Global maternal health.
VerifiedAdded on 2023/01/06
|15
|3168
|75
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Running Head Global maternal health 0
Global Maternal health
Student Name
[Pick the date]
Global Maternal health
Student Name
[Pick the date]
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global maternal health 1
Contents
Introduction......................................................................................................................................3
Observation......................................................................................................................................4
Enablers to enhancing global maternal health.................................................................................4
Barriers to improving Aboriginal childbearing women well-being................................................5
Cultural competence while communicating with the childbearing woman.....................................6
Cultural awareness: 6
Sensitivity: 6
Safety and security:..........................................................................................................................6
Global maternal health care Knowledge..........................................................................................7
Various maternity programs............................................................................................................8
Maternal health Experience of an indigenous childbearing woman in Australia............................9
Recommendations............................................................................................................................9
Conclusion.....................................................................................................................................11
References......................................................................................................................................13
Contents
Introduction......................................................................................................................................3
Observation......................................................................................................................................4
Enablers to enhancing global maternal health.................................................................................4
Barriers to improving Aboriginal childbearing women well-being................................................5
Cultural competence while communicating with the childbearing woman.....................................6
Cultural awareness: 6
Sensitivity: 6
Safety and security:..........................................................................................................................6
Global maternal health care Knowledge..........................................................................................7
Various maternity programs............................................................................................................8
Maternal health Experience of an indigenous childbearing woman in Australia............................9
Recommendations............................................................................................................................9
Conclusion.....................................................................................................................................11
References......................................................................................................................................13
Global maternal health 2
Introduction
As a professional practitioner in a national social group, I have observed and experienced
the condition of aboriginal childbearing women of Australia.
During my practice, I found that Aboriginal childbearing women experienced poorer
health compared to non-indigenous women’s of Australia. I observe that aboriginal women
are suffering from depression and forced elimination from family relationships. It seemed to
me that Aboriginal women of Australia faced racism and physical assault during pregnancy. I
have communicated with my fellows to safeguard the indigenous women and educate them
about prenatal services.
I noticed in my professional practice that immigrants and refugees women are suffering
from depression and stress. Our team was having a discussion on the condition of aboriginal
childbearing women and during the discussion, one of my teammates told me that the united
nation general assembly collaborated with Canada and Germany to improve the maternal
health of immigrant’s women and refugees.
Further discussion, is on the enablers and barriers of global maternal health, enablers
where women provided with the pregnancy-related information, cultural safety and family
support. There are some barriers, which halts the growth of global maternal health. Poor
health discrimination or discrimination is a barrier to improving global maternal health.
I have taken a part in various program to experience the Aboriginal childbearing women
of Australia like prenatal nutrition program and maternal child health program.
The experience of Aboriginal childbearing women in Australia is poorest compared to
non-indigenous women of Australia. Birth rates are likely very low or premature death is
very high. Recommendations, which can improve the maternal health of indigenous
childbearing women of Australia encourage the women to access the maternal health services
provided by the health specialists.
Introduction
As a professional practitioner in a national social group, I have observed and experienced
the condition of aboriginal childbearing women of Australia.
During my practice, I found that Aboriginal childbearing women experienced poorer
health compared to non-indigenous women’s of Australia. I observe that aboriginal women
are suffering from depression and forced elimination from family relationships. It seemed to
me that Aboriginal women of Australia faced racism and physical assault during pregnancy. I
have communicated with my fellows to safeguard the indigenous women and educate them
about prenatal services.
I noticed in my professional practice that immigrants and refugees women are suffering
from depression and stress. Our team was having a discussion on the condition of aboriginal
childbearing women and during the discussion, one of my teammates told me that the united
nation general assembly collaborated with Canada and Germany to improve the maternal
health of immigrant’s women and refugees.
Further discussion, is on the enablers and barriers of global maternal health, enablers
where women provided with the pregnancy-related information, cultural safety and family
support. There are some barriers, which halts the growth of global maternal health. Poor
health discrimination or discrimination is a barrier to improving global maternal health.
I have taken a part in various program to experience the Aboriginal childbearing women
of Australia like prenatal nutrition program and maternal child health program.
