Heart failure Assignment PDF
VerifiedAdded on 2021/05/31
|7
|1515
|66
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: HEART FAILURE 1
Heart Failure
Name
Institutional Affiliation
Heart Failure
Name
Institutional Affiliation
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
HEART FAILURE 2
Heart Failure
Borlaug (2014) defines heart failure as the inability of the heart to pump blood to meet
the body’s demand, and this can be due to systolic or diastolic function.
Pathophysiology of Heart Failure
Heart failure results from interplay between systems like the renin angiotensin (RAAS),
sympathetic nervous (SNS) and the natriuretic peptide system (Volpe, Carnovali and
Mastromarino, 2016). The RAAS and SNS are the main mechanisms of heart failure, which
occur after prolonged attempt to maintain circulatory hemostasis by maintaining cardiac output
and peripheral resistance. Volpe et al. (2016) further suggests that prolonged activation of these
systems lead to worsening of heart failure and congestion especially when medical intervention
is not initiated. In the case study, Trevor’s doctor initiated heart failure medication in a bid to
manage it but other underlying conditions accelerated it.
According to Alpert, Lavie, Agrawal, Aggarwal and Kumar (2014), obesity has been
linked to development of heart failure in both men and women. Trevor’s Body Mass Index
(BMI) of 41 suggests obesity. His obesity could have been contributed by his sedentary lifestyle
of less physical activity and high fat diet of steak and chips every weekend. Male gender and
advanced age as Trevor’s imposes a risk factor for developing heart failure. Women are
protected from premature cardiovascular risks (Johansson et al., 2015)
Study conducted by Johansson et al. (2015) found out that the mean age for developing
heart failure for patients with type 2 diabetes as Trevor was about 75 years. 61% of these patients
were men. Having uncontrolled type 2 diabetes as evidenced by Trevor’s high fasting blood
sugar and HbA1c is a risk factor of developing heart failure. Ischemic heart Disease (IHD) is
Heart Failure
Borlaug (2014) defines heart failure as the inability of the heart to pump blood to meet
the body’s demand, and this can be due to systolic or diastolic function.
Pathophysiology of Heart Failure
Heart failure results from interplay between systems like the renin angiotensin (RAAS),
sympathetic nervous (SNS) and the natriuretic peptide system (Volpe, Carnovali and
Mastromarino, 2016). The RAAS and SNS are the main mechanisms of heart failure, which
occur after prolonged attempt to maintain circulatory hemostasis by maintaining cardiac output
and peripheral resistance. Volpe et al. (2016) further suggests that prolonged activation of these
systems lead to worsening of heart failure and congestion especially when medical intervention
is not initiated. In the case study, Trevor’s doctor initiated heart failure medication in a bid to
manage it but other underlying conditions accelerated it.
According to Alpert, Lavie, Agrawal, Aggarwal and Kumar (2014), obesity has been
linked to development of heart failure in both men and women. Trevor’s Body Mass Index
(BMI) of 41 suggests obesity. His obesity could have been contributed by his sedentary lifestyle
of less physical activity and high fat diet of steak and chips every weekend. Male gender and
advanced age as Trevor’s imposes a risk factor for developing heart failure. Women are
protected from premature cardiovascular risks (Johansson et al., 2015)
Study conducted by Johansson et al. (2015) found out that the mean age for developing
heart failure for patients with type 2 diabetes as Trevor was about 75 years. 61% of these patients
were men. Having uncontrolled type 2 diabetes as evidenced by Trevor’s high fasting blood
sugar and HbA1c is a risk factor of developing heart failure. Ischemic heart Disease (IHD) is
HEART FAILURE 3
another risk factor as evidenced by Johansson et al’s. (2015) study. Initial Trevor’s diagnosis was
IHD after a workup by his doctor. Smoking is also a contributing factor.
