HLTENN013 Nursing Diploma: Implementing Care Plan for Elderly
VerifiedAdded on 2022/11/10
|22
|4372
|263
Report
AI Summary
This assignment presents a nursing care plan focused on implementing and monitoring care for an 85-year-old male, Mr. John Woods, with a complex medical history including heart attack, hypertension, osteoarthritis, gout, depression, anxiety, Alzheimer's dementia, and involuntary urination. The care plan addresses medical diagnoses, theories of aging, and physiological changes associated with aging. It explores primary health services, strategies for dementia and challenging behaviors, oral hygiene, pain management, and complementary therapies. The document details pharmacological and non-pharmacological interventions, including medication, cognitive stimulation therapy, aromatherapy, and reality orientation. It also emphasizes the importance of oral hygiene and pain management strategies, such as the RICE method, for conditions like osteoarthritis. A nursing care plan is included, providing a structured approach to addressing Mr. John's specific needs and improving his quality of life. This student contributed assignment is available on Desklib, a platform offering a range of study tools and resources for students.

IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Name of the Student
Name of the University
Author Note
IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Table of Contents
Part A:..................................................................................................................................2
Medical Diagnosis:..........................................................................................................2
Theory of Ageing:............................................................................................................3
Physiology of Ageing:.....................................................................................................4
Primary health services:...................................................................................................5
Strategies and Interventions for dementia and challenging behaviours:.........................6
Oral Hygiene:...................................................................................................................7
Pain:.................................................................................................................................8
Complementary Therapies:..............................................................................................9
Part B:................................................................................................................................10
Nursing care plan:.........................................................................................................10
References:........................................................................................................................14
Table of Contents
Part A:..................................................................................................................................2
Medical Diagnosis:..........................................................................................................2
Theory of Ageing:............................................................................................................3
Physiology of Ageing:.....................................................................................................4
Primary health services:...................................................................................................5
Strategies and Interventions for dementia and challenging behaviours:.........................6
Oral Hygiene:...................................................................................................................7
Pain:.................................................................................................................................8
Complementary Therapies:..............................................................................................9
Part B:................................................................................................................................10
Nursing care plan:.........................................................................................................10
References:........................................................................................................................14
2IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Part A:
Medical Diagnosis:
This part discusses the medical history of Mr John Woods, who is an eighty-five years
old male. According to the medical reports, he was seen to have experienced from a heart attack
eight years ago. He also suffered from hypertension thirteen years ago. Recent records proved
the presence of osteoarthritis and gout in his left knee. Depression and anxiety were also
diagnosed two years ago. Involuntary urination, along with Alzheimer's dementia, was also
found in his recent medical records. Doctors have asked him to move with a wheelchair. This
condition of him was responsible for his left knee pain. According to the records, Mr John has
been found to have suffered from falling two times in six months. However, he never
experienced any injury from the falls. The above-stated records prove the presence of specific
psychological and physical problems associated with Mr John. Some of the issues include
forgetting to eat at the right time, not recognizing the time for daily activity and holding the left
knee while walking. Also included are getting showers at late night and getting sad while finding
his sister. All these problems were noted during his tenure in hospital. As a result, it can be stated
that his past medical history significantly impacts his present condition.
Part A:
Medical Diagnosis:
This part discusses the medical history of Mr John Woods, who is an eighty-five years
old male. According to the medical reports, he was seen to have experienced from a heart attack
eight years ago. He also suffered from hypertension thirteen years ago. Recent records proved
the presence of osteoarthritis and gout in his left knee. Depression and anxiety were also
diagnosed two years ago. Involuntary urination, along with Alzheimer's dementia, was also
found in his recent medical records. Doctors have asked him to move with a wheelchair. This
condition of him was responsible for his left knee pain. According to the records, Mr John has
been found to have suffered from falling two times in six months. However, he never
experienced any injury from the falls. The above-stated records prove the presence of specific
psychological and physical problems associated with Mr John. Some of the issues include
forgetting to eat at the right time, not recognizing the time for daily activity and holding the left
knee while walking. Also included are getting showers at late night and getting sad while finding
his sister. All these problems were noted during his tenure in hospital. As a result, it can be stated
that his past medical history significantly impacts his present condition.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Theory of Ageing:
Many mechanisms and theories exist for age-related changes and the process of ageing.