The experience of Aboriginal childbearing women in Australia is poorest compared to
non-indigenous women of Australia. Birth rates are likely very low or premature death is
very high. Recommendations, which can improve the maternal health of indigenous
childbearing women of Australia encourage the women to access the maternal health services
provided by the health specialists.
Global maternal health 3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global maternal health 4
Observation
During my professional practice, I have noticed that immigrant and migrant woman is
suffering from stress and high blood pressure during the pregnancy period. I felt dreadful that
an immigrant’s woman shifted from one country to another because of racism, religion,
political opinion, and community differences ( Burns & MacRae, 2013).
Personal experience: As a practitioner, I provided services to the aboriginal childbearing
women so I have seen that one woman engaged in smoking during her pregnancy and
develop respiratory infections and asthma I have tried my best to treat her but she died after
3-4 days. As a practitioner, our team generates ways to improve the physical, psychological
and reproductive health of a larger number of immigrant’s woman because the health of a
woman is important during the pregnancy because of the threat of inevitable adverse
parental.
During my practice, I have noticed and realized that the protection of the childbearing
woman and social support is very crucial. Our social group plays a vital role in boosting the
health of the childbearing woman. I have been examined that 77% childbearing woman
settled in the high-income countries like Germany, Canada or Sweden due to racism and
discrimination.
Enablers to enhancing global maternal health
In my experience, I have realized that it is necessary to provide primary education to
the women or certifying universal admission. Enhance education from primary to
higher education, for example, Girl’s primary school enrollment.
When I worked as a practitioner, I have realized that health care providers did not
maintain hygiene at hospitals so according to me the hygiene facilities should
improve and provide clean water to the childbearing woman.
During my practice an incident happened, Aboriginal women admitted in a hospital,
her condition was not good, the health service providers of that hospital ignoring her
and refuse to provide her a treatment, and it is hard to explain that what I felt at that
Observation
During my professional practice, I have noticed that immigrant and migrant woman is
suffering from stress and high blood pressure during the pregnancy period. I felt dreadful that
an immigrant’s woman shifted from one country to another because of racism, religion,
political opinion, and community differences ( Burns & MacRae, 2013).
Personal experience: As a practitioner, I provided services to the aboriginal childbearing
women so I have seen that one woman engaged in smoking during her pregnancy and
develop respiratory infections and asthma I have tried my best to treat her but she died after
3-4 days. As a practitioner, our team generates ways to improve the physical, psychological
and reproductive health of a larger number of immigrant’s woman because the health of a
woman is important during the pregnancy because of the threat of inevitable adverse
parental.
During my practice, I have noticed and realized that the protection of the childbearing
woman and social support is very crucial. Our social group plays a vital role in boosting the
health of the childbearing woman. I have been examined that 77% childbearing woman
settled in the high-income countries like Germany, Canada or Sweden due to racism and
discrimination.
Enablers to enhancing global maternal health
In my experience, I have realized that it is necessary to provide primary education to
the women or certifying universal admission. Enhance education from primary to
higher education, for example, Girl’s primary school enrollment.
When I worked as a practitioner, I have realized that health care providers did not
maintain hygiene at hospitals so according to me the hygiene facilities should
improve and provide clean water to the childbearing woman.