Trevor experiences signs and symptoms of heart failure like breathlessness that needs
him to be propped up during sleep, easy fatigability on exertion, chest tightness, sweating, being
pale and production of frothy sputum. Clinical assessment reveals features of pleural effusion,
edema on both lower limbs and cardiomegaly. The Electrocardiogram (ECG) changes suggest a
left ventricular hypertrophy and inferior myocardial infarction due to left axis deviation. This is
supported by Vijayakrishnan et al. (2014). They outline these signs and symptoms of heart
failure in addition to high heart rate and jugular venous pressure elevation that Trevor has.
Pharmacology of Heart Failure
Down regulation of the RAAS with angiotensin converting enzyme (ACE) inhibitors and
angiotensin receptor blockers (ARBs), mineralocorticoid antagonists and beta blockers for the
sympathetic nervous system are the mainstream pharmacological interventions of heart failure
(Volpe et al. 2016). Trevor is on ACE inhibitor, enalapril and a beta blocker metoprolol.
Enalapril is hydrolysed to an active metabolite (enalaprilat) in the liver after oral ingestion. Onset
of action is about one hour, with duration of action of 12-24 hours (Tarkiainen et al., 2015). It
then inhibits conversion of angiotensinogen to angiotensin I and II that inhibit salt and water
retention by the kidney. Enalapril is used in combination with furosemide which is a loop
diuretic which blocks the Na-Cl-K transporter encouraging free water loss. It is excreted
unchanged in urine (Bullock and Manias, 2016). Prescribing both digoxin and furosemide to
Trevor means that close monitoring of blood potassium level should be done since hypokalemia
increases digoxin toxicity. Digoxin is a cardiac glycoside that works by inhibiting sodium
another risk factor as evidenced by Johansson et al’s. (2015) study. Initial Trevor’s diagnosis was
IHD after a workup by his doctor. Smoking is also a contributing factor.
Trevor experiences signs and symptoms of heart failure like breathlessness that needs
him to be propped up during sleep, easy fatigability on exertion, chest tightness, sweating, being
pale and production of frothy sputum. Clinical assessment reveals features of pleural effusion,
edema on both lower limbs and cardiomegaly. The Electrocardiogram (ECG) changes suggest a
left ventricular hypertrophy and inferior myocardial infarction due to left axis deviation. This is
supported by Vijayakrishnan et al. (2014). They outline these signs and symptoms of heart
failure in addition to high heart rate and jugular venous pressure elevation that Trevor has.
Pharmacology of Heart Failure
Down regulation of the RAAS with angiotensin converting enzyme (ACE) inhibitors and
angiotensin receptor blockers (ARBs), mineralocorticoid antagonists and beta blockers for the
sympathetic nervous system are the mainstream pharmacological interventions of heart failure
(Volpe et al. 2016). Trevor is on ACE inhibitor, enalapril and a beta blocker metoprolol.
Enalapril is hydrolysed to an active metabolite (enalaprilat) in the liver after oral ingestion. Onset
of action is about one hour, with duration of action of 12-24 hours (Tarkiainen et al., 2015). It
then inhibits conversion of angiotensinogen to angiotensin I and II that inhibit salt and water
retention by the kidney. Enalapril is used in combination with furosemide which is a loop
diuretic which blocks the Na-Cl-K transporter encouraging free water loss. It is excreted
unchanged in urine (Bullock and Manias, 2016). Prescribing both digoxin and furosemide to
Trevor means that close monitoring of blood potassium level should be done since hypokalemia
increases digoxin toxicity. Digoxin is a cardiac glycoside that works by inhibiting sodium
HEART FAILURE 4
potassium pump that reduces the calcium efflux thus decreasing heart rate. It has a long half-life
and excreted via kidneys so Trevor’s renal function tests have to be done.