Most of the theories that are used to describe the age-related issues consist of three points
(Iwarsson, 2018):
Problems associated with ageing must always be occurring in all members of the
human population.
The age-related problems must be progressive with time. The older the person
grows, the more the effectiveness of the health issue.
The changes must always be an organ dysfunction, ultimately causing the human
body to fail.
There are two theories of ageing; one is a non-programmed theory (based on evolutionary
concepts). The other is a programmed theory (ageing and age-related issues as a result of
biological changes inside the human body). Another method is also available called the damage
or error theory. This theory is more applicable in every case since it states that ageing is a result
of damaging vital parts and tissues with an increase in age (Gladyshev, 2014). According to the
case study provided, medical reports of Mr John mainly states about damaging effects inside his
body. In a broader sense, damage of internal organs, cells and tissues, bones and muscle
destruction are the main reasons for the death of a person at a very high age. This theory can be
related to this study. Mr Woods was suffering from osteoarthritis (bone problem) and a heart
attack history which has made his body weaker with age. He was also found to suffer from
Alzheimer's dementia which is very prevalent in old aged people (Alzheimer, 2015). Brain cells
decay in Alzheimer's disease, which makes the patient lose his consciousness, and this is evident
Theory of Ageing:
Many mechanisms and theories exist for age-related changes and the process of ageing.
Most of the theories that are used to describe the age-related issues consist of three points
(Iwarsson, 2018):
Problems associated with ageing must always be occurring in all members of the
human population.
The age-related problems must be progressive with time. The older the person
grows, the more the effectiveness of the health issue.
The changes must always be an organ dysfunction, ultimately causing the human
body to fail.
There are two theories of ageing; one is a non-programmed theory (based on evolutionary
concepts). The other is a programmed theory (ageing and age-related issues as a result of
biological changes inside the human body). Another method is also available called the damage
or error theory. This theory is more applicable in every case since it states that ageing is a result
of damaging vital parts and tissues with an increase in age (Gladyshev, 2014). According to the
case study provided, medical reports of Mr John mainly states about damaging effects inside his
body. In a broader sense, damage of internal organs, cells and tissues, bones and muscle
destruction are the main reasons for the death of a person at a very high age. This theory can be
related to this study. Mr Woods was suffering from osteoarthritis (bone problem) and a heart
attack history which has made his body weaker with age. He was also found to suffer from
Alzheimer's dementia which is very prevalent in old aged people (Alzheimer, 2015). Brain cells
decay in Alzheimer's disease, which makes the patient lose his consciousness, and this is evident
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
in this study also. Osteoarthritis chances are mainly higher in aged people. This condition is
related to joint problems which primarily ensure the decaying of synovial fluid. The above
problem arises when the genes responsible for the final synthesis of synovial fluid, gets
destroyed (Glyn-Jones, 2015).
Physiology of Ageing:
As per the article was written by McPhee et al., (2016) specific physiological changes
like lower cardiac output, a massive increase in blood pressure, respiratory problems and
immunity disorders occur more with ageing. According to the case study given, Mr John Woods
is eighty-five years old. Therefore, it can be expected that all problems that were found to be
associated with John, were a result of his age or from previous experience. Since he suffered
from myocardial infarction in the past, he had lower cardiac output. This made his circulatory
system to be in danger. Osteoarthritis and gout found in his left knee make the age factor more
evident in causing the illnesses (Greene & Loeser, 2015). These conditions arise when the person
grows old and is having problems with their diet. Alzheimer condition was affecting his sense of
consciousness. As people grow old, they eventually lose the power of memorizing things and
integrating every fact that he or she visualizes (Martschuk & Sporer, 2018). Therefore,
Alzheimer's dementia was affecting him significantly. Cell repair and regeneration processes also
wear off with age. Alzheimer's disease causes the brain neuron (nerve cells) to decay. As the
person grows old, he or she automatically loses the power of cell repair and regeneration. In a
summation, Alzheimer condition was doubling its effect on Mr John. Anxiety with depression
has nothing to be related to age. However, Mr John's, anxiety and depression was carried along
with his previous disease exposures and his current condition. Therefore it can be stated that
in this study also. Osteoarthritis chances are mainly higher in aged people. This condition is
related to joint problems which primarily ensure the decaying of synovial fluid. The above
problem arises when the genes responsible for the final synthesis of synovial fluid, gets
destroyed (Glyn-Jones, 2015).
