Early Intervention Services for Infants and Toddles at Risk for Developmental Delays
VerifiedAdded on 2022/01/22
|135
|23968
|427
AI Summary
Thus the family's increased ability to cope with the presence of an exceptional child, and perhaps the child's increased eligibility for employment provide economic and social benefits (NIMH, 2008, pp. 11-12) In the Early Intervention Program (EIP), the primary prevention level is to reduce the occurrence of developmental disability through reduction of risk factors such as low birth weight, malnutrition and family awareness that child development can be influenced by their efforts.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
1
INTRODUCTION
1.1 CONTEXT OF THE STUDY
Early Intervention Services are special services for infants and toddlers
at risk for developmental delays. These services are designed to identify and meet children’s
needs in five developmental areas. These are physical, cognitive, communication, social or
emotional development, sensory and adaptive development. Early intervention includes
provision of services to such children and their families for the purpose of lessening the
effects of the condition. Early intervention can be remedial or preventive in nature-
remediating the existing developmental problems or preventing their occurrence.
Early Intervention Services are effective ways to address the needs of
infants and toddlers with developmental delays or disabilities. To ascertain the eligibility of
the child for early intervention certain screening and diagnostic measures are adopted. Some
children develop more slowly than the others or develop in ways that seem different from
other children. Any deviation from the normal development should be dealt with at the
earliest as it may lead to a developmental delay or the child may be at risk of developing
developmental delays.
The rate of human learning and development is most rapid in the early
years of life. Timing of intervention becomes particularly important when a child runs the
risk of missing an opportunity to learn during a state of maximum readiness. If the most
teachable moments or stages of greatest readiness are not taken advantage of, a child may
have difficulty in learning a particular skill at a later time. It is possible through early
identification and appropriate intervention that children can be helped to reach their
maximum potential.
INTRODUCTION
1.1 CONTEXT OF THE STUDY
Early Intervention Services are special services for infants and toddlers
at risk for developmental delays. These services are designed to identify and meet children’s
needs in five developmental areas. These are physical, cognitive, communication, social or
emotional development, sensory and adaptive development. Early intervention includes
provision of services to such children and their families for the purpose of lessening the
effects of the condition. Early intervention can be remedial or preventive in nature-
remediating the existing developmental problems or preventing their occurrence.
Early Intervention Services are effective ways to address the needs of
infants and toddlers with developmental delays or disabilities. To ascertain the eligibility of
the child for early intervention certain screening and diagnostic measures are adopted. Some
children develop more slowly than the others or develop in ways that seem different from
other children. Any deviation from the normal development should be dealt with at the
earliest as it may lead to a developmental delay or the child may be at risk of developing
developmental delays.
The rate of human learning and development is most rapid in the early
years of life. Timing of intervention becomes particularly important when a child runs the
risk of missing an opportunity to learn during a state of maximum readiness. If the most
teachable moments or stages of greatest readiness are not taken advantage of, a child may
have difficulty in learning a particular skill at a later time. It is possible through early
identification and appropriate intervention that children can be helped to reach their
maximum potential.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
2
Early intervention services also have a significant impact on the parents and siblings of an
exceptional infant or young child. The family of a young exceptional child often feels
disappointed socially isolated and suffers from added stress, frustration, chronic, sorrow,
anxiety and helplessness. The compounded stress with the presence of an exceptional child
may affect the family’s well being which in turn may interfere with the child’s development.
Early intervention can result in parents having improved attitudes about themselves and their
child, improved information and skills for teaching their child and more time for leisure and
enjoyment.
Intervening early is also beneficial to the society at large as it ensures
the child’s developmental and educational gains which will decrease its dependence upon
social institutions. Thus the family’s increased ability to cope with the presence of an
exceptional child, and perhaps the child’s increased eligibility for employment provide
economic as well as social benefits (NIMH, 2008, pp. 11-12)
In Early Intervention Program (EIP), the primary prevention level is to
reduce the occurrence of developmental disability through reduction of risk factors such as
low birth weight, malnutrition and family awareness that child development can be
influenced by their efforts. At a Secondary Prevention level, the goal is to reduce the extent
of manifested childhood disability and shorten its duration. Infant stimulation and
remediation programs operate at this level. In Tertiary Prevention, the aim is to prevent or
reduce complications of disability (physical and behavioral) that lead to a need for
institutionalization. The Program should also enhance the family’s understanding of its
infant’s limitations, strengths and needs, and promote the family’s ability to advocate for its
Early intervention services also have a significant impact on the parents and siblings of an
exceptional infant or young child. The family of a young exceptional child often feels
disappointed socially isolated and suffers from added stress, frustration, chronic, sorrow,
anxiety and helplessness. The compounded stress with the presence of an exceptional child
may affect the family’s well being which in turn may interfere with the child’s development.
Early intervention can result in parents having improved attitudes about themselves and their
child, improved information and skills for teaching their child and more time for leisure and
enjoyment.
Intervening early is also beneficial to the society at large as it ensures
the child’s developmental and educational gains which will decrease its dependence upon
social institutions. Thus the family’s increased ability to cope with the presence of an
exceptional child, and perhaps the child’s increased eligibility for employment provide
economic as well as social benefits (NIMH, 2008, pp. 11-12)
In Early Intervention Program (EIP), the primary prevention level is to
reduce the occurrence of developmental disability through reduction of risk factors such as
low birth weight, malnutrition and family awareness that child development can be
influenced by their efforts. At a Secondary Prevention level, the goal is to reduce the extent
of manifested childhood disability and shorten its duration. Infant stimulation and
remediation programs operate at this level. In Tertiary Prevention, the aim is to prevent or
reduce complications of disability (physical and behavioral) that lead to a need for
institutionalization. The Program should also enhance the family’s understanding of its
infant’s limitations, strengths and needs, and promote the family’s ability to advocate for its
3
infant. For effective intervention, a multi-disciplinary team approach has been advocated, the
composition of which may vary depending on the available resources.
1.2 NEED AND SIGNIFICANCE OF STUDY
The rationale behind Early Intervention is that much of what the child
learns as an infant or a very young child is important to the development of later
competencies. This implies that early learning is foundation to later learning which is one of
the principles of child development.
This gets ample support from Piaget’s theory of Cognitive
development in which intelligence is depicted as a developmental phenomenon and an
adaptive process. The basic behavior patterns or schemes which are acquired, repeated,
integrated or in combination form complex response patterns which help in achieving higher
cognitive proficiency. He also considered this early age of 0-2 as Sensory-motor period.
Hence the early age period is the most appropriate period to lay the basic foundations for
further development and learning. The early childhood period is considered a critical period
and early intervention programmes utilize these periods to the best advantage of the child.
(NIMH, 2008, p.13)
Early Intervention Services include a range of healthcare,
developmental, therapeutic, social and cultural services for young children and their families.
Children grow very rapidly in early years and any stimulation at this stage helps to promote a
child’s optimum growth and development.
Thus it is presumed that early intervention provides the brain a second
chance to revisit some of the developmental stages which have once been omitted or
incomplete.
infant. For effective intervention, a multi-disciplinary team approach has been advocated, the
composition of which may vary depending on the available resources.
1.2 NEED AND SIGNIFICANCE OF STUDY
The rationale behind Early Intervention is that much of what the child
learns as an infant or a very young child is important to the development of later
competencies. This implies that early learning is foundation to later learning which is one of
the principles of child development.
This gets ample support from Piaget’s theory of Cognitive
development in which intelligence is depicted as a developmental phenomenon and an
adaptive process. The basic behavior patterns or schemes which are acquired, repeated,
integrated or in combination form complex response patterns which help in achieving higher
cognitive proficiency. He also considered this early age of 0-2 as Sensory-motor period.
Hence the early age period is the most appropriate period to lay the basic foundations for
further development and learning. The early childhood period is considered a critical period
and early intervention programmes utilize these periods to the best advantage of the child.
(NIMH, 2008, p.13)
Early Intervention Services include a range of healthcare,
developmental, therapeutic, social and cultural services for young children and their families.
Children grow very rapidly in early years and any stimulation at this stage helps to promote a
child’s optimum growth and development.
Thus it is presumed that early intervention provides the brain a second
chance to revisit some of the developmental stages which have once been omitted or
incomplete.
4
Therefore the basis for early intervention is that by providing a
stimulating environment, creating appropriate opportunities for learning and providing
support to the families, young children who are at risk or already have developmental delays
could be helped.
Intervention encourages and helps parents to gain skills in observing
their infants and young children, and in understanding that children learn from their play.
Parents are helped to become aware of materials and activities that are suitable for children at
each stage of development, and the community resources and services are made available to
them as they work with their children.
The child is considered to be “at risk” because of adverse genetic,
prenatal, perinatal, neonatal or environmental influences that may lead to subsequent
development of a handicap or developmental deviation. Intelligence and other human
capacities are not fixed at birth, but rather they are shaped to some extent by environmental
influences and through learning. Handicapping conditions may interfere with development
and learning due to which disability becomes serious and secondary handicaps may appear.
Parents need special assistance in establishing meaningful patterns of parenting a
handicapping conditions or a child at risk. Parental involvement is considered to be a key
element in the success of early intervention programs. Parental involvement is necessary in
providing adequate care, stimulation and training for their child during critical years when
basic developmental skills should be established.
Many reasons have been offered for why parents should be involved in
early intervention programs. (Bristol & Gallagher, 1982; Peterson, 1987; Turnbull &
Turnbull, 1986)
Therefore the basis for early intervention is that by providing a
stimulating environment, creating appropriate opportunities for learning and providing
support to the families, young children who are at risk or already have developmental delays
could be helped.
Intervention encourages and helps parents to gain skills in observing
their infants and young children, and in understanding that children learn from their play.
Parents are helped to become aware of materials and activities that are suitable for children at
each stage of development, and the community resources and services are made available to
them as they work with their children.
The child is considered to be “at risk” because of adverse genetic,
prenatal, perinatal, neonatal or environmental influences that may lead to subsequent
development of a handicap or developmental deviation. Intelligence and other human
capacities are not fixed at birth, but rather they are shaped to some extent by environmental
influences and through learning. Handicapping conditions may interfere with development
and learning due to which disability becomes serious and secondary handicaps may appear.
Parents need special assistance in establishing meaningful patterns of parenting a
handicapping conditions or a child at risk. Parental involvement is considered to be a key
element in the success of early intervention programs. Parental involvement is necessary in
providing adequate care, stimulation and training for their child during critical years when
basic developmental skills should be established.
Many reasons have been offered for why parents should be involved in
early intervention programs. (Bristol & Gallagher, 1982; Peterson, 1987; Turnbull &
Turnbull, 1986)
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
5
The following rationales are frequently offered as to why it is
important to involve parents:
Parents are responsible for the welfare of their children. Most parents want a voice in how
their child is educated because they are ultimately responsible for the child's well-being
and welfare.
Early intervention programs which involve parents result in greater benefits for children.
It is often alleged that, by involving the family (i.e., the people with whom the child
spends the majority of his or her time), the benefits of early intervention programs will be
strengthened.
Parent involvement activities benefit parents and family members. By helping parents
understand their child's current situation and potential and how to manage their child's
needs and demands, it is often claimed that parents will have reduced levels of stress,
more satisfaction, and a more realistic perception of what is possible and desirable.
Participation in early intervention programs also exposes parents to other agencies and
services which may be useful to them in other aspects of their life.
By involving parents, the same outcomes can be achieved at less cost. Early intervention
services can be very expensive. If parents can be used to deliver a portion of the services,
it is often suggested that the costs of early intervention can be dramatically reduced.
The benefits of early intervention are maintained better if parents are involved. It is often
argued that the involvement of parents will reinforce and maintain the benefits of early
intervention because they are the only ones who will be consistently involved with the
The following rationales are frequently offered as to why it is
important to involve parents:
Parents are responsible for the welfare of their children. Most parents want a voice in how
their child is educated because they are ultimately responsible for the child's well-being
and welfare.
Early intervention programs which involve parents result in greater benefits for children.
It is often alleged that, by involving the family (i.e., the people with whom the child
spends the majority of his or her time), the benefits of early intervention programs will be
strengthened.
Parent involvement activities benefit parents and family members. By helping parents
understand their child's current situation and potential and how to manage their child's
needs and demands, it is often claimed that parents will have reduced levels of stress,
more satisfaction, and a more realistic perception of what is possible and desirable.
Participation in early intervention programs also exposes parents to other agencies and
services which may be useful to them in other aspects of their life.
By involving parents, the same outcomes can be achieved at less cost. Early intervention
services can be very expensive. If parents can be used to deliver a portion of the services,
it is often suggested that the costs of early intervention can be dramatically reduced.
The benefits of early intervention are maintained better if parents are involved. It is often
argued that the involvement of parents will reinforce and maintain the benefits of early
intervention because they are the only ones who will be consistently involved with the
6
child. Responsibilities of agencies may change, the family may move, funding may be
cut, but the child will always be a member of his/her family.
Hence, it is important, that parents of children with developmental
disabilities be aware and be fully involved in early intervention services. In this context, there
is a need to study about the awareness and involvement of parents in early intervention, its
services and benefits for their children suffering from developmental disabilities.
1.3 SCOPE OF THE STUDY
This study is expected to throw light on the need for parental
awareness and involvement in early intervention. The advantage of examining the parental
awareness and involvement on different aspects of early intervention are that they can
increase the knowledge base regarding parental awareness and involvement. Another
advantage of the study is that, recommendations can be made to early intervention centers
and families on the need to be aware and involved in various aspects of early intervention for
the benefit of disabled children. It is hoped that, the findings of the study will help the
administrators and therapists of early intervention centers to create awareness among the
parents on the importance of parental involvement in early intervention. The investigator
expects the results of the study would be of use to all, concerned with the education, training
and development of children with developmental disabilities.
1.4 STATEMENT OF THE PROBLEM
The study aims in ascertaining the level of awareness and involvement
of parents on early Intervention of children with developmental disabilities. Therefore, the
study is entitled as “Awareness and Involvement of Parents in Early Intervention of
Children with Developmental disabilities”
child. Responsibilities of agencies may change, the family may move, funding may be
cut, but the child will always be a member of his/her family.
Hence, it is important, that parents of children with developmental
disabilities be aware and be fully involved in early intervention services. In this context, there
is a need to study about the awareness and involvement of parents in early intervention, its
services and benefits for their children suffering from developmental disabilities.
1.3 SCOPE OF THE STUDY
This study is expected to throw light on the need for parental
awareness and involvement in early intervention. The advantage of examining the parental
awareness and involvement on different aspects of early intervention are that they can
increase the knowledge base regarding parental awareness and involvement. Another
advantage of the study is that, recommendations can be made to early intervention centers
and families on the need to be aware and involved in various aspects of early intervention for
the benefit of disabled children. It is hoped that, the findings of the study will help the
administrators and therapists of early intervention centers to create awareness among the
parents on the importance of parental involvement in early intervention. The investigator
expects the results of the study would be of use to all, concerned with the education, training
and development of children with developmental disabilities.
1.4 STATEMENT OF THE PROBLEM
The study aims in ascertaining the level of awareness and involvement
of parents on early Intervention of children with developmental disabilities. Therefore, the
study is entitled as “Awareness and Involvement of Parents in Early Intervention of
Children with Developmental disabilities”
7
1.5 OPERATIONAL DEFINITIONS
Definitions of the important terms used in this study are given below:-
AWARENESS
Knowledge or perception of a situation or fact.
INVOLVEMENT
To cause someone to be associated with someone or something.
In this study, ‘Parental involvement’ means the active role of parents in their child’s early
intervention program.
PARENTS
Father or Mother of children with developmental disabilities.
EARLY INTERVENTION
Early Intervention is a term, which broadly refers to a wide range of experiences and supports
provided to children, parents and families during the pregnancy, infancy and early childhood
period of development.
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Developmental disabilities are a group of conditions due to impairment in physical, learning,
language or behavior areas. These conditions begin during the developmental period, may
impact day to day functioning and usually last through a person’s life.
1.5 OPERATIONAL DEFINITIONS
Definitions of the important terms used in this study are given below:-
AWARENESS
Knowledge or perception of a situation or fact.
INVOLVEMENT
To cause someone to be associated with someone or something.
In this study, ‘Parental involvement’ means the active role of parents in their child’s early
intervention program.
PARENTS
Father or Mother of children with developmental disabilities.
EARLY INTERVENTION
Early Intervention is a term, which broadly refers to a wide range of experiences and supports
provided to children, parents and families during the pregnancy, infancy and early childhood
period of development.
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Developmental disabilities are a group of conditions due to impairment in physical, learning,
language or behavior areas. These conditions begin during the developmental period, may
impact day to day functioning and usually last through a person’s life.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
1.6 OBJECTIVES OF THE STUDY
General Objective
To find out the level of awareness and involvement of parents in Early Intervention of
children with developmental disabilities.
Specific Objectives
1. To find out the level of awareness of parents on the importance of Early Intervention.
2. To find out the level of awareness of parents on the importance of parental involvement
in Early Intervention.
3. To find out the level of awareness of parents on developmental disabilities.
4. To find out the level of awareness of parents regarding the Early Intervention services.
5. To find out the level of awareness of parents on Early Intervention with respect to Socio
Demographic Variables.
6. To find out the level of involvement of parents in their child’s Early Intervention
Program.
7. To find out the level of involvement of parents with respect to certain socio-demographic
variables.
1.7 HYPOTHESIS
On the basis of the objectives of the study the researcher developed the following
hypothesis.
There is no significant difference in the level of awareness of parents on early
intervention with respect to selected Socio-demographic variables.
1.6 OBJECTIVES OF THE STUDY
General Objective
To find out the level of awareness and involvement of parents in Early Intervention of
children with developmental disabilities.
Specific Objectives
1. To find out the level of awareness of parents on the importance of Early Intervention.
2. To find out the level of awareness of parents on the importance of parental involvement
in Early Intervention.
3. To find out the level of awareness of parents on developmental disabilities.
4. To find out the level of awareness of parents regarding the Early Intervention services.
5. To find out the level of awareness of parents on Early Intervention with respect to Socio
Demographic Variables.
6. To find out the level of involvement of parents in their child’s Early Intervention
Program.
7. To find out the level of involvement of parents with respect to certain socio-demographic
variables.
1.7 HYPOTHESIS
On the basis of the objectives of the study the researcher developed the following
hypothesis.
There is no significant difference in the level of awareness of parents on early
intervention with respect to selected Socio-demographic variables.
9
There is no significant difference in the level of involvement of parents in early
intervention with respect to selected Socio demographic variables.
1.8 METHODOLOGY IN BRIEF
Methodology implies to the methods the researcher intend to use to collect data. It is the
systematic theoretical analysis of the methods applied to a field of study.
Research Design
The present study attempts to reveal the awareness and involvement of parents in early
intervention of children with developmental disabilities. Descriptive Survey Design is chosen
for the present study.
Population
The study is conducted on a sample of parents of 110 children with developmental disabilities
receiving early intervention from various early intervention centres in Kottayam and
Ernakulam districts.
Sampling Method
Random Sampling technique will be used to select the sample. The study will be conducted
on a sample of parents of 110 children with developmental disabilities.
Tools
The tools for data collection are
Demographic data sheet
Awareness Inventory prepared by the researcher.
Parent Involvement Scale prepared by the researcher.
There is no significant difference in the level of involvement of parents in early
intervention with respect to selected Socio demographic variables.
1.8 METHODOLOGY IN BRIEF
Methodology implies to the methods the researcher intend to use to collect data. It is the
systematic theoretical analysis of the methods applied to a field of study.
Research Design
The present study attempts to reveal the awareness and involvement of parents in early
intervention of children with developmental disabilities. Descriptive Survey Design is chosen
for the present study.
Population
The study is conducted on a sample of parents of 110 children with developmental disabilities
receiving early intervention from various early intervention centres in Kottayam and
Ernakulam districts.
Sampling Method
Random Sampling technique will be used to select the sample. The study will be conducted
on a sample of parents of 110 children with developmental disabilities.
Tools
The tools for data collection are
Demographic data sheet
Awareness Inventory prepared by the researcher.
Parent Involvement Scale prepared by the researcher.
10
Data Collection Procedure
All the tools are developed by the investigator and administered on the sample. The
investigator personally contacted the authorities of Early Intervention Centres. The scope of
the study was briefly explained to them and their permission was sought before collecting
data from parents. Permission of parents was also sought either directly or indirectly through
the authorities. The inventories were distributed and the guidelines and instruction on filling
the inventory were given to the parents by the investigator. The parents filled in the general
data sheet, Parental Awareness Inventory and Parental Involvement Inventory. The collected
data were analyzed with respect to a number of background variables. The following
statistical techniques were used for this purpose:
1) Computation of frequencies and percentages
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of‘t’ value to test the significance of difference between the means of two
groups of data.
4) One Way Analysis of Variance to test the significance of difference between the means of
three or more groups of data
1.9 DELIMITATION
The study is delimited to
Parents of children with developmental disabilities receiving early intervention services
from centres of Kottayam and Ernakulam district.
Data Collection Procedure
All the tools are developed by the investigator and administered on the sample. The
investigator personally contacted the authorities of Early Intervention Centres. The scope of
the study was briefly explained to them and their permission was sought before collecting
data from parents. Permission of parents was also sought either directly or indirectly through
the authorities. The inventories were distributed and the guidelines and instruction on filling
the inventory were given to the parents by the investigator. The parents filled in the general
data sheet, Parental Awareness Inventory and Parental Involvement Inventory. The collected
data were analyzed with respect to a number of background variables. The following
statistical techniques were used for this purpose:
1) Computation of frequencies and percentages
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of‘t’ value to test the significance of difference between the means of two
groups of data.
4) One Way Analysis of Variance to test the significance of difference between the means of
three or more groups of data
1.9 DELIMITATION
The study is delimited to
Parents of children with developmental disabilities receiving early intervention services
from centres of Kottayam and Ernakulam district.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
11
Sample: The size of the sample studied was only 110 and it was taken from only 2
districts of Kerala. A larger sample selected from various other districts could have given
scope for wider generalization to the findings. Moreover, the population being scattered,
did not permit the investigator to increase the sample size.
Time: The present study has been conducted within a limited period of time
Sample: The size of the sample studied was only 110 and it was taken from only 2
districts of Kerala. A larger sample selected from various other districts could have given
scope for wider generalization to the findings. Moreover, the population being scattered,
did not permit the investigator to increase the sample size.
Time: The present study has been conducted within a limited period of time
12
REVIEW OF RELATED LITERATURE
2.1 INTRODUCTION
Literature in Research Methodology refers to the knowledge of a
particular area of investigation of any discipline which includes both theory and practice.
Review means to organize the knowledge of the specific area of research to evolve an edifice
of knowledge, to show that our study would be an addition to that particular field. The task of
review of literature is highly creative and tedious, as the researcher has to synthesize the
available knowledge of the field in a unique way to provide the rationale for his study.
A thorough sophisticated literature review is the foundation and
inspiration for substantial, useful research. Literature review is the written systematic
summary of the research which is conducted on a particular topic. Review of literature is
important any other component of the research process.
When every piece of the ongoing research is connected with the work
already done, it attains an overall relevance and purpose. Review of literature thus becomes a
link between the research proposed and the study already conducted. It conveys to the reader
about those aspects that have already been established or conclude by other authors, and also
give a chance to the reader to appreciate the evidence that has already been collected by
previous research and thus presents the current research work in the right perspective.
A review of literature highlights the differences in opinion,
contradictory findings or evidence and the various explanations given for the conclusions and
REVIEW OF RELATED LITERATURE
2.1 INTRODUCTION
Literature in Research Methodology refers to the knowledge of a
particular area of investigation of any discipline which includes both theory and practice.
Review means to organize the knowledge of the specific area of research to evolve an edifice
of knowledge, to show that our study would be an addition to that particular field. The task of
review of literature is highly creative and tedious, as the researcher has to synthesize the
available knowledge of the field in a unique way to provide the rationale for his study.
A thorough sophisticated literature review is the foundation and
inspiration for substantial, useful research. Literature review is the written systematic
summary of the research which is conducted on a particular topic. Review of literature is
important any other component of the research process.
When every piece of the ongoing research is connected with the work
already done, it attains an overall relevance and purpose. Review of literature thus becomes a
link between the research proposed and the study already conducted. It conveys to the reader
about those aspects that have already been established or conclude by other authors, and also
give a chance to the reader to appreciate the evidence that has already been collected by
previous research and thus presents the current research work in the right perspective.
A review of literature highlights the differences in opinion,
contradictory findings or evidence and the various explanations given for the conclusions and
13
differences by various authors. Such analysis can lead to new possibility that can be
researched upon in the current study. Thus review of literature is an inevitable part of a
Research.
2.2 REVIEW OF RELATED LITERATURE
Early Intervention is defined by Stephens and Tauber (2001) in two
parts; early refers to the most critical period of a child’s development between birth and three
years of age. Intervention refers to programme implementation designed to maintain or
enhance the child’s development in natural environments and as a member of a family.
Dunst (2007) proposed a definition of early (childhood) intervention as
the experiences and opportunities afforded to infants and toddlers (and preschoolers) with
disabilities by the children’s parents and other primary caregivers (including service
providers) that are intended to promote the children’s acquisition and use of behavioral
competencies to shape and influence their prosocial interactions with people and objects.
Early childhood intervention by definition is relationship-based as
families work together with the practitioners as equal partners to design a service plan that is
responsive to family priorities and child needs. Parents and caregivers are the experts on the
unique characteristics of the child and invaluable informants on the child’s strengths,
interests, and abilities, as well as the naturally occurring learning opportunities that exist in
the child and family’s life. The contemporary model of early childhood intervention is
family-centered, and these adult-to-adult interactions between caregivers and professionals
differences by various authors. Such analysis can lead to new possibility that can be
researched upon in the current study. Thus review of literature is an inevitable part of a
Research.
2.2 REVIEW OF RELATED LITERATURE
Early Intervention is defined by Stephens and Tauber (2001) in two
parts; early refers to the most critical period of a child’s development between birth and three
years of age. Intervention refers to programme implementation designed to maintain or
enhance the child’s development in natural environments and as a member of a family.
Dunst (2007) proposed a definition of early (childhood) intervention as
the experiences and opportunities afforded to infants and toddlers (and preschoolers) with
disabilities by the children’s parents and other primary caregivers (including service
providers) that are intended to promote the children’s acquisition and use of behavioral
competencies to shape and influence their prosocial interactions with people and objects.
Early childhood intervention by definition is relationship-based as
families work together with the practitioners as equal partners to design a service plan that is
responsive to family priorities and child needs. Parents and caregivers are the experts on the
unique characteristics of the child and invaluable informants on the child’s strengths,
interests, and abilities, as well as the naturally occurring learning opportunities that exist in
the child and family’s life. The contemporary model of early childhood intervention is
family-centered, and these adult-to-adult interactions between caregivers and professionals
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
14
can significantly influence the family’s well-being, parenting skills, and positive parental
perceptions of their child’s behavior (Dunst, 2007).
Derrington et al., (2003) stated early intervention is a term commonly
used to encompass a system of services delivered to children with, or at risk for,
developmental delays, before their third birthday.
2.2.1 STUDIES RELATED TO IMPORTANCE OF EARLY INTERVENTION
Derrington et al., (2003) conducted a study on the effectiveness of early
intervention services reported that early experiences and stimulation are critical for optimal
brain development, suggesting the considerable capacity of early intervention to affect the
child. The brain develops by an "experience-dependent" process, where experience activates
certain pathways in the brain and not others. The study indicates that early intervention
ameliorates or prevents developmental delays and gives support to families of children with
delays. Reasons given are:
Neurological evidence supports the provision of intervention early in a child’s life
when the brain is creating connections that will later sub serve all behavior and skills.
Research shows that early intervention during the postnatal period, infancy,
toddlerhood, and early childhood is effective for pre-term, Low Birth Weight and
Very Low Birth Weight children; children with Down Syndrome, cerebral palsy,
expressive language delays, and visual and hearing impairments. It enhances short-
term and long-term physical, cognitive, behavioral, social, emotional, and language
can significantly influence the family’s well-being, parenting skills, and positive parental
perceptions of their child’s behavior (Dunst, 2007).
Derrington et al., (2003) stated early intervention is a term commonly
used to encompass a system of services delivered to children with, or at risk for,
developmental delays, before their third birthday.
2.2.1 STUDIES RELATED TO IMPORTANCE OF EARLY INTERVENTION
Derrington et al., (2003) conducted a study on the effectiveness of early
intervention services reported that early experiences and stimulation are critical for optimal
brain development, suggesting the considerable capacity of early intervention to affect the
child. The brain develops by an "experience-dependent" process, where experience activates
certain pathways in the brain and not others. The study indicates that early intervention
ameliorates or prevents developmental delays and gives support to families of children with
delays. Reasons given are:
Neurological evidence supports the provision of intervention early in a child’s life
when the brain is creating connections that will later sub serve all behavior and skills.
Research shows that early intervention during the postnatal period, infancy,
toddlerhood, and early childhood is effective for pre-term, Low Birth Weight and
Very Low Birth Weight children; children with Down Syndrome, cerebral palsy,
expressive language delays, and visual and hearing impairments. It enhances short-
term and long-term physical, cognitive, behavioral, social, emotional, and language
15
development and reduces the incidence of developmental delays for biologically at
risk children.
Effective intervention can be carried out by parents of various backgrounds in the
home as well as by professionals in a centre.
Early intervention assists the family in obtaining adaptive devices to support the
child’s participation in everyday activities.
Early intervention provides different sources of social support to the family, which
reduces the impact of stress on the family and enhances parent-child interaction and
consequently child development.
Experiences early in life are especially crucial in organizing the
brain's basic structures, as they create the neural foundation for all subsequent
development and behavior (Greenough et al., 1987)
Majnemer (1998) conducted a study on benefits of early intervention
for children with developmental disabilities reported that early Intervention are programmes
designed to enhance the developmental competence of participants and to prevent or
minimize developmental delays. Children targeted for early intervention may either include
environmentally or biologically vulnerable children, or those with established developmental
deficits.
The developmental period of a child has critical importance for learning
and it is even more so in case of a disabled child. The earlier the disability is detected, the
easier it is to effectively help the child both medically and educationally. (Joubish, et al.,
2015)
development and reduces the incidence of developmental delays for biologically at
risk children.
Effective intervention can be carried out by parents of various backgrounds in the
home as well as by professionals in a centre.
Early intervention assists the family in obtaining adaptive devices to support the
child’s participation in everyday activities.
Early intervention provides different sources of social support to the family, which
reduces the impact of stress on the family and enhances parent-child interaction and
consequently child development.
Experiences early in life are especially crucial in organizing the
brain's basic structures, as they create the neural foundation for all subsequent
development and behavior (Greenough et al., 1987)
Majnemer (1998) conducted a study on benefits of early intervention
for children with developmental disabilities reported that early Intervention are programmes
designed to enhance the developmental competence of participants and to prevent or
minimize developmental delays. Children targeted for early intervention may either include
environmentally or biologically vulnerable children, or those with established developmental
deficits.
The developmental period of a child has critical importance for learning
and it is even more so in case of a disabled child. The earlier the disability is detected, the
easier it is to effectively help the child both medically and educationally. (Joubish, et al.,
2015)
16
Landesman Ramey and Ramey (1999) studied the effects of early
experience and early intervention and stated that for 4 decades, vigorous efforts have been
based on the premise that early intervention for children of poverty and, more recently, for
children with developmental disabilities can yield significant improvements in cognitive,
academic, and social outcomes. The study briefly summarized the history of those efforts and
presented a conceptual framework to understand the design, research, and policy relevance of
these early interventions. This framework, biosocial developmental contextualism, derives
from social ecology, developmental systems theory, developmental epidemiology, and
developmental neurobiology. Those integrative perspective predicts that fragmented, weak
efforts in early intervention are not likely to succeed, whereas intensive, high-quality,
ecologically pervasive interventions can and do. Relevant evidence was also summarized in 6
principles about efficacy of early intervention. The public policy challenge in early
intervention is to contain costs by more precisely targeting early interventions to those who
most need and benefit from these interventions. The empirical evidence on biobehavioral
effects of early experience and early intervention has direct relevance to federal and state
policy development and resource allocation.
Beena (2016) conducted a study on early Intervention in Children with
Developmental Disabilities reported that Developmental disabilities consist of conditions that
delay or impair the physical, cognitive, and/or psychological development of children. If not
intervened at the earliest, these disabilities will cause significant negative impact on multiple
domains of functioning such as learning, language, self-care and capacity for independent
living.
Landesman Ramey and Ramey (1999) studied the effects of early
experience and early intervention and stated that for 4 decades, vigorous efforts have been
based on the premise that early intervention for children of poverty and, more recently, for
children with developmental disabilities can yield significant improvements in cognitive,
academic, and social outcomes. The study briefly summarized the history of those efforts and
presented a conceptual framework to understand the design, research, and policy relevance of
these early interventions. This framework, biosocial developmental contextualism, derives
from social ecology, developmental systems theory, developmental epidemiology, and
developmental neurobiology. Those integrative perspective predicts that fragmented, weak
efforts in early intervention are not likely to succeed, whereas intensive, high-quality,
ecologically pervasive interventions can and do. Relevant evidence was also summarized in 6
principles about efficacy of early intervention. The public policy challenge in early
intervention is to contain costs by more precisely targeting early interventions to those who
most need and benefit from these interventions. The empirical evidence on biobehavioral
effects of early experience and early intervention has direct relevance to federal and state
policy development and resource allocation.
Beena (2016) conducted a study on early Intervention in Children with
Developmental Disabilities reported that Developmental disabilities consist of conditions that
delay or impair the physical, cognitive, and/or psychological development of children. If not
intervened at the earliest, these disabilities will cause significant negative impact on multiple
domains of functioning such as learning, language, self-care and capacity for independent
living.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
17
Infancy and early childhood are important times in any child’s life. For
children with disabilities, the early years are critical for a number of reasons. First, the earlier
a child is identified as having a developmental delay or disability, the greater the likelihood
the child will benefit from intervention strategies designed to compensate for the child’s
needs (Guralnick, 2005). Second, families benefit from the support given to them through the
intervention process (Dunst, 2007). Third, schools and communities benefit from a decrease
in costs because more children arrive at school ready to learn (Carta & Kong, 2007).
Early intervention services are multidisciplinary services provided to
children with developmental disabilities, delays, or risks during the first few years of life. The
goal of these programs is to promote the health and optimal development of the children as
well as to support adaptive parenting and positive functioning of their families (Meisels &
Shonkoff, 2000).
Positive early experiences are essential prerequisites for later success in
school, the workplace, and the community. Services to young children who have or are at risk
for developmental delays have been shown to positively impact outcomes across
developmental domains, including health, language and communication, cognitive
development and social/emotional development. Families benefit from early intervention by
being able to better meet their children’s special needs from an early age and throughout their
lives. Benefits to society include reducing economic burden through a decreased need for
special education. (Meisels & Shonkoff, 2000)
Infancy and early childhood are important times in any child’s life. For
children with disabilities, the early years are critical for a number of reasons. First, the earlier
a child is identified as having a developmental delay or disability, the greater the likelihood
the child will benefit from intervention strategies designed to compensate for the child’s
needs (Guralnick, 2005). Second, families benefit from the support given to them through the
intervention process (Dunst, 2007). Third, schools and communities benefit from a decrease
in costs because more children arrive at school ready to learn (Carta & Kong, 2007).
Early intervention services are multidisciplinary services provided to
children with developmental disabilities, delays, or risks during the first few years of life. The
goal of these programs is to promote the health and optimal development of the children as
well as to support adaptive parenting and positive functioning of their families (Meisels &
Shonkoff, 2000).
Positive early experiences are essential prerequisites for later success in
school, the workplace, and the community. Services to young children who have or are at risk
for developmental delays have been shown to positively impact outcomes across
developmental domains, including health, language and communication, cognitive
development and social/emotional development. Families benefit from early intervention by
being able to better meet their children’s special needs from an early age and throughout their
lives. Benefits to society include reducing economic burden through a decreased need for
special education. (Meisels & Shonkoff, 2000)
18
Jain et al., (2013) aimed to identify the age at first concern and age at
referral for rehabilitation services in children with developmental disabilities in India. Two
hundred fifty-nine children were included and data were collected from the parents. In
children with developmental disabilities (excluding autism spectrum disorders), median age
at initial concern was 7 months and age at referral for rehabilitation services was 13 months.
In children with autism spectrum disorders, median age at initial concern was 24 months and
age at referral was 42 months. Physician’s recognition of the condition, single child,
institutional delivery and neonatal admission ≥4 days were associated with early referral. The
common reasons cited by the parents for delay in services were reassurance by physicians or
family members and non-referral by the physicians. The study concluded that, routine
screening for developmental problems (including autism) and improving the awareness of
these conditions among physicians and society would lead to early referral.
Wolery and Bredekamp’s work (as cited in Chippett Darryl, 1999)
offers seven outcomes as defensible goals for programs supporting developmentally delayed
children and their families. They suggest that programs should seek:
1. To support families in achieving their own goals,
2. To promote children's engagement, independence, and mastery,
3. To promote children's development in key domains,
4. To build and support children's social competence,
5. To promote children's generalized use of skills,
Jain et al., (2013) aimed to identify the age at first concern and age at
referral for rehabilitation services in children with developmental disabilities in India. Two
hundred fifty-nine children were included and data were collected from the parents. In
children with developmental disabilities (excluding autism spectrum disorders), median age
at initial concern was 7 months and age at referral for rehabilitation services was 13 months.
In children with autism spectrum disorders, median age at initial concern was 24 months and
age at referral was 42 months. Physician’s recognition of the condition, single child,
institutional delivery and neonatal admission ≥4 days were associated with early referral. The
common reasons cited by the parents for delay in services were reassurance by physicians or
family members and non-referral by the physicians. The study concluded that, routine
screening for developmental problems (including autism) and improving the awareness of
these conditions among physicians and society would lead to early referral.
Wolery and Bredekamp’s work (as cited in Chippett Darryl, 1999)
offers seven outcomes as defensible goals for programs supporting developmentally delayed
children and their families. They suggest that programs should seek:
1. To support families in achieving their own goals,
2. To promote children's engagement, independence, and mastery,
3. To promote children's development in key domains,
4. To build and support children's social competence,
5. To promote children's generalized use of skills,

19
6. To provide and prepare children for normalized Life experiences, and
7. To prevent the emergence of future problems or disabilities.
Brusnahan and Klingenberg (2010) conducted study on evidence-based
practice for young children with Autism Spectrum Disorders, on the basis of the
recommendation of National Resource Council and National Professional Development
Center ASD and suggested guidance to professionals in setting educational programmes that
use effective, research-based interventions for young children with autism spectrum disorders
in early childhood special education.
The following are the specific priority areas of need for autism
spectrum disorder programming.
1. Functional spontaneous communication: Functional spontaneous communication should be
the primary focus of early education. For very young children, programming should be based
on the assumption that most children can learn to speak. Effective teaching techniques for
both verbal language and alternative modes of functional communication, drawn from the
empirical and theoretical literature, should be vigorously applied across settings.
2. Social instruction: Social instruction should be delivered throughout the day in various
settings, using specific activities and interventions planned to meet age-appropriate,
individualized social goals (e.g., with very young children, response to maternal imitation;
with preschool children, cooperative activities with peers).
6. To provide and prepare children for normalized Life experiences, and
7. To prevent the emergence of future problems or disabilities.
Brusnahan and Klingenberg (2010) conducted study on evidence-based
practice for young children with Autism Spectrum Disorders, on the basis of the
recommendation of National Resource Council and National Professional Development
Center ASD and suggested guidance to professionals in setting educational programmes that
use effective, research-based interventions for young children with autism spectrum disorders
in early childhood special education.
The following are the specific priority areas of need for autism
spectrum disorder programming.
1. Functional spontaneous communication: Functional spontaneous communication should be
the primary focus of early education. For very young children, programming should be based
on the assumption that most children can learn to speak. Effective teaching techniques for
both verbal language and alternative modes of functional communication, drawn from the
empirical and theoretical literature, should be vigorously applied across settings.
2. Social instruction: Social instruction should be delivered throughout the day in various
settings, using specific activities and interventions planned to meet age-appropriate,
individualized social goals (e.g., with very young children, response to maternal imitation;
with preschool children, cooperative activities with peers).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
20
3. Play skills: The teaching of play skills should focus on play with peers, with additional
instruction in appropriate use of toys and other materials.
4. Cognitive development: Other instruction aimed at goals for cognitive development should
also be carried out in the context in which the skills are expected to be used with
generalization and maintenance in natural contexts as important as the acquisition of new
skills. Because new skills have to be learned before they can be generalized, the
documentation of rates of acquisition is an important first step. Methods of introduction of
new skills may differ from teaching strategies to support generalization and maintenance.
5. Proactive approaches to behavior problems: Intervention strategies that address problem
behaviors should incorporate information about the contexts in which the behaviors occur;
positive, proactive approaches; and the range of techniques that have empirical support (e.g.,
functional assessment, functional communication training, reinforcement of alternative
behaviors).
6. Functional academic skills: Functional academic skills should be taught when appropriate
to the skills and needs of a child.
In addition to goals and priority areas, the recommendations for educational programming
are:
1. Intervention should begin as soon as a child is suspected of having autism spectrum
disorder.
3. Play skills: The teaching of play skills should focus on play with peers, with additional
instruction in appropriate use of toys and other materials.
4. Cognitive development: Other instruction aimed at goals for cognitive development should
also be carried out in the context in which the skills are expected to be used with
generalization and maintenance in natural contexts as important as the acquisition of new
skills. Because new skills have to be learned before they can be generalized, the
documentation of rates of acquisition is an important first step. Methods of introduction of
new skills may differ from teaching strategies to support generalization and maintenance.
5. Proactive approaches to behavior problems: Intervention strategies that address problem
behaviors should incorporate information about the contexts in which the behaviors occur;
positive, proactive approaches; and the range of techniques that have empirical support (e.g.,
functional assessment, functional communication training, reinforcement of alternative
behaviors).
6. Functional academic skills: Functional academic skills should be taught when appropriate
to the skills and needs of a child.
In addition to goals and priority areas, the recommendations for educational programming
are:
1. Intervention should begin as soon as a child is suspected of having autism spectrum
disorder.
21
2. Intervention should include a child’s active engagement in systematically planned,
age and developmentally appropriate activity toward identified objectives. It is
recommended that intervention occur a minimum of a full school day, at least 5 days a
week (25 hours) with year round programming.
3. Intervention should include teaching that is planned and organized around repeated
short intervals. These intervals should be individualized daily and include one to-one
as well as very small group instructions. All intervention should focus on meeting
individualized goals.
4. Intervention should include the inclusion of a family component, including parent
training.
5. Intervention should include mechanisms for ongoing evaluation of program and
child’s progress, with adjustments made accordingly.
6. Intervention should include inclusive opportunities. For example, to the extent that it
leads to the acquisition of a child’s educational goals, specialized instruction should
occur in a setting in which ongoing interactions occur with typically developing
children.
Meisels and Shonkof’s study (as cited in Chippett. Darryl, 1999) found
that, it is especially critical to intervene early in the life of children who are developmentally
delayed if they are to be provided with the tools necessary to develop to their Full potential.
Helping children develop to their fullest potential before entering kindergarten enables them
to meet with greater success in school. The more skills a child has developed before entering
kindergarten, the fewer the demands placed on the system for individual and remedial
supports. While providing educational resources to developmentally delayed preschoolers
2. Intervention should include a child’s active engagement in systematically planned,
age and developmentally appropriate activity toward identified objectives. It is
recommended that intervention occur a minimum of a full school day, at least 5 days a
week (25 hours) with year round programming.
3. Intervention should include teaching that is planned and organized around repeated
short intervals. These intervals should be individualized daily and include one to-one
as well as very small group instructions. All intervention should focus on meeting
individualized goals.
4. Intervention should include the inclusion of a family component, including parent
training.
5. Intervention should include mechanisms for ongoing evaluation of program and
child’s progress, with adjustments made accordingly.
6. Intervention should include inclusive opportunities. For example, to the extent that it
leads to the acquisition of a child’s educational goals, specialized instruction should
occur in a setting in which ongoing interactions occur with typically developing
children.
Meisels and Shonkof’s study (as cited in Chippett. Darryl, 1999) found
that, it is especially critical to intervene early in the life of children who are developmentally
delayed if they are to be provided with the tools necessary to develop to their Full potential.
Helping children develop to their fullest potential before entering kindergarten enables them
to meet with greater success in school. The more skills a child has developed before entering
kindergarten, the fewer the demands placed on the system for individual and remedial
supports. While providing educational resources to developmentally delayed preschoolers
22
and their families can, in the long term, decrease the costs of education such children, it is the
individual benefits to children that must guide the development and implementation of early
childhood education and intervention programs.
2.2.2 RELATED LITERATURE ON IMPORTANCE OF PARENTAL
INVOLVEMENT IN EARLY INTERVENTION
One of the most frequent assertions coming from reviews of early
intervention program effectiveness is that parental involvement contributes directly to
intervention success (Bronfenbrenner, 1974)
Turnbull’s study (as cited in Sukumaran, 2000) points to the need for
parental involvement. It points to the need for providing parents with some understanding of
the nature of their children’s problems and indicates the importance of sharing educational
and treatment methods and goals.
With regard to early intervention programs for children who are
handicapped, disadvantaged, or at risk, most people would agree with McConachie (1986)
that the general parameters of parent involvement include one or more of the following
components: • Teaching parents specific intervention skills to assist them in becoming more
effective change agents with their child. • Providing social and emotional support to family
members. • Exchange of information between parents and professionals. • Participation of
parents as team members in assessment or program planning • Development of appropriate
parent-child relationships. • Assisting parents in accessing community resources.
and their families can, in the long term, decrease the costs of education such children, it is the
individual benefits to children that must guide the development and implementation of early
childhood education and intervention programs.
2.2.2 RELATED LITERATURE ON IMPORTANCE OF PARENTAL
INVOLVEMENT IN EARLY INTERVENTION
One of the most frequent assertions coming from reviews of early
intervention program effectiveness is that parental involvement contributes directly to
intervention success (Bronfenbrenner, 1974)
Turnbull’s study (as cited in Sukumaran, 2000) points to the need for
parental involvement. It points to the need for providing parents with some understanding of
the nature of their children’s problems and indicates the importance of sharing educational
and treatment methods and goals.
With regard to early intervention programs for children who are
handicapped, disadvantaged, or at risk, most people would agree with McConachie (1986)
that the general parameters of parent involvement include one or more of the following
components: • Teaching parents specific intervention skills to assist them in becoming more
effective change agents with their child. • Providing social and emotional support to family
members. • Exchange of information between parents and professionals. • Participation of
parents as team members in assessment or program planning • Development of appropriate
parent-child relationships. • Assisting parents in accessing community resources.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
23
Parent involvement is essential for successful early intervention
programs are found in the 1986 Amendments to the Education of the Handicapped Act
(Public Law 99-457), which established what amounts to mandated early intervention
programs for all children with handicaps. The committee report, which describes Congress'
rationale behind the legislation, stated, The committee received overwhelming testimony
affirming the family as the primary learning environment for children under six years of age
and pointing out the critical need for parents and professionals to function in a collaborative
manner. (Gilkerson et. al., 1987).
White and Moss (1992) analyzed the evidence from previous research
regarding the benefits associated with the involvement of parents in early intervention
programs and concluded the rationale for involving parents in early intervention programs.
Parents have an obligation to be involved because they are ultimately responsible for their
child's welfare. Involved parents provide better political support and advocacy. Early
intervention programs which involve parents result in greater benefits for children. Parent
involvement results in benefits for the parents and family members. By involving parents, the
same outcomes can be achieved at less cost. The benefits of early intervention are maintained
better.
Many reasons have been offered for why parents should be involved in
early intervention programs (Bristol & Gallagher, 1982; Peterson, 1987; Turnbull &
Turnbull, 1986)
Parent involvement is essential for successful early intervention
programs are found in the 1986 Amendments to the Education of the Handicapped Act
(Public Law 99-457), which established what amounts to mandated early intervention
programs for all children with handicaps. The committee report, which describes Congress'
rationale behind the legislation, stated, The committee received overwhelming testimony
affirming the family as the primary learning environment for children under six years of age
and pointing out the critical need for parents and professionals to function in a collaborative
manner. (Gilkerson et. al., 1987).
White and Moss (1992) analyzed the evidence from previous research
regarding the benefits associated with the involvement of parents in early intervention
programs and concluded the rationale for involving parents in early intervention programs.
Parents have an obligation to be involved because they are ultimately responsible for their
child's welfare. Involved parents provide better political support and advocacy. Early
intervention programs which involve parents result in greater benefits for children. Parent
involvement results in benefits for the parents and family members. By involving parents, the
same outcomes can be achieved at less cost. The benefits of early intervention are maintained
better.
Many reasons have been offered for why parents should be involved in
early intervention programs (Bristol & Gallagher, 1982; Peterson, 1987; Turnbull &
Turnbull, 1986)

24
The following six rationales have been identified that which are
frequently offered as to why it is important to involve parents: • Parents are responsible for
the welfare of their children. Most parents want a voice in how their child is educated
because they are ultimately responsible for the child's well-being and welfare. Some argue
that, even if parents wanted to relinquish that responsibility to schools or government
agencies, they should not be allowed to do so.
• Involved parents provide better political support and advocacy. Some claim that, if parents
have first-hand information about their child's early intervention program, they will be in a
better position to advocate the further growth and support of those programs. This argument
suggests that, even if programs have very good evidence that there are substantial benefits
resulting from participation, it is absolutely essential in times of fiscal restraint to make sure
that a broad constituency understands and supports their continued growth and funding.
• Early intervention programs which involve parents result in greater benefits for children. It
is often alleged that, by involving the family (i.e., the people with whom the child spends the
majority of his or her time), the benefits of early intervention programs will be strengthened.
Parent involvement activities benefit parents and family members. By helping parents
understand their child's current situation and potential and how to manage their child's
needs and demands, it is often claimed that parents will have reduced levels of stress,
more satisfaction, and a more realistic perception of what is possible and desirable.
Participation in early intervention programs also exposes parents to other agencies and
services which may be useful to them in other aspects of their life.
The following six rationales have been identified that which are
frequently offered as to why it is important to involve parents: • Parents are responsible for
the welfare of their children. Most parents want a voice in how their child is educated
because they are ultimately responsible for the child's well-being and welfare. Some argue
that, even if parents wanted to relinquish that responsibility to schools or government
agencies, they should not be allowed to do so.
• Involved parents provide better political support and advocacy. Some claim that, if parents
have first-hand information about their child's early intervention program, they will be in a
better position to advocate the further growth and support of those programs. This argument
suggests that, even if programs have very good evidence that there are substantial benefits
resulting from participation, it is absolutely essential in times of fiscal restraint to make sure
that a broad constituency understands and supports their continued growth and funding.
• Early intervention programs which involve parents result in greater benefits for children. It
is often alleged that, by involving the family (i.e., the people with whom the child spends the
majority of his or her time), the benefits of early intervention programs will be strengthened.
Parent involvement activities benefit parents and family members. By helping parents
understand their child's current situation and potential and how to manage their child's
needs and demands, it is often claimed that parents will have reduced levels of stress,
more satisfaction, and a more realistic perception of what is possible and desirable.
Participation in early intervention programs also exposes parents to other agencies and
services which may be useful to them in other aspects of their life.
25
By involving parents, the same outcomes can be achieved at less cost. Early intervention
services can be very expensive. If parents can be used to deliver a portion of the services,
it is often suggested that the costs of early intervention can be dramatically reduced.
The benefits of early intervention are maintained better if parents are involved. It is often
argued that the involvement of parents will reinforce and maintain the benefits of early
intervention because they are the only ones who will be consistently involved with the
child. Responsibilities of agencies may change, the family may move, funding may be
cut, but the child will always be a member of his/her family.
The division of early childhood recommended practices (as cited in
Chippett Darryl, 1999) are intended to promote family participation as paramount, both in
terms of decision making for their own children and policy making in general. The parental
role is one of full partnership with professionals in all aspects of early intervention. Parents
are deemed to have an equal role in all aspects of the program from policy making to
program evaluation. Collaboration and the building of positive relationships between parents
and professionals that are based on a mutual respect are stated as being a necessary solid
foundation on which to build a successful early intervention program.
By involving parents, the same outcomes can be achieved at less cost. Early intervention
services can be very expensive. If parents can be used to deliver a portion of the services,
it is often suggested that the costs of early intervention can be dramatically reduced.