Using metoprolol has more benefits to Trevor. It has a role in relieving chest pain due to
acute myocardial infarction and also relieve congestion in heart failure. It selectively blocks beta
1 receptors in heart therefore reducing heart rate, contractility and blood pressure. Morphine is
among the drugs prescribed for Trevor’s severe myocardial infarction pain. It is an opioid that
binds to the mu receptor in the central nervous system producing analgesia (Bullock and Manias,
2016). Use of opioids are regulated by the law as part of legal policy. Therefore a legal landscape
for managing opioid addiction and side effects must be there (Davis and Carr, 2017). A
physician must be registered to conduct a narcotic treatment programme. For such laws to be
enforced, a multidisciplinary team that involve health care staff and law enforcers must be
engaged.
potassium pump that reduces the calcium efflux thus decreasing heart rate. It has a long half-life
and excreted via kidneys so Trevor’s renal function tests have to be done.
Using metoprolol has more benefits to Trevor. It has a role in relieving chest pain due to
acute myocardial infarction and also relieve congestion in heart failure. It selectively blocks beta
1 receptors in heart therefore reducing heart rate, contractility and blood pressure. Morphine is
among the drugs prescribed for Trevor’s severe myocardial infarction pain. It is an opioid that
binds to the mu receptor in the central nervous system producing analgesia (Bullock and Manias,
2016). Use of opioids are regulated by the law as part of legal policy. Therefore a legal landscape
for managing opioid addiction and side effects must be there (Davis and Carr, 2017). A
physician must be registered to conduct a narcotic treatment programme. For such laws to be
enforced, a multidisciplinary team that involve health care staff and law enforcers must be
engaged.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
HEART FAILURE 5
References
Borlaug, B. A. (2014). The pathophysiology of heart failure with preserved ejection fraction.
Nature Reviews Cardiology, 11(9), 507.
Volpe, M., Carnovali, M., & Mastromarino, V. (2016). The natriuretic peptides system in the
pathophysiology of heart failure: from molecular basis to treatment. Clinical Science,
130(2), 57-77.
Alpert, M. A., Lavie, C. J., Agrawal, H., Aggarwal, K. B., & Kumar, S. A. (2014). Obesity and
heart failure: epidemiology, pathophysiology, clinical manifestations, and management.
Translational Research, 164(4), 345-356.
Johansson, I., Dahlström, U., Edner, M., Näsman, P., Rydén, L., & Norhammar, A. (2015). Risk
factors, treatment and prognosis in men and women with heart failure with and without
diabetes. Heart, 101(14), 1139-1148.
Vijayakrishnan, R., Steinhubl, S. R., Ng, K., Sun, J., Byrd, R. J., Daar, Z., ... & Stewart, W. F.
(2014). Prevalence of heart failure signs and symptoms in a large primary care population
identified through the use of text and data mining of the electronic health record. Journal
of cardiac failure, 20(7), 459-464.
Tarkiainen, E. K., Tornio, A., Holmberg, M. T., Launiainen, T., Neuvonen, P. J., Backman, J. T.,
& Niemi, M. (2015). Effect of carboxylesterase 1 c. 428G> A single nucleotide variation
on the pharmacokinetics of quinapril and enalapril. British journal of clinical
pharmacology, 80(5), 1131-1138.
Bullock, S. & Manias, E. (2016) Fundamentals of Pharmacology Pearson, Frenchs Forest
References
Borlaug, B. A. (2014). The pathophysiology of heart failure with preserved ejection fraction.
Nature Reviews Cardiology, 11(9), 507.
Volpe, M., Carnovali, M., & Mastromarino, V. (2016). The natriuretic peptides system in the
pathophysiology of heart failure: from molecular basis to treatment. Clinical Science,
130(2), 57-77.
Alpert, M. A., Lavie, C. J., Agrawal, H., Aggarwal, K. B., & Kumar, S. A. (2014). Obesity and
heart failure: epidemiology, pathophysiology, clinical manifestations, and management.
Translational Research, 164(4), 345-356.