During my practice an incident happened, Aboriginal women admitted in a hospital,
her condition was not good, the health service providers of that hospital ignoring her
and refuse to provide her a treatment, and it is hard to explain that what I felt at that
Global maternal health 5
time. According to me, this inequalities and racism should decrease. Economic
development and good governance are essential for enhancing global maternal health
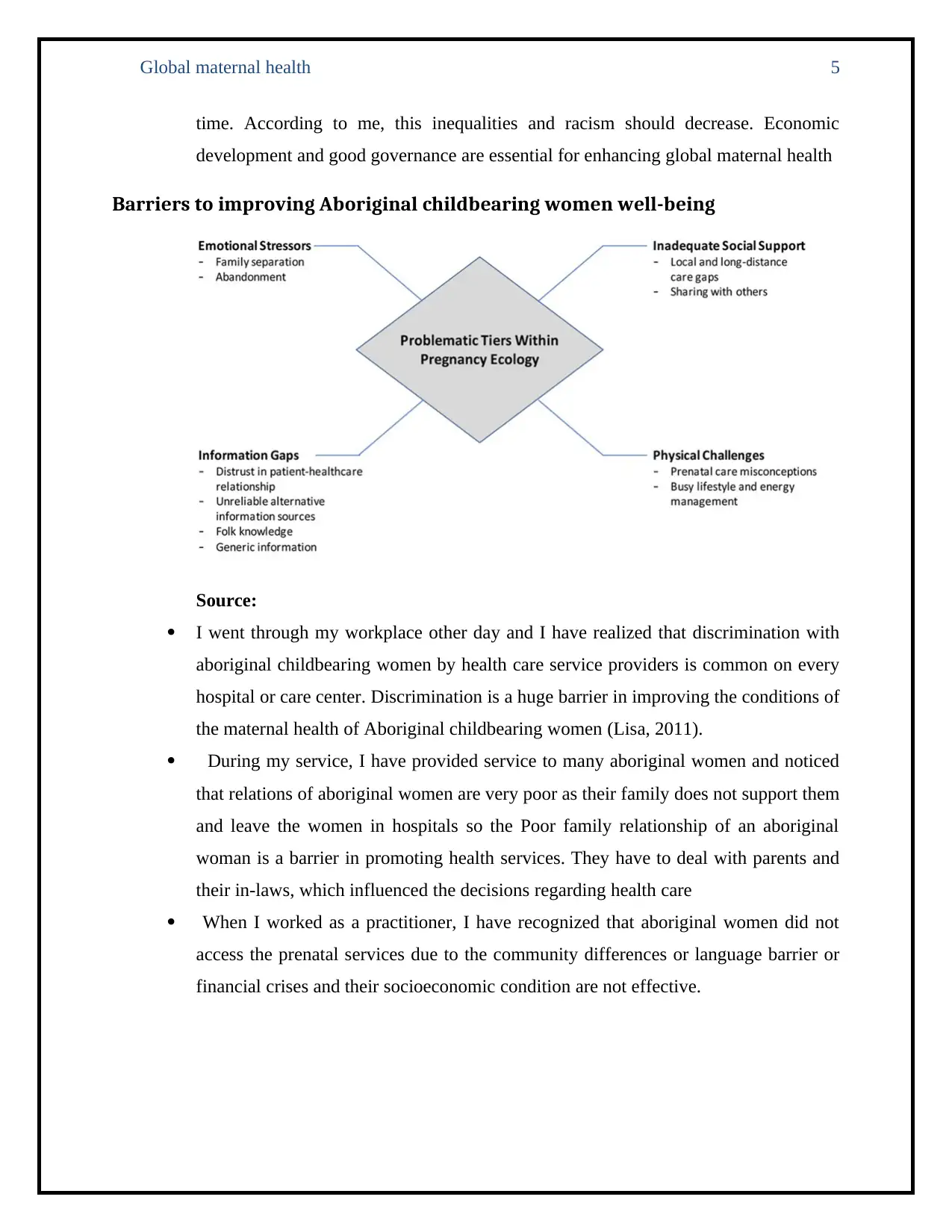
Barriers to improving Aboriginal childbearing women well-being
Source:
I went through my workplace other day and I have realized that discrimination with
aboriginal childbearing women by health care service providers is common on every
hospital or care center. Discrimination is a huge barrier in improving the conditions of
the maternal health of Aboriginal childbearing women (Lisa, 2011).
During my service, I have provided service to many aboriginal women and noticed
that relations of aboriginal women are very poor as their family does not support them
and leave the women in hospitals so the Poor family relationship of an aboriginal
woman is a barrier in promoting health services. They have to deal with parents and
their in-laws, which influenced the decisions regarding health care
When I worked as a practitioner, I have recognized that aboriginal women did not
access the prenatal services due to the community differences or language barrier or
financial crises and their socioeconomic condition are not effective.
time. According to me, this inequalities and racism should decrease. Economic
development and good governance are essential for enhancing global maternal health
Barriers to improving Aboriginal childbearing women well-being
Source:
I went through my workplace other day and I have realized that discrimination with
aboriginal childbearing women by health care service providers is common on every
hospital or care center. Discrimination is a huge barrier in improving the conditions of
the maternal health of Aboriginal childbearing women (Lisa, 2011).