Physiology of Ageing:
As per the article was written by McPhee et al., (2016) specific physiological changes
like lower cardiac output, a massive increase in blood pressure, respiratory problems and
immunity disorders occur more with ageing. According to the case study given, Mr John Woods
is eighty-five years old. Therefore, it can be expected that all problems that were found to be
associated with John, were a result of his age or from previous experience. Since he suffered
from myocardial infarction in the past, he had lower cardiac output. This made his circulatory
system to be in danger. Osteoarthritis and gout found in his left knee make the age factor more
evident in causing the illnesses (Greene & Loeser, 2015). These conditions arise when the person
grows old and is having problems with their diet. Alzheimer condition was affecting his sense of
consciousness. As people grow old, they eventually lose the power of memorizing things and
integrating every fact that he or she visualizes (Martschuk & Sporer, 2018). Therefore,
Alzheimer's dementia was affecting him significantly. Cell repair and regeneration processes also
wear off with age. Alzheimer's disease causes the brain neuron (nerve cells) to decay. As the
person grows old, he or she automatically loses the power of cell repair and regeneration. In a
summation, Alzheimer condition was doubling its effect on Mr John. Anxiety with depression
has nothing to be related to age. However, Mr John's, anxiety and depression was carried along
with his previous disease exposures and his current condition. Therefore it can be stated that
5IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
many kinds of health problems are associated with age and it increases its effect at older
generations.
many kinds of health problems are associated with age and it increases its effect at older
generations.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Primary health services:
Primary health care services are defined to be the level of entry to a health system. This
service mainly starts from a broad activity range in promotion of health and prevention strategies
ending at treatment and managing acute and chronic conditions. One primary health service
which can be applicable for this issue is appointing a nurse (Biezen et al., 2016). Mr John was
found to be absent from his wheelchair while ambulating. He was seen walking with his bad left
knee. If a general nurse practitioner is appointed to Mr John, then she can take care of him in all
possible ways. The caring processes can be helping Mr John during urinating, having food at
correct times, assisting while walking, taking care of his medicine timings and other cares.
Another primary healthcare service can be appointing Mr John with osteopaths (Steel et al.,
2019). These health professionals provide the patient with physical manipulation of muscles and
bones. Since Mr John is stated to be someone who is suffering from osteoarthritis, osteopaths can
solve the issue faster than general physicians. Osteopaths provide medicines for muscle
relaxation, engages the patient in physical exercises and can also perform surgery if needed.
Although age is a factor during physical exercises, Mr John can be asked to do some stretching
exercises for his knee by his osteopath. These exercises can cure the problem if not brought to a
serious stage.
Primary health services:
Primary health care services are defined to be the level of entry to a health system. This
service mainly starts from a broad activity range in promotion of health and prevention strategies
ending at treatment and managing acute and chronic conditions. One primary health service
which can be applicable for this issue is appointing a nurse (Biezen et al., 2016). Mr John was
found to be absent from his wheelchair while ambulating. He was seen walking with his bad left
knee. If a general nurse practitioner is appointed to Mr John, then she can take care of him in all
possible ways. The caring processes can be helping Mr John during urinating, having food at
correct times, assisting while walking, taking care of his medicine timings and other cares.
Another primary healthcare service can be appointing Mr John with osteopaths (Steel et al.,
2019). These health professionals provide the patient with physical manipulation of muscles and
bones. Since Mr John is stated to be someone who is suffering from osteoarthritis, osteopaths can
solve the issue faster than general physicians. Osteopaths provide medicines for muscle
relaxation, engages the patient in physical exercises and can also perform surgery if needed.
Although age is a factor during physical exercises, Mr John can be asked to do some stretching
exercises for his knee by his osteopath. These exercises can cure the problem if not brought to a
serious stage.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Strategies and Interventions for dementia and challenging behaviours:
There are several strategies and interventions that can be used to tackle the condition of
dementia in patients. These strategies are both pharmacological and non-pharmacological (Dyer
et al., 2018). Pharmacological intervention includes drug intervention, which will be discussed
at first. Anti-dementia drugs can be prescribed by doctors to slow down the progression of
dementia. No radical cure for dementia is available. According to the medication report of Mr
John, he was medicated by Atenolol (anti-dementia drug). This drug helps to reduce heart-related
chest pain during dementia. Other drugs that can be administered are acetylcholine inhibitors and
memantine used for blocking excess glutamate production in brain cells (Wattis et al., 2017).