The benefits of early intervention are maintained better if parents are involved. It is often
argued that the involvement of parents will reinforce and maintain the benefits of early
intervention because they are the only ones who will be consistently involved with the
child. Responsibilities of agencies may change, the family may move, funding may be
cut, but the child will always be a member of his/her family.
The division of early childhood recommended practices (as cited in
Chippett Darryl, 1999) are intended to promote family participation as paramount, both in
terms of decision making for their own children and policy making in general. The parental
role is one of full partnership with professionals in all aspects of early intervention. Parents
are deemed to have an equal role in all aspects of the program from policy making to
program evaluation. Collaboration and the building of positive relationships between parents
and professionals that are based on a mutual respect are stated as being a necessary solid
foundation on which to build a successful early intervention program.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
26
2.2.3 RELATED LITERATURE ON DEVELOPMENTAL DISABILITIES
Developmental disability is a permanent cognitive and/or physical
impairment that usually occurs in the early years of life but can occur any time before the age
of 18 years.
The royal Australasian college of physicians (2013), in their statement
on early intervention for children with developmental disabilities stated Developmental
disability as a permanent cognitive and/or physical impairment that usually occurs in the
early years of life but can occur anytime before the age of 18 years thus time being the crucial
component. However, its usage in the early years of life may be limited as it may be difficult
to predict the longer term developmental trajectory.
Beena (2016) conducted a study on early Intervention in Children with
Developmental Disabilities reported that Developmental disabilities consist of conditions that
delay or impair the physical, cognitive, and/or psychological development of children. If not
intervened at the earliest, these disabilities will cause significant negative impact on multiple
domains of functioning such as learning, language, self-care and capacity for independent
living. Common developmental disabilities include autism spectrum disorders, intellectual
disabilities, developmental delay and cerebral palsy. About one fourth of young children in
developing countries is at risk for or has developmental delay or disabilities. Inadequate
stimulation has significant negative impact on physical, socio emotional and cognitive
development of children. Hence early scientific intervention programs are necessary in the
management of children at risk for developmental delay.
2.2.3 RELATED LITERATURE ON DEVELOPMENTAL DISABILITIES
Developmental disability is a permanent cognitive and/or physical
impairment that usually occurs in the early years of life but can occur any time before the age
of 18 years.
The royal Australasian college of physicians (2013), in their statement
on early intervention for children with developmental disabilities stated Developmental
disability as a permanent cognitive and/or physical impairment that usually occurs in the
early years of life but can occur anytime before the age of 18 years thus time being the crucial
component. However, its usage in the early years of life may be limited as it may be difficult
to predict the longer term developmental trajectory.
Beena (2016) conducted a study on early Intervention in Children with
Developmental Disabilities reported that Developmental disabilities consist of conditions that
delay or impair the physical, cognitive, and/or psychological development of children. If not
intervened at the earliest, these disabilities will cause significant negative impact on multiple
domains of functioning such as learning, language, self-care and capacity for independent
living. Common developmental disabilities include autism spectrum disorders, intellectual
disabilities, developmental delay and cerebral palsy. About one fourth of young children in
developing countries is at risk for or has developmental delay or disabilities. Inadequate
stimulation has significant negative impact on physical, socio emotional and cognitive
development of children. Hence early scientific intervention programs are necessary in the
management of children at risk for developmental delay.
27
Bernheimer and Keogh’s study (as cited in Chippett Darryl, 1999)
defines developmental disabilities as "...chronic disabilities which result from mental and/or
physical impairment and manifest themselves in substantial functional limitations in such
areas as academic skills, communication, social skills, mobility, self-care, and capacity for
independent living". Children in this category include those with Down's syndrome, autism,
spina bifida, and cerebral palsy. Developmental delay exists in children when they “...
manifest signs of slow development and language and communication problems, but ...
exhibit no clear signs of associated physical or biological impairments"
Panteliadis et al., (2015) describes cerebral palsy (CP) as one of the
most common congenital or acquired neurological impairments in paediatric patients, and
refers to a group of children with motor disability and related functional defects. The visible
core of CP is characterized by abnormal coordination of movements and/or muscle tone
which manifest very early in the development. Resulting from pre- or perinatal brain damage
CP is not a progressive condition.
Cerebral Palsy describes a group of permanent disorders of the
development and posture, causing activity limitation that are attributed to non-progressive
disturbances that occurred in the developing fetal or infant brain. The motor disorders of
cerebral palsy are often accompanied by disturbances of sensation, perception, cognition,
communication, and behaviour, by epilepsy, and by secondary musculoskeletal problems.
(Bax, et al., 2005)
Bernheimer and Keogh’s study (as cited in Chippett Darryl, 1999)
defines developmental disabilities as "...chronic disabilities which result from mental and/or
physical impairment and manifest themselves in substantial functional limitations in such
areas as academic skills, communication, social skills, mobility, self-care, and capacity for
independent living". Children in this category include those with Down's syndrome, autism,
spina bifida, and cerebral palsy. Developmental delay exists in children when they “...
manifest signs of slow development and language and communication problems, but ...
exhibit no clear signs of associated physical or biological impairments"
Panteliadis et al., (2015) describes cerebral palsy (CP) as one of the
most common congenital or acquired neurological impairments in paediatric patients, and
refers to a group of children with motor disability and related functional defects. The visible
core of CP is characterized by abnormal coordination of movements and/or muscle tone
which manifest very early in the development. Resulting from pre- or perinatal brain damage
CP is not a progressive condition.
Cerebral Palsy describes a group of permanent disorders of the
development and posture, causing activity limitation that are attributed to non-progressive
disturbances that occurred in the developing fetal or infant brain. The motor disorders of
cerebral palsy are often accompanied by disturbances of sensation, perception, cognition,
communication, and behaviour, by epilepsy, and by secondary musculoskeletal problems.
(Bax, et al., 2005)
28
Naletilić et.al (2009) conducted a study on early diagnosis, intervention
and risk factors of cerebral palsy and suggested them to be crucial a factor in cerebral palsy
(CP) treatment. They observed 347 children diagnosed for CP in Clinical Hospital Mostar,
Bosnia and Herzegovina, and studied the relationship between (a) intervention start point and
the final motor outcome, (b) intensity of treatment and final outcome, and (c) relationship
between documented risk factors and early diagnosis of the CP. Their study suggested that it
is possible to relatively accurately diagnose the CP in the first trimester. Previous
miscarriages, sepsis and intracerebral haemorrhage were significantly related to early
diagnosis, while delivery outcome, respiratory distress syndrome, premature birth,
intracerebral haemorrhage, sepsis, meningitis, hydrocephalus and convulsions were found as
significantly related to final motor CP outcome. They found no significant influence of the
intervention intensity and final diagnosis. Their results support the idea that the intervention
start point has to be considered as one of the most important factors for the effective
intervention program.
Karande and Kulkarni (2008) stated that Cerebral palsy is a term used
to describe a group of non progressive disorders that manifest as abnormalities of motion and
posture. These disorders result from a central nervous system (CNS) injury sustained in the
early period of brain development, usually defined as the first three to five years of life.
Cerebral palsy is a clinical diagnosis made by an awareness of risk factors, regular
developmental screening of all high risk babies and neurological examination. Abnormal
motor control and tone in the absence of an underlying progressive disease is the clinical
hallmark of this condition. The evaluation of a child with cerebral palsy is an ongoing process
Naletilić et.al (2009) conducted a study on early diagnosis, intervention
and risk factors of cerebral palsy and suggested them to be crucial a factor in cerebral palsy
(CP) treatment. They observed 347 children diagnosed for CP in Clinical Hospital Mostar,
Bosnia and Herzegovina, and studied the relationship between (a) intervention start point and
the final motor outcome, (b) intensity of treatment and final outcome, and (c) relationship
between documented risk factors and early diagnosis of the CP. Their study suggested that it
is possible to relatively accurately diagnose the CP in the first trimester. Previous
miscarriages, sepsis and intracerebral haemorrhage were significantly related to early
diagnosis, while delivery outcome, respiratory distress syndrome, premature birth,
intracerebral haemorrhage, sepsis, meningitis, hydrocephalus and convulsions were found as
significantly related to final motor CP outcome. They found no significant influence of the
intervention intensity and final diagnosis. Their results support the idea that the intervention
start point has to be considered as one of the most important factors for the effective
intervention program.
Karande and Kulkarni (2008) stated that Cerebral palsy is a term used
to describe a group of non progressive disorders that manifest as abnormalities of motion and
posture. These disorders result from a central nervous system (CNS) injury sustained in the
early period of brain development, usually defined as the first three to five years of life.
Cerebral palsy is a clinical diagnosis made by an awareness of risk factors, regular
developmental screening of all high risk babies and neurological examination. Abnormal
motor control and tone in the absence of an underlying progressive disease is the clinical
hallmark of this condition. The evaluation of a child with cerebral palsy is an ongoing process
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
29
as its clinical manifestations may change with time due to growth and developmental
plasticity and maturation of the CNS. Because the injury is central in origin, majority of
children are likely to have associated CNS impairments such as mental retardation, epilepsy,
ophthalmologic defects, hearing impairment and speech disorders. It is important to
remember that these comorbidities may not be apparent at the time of diagnosis. Recognizing
and managing its comorbidities is as important as treating the motor- disabilities.
Karande and Kulkarni (2008) concluded that Parental knowledge of
cerebral palsy was inadequate. A single-session educational program could significantly
improve parental knowledge about many core basic issues regarding cerebral palsy.
Herskind et. al (2014) argue that infants with possible cerebral palsy
(CP) are commonly assumed to benefit from early diagnosis and early intervention, but
substantial evidence for that is lacking. They argue that there is no consensus in the literature
on a definition of ‘early’, but focuses on interventions initiated within the first 6 months after
term age. They cover basic neuroscience, arguing for a beneficial effect of early intervention,
and discusses why clinical research to support that convincingly was lacking. They argue that
infants offered early intervention in future clinical studies must be identified carefully, and
that the intervention should be focused on infants showing early signs of CP to determine an
effect of treatment. Such signs may be efficiently detected by a combination of neuroimaging
and the General Movements Assessment.
Individuals with Disabilities Education Improvement Act (IDEIA)(
2004) stipulates that autism is characterized by the following: Autism means a
as its clinical manifestations may change with time due to growth and developmental
plasticity and maturation of the CNS. Because the injury is central in origin, majority of
children are likely to have associated CNS impairments such as mental retardation, epilepsy,
ophthalmologic defects, hearing impairment and speech disorders. It is important to
remember that these comorbidities may not be apparent at the time of diagnosis. Recognizing
and managing its comorbidities is as important as treating the motor- disabilities.
Karande and Kulkarni (2008) concluded that Parental knowledge of
cerebral palsy was inadequate. A single-session educational program could significantly
improve parental knowledge about many core basic issues regarding cerebral palsy.
Herskind et. al (2014) argue that infants with possible cerebral palsy
(CP) are commonly assumed to benefit from early diagnosis and early intervention, but
substantial evidence for that is lacking. They argue that there is no consensus in the literature
on a definition of ‘early’, but focuses on interventions initiated within the first 6 months after
term age. They cover basic neuroscience, arguing for a beneficial effect of early intervention,
and discusses why clinical research to support that convincingly was lacking. They argue that
infants offered early intervention in future clinical studies must be identified carefully, and
that the intervention should be focused on infants showing early signs of CP to determine an
effect of treatment. Such signs may be efficiently detected by a combination of neuroimaging
and the General Movements Assessment.
Individuals with Disabilities Education Improvement Act (IDEIA)(
2004) stipulates that autism is characterized by the following: Autism means a
30
developmental disability significantly affecting verbal and nonverbal communication and
social interaction, generally evident before age three that adversely affects a child’s education
performance. Other characteristics often associated with autism are engagement in repetitive
activities and stereotyped movements, resistance to environmental change or change in daily
routines, and unusual responses to sensory experiences. Autism does not apply if a child’s
educational performance is adversely affected primarily because the child has an emotional
disturbance.
Scheuermann & Webber’s Work (as cited in Banda & Grimmett, 2008)
defines children with autism as often having difficulty with social interactions and
communication. In addition, these children may display deficits in life skills and/or exhibit
problem behaviors including stereotypic behaviors, self-injurious behaviors, hyper- or
hyposensitivity to sound, taste, smell, etc. Because of this, children with autism often
develop dependence on adult caregivers to provide support to learn new skills, and to stay on-
task and on-schedule throughout the activities at school, home, and other community settings.
Thus, the challenge for parents and teachers is to decrease the dependence on adults and to
increase the childrens independence in daily living, communication, socialization skills.
Levy (2007) describes the essential features of autistic disorder as, the
presence of markedly abnormal or impaired development in social interaction and
communication, and a markedly restricted repertoire of activity and interests. The impairment
in social interaction is gross and sustained, and there may be marked impairment in the use of
multiple non-verbal behaviours (e.g. eye to-eye gaze, facial expression, body postures and
gestures). There may also be a lack of varied, spontaneous make-believe play or social
developmental disability significantly affecting verbal and nonverbal communication and
social interaction, generally evident before age three that adversely affects a child’s education
performance. Other characteristics often associated with autism are engagement in repetitive
activities and stereotyped movements, resistance to environmental change or change in daily
routines, and unusual responses to sensory experiences. Autism does not apply if a child’s
educational performance is adversely affected primarily because the child has an emotional
disturbance.
Scheuermann & Webber’s Work (as cited in Banda & Grimmett, 2008)
defines children with autism as often having difficulty with social interactions and
communication. In addition, these children may display deficits in life skills and/or exhibit
problem behaviors including stereotypic behaviors, self-injurious behaviors, hyper- or
hyposensitivity to sound, taste, smell, etc. Because of this, children with autism often
develop dependence on adult caregivers to provide support to learn new skills, and to stay on-
task and on-schedule throughout the activities at school, home, and other community settings.
Thus, the challenge for parents and teachers is to decrease the dependence on adults and to
increase the childrens independence in daily living, communication, socialization skills.
Levy (2007) describes the essential features of autistic disorder as, the
presence of markedly abnormal or impaired development in social interaction and
communication, and a markedly restricted repertoire of activity and interests. The impairment
in social interaction is gross and sustained, and there may be marked impairment in the use of
multiple non-verbal behaviours (e.g. eye to-eye gaze, facial expression, body postures and
gestures). There may also be a lack of varied, spontaneous make-believe play or social
31
imitative play appropriate to developmental level. Speech development is delayed and the
pitch, intonation, rate, rhythm or stress may be abnormal, with abnormal grammar and
repetitive use of language or idiosyncratic language. Behavioural symptoms include odd
responses to sensory stimuli (e.g. oversensitivity to sounds or being touched, and fascination
to certain repetitive stimuli and a lack of fear in response to real danger), as well as over-
activity, short attention span, impulsivity, aggression, and self-injurious behaviour.
Autism is a childhood developmental disorder that appears in the first
three years of life. There are many possible symptoms individuals with autism experience.
One human autistic behavior in children ages one to four is the lack of play development and
social skills. Children with autism oftentimes engage in nonsocial activities while choosing to
play with a restricted selection of objects for long periods of time. They tend to spend
considerably less time playing functionally than children without autism (Fabienneet al.,
2008).
Menon, ( 2012) stated, Autism is the most common condition in a
group of developmental disorders knows as the Autism Spectrum Disorders. Autism is
characterized by impaired social interaction, problems with verbal and non verbal
communication, and unusual repetitive, or severely limited activities and interests. The
hallmark feature of autism is impaired social interaction.
Webster et al., (2004) studied the parental perspectives on early
intensive intervention for children diagnosed with autistic spectrum disorder and focused in
imitative play appropriate to developmental level. Speech development is delayed and the
pitch, intonation, rate, rhythm or stress may be abnormal, with abnormal grammar and
repetitive use of language or idiosyncratic language. Behavioural symptoms include odd
responses to sensory stimuli (e.g. oversensitivity to sounds or being touched, and fascination
to certain repetitive stimuli and a lack of fear in response to real danger), as well as over-
activity, short attention span, impulsivity, aggression, and self-injurious behaviour.
Autism is a childhood developmental disorder that appears in the first
three years of life. There are many possible symptoms individuals with autism experience.
One human autistic behavior in children ages one to four is the lack of play development and
social skills. Children with autism oftentimes engage in nonsocial activities while choosing to
play with a restricted selection of objects for long periods of time. They tend to spend
considerably less time playing functionally than children without autism (Fabienneet al.,
2008).
Menon, ( 2012) stated, Autism is the most common condition in a
group of developmental disorders knows as the Autism Spectrum Disorders. Autism is
characterized by impaired social interaction, problems with verbal and non verbal
communication, and unusual repetitive, or severely limited activities and interests. The
hallmark feature of autism is impaired social interaction.
Webster et al., (2004) studied the parental perspectives on early
intensive intervention for children diagnosed with autistic spectrum disorder and focused in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
32
detail on the experiences and perceptions of parents of children with ASD receiving early
intensive support.
Autistic spectrum disorder (ASD) can affect family life severely,
causing high levels of anxiety, stress, isolation and uncertainty for parents and siblings.
Children with ASD typically show delayed or abnormal development from infancy onwards,
particularly in social interaction, communication and cognition, and may never mature to
independence in adult life. More extreme features can include ritualistic behaviour,
exaggerated emotional reactions, aggression and self-injury. Although ASD is presumed to
have a neurological basis, we currently lack an unequivocal theory for ASD on which to
found intervention (Bishop, 1993; Medical Research Council, 2000; Rutter et al., 1994).
Koegel et al., (2013) studied the importance of early identification and
intervention for children with or at risk for autism spectrum disorders found that there has
been a dramatic rise in the number of children being diagnosed with autism spectrum
disorders (ASD), which has led to increased attention paid to assessment and intervention
issues. This manuscript agrees with Camarata (2014) that the evidence base for early
assessment and intervention should be expanded. Reliable diagnosis has been documented
during infancy and toddlerhood, and evidence suggests that the earlier the onset of
intervention, the greater likelihood of an improved developmental trajectory. It is argued that
early intervention is more cost and time efficient than a wait and see approach.
Sacrey et al., (2015) conducted a study with the objective to overview
recent findings on early detection/diagnosis of autism spectrum disorders, as well as clinical
detail on the experiences and perceptions of parents of children with ASD receiving early
intensive support.
Autistic spectrum disorder (ASD) can affect family life severely,
causing high levels of anxiety, stress, isolation and uncertainty for parents and siblings.
Children with ASD typically show delayed or abnormal development from infancy onwards,
particularly in social interaction, communication and cognition, and may never mature to
independence in adult life. More extreme features can include ritualistic behaviour,
exaggerated emotional reactions, aggression and self-injury. Although ASD is presumed to
have a neurological basis, we currently lack an unequivocal theory for ASD on which to
found intervention (Bishop, 1993; Medical Research Council, 2000; Rutter et al., 1994).
Koegel et al., (2013) studied the importance of early identification and
intervention for children with or at risk for autism spectrum disorders found that there has
been a dramatic rise in the number of children being diagnosed with autism spectrum
disorders (ASD), which has led to increased attention paid to assessment and intervention
issues. This manuscript agrees with Camarata (2014) that the evidence base for early
assessment and intervention should be expanded. Reliable diagnosis has been documented
during infancy and toddlerhood, and evidence suggests that the earlier the onset of
intervention, the greater likelihood of an improved developmental trajectory. It is argued that
early intervention is more cost and time efficient than a wait and see approach.
Sacrey et al., (2015) conducted a study with the objective to overview
recent findings on early detection/diagnosis of autism spectrum disorders, as well as clinical
33
trials of early interventions for toddlers at risk for/diagnosed with autism spectrum disorder.
Their findings were: Prospective studies of infants at high risk of autism spectrum disorder
had yielded significant advances in understanding early development in autism spectrum
disorder. Findings from prospective studies indicate that abnormalities in social
communication and repetitive behaviours emerge during the second year, whereas additional
‘‘prodromal features’’ (motor and sensory abnormalities) emerge in the first year.
Subsequently, exciting progress has been made in establishing the efficacy of autism
spectrum disorder–specific interventions for toddlers as young as 15 months. Finally, efforts
occur to characterize autism spectrum disorder–specific characteristics in genetic syndromes
with concurrent autism spectrum disorder symptomatology. They concluded that substantial
progress in characterizing early developmental trajectories as well as the identification of
specific behavioral markers had aided early detection. Work still remains to ensure that
research findings are translated into clinical practice for uptake in the health care system.
According to American Association on Mental Retardation (1992),
Mental Retardation refers to substantial limitations in present functioning. It is characterized
by significantly sub-average intellectual functioning, existing concurrently with related
limitations in two or more of the following applicable adaptive skill areas: communication,
self-care, home living, social skills, community use, self direction, health and safety,
functional academics, leisure and work. Mental retardation manifests before age 18.
Lai et al., (2014) conducted a retrospective cohort study to understand
the predictors of effectiveness of early intervention on children with intellectual disability.
They recruited children who were treated for intellectual disability at a teaching hospital and
trials of early interventions for toddlers at risk for/diagnosed with autism spectrum disorder.
Their findings were: Prospective studies of infants at high risk of autism spectrum disorder
had yielded significant advances in understanding early development in autism spectrum
disorder. Findings from prospective studies indicate that abnormalities in social
communication and repetitive behaviours emerge during the second year, whereas additional
‘‘prodromal features’’ (motor and sensory abnormalities) emerge in the first year.
Subsequently, exciting progress has been made in establishing the efficacy of autism
spectrum disorder–specific interventions for toddlers as young as 15 months. Finally, efforts
occur to characterize autism spectrum disorder–specific characteristics in genetic syndromes
with concurrent autism spectrum disorder symptomatology. They concluded that substantial
progress in characterizing early developmental trajectories as well as the identification of
specific behavioral markers had aided early detection. Work still remains to ensure that
research findings are translated into clinical practice for uptake in the health care system.
According to American Association on Mental Retardation (1992),
Mental Retardation refers to substantial limitations in present functioning. It is characterized
by significantly sub-average intellectual functioning, existing concurrently with related
limitations in two or more of the following applicable adaptive skill areas: communication,
self-care, home living, social skills, community use, self direction, health and safety,
functional academics, leisure and work. Mental retardation manifests before age 18.
Lai et al., (2014) conducted a retrospective cohort study to understand
the predictors of effectiveness of early intervention on children with intellectual disability.
They recruited children who were treated for intellectual disability at a teaching hospital and
34
had two IQ tests from 2001 to 2005 and used the difference between the two tests as the
indicator of effectiveness. The participants included 23 boys and 13 girls 56.5 ± 5.9 months
of age at the first test and 73.4 ± 4.9 months at the second. The results showed that the IQ
increased from 57.0 ± 8.0 to 65.1 ± 12.3 (p < 0.001). This study showed that early
intervention can improve the IQ of children with ID, and the earlier the intervention the
better. In addition, the effectiveness is more prominent in boys and in children with a low
maternal educational level.
Guralnick (2005) reviewed the existing knowledge base in the field of
early intervention for children with intellectual disabilities and considered the prospects for
the future for improving early intervention outcomes in four areas such as the issues of
specificity, translational research, mental health and social competence, and systems
development at the community level.
Guralnick (2005) states that a number of young children likely to be
affected by intellectual disability worldwide is eclipsed only by the diversity and complexity
of the developmental patterns. The expectations are quite high that much can be
accomplished during the first 5 years of life through the thoughtful implementation of
systematic, comprehensive, experientially based early intervention programmes. More
specifically, it is anticipated that early intervention will enhance the development of young
children already exhibiting intellectual delays (of known or unknown etiology) both by
altering their developmental trajectories and by preventing secondary complications from
occurring. For children at risk of intellectual delays because of a variety of biological and/or
environmental conditions, it is expected that these delays can be prevented entirely or their
had two IQ tests from 2001 to 2005 and used the difference between the two tests as the
indicator of effectiveness. The participants included 23 boys and 13 girls 56.5 ± 5.9 months
of age at the first test and 73.4 ± 4.9 months at the second. The results showed that the IQ
increased from 57.0 ± 8.0 to 65.1 ± 12.3 (p < 0.001). This study showed that early
intervention can improve the IQ of children with ID, and the earlier the intervention the
better. In addition, the effectiveness is more prominent in boys and in children with a low
maternal educational level.
Guralnick (2005) reviewed the existing knowledge base in the field of
early intervention for children with intellectual disabilities and considered the prospects for
the future for improving early intervention outcomes in four areas such as the issues of
specificity, translational research, mental health and social competence, and systems
development at the community level.
Guralnick (2005) states that a number of young children likely to be
affected by intellectual disability worldwide is eclipsed only by the diversity and complexity
of the developmental patterns. The expectations are quite high that much can be
accomplished during the first 5 years of life through the thoughtful implementation of
systematic, comprehensive, experientially based early intervention programmes. More
specifically, it is anticipated that early intervention will enhance the development of young
children already exhibiting intellectual delays (of known or unknown etiology) both by
altering their developmental trajectories and by preventing secondary complications from
occurring. For children at risk of intellectual delays because of a variety of biological and/or
environmental conditions, it is expected that these delays can be prevented entirely or their
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
35
magnitude minimized. These admittedly high expectations on the benefits of early
intervention rest on a number of grounds. Certainly, compassionate and pragmatic rationales
can be invoked, especially given the central roles parents play in the development of their
young children. Clearly, it is essential to be able to address the needs of families during this
most stressful period and to focus on issues that support the adaptations that are and will be
necessary to strengthen those families and to maximize child development.
Landesman Ramey and Ramey (1999) states that early intervention is
deemed essential to prevent mental retardation and poor intellectual development in children
whose families do not provide adequate stimulation in the early years of life.
The mounting evidence about the significance of early experience in
brain development, recently summarized in Rethinking the Brain: New Insights into Early
Development (Shore, 1997), provides a stronger than ever impetus for systematic efforts to
enhance children's learning opportunities and development in the first three years of life.
Changes in very young children's cognitive, social, and emotional development are, of
course, interrelated and neurobiologically mediated. Important developmental
neurobiological mediators currently hypothesized to be implicated in early experience include
neurotransmitter changes (such as in the serotonin and dopamine levels and the endorphin
system), synaptic pruning as a function of experience (particularly use-dependent neural
network development), and gene activation associated with experience (Shore, 1997).
Approximately 60% of known genes are estimated to influence brain development, and their
expression often depends on specific environmental inputs. This complex cascade, although
only partially understood, has led developmental neuroscientists, developmental
magnitude minimized. These admittedly high expectations on the benefits of early
intervention rest on a number of grounds. Certainly, compassionate and pragmatic rationales
can be invoked, especially given the central roles parents play in the development of their
young children. Clearly, it is essential to be able to address the needs of families during this
most stressful period and to focus on issues that support the adaptations that are and will be
necessary to strengthen those families and to maximize child development.
Landesman Ramey and Ramey (1999) states that early intervention is
deemed essential to prevent mental retardation and poor intellectual development in children
whose families do not provide adequate stimulation in the early years of life.
The mounting evidence about the significance of early experience in
brain development, recently summarized in Rethinking the Brain: New Insights into Early
Development (Shore, 1997), provides a stronger than ever impetus for systematic efforts to
enhance children's learning opportunities and development in the first three years of life.
Changes in very young children's cognitive, social, and emotional development are, of
course, interrelated and neurobiologically mediated. Important developmental
neurobiological mediators currently hypothesized to be implicated in early experience include
neurotransmitter changes (such as in the serotonin and dopamine levels and the endorphin
system), synaptic pruning as a function of experience (particularly use-dependent neural
network development), and gene activation associated with experience (Shore, 1997).
Approximately 60% of known genes are estimated to influence brain development, and their
expression often depends on specific environmental inputs. This complex cascade, although
only partially understood, has led developmental neuroscientists, developmental
36
psychologists, and early interventionists to reframe the overly simplistic nature versus nurture
debate. In a consensus report integrating the latest neuroscience and early intervention
findings (Shore, 1997) powerful single conclusion emerged:
All of this evidence leads to a single conclusion: how humans develop
and learn depends critically and continually on the interplay between nature (an individual's
genetic endowment) and nurture (the nutrition, surroundings, care, stimulation, and teaching
that are provided or withheld). The roles of nature and nurture in determining intelligence and
emotional resilience should not be weighted quantitatively; genetic and environmental factors
have a more dynamic, qualitative interplay that cannot be reduced to a simple equation. Both
factors are crucial. New knowledge about brain function should end the "nature or nurture"
debate once and for all. (Shore, 1997)
2.2.4 RELATED LITERATURE ON EARLY INTERVENTION SERVICES
Panteliadis et al., (2015) reviewed the three general spastic
manifestations of CP hemiplegia, diplegia and tetraplegia and described the diagnostic
procedures and delineated a time schedule for an early intervention. Without systematic
medical and physiotherapeutic support the dystonia leads to muscle contractions and to
deterioration of the handicap.
Hadders-Algra’s study (as cited in Panteliadis et al.,2015) gives several
considerations on decisions regarding therapeutic interventions for Cerebral Palsy such as
neural plasticity and critical periods of development, extent of brain injury and signs
predicting prognosis, familial environment, and concepts and goals of intervention.
psychologists, and early interventionists to reframe the overly simplistic nature versus nurture
debate. In a consensus report integrating the latest neuroscience and early intervention
findings (Shore, 1997) powerful single conclusion emerged:
All of this evidence leads to a single conclusion: how humans develop
and learn depends critically and continually on the interplay between nature (an individual's
genetic endowment) and nurture (the nutrition, surroundings, care, stimulation, and teaching
that are provided or withheld). The roles of nature and nurture in determining intelligence and
emotional resilience should not be weighted quantitatively; genetic and environmental factors
have a more dynamic, qualitative interplay that cannot be reduced to a simple equation. Both
factors are crucial. New knowledge about brain function should end the "nature or nurture"
debate once and for all. (Shore, 1997)
2.2.4 RELATED LITERATURE ON EARLY INTERVENTION SERVICES
Panteliadis et al., (2015) reviewed the three general spastic
manifestations of CP hemiplegia, diplegia and tetraplegia and described the diagnostic
procedures and delineated a time schedule for an early intervention. Without systematic
medical and physiotherapeutic support the dystonia leads to muscle contractions and to
deterioration of the handicap.
Hadders-Algra’s study (as cited in Panteliadis et al.,2015) gives several
considerations on decisions regarding therapeutic interventions for Cerebral Palsy such as
neural plasticity and critical periods of development, extent of brain injury and signs
predicting prognosis, familial environment, and concepts and goals of intervention.
37
Panteliadis et al., (2015) summarises the most important points
concerning early treatment for Cerebral Palsy. They are
to start general supportive activities within the first year of life to achieve the best
possible benefit for the child.
to assure a loving and stimulating atmosphere during the training and to perform the
exercises with the family members or the next caregivers.
to provide not only technical guidance but also psychological and psychosocial
support to the caregivers.
to communicate not only active but also passive interventions such as in feeding,
bedding and head control (handling) to the caregivers in order to help to avoid
contractures or hip dislocation.
to adjust the treatment setting individually and include frequent repetitions and
positive feedback to promote the essential intrinsic motivation and self-activity.
to promote sensori-motor (and mental) development analogous to that in normal
children; it may be necessary to divide the training in very small development steps,
to implement specific and targeted therapies or even Constraint-induced movement
therapy (CIMT) at an appropriate age. For example, training the hand-mouth
movement is a goal-oriented activity which is possibly achieved only with the support
of the postural control, and
to address associated symptoms separately such as deficits in oral motor skills or
eating disorders.
Panteliadis et al., (2015) summarises the most important points
concerning early treatment for Cerebral Palsy. They are
to start general supportive activities within the first year of life to achieve the best
possible benefit for the child.
to assure a loving and stimulating atmosphere during the training and to perform the
exercises with the family members or the next caregivers.
to provide not only technical guidance but also psychological and psychosocial
support to the caregivers.
to communicate not only active but also passive interventions such as in feeding,
bedding and head control (handling) to the caregivers in order to help to avoid
contractures or hip dislocation.
to adjust the treatment setting individually and include frequent repetitions and
positive feedback to promote the essential intrinsic motivation and self-activity.
to promote sensori-motor (and mental) development analogous to that in normal
children; it may be necessary to divide the training in very small development steps,
to implement specific and targeted therapies or even Constraint-induced movement
therapy (CIMT) at an appropriate age. For example, training the hand-mouth
movement is a goal-oriented activity which is possibly achieved only with the support
of the postural control, and
to address associated symptoms separately such as deficits in oral motor skills or
eating disorders.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
38
McWilliam et al., (1996) conducted a study on therapy services in early
intervention: Current status, barriers, and recommendations and assessed the major
challenges in providing specialized therapies to infants, toddlers, and preschoolers with
disabilities. Result of the study showed that a shortage of pediatric therapists and
policy/administrative constraints caused services to be of lower quality than desired and also
found that concepts of "needing" therapy were muddled and that most people said that "more
is better" as long as the quality is high enough.
Children with disabilities or who are at risk for disabilities often require
intervention in motor and communication development, so occupational therapy, physical
therapy, or speech-language therapy are frequently involved. Early intervention services also
consist, however, of generalists such as early childhood professionals (e.g., early childhood
teachers) and other non therapist professionals (e.g., early childhood special educators, social
workers). Furthermore, families are key players as members of their child's intervention team
through both informal and formal activities. This study explores stakeholders' perceptions of
therapy and the capability of the current number of therapists to meet the demands for
therapy. ( McWilliam et al., 1996)
Pihlar (2013) conducted a study from activity to participation –
occupational therapy intervention for CP children reported that for children participation in
day-to-day formal and informal activities is a vital part of their development. Participation in
activities is the context in which children form friendships, develop skills and competencies,
express creativity, achieve mental and physical health, and determine meaning and purpose in
life. Children with cerebral palsy receive a variety of long-term physical and occupational
McWilliam et al., (1996) conducted a study on therapy services in early
intervention: Current status, barriers, and recommendations and assessed the major
challenges in providing specialized therapies to infants, toddlers, and preschoolers with
disabilities. Result of the study showed that a shortage of pediatric therapists and
policy/administrative constraints caused services to be of lower quality than desired and also
found that concepts of "needing" therapy were muddled and that most people said that "more
is better" as long as the quality is high enough.
Children with disabilities or who are at risk for disabilities often require
intervention in motor and communication development, so occupational therapy, physical
therapy, or speech-language therapy are frequently involved. Early intervention services also
consist, however, of generalists such as early childhood professionals (e.g., early childhood
teachers) and other non therapist professionals (e.g., early childhood special educators, social
workers). Furthermore, families are key players as members of their child's intervention team
through both informal and formal activities. This study explores stakeholders' perceptions of
therapy and the capability of the current number of therapists to meet the demands for
therapy. ( McWilliam et al., 1996)
Pihlar (2013) conducted a study from activity to participation –
occupational therapy intervention for CP children reported that for children participation in
day-to-day formal and informal activities is a vital part of their development. Participation in
activities is the context in which children form friendships, develop skills and competencies,
express creativity, achieve mental and physical health, and determine meaning and purpose in
life. Children with cerebral palsy receive a variety of long-term physical and occupational
39
therapy interventions to facilitate development and to enhance functional independence in
movement, self-care, play, school activities and leisure. The issues presented by cerebral
palsy children and their families are complex and require understanding of multiple levels of
performance. Successful occupational therapy intervention of these multiple layers of
function requires the use of multiple frames of reference, theories and models. Occupational
performance and participation in different activities, is the main goal of occupational therapy
intervention.
Mather and Weinstein (1988) studied the partnership of teachers and
therapists in early intervention. The study traced the background and history of occupational
therapy and special education as they relate to the birth- to 3-year-old population. The study
revealed that as teachers and therapists shared the framework of their professions, a system of
role-release began. Common ground was found in problem solving, case conferences, shared
observation, and record keeping. Mutual trust was established and an eagerness to work
towards the best educational program for these young children became a priority.
The philosophical premise of Occupational Therapy is the belief that
purposeful activity, including its interpersonal and environmental components, may be used
to prevent and mediate dysfunction, and to elicit maximum adaptation. Activity as used by
occupational therapy personnel includes both an intrinsic and therapeutic purpose (American
Occupational Therapy Association, 1979).
Boyt Shell et al., (2014) as stated in Willard & Spackman's
occupational therapy, emphasized the importance of Occupational therapy. It reported that,
therapy interventions to facilitate development and to enhance functional independence in
movement, self-care, play, school activities and leisure. The issues presented by cerebral
palsy children and their families are complex and require understanding of multiple levels of
performance. Successful occupational therapy intervention of these multiple layers of
function requires the use of multiple frames of reference, theories and models. Occupational
performance and participation in different activities, is the main goal of occupational therapy
intervention.
Mather and Weinstein (1988) studied the partnership of teachers and
therapists in early intervention. The study traced the background and history of occupational
therapy and special education as they relate to the birth- to 3-year-old population. The study
revealed that as teachers and therapists shared the framework of their professions, a system of
role-release began. Common ground was found in problem solving, case conferences, shared
observation, and record keeping. Mutual trust was established and an eagerness to work
towards the best educational program for these young children became a priority.
The philosophical premise of Occupational Therapy is the belief that
purposeful activity, including its interpersonal and environmental components, may be used
to prevent and mediate dysfunction, and to elicit maximum adaptation. Activity as used by
occupational therapy personnel includes both an intrinsic and therapeutic purpose (American
Occupational Therapy Association, 1979).
Boyt Shell et al., (2014) as stated in Willard & Spackman's
occupational therapy, emphasized the importance of Occupational therapy. It reported that,
40
since the 1950s, occupational therapists have been involved with young children. Most of the
early programs included children who were diagnosed with biological impairments. Therapy
emphasized independence in function, increasing motor ability, and improving perceptual,
communication, and social skills. Treatment approaches were varied, but all were attempting
to understand normal human development, neurophysiology, and techniques of evaluation.
Therapists began to incorporate into therapy programs the ideas and developmental
approaches most appropriate for the specific patient.
Haley et al., (1988) investigated the patterns of physical and
occupational therapy implementation in early motor intervention and submitted a
comprehensive program evaluation report describing the implementation variation of
physical and occupational therapy for 43 infants with motor delays across six early
intervention programs. The study reported that variations in the intensity of intervention were
related to therapist availability and the severity of infant motor delay.
Batool and Ijaz (2015) conducted a study to evaluate the effectiveness
of Speech and Language Therapy for Children with Autism Spectrum Disorder using ABA
and Pre and Post test research design. The result showed significant differences in children’s
rating on CARS. The scores improved after the therapy and severity of symptoms decreased
from severe to moderate category. The findings of the study concluded that Speech and
language helps enhancing speech, vocabulary, verbal and non verbal communication as well
as sentence building in children with Autism Spectrum Disorder.
since the 1950s, occupational therapists have been involved with young children. Most of the
early programs included children who were diagnosed with biological impairments. Therapy
emphasized independence in function, increasing motor ability, and improving perceptual,
communication, and social skills. Treatment approaches were varied, but all were attempting
to understand normal human development, neurophysiology, and techniques of evaluation.
Therapists began to incorporate into therapy programs the ideas and developmental
approaches most appropriate for the specific patient.
Haley et al., (1988) investigated the patterns of physical and
occupational therapy implementation in early motor intervention and submitted a
comprehensive program evaluation report describing the implementation variation of
physical and occupational therapy for 43 infants with motor delays across six early
intervention programs. The study reported that variations in the intensity of intervention were
related to therapist availability and the severity of infant motor delay.
Batool and Ijaz (2015) conducted a study to evaluate the effectiveness
of Speech and Language Therapy for Children with Autism Spectrum Disorder using ABA
and Pre and Post test research design. The result showed significant differences in children’s
rating on CARS. The scores improved after the therapy and severity of symptoms decreased
from severe to moderate category. The findings of the study concluded that Speech and
language helps enhancing speech, vocabulary, verbal and non verbal communication as well
as sentence building in children with Autism Spectrum Disorder.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
41
Goldstein (2002) conducted a study on communication intervention for
children with Autism: a review of treatment efficacy and reviewed various empirical studies
which evaluated the benefits of speech and language interventions. The study revealed that
interventions incorporating sign language, discrete trial training, and milieu teaching
procedures had been successfully used to expand the communication repertoires of children
with autism. Other important developments in the field stemmed from interventions designed
to replace challenging behaviors and to promote social and scripted interactions.
Opp and Thurmair (1993) studied the bavarian concept of early
intervention for children with developmental delays and children with disabilities. The
concept, development, and experiences of the Bavarian early intervention system were traced
through a historical perspective. Current discussions, pros and cons of proximal (homebound)
and centralized (center-based) services, the call for a changing paradigm of early
intervention, and perspectives concerning Bavarian early intervention were covered in the
study. From the study it was revealed that apart from flexibility for centres to design their
own organizational fit, interdisciplinary work is what matters. Early intervention specialists
need some kind of a base where they can meet as a team and share the competencies of
different professions. It is of central importance for the quality of early intervention that
physical, occupational, and speech therapists; special educators; physicians; and other
professionals engage in interdisciplinary cooperation in handling the diverse task profiles of
early intervention for children with developmental risks and disabilities. Interdisciplinarity,
the quintessence of more than 20 years experience in the early education of children with
developmental risks and/or disabilities in Bavaria, is not easy, but it is indispensable. The
Goldstein (2002) conducted a study on communication intervention for
children with Autism: a review of treatment efficacy and reviewed various empirical studies
which evaluated the benefits of speech and language interventions. The study revealed that
interventions incorporating sign language, discrete trial training, and milieu teaching
procedures had been successfully used to expand the communication repertoires of children
with autism. Other important developments in the field stemmed from interventions designed
to replace challenging behaviors and to promote social and scripted interactions.
Opp and Thurmair (1993) studied the bavarian concept of early
intervention for children with developmental delays and children with disabilities. The
concept, development, and experiences of the Bavarian early intervention system were traced
through a historical perspective. Current discussions, pros and cons of proximal (homebound)
and centralized (center-based) services, the call for a changing paradigm of early
intervention, and perspectives concerning Bavarian early intervention were covered in the
study. From the study it was revealed that apart from flexibility for centres to design their
own organizational fit, interdisciplinary work is what matters. Early intervention specialists
need some kind of a base where they can meet as a team and share the competencies of
different professions. It is of central importance for the quality of early intervention that
physical, occupational, and speech therapists; special educators; physicians; and other
professionals engage in interdisciplinary cooperation in handling the diverse task profiles of
early intervention for children with developmental risks and disabilities. Interdisciplinarity,
the quintessence of more than 20 years experience in the early education of children with
developmental risks and/or disabilities in Bavaria, is not easy, but it is indispensable. The
42
"working team" has to be backed up by in-service training opportunities and by well-planned
and institutionalized team meetings.
Corsello (2005) reviewed the existing intervention programs and
empirical studies on the intervention strategies with a particular emphasis on the birth to 3
age group. The study recognizes the importance of screening and the role of the pediatrician
as critical and recognizes the stability of early diagnosis over time and the importance of
early intervention. The study points out that experts working with children with autism agree
that early intervention is critical. There is professional consensus about certain crucial aspects
of treatment (intensity, family involvement, and focus on generalization) and empirical
evidence for certain intervention strategies. However, study argues that there are many
programs developed for children with autism that differ in philosophy and a lack of research
comparing the various intervention programs. Most of the programs for children with autism
that exist are designed for children of preschool age, and not all are widely known or
available. While outcome data are published for some of these programs, empirical studies
comparing intervention programs are lacking.
2.2.5 RELATED LITERATURE ON THE INVOLVEMENT OF PARENTS IN
EARLY INTERVENTION
Grover (2005) If given appropriate care, children make remarkable
gains in physical and motor development, in linguistic and cognitive functioning as well as
dramatic progress in their emotional, social, regulatory and moral capacities’. That is why it
is so important that children have appropriate supports in terms of the following: protection
"working team" has to be backed up by in-service training opportunities and by well-planned
and institutionalized team meetings.
Corsello (2005) reviewed the existing intervention programs and
empirical studies on the intervention strategies with a particular emphasis on the birth to 3
age group. The study recognizes the importance of screening and the role of the pediatrician
as critical and recognizes the stability of early diagnosis over time and the importance of
early intervention. The study points out that experts working with children with autism agree
that early intervention is critical. There is professional consensus about certain crucial aspects
of treatment (intensity, family involvement, and focus on generalization) and empirical
evidence for certain intervention strategies. However, study argues that there are many
programs developed for children with autism that differ in philosophy and a lack of research
comparing the various intervention programs. Most of the programs for children with autism
that exist are designed for children of preschool age, and not all are widely known or
available. While outcome data are published for some of these programs, empirical studies
comparing intervention programs are lacking.
2.2.5 RELATED LITERATURE ON THE INVOLVEMENT OF PARENTS IN
EARLY INTERVENTION
Grover (2005) If given appropriate care, children make remarkable
gains in physical and motor development, in linguistic and cognitive functioning as well as
dramatic progress in their emotional, social, regulatory and moral capacities’. That is why it
is so important that children have appropriate supports in terms of the following: protection
43
(an environment that is safe from physical and emotional harm); good health (safe water,
hygiene); appropriate nutrition (including exclusive breastfeeding for the first six months),
stimulation (opportunities to explore the world, express curiosity, engage in problem
solving); language development (listening and responding); and most of all in terms of
interaction with and attachment to caring adults.
Mahoney et al., (1998) conducted a study on the relationship of parent-
child interaction to the effectiveness of early intervention Services for at-risk Children and
children with disabilities. The purpose of this investigation was to reexamine the
developmental outcomes attained in four independent intervention research studies in
relationship to parent-child interaction and indicated that intervention effects on child
development were unlikely to occur unless mothers modified their style of interacting with
their children.
Watts Pappas et al., (2015) in their study explored the parental beliefs
and experiences regarding involvement in speech intervention for their child with mild to
moderate speech sound disorder (SSD) using multiple, sequential interviews conducted
during a course of treatment. Twenty-one interviews were conducted with seven parents of
six children with SSD: (1) after their child’s initial assessment, (2) during intervention and
(3) at the conclusion of an intervention block. Qualitative analysis of the interviews revealed
several factors that influenced the parents’ beliefs and experiences. These included: (1) their
motivation to do the right thing by their child; (2) their expectations of parent/ professional
roles; (3) their interactions with their child in the experience; (4) their interactions with the
speech language therapist (SLT); and (5) the nature of the child’s difficulties. The parents in
(an environment that is safe from physical and emotional harm); good health (safe water,
hygiene); appropriate nutrition (including exclusive breastfeeding for the first six months),
stimulation (opportunities to explore the world, express curiosity, engage in problem
solving); language development (listening and responding); and most of all in terms of
interaction with and attachment to caring adults.
Mahoney et al., (1998) conducted a study on the relationship of parent-
child interaction to the effectiveness of early intervention Services for at-risk Children and
children with disabilities. The purpose of this investigation was to reexamine the
developmental outcomes attained in four independent intervention research studies in
relationship to parent-child interaction and indicated that intervention effects on child
development were unlikely to occur unless mothers modified their style of interacting with
their children.
Watts Pappas et al., (2015) in their study explored the parental beliefs
and experiences regarding involvement in speech intervention for their child with mild to
moderate speech sound disorder (SSD) using multiple, sequential interviews conducted
during a course of treatment. Twenty-one interviews were conducted with seven parents of
six children with SSD: (1) after their child’s initial assessment, (2) during intervention and
(3) at the conclusion of an intervention block. Qualitative analysis of the interviews revealed
several factors that influenced the parents’ beliefs and experiences. These included: (1) their
motivation to do the right thing by their child; (2) their expectations of parent/ professional
roles; (3) their interactions with their child in the experience; (4) their interactions with the
speech language therapist (SLT); and (5) the nature of the child’s difficulties. The parents in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
44
the study wanted to be involved in their child’s intervention but were reluctant to participate
in intervention sessions. This preference appeared to be influenced by prior expectations of
parent/ professional roles and a belief that they would ‘interfere’ in the session. Additionally,
whilst the parents appreciated being asked for their opinion regarding intervention goals and
activities, they had a preference for the therapist to take the lead. Parental belief in the SLT as
the expert influenced this preference, but the SLTs’ beliefs and practice may also have played
a role. The less pervasive nature of the child’s difficulties influenced the form of service
preferred by the parents. Most particularly, the parents were more eager to work with their
child at home and had a more marked preference for intervention sessions with the SLT to
focus on their child rather than their family than did parents of children with pervasive
disabilities investigated in other studies. The findings of the study have implications for how
therapists may best work with families of children with less pervasive difficulties in
intervention.
Nelson (2015) investigated the ways in which parents of children aged
2-7 with autism were involved in their children’s early intervention programs and how their
involvement influenced their child’s social skills and behavior. The study explored the
association between parental involvement and the positive behavior and social skills of
children with autism receiving services through an early intervention program.
Kurani et al., (2009) studied the impact of parents’ involvement and
engagement in a learning readiness programme for children with severe and profound
intellectual disability and complex needs in India. The study concluded that the role and
impact of parents as co-trainers of children with severe learning disability and complex needs
the study wanted to be involved in their child’s intervention but were reluctant to participate
in intervention sessions. This preference appeared to be influenced by prior expectations of
parent/ professional roles and a belief that they would ‘interfere’ in the session. Additionally,
whilst the parents appreciated being asked for their opinion regarding intervention goals and
activities, they had a preference for the therapist to take the lead. Parental belief in the SLT as
the expert influenced this preference, but the SLTs’ beliefs and practice may also have played
a role. The less pervasive nature of the child’s difficulties influenced the form of service
preferred by the parents. Most particularly, the parents were more eager to work with their
child at home and had a more marked preference for intervention sessions with the SLT to
focus on their child rather than their family than did parents of children with pervasive
disabilities investigated in other studies. The findings of the study have implications for how
therapists may best work with families of children with less pervasive difficulties in
intervention.
Nelson (2015) investigated the ways in which parents of children aged
2-7 with autism were involved in their children’s early intervention programs and how their
involvement influenced their child’s social skills and behavior. The study explored the
association between parental involvement and the positive behavior and social skills of
children with autism receiving services through an early intervention program.
Kurani et al., (2009) studied the impact of parents’ involvement and
engagement in a learning readiness programme for children with severe and profound
intellectual disability and complex needs in India. The study concluded that the role and
impact of parents as co-trainers of children with severe learning disability and complex needs
45
cannot be underestimated; nor can the role and impact of joint multidisciplinary team effort.
If a timely, intensive special education, training and therapeutic programme is provided by
teachers, therapists and parents as a team; children (4 to 12 years) with severe and profound
learning disabilities and complex needs are able to achieve independence in personal social
skills, living without excessive assistance from parents and other adults.
Shonkoff et al., (1986) conducted a quantitative analysis of the effects
of early intervention for disabled infants and their families by evaluating 31 selected studies.
The results indicated that early intervention was effective in promoting developmental
progress in infants and toddlers with biologically based disabilities. It was found that, the
programs that served a heterogeneous group of children, provided a structured curriculum
and which targeted their efforts on parents and children together appeared to be the most
effective.
CONCLUSION
Review has provided evidence that the researcher is familiar with what
is already known and what is still unknown. The researcher has done a comprehensive and
exhaustive literature review. This work enabled the researcher to go through and furnish
current theoretical and empirical knowledge about Early Intervention for children with
Developmental Disabilities and the importance of Parental Involvement in Early Intervention
Programmes.
cannot be underestimated; nor can the role and impact of joint multidisciplinary team effort.
If a timely, intensive special education, training and therapeutic programme is provided by
teachers, therapists and parents as a team; children (4 to 12 years) with severe and profound
learning disabilities and complex needs are able to achieve independence in personal social
skills, living without excessive assistance from parents and other adults.
Shonkoff et al., (1986) conducted a quantitative analysis of the effects
of early intervention for disabled infants and their families by evaluating 31 selected studies.
The results indicated that early intervention was effective in promoting developmental
progress in infants and toddlers with biologically based disabilities. It was found that, the
programs that served a heterogeneous group of children, provided a structured curriculum
and which targeted their efforts on parents and children together appeared to be the most
effective.
CONCLUSION
Review has provided evidence that the researcher is familiar with what
is already known and what is still unknown. The researcher has done a comprehensive and
exhaustive literature review. This work enabled the researcher to go through and furnish
current theoretical and empirical knowledge about Early Intervention for children with
Developmental Disabilities and the importance of Parental Involvement in Early Intervention
Programmes.