During my service, I have provided service to many aboriginal women and noticed
that relations of aboriginal women are very poor as their family does not support them
and leave the women in hospitals so the Poor family relationship of an aboriginal
woman is a barrier in promoting health services. They have to deal with parents and
their in-laws, which influenced the decisions regarding health care
When I worked as a practitioner, I have recognized that aboriginal women did not
access the prenatal services due to the community differences or language barrier or
financial crises and their socioeconomic condition are not effective.

Global maternal health 6
Cultural competence while communicating with the childbearing
woman
Cultural awareness: During my professional practice, I interact with the different
women who belong to different culture and background and they are dissimilar to my own
culture. Language is a big problem for the aboriginal women so we appointed an interpreter
to help the women and me and my teammates accessed the economic and geographical
culture of women to help her during the treatment. I noticed that health care providers of
aboriginal women did not identify the culture of women, which creates a problem of
communication. We implement the campaign, to help the aboriginal childbearing women of
Australia and to reduce communication barrier. Health service providers should provide
services suitable for their background and culture. Our teams provide education about
pregnancy and give them social support ( Parker, 2014).
Sensitivity: I have noticed that aboriginal women worked during the pregnancy to earn
the money and to survive with the family, which affects their health and results in a lack of
energy and fatigue. We suggest various exercises but they do not attend the session and
prenatal education. As I noticed, health care providers did not communicate with aboriginals
in their favored language. Health care providers must communicate in their favored language
and encourage them to attend classes ( Quiggin, 2002).
Safety and security: When I worked as a practitioner, I have treated a woman who is
Aboriginal and she explained her condition to me that she suffered from the sexual abuse and
physical assault in the care centers or by the health care service providers. I have taken
several steps to provide safety and security to the aboriginal’s childbearing women and to
funding social support. Health care providers should ensure safety or dignity of aboriginal
childbearing women irrespective of their nationality. Ensure that childbearing woman is free
from the physical exploitation and abuse in Australia. The Facility of households to a
pregnant woman should provide. The health service providers should give facility of Funding
for their livelihood
Cultural competence while communicating with the childbearing
woman
Cultural awareness: During my professional practice, I interact with the different
women who belong to different culture and background and they are dissimilar to my own
culture. Language is a big problem for the aboriginal women so we appointed an interpreter
to help the women and me and my teammates accessed the economic and geographical
culture of women to help her during the treatment. I noticed that health care providers of
aboriginal women did not identify the culture of women, which creates a problem of
communication. We implement the campaign, to help the aboriginal childbearing women of
Australia and to reduce communication barrier. Health service providers should provide
services suitable for their background and culture. Our teams provide education about
pregnancy and give them social support ( Parker, 2014).
Sensitivity: I have noticed that aboriginal women worked during the pregnancy to earn
the money and to survive with the family, which affects their health and results in a lack of
energy and fatigue. We suggest various exercises but they do not attend the session and
prenatal education. As I noticed, health care providers did not communicate with aboriginals
in their favored language. Health care providers must communicate in their favored language
and encourage them to attend classes ( Quiggin, 2002).