Non-pharmacological strategies take second place in intervention strategies. Cognitive
Stimulation Therapy can be used to cure people with moderate dementia. Counsellors who
communicate with the patient in a very skilful manner conduct therapeutic sessions. This process
helps the patient to express his problems clearly to the counsellor and eventually get cured by
regaining self-consciousness (Yates et al., 2017). Aromatherapy stands third among the
intervention strategies to tackle dementia. This treatment is a complementary therapeutic
procedure. The process involves usage of smells, bathing and massage to provoke good emotions
in a person facing dementia. Lavender and Melissa balm oil is used in this therapy. As stated in
this case study, Mr John has been recently diagnosed for Alzheimer’s dementia. Certain
conditions including loss of memory, loss of self-consciousness, anxiety, depression and loss of
visual integrative power, are central problems of Mr John. Application of Aromatherapy can
solve the issue in loss of self-consciousness and anxiety (Kim et al., 2019). The fourth strategy is
Reality Orientation strategy. The primary aim of this strategy is to remind the patient of his
present situation. As per the study records, Mr John is never conscious of time. He was found to
Strategies and Interventions for dementia and challenging behaviours:
There are several strategies and interventions that can be used to tackle the condition of
dementia in patients. These strategies are both pharmacological and non-pharmacological (Dyer
et al., 2018). Pharmacological intervention includes drug intervention, which will be discussed
at first. Anti-dementia drugs can be prescribed by doctors to slow down the progression of
dementia. No radical cure for dementia is available. According to the medication report of Mr
John, he was medicated by Atenolol (anti-dementia drug). This drug helps to reduce heart-related
chest pain during dementia. Other drugs that can be administered are acetylcholine inhibitors and
memantine used for blocking excess glutamate production in brain cells (Wattis et al., 2017).
Non-pharmacological strategies take second place in intervention strategies. Cognitive
Stimulation Therapy can be used to cure people with moderate dementia. Counsellors who
communicate with the patient in a very skilful manner conduct therapeutic sessions. This process
helps the patient to express his problems clearly to the counsellor and eventually get cured by
regaining self-consciousness (Yates et al., 2017). Aromatherapy stands third among the
intervention strategies to tackle dementia. This treatment is a complementary therapeutic
procedure. The process involves usage of smells, bathing and massage to provoke good emotions
in a person facing dementia. Lavender and Melissa balm oil is used in this therapy. As stated in
this case study, Mr John has been recently diagnosed for Alzheimer’s dementia. Certain
conditions including loss of memory, loss of self-consciousness, anxiety, depression and loss of
visual integrative power, are central problems of Mr John. Application of Aromatherapy can
solve the issue in loss of self-consciousness and anxiety (Kim et al., 2019). The fourth strategy is
Reality Orientation strategy. The primary aim of this strategy is to remind the patient of his
present situation. As per the study records, Mr John is never conscious of time. He was found to
8IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
be awake late at night and was waiting for lunch. He was also found to having a shower at late at
night. These conditions can be solved by the above-stated strategy (Camargo, Justus & Retzlaff,
2015). As per the medication records of Mr John, it was found that he was administered with two
drugs (Panadol and Atenolol) which reduced pain. Therefore it is evident that he was suffering
from pain which can be a challenging behaviour for applying these therapies. Communication
strategies must be soft since the person is facing dementia. Dementia patients have a very high
chance of getting agitated often. Thus, a proper care for the communication means with the
patient has to be taken.