46
METHODOLOGY
3.1 INTRODUCTION
Methodology is the systematic, theoretical analysis of the methods
applied to a field of study. Research methodology is a collective term for the structured
process of conducting research. There are many different methodologies used in various
types of research. Methodology of investigation is the core of every research work. It is the
way and methods adopted for the completion of research work.
This chapter attempts to provide details with regard to the methodology
of the study. This includes details of the tools used, sample selected for the study, procedure
of data collection, scoring, and statistics used. These are discussed under respective titles.
3.2 RESEARCH DESIGN
The research design provides a complete guideline for data collection.
It is a systematic plan for what is to be done, how it will be done and how the data will be
analysed.
In order to achieve the objectives of the study, the investigator selected
the descriptive survey method to analyse the level of parental awareness and involvement in
early intervention of children with developmental disabilities. Descriptive research involves
collecting data in order to test hypothesis or answer questions concerning the current status of
the subject of the study. A survey is conducted to accumulate data from a selected group of
population so as to find out the current status of that population with respect to various
variables.
METHODOLOGY
3.1 INTRODUCTION
Methodology is the systematic, theoretical analysis of the methods
applied to a field of study. Research methodology is a collective term for the structured
process of conducting research. There are many different methodologies used in various
types of research. Methodology of investigation is the core of every research work. It is the
way and methods adopted for the completion of research work.
This chapter attempts to provide details with regard to the methodology
of the study. This includes details of the tools used, sample selected for the study, procedure
of data collection, scoring, and statistics used. These are discussed under respective titles.
3.2 RESEARCH DESIGN
The research design provides a complete guideline for data collection.
It is a systematic plan for what is to be done, how it will be done and how the data will be
analysed.
In order to achieve the objectives of the study, the investigator selected
the descriptive survey method to analyse the level of parental awareness and involvement in
early intervention of children with developmental disabilities. Descriptive research involves
collecting data in order to test hypothesis or answer questions concerning the current status of
the subject of the study. A survey is conducted to accumulate data from a selected group of
population so as to find out the current status of that population with respect to various
variables.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
47
3.3 POPULATION
The population selected for this study consisted of parents of children
with developmental disabilities attending early intervention services in different parts of
Kottayam and Ernakulam districts of Kerala State.
3.4 SAMPLES FOR THE STUDY
In this study the investigator selected parents of 110 children with developmental disabilities
attending early intervention services in different parts of Kottayam and Ernakulam districts of
Kerala..
Sample Design
Random Sampling Technique was used to select the sample. The sample consists of 57
parents of Kottayam district and 53 parents of Ernakulam district. The following tables that
show the classification of samples on the basis of gender, age, location, education,
employment, religion and years in early intervention are given:
3.3 POPULATION
The population selected for this study consisted of parents of children
with developmental disabilities attending early intervention services in different parts of
Kottayam and Ernakulam districts of Kerala State.
3.4 SAMPLES FOR THE STUDY
In this study the investigator selected parents of 110 children with developmental disabilities
attending early intervention services in different parts of Kottayam and Ernakulam districts of
Kerala..
Sample Design
Random Sampling Technique was used to select the sample. The sample consists of 57
parents of Kottayam district and 53 parents of Ernakulam district. The following tables that
show the classification of samples on the basis of gender, age, location, education,
employment, religion and years in early intervention are given:
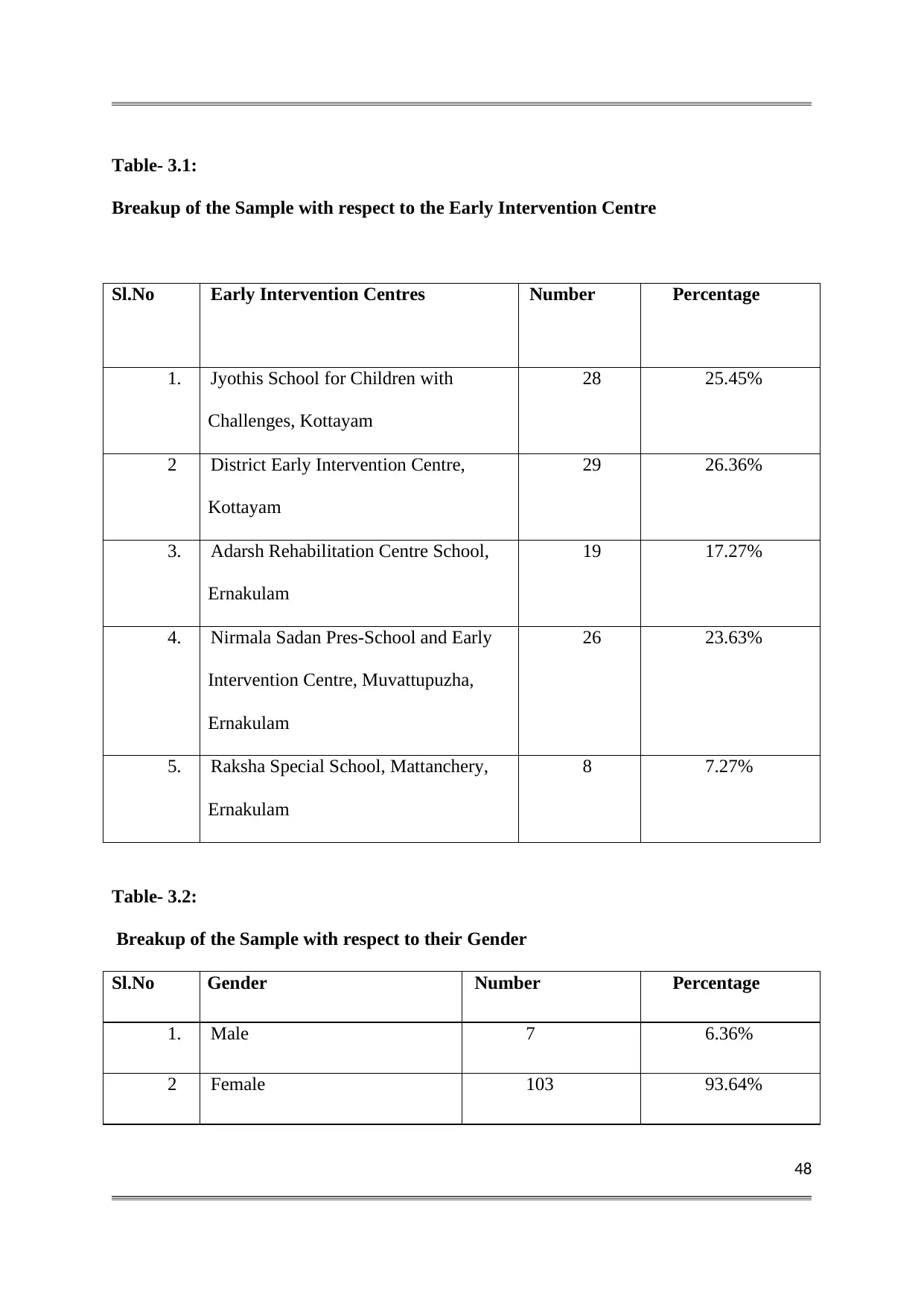
48
Table- 3.1:
Breakup of the Sample with respect to the Early Intervention Centre
Sl.No Early Intervention Centres Number Percentage
1. Jyothis School for Children with
Challenges, Kottayam
28 25.45%
2 District Early Intervention Centre,
Kottayam
29 26.36%
3. Adarsh Rehabilitation Centre School,
Ernakulam
19 17.27%
4. Nirmala Sadan Pres-School and Early
Intervention Centre, Muvattupuzha,
Ernakulam
26 23.63%
5. Raksha Special School, Mattanchery,
Ernakulam
8 7.27%
Table- 3.2:
Breakup of the Sample with respect to their Gender
Sl.No Gender Number Percentage
1. Male 7 6.36%
2 Female 103 93.64%
Table- 3.1:
Breakup of the Sample with respect to the Early Intervention Centre
Sl.No Early Intervention Centres Number Percentage
1. Jyothis School for Children with
Challenges, Kottayam
28 25.45%
2 District Early Intervention Centre,
Kottayam
29 26.36%
3. Adarsh Rehabilitation Centre School,
Ernakulam
19 17.27%
4. Nirmala Sadan Pres-School and Early
Intervention Centre, Muvattupuzha,
Ernakulam
26 23.63%
5. Raksha Special School, Mattanchery,
Ernakulam
8 7.27%
Table- 3.2:
Breakup of the Sample with respect to their Gender
Sl.No Gender Number Percentage
1. Male 7 6.36%
2 Female 103 93.64%
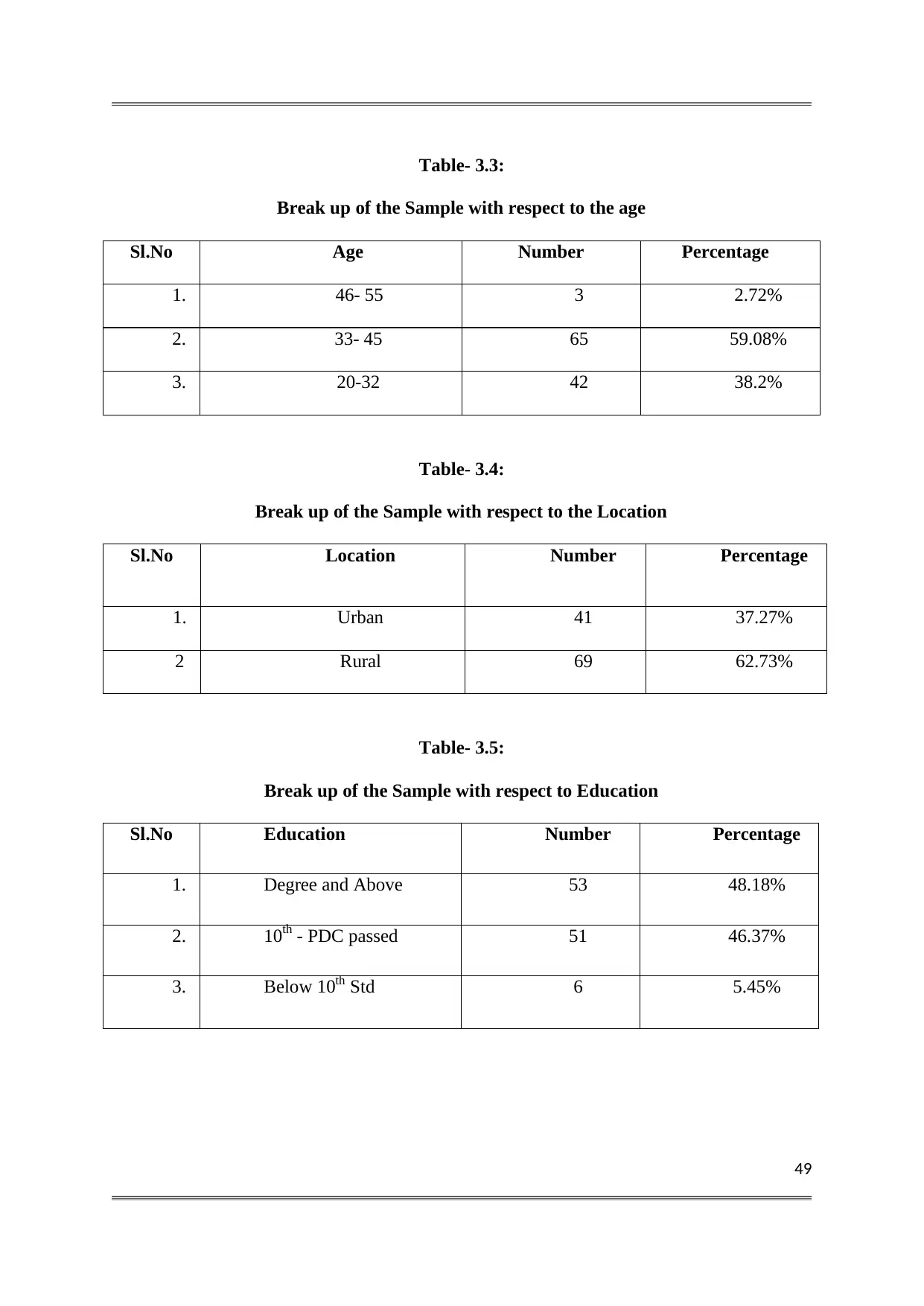
49
Table- 3.3:
Break up of the Sample with respect to the age
Sl.No Age Number Percentage
1. 46- 55 3 2.72%
2. 33- 45 65 59.08%
3. 20-32 42 38.2%
Table- 3.4:
Break up of the Sample with respect to the Location
Sl.No Location Number Percentage
1. Urban 41 37.27%
2 Rural 69 62.73%
Table- 3.5:
Break up of the Sample with respect to Education
Sl.No Education Number Percentage
1. Degree and Above 53 48.18%
2. 10th - PDC passed 51 46.37%
3. Below 10th Std 6 5.45%
Table- 3.3:
Break up of the Sample with respect to the age
Sl.No Age Number Percentage
1. 46- 55 3 2.72%
2. 33- 45 65 59.08%
3. 20-32 42 38.2%
Table- 3.4:
Break up of the Sample with respect to the Location
Sl.No Location Number Percentage
1. Urban 41 37.27%
2 Rural 69 62.73%
Table- 3.5:
Break up of the Sample with respect to Education
Sl.No Education Number Percentage
1. Degree and Above 53 48.18%
2. 10th - PDC passed 51 46.37%
3. Below 10th Std 6 5.45%
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
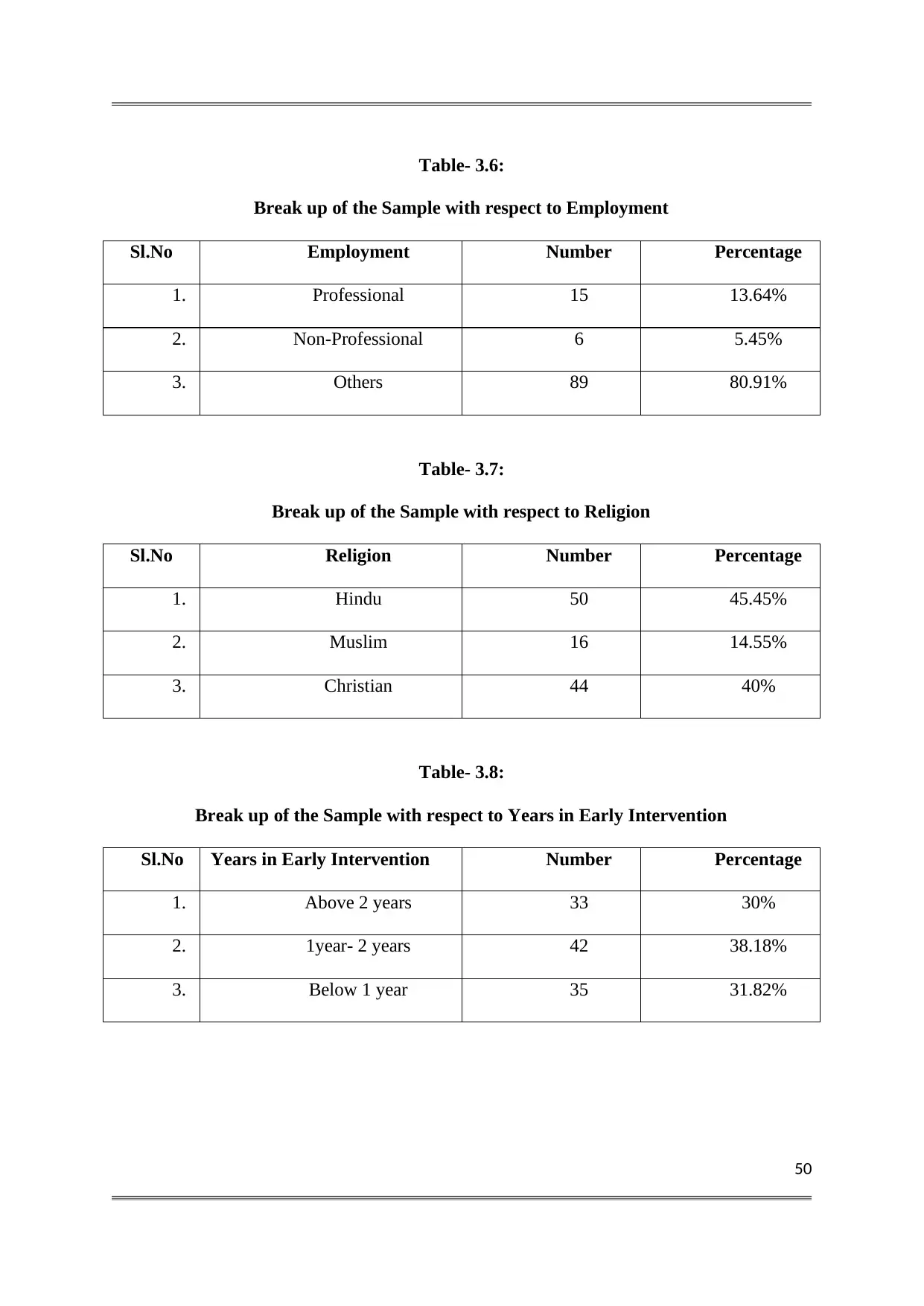
50
Table- 3.6:
Break up of the Sample with respect to Employment
Sl.No Employment Number Percentage
1. Professional 15 13.64%
2. Non-Professional 6 5.45%
3. Others 89 80.91%
Table- 3.7:
Break up of the Sample with respect to Religion
Sl.No Religion Number Percentage
1. Hindu 50 45.45%
2. Muslim 16 14.55%
3. Christian 44 40%
Table- 3.8:
Break up of the Sample with respect to Years in Early Intervention
Sl.No Years in Early Intervention Number Percentage
1. Above 2 years 33 30%
2. 1year- 2 years 42 38.18%
3. Below 1 year 35 31.82%
Table- 3.6:
Break up of the Sample with respect to Employment
Sl.No Employment Number Percentage
1. Professional 15 13.64%
2. Non-Professional 6 5.45%
3. Others 89 80.91%
Table- 3.7:
Break up of the Sample with respect to Religion
Sl.No Religion Number Percentage
1. Hindu 50 45.45%
2. Muslim 16 14.55%
3. Christian 44 40%
Table- 3.8:
Break up of the Sample with respect to Years in Early Intervention
Sl.No Years in Early Intervention Number Percentage
1. Above 2 years 33 30%
2. 1year- 2 years 42 38.18%
3. Below 1 year 35 31.82%
51
3.5 TOOLS USED FOR DATA COLLECTION
The present study attempts to reveal the parental awareness and
involvement in early intervention of children with developmental disabilities. For this
purpose, the investigator developed a Likert type awareness inventory for the collection of
data.
The following tools and techniques were used for collecting data for
the present study.
1. General Data Sheet
2. Parental Awareness Inventory
3. Parental Involvement Scale
Description of Tools
3.5.1. General Data Sheet
The investigator developed a general data sheet to collect relevant data
on certain selected socio-demographic variables. The general data sheet was included to
obtain information needed for classifying the sample into subgroups on the basis of variables
such as age, gender, location, religion, education, employment, and the years spent in early
intervention. The general data sheet was to be filled by the parents. It is provided in the
Appendix.
3.5.2 Parental Awareness Inventory
The inventory developed by the investigator contained 46 statements in
total. It was developed to collect parental awareness regarding early intervention of children
with developmental disabilities.
3.5 TOOLS USED FOR DATA COLLECTION
The present study attempts to reveal the parental awareness and
involvement in early intervention of children with developmental disabilities. For this
purpose, the investigator developed a Likert type awareness inventory for the collection of
data.
The following tools and techniques were used for collecting data for
the present study.
1. General Data Sheet
2. Parental Awareness Inventory
3. Parental Involvement Scale
Description of Tools
3.5.1. General Data Sheet
The investigator developed a general data sheet to collect relevant data
on certain selected socio-demographic variables. The general data sheet was included to
obtain information needed for classifying the sample into subgroups on the basis of variables
such as age, gender, location, religion, education, employment, and the years spent in early
intervention. The general data sheet was to be filled by the parents. It is provided in the
Appendix.
3.5.2 Parental Awareness Inventory
The inventory developed by the investigator contained 46 statements in
total. It was developed to collect parental awareness regarding early intervention of children
with developmental disabilities.
52
In order to facilitate the analysis of data, the statements were grouped
based on the objectives of the study. The inventory consisted of four sections that included,
Parental Awareness on the Importance of Early Intervention, Importance of Parental
Involvement in Early Intervention, Developmental Disabilities and Early Intervention
Services. The first section was meant to measure the level of parental awareness on the
importance of early intervention. It contains 10 statements. The second section was meant to
measure the level of parental awareness on the Importance of Parental Involvement in Early
Intervention. It contains 7 items. The third section was meant to measure the level of
awareness on Developmental disabilities and it contains 16 items. And the last section of
Parental Awareness inventory was meant to measure the Parental Awareness on the Early
Intervention Services. It includes 13 items. The statements of the inventory were selected
after thorough review of available literature. There were both positive and negative
statements. The responses were rated on a five point rating scale, with option such as
“Strongly agree, Agree, Uncertain, Disagree, and strongly disagree. The respondents were
asked to put a tick mark on the appropriate options.
3.5.3 Parental Involvement Scale
The inventory developed by the investigator contained 11 items. It was
developed to collect the level of involvement of parents in early intervention. The statement
of the scale was selected after thorough review of available literature. The responses were
rated on a three point rating scale, with options such as, Always, sometimes and Never.
In order to facilitate the analysis of data, the statements were grouped
based on the objectives of the study. The inventory consisted of four sections that included,
Parental Awareness on the Importance of Early Intervention, Importance of Parental
Involvement in Early Intervention, Developmental Disabilities and Early Intervention
Services. The first section was meant to measure the level of parental awareness on the
importance of early intervention. It contains 10 statements. The second section was meant to
measure the level of parental awareness on the Importance of Parental Involvement in Early
Intervention. It contains 7 items. The third section was meant to measure the level of
awareness on Developmental disabilities and it contains 16 items. And the last section of
Parental Awareness inventory was meant to measure the Parental Awareness on the Early
Intervention Services. It includes 13 items. The statements of the inventory were selected
after thorough review of available literature. There were both positive and negative
statements. The responses were rated on a five point rating scale, with option such as
“Strongly agree, Agree, Uncertain, Disagree, and strongly disagree. The respondents were
asked to put a tick mark on the appropriate options.
3.5.3 Parental Involvement Scale
The inventory developed by the investigator contained 11 items. It was
developed to collect the level of involvement of parents in early intervention. The statement
of the scale was selected after thorough review of available literature. The responses were
rated on a three point rating scale, with options such as, Always, sometimes and Never.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
53
3.5.4 Standardization procedure
Parental Awareness Inventory
The investigator developed the Parental Awareness Inventory grouped
under 4 objectives. Using the tool, the investigator collected data from 57 parents of
Kottayam district and 53 parents of Ernakulam district. The scoring of each response was
done according to the score key. After computing the sum of each inventory the investigator
arranged the scores of each inventory in ascending order and then selected the upper and
lower one-third of these scores. For getting the significant items, the investigator took the
scores of each item from upper and lower part and computed the‘t’ value , and determined the
significance. After completing the item analysis, the investigator got 9 items from the first
objective, 5 items from the second objective, and 12 items each from the third and fourth
objectives.
Parental Involvement Scale
The investigator developed Parental Involvement Scale consisting of
11 items. Using the tool, the investigator collected data from 57 parents of Ernakulam
district. The scoring of each response was done according to the score key. After computing
the sum of each scale, the investigator arranged the scores in ascending order and then
selected the upper and lower one-third of these scores. For getting the significant items, the
investigator conducted the item analysis. For this process, the investigator took the scores of
each item from upper and lower part and computed the ‘t’ value and determined the
significance. After item analysis it was found that all the items were significant in Parent
Involvement Scale.
3.5.4 Standardization procedure
Parental Awareness Inventory
The investigator developed the Parental Awareness Inventory grouped
under 4 objectives. Using the tool, the investigator collected data from 57 parents of
Kottayam district and 53 parents of Ernakulam district. The scoring of each response was
done according to the score key. After computing the sum of each inventory the investigator
arranged the scores of each inventory in ascending order and then selected the upper and
lower one-third of these scores. For getting the significant items, the investigator took the
scores of each item from upper and lower part and computed the‘t’ value , and determined the
significance. After completing the item analysis, the investigator got 9 items from the first
objective, 5 items from the second objective, and 12 items each from the third and fourth
objectives.
Parental Involvement Scale
The investigator developed Parental Involvement Scale consisting of
11 items. Using the tool, the investigator collected data from 57 parents of Ernakulam
district. The scoring of each response was done according to the score key. After computing
the sum of each scale, the investigator arranged the scores in ascending order and then
selected the upper and lower one-third of these scores. For getting the significant items, the
investigator conducted the item analysis. For this process, the investigator took the scores of
each item from upper and lower part and computed the ‘t’ value and determined the
significance. After item analysis it was found that all the items were significant in Parent
Involvement Scale.
54
Reliability of Parental Awareness Inventory
The reliability of the newly constructed awareness scale was found.
The split half reliability was found to be 0.900. This coefficient indicates a reasonable high
level of reliability.
Reliability of Parental Involvement Scale
The reliability of the newly constructed Parental Involvement scale was
found. The split half reliability was found to be 0.885. This coefficient indicates a reasonable
high level of reliability.
3.6 SCORING
The Parental Awareness Inventory consisted of 46 items grouped under
4 objectives. For each statement, five alternative responses were given, such as, Strongly
Agree, Agree, Uncertain, Disagree and Strongly Disagree. For the positive statements, the
responses were assigned values 4,3,2,1,0 respectively and for negative statements the
responses were assigned values 0,1,2,3,4 respectively. The sum total of 46 items, provided
the total score of parents. The maximum obtainable score is 184 and Minimum obtainable
score 0.
The second Inventory i.e, Parental Involvement Inventory consists of 11 items. For
each statement, 3 alternatives were given, such as, Always, Sometimes and Never. The values
assigned were 2,1,0 respectively. The sum total of 11 items, provided the total score of
parents. The maximum obtainable score is 22 and minimum obtainable score 0.
Reliability of Parental Awareness Inventory
The reliability of the newly constructed awareness scale was found.
The split half reliability was found to be 0.900. This coefficient indicates a reasonable high
level of reliability.
Reliability of Parental Involvement Scale
The reliability of the newly constructed Parental Involvement scale was
found. The split half reliability was found to be 0.885. This coefficient indicates a reasonable
high level of reliability.
3.6 SCORING
The Parental Awareness Inventory consisted of 46 items grouped under
4 objectives. For each statement, five alternative responses were given, such as, Strongly
Agree, Agree, Uncertain, Disagree and Strongly Disagree. For the positive statements, the
responses were assigned values 4,3,2,1,0 respectively and for negative statements the
responses were assigned values 0,1,2,3,4 respectively. The sum total of 46 items, provided
the total score of parents. The maximum obtainable score is 184 and Minimum obtainable
score 0.
The second Inventory i.e, Parental Involvement Inventory consists of 11 items. For
each statement, 3 alternatives were given, such as, Always, Sometimes and Never. The values
assigned were 2,1,0 respectively. The sum total of 11 items, provided the total score of
parents. The maximum obtainable score is 22 and minimum obtainable score 0.
55
3.7 PROCEDURE FOR DATA COLLECTION
The investigator personally contacted the authorities of Early
Intervention Centres. The scope of the study was briefly explained to them and their
permission was sought before collecting data from parents. Permission of parents was also
sought either directly or indirectly through the authorities. The inventories were distributed
and the guidelines and instruction on filling the inventory were given to the parents by the
investigator. Accordingly, the parents filled in the general data sheet, Parental Awareness
Inventory and Parental Involvement Inventory. Assurance was given to the parents, that the
responses given by them would be used for research purposes only.
3.8 STATISTICAL TECHNIQUES USED
The collected data were analyzed with respect to a number of
background variables. The following statistical techniques were used for this purpose:
1) Computation of frequencies and percentages
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of‘t’ value to test the significance of difference between the means of two
groups of data.
4) One Way Analysis of Variance to test the significance of difference between the means of
three or more groups of data
3.7 PROCEDURE FOR DATA COLLECTION
The investigator personally contacted the authorities of Early
Intervention Centres. The scope of the study was briefly explained to them and their
permission was sought before collecting data from parents. Permission of parents was also
sought either directly or indirectly through the authorities. The inventories were distributed
and the guidelines and instruction on filling the inventory were given to the parents by the
investigator. Accordingly, the parents filled in the general data sheet, Parental Awareness
Inventory and Parental Involvement Inventory. Assurance was given to the parents, that the
responses given by them would be used for research purposes only.
3.8 STATISTICAL TECHNIQUES USED
The collected data were analyzed with respect to a number of
background variables. The following statistical techniques were used for this purpose:
1) Computation of frequencies and percentages
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of‘t’ value to test the significance of difference between the means of two
groups of data.
4) One Way Analysis of Variance to test the significance of difference between the means of
three or more groups of data
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
56
DATA ANALYSIS AND INTERPRETATION
4.1 INTRODUCTION
This chapter deals with the analysis and interpretation of the data
collected using the tools. The analysis and interpretation of the collected data was done on the
basis of the objectives of the study. The objective of the study is to find out the level of
parental awareness and involvement in the early intervention of children with developmental
disabilities. The analysis and interpretation of the results have been presented under the
following heads.
Total Parental Awareness in Early Intervention of children with developmental
disabilities
Parental Awareness on the importance of Early Intervention.
Parental Awareness on the importance of Parental Involvement
Parental Awareness of Developmental Disabilities.
Parental Awareness on Early Intervention Services.
Parental Awareness with respect to certain child related and parent related variable.
Total Parental Involvement in Early Intervention of children with developmental
disabilities.
Parental Involvement in early intervention with respect to certain child related and
parent related variable.
DATA ANALYSIS AND INTERPRETATION
4.1 INTRODUCTION
This chapter deals with the analysis and interpretation of the data
collected using the tools. The analysis and interpretation of the collected data was done on the
basis of the objectives of the study. The objective of the study is to find out the level of
parental awareness and involvement in the early intervention of children with developmental
disabilities. The analysis and interpretation of the results have been presented under the
following heads.
Total Parental Awareness in Early Intervention of children with developmental
disabilities
Parental Awareness on the importance of Early Intervention.
Parental Awareness on the importance of Parental Involvement
Parental Awareness of Developmental Disabilities.
Parental Awareness on Early Intervention Services.
Parental Awareness with respect to certain child related and parent related variable.
Total Parental Involvement in Early Intervention of children with developmental
disabilities.
Parental Involvement in early intervention with respect to certain child related and
parent related variable.
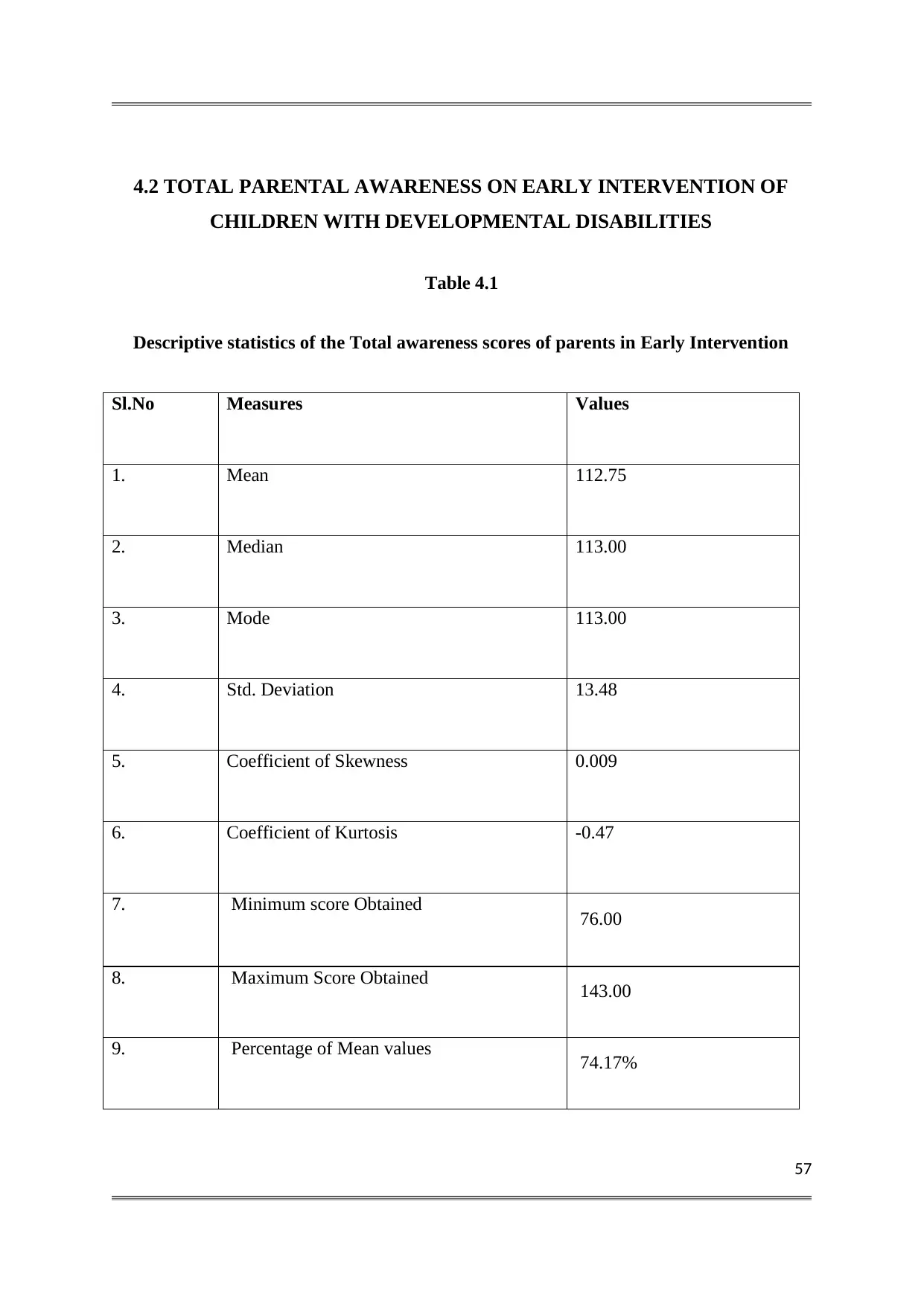
57
4.2 TOTAL PARENTAL AWARENESS ON EARLY INTERVENTION OF
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Table 4.1
Descriptive statistics of the Total awareness scores of parents in Early Intervention
Sl.No Measures Values
1. Mean 112.75
2. Median 113.00
3. Mode 113.00
4. Std. Deviation 13.48
5. Coefficient of Skewness 0.009
6. Coefficient of Kurtosis -0.47
7. Minimum score Obtained 76.00
8. Maximum Score Obtained 143.00
9. Percentage of Mean values 74.17%
4.2 TOTAL PARENTAL AWARENESS ON EARLY INTERVENTION OF
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Table 4.1
Descriptive statistics of the Total awareness scores of parents in Early Intervention
Sl.No Measures Values
1. Mean 112.75
2. Median 113.00
3. Mode 113.00
4. Std. Deviation 13.48
5. Coefficient of Skewness 0.009
6. Coefficient of Kurtosis -0.47
7. Minimum score Obtained 76.00
8. Maximum Score Obtained 143.00
9. Percentage of Mean values 74.17%
58
Table 4.1 shows that the mean score is 112.75, that point to average
level of awareness of parents in early intervention. The median is 113 that mean the 50% of
the parents have a score above 113 and remaining 50% have a score below 113. The mode is
113 that mean 113 are the most repeated score in this distribution. The standard deviation of
the awareness scores of parents is 13.48, which shows that the scores are not closely packed
and there is reasonable scatter among the awareness scores. The range of the score is 67. The
Skewness is 0.009 this positive skewness shows that the scores are massed at the left end of
the distribution. The Kurtosis of the awareness scores is -0.47, this value is less than 0.263
so the nature of the distribution is Leptokurtic. The minimum score obtained is 76 and the
maximum score obtained is 143. The percentage of mean value is 74.17%. Hence, most of
the parents have high level of awareness on early intervention.
Table 4.1 shows that the mean score is 112.75, that point to average
level of awareness of parents in early intervention. The median is 113 that mean the 50% of
the parents have a score above 113 and remaining 50% have a score below 113. The mode is
113 that mean 113 are the most repeated score in this distribution. The standard deviation of
the awareness scores of parents is 13.48, which shows that the scores are not closely packed
and there is reasonable scatter among the awareness scores. The range of the score is 67. The
Skewness is 0.009 this positive skewness shows that the scores are massed at the left end of
the distribution. The Kurtosis of the awareness scores is -0.47, this value is less than 0.263
so the nature of the distribution is Leptokurtic. The minimum score obtained is 76 and the
maximum score obtained is 143. The percentage of mean value is 74.17%. Hence, most of
the parents have high level of awareness on early intervention.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
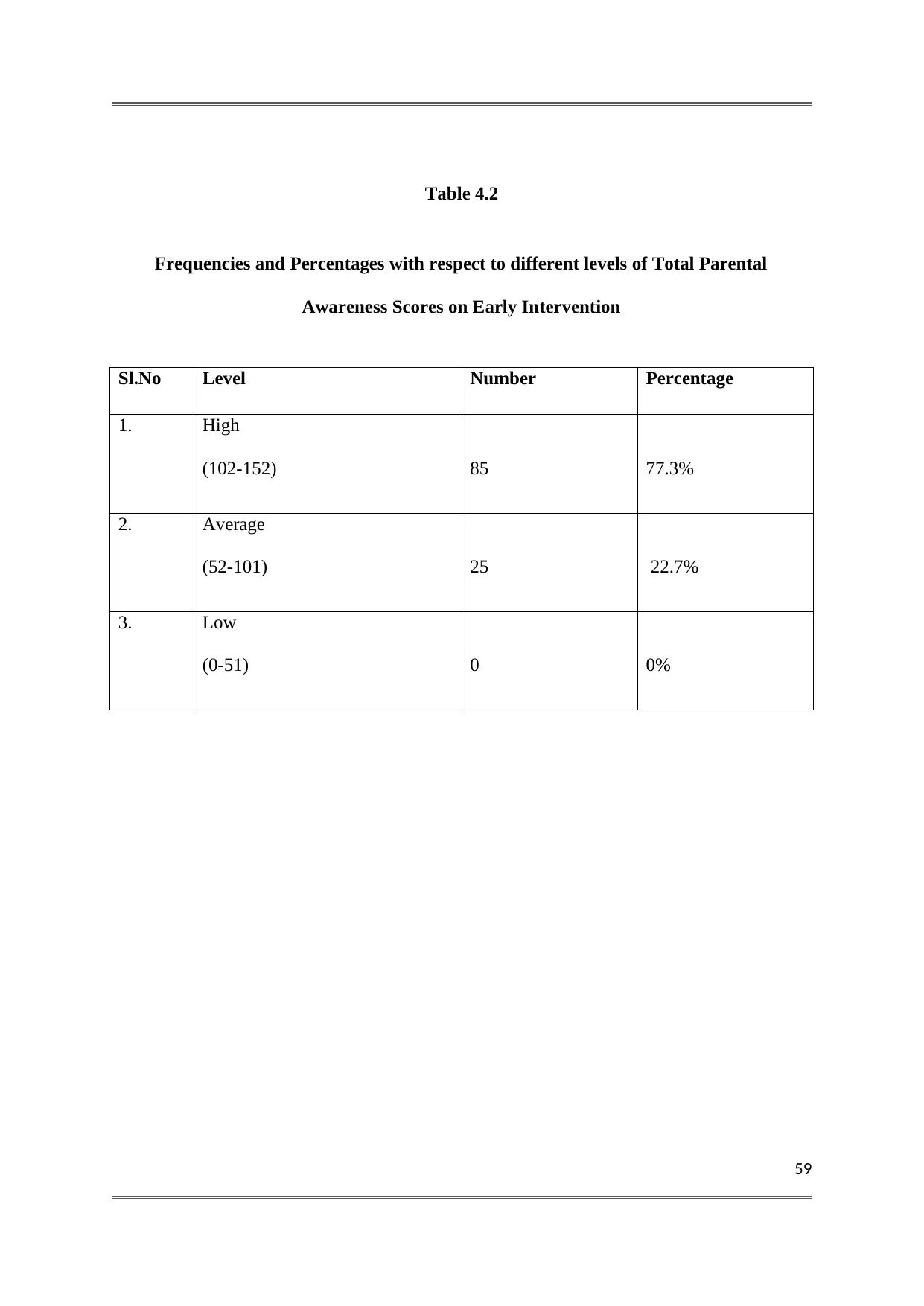
59
Table 4.2
Frequencies and Percentages with respect to different levels of Total Parental
Awareness Scores on Early Intervention
Sl.No Level Number Percentage
1. High
(102-152) 85 77.3%
2. Average
(52-101) 25 22.7%
3. Low
(0-51) 0 0%
Table 4.2
Frequencies and Percentages with respect to different levels of Total Parental
Awareness Scores on Early Intervention
Sl.No Level Number Percentage
1. High
(102-152) 85 77.3%
2. Average
(52-101) 25 22.7%
3. Low
(0-51) 0 0%
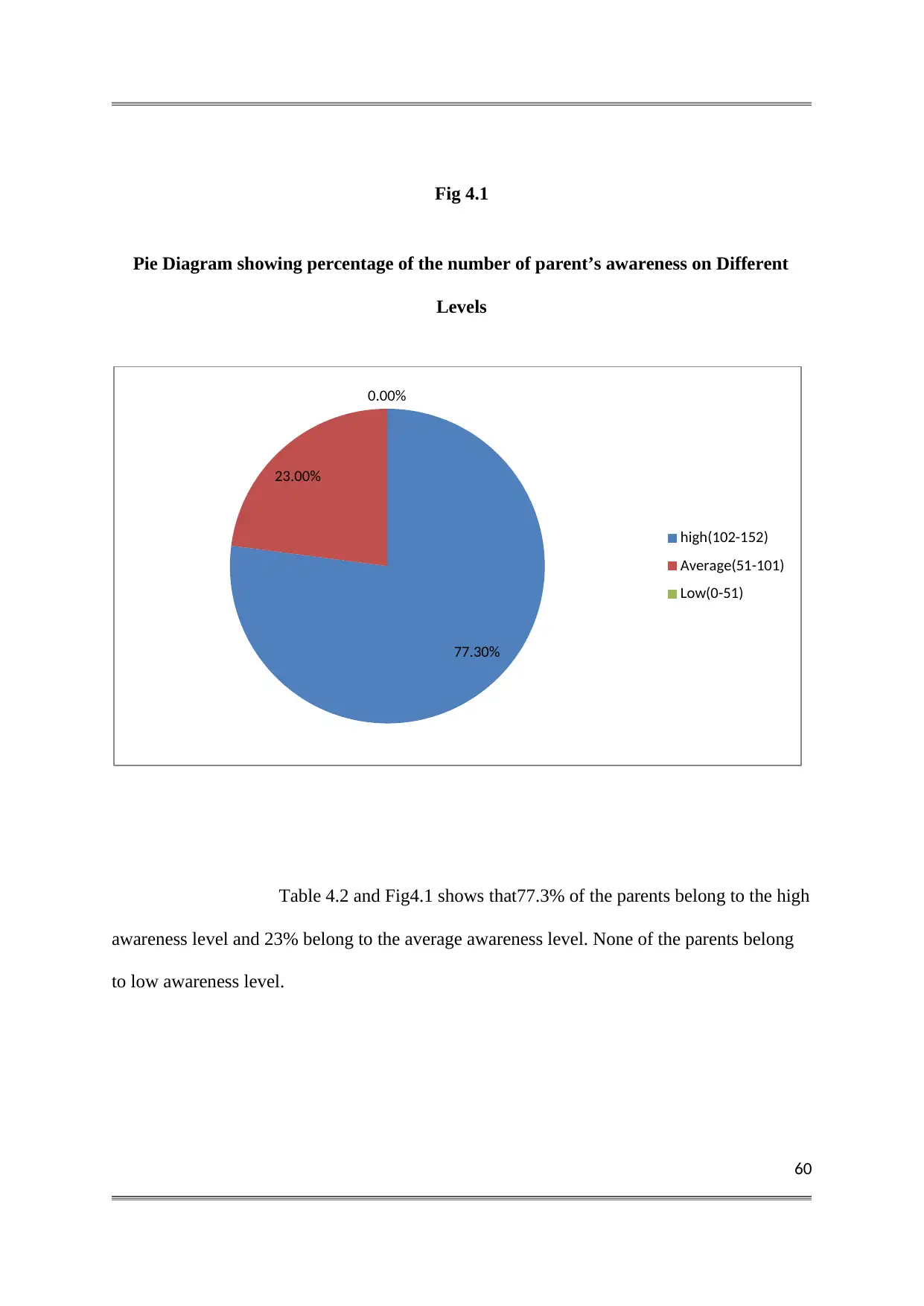
60
Fig 4.1
Pie Diagram showing percentage of the number of parent’s awareness on Different
Levels
Table 4.2 and Fig4.1 shows that77.3% of the parents belong to the high
awareness level and 23% belong to the average awareness level. None of the parents belong
to low awareness level.
77.30%
23.00%
0.00%
high(102-152)
Average(51-101)
Low(0-51)
Fig 4.1
Pie Diagram showing percentage of the number of parent’s awareness on Different
Levels
Table 4.2 and Fig4.1 shows that77.3% of the parents belong to the high
awareness level and 23% belong to the average awareness level. None of the parents belong
to low awareness level.
77.30%
23.00%
0.00%
high(102-152)
Average(51-101)
Low(0-51)
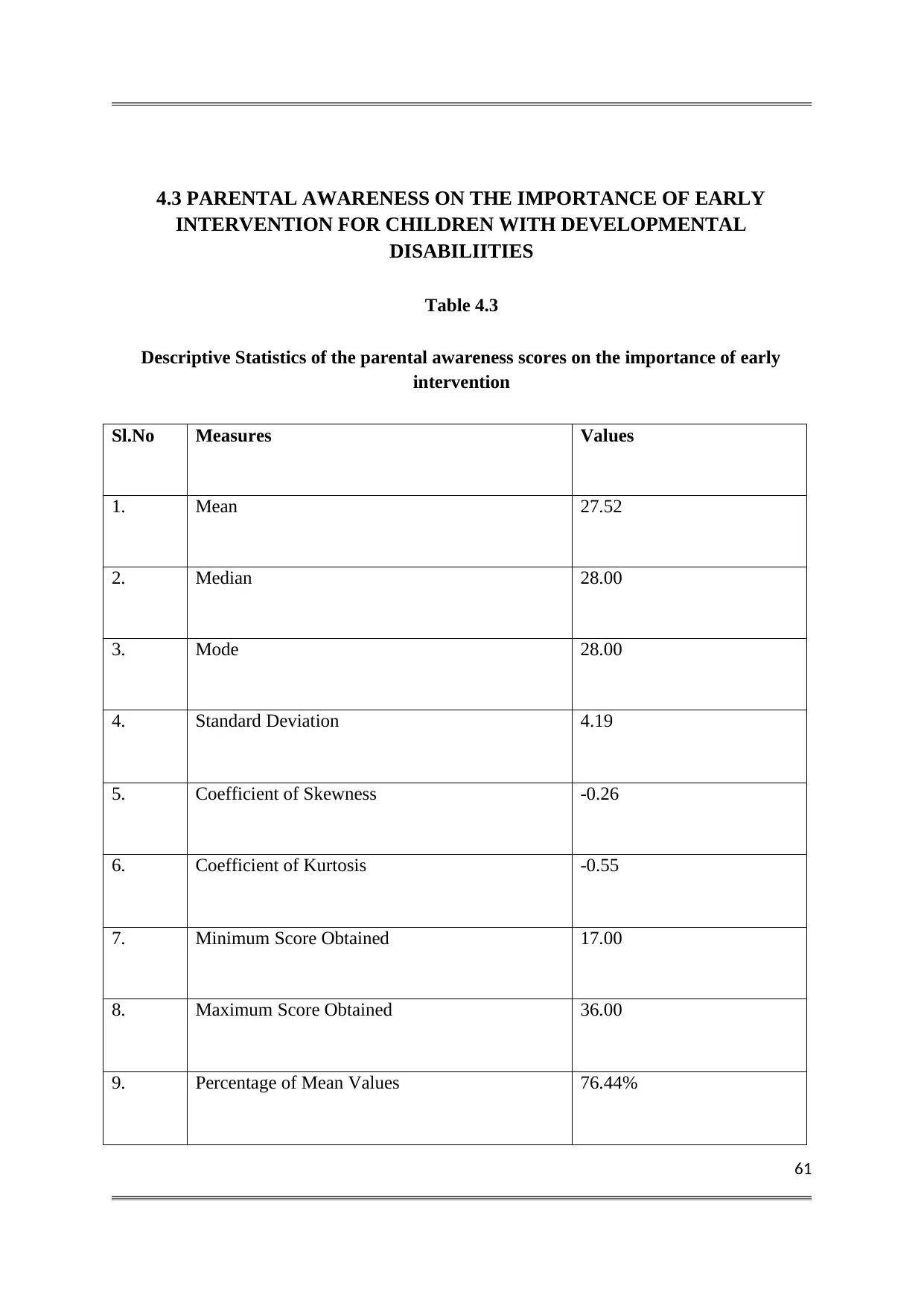
61
4.3 PARENTAL AWARENESS ON THE IMPORTANCE OF EARLY
INTERVENTION FOR CHILDREN WITH DEVELOPMENTAL
DISABILIITIES
Table 4.3
Descriptive Statistics of the parental awareness scores on the importance of early
intervention
Sl.No Measures Values
1. Mean 27.52
2. Median 28.00
3. Mode 28.00
4. Standard Deviation 4.19
5. Coefficient of Skewness -0.26
6. Coefficient of Kurtosis -0.55
7. Minimum Score Obtained 17.00
8. Maximum Score Obtained 36.00
9. Percentage of Mean Values 76.44%
4.3 PARENTAL AWARENESS ON THE IMPORTANCE OF EARLY
INTERVENTION FOR CHILDREN WITH DEVELOPMENTAL
DISABILIITIES
Table 4.3
Descriptive Statistics of the parental awareness scores on the importance of early
intervention
Sl.No Measures Values
1. Mean 27.52
2. Median 28.00
3. Mode 28.00
4. Standard Deviation 4.19
5. Coefficient of Skewness -0.26
6. Coefficient of Kurtosis -0.55
7. Minimum Score Obtained 17.00
8. Maximum Score Obtained 36.00
9. Percentage of Mean Values 76.44%
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
62
Table 4.3 shows that the mean score is 27.52 that points to high level
of awareness of parents regarding the importance of early intervention. The median is 28 that
mean the 50% of the parents have a score above 28 and remaining 50% have the score below
28. The mode is 28 that mean 28 are the most repeated scores in this distribution. The
standard deviation of the awareness scores of parents is 4.19 which show that the scores are
not closely packed and there is reasonable scatter among the awareness scores. The range of
the score is 19. The skewness is -0.26 this negative skewness shows that the scores are
massed at the right end. The kurtosis of the awareness scores is -0.55, this value is less than
0.26 so the distribution is Leptokurtic. The minimum score obtained is 17 and maximum
score obtained is 36. The percentage of mean value is 76.44% so most of the parents have
high level of awareness regarding the importance of Early Intervention.
Table 4.3 shows that the mean score is 27.52 that points to high level
of awareness of parents regarding the importance of early intervention. The median is 28 that
mean the 50% of the parents have a score above 28 and remaining 50% have the score below
28. The mode is 28 that mean 28 are the most repeated scores in this distribution. The
standard deviation of the awareness scores of parents is 4.19 which show that the scores are
not closely packed and there is reasonable scatter among the awareness scores. The range of
the score is 19. The skewness is -0.26 this negative skewness shows that the scores are
massed at the right end. The kurtosis of the awareness scores is -0.55, this value is less than
0.26 so the distribution is Leptokurtic. The minimum score obtained is 17 and maximum
score obtained is 36. The percentage of mean value is 76.44% so most of the parents have
high level of awareness regarding the importance of Early Intervention.
