed and unexposed subjects. Here, women can be stated to be more
concerned about having less weight, and thus, they underestimate the weight and states than
their original weights. However, men provide accurate weights and thus the differential
misclassification is seen in this case.
8EPIDEMIOLOGY
References
Ahlbom, A. (2017). Biostatistics for epidemiologists. CRC Press.
Ananth, C. V., &Schisterman, E. F. (2017). Confounding, causality, and confusion: the role
of intermediate variables in interpreting observational studies in obstetrics. American
journal of obstetrics and gynecology, 217(2), 167-175.
March, D., Begg, M., Wiggin, M., & Begg, M. (2018). The integrated approach to teaching
Biostatistics and Epidemiology at Columbia. European Journal of Public
Health, 28(suppl_4), cky218-008.
Rao, D., Kumar, S., Mohanraj, R., Frey, S., Manhart, L. E., & Kaysen, D. L. (2016). The
impact of domestic violence and depressive symptoms on preterm birth in South
India. Social psychiatry and psychiatric epidemiology, 51(2), 225-232.
Steele, S. J., Abrahams, N., Duncan, K., Woollett, N., Hwang, B., O’Connell, L., ... &
Shroufi, A. (2019). The epidemiology of rape and sexual violence in the platinum
mining district of Rustenburg, South Africa: Prevalence, and factors associated with
sexual violence. PLoS one, 14(7), e0216449.
Vachhani, P. V., Bhimani, N. R., Purani, S. K., & Kartha, G. P. (2017). Epidemiology of
domestic violence among married women: a community based cross-sectional
study. International Journal Of Community Medicine And Public Health, 4(4), 1353-
1359.
Wassertheil-Smoller, S., & Smoller, J. (2015). Biostatistics and epidemiology: a primer for
health and biomedical professionals.Springer.
References
Ahlbom, A. (2017). Biostatistics for epidemiologists. CRC Press.
Ananth, C. V., &Schisterman, E. F. (2017). Confounding, causality, and confusion: the role
of intermediate variables in interpreting observational studies in obstetrics. American
journal of obstetrics and gynecology, 217(2), 167-175.
March, D., Begg, M., Wiggin, M., & Begg, M. (2018). The integrated approach to teaching
Biostatistics and Epidemiology at Columbia. European Journal of Public
Health, 28(suppl_4), cky218-008.
Rao, D., Kumar, S., Mohanraj, R., Frey, S., Manhart, L. E., & Kaysen, D. L. (2016). The
impact of domestic violence and depressive symptoms on preterm birth in South
India. Social psychiatry and psychiatric epidemiology, 51(2), 225-232.
Steele, S. J., Abrahams, N., Duncan, K., Woollett, N., Hwang, B., O’Connell, L., ... &
Shroufi, A. (2019). The epidemiology of rape and sexual violence in the platinum
mining district of Rustenburg, South Africa: Prevalence, and factors associated with
sexual violence. PLoS one, 14(7), e0216449.
Vachhani, P. V., Bhimani, N. R., Purani, S. K., & Kartha, G. P. (2017). Epidemiology of
domestic violence among married women: a community based cross-sectional
study. International Journal Of Community Medicine And Public Health, 4(4), 1353-
1359.
Wassertheil-Smoller, S., & Smoller, J. (2015). Biostatistics and epidemiology: a primer for
health and biomedical professionals.Springer.
1 out of 9
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.