Oral Hygiene:
According to the case study provided, Mr John needed dental care for both lower and
upper dentures. This factor proved that he had some problems associated with teeth. As a result,
his oral hygiene can be stated to be in bad condition. Eating less or having less food adds fewer
nutrients to his diet. Oral health needs to be taken care of since certain opportunistic infections
have chances of occurrence inside the mouth. These infections can be bacterial or fungal and
take a long time to cure if left untreated (Kholy, Genco, & Van Dyke, 2015). Oral hygiene is not
only based on the good condition of teeth and inner parts of mouth by regular brushing and
rinsing but also having proper food. Therefore, reasonable care has to be taken of Mr John in his
nutrition. Nurses should ensure that he is having his food at right times and brushing his teeth
properly. They must also provide him with proper dental care procedures so that the problems
with upper and lower dentures are cured. Mr John can also be provided with certain nutrients by
injecting liquid food into his body (Denisart et al., 2016). This procedure will be helpful for Mr
John since he does not take his food always. Mouth cleansers can also be incorporated into his
oral hygiene medicine list. This product will keep his mouth clean and fresh after meals and after
be awake late at night and was waiting for lunch. He was also found to having a shower at late at
night. These conditions can be solved by the above-stated strategy (Camargo, Justus & Retzlaff,
2015). As per the medication records of Mr John, it was found that he was administered with two
drugs (Panadol and Atenolol) which reduced pain. Therefore it is evident that he was suffering
from pain which can be a challenging behaviour for applying these therapies. Communication
strategies must be soft since the person is facing dementia. Dementia patients have a very high
chance of getting agitated often. Thus, a proper care for the communication means with the
patient has to be taken.
Oral Hygiene:
According to the case study provided, Mr John needed dental care for both lower and
upper dentures. This factor proved that he had some problems associated with teeth. As a result,
his oral hygiene can be stated to be in bad condition. Eating less or having less food adds fewer
nutrients to his diet. Oral health needs to be taken care of since certain opportunistic infections
have chances of occurrence inside the mouth. These infections can be bacterial or fungal and
take a long time to cure if left untreated (Kholy, Genco, & Van Dyke, 2015). Oral hygiene is not
only based on the good condition of teeth and inner parts of mouth by regular brushing and
rinsing but also having proper food. Therefore, reasonable care has to be taken of Mr John in his
nutrition. Nurses should ensure that he is having his food at right times and brushing his teeth
properly. They must also provide him with proper dental care procedures so that the problems
with upper and lower dentures are cured. Mr John can also be provided with certain nutrients by
injecting liquid food into his body (Denisart et al., 2016). This procedure will be helpful for Mr
John since he does not take his food always. Mouth cleansers can also be incorporated into his
oral hygiene medicine list. This product will keep his mouth clean and fresh after meals and after
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
waking up. On a summary, these are the oral hygiene procedures that can be implemented in the
case of Mr John.
Pain:
The primary evidence of the person is suffering from pain is the condition of his left
knee. According to the case study provided, Mr John has been suffering from a left knee pain
which also made his walking difficult than before. PRN Panadol, Voltaren Emulgel and Atenolol
are all pain-reducing drugs and ointments (Palmer, 2016). These drugs were observed in the
medical records provided for Mr John. As a result, it can be stated that Mr John was
experiencing pain in moderate to severe levels. The fact that Mr John has been suffering from
pain even after medications is evident from his present condition. According to the case study,
Mr John has been found to suffer from left knee gout and osteoarthritis. Therefore, new and more
effective drugs can be administered to reduce his pain. Osteoarthritis has to be solved too to
lessen the physical sufferings from the root cause. RICE (Rest, ice, compression, and elevation)
strategy can be used to cure knee pains which arise from arthritis (Gillette & Merrick, 2018).
This is a prolonged process but much useful because it does not include the use of synthetic
drugs. NSAID (Non-Stimulatory Anti-inflammatory Drugs) can be administered to cure knee
pain problem. These drugs are Ibuprofen and Naproxen (Edwards et al., 2016). They act directly
on the target site and do not cause any inflammation upon action. Therefore this strategy can be
safer for Mr John, who already has gout on left knee.
waking up. On a summary, these are the oral hygiene procedures that can be implemented in the
case of Mr John.
Pain:
The primary evidence of the person is suffering from pain is the condition of his left
knee. According to the case study provided, Mr John has been suffering from a left knee pain
which also made his walking difficult than before. PRN Panadol, Voltaren Emulgel and Atenolol
are all pain-reducing drugs and ointments (Palmer, 2016). These drugs were observed in the
medical records provided for Mr John. As a result, it can be stated that Mr John was
experiencing pain in moderate to severe levels. The fact that Mr John has been suffering from
pain even after medications is evident from his present condition. According to the case study,
Mr John has been found to suffer from left knee gout and osteoarthritis. Therefore, new and more
effective drugs can be administered to reduce his pain. Osteoarthritis has to be solved too to
lessen the physical sufferings from the root cause. RICE (Rest, ice, compression, and elevation)
strategy can be used to cure knee pains which arise from arthritis (Gillette & Merrick, 2018).