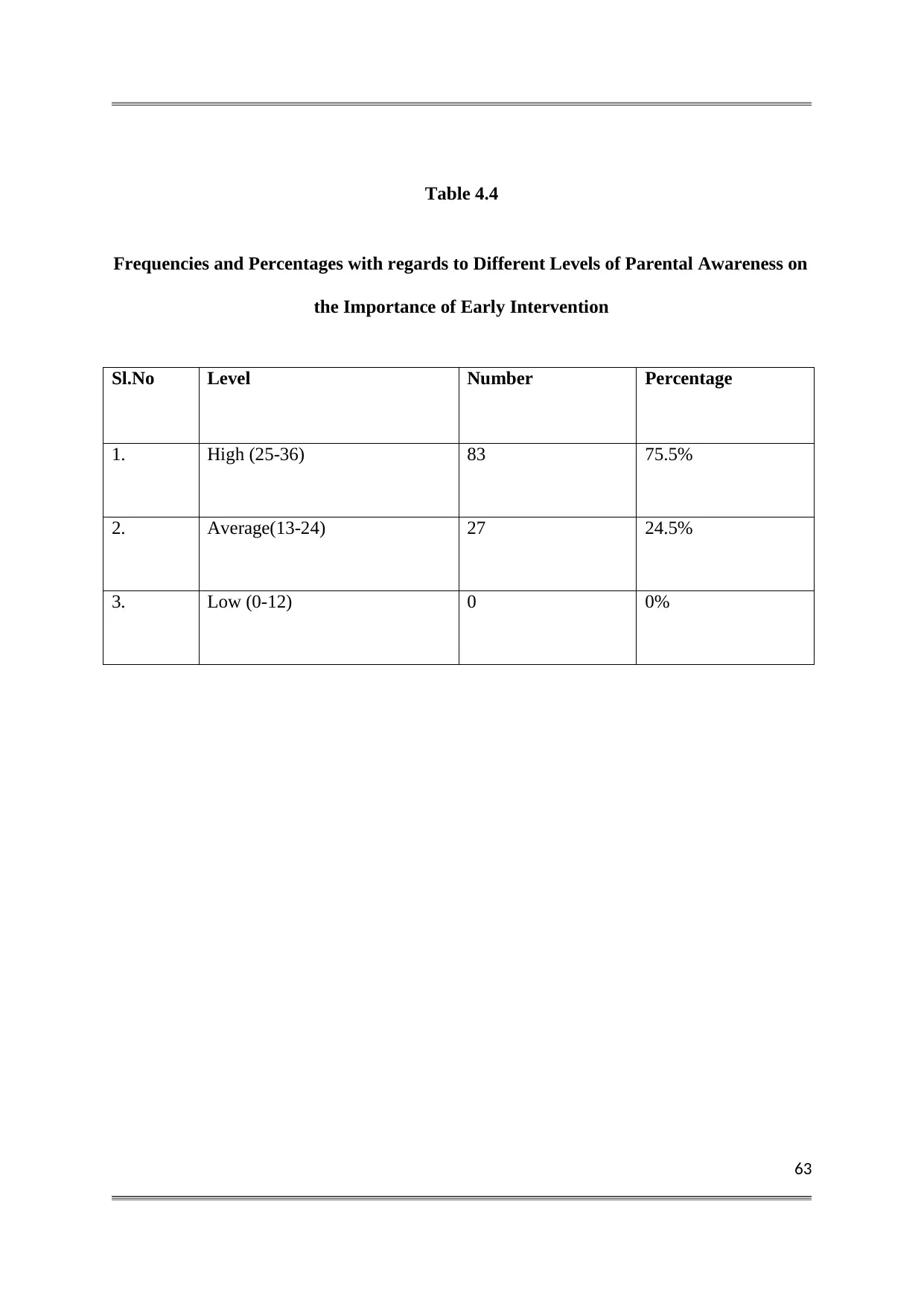
63
Table 4.4
Frequencies and Percentages with regards to Different Levels of Parental Awareness on
the Importance of Early Intervention
Sl.No Level Number Percentage
1. High (25-36) 83 75.5%
2. Average(13-24) 27 24.5%
3. Low (0-12) 0 0%
Table 4.4
Frequencies and Percentages with regards to Different Levels of Parental Awareness on
the Importance of Early Intervention
Sl.No Level Number Percentage
1. High (25-36) 83 75.5%
2. Average(13-24) 27 24.5%
3. Low (0-12) 0 0%
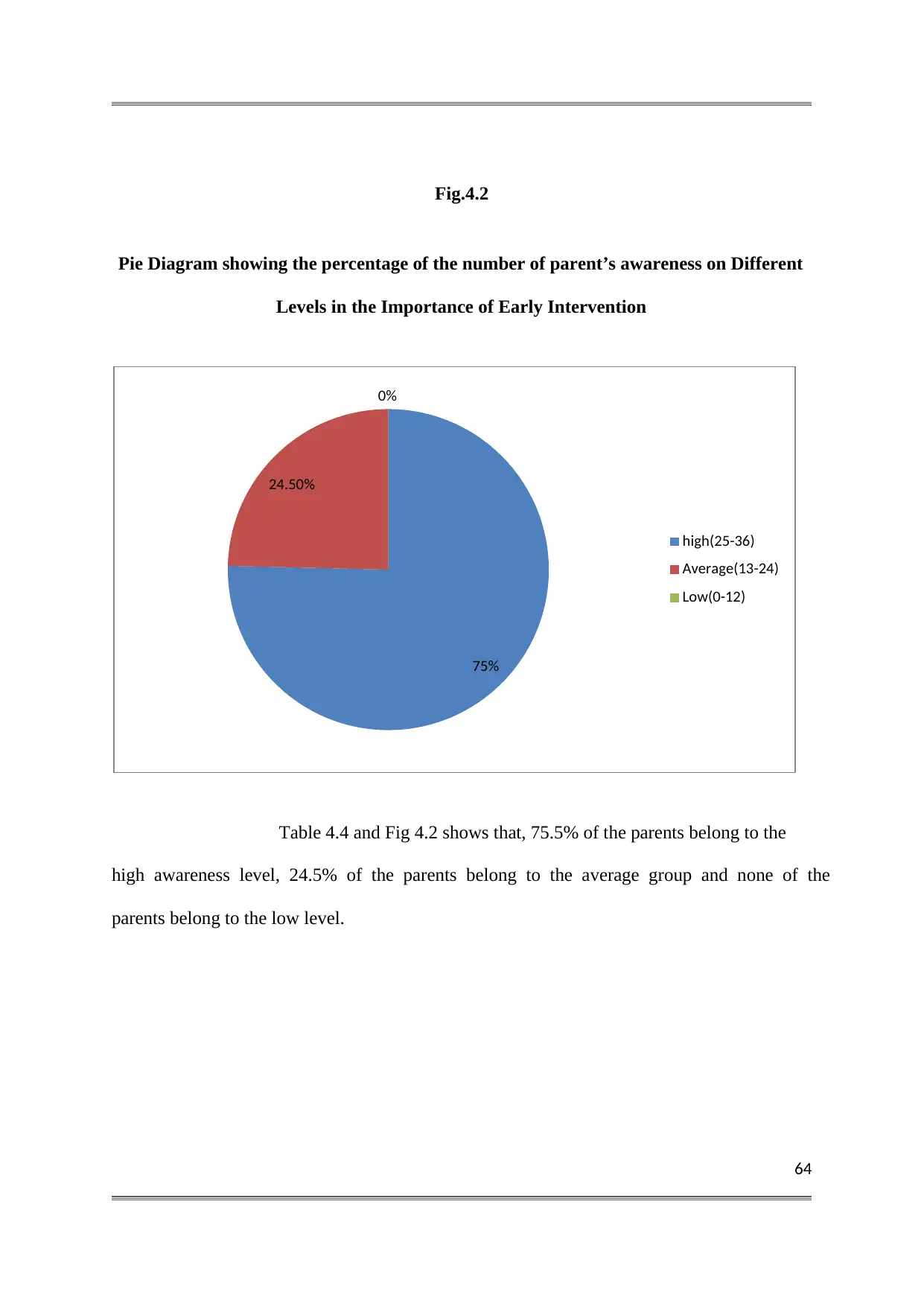
64
Fig.4.2
Pie Diagram showing the percentage of the number of parent’s awareness on Different
Levels in the Importance of Early Intervention
Table 4.4 and Fig 4.2 shows that, 75.5% of the parents belong to the
high awareness level, 24.5% of the parents belong to the average group and none of the
parents belong to the low level.
75%
24.50%
0%
high(25-36)
Average(13-24)
Low(0-12)
Fig.4.2
Pie Diagram showing the percentage of the number of parent’s awareness on Different
Levels in the Importance of Early Intervention
Table 4.4 and Fig 4.2 shows that, 75.5% of the parents belong to the
high awareness level, 24.5% of the parents belong to the average group and none of the
parents belong to the low level.
75%
24.50%
0%
high(25-36)
Average(13-24)
Low(0-12)
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
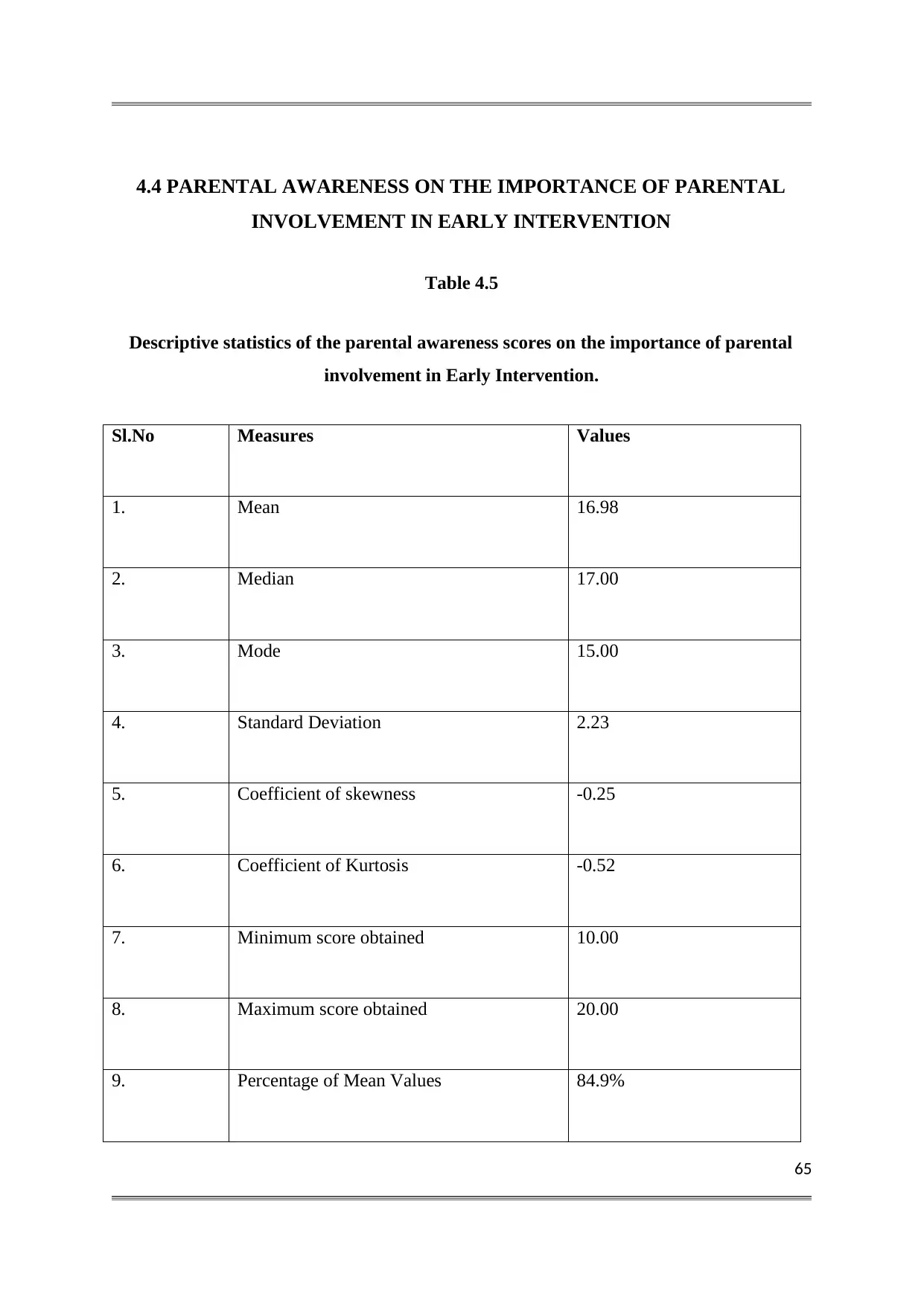
65
4.4 PARENTAL AWARENESS ON THE IMPORTANCE OF PARENTAL
INVOLVEMENT IN EARLY INTERVENTION
Table 4.5
Descriptive statistics of the parental awareness scores on the importance of parental
involvement in Early Intervention.
Sl.No Measures Values
1. Mean 16.98
2. Median 17.00
3. Mode 15.00
4. Standard Deviation 2.23
5. Coefficient of skewness -0.25
6. Coefficient of Kurtosis -0.52
7. Minimum score obtained 10.00
8. Maximum score obtained 20.00
9. Percentage of Mean Values 84.9%
4.4 PARENTAL AWARENESS ON THE IMPORTANCE OF PARENTAL
INVOLVEMENT IN EARLY INTERVENTION
Table 4.5
Descriptive statistics of the parental awareness scores on the importance of parental
involvement in Early Intervention.
Sl.No Measures Values
1. Mean 16.98
2. Median 17.00
3. Mode 15.00
4. Standard Deviation 2.23
5. Coefficient of skewness -0.25
6. Coefficient of Kurtosis -0.52
7. Minimum score obtained 10.00
8. Maximum score obtained 20.00
9. Percentage of Mean Values 84.9%
66
Table 4.5 shows that the mean score is 16.98 that points to high level
of awareness of parents regarding the importance of parental involvement in early
intervention. The median is 17, which mean the 50% of the parents have a score above 17
and remaining 50% have the score below 17. As per the table 4.5, mode is 15, which means
15 is the most repeated score in this distribution. The standard deviation of the awareness
scores of parents is 2.23 which show that the scores are not closely packed and that there is
reasonable scatter among the awareness scores. The range of the score is 67. The skewness is
-0.25, this negative skewness shows that the scores are massed at right end. The kurtosis of
the awareness scores is -0.52, this value is lesser than 0.263 so the distribution is leptokurtic.
The minimum score obtained 10 and the maximum score obtained is 20. The percentage of
the mean value is 84.9% so the most of the parents have high level of awareness regarding
the importance of parental involvement in early intervention.
Table 4.5 shows that the mean score is 16.98 that points to high level
of awareness of parents regarding the importance of parental involvement in early
intervention. The median is 17, which mean the 50% of the parents have a score above 17
and remaining 50% have the score below 17. As per the table 4.5, mode is 15, which means
15 is the most repeated score in this distribution. The standard deviation of the awareness
scores of parents is 2.23 which show that the scores are not closely packed and that there is
reasonable scatter among the awareness scores. The range of the score is 67. The skewness is
-0.25, this negative skewness shows that the scores are massed at right end. The kurtosis of
the awareness scores is -0.52, this value is lesser than 0.263 so the distribution is leptokurtic.
The minimum score obtained 10 and the maximum score obtained is 20. The percentage of
the mean value is 84.9% so the most of the parents have high level of awareness regarding
the importance of parental involvement in early intervention.
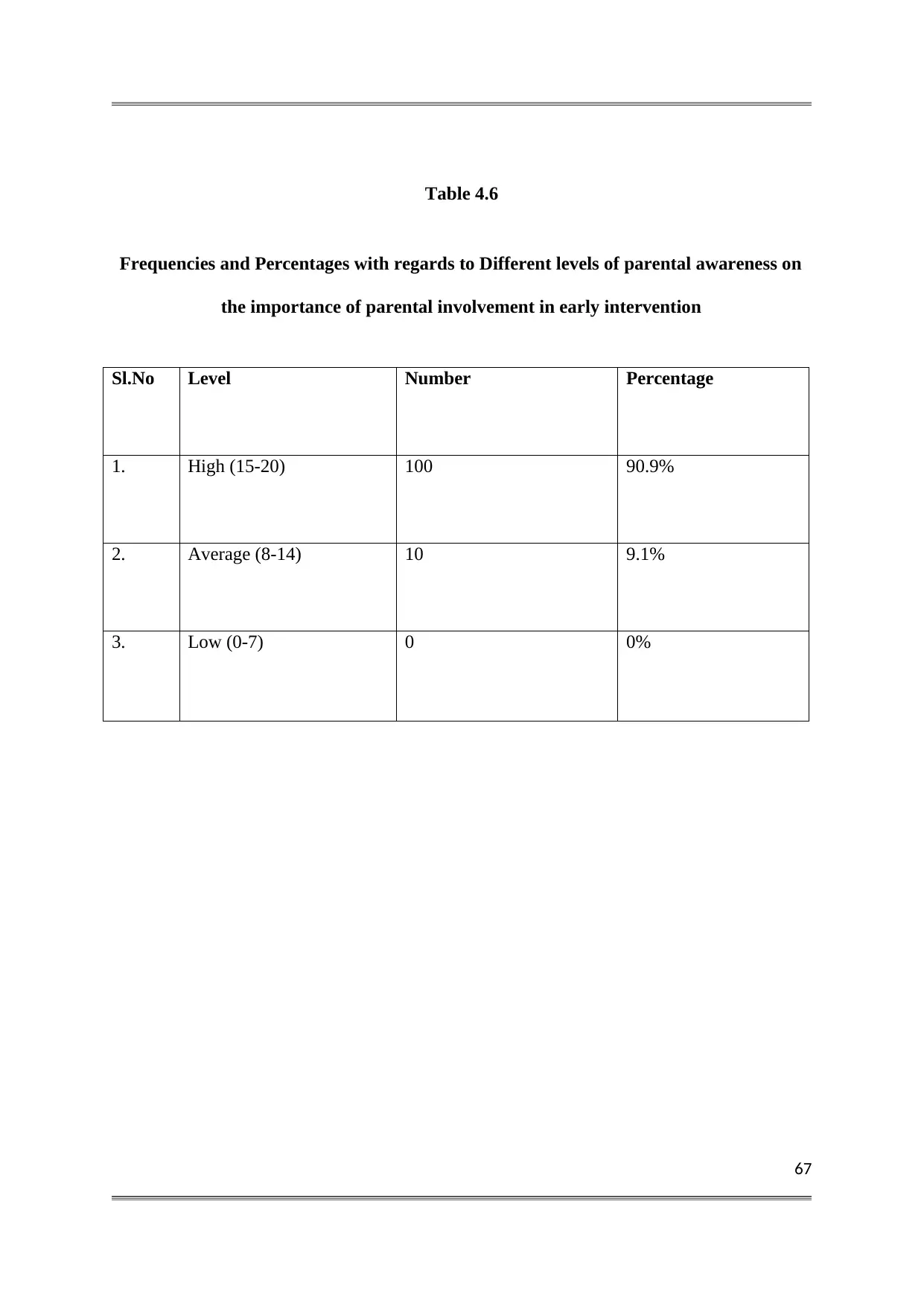
67
Table 4.6
Frequencies and Percentages with regards to Different levels of parental awareness on
the importance of parental involvement in early intervention
Sl.No Level Number Percentage
1. High (15-20) 100 90.9%
2. Average (8-14) 10 9.1%
3. Low (0-7) 0 0%
Table 4.6
Frequencies and Percentages with regards to Different levels of parental awareness on
the importance of parental involvement in early intervention
Sl.No Level Number Percentage
1. High (15-20) 100 90.9%
2. Average (8-14) 10 9.1%
3. Low (0-7) 0 0%
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
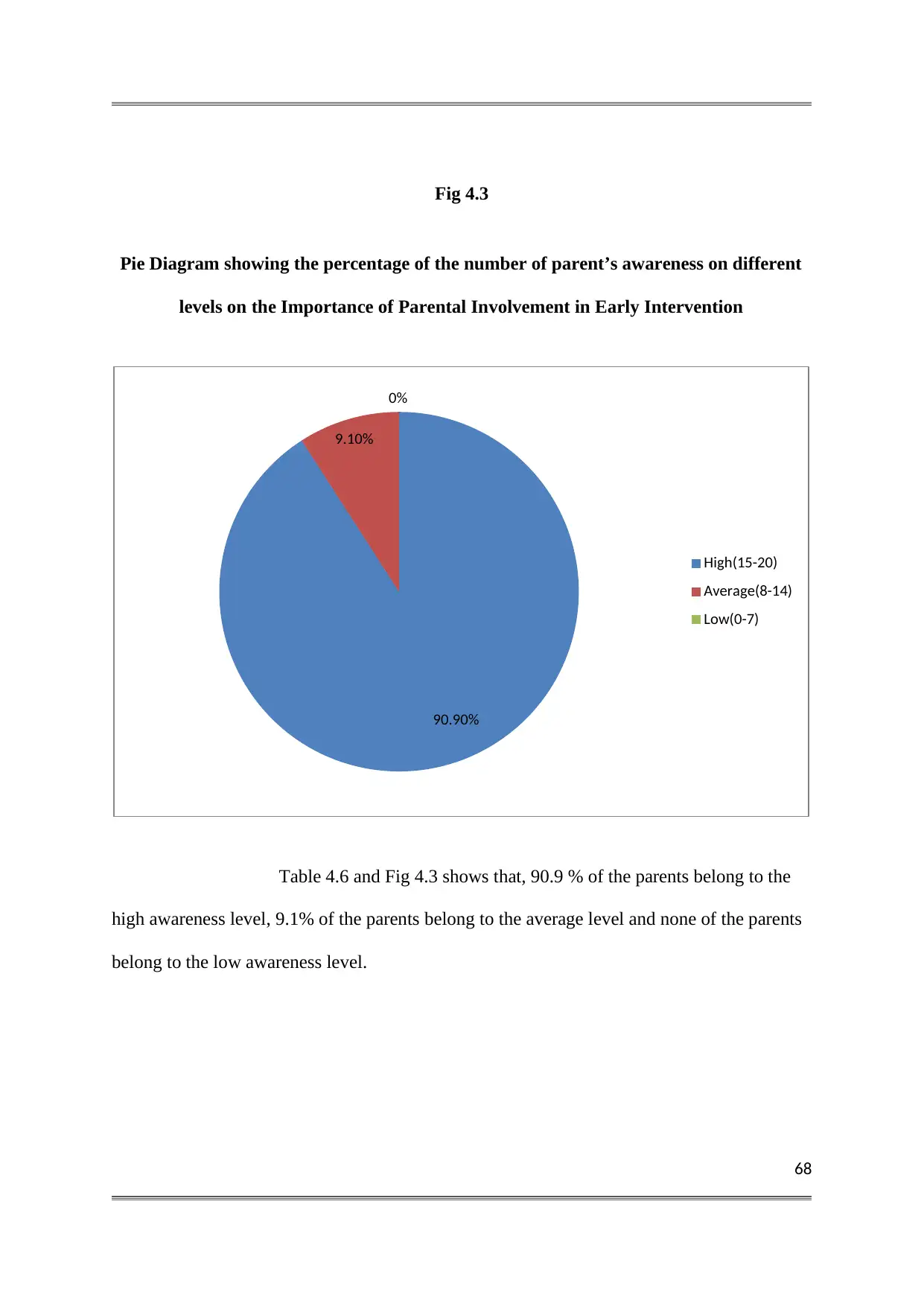
68
Fig 4.3
Pie Diagram showing the percentage of the number of parent’s awareness on different
levels on the Importance of Parental Involvement in Early Intervention
Table 4.6 and Fig 4.3 shows that, 90.9 % of the parents belong to the
high awareness level, 9.1% of the parents belong to the average level and none of the parents
belong to the low awareness level.
90.90%
9.10%
0%
High(15-20)
Average(8-14)
Low(0-7)
Fig 4.3
Pie Diagram showing the percentage of the number of parent’s awareness on different
levels on the Importance of Parental Involvement in Early Intervention
Table 4.6 and Fig 4.3 shows that, 90.9 % of the parents belong to the
high awareness level, 9.1% of the parents belong to the average level and none of the parents
belong to the low awareness level.
90.90%
9.10%
0%
High(15-20)
Average(8-14)
Low(0-7)
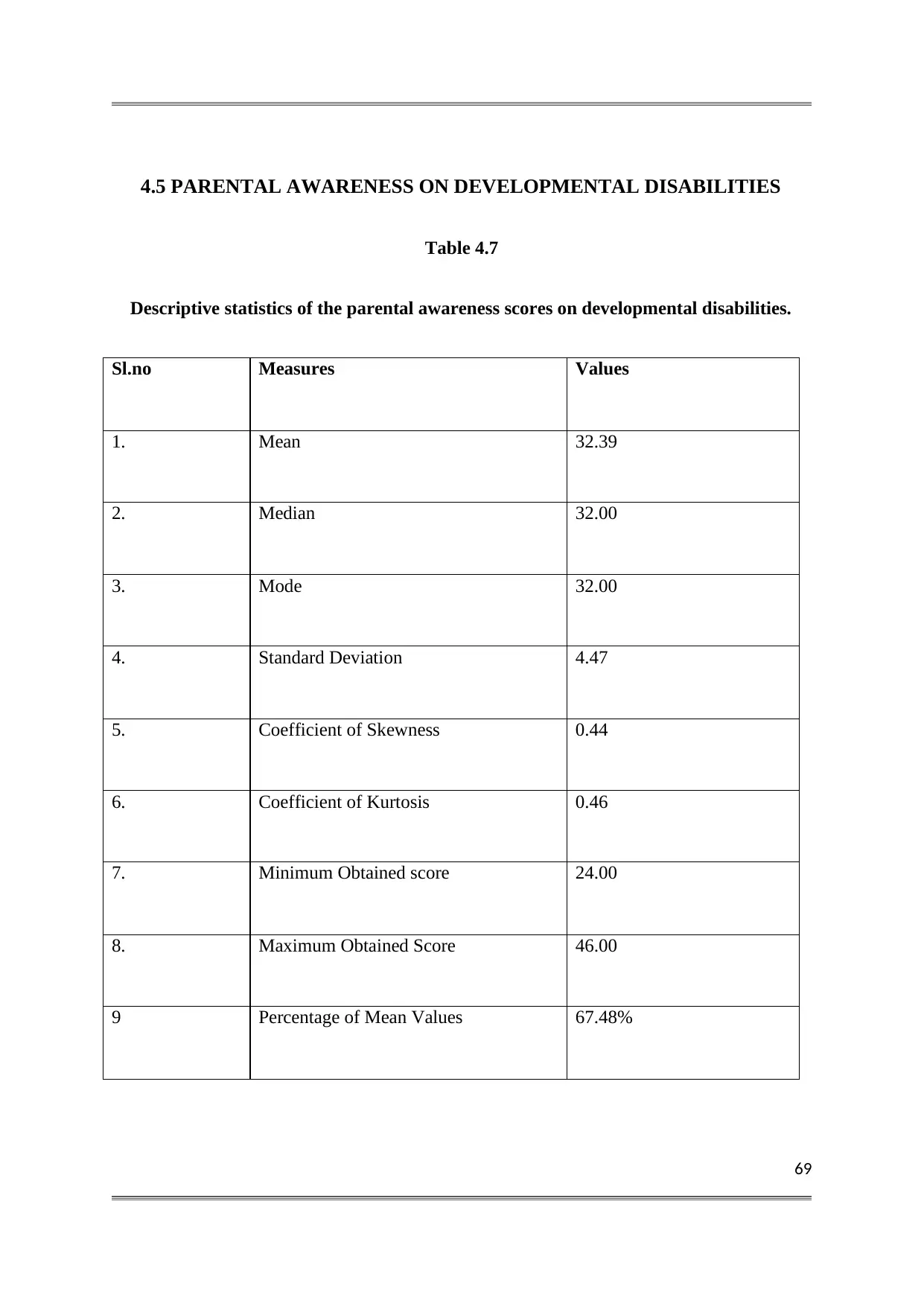
69
4.5 PARENTAL AWARENESS ON DEVELOPMENTAL DISABILITIES
Table 4.7
Descriptive statistics of the parental awareness scores on developmental disabilities.
Sl.no Measures Values
1. Mean 32.39
2. Median 32.00
3. Mode 32.00
4. Standard Deviation 4.47
5. Coefficient of Skewness 0.44
6. Coefficient of Kurtosis 0.46
7. Minimum Obtained score 24.00
8. Maximum Obtained Score 46.00
9 Percentage of Mean Values 67.48%
4.5 PARENTAL AWARENESS ON DEVELOPMENTAL DISABILITIES
Table 4.7
Descriptive statistics of the parental awareness scores on developmental disabilities.
Sl.no Measures Values
1. Mean 32.39
2. Median 32.00
3. Mode 32.00
4. Standard Deviation 4.47
5. Coefficient of Skewness 0.44
6. Coefficient of Kurtosis 0.46
7. Minimum Obtained score 24.00
8. Maximum Obtained Score 46.00
9 Percentage of Mean Values 67.48%
70
Table 4.7 shows that the mean score is 32.39 that points to average
level of awareness of parents regarding developmental disabilities. The median is 32, which
means that 50% of the parents have a score above 32 and remaining 50% have the score
below 32. As per the Table 4.7 mode is 32, which means 32 is the most repeated scores in
this distribution. The standard deviation of the awareness scores of parents is 4.47 which
shows that the scores are not closely packed and that there is reasonable scatter among the
awareness scores. The range of the score is 22. The coefficient of skewness is 0.44 this
positive skewness shows that the scores are massed at the left end. The kurtosis of the
awareness scores is 0.46, this value is greater than 0.263 so the distribution is platykurtic. The
minimum score obtained is 24 and the maximum score obtained is 46. The percentage of
mean value is 67.48% so the most of the parents have a high level of awareness regarding
developmental disabilities.
Table 4.7 shows that the mean score is 32.39 that points to average
level of awareness of parents regarding developmental disabilities. The median is 32, which
means that 50% of the parents have a score above 32 and remaining 50% have the score
below 32. As per the Table 4.7 mode is 32, which means 32 is the most repeated scores in
this distribution. The standard deviation of the awareness scores of parents is 4.47 which
shows that the scores are not closely packed and that there is reasonable scatter among the
awareness scores. The range of the score is 22. The coefficient of skewness is 0.44 this
positive skewness shows that the scores are massed at the left end. The kurtosis of the
awareness scores is 0.46, this value is greater than 0.263 so the distribution is platykurtic. The
minimum score obtained is 24 and the maximum score obtained is 46. The percentage of
mean value is 67.48% so the most of the parents have a high level of awareness regarding
developmental disabilities.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
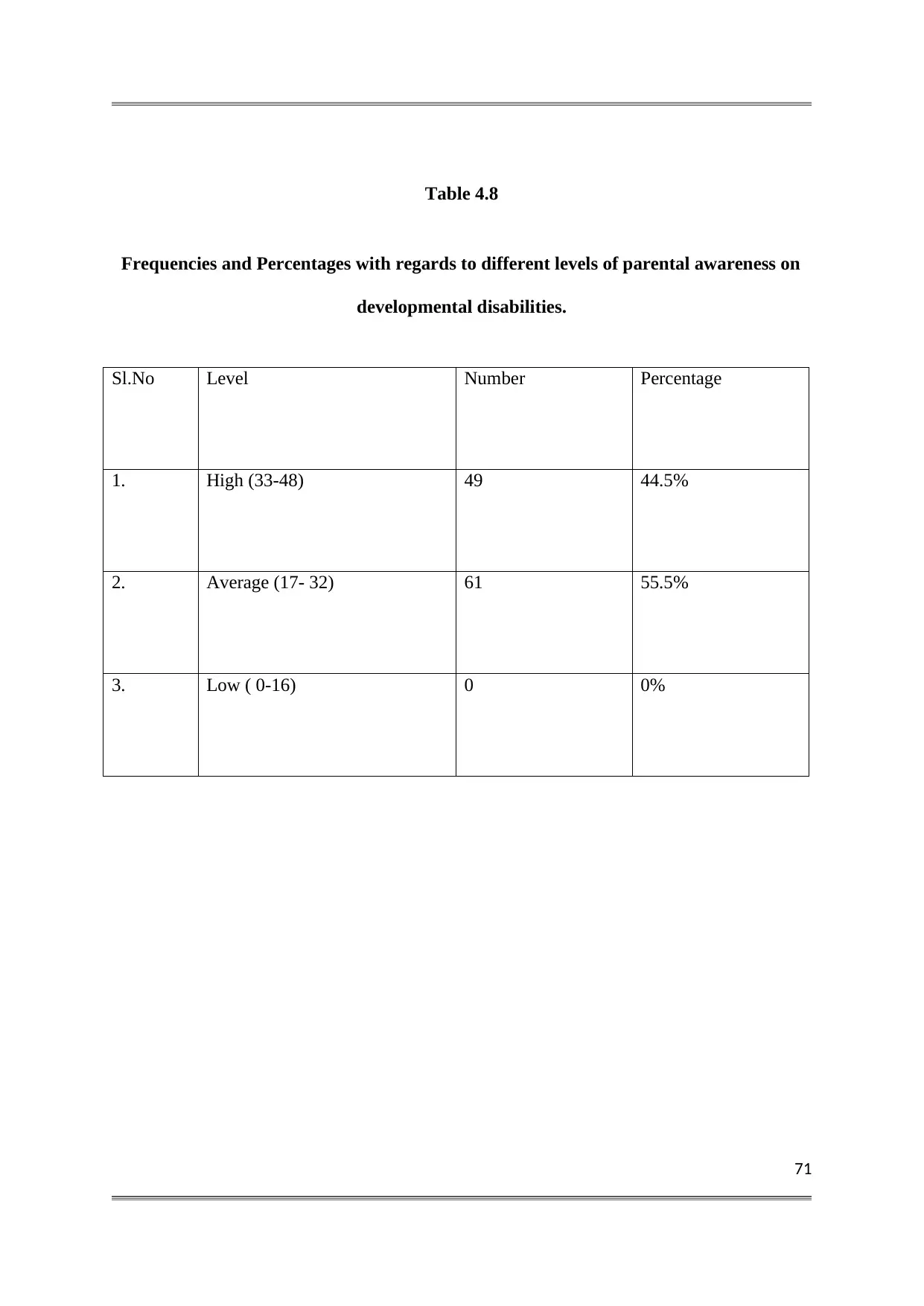
71
Table 4.8
Frequencies and Percentages with regards to different levels of parental awareness on
developmental disabilities.
Sl.No Level Number Percentage
1. High (33-48) 49 44.5%
2. Average (17- 32) 61 55.5%
3. Low ( 0-16) 0 0%
Table 4.8
Frequencies and Percentages with regards to different levels of parental awareness on
developmental disabilities.
Sl.No Level Number Percentage
1. High (33-48) 49 44.5%
2. Average (17- 32) 61 55.5%
3. Low ( 0-16) 0 0%
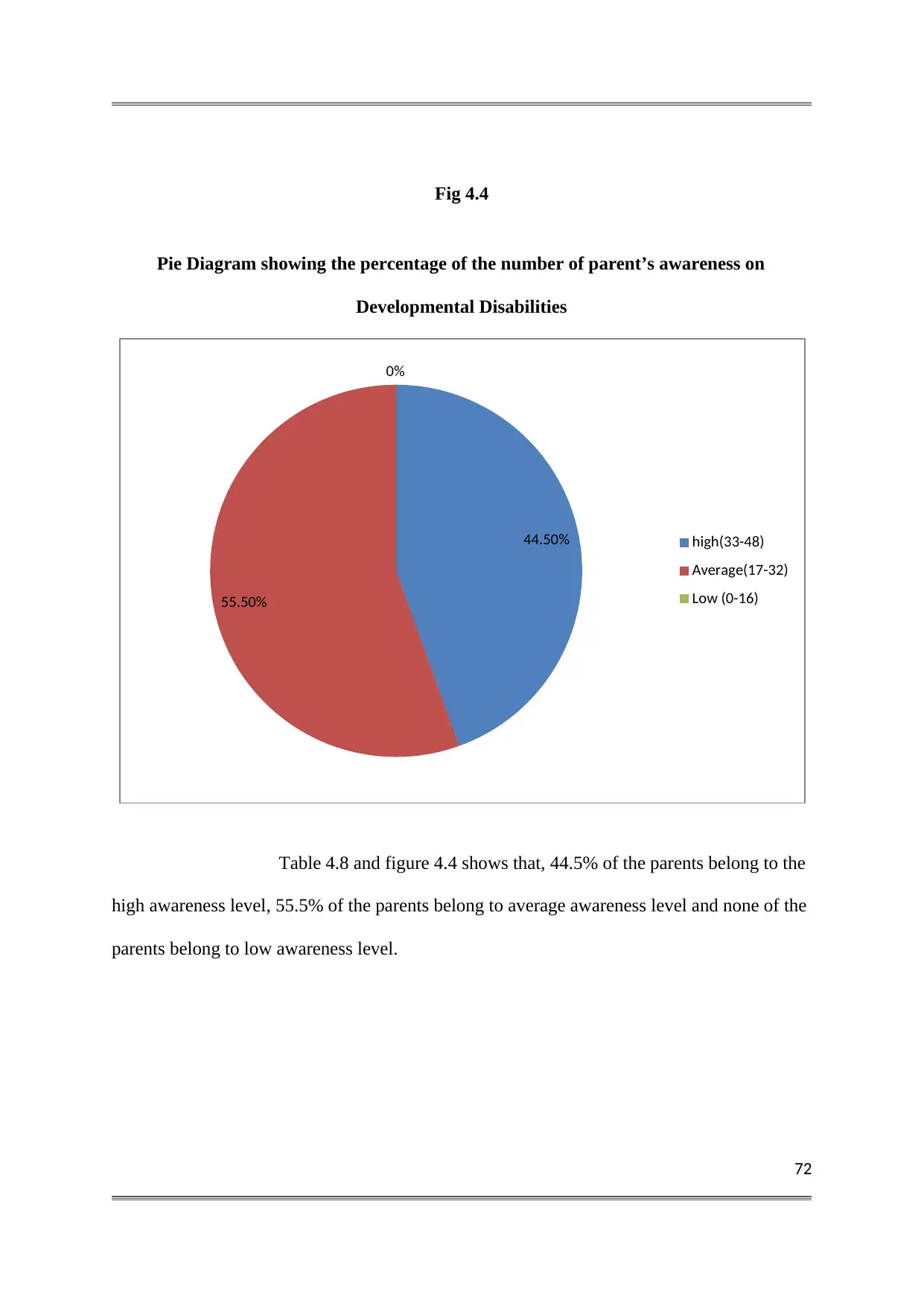
72
Fig 4.4
Pie Diagram showing the percentage of the number of parent’s awareness on
Developmental Disabilities
Table 4.8 and figure 4.4 shows that, 44.5% of the parents belong to the
high awareness level, 55.5% of the parents belong to average awareness level and none of the
parents belong to low awareness level.
44.50%
55.50%
0%
high(33-48)
Average(17-32)
Low (0-16)
Fig 4.4
Pie Diagram showing the percentage of the number of parent’s awareness on
Developmental Disabilities
Table 4.8 and figure 4.4 shows that, 44.5% of the parents belong to the
high awareness level, 55.5% of the parents belong to average awareness level and none of the
parents belong to low awareness level.
44.50%
55.50%
0%
high(33-48)
Average(17-32)
Low (0-16)
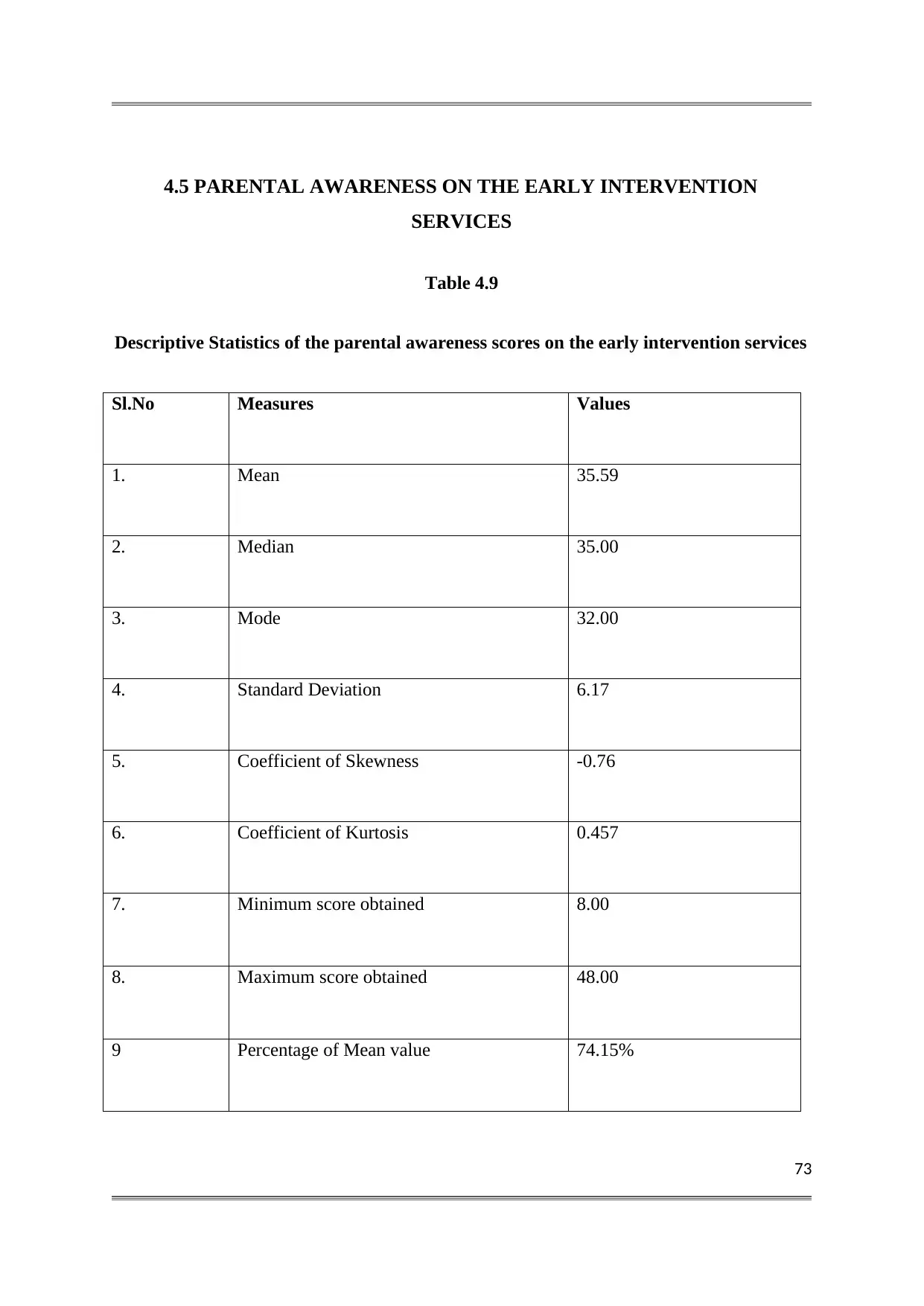
73
4.5 PARENTAL AWARENESS ON THE EARLY INTERVENTION
SERVICES
Table 4.9
Descriptive Statistics of the parental awareness scores on the early intervention services
Sl.No Measures Values
1. Mean 35.59
2. Median 35.00
3. Mode 32.00
4. Standard Deviation 6.17
5. Coefficient of Skewness -0.76
6. Coefficient of Kurtosis 0.457
7. Minimum score obtained 8.00
8. Maximum score obtained 48.00
9 Percentage of Mean value 74.15%
4.5 PARENTAL AWARENESS ON THE EARLY INTERVENTION
SERVICES
Table 4.9
Descriptive Statistics of the parental awareness scores on the early intervention services
Sl.No Measures Values
1. Mean 35.59
2. Median 35.00
3. Mode 32.00
4. Standard Deviation 6.17
5. Coefficient of Skewness -0.76
6. Coefficient of Kurtosis 0.457
7. Minimum score obtained 8.00
8. Maximum score obtained 48.00
9 Percentage of Mean value 74.15%
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
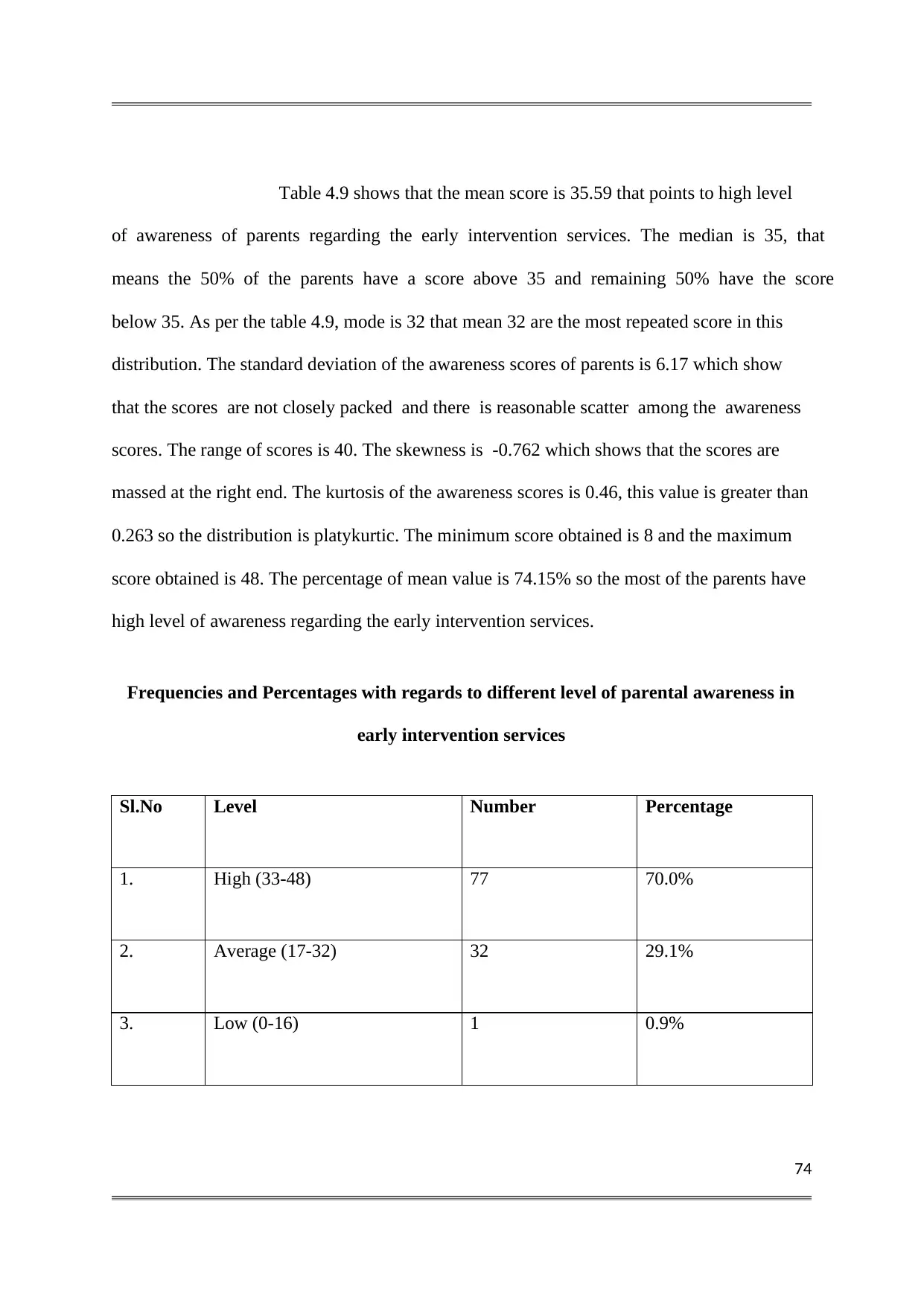
74
Table 4.9 shows that the mean score is 35.59 that points to high level
of awareness of parents regarding the early intervention services. The median is 35, that
means the 50% of the parents have a score above 35 and remaining 50% have the score
below 35. As per the table 4.9, mode is 32 that mean 32 are the most repeated score in this
distribution. The standard deviation of the awareness scores of parents is 6.17 which show
that the scores are not closely packed and there is reasonable scatter among the awareness
scores. The range of scores is 40. The skewness is -0.762 which shows that the scores are
massed at the right end. The kurtosis of the awareness scores is 0.46, this value is greater than
0.263 so the distribution is platykurtic. The minimum score obtained is 8 and the maximum
score obtained is 48. The percentage of mean value is 74.15% so the most of the parents have
high level of awareness regarding the early intervention services.
Frequencies and Percentages with regards to different level of parental awareness in
early intervention services
Sl.No Level Number Percentage
1. High (33-48) 77 70.0%
2. Average (17-32) 32 29.1%
3. Low (0-16) 1 0.9%
Table 4.9 shows that the mean score is 35.59 that points to high level
of awareness of parents regarding the early intervention services. The median is 35, that
means the 50% of the parents have a score above 35 and remaining 50% have the score
below 35. As per the table 4.9, mode is 32 that mean 32 are the most repeated score in this
distribution. The standard deviation of the awareness scores of parents is 6.17 which show
that the scores are not closely packed and there is reasonable scatter among the awareness
scores. The range of scores is 40. The skewness is -0.762 which shows that the scores are
massed at the right end. The kurtosis of the awareness scores is 0.46, this value is greater than
0.263 so the distribution is platykurtic. The minimum score obtained is 8 and the maximum
score obtained is 48. The percentage of mean value is 74.15% so the most of the parents have
high level of awareness regarding the early intervention services.
Frequencies and Percentages with regards to different level of parental awareness in
early intervention services
Sl.No Level Number Percentage
1. High (33-48) 77 70.0%
2. Average (17-32) 32 29.1%
3. Low (0-16) 1 0.9%
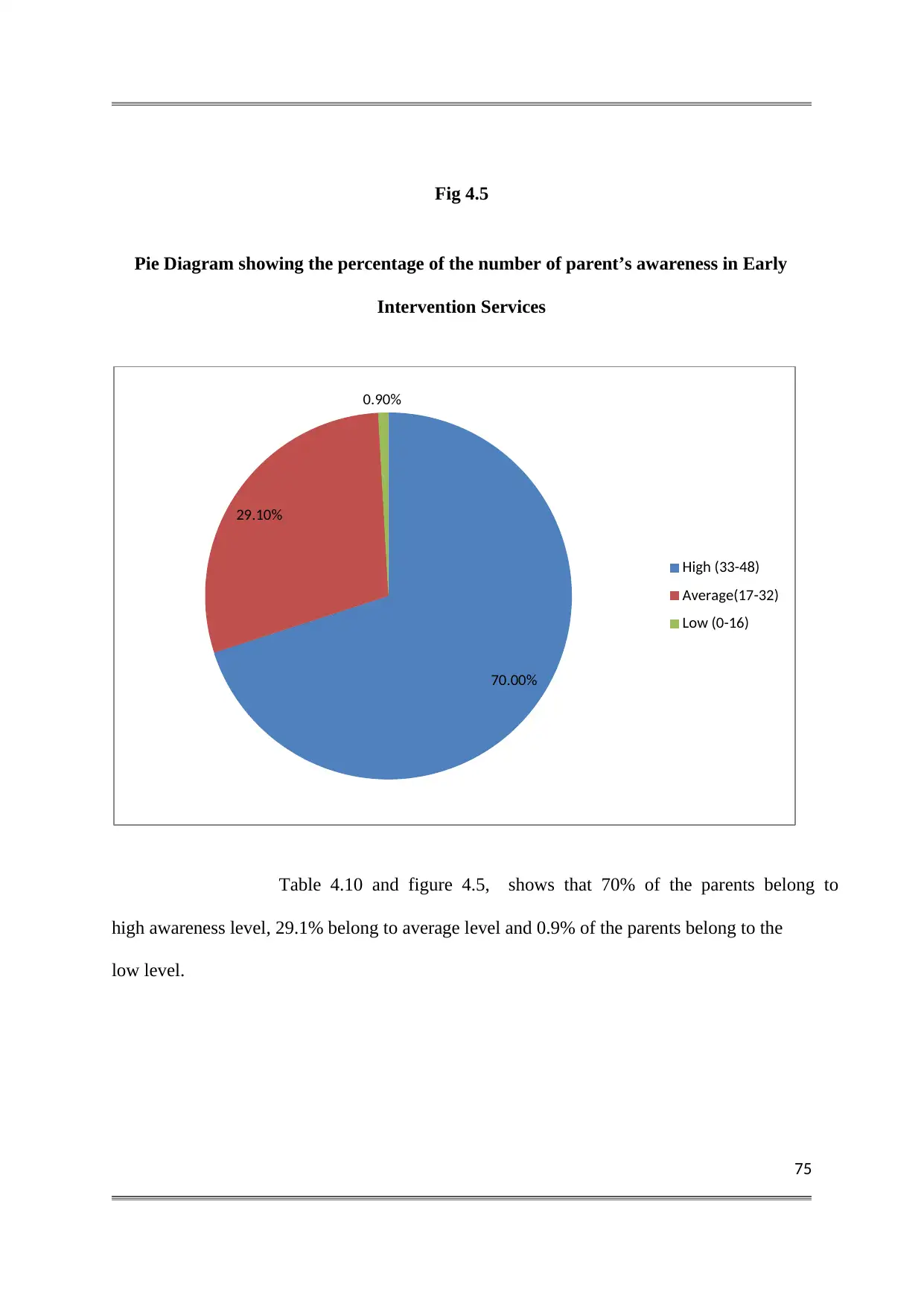
75
Fig 4.5
Pie Diagram showing the percentage of the number of parent’s awareness in Early
Intervention Services
Table 4.10 and figure 4.5, shows that 70% of the parents belong to
high awareness level, 29.1% belong to average level and 0.9% of the parents belong to the
low level.