Johansson, I., Dahlström, U., Edner, M., Näsman, P., Rydén, L., & Norhammar, A. (2015). Risk
factors, treatment and prognosis in men and women with heart failure with and without
diabetes. Heart, 101(14), 1139-1148.
Vijayakrishnan, R., Steinhubl, S. R., Ng, K., Sun, J., Byrd, R. J., Daar, Z., ... & Stewart, W. F.
(2014). Prevalence of heart failure signs and symptoms in a large primary care population
identified through the use of text and data mining of the electronic health record. Journal
of cardiac failure, 20(7), 459-464.
Tarkiainen, E. K., Tornio, A., Holmberg, M. T., Launiainen, T., Neuvonen, P. J., Backman, J. T.,
& Niemi, M. (2015). Effect of carboxylesterase 1 c. 428G> A single nucleotide variation
on the pharmacokinetics of quinapril and enalapril. British journal of clinical
pharmacology, 80(5), 1131-1138.
Bullock, S. & Manias, E. (2016) Fundamentals of Pharmacology Pearson, Frenchs Forest
HEART FAILURE 6
Davis, C. S., & Carr, D. H. (2017). The Law and Policy of Opioids for Pain Management,
Addiction Treatment, and Overdose Reversal. Ind. Health L. Rev., 14, 1.
Peter, D., Robinson, P., Jordan, M., Lawrence, S., Casey, K., & Salas-Lopez, D. (2015).
Reducing readmissions using teach-back: enhancing patient and family education.
Journal of Nursing Administration, 45(1), 35-42.
Davis, C. S., & Carr, D. H. (2017). The Law and Policy of Opioids for Pain Management,
Addiction Treatment, and Overdose Reversal. Ind. Health L. Rev., 14, 1.
Peter, D., Robinson, P., Jordan, M., Lawrence, S., Casey, K., & Salas-Lopez, D. (2015).
Reducing readmissions using teach-back: enhancing patient and family education.
Journal of Nursing Administration, 45(1), 35-42.
HEART FAILURE 7
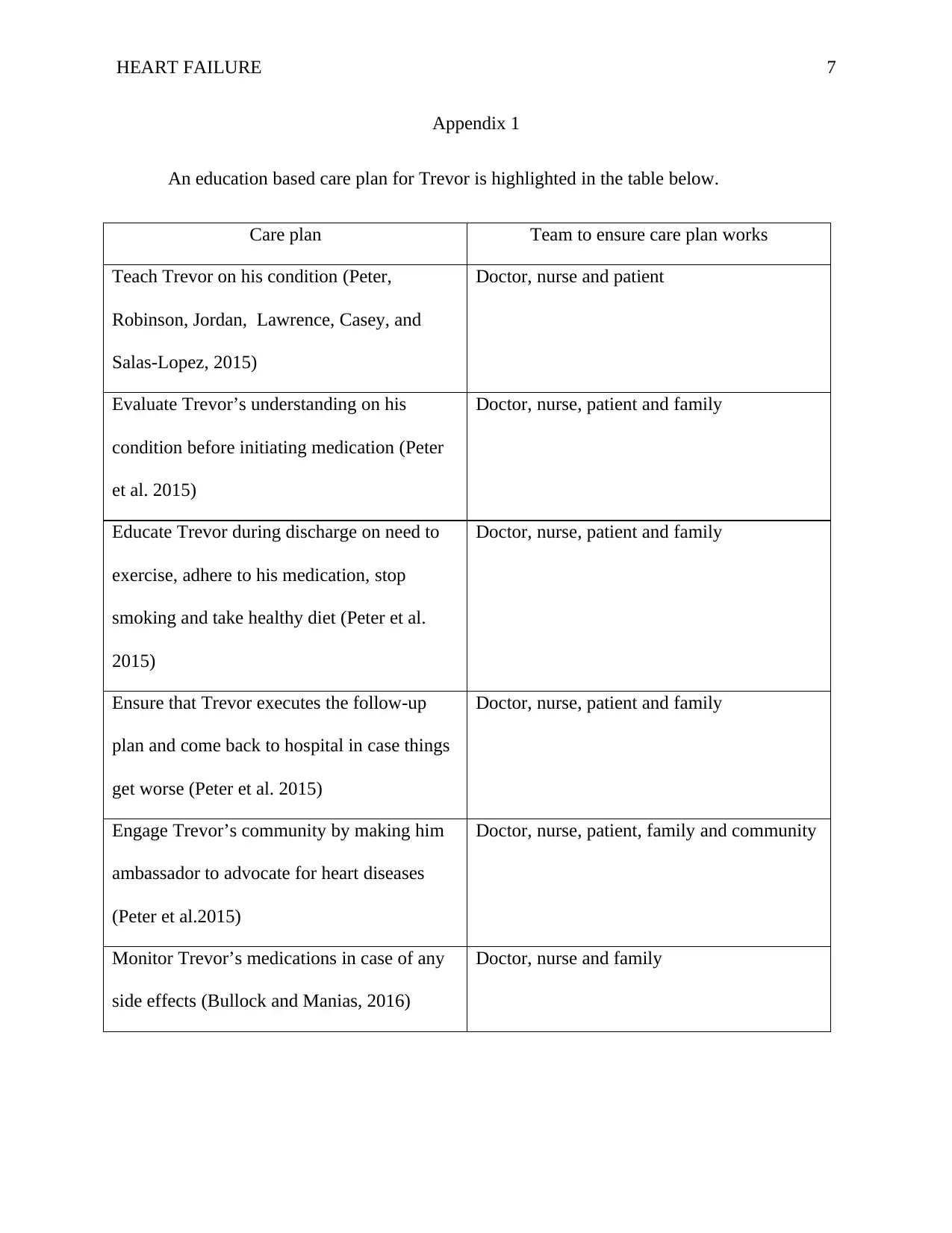
Appendix 1
An education based care plan for Trevor is highlighted in the table below.
Care plan Team to ensure care plan works