This is a prolonged process but much useful because it does not include the use of synthetic
drugs. NSAID (Non-Stimulatory Anti-inflammatory Drugs) can be administered to cure knee
pain problem. These drugs are Ibuprofen and Naproxen (Edwards et al., 2016). They act directly
on the target site and do not cause any inflammation upon action. Therefore this strategy can be
safer for Mr John, who already has gout on left knee.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
Complementary Therapies:
Therapies like massage therapies can be beneficial for Mr John since he suffers from
knee pain (Kabiri, Hasanpour-Dehkordi & Deris, (2018). Aromatherapy, as stated earlier, can
also be used to tackle his dementia condition. Application of Aromatherapy can solve the
problem with loss of self-consciousness and anxiety (Kim et al., 2019).
Massage therapies:
Massage therapies are very effective in curing physical problems. Knee pain is a
condition of osteoarthritis which can be solved by massages. Using appropriate oil for the
massage will help in reducing the friction in between bones and decrease the pain (Kabiri,
Hasanpour-Dehkordi & Deris, 2018).
Aromatherapy:
Eucalyptus radiata oil can be used to as an alternative to direct massage therapy. This oil
has a soothing aroma which helps to relax the patients mind. Therefore it is named as
aromatherapy. This oil is adsorbed as a faster rate which gradually increases the rate of recovery
from osteoarthritic condition (Kim et al., 2019).
Therapies using Choline esterase inhibitors:
Donepezil and glanatamine acts chemical messengers to help the patient in improving his
judgement and memory levels. These drugs help in proving alternate chemical messengers to
continue the proper functioning of nerve cells in turn reducing dementia temporarily (Edwards et
al., 2016).
Complementary Therapies:
Therapies like massage therapies can be beneficial for Mr John since he suffers from
knee pain (Kabiri, Hasanpour-Dehkordi & Deris, (2018). Aromatherapy, as stated earlier, can
also be used to tackle his dementia condition. Application of Aromatherapy can solve the
problem with loss of self-consciousness and anxiety (Kim et al., 2019).
Massage therapies:
Massage therapies are very effective in curing physical problems. Knee pain is a
condition of osteoarthritis which can be solved by massages. Using appropriate oil for the
massage will help in reducing the friction in between bones and decrease the pain (Kabiri,
Hasanpour-Dehkordi & Deris, 2018).
Aromatherapy:
Eucalyptus radiata oil can be used to as an alternative to direct massage therapy. This oil
has a soothing aroma which helps to relax the patients mind. Therefore it is named as
aromatherapy. This oil is adsorbed as a faster rate which gradually increases the rate of recovery
from osteoarthritic condition (Kim et al., 2019).
Therapies using Choline esterase inhibitors:
Donepezil and glanatamine acts chemical messengers to help the patient in improving his
judgement and memory levels. These drugs help in proving alternate chemical messengers to
continue the proper functioning of nerve cells in turn reducing dementia temporarily (Edwards et
al., 2016).