70.00%
29.10%
0.90%
High (33-48)
Average(17-32)
Low (0-16)
Fig 4.5
Pie Diagram showing the percentage of the number of parent’s awareness in Early
Intervention Services
Table 4.10 and figure 4.5, shows that 70% of the parents belong to
high awareness level, 29.1% belong to average level and 0.9% of the parents belong to the
low level.
70.00%
29.10%
0.90%
High (33-48)
Average(17-32)
Low (0-16)
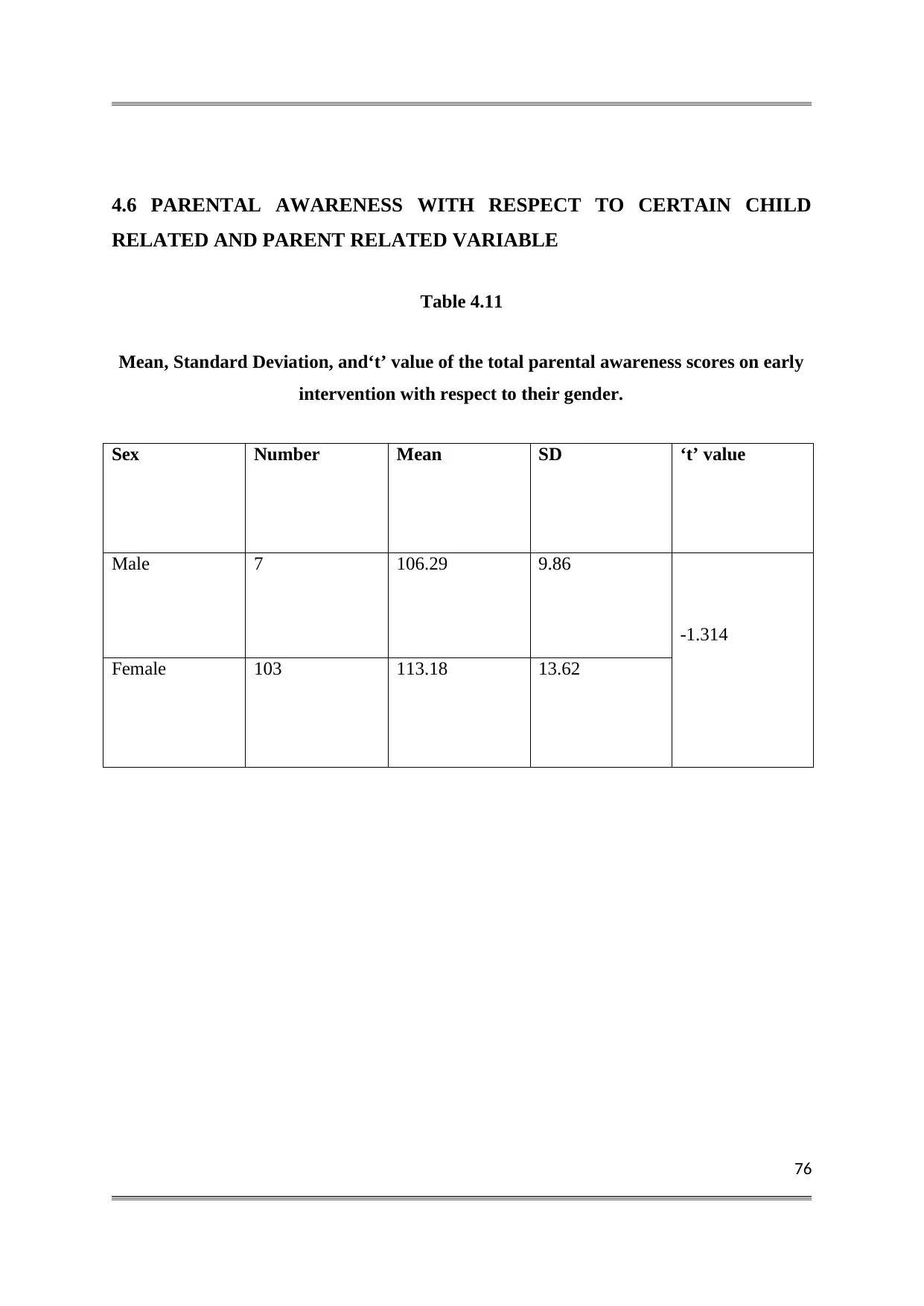
76
4.6 PARENTAL AWARENESS WITH RESPECT TO CERTAIN CHILD
RELATED AND PARENT RELATED VARIABLE
Table 4.11
Mean, Standard Deviation, and‘t’ value of the total parental awareness scores on early
intervention with respect to their gender.
Sex Number Mean SD ‘t’ value
Male 7 106.29 9.86
-1.314
Female 103 113.18 13.62
4.6 PARENTAL AWARENESS WITH RESPECT TO CERTAIN CHILD
RELATED AND PARENT RELATED VARIABLE
Table 4.11
Mean, Standard Deviation, and‘t’ value of the total parental awareness scores on early
intervention with respect to their gender.
Sex Number Mean SD ‘t’ value
Male 7 106.29 9.86
-1.314
Female 103 113.18 13.62
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
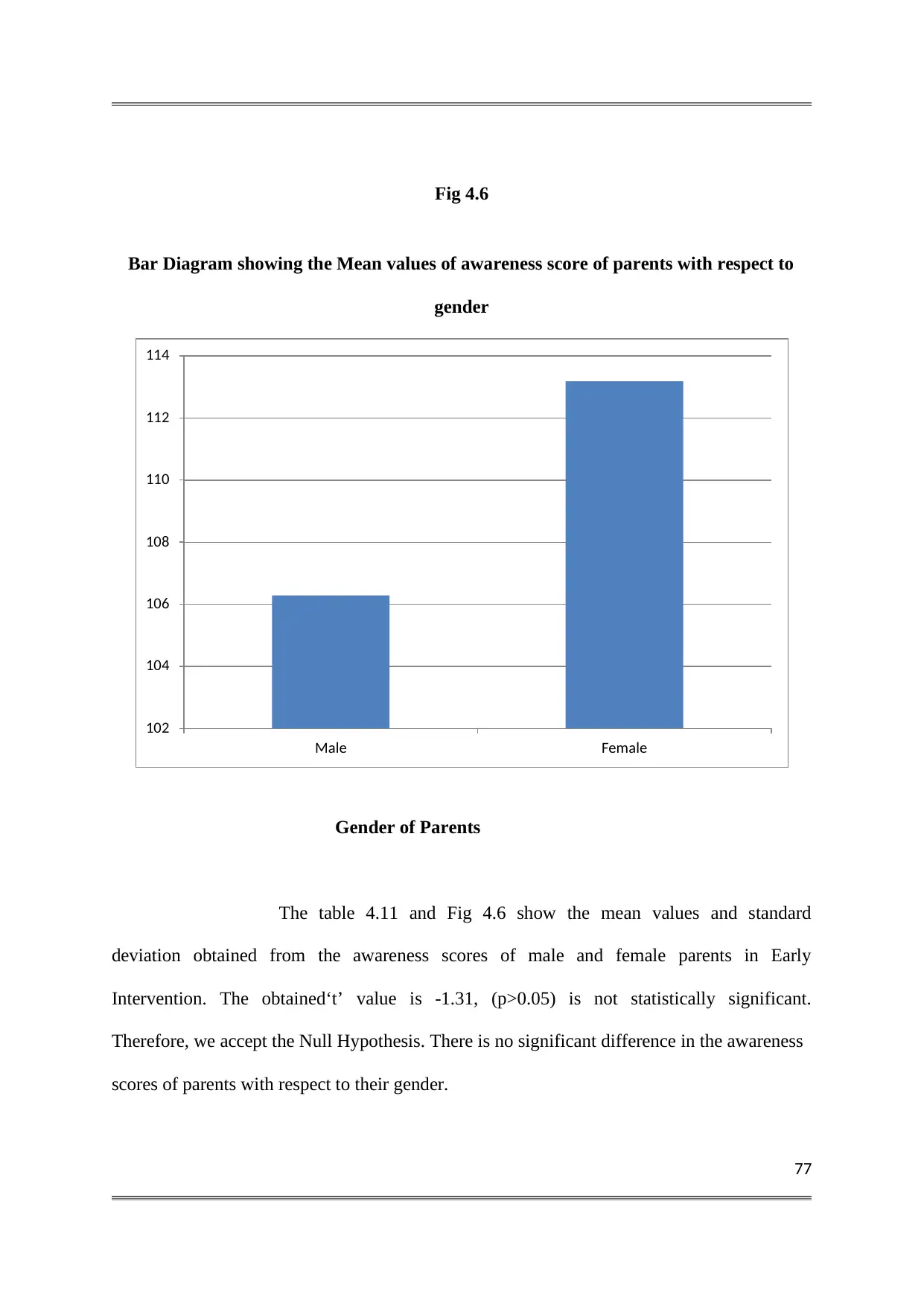
77
Fig 4.6
Bar Diagram showing the Mean values of awareness score of parents with respect to
gender
Gender of Parents
The table 4.11 and Fig 4.6 show the mean values and standard
deviation obtained from the awareness scores of male and female parents in Early
Intervention. The obtained‘t’ value is -1.31, (p>0.05) is not statistically significant.
Therefore, we accept the Null Hypothesis. There is no significant difference in the awareness
scores of parents with respect to their gender.
102
104
106
108
110
112
114
Male Female
Fig 4.6
Bar Diagram showing the Mean values of awareness score of parents with respect to
gender
Gender of Parents
The table 4.11 and Fig 4.6 show the mean values and standard
deviation obtained from the awareness scores of male and female parents in Early
Intervention. The obtained‘t’ value is -1.31, (p>0.05) is not statistically significant.
Therefore, we accept the Null Hypothesis. There is no significant difference in the awareness
scores of parents with respect to their gender.
102
104
106
108
110
112
114
Male Female
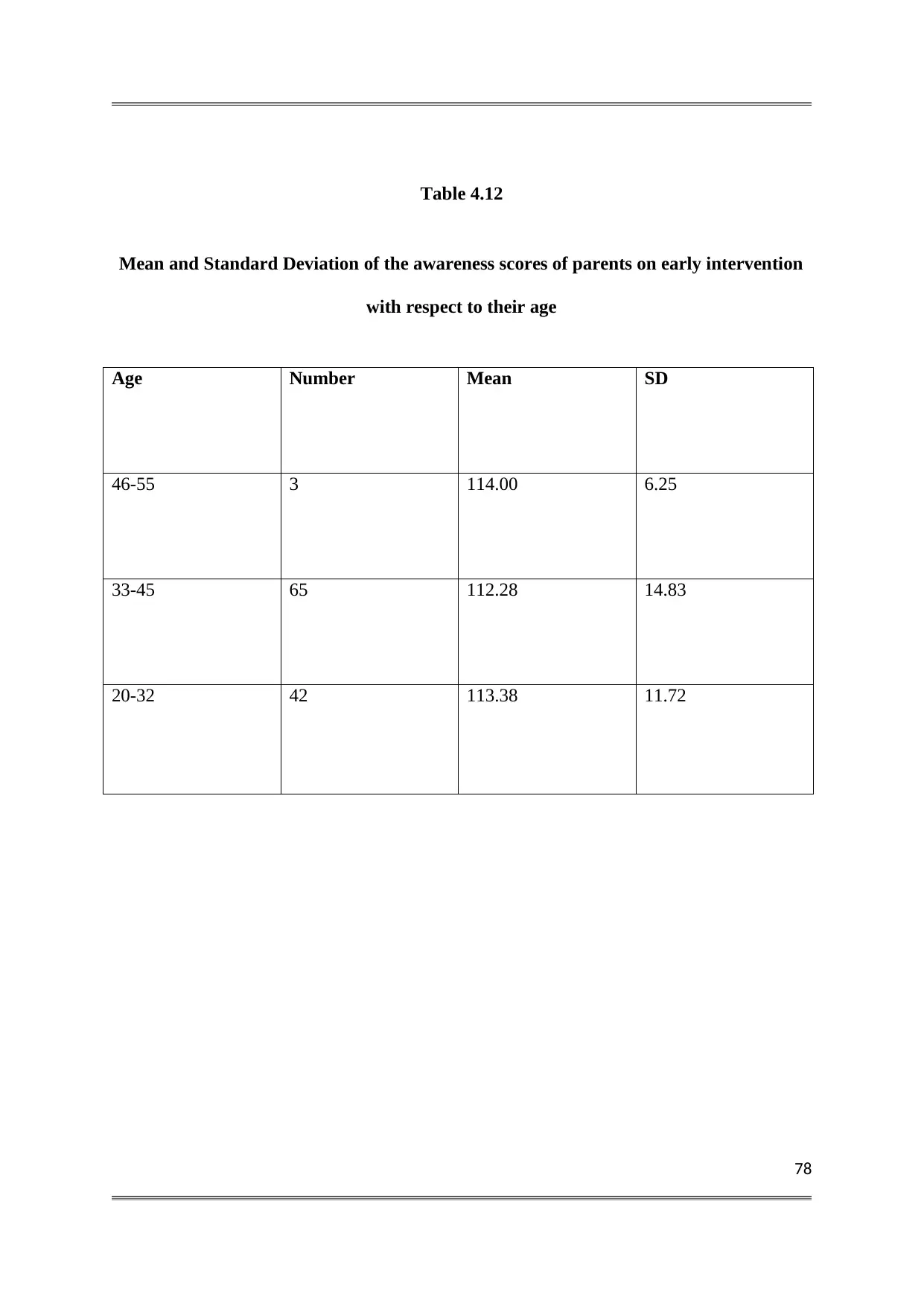
78
Table 4.12
Mean and Standard Deviation of the awareness scores of parents on early intervention
with respect to their age
Age Number Mean SD
46-55 3 114.00 6.25
33-45 65 112.28 14.83
20-32 42 113.38 11.72
Table 4.12
Mean and Standard Deviation of the awareness scores of parents on early intervention
with respect to their age
Age Number Mean SD
46-55 3 114.00 6.25
33-45 65 112.28 14.83
20-32 42 113.38 11.72
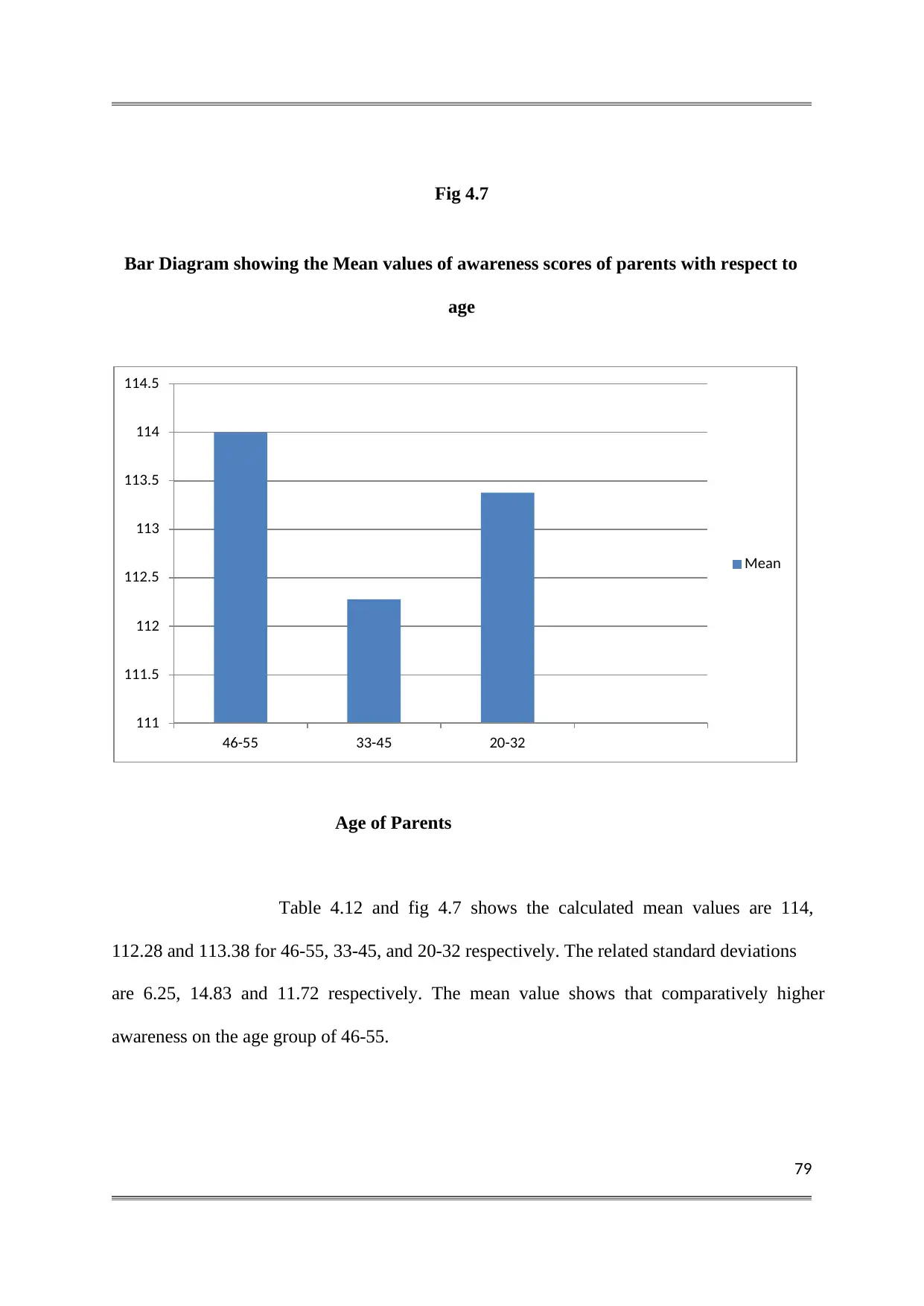
79
Fig 4.7
Bar Diagram showing the Mean values of awareness scores of parents with respect to
age
Age of Parents
Table 4.12 and fig 4.7 shows the calculated mean values are 114,
112.28 and 113.38 for 46-55, 33-45, and 20-32 respectively. The related standard deviations
are 6.25, 14.83 and 11.72 respectively. The mean value shows that comparatively higher
awareness on the age group of 46-55.
111
111.5
112
112.5
113
113.5
114
114.5
46-55 33-45 20-32
Mean
Fig 4.7
Bar Diagram showing the Mean values of awareness scores of parents with respect to
age
Age of Parents
Table 4.12 and fig 4.7 shows the calculated mean values are 114,
112.28 and 113.38 for 46-55, 33-45, and 20-32 respectively. The related standard deviations
are 6.25, 14.83 and 11.72 respectively. The mean value shows that comparatively higher
awareness on the age group of 46-55.
111
111.5
112
112.5
113
113.5
114
114.5
46-55 33-45 20-32
Mean
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
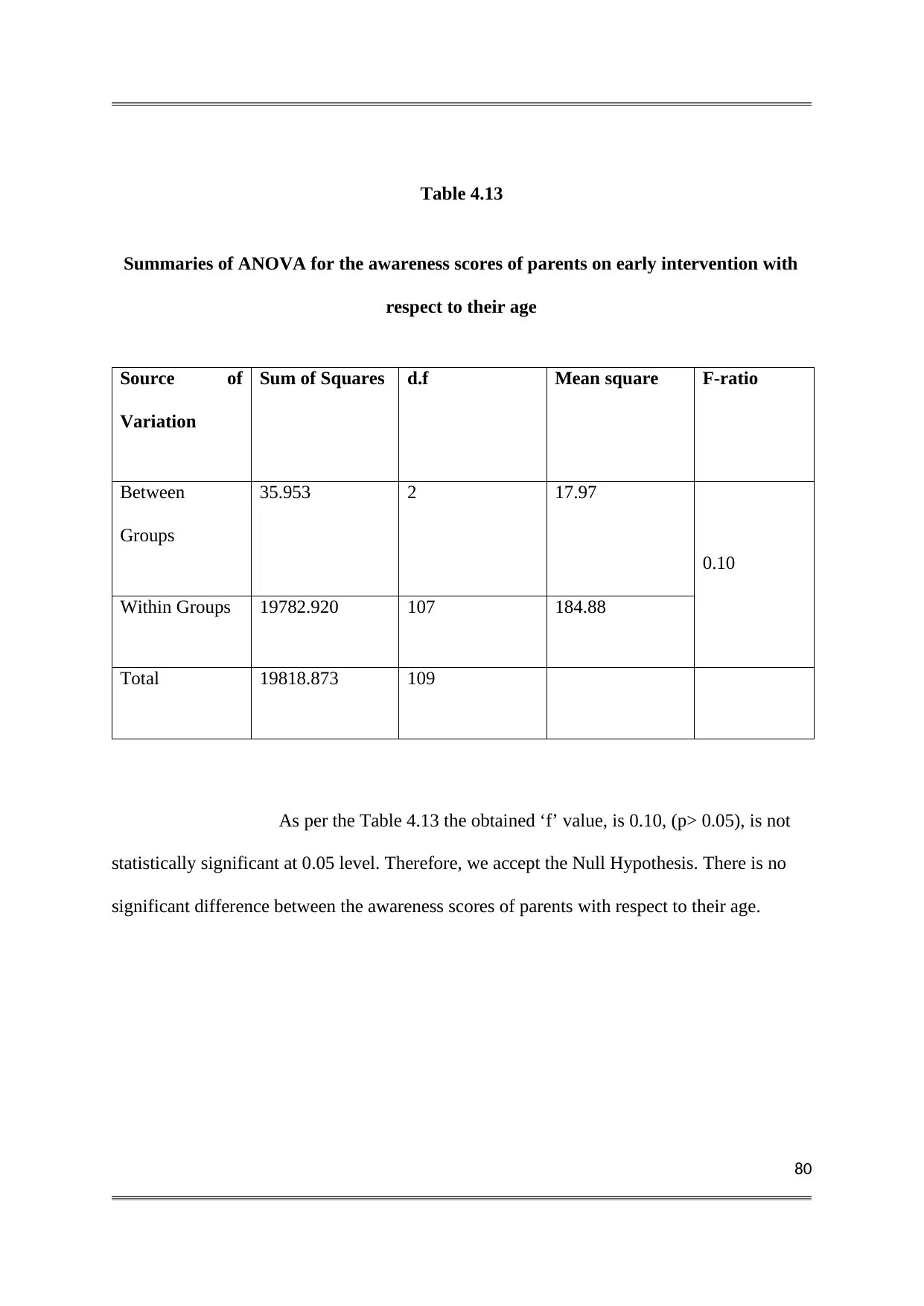
80
Table 4.13
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to their age
Source of
Variation
Sum of Squares d.f Mean square F-ratio
Between
Groups
35.953 2 17.97
0.10
Within Groups 19782.920 107 184.88
Total 19818.873 109
As per the Table 4.13 the obtained ‘f’ value, is 0.10, (p> 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their age.
Table 4.13
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to their age
Source of
Variation
Sum of Squares d.f Mean square F-ratio
Between
Groups
35.953 2 17.97
0.10
Within Groups 19782.920 107 184.88
Total 19818.873 109
As per the Table 4.13 the obtained ‘f’ value, is 0.10, (p> 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their age.
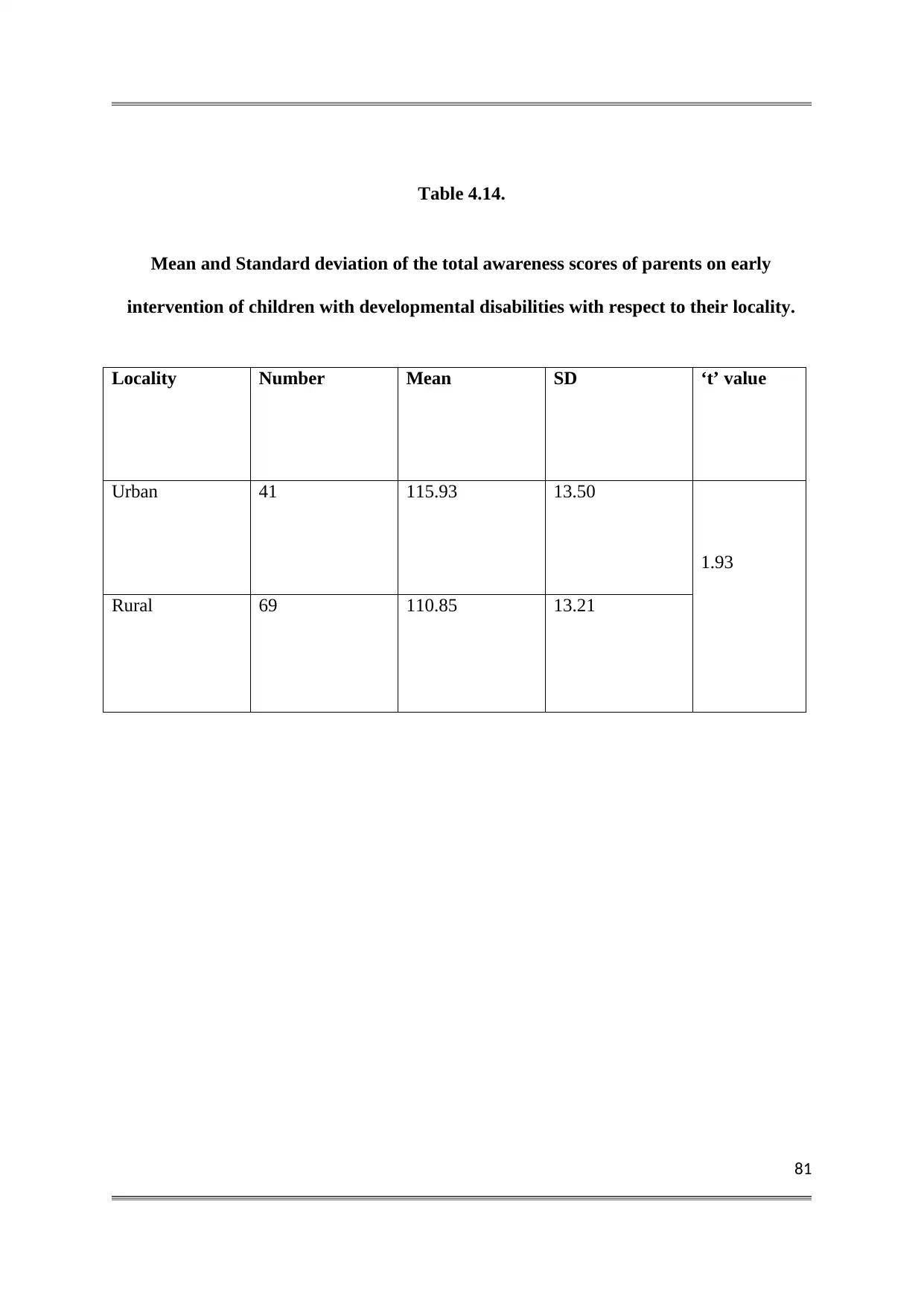
81
Table 4.14.
Mean and Standard deviation of the total awareness scores of parents on early
intervention of children with developmental disabilities with respect to their locality.
Locality Number Mean SD ‘t’ value
Urban 41 115.93 13.50
1.93
Rural 69 110.85 13.21
Table 4.14.
Mean and Standard deviation of the total awareness scores of parents on early
intervention of children with developmental disabilities with respect to their locality.
Locality Number Mean SD ‘t’ value
Urban 41 115.93 13.50
1.93
Rural 69 110.85 13.21
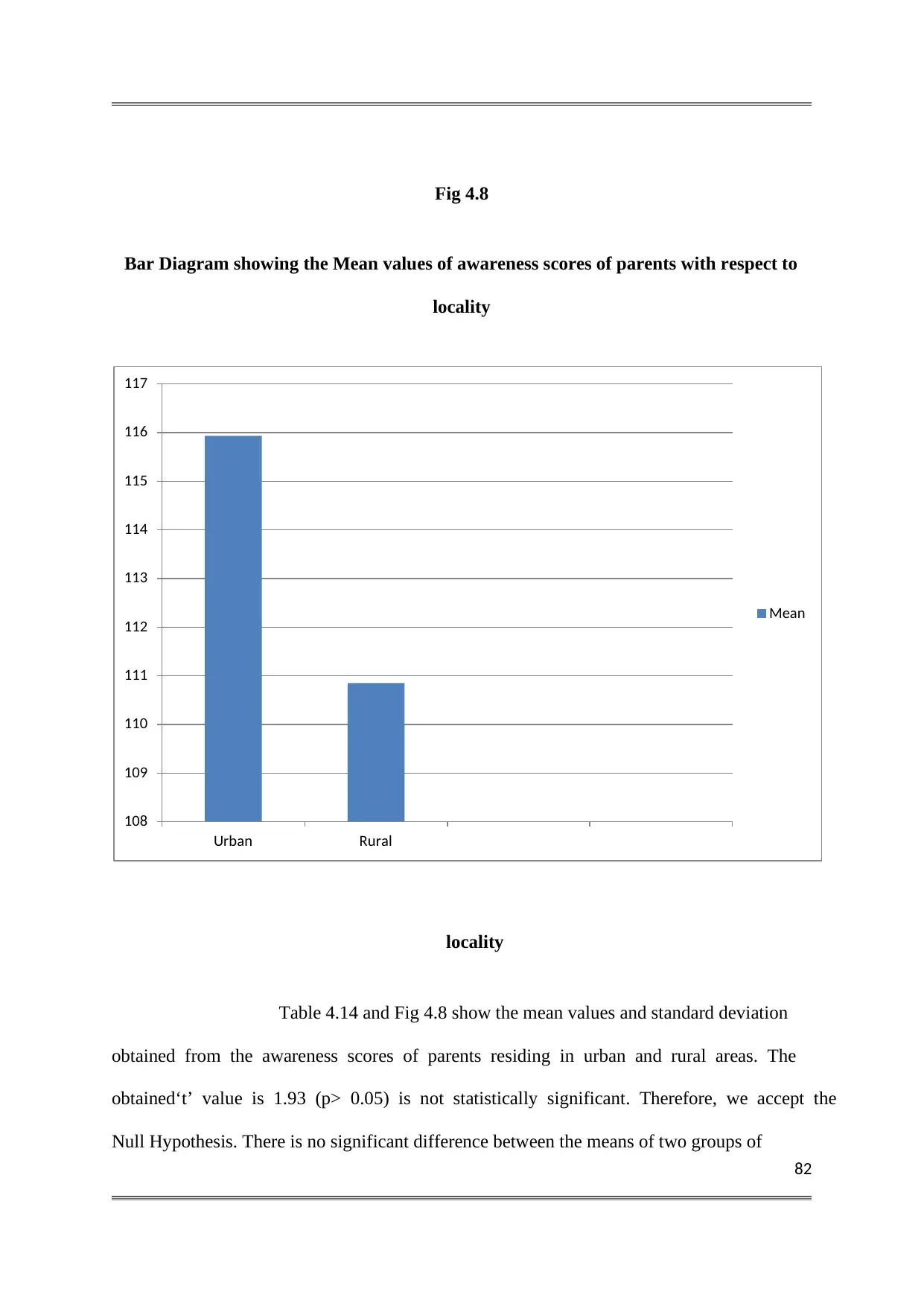
82
Fig 4.8
Bar Diagram showing the Mean values of awareness scores of parents with respect to
locality
locality
Table 4.14 and Fig 4.8 show the mean values and standard deviation
obtained from the awareness scores of parents residing in urban and rural areas. The
obtained‘t’ value is 1.93 (p> 0.05) is not statistically significant. Therefore, we accept the
Null Hypothesis. There is no significant difference between the means of two groups of
108
109
110
111
112
113
114
115
116
117
Urban Rural
Mean
Fig 4.8
Bar Diagram showing the Mean values of awareness scores of parents with respect to
locality
locality
Table 4.14 and Fig 4.8 show the mean values and standard deviation
obtained from the awareness scores of parents residing in urban and rural areas. The
obtained‘t’ value is 1.93 (p> 0.05) is not statistically significant. Therefore, we accept the
Null Hypothesis. There is no significant difference between the means of two groups of
108
109
110
111
112
113
114
115
116
117
Urban Rural
Mean
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
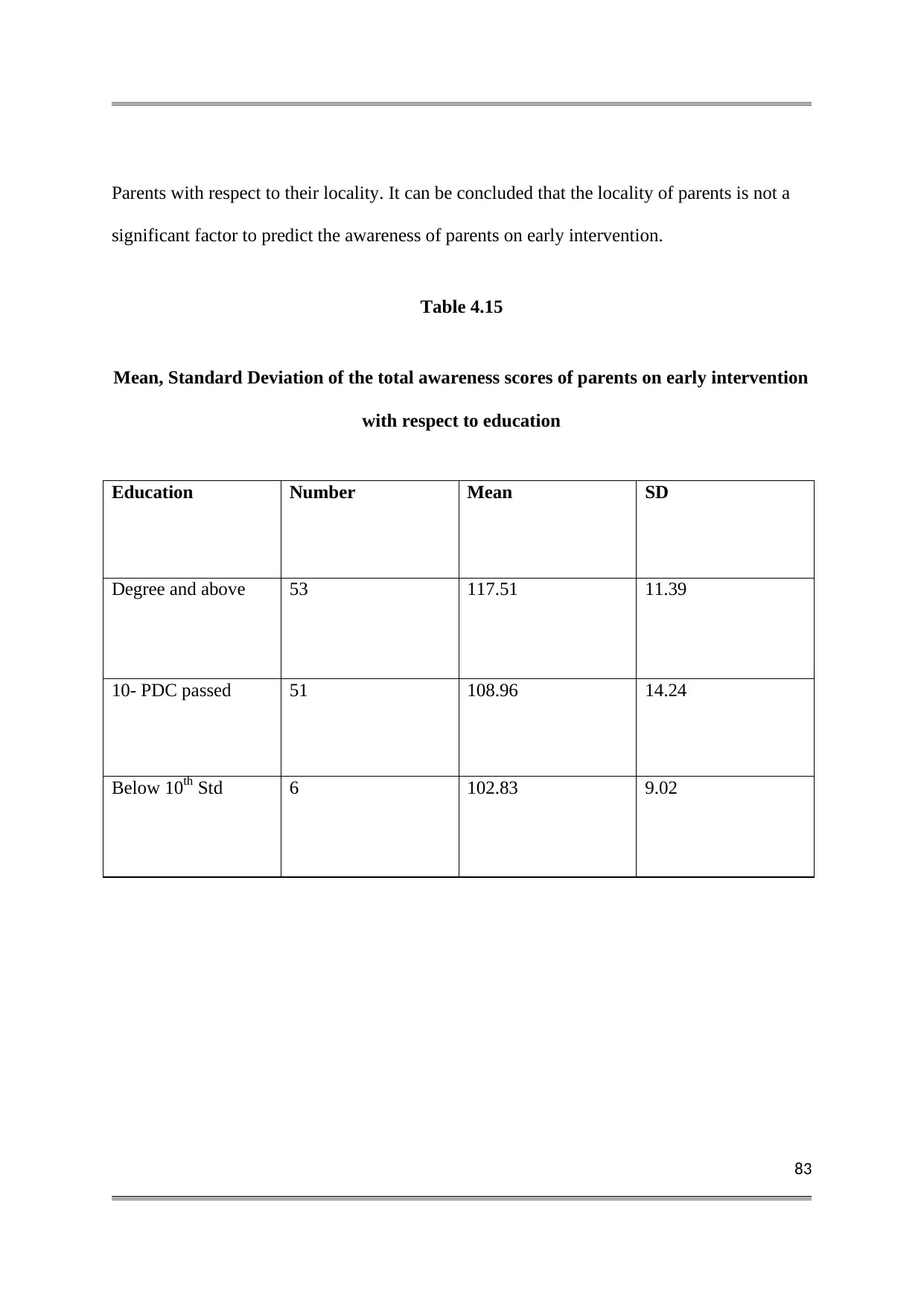
83
Parents with respect to their locality. It can be concluded that the locality of parents is not a
significant factor to predict the awareness of parents on early intervention.
Table 4.15
Mean, Standard Deviation of the total awareness scores of parents on early intervention
with respect to education
Education Number Mean SD
Degree and above 53 117.51 11.39
10- PDC passed 51 108.96 14.24
Below 10th Std 6 102.83 9.02
Parents with respect to their locality. It can be concluded that the locality of parents is not a
significant factor to predict the awareness of parents on early intervention.
Table 4.15
Mean, Standard Deviation of the total awareness scores of parents on early intervention
with respect to education
Education Number Mean SD
Degree and above 53 117.51 11.39
10- PDC passed 51 108.96 14.24
Below 10th Std 6 102.83 9.02
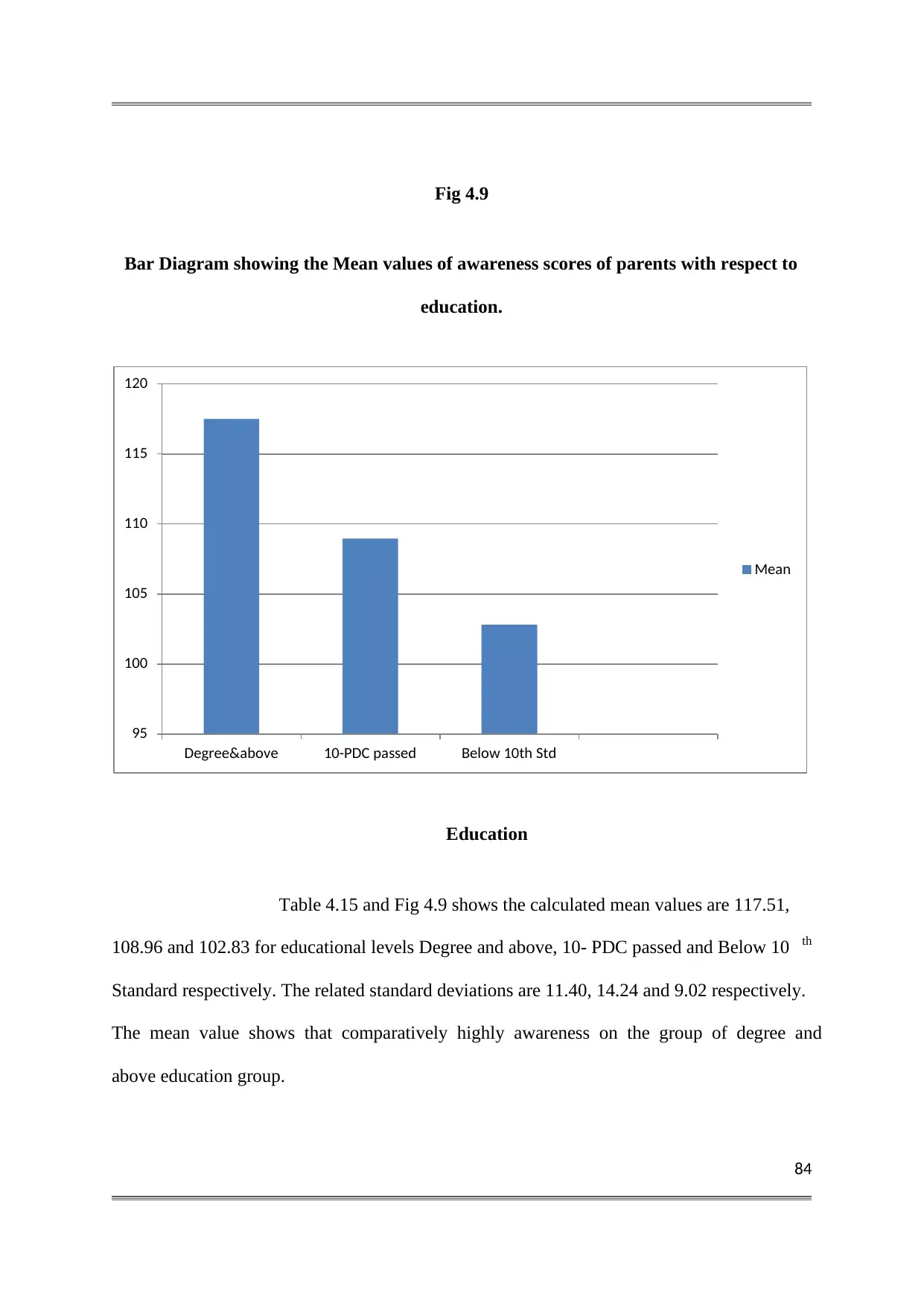
84
Fig 4.9
Bar Diagram showing the Mean values of awareness scores of parents with respect to
education.
Education
Table 4.15 and Fig 4.9 shows the calculated mean values are 117.51,
108.96 and 102.83 for educational levels Degree and above, 10- PDC passed and Below 10 th
Standard respectively. The related standard deviations are 11.40, 14.24 and 9.02 respectively.
The mean value shows that comparatively highly awareness on the group of degree and
above education group.
95
100
105
110
115
120
Degree&above 10-PDC passed Below 10th Std
Mean
Fig 4.9
Bar Diagram showing the Mean values of awareness scores of parents with respect to
education.
Education
Table 4.15 and Fig 4.9 shows the calculated mean values are 117.51,
108.96 and 102.83 for educational levels Degree and above, 10- PDC passed and Below 10 th
Standard respectively. The related standard deviations are 11.40, 14.24 and 9.02 respectively.
The mean value shows that comparatively highly awareness on the group of degree and
above education group.
95
100
105
110
115
120
Degree&above 10-PDC passed Below 10th Std
Mean
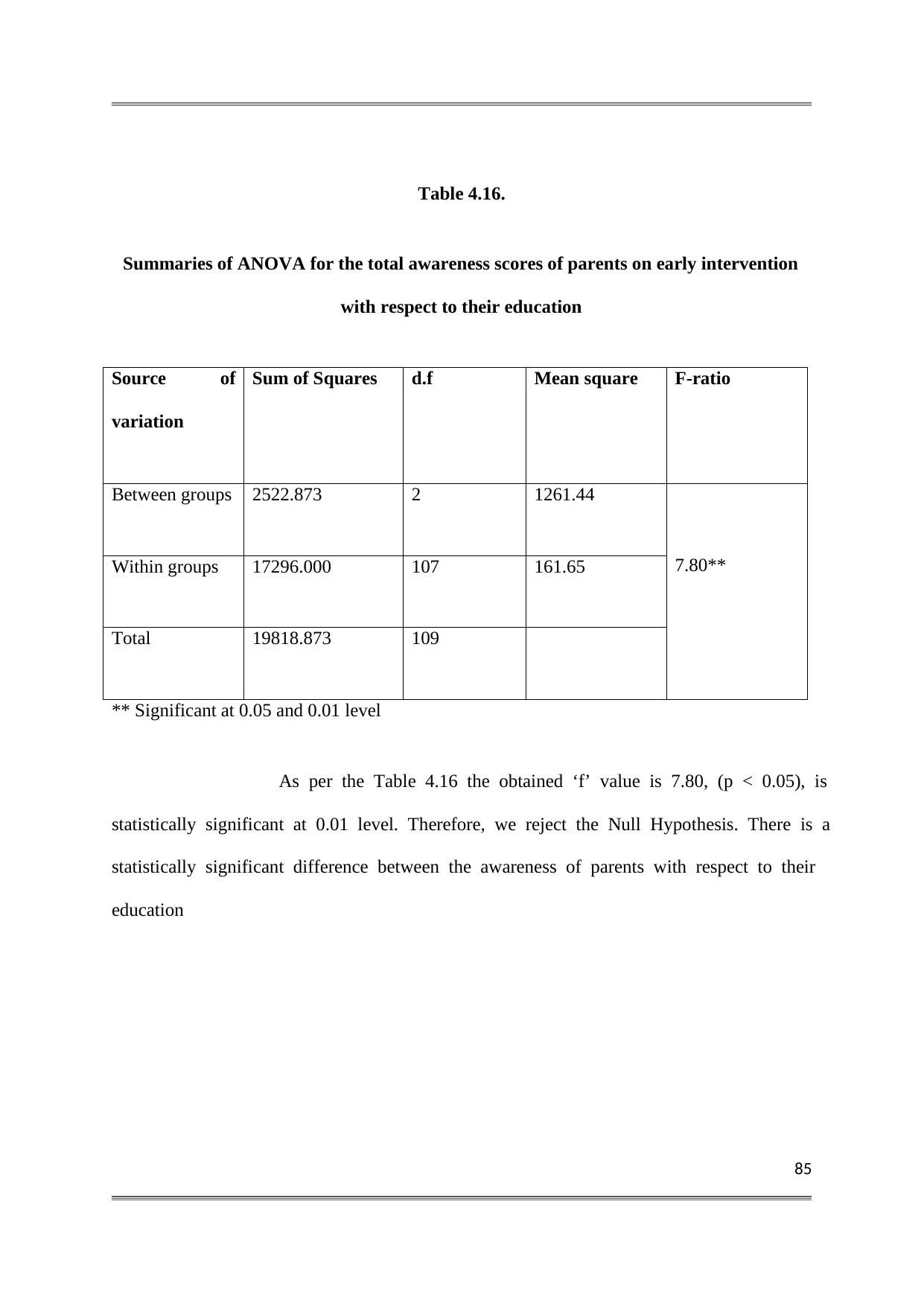
85
Table 4.16.
Summaries of ANOVA for the total awareness scores of parents on early intervention
with respect to their education
Source of
variation
Sum of Squares d.f Mean square F-ratio
Between groups 2522.873 2 1261.44
7.80**Within groups 17296.000 107 161.65
Total 19818.873 109
** Significant at 0.05 and 0.01 level
As per the Table 4.16 the obtained ‘f’ value is 7.80, (p < 0.05), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis. There is a
statistically significant difference between the awareness of parents with respect to their
education
Table 4.16.
Summaries of ANOVA for the total awareness scores of parents on early intervention
with respect to their education
Source of
variation
Sum of Squares d.f Mean square F-ratio
Between groups 2522.873 2 1261.44
7.80**Within groups 17296.000 107 161.65
Total 19818.873 109
** Significant at 0.05 and 0.01 level
As per the Table 4.16 the obtained ‘f’ value is 7.80, (p < 0.05), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis. There is a
statistically significant difference between the awareness of parents with respect to their
education
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
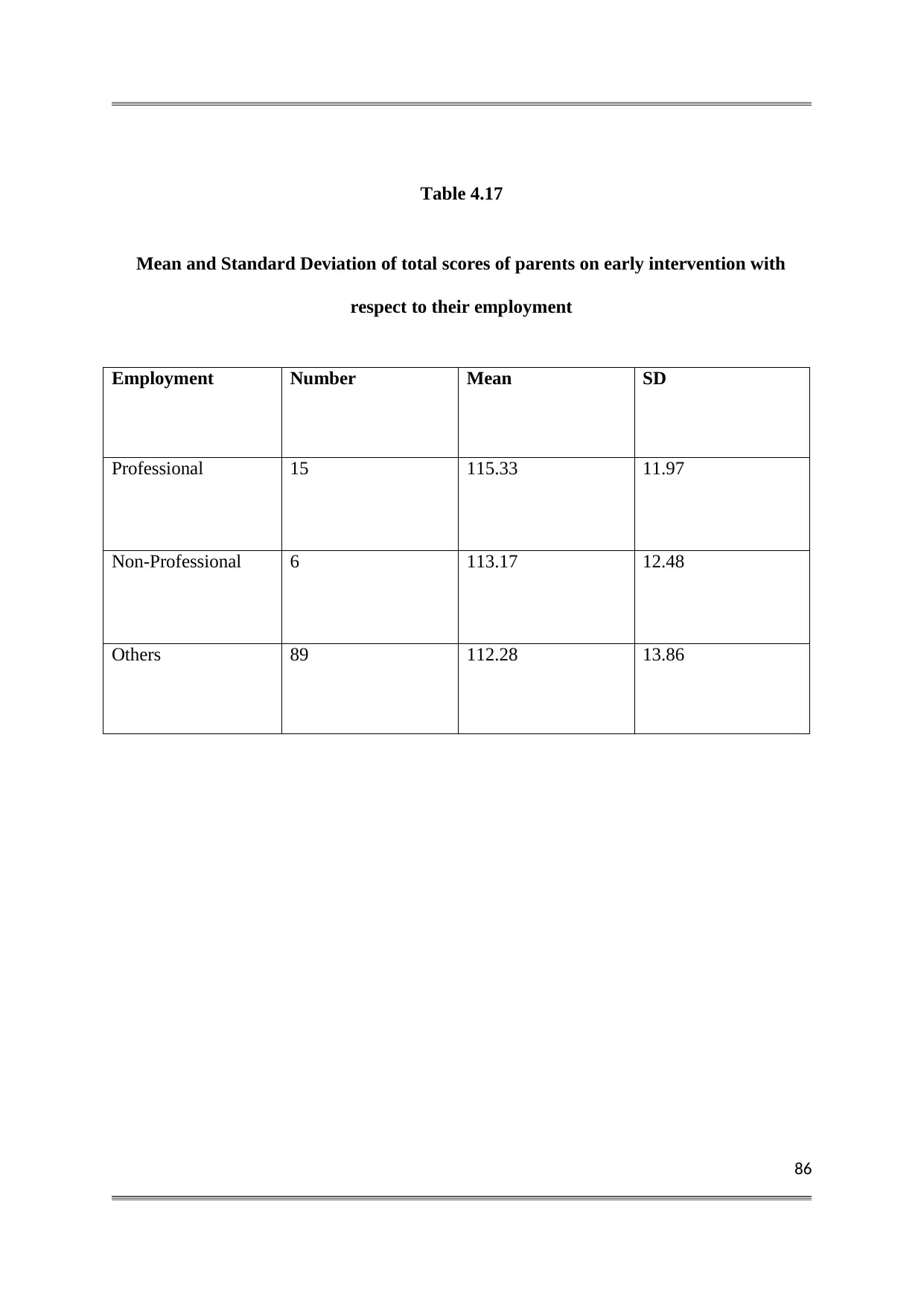
86
Table 4.17
Mean and Standard Deviation of total scores of parents on early intervention with
respect to their employment
Employment Number Mean SD
Professional 15 115.33 11.97
Non-Professional 6 113.17 12.48
Others 89 112.28 13.86
Table 4.17
Mean and Standard Deviation of total scores of parents on early intervention with
respect to their employment
Employment Number Mean SD
Professional 15 115.33 11.97
Non-Professional 6 113.17 12.48
Others 89 112.28 13.86
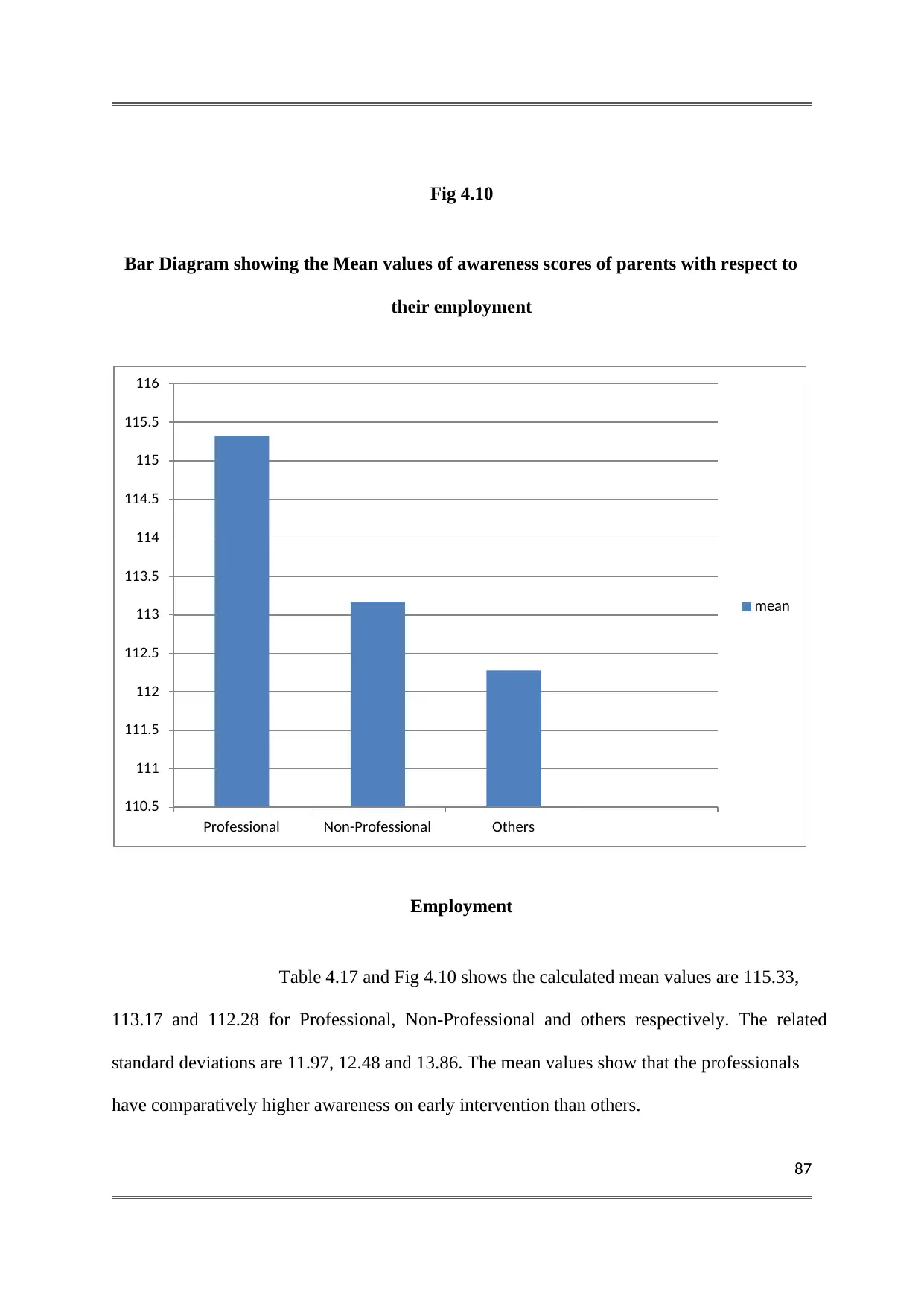
87
Fig 4.10
Bar Diagram showing the Mean values of awareness scores of parents with respect to
their employment
Employment
Table 4.17 and Fig 4.10 shows the calculated mean values are 115.33,
113.17 and 112.28 for Professional, Non-Professional and others respectively. The related
standard deviations are 11.97, 12.48 and 13.86. The mean values show that the professionals
have comparatively higher awareness on early intervention than others.