Safety and security: When I worked as a practitioner, I have treated a woman who is
Aboriginal and she explained her condition to me that she suffered from the sexual abuse and
physical assault in the care centers or by the health care service providers. I have taken
several steps to provide safety and security to the aboriginal’s childbearing women and to
funding social support. Health care providers should ensure safety or dignity of aboriginal
childbearing women irrespective of their nationality. Ensure that childbearing woman is free
from the physical exploitation and abuse in Australia. The Facility of households to a
pregnant woman should provide. The health service providers should give facility of Funding
for their livelihood
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global maternal health 7
Global maternal health care Knowledge
As a health practitioner, I studied that every day 830 women approximately die by the
reason related to pregnancy and childbirth. I learned that 99% of woman’s dies from causes
related to pregnancy and childbirth and most of them are Aboriginals and from sub-Saharan
and Africa. Major patients that I have treated are teenage girls who are under the age of 15
who are suffering from depression and stress, which causes the death of adolescent girls in
Australia
During my practice, I have seen a woman and teenage girls are dying because of the
complications related to pregnancy and childbirth. According to me the major complications
of death are:
Severe bleeding after the childbirth
Severe Infections
High blood pressure during the prenatal period
Complications related to the delivery
Insecure abortion
I have studied during my practice that 75% women died because of complications
during the pregnancy and main reason for this is that the health providers should not
skillfully handle the situations and did not maintain expert care during childbirth. Care or
support after pregnancy is very crucial. It is very crucial that health care providers are
professional in nature and there must be an availability of treatment as it can create the
difference between life and death for both patient and the newborn baby
In my experience, I have seen many women who do not access health care services
during the prenatal period as of poverty and lack of information reasons or due to the
different cultural practices. Many women came and share their problem with me
difficulty of distance because they live in a rural area or underdeveloped places, which
create a problem of access to maternal services.
.
Global maternal health care Knowledge
As a health practitioner, I studied that every day 830 women approximately die by the
reason related to pregnancy and childbirth. I learned that 99% of woman’s dies from causes
related to pregnancy and childbirth and most of them are Aboriginals and from sub-Saharan
and Africa. Major patients that I have treated are teenage girls who are under the age of 15
who are suffering from depression and stress, which causes the death of adolescent girls in
Australia
During my practice, I have seen a woman and teenage girls are dying because of the
complications related to pregnancy and childbirth. According to me the major complications
of death are:
Severe bleeding after the childbirth
Severe Infections
High blood pressure during the prenatal period
Complications related to the delivery
Insecure abortion
I have studied during my practice that 75% women died because of complications
during the pregnancy and main reason for this is that the health providers should not
skillfully handle the situations and did not maintain expert care during childbirth. Care or
support after pregnancy is very crucial. It is very crucial that health care providers are
professional in nature and there must be an availability of treatment as it can create the
difference between life and death for both patient and the newborn baby
In my experience, I have seen many women who do not access health care services
during the prenatal period as of poverty and lack of information reasons or due to the
different cultural practices. Many women came and share their problem with me
difficulty of distance because they live in a rural area or underdeveloped places, which
create a problem of access to maternal services.
.
Global maternal health 8
Various maternity programs
During my practice, I have worked with many maternity programs such as prenatal
nutrition program and maternal child health programs.
a) Prenatal Nutrition program
I have worked with this program and the vital motive of this program is to educate or
attract the woman about the prenatal care services and sustained their connection to the
broader community through healthiness and social cares. I have worked there to supply
nutrients to aboriginal childbearing woman, which is necessary for their healthy
pregnancy. Vital activities of this program are to give education to the woman about
infant attachment and newborn development or social support services of health care
providers (Horton, 2019).
According to my study, there are 3300 aboriginal women of childbearing age are
present in the communities. When I worked with this program, I have realized that this
program was a launch to develop the nutritional health of the Aboriginal childbearing
woman. While treatment of childbearing woman I have learned that it is essential to
provide education and support, nutritional screening and maternal nourishment to the
childbearing woman. I have developed a diet plan of prenatal and breastfeeding women
to improve their condition but some of them follow and some of them not
b) Maternal child health program: I have experienced maternal health of mother
through this program. They support aboriginal childbearing women including their family
for development and lifetime potential. Through this program, I have provided nutrition
knowledge to the childbearing women and provide the facility of home visits to
aboriginal childbearing women. Health promotion and pregnancy awareness is the main
objective of MCH’s ( Zulfiqar, 2013).