Teach Trevor on his condition (Peter,
Robinson, Jordan, Lawrence, Casey, and
Salas-Lopez, 2015)
Doctor, nurse and patient
Evaluate Trevor’s understanding on his
condition before initiating medication (Peter
et al. 2015)
Doctor, nurse, patient and family
Educate Trevor during discharge on need to
exercise, adhere to his medication, stop
smoking and take healthy diet (Peter et al.
2015)
Doctor, nurse, patient and family
Ensure that Trevor executes the follow-up
plan and come back to hospital in case things
get worse (Peter et al. 2015)
Doctor, nurse, patient and family
Engage Trevor’s community by making him
ambassador to advocate for heart diseases
(Peter et al.2015)
Doctor, nurse, patient, family and community
Monitor Trevor’s medications in case of any
side effects (Bullock and Manias, 2016)
Doctor, nurse and family
Appendix 1
An education based care plan for Trevor is highlighted in the table below.
Care plan Team to ensure care plan works
Teach Trevor on his condition (Peter,
Robinson, Jordan, Lawrence, Casey, and
Salas-Lopez, 2015)
Doctor, nurse and patient
Evaluate Trevor’s understanding on his
condition before initiating medication (Peter
et al. 2015)
Doctor, nurse, patient and family
Educate Trevor during discharge on need to
exercise, adhere to his medication, stop
smoking and take healthy diet (Peter et al.
2015)
Doctor, nurse, patient and family
Ensure that Trevor executes the follow-up
plan and come back to hospital in case things
get worse (Peter et al. 2015)
Doctor, nurse, patient and family
Engage Trevor’s community by making him
ambassador to advocate for heart diseases
(Peter et al.2015)
Doctor, nurse, patient, family and community
Monitor Trevor’s medications in case of any
side effects (Bullock and Manias, 2016)
Doctor, nurse and family
1 out of 7
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.