110.5
111
111.5
112
112.5
113
113.5
114
114.5
115
115.5
116
Professional Non-Professional Others
mean
Fig 4.10
Bar Diagram showing the Mean values of awareness scores of parents with respect to
their employment
Employment
Table 4.17 and Fig 4.10 shows the calculated mean values are 115.33,
113.17 and 112.28 for Professional, Non-Professional and others respectively. The related
standard deviations are 11.97, 12.48 and 13.86. The mean values show that the professionals
have comparatively higher awareness on early intervention than others.
110.5
111
111.5
112
112.5
113
113.5
114
114.5
115
115.5
116
Professional Non-Professional Others
mean
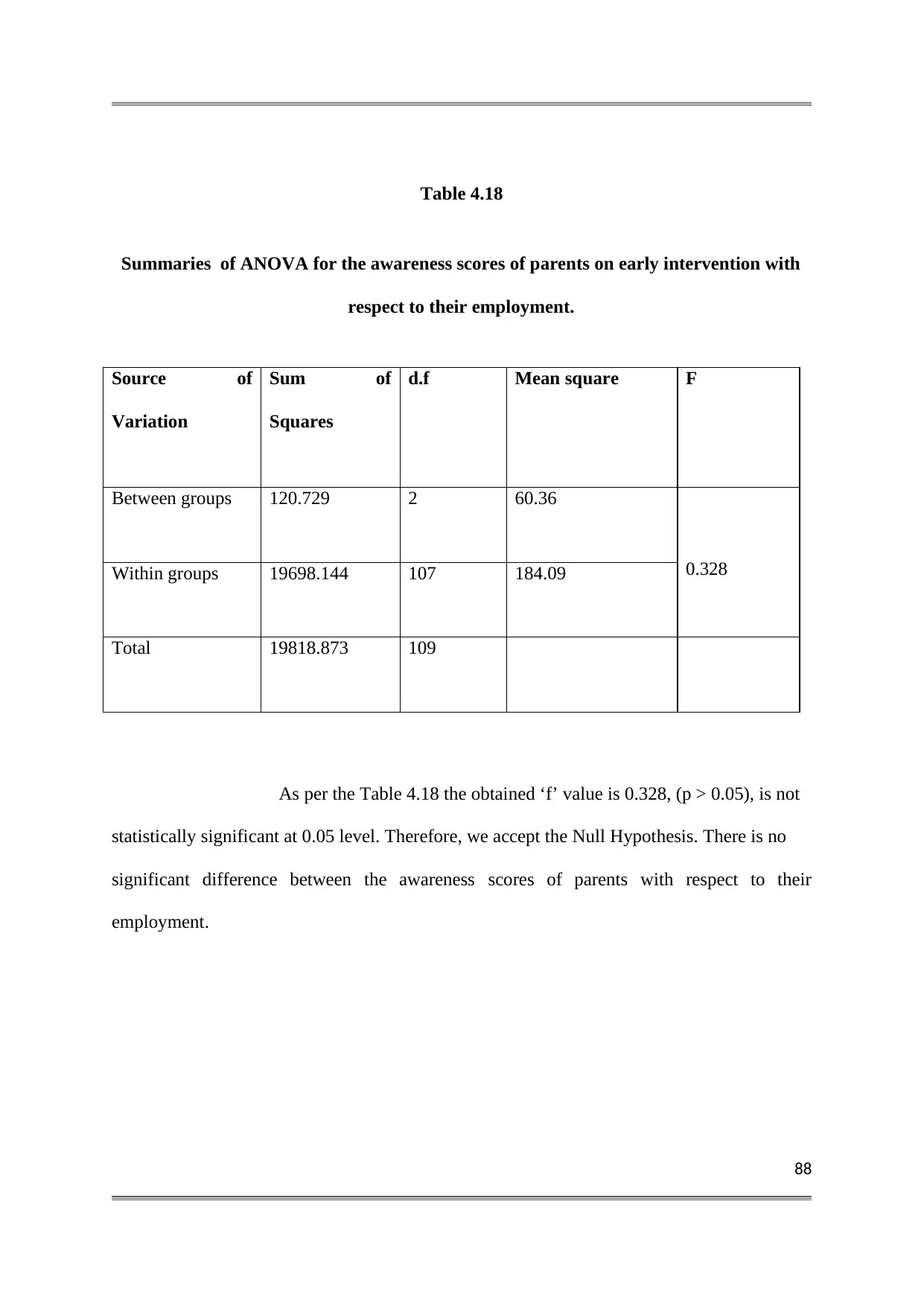
88
Table 4.18
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to their employment.
Source of
Variation
Sum of
Squares
d.f Mean square F
Between groups 120.729 2 60.36
0.328Within groups 19698.144 107 184.09
Total 19818.873 109
As per the Table 4.18 the obtained ‘f’ value is 0.328, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their
employment.
Table 4.18
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to their employment.
Source of
Variation
Sum of
Squares
d.f Mean square F
Between groups 120.729 2 60.36
0.328Within groups 19698.144 107 184.09
Total 19818.873 109
As per the Table 4.18 the obtained ‘f’ value is 0.328, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their
employment.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
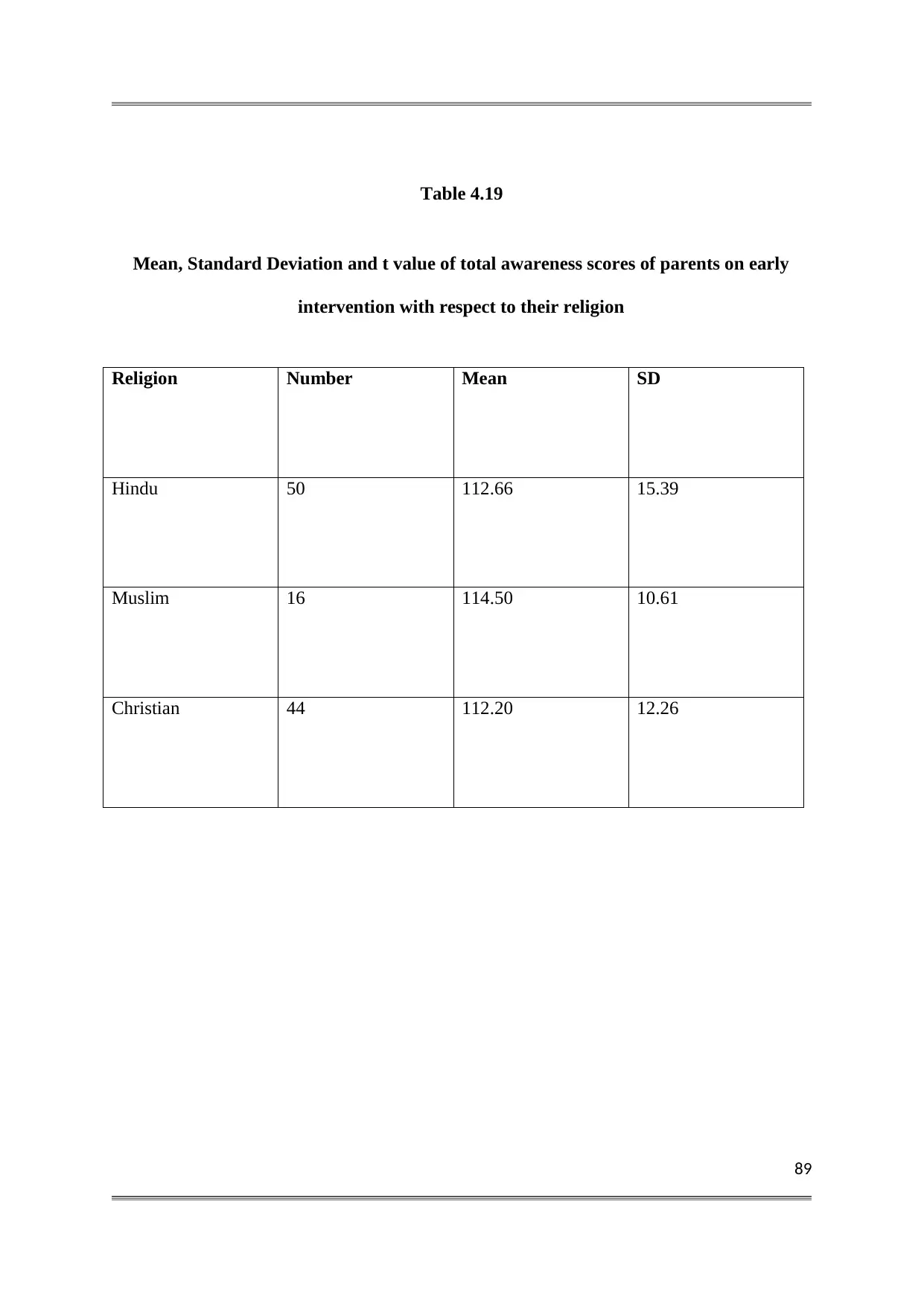
89
Table 4.19
Mean, Standard Deviation and t value of total awareness scores of parents on early
intervention with respect to their religion
Religion Number Mean SD
Hindu 50 112.66 15.39
Muslim 16 114.50 10.61
Christian 44 112.20 12.26
Table 4.19
Mean, Standard Deviation and t value of total awareness scores of parents on early
intervention with respect to their religion
Religion Number Mean SD
Hindu 50 112.66 15.39
Muslim 16 114.50 10.61
Christian 44 112.20 12.26
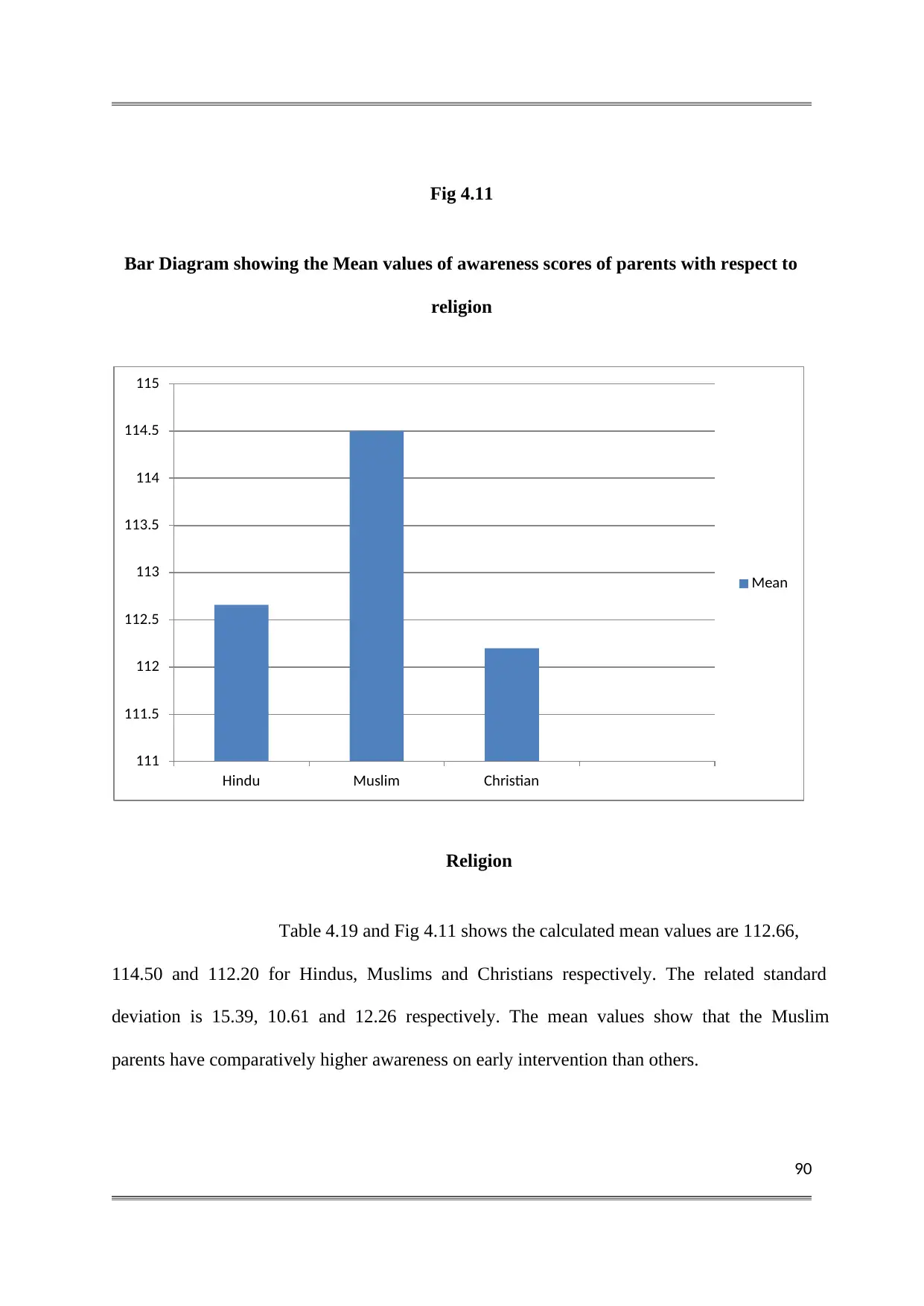
90
Fig 4.11
Bar Diagram showing the Mean values of awareness scores of parents with respect to
religion
Religion
Table 4.19 and Fig 4.11 shows the calculated mean values are 112.66,
114.50 and 112.20 for Hindus, Muslims and Christians respectively. The related standard
deviation is 15.39, 10.61 and 12.26 respectively. The mean values show that the Muslim
parents have comparatively higher awareness on early intervention than others.
111
111.5
112
112.5
113
113.5
114
114.5
115
Hindu Muslim Christian
Mean
Fig 4.11
Bar Diagram showing the Mean values of awareness scores of parents with respect to
religion
Religion
Table 4.19 and Fig 4.11 shows the calculated mean values are 112.66,
114.50 and 112.20 for Hindus, Muslims and Christians respectively. The related standard
deviation is 15.39, 10.61 and 12.26 respectively. The mean values show that the Muslim
parents have comparatively higher awareness on early intervention than others.
111
111.5
112
112.5
113
113.5
114
114.5
115
Hindu Muslim Christian
Mean
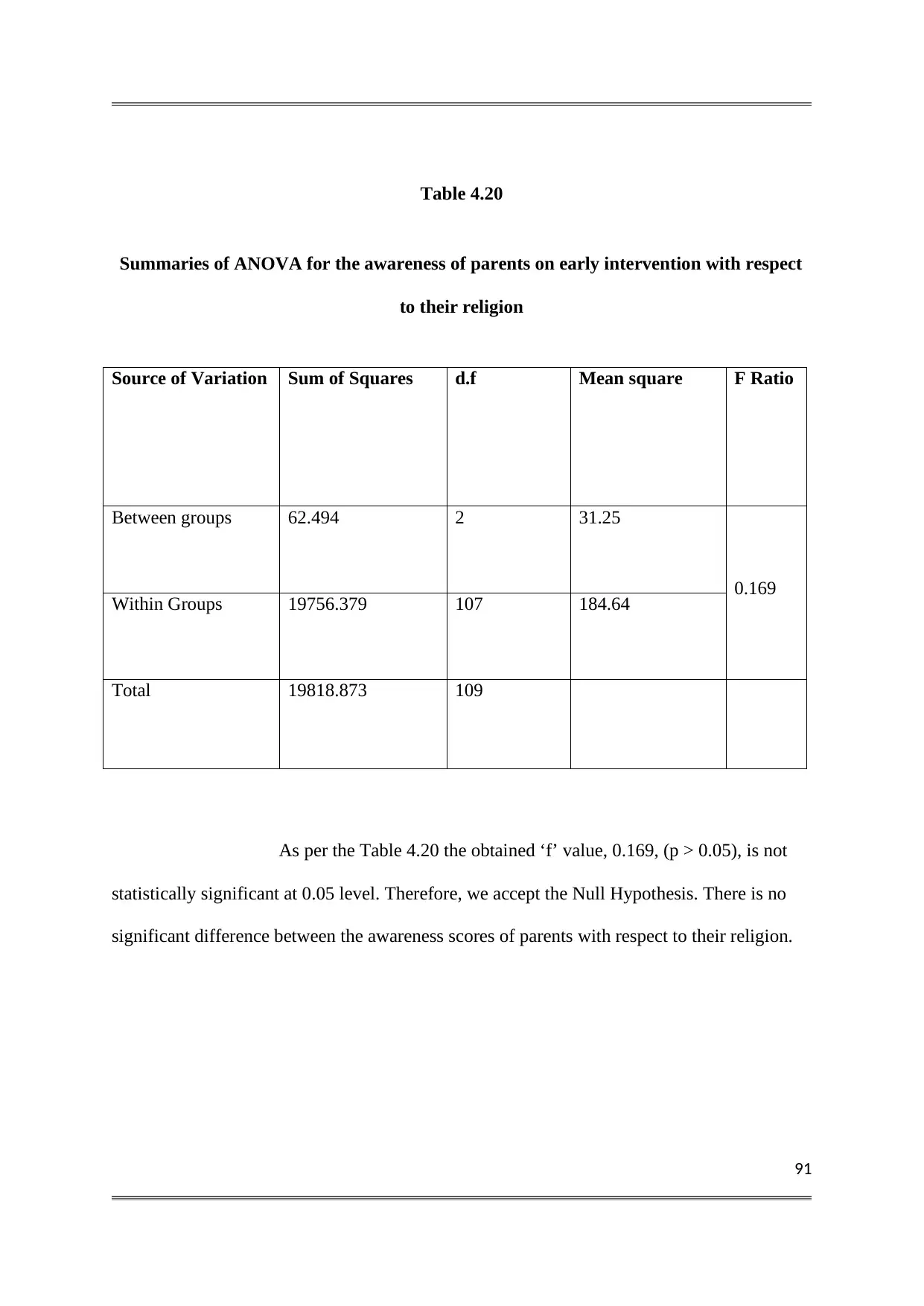
91
Table 4.20
Summaries of ANOVA for the awareness of parents on early intervention with respect
to their religion
Source of Variation Sum of Squares d.f Mean square F Ratio
Between groups 62.494 2 31.25
0.169
Within Groups 19756.379 107 184.64
Total 19818.873 109
As per the Table 4.20 the obtained ‘f’ value, 0.169, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their religion.
Table 4.20
Summaries of ANOVA for the awareness of parents on early intervention with respect
to their religion
Source of Variation Sum of Squares d.f Mean square F Ratio
Between groups 62.494 2 31.25
0.169
Within Groups 19756.379 107 184.64
Total 19818.873 109
As per the Table 4.20 the obtained ‘f’ value, 0.169, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the awareness scores of parents with respect to their religion.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
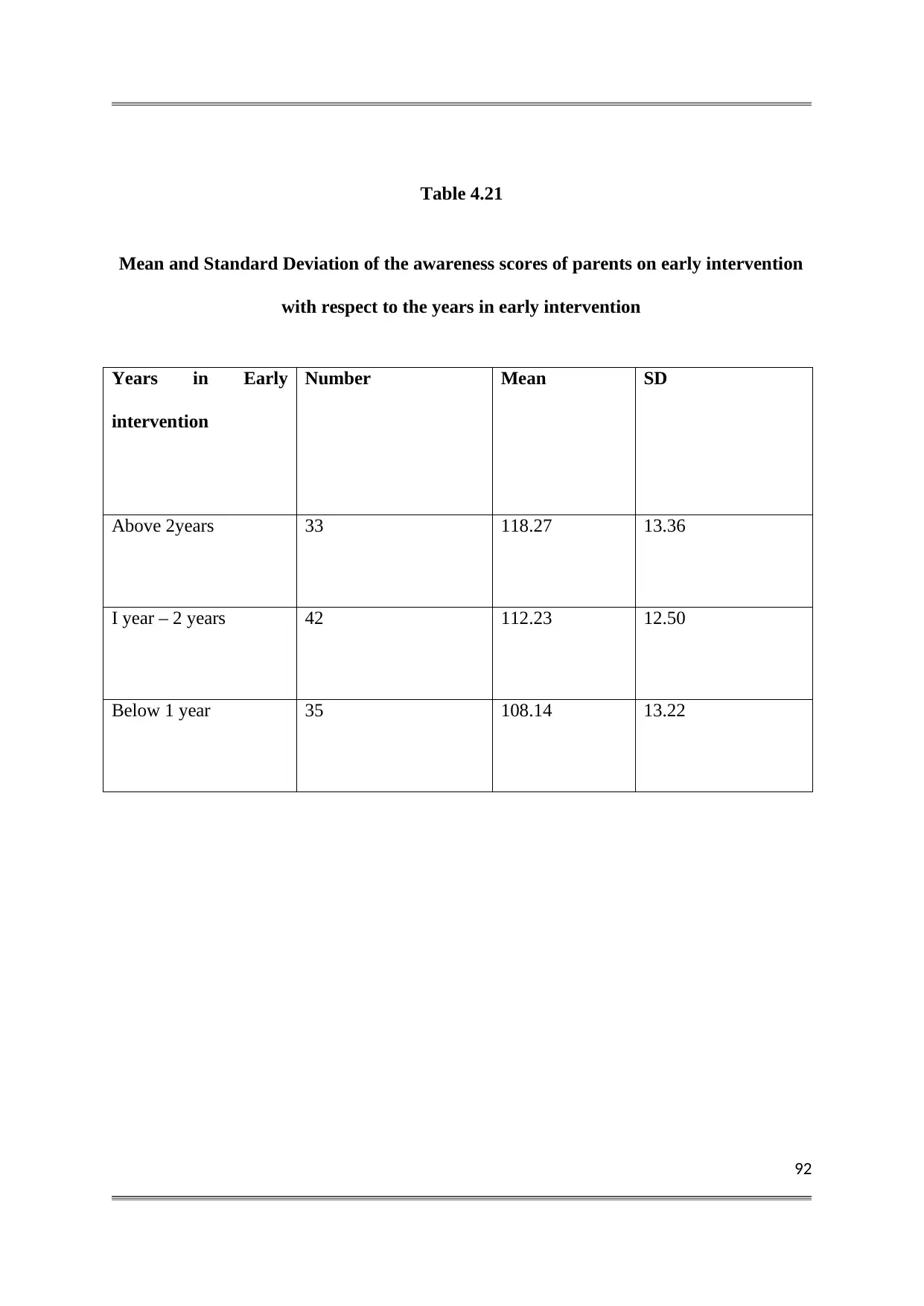
92
Table 4.21
Mean and Standard Deviation of the awareness scores of parents on early intervention
with respect to the years in early intervention
Years in Early
intervention
Number Mean SD
Above 2years 33 118.27 13.36
I year – 2 years 42 112.23 12.50
Below 1 year 35 108.14 13.22
Table 4.21
Mean and Standard Deviation of the awareness scores of parents on early intervention
with respect to the years in early intervention
Years in Early
intervention
Number Mean SD
Above 2years 33 118.27 13.36
I year – 2 years 42 112.23 12.50
Below 1 year 35 108.14 13.22
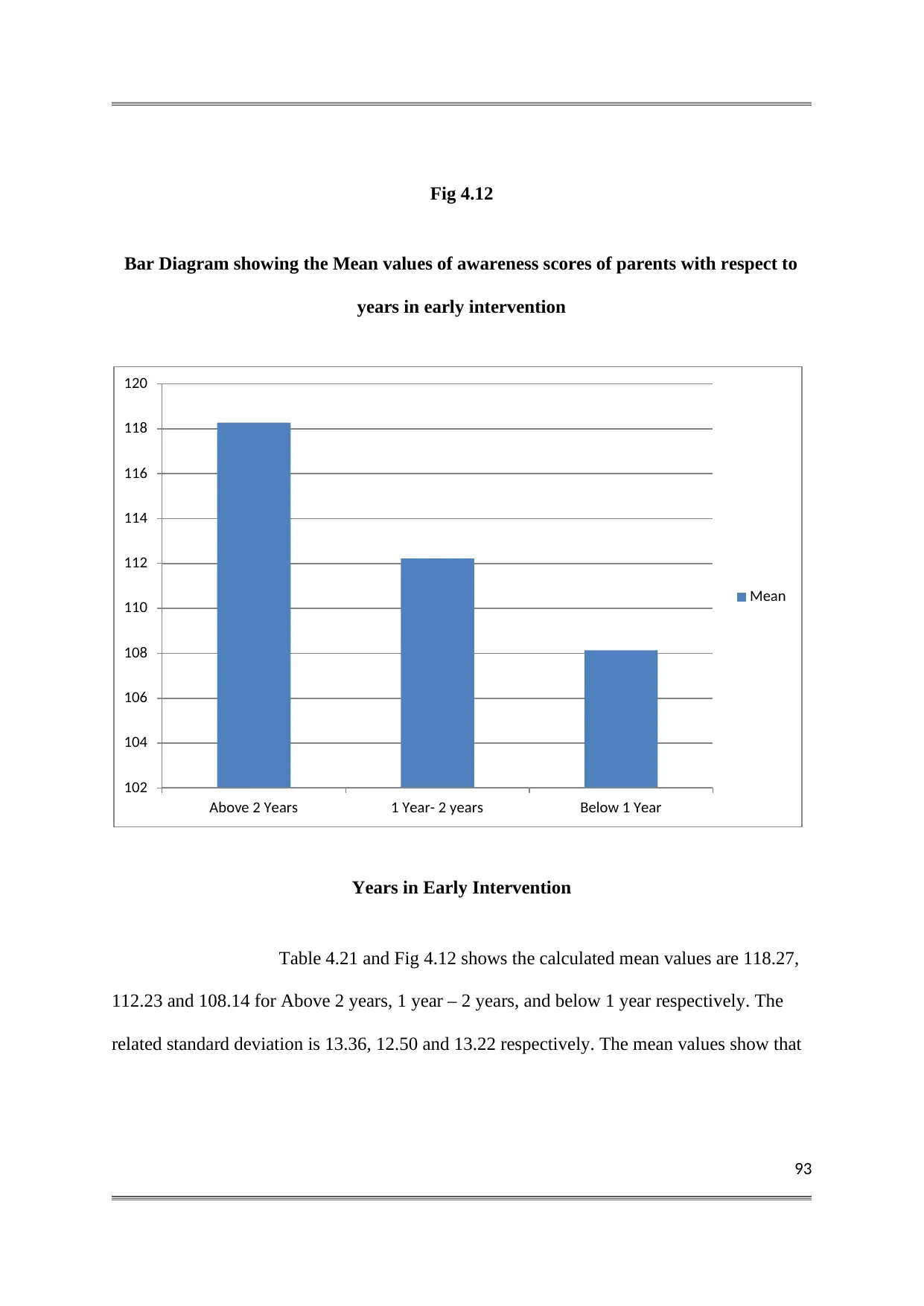
93
Fig 4.12
Bar Diagram showing the Mean values of awareness scores of parents with respect to
years in early intervention
Years in Early Intervention
Table 4.21 and Fig 4.12 shows the calculated mean values are 118.27,
112.23 and 108.14 for Above 2 years, 1 year – 2 years, and below 1 year respectively. The
related standard deviation is 13.36, 12.50 and 13.22 respectively. The mean values show that
102
104
106
108
110
112
114
116
118
120
Above 2 Years 1 Year- 2 years Below 1 Year
Mean
Fig 4.12
Bar Diagram showing the Mean values of awareness scores of parents with respect to
years in early intervention
Years in Early Intervention
Table 4.21 and Fig 4.12 shows the calculated mean values are 118.27,
112.23 and 108.14 for Above 2 years, 1 year – 2 years, and below 1 year respectively. The
related standard deviation is 13.36, 12.50 and 13.22 respectively. The mean values show that
102
104
106
108
110
112
114
116
118
120
Above 2 Years 1 Year- 2 years Below 1 Year
Mean
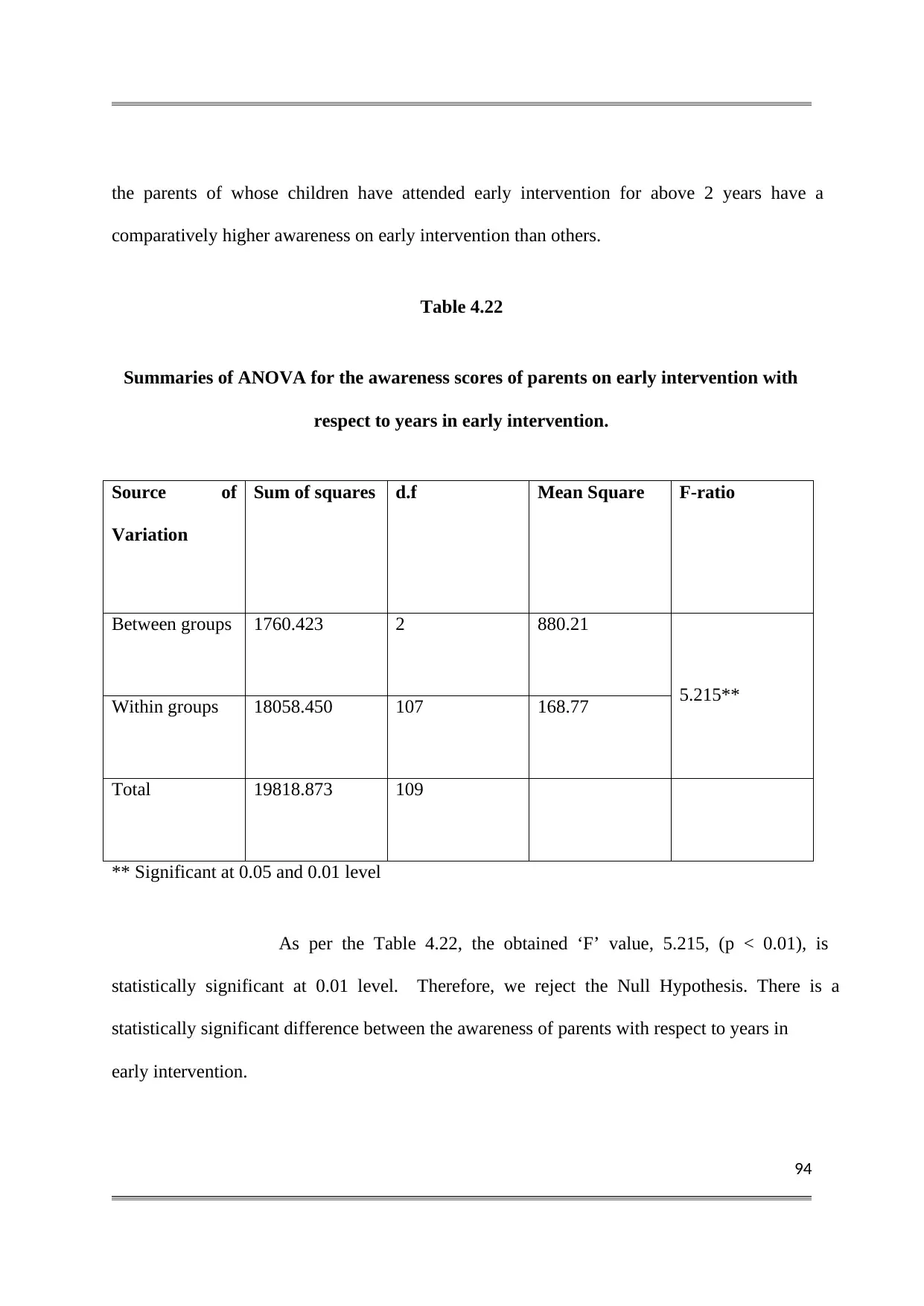
94
the parents of whose children have attended early intervention for above 2 years have a
comparatively higher awareness on early intervention than others.
Table 4.22
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to years in early intervention.
Source of
Variation
Sum of squares d.f Mean Square F-ratio
Between groups 1760.423 2 880.21
5.215**
Within groups 18058.450 107 168.77
Total 19818.873 109
** Significant at 0.05 and 0.01 level
As per the Table 4.22, the obtained ‘F’ value, 5.215, (p < 0.01), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis. There is a
statistically significant difference between the awareness of parents with respect to years in
early intervention.
the parents of whose children have attended early intervention for above 2 years have a
comparatively higher awareness on early intervention than others.
Table 4.22
Summaries of ANOVA for the awareness scores of parents on early intervention with
respect to years in early intervention.
Source of
Variation
Sum of squares d.f Mean Square F-ratio
Between groups 1760.423 2 880.21
5.215**
Within groups 18058.450 107 168.77
Total 19818.873 109
** Significant at 0.05 and 0.01 level
As per the Table 4.22, the obtained ‘F’ value, 5.215, (p < 0.01), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis. There is a
statistically significant difference between the awareness of parents with respect to years in
early intervention.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
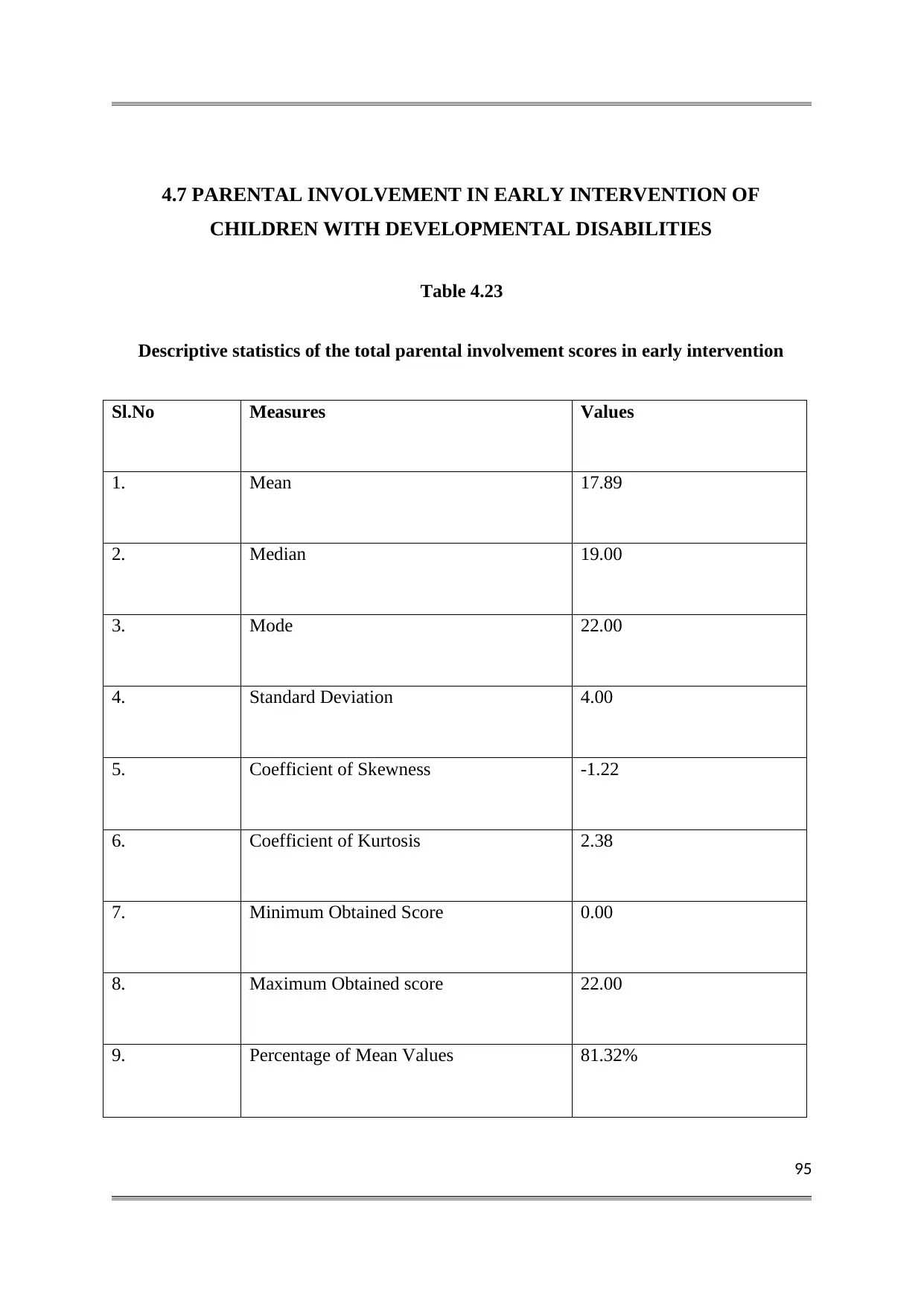
95
4.7 PARENTAL INVOLVEMENT IN EARLY INTERVENTION OF
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Table 4.23
Descriptive statistics of the total parental involvement scores in early intervention
Sl.No Measures Values
1. Mean 17.89
2. Median 19.00
3. Mode 22.00
4. Standard Deviation 4.00
5. Coefficient of Skewness -1.22
6. Coefficient of Kurtosis 2.38
7. Minimum Obtained Score 0.00
8. Maximum Obtained score 22.00
9. Percentage of Mean Values 81.32%
4.7 PARENTAL INVOLVEMENT IN EARLY INTERVENTION OF
CHILDREN WITH DEVELOPMENTAL DISABILITIES
Table 4.23
Descriptive statistics of the total parental involvement scores in early intervention
Sl.No Measures Values
1. Mean 17.89
2. Median 19.00
3. Mode 22.00
4. Standard Deviation 4.00
5. Coefficient of Skewness -1.22
6. Coefficient of Kurtosis 2.38
7. Minimum Obtained Score 0.00
8. Maximum Obtained score 22.00
9. Percentage of Mean Values 81.32%
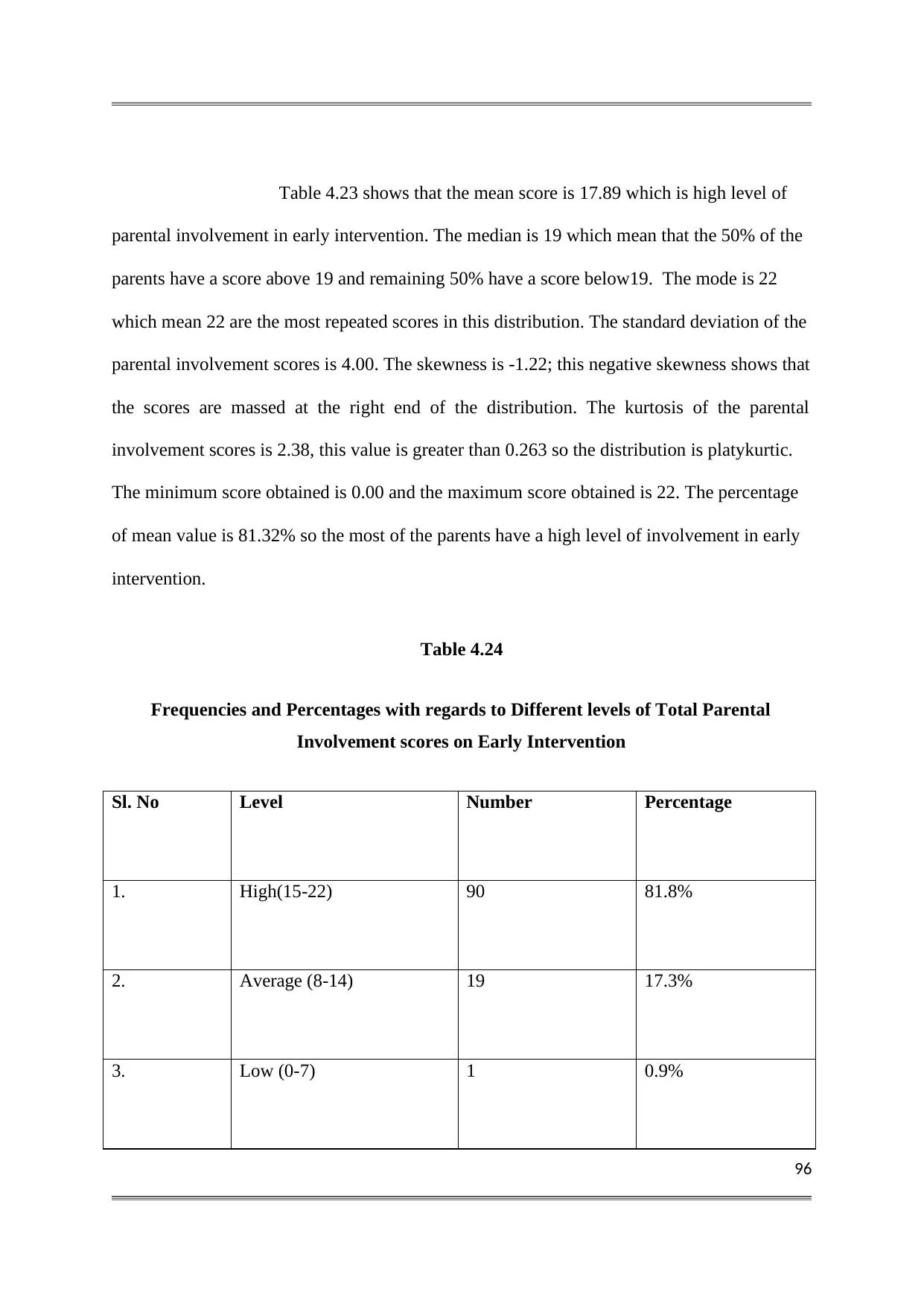
96
Table 4.23 shows that the mean score is 17.89 which is high level of
parental involvement in early intervention. The median is 19 which mean that the 50% of the
parents have a score above 19 and remaining 50% have a score below19. The mode is 22
which mean 22 are the most repeated scores in this distribution. The standard deviation of the
parental involvement scores is 4.00. The skewness is -1.22; this negative skewness shows that
the scores are massed at the right end of the distribution. The kurtosis of the parental
involvement scores is 2.38, this value is greater than 0.263 so the distribution is platykurtic.
The minimum score obtained is 0.00 and the maximum score obtained is 22. The percentage
of mean value is 81.32% so the most of the parents have a high level of involvement in early
intervention.
Table 4.24
Frequencies and Percentages with regards to Different levels of Total Parental
Involvement scores on Early Intervention
Sl. No Level Number Percentage
1. High(15-22) 90 81.8%
2. Average (8-14) 19 17.3%
3. Low (0-7) 1 0.9%
Table 4.23 shows that the mean score is 17.89 which is high level of
parental involvement in early intervention. The median is 19 which mean that the 50% of the
parents have a score above 19 and remaining 50% have a score below19. The mode is 22
which mean 22 are the most repeated scores in this distribution. The standard deviation of the
parental involvement scores is 4.00. The skewness is -1.22; this negative skewness shows that
the scores are massed at the right end of the distribution. The kurtosis of the parental
involvement scores is 2.38, this value is greater than 0.263 so the distribution is platykurtic.
The minimum score obtained is 0.00 and the maximum score obtained is 22. The percentage
of mean value is 81.32% so the most of the parents have a high level of involvement in early
intervention.
Table 4.24
Frequencies and Percentages with regards to Different levels of Total Parental
Involvement scores on Early Intervention
Sl. No Level Number Percentage
1. High(15-22) 90 81.8%
2. Average (8-14) 19 17.3%
3. Low (0-7) 1 0.9%
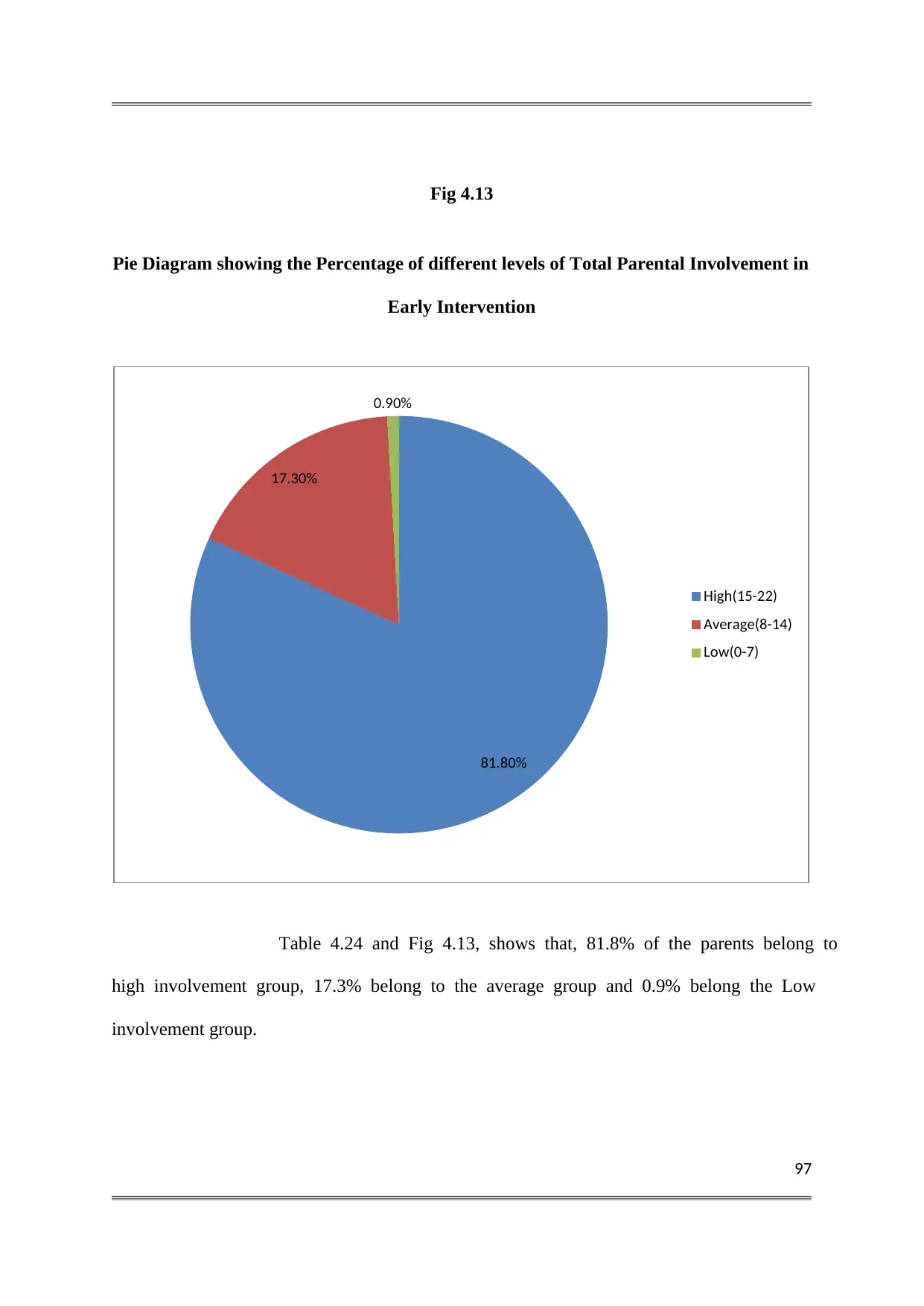
97
Fig 4.13
Pie Diagram showing the Percentage of different levels of Total Parental Involvement in
Early Intervention
Table 4.24 and Fig 4.13, shows that, 81.8% of the parents belong to
high involvement group, 17.3% belong to the average group and 0.9% belong the Low
involvement group.
81.80%
17.30%
0.90%
High(15-22)
Average(8-14)
Low(0-7)
Fig 4.13
Pie Diagram showing the Percentage of different levels of Total Parental Involvement in
Early Intervention
Table 4.24 and Fig 4.13, shows that, 81.8% of the parents belong to
high involvement group, 17.3% belong to the average group and 0.9% belong the Low
involvement group.