Various maternity programs
During my practice, I have worked with many maternity programs such as prenatal
nutrition program and maternal child health programs.
a) Prenatal Nutrition program
I have worked with this program and the vital motive of this program is to educate or
attract the woman about the prenatal care services and sustained their connection to the
broader community through healthiness and social cares. I have worked there to supply
nutrients to aboriginal childbearing woman, which is necessary for their healthy
pregnancy. Vital activities of this program are to give education to the woman about
infant attachment and newborn development or social support services of health care
providers (Horton, 2019).
According to my study, there are 3300 aboriginal women of childbearing age are
present in the communities. When I worked with this program, I have realized that this
program was a launch to develop the nutritional health of the Aboriginal childbearing
woman. While treatment of childbearing woman I have learned that it is essential to
provide education and support, nutritional screening and maternal nourishment to the
childbearing woman. I have developed a diet plan of prenatal and breastfeeding women
to improve their condition but some of them follow and some of them not
b) Maternal child health program: I have experienced maternal health of mother
through this program. They support aboriginal childbearing women including their family
for development and lifetime potential. Through this program, I have provided nutrition
knowledge to the childbearing women and provide the facility of home visits to
aboriginal childbearing women. Health promotion and pregnancy awareness is the main
objective of MCH’s ( Zulfiqar, 2013).
Global maternal health 9
c) Aboriginal Midwifery in Australia: As a practitioner, I have learned about a facility
who provide by health specialists. In this facility, midwifery-training service including
communal based birthing services. They teach childbearing women traditional and
modern methods which essential for birth, labor, and postpartum care. I have seen many
women who take part in these programs especially Aboriginal childbearing women.
Maternal health Experience of an indigenous childbearing woman in
Australia
I have learned many things during my professional practice in Australia such as
aboriginal’s newborns have inferior birth results as compared to non-aboriginal infants in
Western Australia. I have seen many childbearing women who suffered assault during
pregnancy and Infection during the prenatal period. Twenty-seven percent of birth in
Australia has negative outcomes. As a health professional, I have treated many women who
were addicted to smoking and alcohol ( Bronwyn, 2010).
After working with so many days, the outcomes are positive in some areas such as
violence against the childbearing women decreased as stated by national personal safety
survey. This happens because of the awareness and education provides by the health care
providers. Our teammates draft a plan to provide materiality service to the childbearing
women like the introduction of traditional practice and identification of women’s culture with
land and country or by supporting their culture (Mary, 2010).
I have observed that the birth rate of aboriginals is low, compared to the non-indigenous
women because of the Discrimination with aboriginal women. I helped many childbearing
women and provide them education, employment, and cultural safety. Health care providers
should educate aboriginal childbearing women about prenatal knowledge.
Recommendations
After my professional practice with aboriginal childbearing women, I would like to suggest
some practices, which can improve the condition of aboriginal women in Australia.
c) Aboriginal Midwifery in Australia: As a practitioner, I have learned about a facility
who provide by health specialists. In this facility, midwifery-training service including
communal based birthing services. They teach childbearing women traditional and
modern methods which essential for birth, labor, and postpartum care. I have seen many
women who take part in these programs especially Aboriginal childbearing women.
Maternal health Experience of an indigenous childbearing woman in
Australia
I have learned many things during my professional practice in Australia such as
aboriginal’s newborns have inferior birth results as compared to non-aboriginal infants in
Western Australia. I have seen many childbearing women who suffered assault during
pregnancy and Infection during the prenatal period. Twenty-seven percent of birth in
Australia has negative outcomes. As a health professional, I have treated many women who
were addicted to smoking and alcohol ( Bronwyn, 2010).
After working with so many days, the outcomes are positive in some areas such as
violence against the childbearing women decreased as stated by national personal safety
survey. This happens because of the awareness and education provides by the health care
providers. Our teammates draft a plan to provide materiality service to the childbearing
women like the introduction of traditional practice and identification of women’s culture with
land and country or by supporting their culture (Mary, 2010).
I have observed that the birth rate of aboriginals is low, compared to the non-indigenous
women because of the Discrimination with aboriginal women. I helped many childbearing
women and provide them education, employment, and cultural safety. Health care providers
should educate aboriginal childbearing women about prenatal knowledge.