11IMPLEMENT AND MONITOR CARE OF THE OLDER PERSON
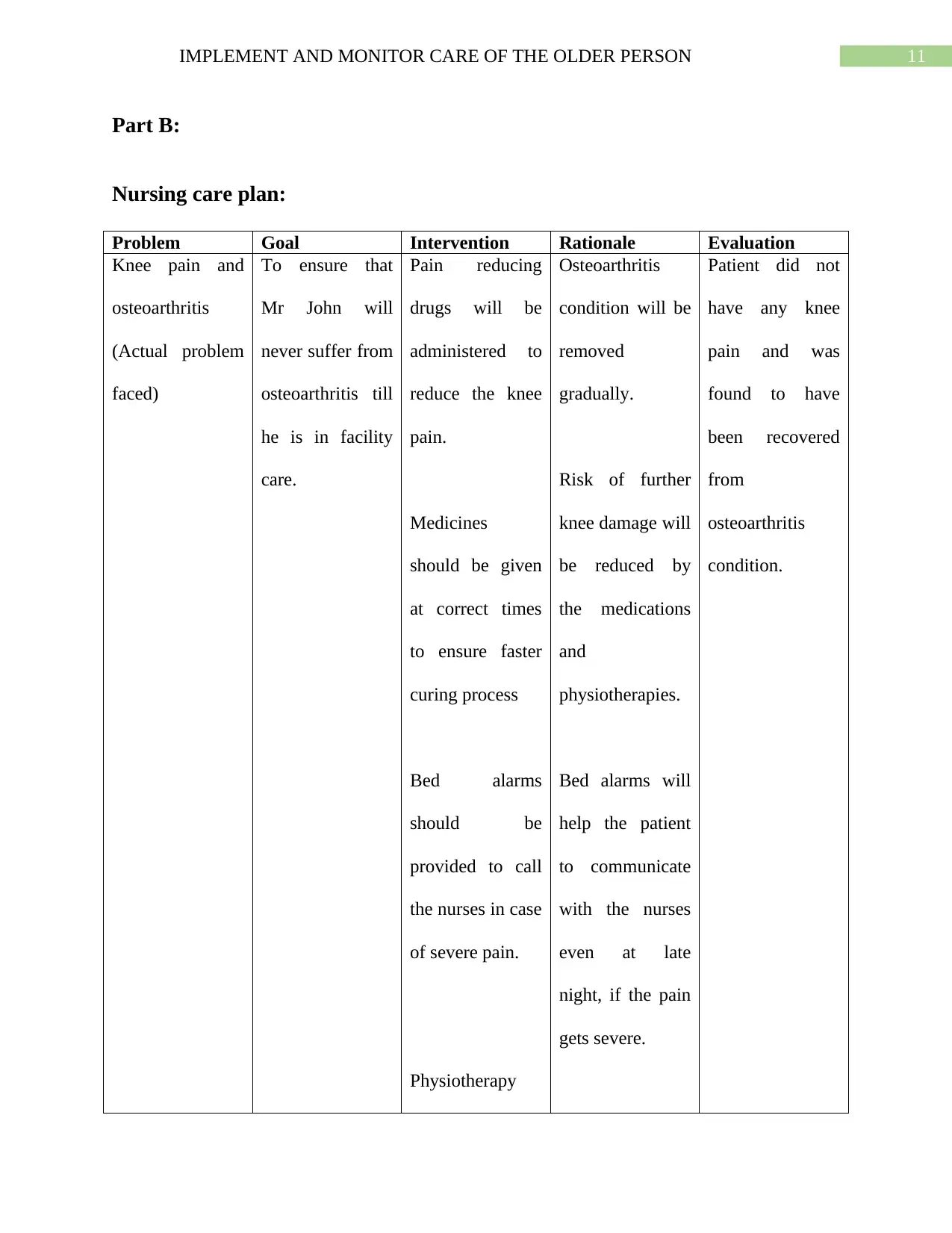
Part B:
Nursing care plan:
Problem Goal Intervention Rationale Evaluation
Knee pain and
osteoarthritis
(Actual problem
faced)
To ensure that
Mr John will
never suffer from
osteoarthritis till
he is in facility
care.
Pain reducing
drugs will be
administered to
reduce the knee
pain.
Medicines
should be given
at correct times
to ensure faster
curing process
Bed alarms
should be
provided to call
the nurses in case
of severe pain.
Physiotherapy
Osteoarthritis
condition will be
removed
gradually.
Risk of further
knee damage will
be reduced by
the medications
and
physiotherapies.
Bed alarms will
help the patient
to communicate
with the nurses
even at late
night, if the pain
gets severe.
Patient did not
have any knee
pain and was
found to have
been recovered
from
osteoarthritis
condition.
Part B:
Nursing care plan:
Problem Goal Intervention Rationale Evaluation
Knee pain and
osteoarthritis
(Actual problem
faced)
To ensure that
Mr John will
never suffer from
osteoarthritis till
he is in facility
care.
Pain reducing
drugs will be
administered to
reduce the knee
pain.
Medicines
should be given
at correct times
to ensure faster
curing process
Bed alarms
should be
provided to call
the nurses in case
of severe pain.
Physiotherapy
Osteoarthritis
condition will be
removed
gradually.
Risk of further
knee damage will
be reduced by
the medications
and
physiotherapies.
Bed alarms will
help the patient
to communicate
with the nurses
even at late
night, if the pain
gets severe.
Patient did not
have any knee
pain and was
found to have
been recovered
from
osteoarthritis
condition.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 22
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.