81.80%
17.30%
0.90%
High(15-22)
Average(8-14)
Low(0-7)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
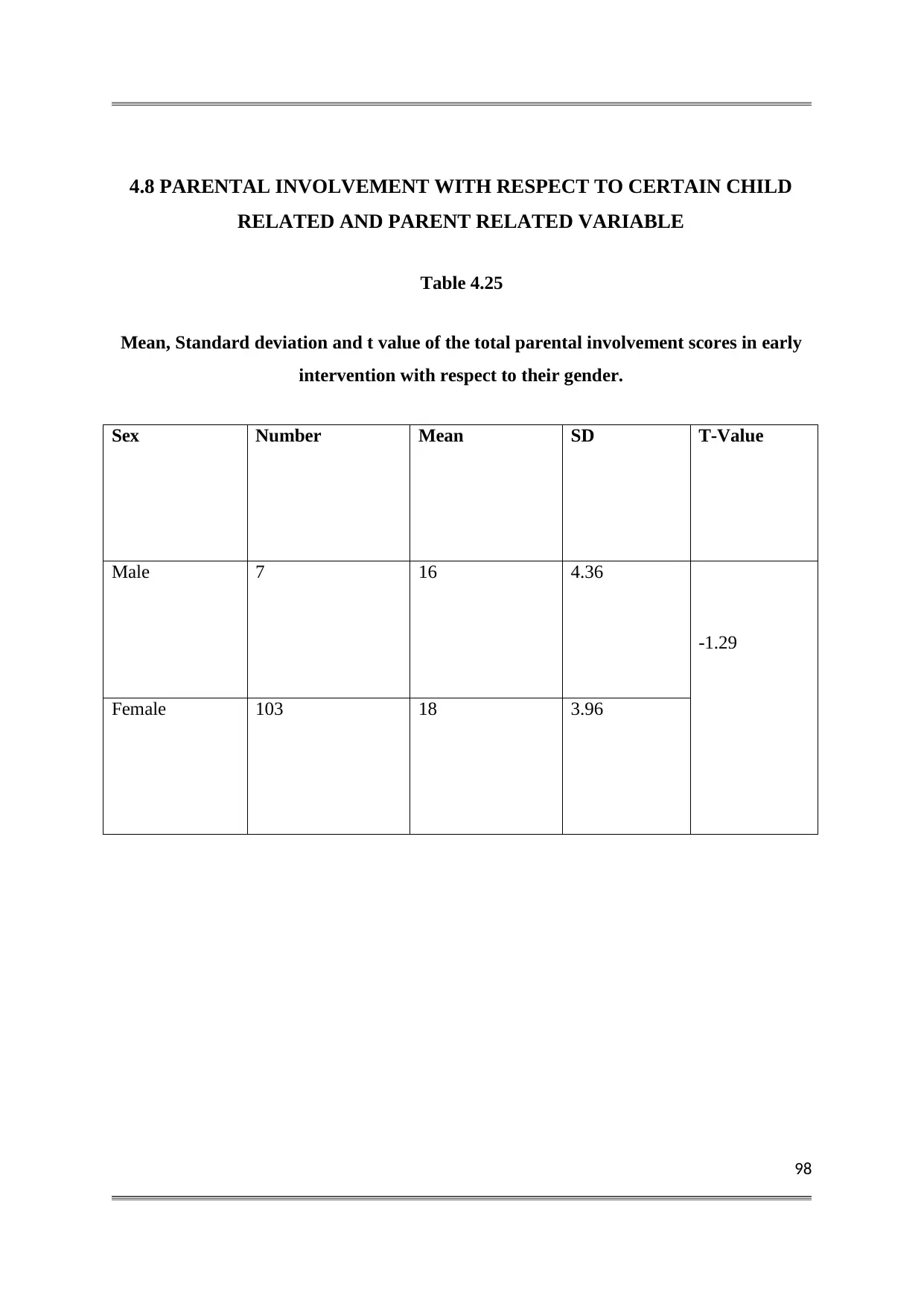
98
4.8 PARENTAL INVOLVEMENT WITH RESPECT TO CERTAIN CHILD
RELATED AND PARENT RELATED VARIABLE
Table 4.25
Mean, Standard deviation and t value of the total parental involvement scores in early
intervention with respect to their gender.
Sex Number Mean SD T-Value
Male 7 16 4.36
-1.29
Female 103 18 3.96
4.8 PARENTAL INVOLVEMENT WITH RESPECT TO CERTAIN CHILD
RELATED AND PARENT RELATED VARIABLE
Table 4.25
Mean, Standard deviation and t value of the total parental involvement scores in early
intervention with respect to their gender.
Sex Number Mean SD T-Value
Male 7 16 4.36
-1.29
Female 103 18 3.96
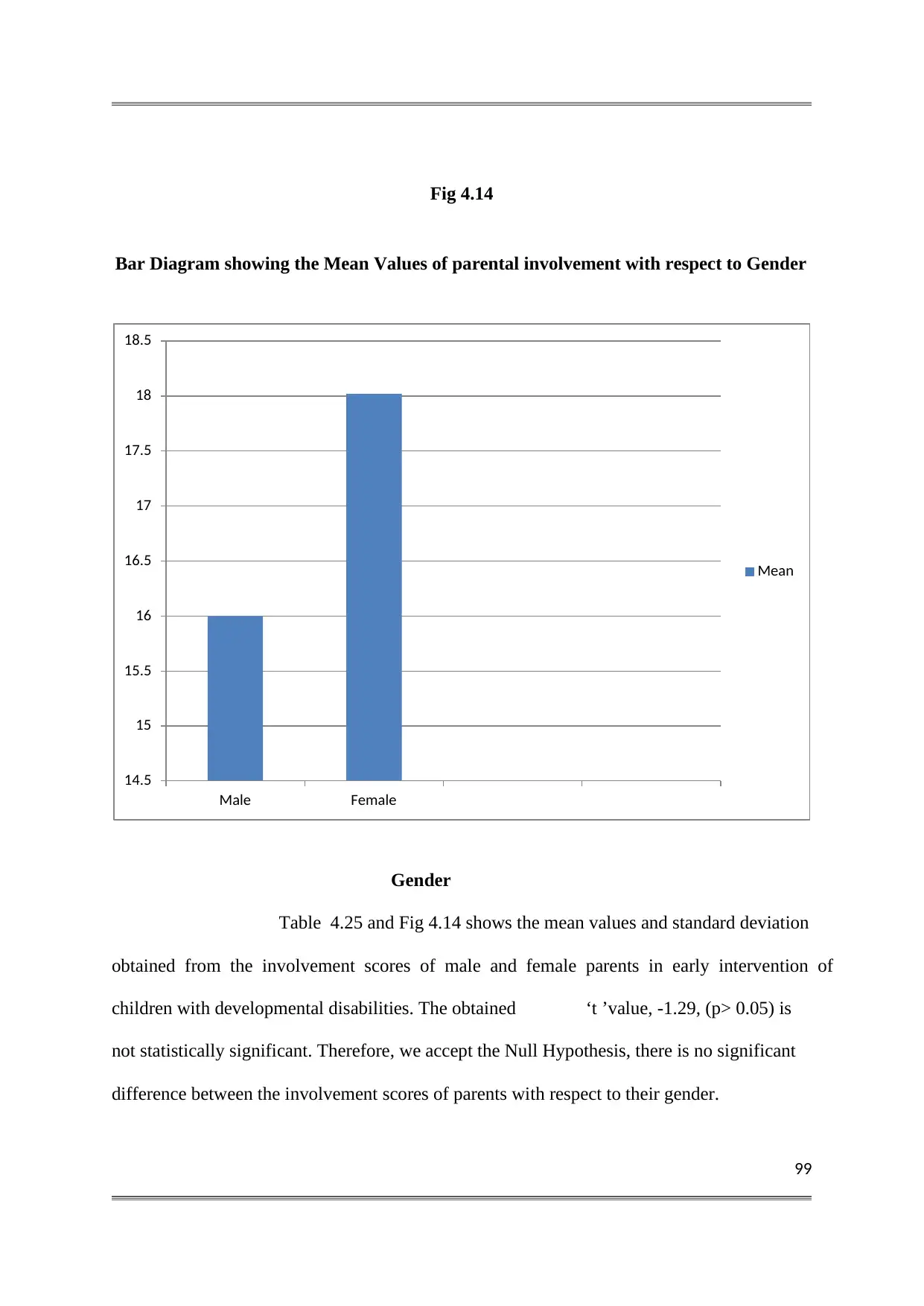
99
Fig 4.14
Bar Diagram showing the Mean Values of parental involvement with respect to Gender
Gender
Table 4.25 and Fig 4.14 shows the mean values and standard deviation
obtained from the involvement scores of male and female parents in early intervention of
children with developmental disabilities. The obtained ‘t ’value, -1.29, (p> 0.05) is
not statistically significant. Therefore, we accept the Null Hypothesis, there is no significant
difference between the involvement scores of parents with respect to their gender.
14.5
15
15.5
16
16.5
17
17.5
18
18.5
Male Female
Mean
Fig 4.14
Bar Diagram showing the Mean Values of parental involvement with respect to Gender
Gender
Table 4.25 and Fig 4.14 shows the mean values and standard deviation
obtained from the involvement scores of male and female parents in early intervention of
children with developmental disabilities. The obtained ‘t ’value, -1.29, (p> 0.05) is
not statistically significant. Therefore, we accept the Null Hypothesis, there is no significant
difference between the involvement scores of parents with respect to their gender.
14.5
15
15.5
16
16.5
17
17.5
18
18.5
Male Female
Mean
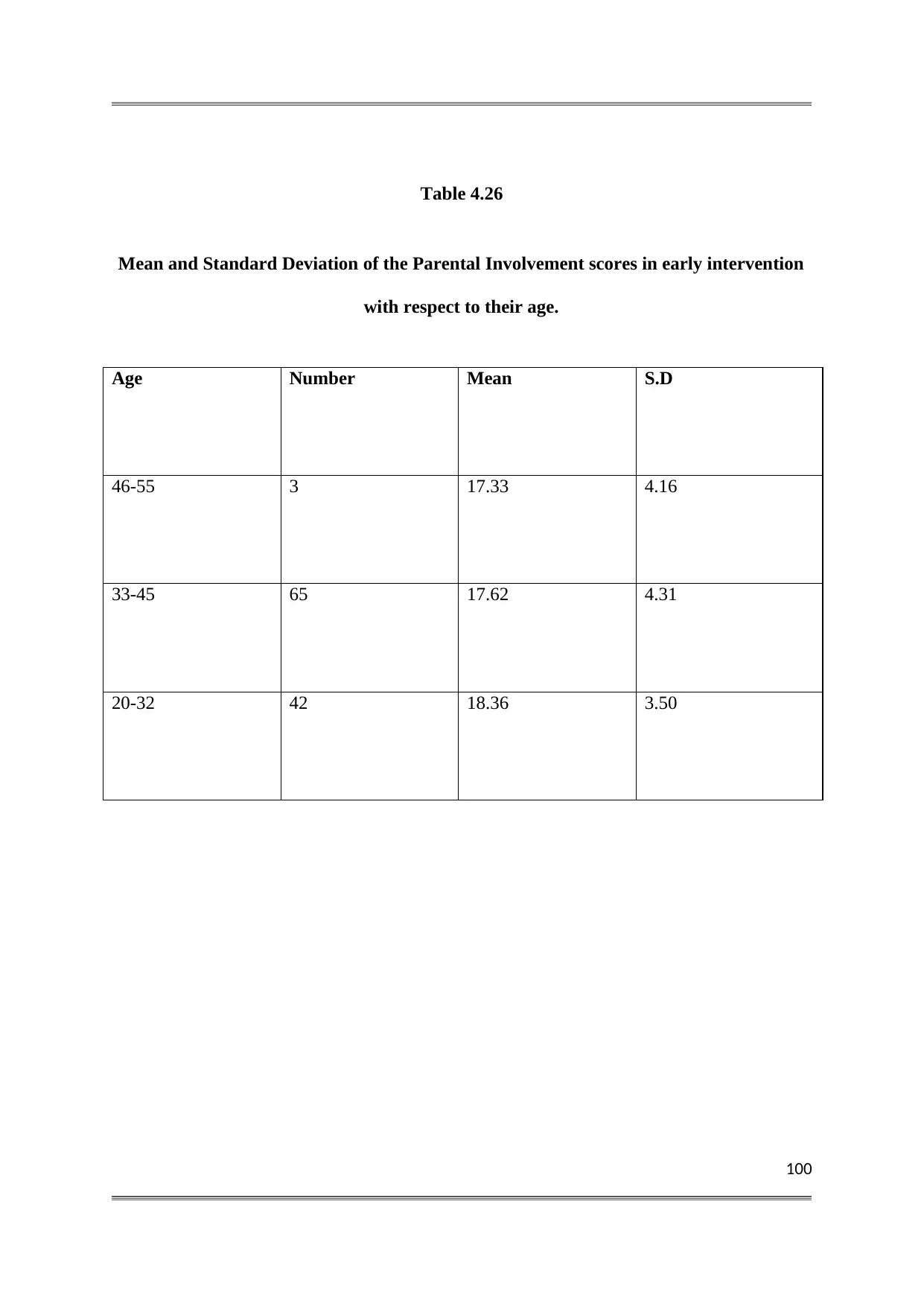
100
Table 4.26
Mean and Standard Deviation of the Parental Involvement scores in early intervention
with respect to their age.
Age Number Mean S.D
46-55 3 17.33 4.16
33-45 65 17.62 4.31
20-32 42 18.36 3.50
Table 4.26
Mean and Standard Deviation of the Parental Involvement scores in early intervention
with respect to their age.
Age Number Mean S.D
46-55 3 17.33 4.16
33-45 65 17.62 4.31
20-32 42 18.36 3.50
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
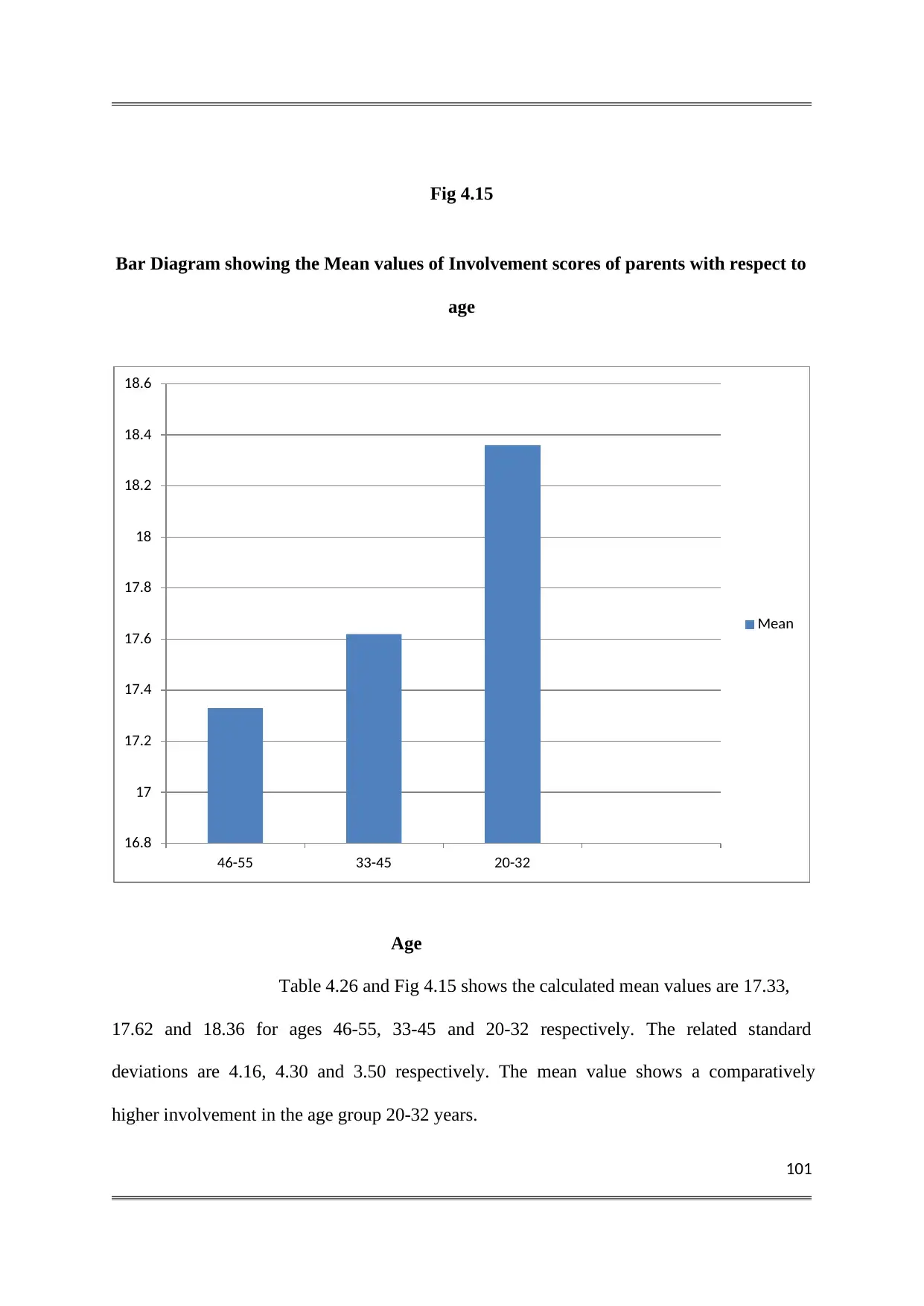
101
Fig 4.15
Bar Diagram showing the Mean values of Involvement scores of parents with respect to
age
Age
Table 4.26 and Fig 4.15 shows the calculated mean values are 17.33,
17.62 and 18.36 for ages 46-55, 33-45 and 20-32 respectively. The related standard
deviations are 4.16, 4.30 and 3.50 respectively. The mean value shows a comparatively
higher involvement in the age group 20-32 years.
16.8
17
17.2
17.4
17.6
17.8
18
18.2
18.4
18.6
46-55 33-45 20-32
Mean
Fig 4.15
Bar Diagram showing the Mean values of Involvement scores of parents with respect to
age
Age
Table 4.26 and Fig 4.15 shows the calculated mean values are 17.33,
17.62 and 18.36 for ages 46-55, 33-45 and 20-32 respectively. The related standard
deviations are 4.16, 4.30 and 3.50 respectively. The mean value shows a comparatively
higher involvement in the age group 20-32 years.
16.8
17
17.2
17.4
17.6
17.8
18
18.2
18.4
18.6
46-55 33-45 20-32
Mean
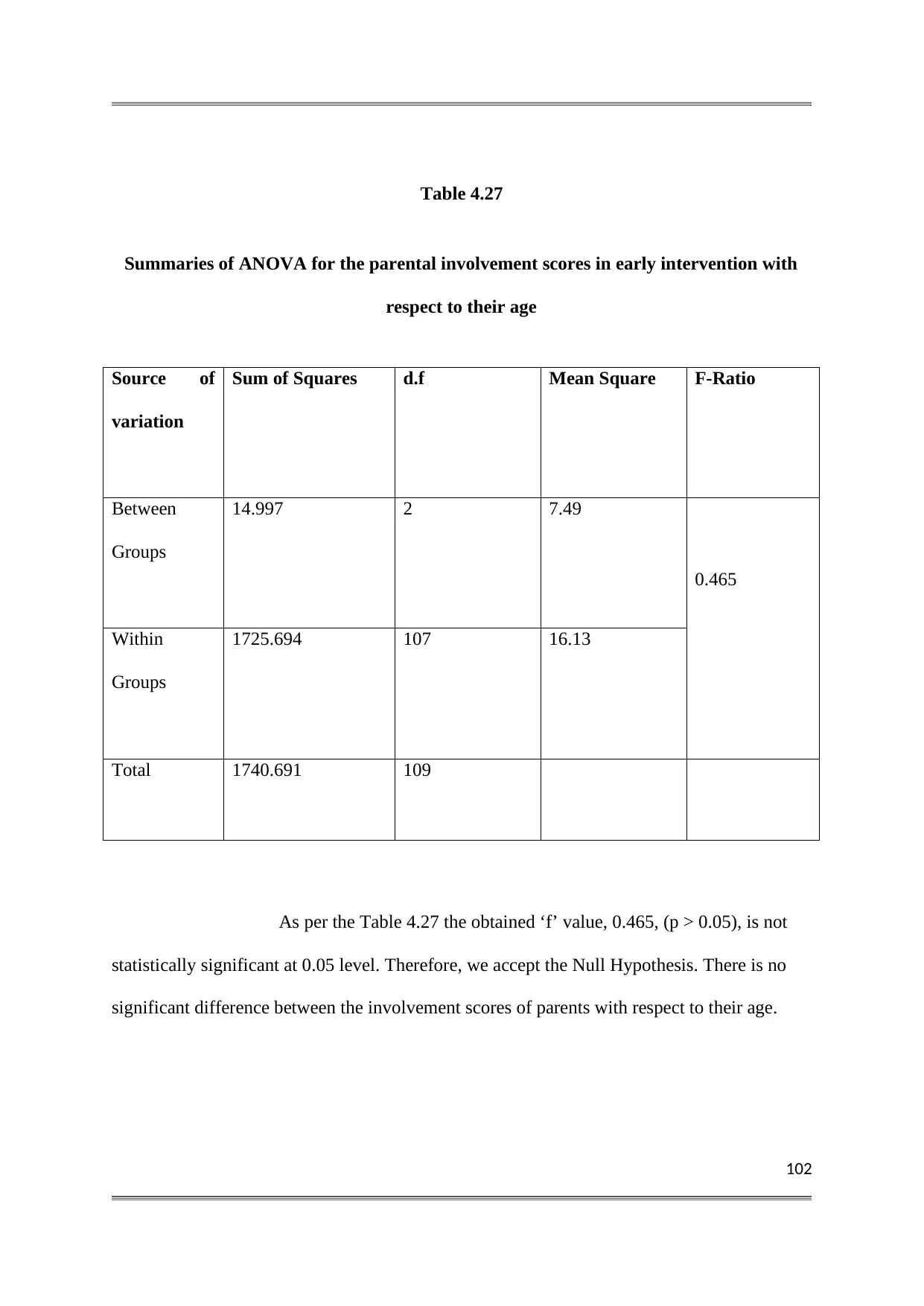
102
Table 4.27
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to their age
Source of
variation
Sum of Squares d.f Mean Square F-Ratio
Between
Groups
14.997 2 7.49
0.465
Within
Groups
1725.694 107 16.13
Total 1740.691 109
As per the Table 4.27 the obtained ‘f’ value, 0.465, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their age.
Table 4.27
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to their age
Source of
variation
Sum of Squares d.f Mean Square F-Ratio
Between
Groups
14.997 2 7.49
0.465
Within
Groups
1725.694 107 16.13
Total 1740.691 109
As per the Table 4.27 the obtained ‘f’ value, 0.465, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their age.
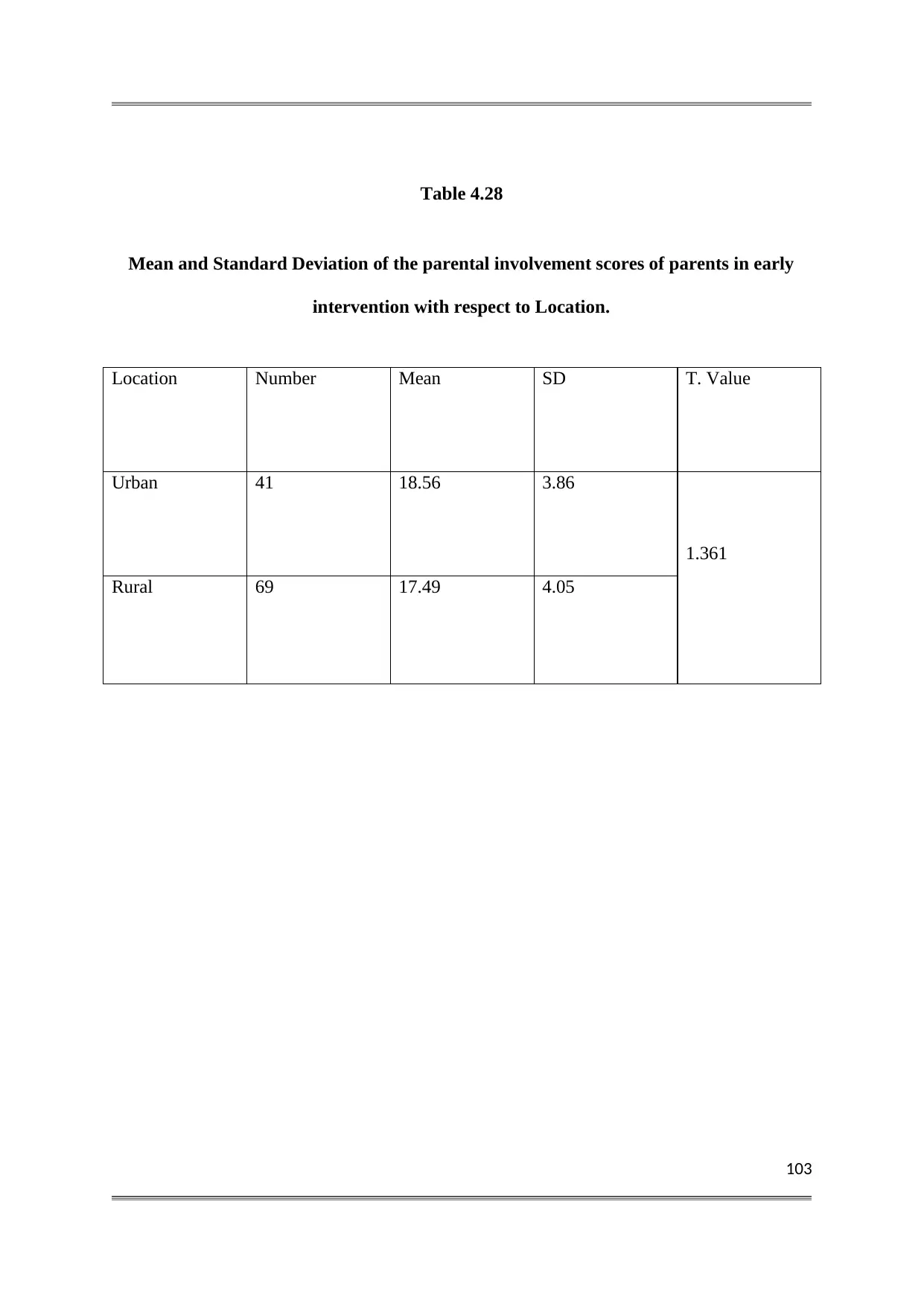
103
Table 4.28
Mean and Standard Deviation of the parental involvement scores of parents in early
intervention with respect to Location.
Location Number Mean SD T. Value
Urban 41 18.56 3.86
1.361
Rural 69 17.49 4.05
Table 4.28
Mean and Standard Deviation of the parental involvement scores of parents in early
intervention with respect to Location.
Location Number Mean SD T. Value
Urban 41 18.56 3.86
1.361
Rural 69 17.49 4.05
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
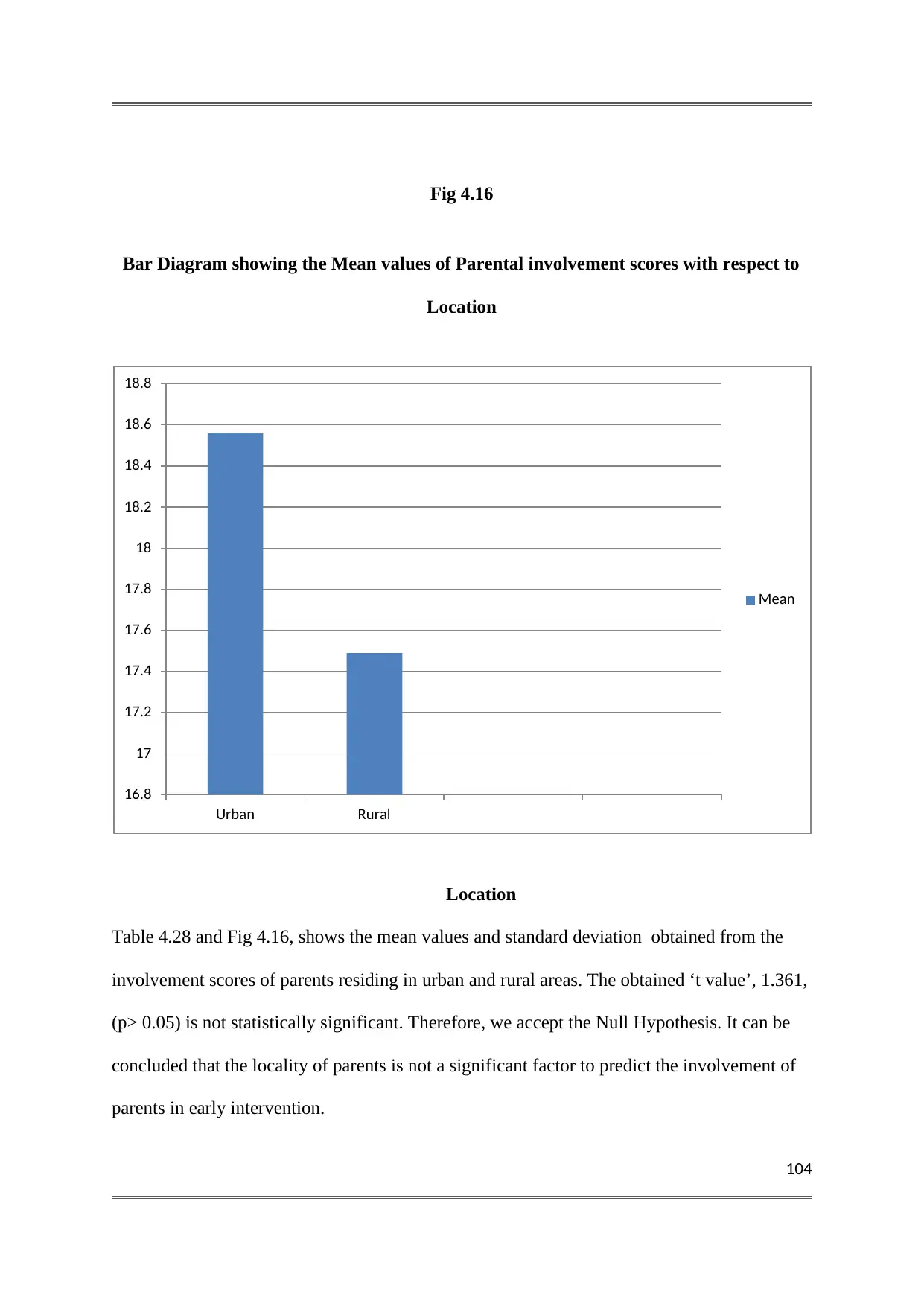
104
Fig 4.16
Bar Diagram showing the Mean values of Parental involvement scores with respect to
Location
Location
Table 4.28 and Fig 4.16, shows the mean values and standard deviation obtained from the
involvement scores of parents residing in urban and rural areas. The obtained ‘t value’, 1.361,
(p> 0.05) is not statistically significant. Therefore, we accept the Null Hypothesis. It can be
concluded that the locality of parents is not a significant factor to predict the involvement of
parents in early intervention.
16.8
17
17.2
17.4
17.6
17.8
18
18.2
18.4
18.6
18.8
Urban Rural
Mean
Fig 4.16
Bar Diagram showing the Mean values of Parental involvement scores with respect to
Location
Location
Table 4.28 and Fig 4.16, shows the mean values and standard deviation obtained from the
involvement scores of parents residing in urban and rural areas. The obtained ‘t value’, 1.361,
(p> 0.05) is not statistically significant. Therefore, we accept the Null Hypothesis. It can be
concluded that the locality of parents is not a significant factor to predict the involvement of
parents in early intervention.
16.8
17
17.2
17.4
17.6
17.8
18
18.2
18.4
18.6
18.8
Urban Rural
Mean
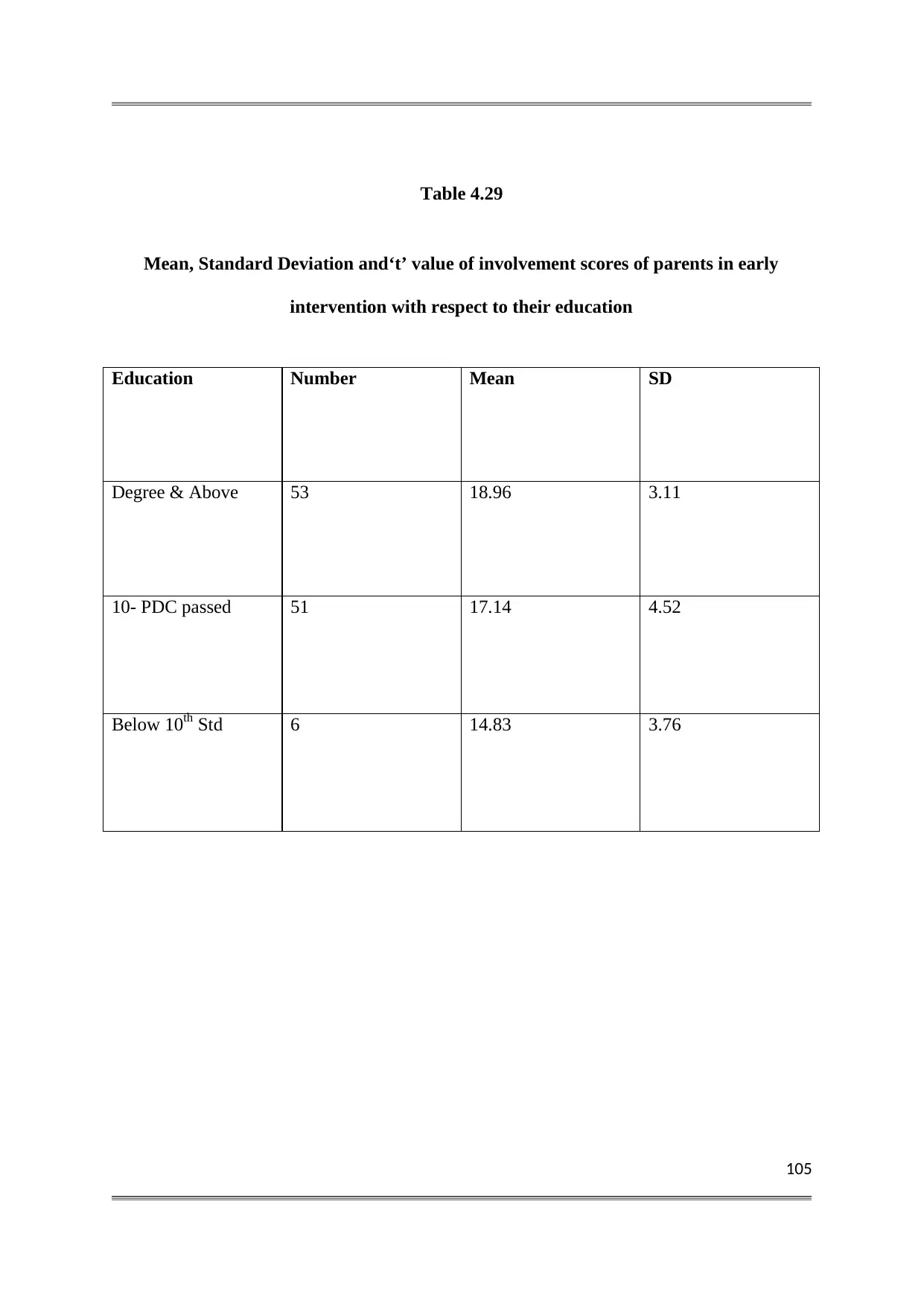
105
Table 4.29
Mean, Standard Deviation and‘t’ value of involvement scores of parents in early
intervention with respect to their education
Education Number Mean SD
Degree & Above 53 18.96 3.11
10- PDC passed 51 17.14 4.52
Below 10th Std 6 14.83 3.76
Table 4.29
Mean, Standard Deviation and‘t’ value of involvement scores of parents in early
intervention with respect to their education
Education Number Mean SD
Degree & Above 53 18.96 3.11
10- PDC passed 51 17.14 4.52
Below 10th Std 6 14.83 3.76
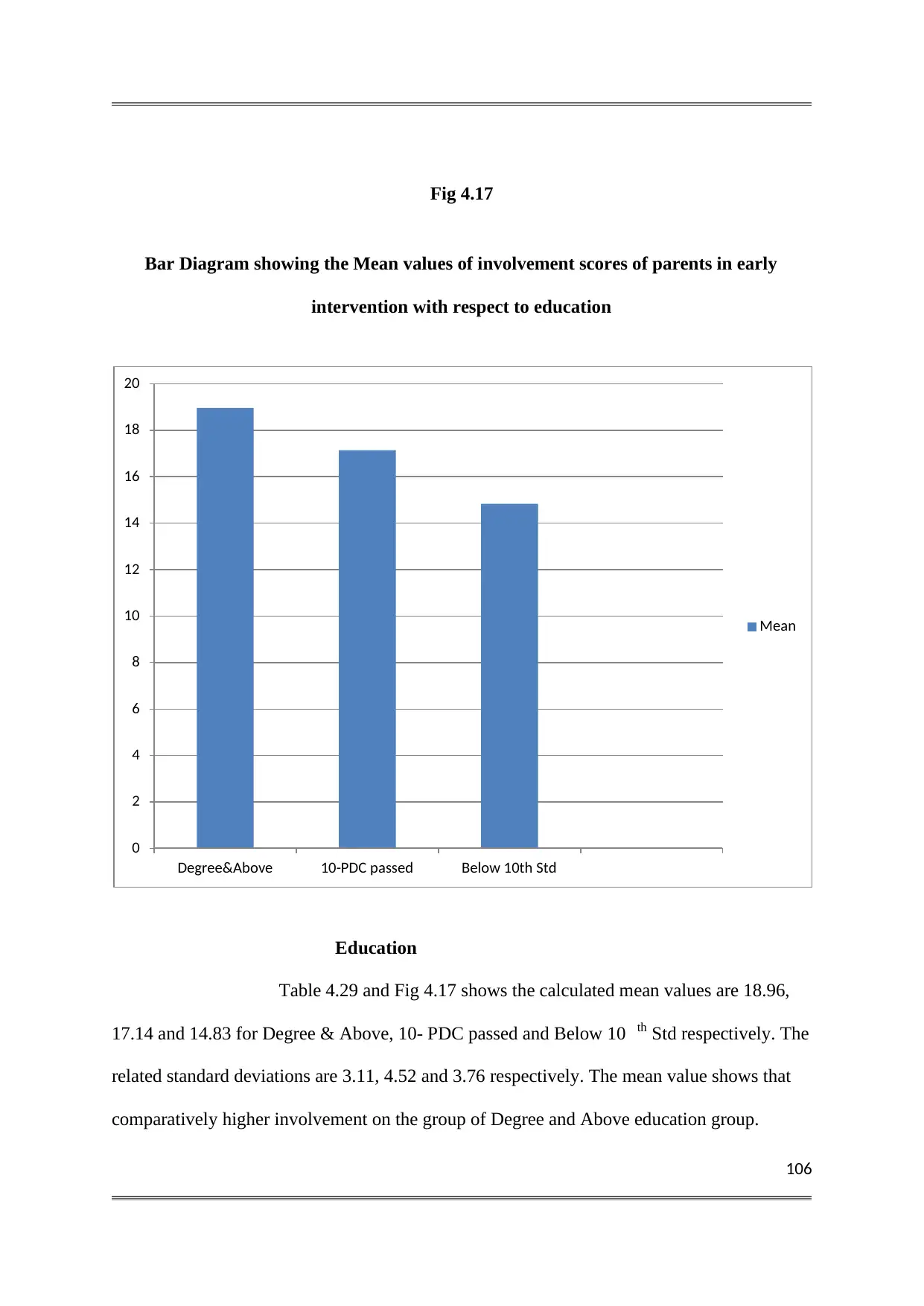
106
Fig 4.17
Bar Diagram showing the Mean values of involvement scores of parents in early
intervention with respect to education
Education
Table 4.29 and Fig 4.17 shows the calculated mean values are 18.96,
17.14 and 14.83 for Degree & Above, 10- PDC passed and Below 10 th Std respectively. The
related standard deviations are 3.11, 4.52 and 3.76 respectively. The mean value shows that
comparatively higher involvement on the group of Degree and Above education group.
0
2
4
6
8
10
12
14
16
18
20
Degree&Above 10-PDC passed Below 10th Std
Mean
Fig 4.17
Bar Diagram showing the Mean values of involvement scores of parents in early
intervention with respect to education
Education
Table 4.29 and Fig 4.17 shows the calculated mean values are 18.96,
17.14 and 14.83 for Degree & Above, 10- PDC passed and Below 10 th Std respectively. The
related standard deviations are 3.11, 4.52 and 3.76 respectively. The mean value shows that
comparatively higher involvement on the group of Degree and Above education group.
0
2
4
6
8
10
12
14
16
18
20
Degree&Above 10-PDC passed Below 10th Std
Mean
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
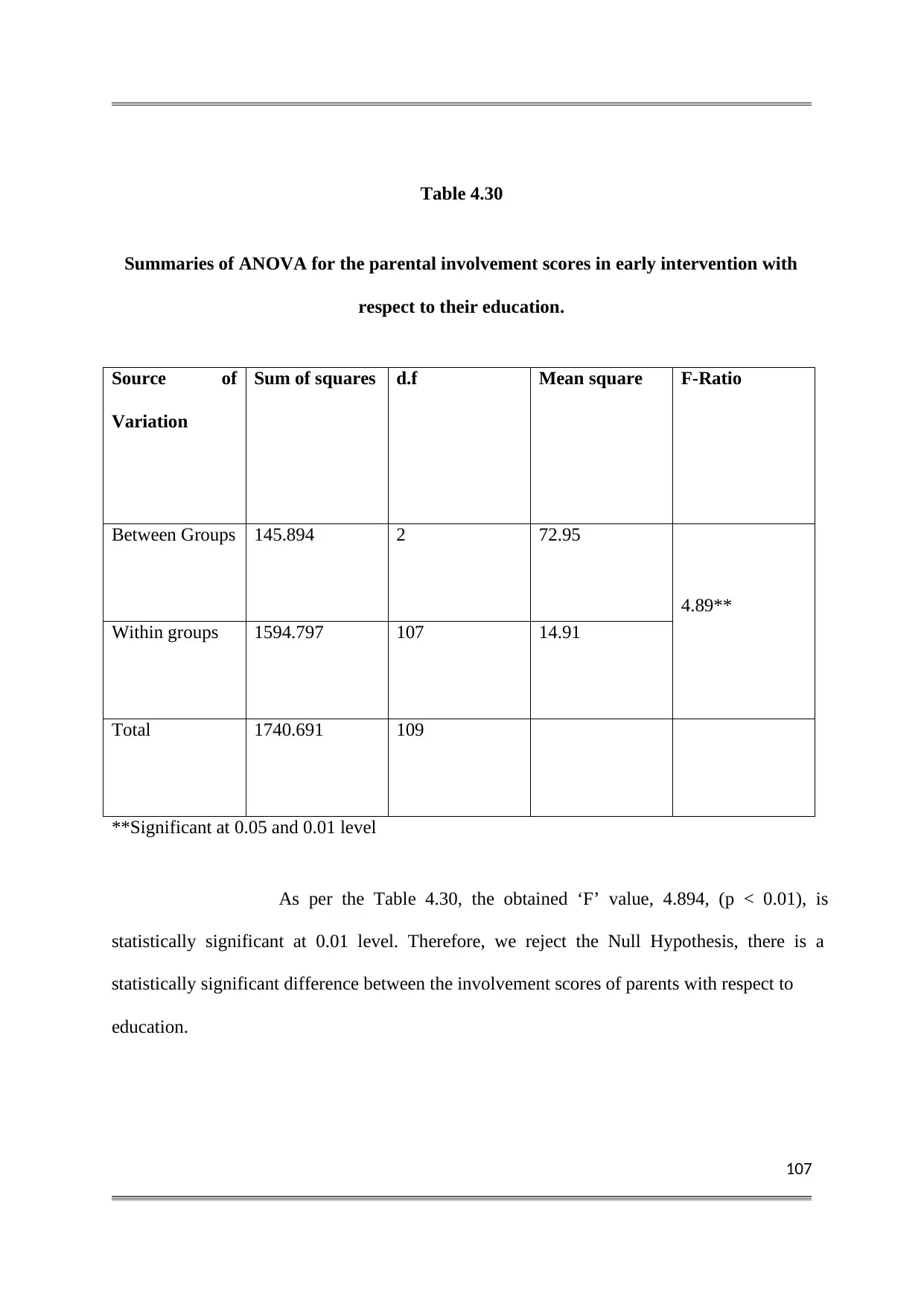
107
Table 4.30
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to their education.
Source of
Variation
Sum of squares d.f Mean square F-Ratio
Between Groups 145.894 2 72.95
4.89**
Within groups 1594.797 107 14.91
Total 1740.691 109
**Significant at 0.05 and 0.01 level
As per the Table 4.30, the obtained ‘F’ value, 4.894, (p < 0.01), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis, there is a
statistically significant difference between the involvement scores of parents with respect to
education.
Table 4.30
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to their education.
Source of
Variation
Sum of squares d.f Mean square F-Ratio
Between Groups 145.894 2 72.95
4.89**
Within groups 1594.797 107 14.91
Total 1740.691 109
**Significant at 0.05 and 0.01 level
As per the Table 4.30, the obtained ‘F’ value, 4.894, (p < 0.01), is
statistically significant at 0.01 level. Therefore, we reject the Null Hypothesis, there is a
statistically significant difference between the involvement scores of parents with respect to
education.
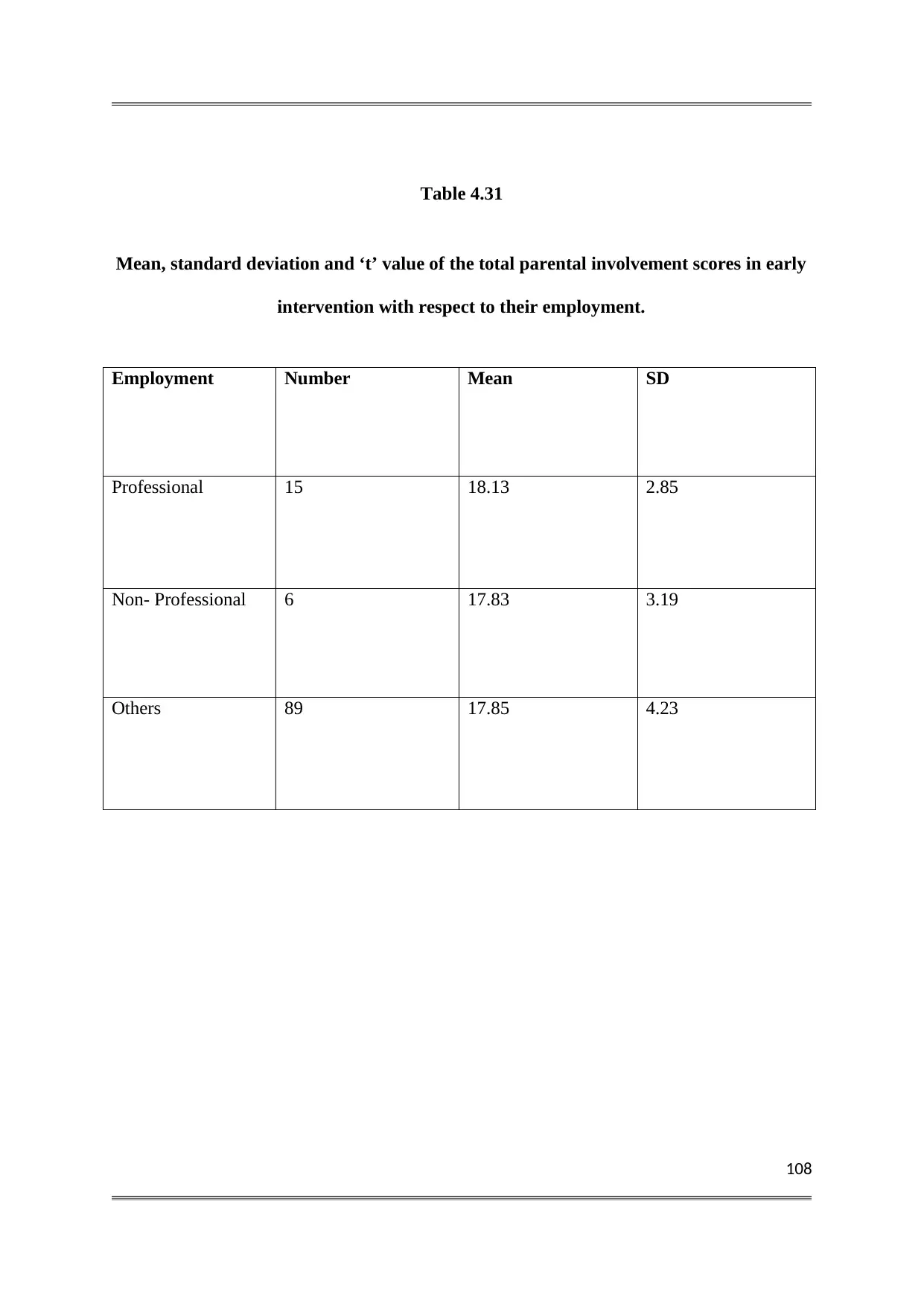
108
Table 4.31
Mean, standard deviation and ‘t’ value of the total parental involvement scores in early
intervention with respect to their employment.
Employment Number Mean SD
Professional 15 18.13 2.85
Non- Professional 6 17.83 3.19
Others 89 17.85 4.23
Table 4.31
Mean, standard deviation and ‘t’ value of the total parental involvement scores in early
intervention with respect to their employment.
Employment Number Mean SD
Professional 15 18.13 2.85
Non- Professional 6 17.83 3.19
Others 89 17.85 4.23
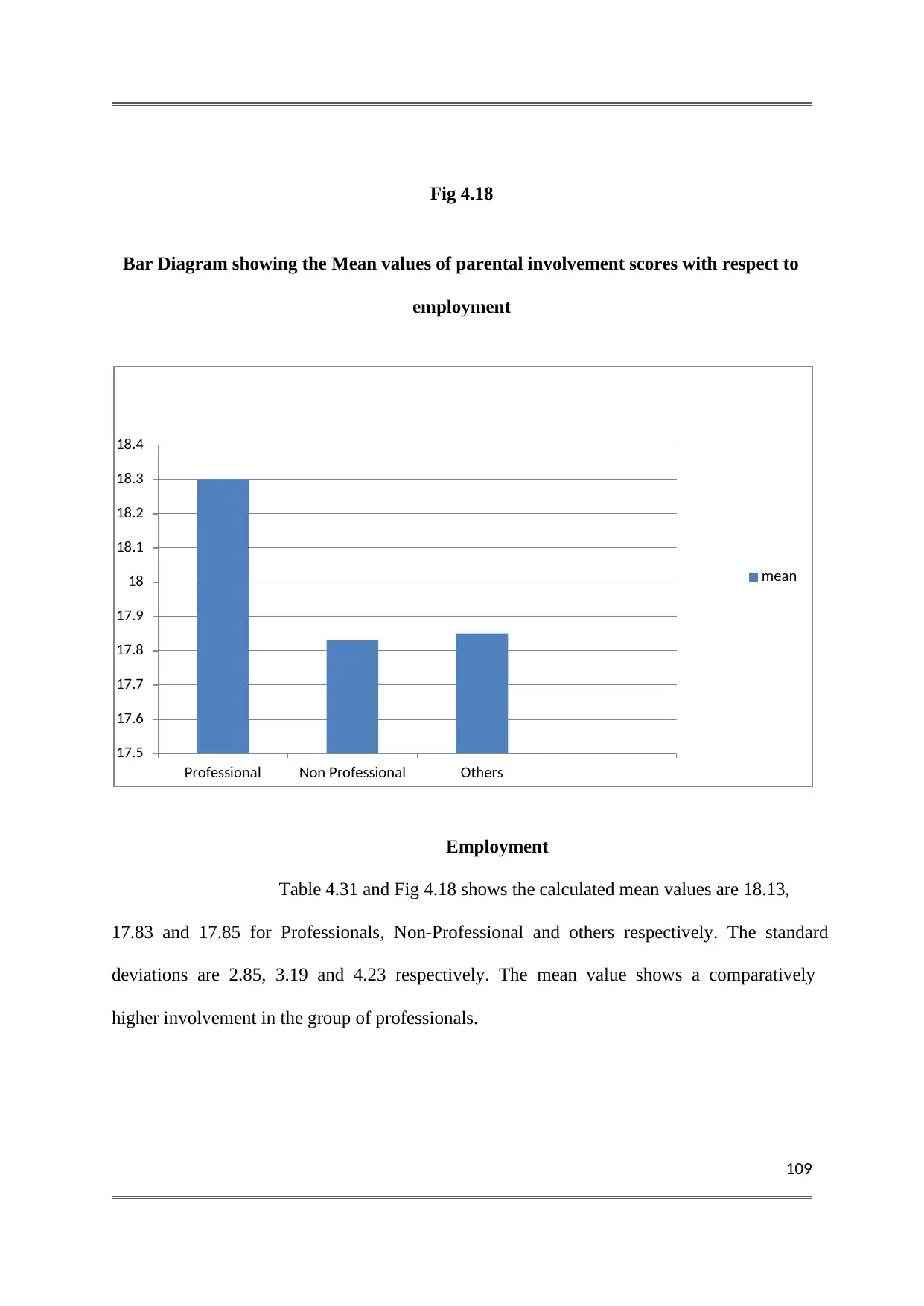
109
Fig 4.18
Bar Diagram showing the Mean values of parental involvement scores with respect to
employment
Employment
Table 4.31 and Fig 4.18 shows the calculated mean values are 18.13,
17.83 and 17.85 for Professionals, Non-Professional and others respectively. The standard
deviations are 2.85, 3.19 and 4.23 respectively. The mean value shows a comparatively
higher involvement in the group of professionals.