Recommendations
After my professional practice with aboriginal childbearing women, I would like to suggest
some practices, which can improve the condition of aboriginal women in Australia.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global maternal health 10
I have experienced that many women’s are not aware of the procedures to access the
maternal services so health care providers and hospitals should explain the antenatal
care and ways of accessing it.
I have observed that women hesitate before accessing the services so to improve
these health care providers must build a Trust-based relationship with the aboriginal
childbearing women.
Mitigation of discrimination with the Aboriginals is very essential so, health care
providers should not treat any women on their culture, religious beliefs and ethnic
beliefs (Kildea, Improving maternity services for Indigenous women in Australia,
2016).
According to me, health care providers must consider all the issues, which impacts on
the childbearing women such as transport, cost of ultrasounds, Medicare rebates.
In my experience, the family of women did not support her so care centers should
support the family relationships and friends
Regular communication with the childbearing women is crucial and consults with her
so she can receive appropriate self-care during the prenatal period.
I have handled Aboriginals women and they come from a different culture language
so before treating childbearing women we should explore the culture of childbearing
women and help the women or discuss everything that she is insecure or nervous
about (Kildea, Improving maternity services for Indigenous, 2016)
Encourage the women and explain each term that women probable to listen to at
antenatal appointments with different health specialists.
Women privacy must be respected and make the situation safe within the hospital or
anywhere women are residing.
Communicate and discuss the women’s perspective about her pregnancy.
Multicultural health workers must assist the women to access the prenatal services
and support to attend the appointments. Provide services, which is similar to women’s
culture and language. Multicultural health workers must communicate with women in
their preferred language (organisation, recommendations on health promotion
interventions for maternal and newborn health , 2015).
I have experienced that many women’s are not aware of the procedures to access the
maternal services so health care providers and hospitals should explain the antenatal
care and ways of accessing it.
I have observed that women hesitate before accessing the services so to improve
these health care providers must build a Trust-based relationship with the aboriginal
childbearing women.
Mitigation of discrimination with the Aboriginals is very essential so, health care
providers should not treat any women on their culture, religious beliefs and ethnic
beliefs (Kildea, Improving maternity services for Indigenous women in Australia,
2016).
According to me, health care providers must consider all the issues, which impacts on
the childbearing women such as transport, cost of ultrasounds, Medicare rebates.
In my experience, the family of women did not support her so care centers should
support the family relationships and friends
Regular communication with the childbearing women is crucial and consults with her
so she can receive appropriate self-care during the prenatal period.
I have handled Aboriginals women and they come from a different culture language
so before treating childbearing women we should explore the culture of childbearing
women and help the women or discuss everything that she is insecure or nervous
about (Kildea, Improving maternity services for Indigenous, 2016)
Encourage the women and explain each term that women probable to listen to at
antenatal appointments with different health specialists.
Women privacy must be respected and make the situation safe within the hospital or
anywhere women are residing.
Communicate and discuss the women’s perspective about her pregnancy.
Multicultural health workers must assist the women to access the prenatal services
and support to attend the appointments. Provide services, which is similar to women’s
culture and language. Multicultural health workers must communicate with women in
their preferred language (organisation, recommendations on health promotion
interventions for maternal and newborn health , 2015).
Global maternal health 11
Conclusion
I have experienced and learned that we need to work more years to maintain a long-term
relationship with Aboriginals. Many programs implemented by Australia but still it is clear
that the gap between the indigenous and non-ingenious are very extensive and varied. I have
learned in my professional practice that for improvement of the global maternal health,
efficient and effective strategies and policies will need to be constant or sustained for the
long term.
Various countries are working together to improve the condition of the ingenious
childbearing women and immigrants or refugees and to work together to attain equality in
well-being status and life expectancy between Aboriginal and immigrants childbearing
women.
Conclusion
I have experienced and learned that we need to work more years to maintain a long-term
relationship with Aboriginals. Many programs implemented by Australia but still it is clear
that the gap between the indigenous and non-ingenious are very extensive and varied. I have
learned in my professional practice that for improvement of the global maternal health,
efficient and effective strategies and policies will need to be constant or sustained for the
long term.
Various countries are working together to improve the condition of the ingenious
childbearing women and immigrants or refugees and to work together to attain equality in
well-being status and life expectancy between Aboriginal and immigrants childbearing
women.
Global maternal health 12
References
Bronwyn, F. (2010). Reempowering ourselves: Australian aboriginal women. Journal of Women
in Culture and Society, 546-550.
Burns, J., & MacRae, A. (2013). Summary of Indigenous. Journal of Australian Indigenous
HealthReviews, 26-35.
Farib, K. (2016). Canadian Indigenous Women’s Perspectives of Maternal Health and Health
Care Services. Journal of Diversity and Equality in Health and Care, 334-348.
Parker, S. (2014). Choice, culture and confidence’. Journal of key findings from the 2012 having
a baby in Queensland Aboriginal and Torres Strait Islander survey, 14.
Quiggin, R. (2002). Protocols for Producing Indigenous Australian. New York: Performing
Cultures.
Zulfiqar, B. (2013). Global maternal, newborn, and child health—so near and yet so far. Journal
of Medicine, 2226-2235.
canada, H. c. (2011). Understanding and Improving Aboriginal Maternal and Child Health in
Canada. Canada.
Dougherty, G. (2013). International migration to Canada. The post-birth health of mothers and
infants by immigration class, 197-207.
Horton, R. (2019). Indigenous Women’s Maternal Health.New York
Kildea, S. (2016). Improving maternity services for Indigenous. America.
Kildea, S. (2016). Improving maternity services for Indigenous women in Australia. Sydney.
Lisa, M. (2011). Refugee claimant women and barriers to health and social services post-birth.
Canadian Journal of Public Health, 286-290.
References
Bronwyn, F. (2010). Reempowering ourselves: Australian aboriginal women. Journal of Women
in Culture and Society, 546-550.
Burns, J., & MacRae, A. (2013). Summary of Indigenous. Journal of Australian Indigenous
HealthReviews, 26-35.
Farib, K. (2016). Canadian Indigenous Women’s Perspectives of Maternal Health and Health
Care Services. Journal of Diversity and Equality in Health and Care, 334-348.
Parker, S. (2014). Choice, culture and confidence’. Journal of key findings from the 2012 having
a baby in Queensland Aboriginal and Torres Strait Islander survey, 14.
Quiggin, R. (2002). Protocols for Producing Indigenous Australian. New York: Performing
Cultures.
Zulfiqar, B. (2013). Global maternal, newborn, and child health—so near and yet so far. Journal
of Medicine, 2226-2235.
canada, H. c. (2011). Understanding and Improving Aboriginal Maternal and Child Health in
Canada. Canada.
Dougherty, G. (2013). International migration to Canada. The post-birth health of mothers and
infants by immigration class, 197-207.
Horton, R. (2019). Indigenous Women’s Maternal Health.New York
Kildea, S. (2016). Improving maternity services for Indigenous. America.
Kildea, S. (2016). Improving maternity services for Indigenous women in Australia. Sydney.
Lisa, M. (2011). Refugee claimant women and barriers to health and social services post-birth.
Canadian Journal of Public Health, 286-290.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global maternal health 13
Mary, C. (2010). Antenatal care perceptions of pregnant African women attending maternity
services in Melbourne, Australia. Journal of Midwifery, 189-201.
organisation, W. h. (2014). to improve maternal health, barriers that limit access to quality
maternal health services must be identified and addressed at all levels of the health
system.
organisation, W. h. (2015). recommendations on health promotion interventions for maternal and
newborn health.
R. stout, R. (2010). Aboriginal Maternal And Infant Health In Canada.Coloumbia.
Mary, C. (2010). Antenatal care perceptions of pregnant African women attending maternity
services in Melbourne, Australia. Journal of Midwifery, 189-201.
organisation, W. h. (2014). to improve maternal health, barriers that limit access to quality
maternal health services must be identified and addressed at all levels of the health
system.
organisation, W. h. (2015). recommendations on health promotion interventions for maternal and
newborn health.
R. stout, R. (2010). Aboriginal Maternal And Infant Health In Canada.Coloumbia.
Global maternal health 14
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.