17.5
17.6
17.7
17.8
17.9
18
18.1
18.2
18.3
18.4
Professional Non Professional Others
mean
Fig 4.18
Bar Diagram showing the Mean values of parental involvement scores with respect to
employment
Employment
Table 4.31 and Fig 4.18 shows the calculated mean values are 18.13,
17.83 and 17.85 for Professionals, Non-Professional and others respectively. The standard
deviations are 2.85, 3.19 and 4.23 respectively. The mean value shows a comparatively
higher involvement in the group of professionals.
17.5
17.6
17.7
17.8
17.9
18
18.1
18.2
18.3
18.4
Professional Non Professional Others
mean
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
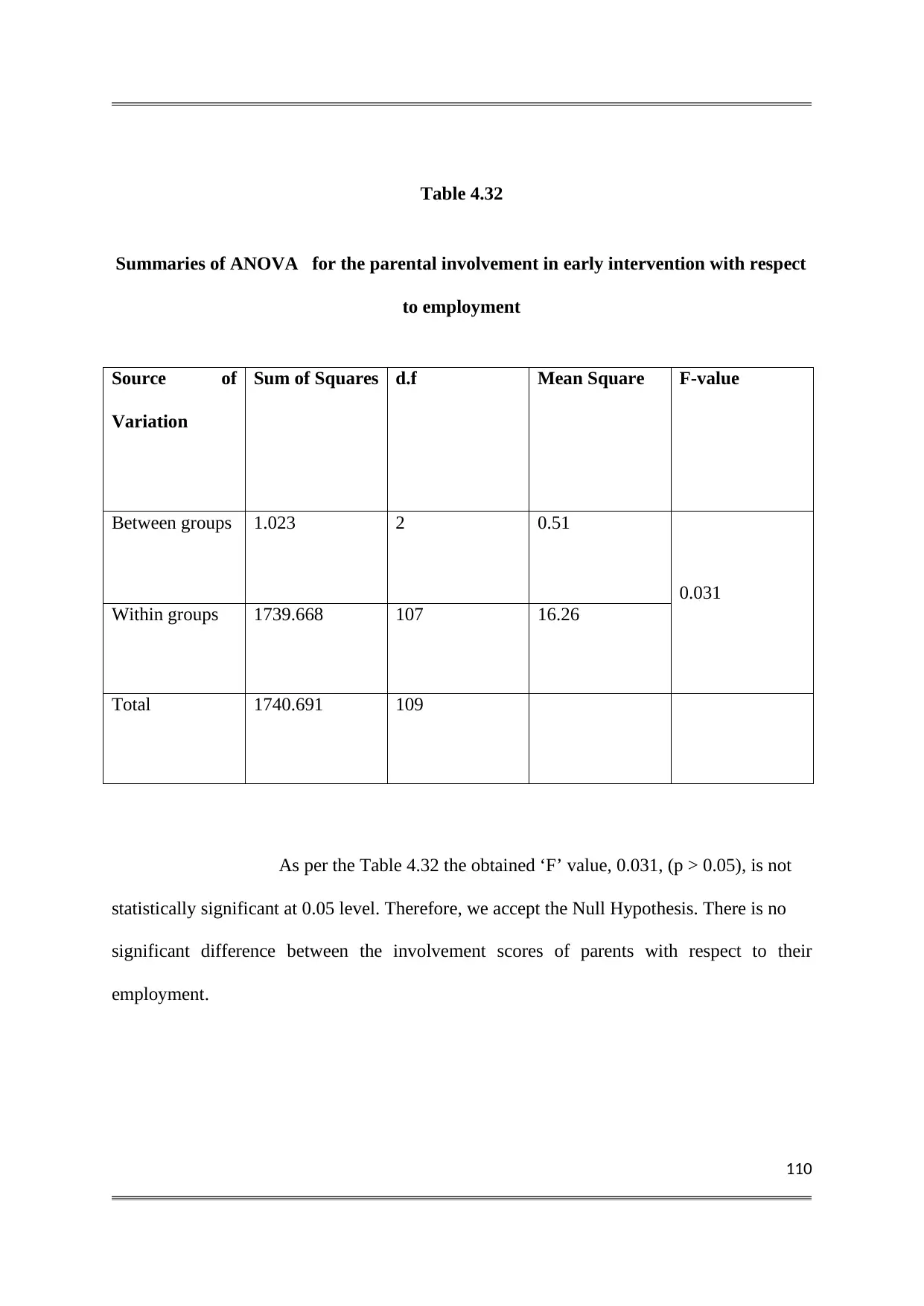
110
Table 4.32
Summaries of ANOVA for the parental involvement in early intervention with respect
to employment
Source of
Variation
Sum of Squares d.f Mean Square F-value
Between groups 1.023 2 0.51
0.031
Within groups 1739.668 107 16.26
Total 1740.691 109
As per the Table 4.32 the obtained ‘F’ value, 0.031, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their
employment.
Table 4.32
Summaries of ANOVA for the parental involvement in early intervention with respect
to employment
Source of
Variation
Sum of Squares d.f Mean Square F-value
Between groups 1.023 2 0.51
0.031
Within groups 1739.668 107 16.26
Total 1740.691 109
As per the Table 4.32 the obtained ‘F’ value, 0.031, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their
employment.
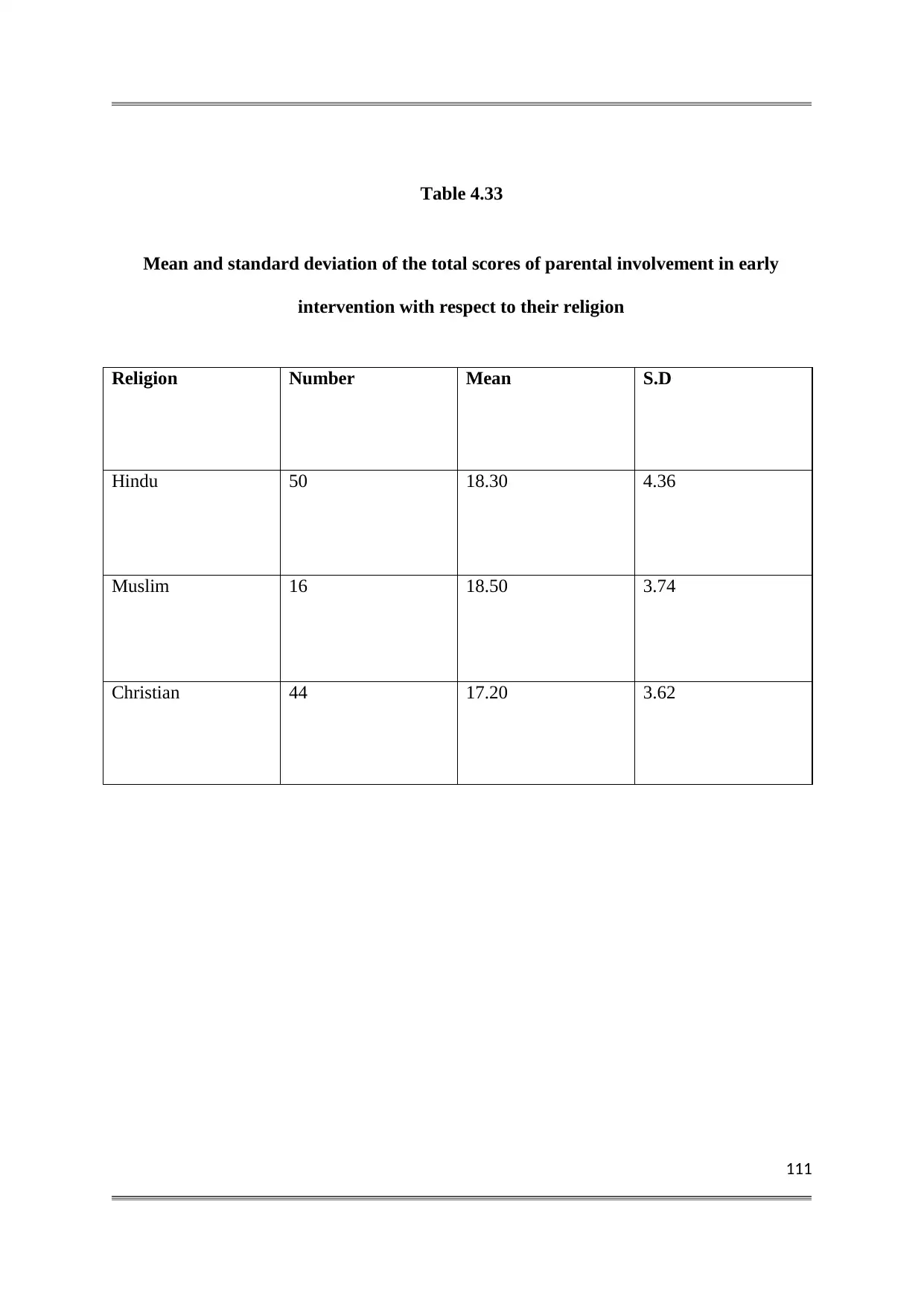
111
Table 4.33
Mean and standard deviation of the total scores of parental involvement in early
intervention with respect to their religion
Religion Number Mean S.D
Hindu 50 18.30 4.36
Muslim 16 18.50 3.74
Christian 44 17.20 3.62
Table 4.33
Mean and standard deviation of the total scores of parental involvement in early
intervention with respect to their religion
Religion Number Mean S.D
Hindu 50 18.30 4.36
Muslim 16 18.50 3.74
Christian 44 17.20 3.62
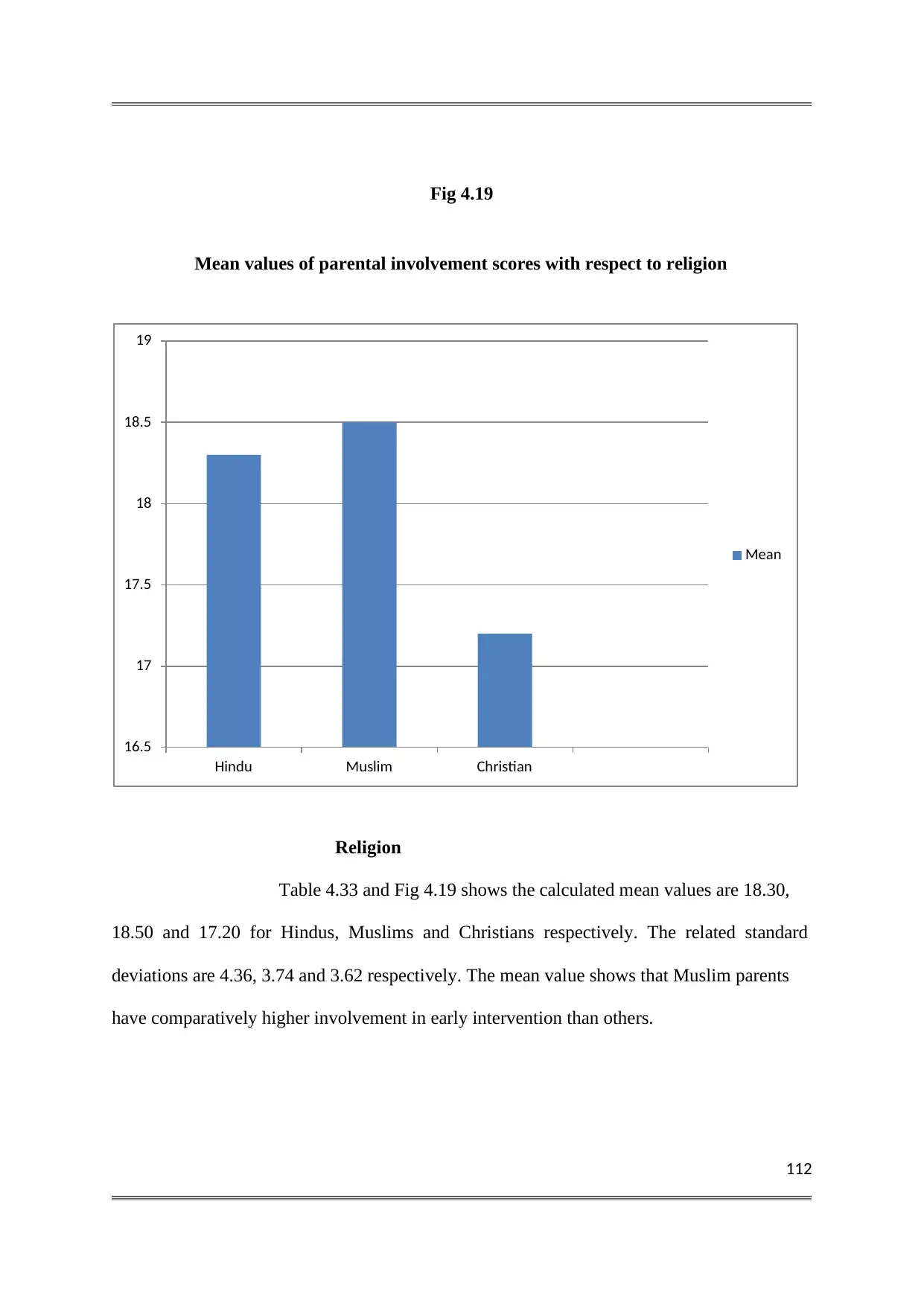
112
Fig 4.19
Mean values of parental involvement scores with respect to religion
Religion
Table 4.33 and Fig 4.19 shows the calculated mean values are 18.30,
18.50 and 17.20 for Hindus, Muslims and Christians respectively. The related standard
deviations are 4.36, 3.74 and 3.62 respectively. The mean value shows that Muslim parents
have comparatively higher involvement in early intervention than others.
16.5
17
17.5
18
18.5
19
Hindu Muslim Christian
Mean
Fig 4.19
Mean values of parental involvement scores with respect to religion
Religion
Table 4.33 and Fig 4.19 shows the calculated mean values are 18.30,
18.50 and 17.20 for Hindus, Muslims and Christians respectively. The related standard
deviations are 4.36, 3.74 and 3.62 respectively. The mean value shows that Muslim parents
have comparatively higher involvement in early intervention than others.
16.5
17
17.5
18
18.5
19
Hindu Muslim Christian
Mean
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
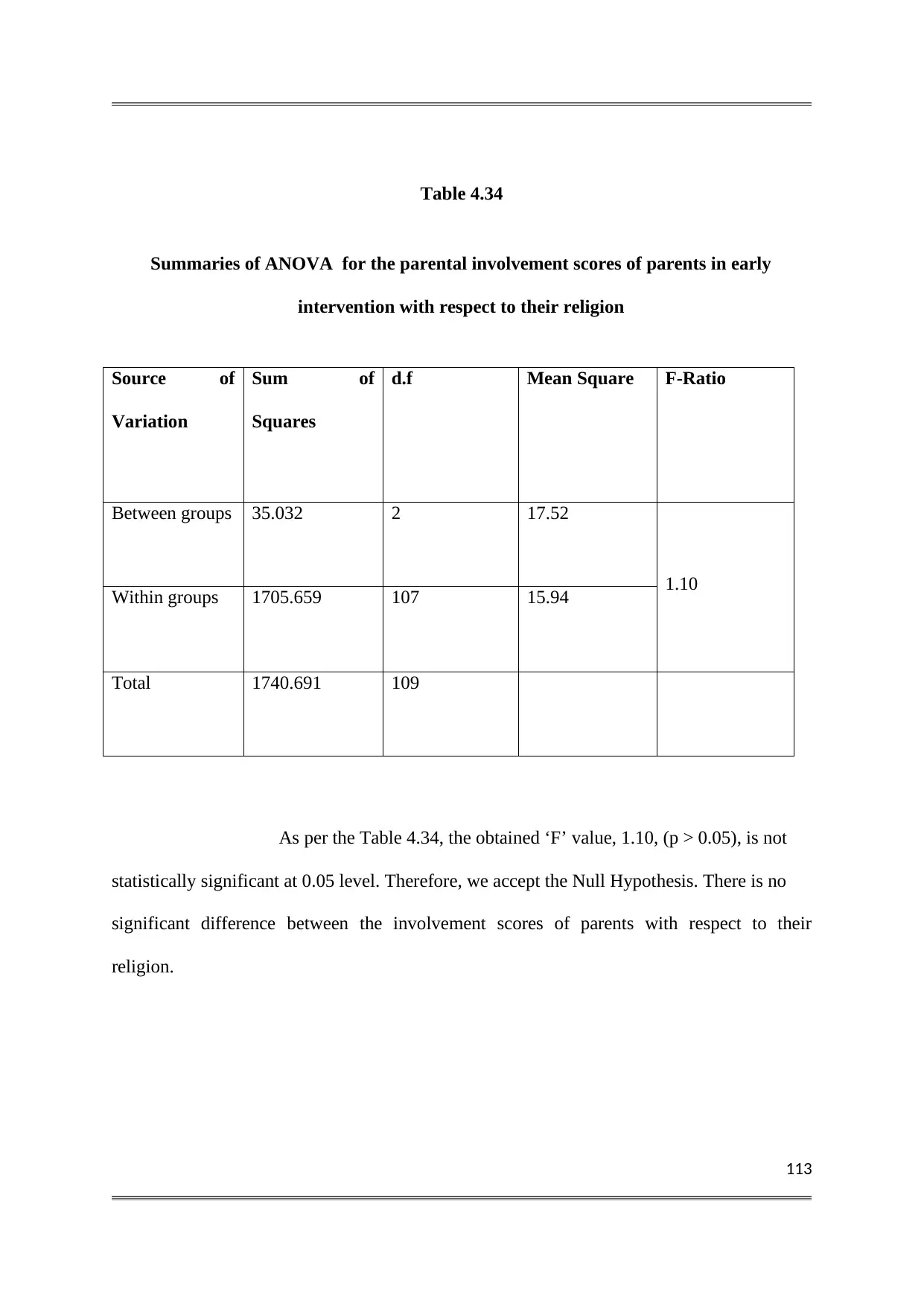
113
Table 4.34
Summaries of ANOVA for the parental involvement scores of parents in early
intervention with respect to their religion
Source of
Variation
Sum of
Squares
d.f Mean Square F-Ratio
Between groups 35.032 2 17.52
1.10
Within groups 1705.659 107 15.94
Total 1740.691 109
As per the Table 4.34, the obtained ‘F’ value, 1.10, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their
religion.
Table 4.34
Summaries of ANOVA for the parental involvement scores of parents in early
intervention with respect to their religion
Source of
Variation
Sum of
Squares
d.f Mean Square F-Ratio
Between groups 35.032 2 17.52
1.10
Within groups 1705.659 107 15.94
Total 1740.691 109
As per the Table 4.34, the obtained ‘F’ value, 1.10, (p > 0.05), is not
statistically significant at 0.05 level. Therefore, we accept the Null Hypothesis. There is no
significant difference between the involvement scores of parents with respect to their
religion.
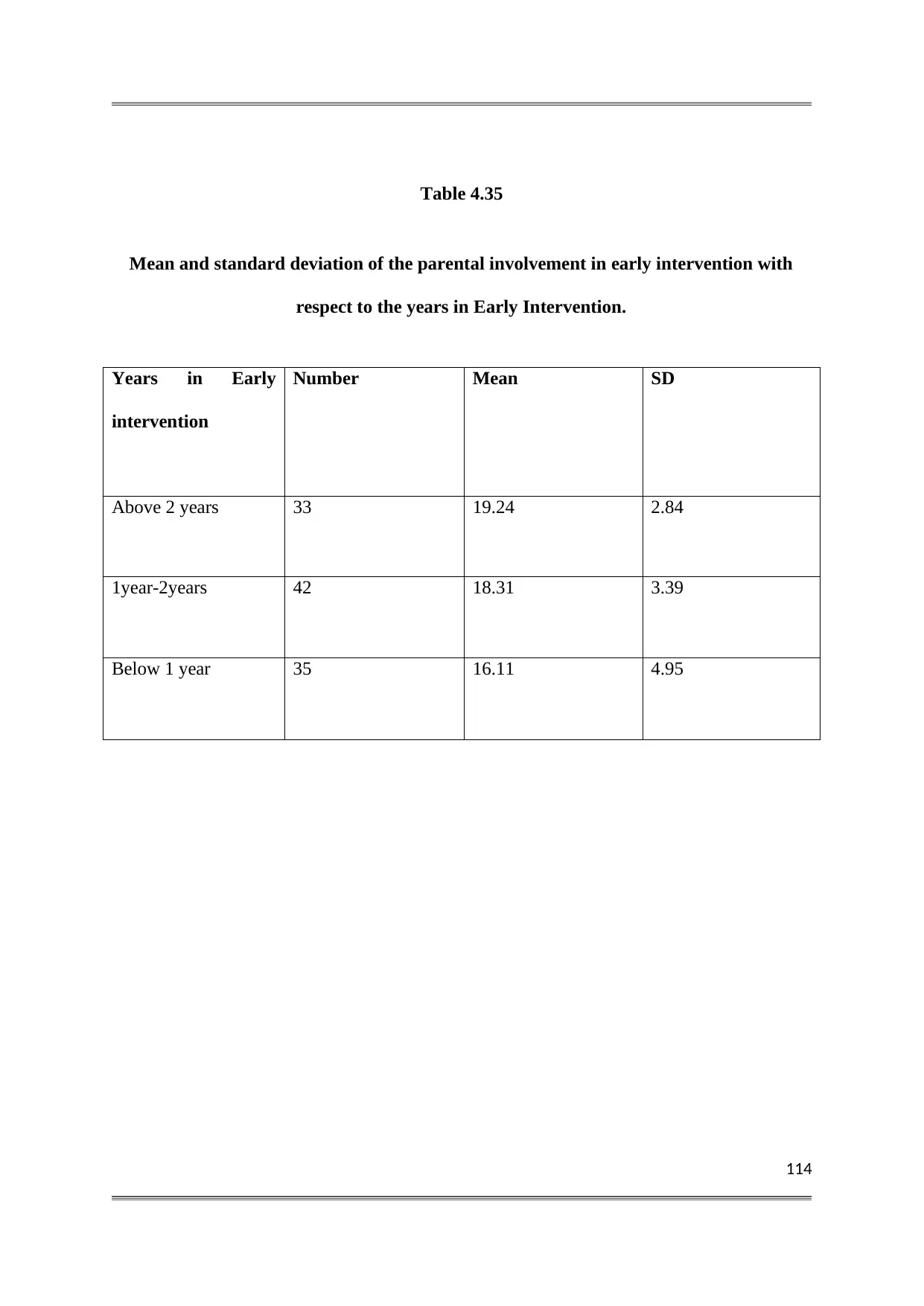
114
Table 4.35
Mean and standard deviation of the parental involvement in early intervention with
respect to the years in Early Intervention.
Years in Early
intervention
Number Mean SD
Above 2 years 33 19.24 2.84
1year-2years 42 18.31 3.39
Below 1 year 35 16.11 4.95
Table 4.35
Mean and standard deviation of the parental involvement in early intervention with
respect to the years in Early Intervention.
Years in Early
intervention
Number Mean SD
Above 2 years 33 19.24 2.84
1year-2years 42 18.31 3.39
Below 1 year 35 16.11 4.95
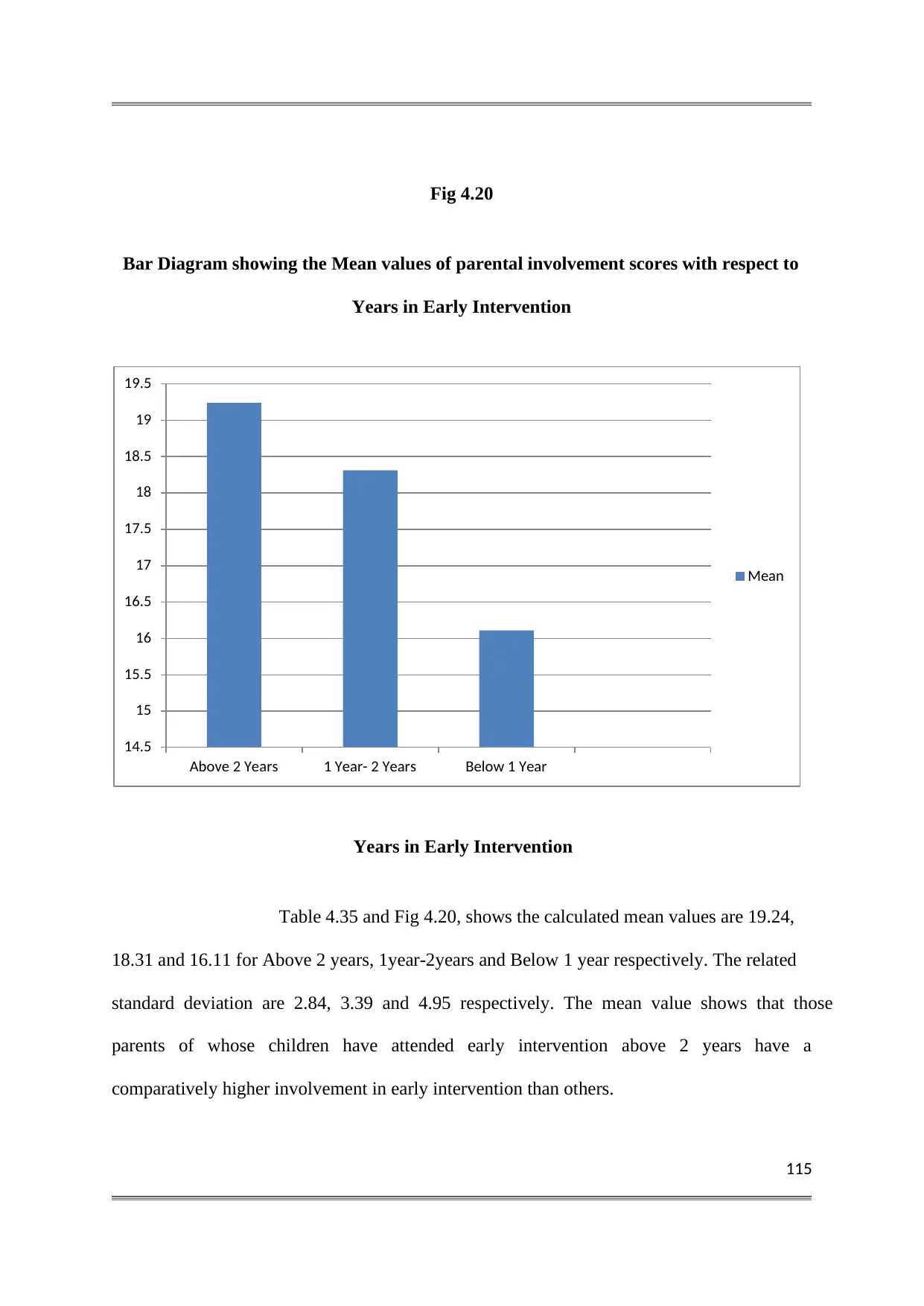
115
Fig 4.20
Bar Diagram showing the Mean values of parental involvement scores with respect to
Years in Early Intervention
Years in Early Intervention
Table 4.35 and Fig 4.20, shows the calculated mean values are 19.24,
18.31 and 16.11 for Above 2 years, 1year-2years and Below 1 year respectively. The related
standard deviation are 2.84, 3.39 and 4.95 respectively. The mean value shows that those
parents of whose children have attended early intervention above 2 years have a
comparatively higher involvement in early intervention than others.
14.5
15
15.5
16
16.5
17
17.5
18
18.5
19
19.5
Above 2 Years 1 Year- 2 Years Below 1 Year
Mean
Fig 4.20
Bar Diagram showing the Mean values of parental involvement scores with respect to
Years in Early Intervention
Years in Early Intervention
Table 4.35 and Fig 4.20, shows the calculated mean values are 19.24,
18.31 and 16.11 for Above 2 years, 1year-2years and Below 1 year respectively. The related
standard deviation are 2.84, 3.39 and 4.95 respectively. The mean value shows that those
parents of whose children have attended early intervention above 2 years have a
comparatively higher involvement in early intervention than others.
14.5
15
15.5
16
16.5
17
17.5
18
18.5
19
19.5
Above 2 Years 1 Year- 2 Years Below 1 Year
Mean
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
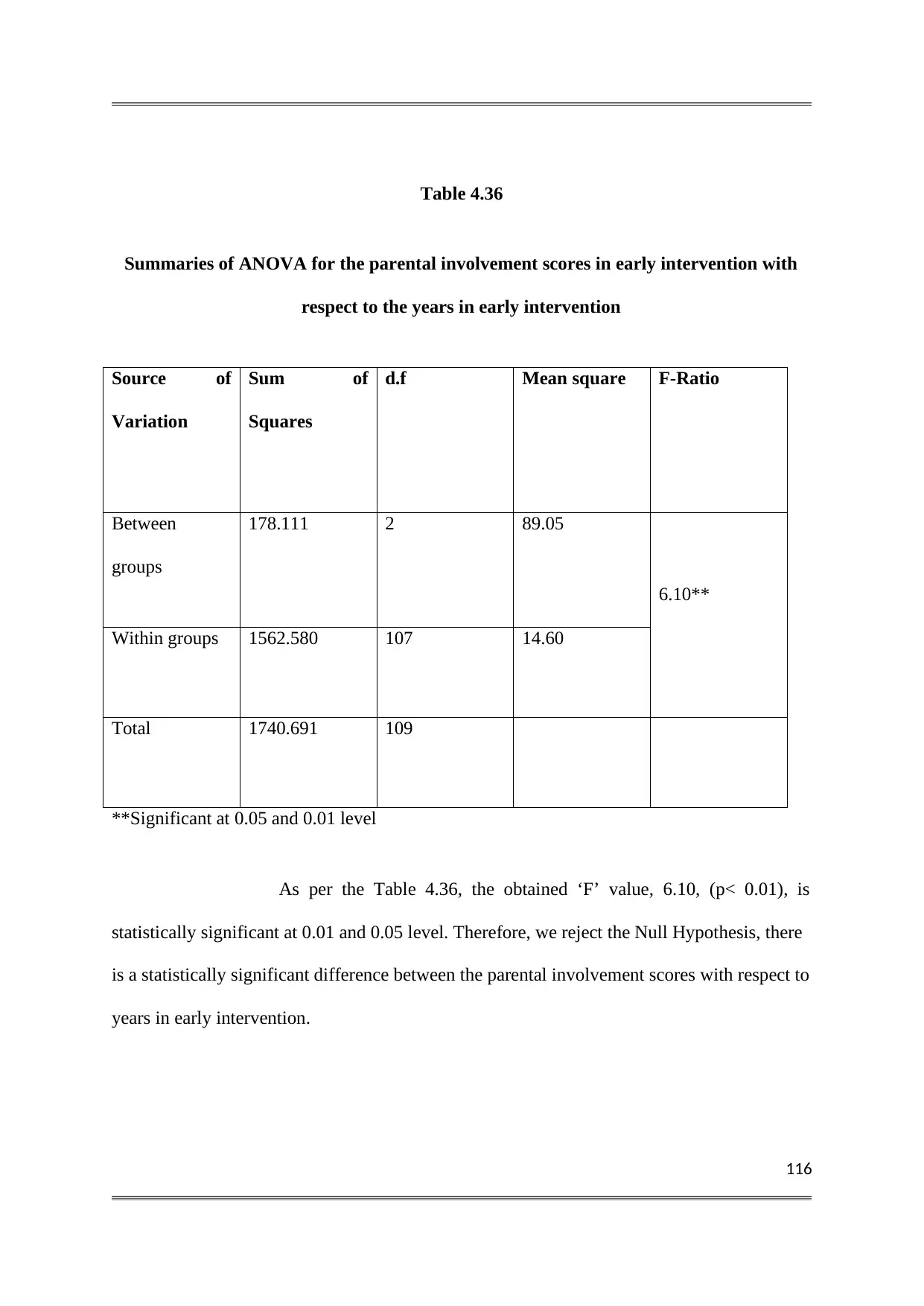
116
Table 4.36
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to the years in early intervention
Source of
Variation
Sum of
Squares
d.f Mean square F-Ratio
Between
groups
178.111 2 89.05
6.10**
Within groups 1562.580 107 14.60
Total 1740.691 109
**Significant at 0.05 and 0.01 level
As per the Table 4.36, the obtained ‘F’ value, 6.10, (p< 0.01), is
statistically significant at 0.01 and 0.05 level. Therefore, we reject the Null Hypothesis, there
is a statistically significant difference between the parental involvement scores with respect to
years in early intervention.
Table 4.36
Summaries of ANOVA for the parental involvement scores in early intervention with
respect to the years in early intervention
Source of
Variation
Sum of
Squares
d.f Mean square F-Ratio
Between
groups
178.111 2 89.05
6.10**
Within groups 1562.580 107 14.60
Total 1740.691 109
**Significant at 0.05 and 0.01 level
As per the Table 4.36, the obtained ‘F’ value, 6.10, (p< 0.01), is
statistically significant at 0.01 and 0.05 level. Therefore, we reject the Null Hypothesis, there
is a statistically significant difference between the parental involvement scores with respect to
years in early intervention.
117
SUMMARY, CONCLUSION AND SUGGESTIONS
The study in Retrospect
The present study has been designed to investigate the different aspects
of parental awareness in Early Intervention of Children with Developmental Disabilities. This
study was also expected to explore the parental involvement in Early Intervention. This
chapter contains a brief summary of the study, followed by the major findings and
conclusions arrived at, as well as the implications of the findings, suggestions based on the
findings and the suggestions for further research.
5.1 OBJECTIVES OF THE STUDY
General Objective
To find out the level of awareness and involvement of parents in Early Intervention of
children with developmental disabilities.
Specific Objectives
1. To find out the level of awareness of parents on the importance of Early Intervention.
2. To find out the level of awareness of parents on the importance of parental involvement in
Early Intervention.
3. To find out the level of awareness of parents regarding the nature of population requiring
early intervention services.
4. To find out the level of awareness of parents regarding the Early Intervention services.
SUMMARY, CONCLUSION AND SUGGESTIONS
The study in Retrospect
The present study has been designed to investigate the different aspects
of parental awareness in Early Intervention of Children with Developmental Disabilities. This
study was also expected to explore the parental involvement in Early Intervention. This
chapter contains a brief summary of the study, followed by the major findings and
conclusions arrived at, as well as the implications of the findings, suggestions based on the
findings and the suggestions for further research.
5.1 OBJECTIVES OF THE STUDY
General Objective
To find out the level of awareness and involvement of parents in Early Intervention of
children with developmental disabilities.
Specific Objectives
1. To find out the level of awareness of parents on the importance of Early Intervention.
2. To find out the level of awareness of parents on the importance of parental involvement in
Early Intervention.
3. To find out the level of awareness of parents regarding the nature of population requiring
early intervention services.
4. To find out the level of awareness of parents regarding the Early Intervention services.
118
5. To find out the level of awareness of parents on Early Intervention with respect to Socio
Demographic Variables.
6. To find out the level of involvement of parents in their child’s Early Intervention Program.
7. To find out the level of involvement of parents with respect to certain socio-demographic
variables.
5.2 HYPOTHESIS
On the basis of the objectives of the study the researcher developed the following
hypothesis.
There is no significant difference in the parental awareness with respect to selected Socio-
demographic variables- such as the age, sex, locality, educational qualification,
occupation, economic status and duration of receiving Early Intervention services.
There is no significant difference in the parental involvement with respect to selected
Socio demographic variables- Such as the age, sex, locality, educational qualification,
socio-economic status, employment.
5.3 METHODOLOGY IN BRIEF
The descriptive survey method was adopted as the method research.
The sample for the present study consists of parents of 110 children with developmental
disabilities receiving early intervention services from various early intervention centres
located in Ernakulam and Kottayam districts of Kerala state. Three different tools were
5. To find out the level of awareness of parents on Early Intervention with respect to Socio
Demographic Variables.
6. To find out the level of involvement of parents in their child’s Early Intervention Program.
7. To find out the level of involvement of parents with respect to certain socio-demographic
variables.
5.2 HYPOTHESIS
On the basis of the objectives of the study the researcher developed the following
hypothesis.
There is no significant difference in the parental awareness with respect to selected Socio-
demographic variables- such as the age, sex, locality, educational qualification,
occupation, economic status and duration of receiving Early Intervention services.
There is no significant difference in the parental involvement with respect to selected
Socio demographic variables- Such as the age, sex, locality, educational qualification,
socio-economic status, employment.
5.3 METHODOLOGY IN BRIEF
The descriptive survey method was adopted as the method research.
The sample for the present study consists of parents of 110 children with developmental
disabilities receiving early intervention services from various early intervention centres
located in Ernakulam and Kottayam districts of Kerala state. Three different tools were
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
119
used for the collection of data. They are: (1) General Data Sheet, (2) Awareness
Inventory, (3) Parental Involvement Scale.
The data collected using these tools were analysed using the following statistical techniques:
1) Computation of frequencies and percentages.
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of ‘t’ value to test the significance of difference between the means of two
groups of data.
5.4 MAJOR FINDINGS
The major findings that have emerged from the study are given below under separate heads.
1.1. Percentage-wise and Level-wise Analysis of Parental Awareness on Early
Interventionof Children with Developmental Disabilities.
a) Percentage-wise Analysis
The Parental awareness on Early Intervention in general was found to
be high (74.17%). The highest percentage of parental awareness was found to be in the
importance of parental involvement in early intervention (84.9%), followed by importance of
Early Intervention (76.44%) and early intervention services (74.15%) and the lowest
percentage of parental awareness was found to be on developmental disabilities (67.48%).
b) Level-wise Analysis
In general the majority of parents (77.3%) were found to be in the
‘High Awareness group’ and 22.7% of the parents belong to the average awareness group,
and none of the parents belong to the low awareness group.
used for the collection of data. They are: (1) General Data Sheet, (2) Awareness
Inventory, (3) Parental Involvement Scale.
The data collected using these tools were analysed using the following statistical techniques:
1) Computation of frequencies and percentages.
2) Computation of arithmetic Mean, Median, Mode, Standard Deviation, Skewness and
Kurtosis.
3) Computation of ‘t’ value to test the significance of difference between the means of two
groups of data.
5.4 MAJOR FINDINGS
The major findings that have emerged from the study are given below under separate heads.
1.1. Percentage-wise and Level-wise Analysis of Parental Awareness on Early
Interventionof Children with Developmental Disabilities.
a) Percentage-wise Analysis
The Parental awareness on Early Intervention in general was found to
be high (74.17%). The highest percentage of parental awareness was found to be in the
importance of parental involvement in early intervention (84.9%), followed by importance of
Early Intervention (76.44%) and early intervention services (74.15%) and the lowest
percentage of parental awareness was found to be on developmental disabilities (67.48%).
b) Level-wise Analysis
In general the majority of parents (77.3%) were found to be in the
‘High Awareness group’ and 22.7% of the parents belong to the average awareness group,
and none of the parents belong to the low awareness group.
120
In Importance of early intervention, it was found that 75.5% of the
parents belong to the high awareness group, 24.5% of the parents belong to the average group
and none of the parents belong to the low awareness group.
In Importance of Parental involvement in Early Intervention, it was
found that 90.9% of the parents belong to the high awareness group, 9.1% of the parents
belong to the average group and none of the parents belong to low awareness group.
In Developmental disabilities, it was found that 44.5% of the parents
belong to the high awareness group, 55.5% of the parents belonged to average awareness
group and none of the parents belong to the low awareness group.
In Early Intervention Services, it was found that 70% of the parents
belong to the high awareness group, 29.1% of the parents belong to the average awareness
group and 0.9% of the parents belong to the low awareness group respectively.
1.2 Percentage-Wise and Level-wise Analysis of Parental Involvement in
EarlyIntervention
a) Percentage-wise Analysis
The Involvement of parents in Early Intervention was found to be high (81.32%).
b) Level-wise Analysis
The majority of parents (81.8%) were found to be in the high involvement group and 17.3%
of the parents belong to the average involvement group and 0.9% of the parents belong to the
low involvement group.
In Importance of early intervention, it was found that 75.5% of the
parents belong to the high awareness group, 24.5% of the parents belong to the average group
and none of the parents belong to the low awareness group.
In Importance of Parental involvement in Early Intervention, it was
found that 90.9% of the parents belong to the high awareness group, 9.1% of the parents
belong to the average group and none of the parents belong to low awareness group.
In Developmental disabilities, it was found that 44.5% of the parents
belong to the high awareness group, 55.5% of the parents belonged to average awareness
group and none of the parents belong to the low awareness group.
In Early Intervention Services, it was found that 70% of the parents
belong to the high awareness group, 29.1% of the parents belong to the average awareness
group and 0.9% of the parents belong to the low awareness group respectively.
1.2 Percentage-Wise and Level-wise Analysis of Parental Involvement in
EarlyIntervention
a) Percentage-wise Analysis
The Involvement of parents in Early Intervention was found to be high (81.32%).
b) Level-wise Analysis
The majority of parents (81.8%) were found to be in the high involvement group and 17.3%
of the parents belong to the average involvement group and 0.9% of the parents belong to the
low involvement group.
121
2.1 Parental Awareness with respect to Certain Child Related and Parent Related
Variables
Education of Parents was found to be a significant factor in the parental awareness in Early
Intervention (F=7.804, p< 0.01)
Years spent in Early Intervention was found to be a significant factor in the parental
awareness in Early Intervention (F=5.215, p< 0.01)
The age of parents was found to be not significant factor in the parental awareness in Early
Intervention (F=0.10, p> 0.05)
The locality of parents was found to be not a significant factor in the parental awareness in
Early Intervention (t= 1.93, p > 0.05)
Sex of parents was found to be not a significant factor in the parental awareness in Early
Intervention (t= -1.31, p > 0.056)
Employment of parents was found to be not a significant factor in the parental awareness in
Early Intervention (F= 0.328, p > 0.05)
The religion of parents was found to be not a significant factor in the parental awareness in
Early Intervention (F= 0.169, p > 0.05)
2.2. Parental Involvement with respect to Certain Child Related and Parent Related
Variables.
Education of Parents was found to be a significant factor in the parental Involvement in Early
Intervention (F=4.894, p< 0.01)
Years spent in Early Intervention was found to be a significant factor in the parental
Involvement in Early Intervention (F=6.10, p< 0.01)
2.1 Parental Awareness with respect to Certain Child Related and Parent Related
Variables
Education of Parents was found to be a significant factor in the parental awareness in Early
Intervention (F=7.804, p< 0.01)
Years spent in Early Intervention was found to be a significant factor in the parental
awareness in Early Intervention (F=5.215, p< 0.01)
The age of parents was found to be not significant factor in the parental awareness in Early
Intervention (F=0.10, p> 0.05)
The locality of parents was found to be not a significant factor in the parental awareness in
Early Intervention (t= 1.93, p > 0.05)
Sex of parents was found to be not a significant factor in the parental awareness in Early
Intervention (t= -1.31, p > 0.056)
Employment of parents was found to be not a significant factor in the parental awareness in
Early Intervention (F= 0.328, p > 0.05)
The religion of parents was found to be not a significant factor in the parental awareness in
Early Intervention (F= 0.169, p > 0.05)
2.2. Parental Involvement with respect to Certain Child Related and Parent Related
Variables.
Education of Parents was found to be a significant factor in the parental Involvement in Early
Intervention (F=4.894, p< 0.01)
Years spent in Early Intervention was found to be a significant factor in the parental
Involvement in Early Intervention (F=6.10, p< 0.01)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
122
The age of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (F=0.465, p> 0.05)
The locality of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (t= 1.36, p > 0.05)
Sex of parents was found to be not a significant factor in the parental Involvement in Early
Intervention (t= -1.29, p > 0.05)
Employment of parents was found to be not a significant factor in the parental involvement in
Early Intervention (F= 0.031, p > 0.05)
The religion of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (F= 1.10, p > 0.05)
5.5 CONCLUSION, IMPLICATIONS AND SUGGESTION
The major conclusions that are arrived at from the present investigation are given below:
The present study revealed that the parental awareness on Early
Intervention was found to be high, the highest percentage of parental awareness was found to
be in the importance of parental involvement in early intervention, followed by importance of
Early Intervention, early intervention services and an average awareness was found to be on
developmental disabilities. The Parental Involvement in Early intervention was also found to
be high.
The Education of parents was found to be a significant factor in the
parental awareness and involvement in Early Intervention. Parents with Degree and above
education were found to have the highest awareness and involvement in Early Intervention.
The age of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (F=0.465, p> 0.05)
The locality of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (t= 1.36, p > 0.05)
Sex of parents was found to be not a significant factor in the parental Involvement in Early
Intervention (t= -1.29, p > 0.05)
Employment of parents was found to be not a significant factor in the parental involvement in
Early Intervention (F= 0.031, p > 0.05)
The religion of parents was found to be not a significant factor in the parental Involvement in
Early Intervention (F= 1.10, p > 0.05)
5.5 CONCLUSION, IMPLICATIONS AND SUGGESTION
The major conclusions that are arrived at from the present investigation are given below:
The present study revealed that the parental awareness on Early
Intervention was found to be high, the highest percentage of parental awareness was found to
be in the importance of parental involvement in early intervention, followed by importance of
Early Intervention, early intervention services and an average awareness was found to be on
developmental disabilities. The Parental Involvement in Early intervention was also found to
be high.
The Education of parents was found to be a significant factor in the
parental awareness and involvement in Early Intervention. Parents with Degree and above
education were found to have the highest awareness and involvement in Early Intervention.
123
The Years in Early intervention was found to be a significant factor in
the parental awareness and involvement in early intervention. Parents of children who have
received early intervention services for two years and above were found to have the highest
awareness and involvement in Early Intervention.
Sex of parents was found to be not a significant factor in the parental
awareness and involvement in early intervention. But comparatively, mothers have higher
awareness and involvement in early intervention than fathers.
Age of the parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. Comparatively highest awareness
was found to be in 46-55 years age group. And highest involvement was found to be in 20-32
years age group.
Locality of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively higher
awareness and involvement in early intervention was found to be parents from urban areas.
Employment of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively highest
awareness and involvement was among the professional parents.
Religion of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively highest
awareness and involvement was found to be in Muslim Parents.
The Years in Early intervention was found to be a significant factor in
the parental awareness and involvement in early intervention. Parents of children who have
received early intervention services for two years and above were found to have the highest
awareness and involvement in Early Intervention.
Sex of parents was found to be not a significant factor in the parental
awareness and involvement in early intervention. But comparatively, mothers have higher
awareness and involvement in early intervention than fathers.
Age of the parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. Comparatively highest awareness
was found to be in 46-55 years age group. And highest involvement was found to be in 20-32
years age group.
Locality of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively higher
awareness and involvement in early intervention was found to be parents from urban areas.
Employment of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively highest
awareness and involvement was among the professional parents.
Religion of parents was found to be not a significant factor in the
parental awareness and involvement in early intervention. But comparatively highest
awareness and involvement was found to be in Muslim Parents.
124
Findings of the study have some implications in the early intervention of children with
developmental disabilities.
Family/Parents forms an integral part of the child’s environment and therefore the
focus of any intervention should be involvement of the family. The high awareness of
parents on early intervention can be utilized for enhancing the involvement of parents
as team members through parent training programmes and family strengthening and
empowering programmes organized by the early intervention centres.
.Parent consultation model of early intervention can be adopted by those parents who
possess high awareness and involvement in early intervention. In this model, parents
take consultation from professionals but carry out the program at home.
Parent centred model of early intervention, where professionals work with parents can
be adopted to produce effective and long lasting changes in their children with
Developmental disabilities. This model of EI is more applicable to mothers who are
home-makers.
Parents with high awareness and involvement in early intervention and who have
found positive results in their children through early intervention, can motivate the
other parents who are stressed and anxious about their child’s developmental delay.
On the basis of the above conclusions, the following suggestions are given.
Medical camps with facilities for early identification, and screening of disabilities
should be organized in places such as schools, churches, community centres etc.
Findings of the study have some implications in the early intervention of children with
developmental disabilities.
Family/Parents forms an integral part of the child’s environment and therefore the
focus of any intervention should be involvement of the family. The high awareness of
parents on early intervention can be utilized for enhancing the involvement of parents
as team members through parent training programmes and family strengthening and
empowering programmes organized by the early intervention centres.
.Parent consultation model of early intervention can be adopted by those parents who
possess high awareness and involvement in early intervention. In this model, parents
take consultation from professionals but carry out the program at home.
Parent centred model of early intervention, where professionals work with parents can
be adopted to produce effective and long lasting changes in their children with
Developmental disabilities. This model of EI is more applicable to mothers who are
home-makers.
Parents with high awareness and involvement in early intervention and who have
found positive results in their children through early intervention, can motivate the
other parents who are stressed and anxious about their child’s developmental delay.
On the basis of the above conclusions, the following suggestions are given.
Medical camps with facilities for early identification, and screening of disabilities
should be organized in places such as schools, churches, community centres etc.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
125
Measures should be taken by the government to ensure availability of early
intervention services to all the sections of the society.
A network of parents having children with developmental disabilities should be
formed so as to help each other on matters regarding education, training, intervention,
parent training programmes etc.
Information materials such as pamphlets, books, guidelines for parents and posters
need to be made available at all the early intervention centres.
There should also be a provision for the visit of therapist and interventionist to the
homes of developmentally disabled infants and thereby helping parents in the home –
based early intervention.
Issues like transportation, lack of awareness, financial and other constraints pose a
hurdle in delivering Early Intervention services. Therefore, establishing Early
intervention Centres all over the country will ensure that services are available at the
doorsteps for a wider population.
The level of involvement of fathers in early intervention should be enhanced so that
both parents can work together towards the optimum development of their child.
5.6. SUGGESTIONS FOR FURTHER STUDY
In the light of the finding that have emerged from the present study and the valuable
experience gained by conducting the investigation, the following topic are suggested for
further study.
Measures should be taken by the government to ensure availability of early
intervention services to all the sections of the society.
A network of parents having children with developmental disabilities should be
formed so as to help each other on matters regarding education, training, intervention,
parent training programmes etc.
Information materials such as pamphlets, books, guidelines for parents and posters
need to be made available at all the early intervention centres.
There should also be a provision for the visit of therapist and interventionist to the
homes of developmentally disabled infants and thereby helping parents in the home –
based early intervention.
Issues like transportation, lack of awareness, financial and other constraints pose a
hurdle in delivering Early Intervention services. Therefore, establishing Early
intervention Centres all over the country will ensure that services are available at the
doorsteps for a wider population.
The level of involvement of fathers in early intervention should be enhanced so that
both parents can work together towards the optimum development of their child.
5.6. SUGGESTIONS FOR FURTHER STUDY
In the light of the finding that have emerged from the present study and the valuable
experience gained by conducting the investigation, the following topic are suggested for
further study.
126
(a) The present study was conducted on sample of parents of 110 developmentally disabled
children selected from two districts of Kerala. The same study may be conducted with a
larger sample drawn from all districts of the state, so that more generalizable findings could
be obtained
(b) Studies may be conducted to find out the factors influencing the parental awareness and
involvement in early intervention.
(c) A study may be conducted to find out the impact of early intervention centres on the
families of children with developmental disabilities.
(d) A study may be conducted to find out the benefits of parental involvement in early
intervention.
(e) Parental perception on early intervention services for their children with developmental
disabilities may be studied.
(f) A further study can be conducted to understand the role of early intervention centres in
reducing the stress of parents of children with developmental disabilities.
(a) The present study was conducted on sample of parents of 110 developmentally disabled
children selected from two districts of Kerala. The same study may be conducted with a
larger sample drawn from all districts of the state, so that more generalizable findings could
be obtained
(b) Studies may be conducted to find out the factors influencing the parental awareness and
involvement in early intervention.
(c) A study may be conducted to find out the impact of early intervention centres on the
families of children with developmental disabilities.
(d) A study may be conducted to find out the benefits of parental involvement in early
intervention.
(e) Parental perception on early intervention services for their children with developmental
disabilities may be studied.
(f) A further study can be conducted to understand the role of early intervention centres in
reducing the stress of parents of children with developmental disabilities.
127
BIBLIOGRAPHY
Alexander, G., Quigg, J., & Armstrong, A. P. (2005). The role of early intervention in
therapy. Retrieved on 11th february 2017, from http://www.leckey.com/pdfs/
American Association on Mental Retardation (1992). Mental Retardation: Definition,
Classification, and Systems of Support. 9th Edn. American Association on Mental
Retardation; Washington
American Occupational Therapy Association (1979). Minutes of the representative assembly,
59th annual conference. American Journal of Occupational Therapy, 33,11, 785.
Banda, D., and Grimmett, E. (2008). Enhancing social and transition behaviors of persons
with autism through activity schedules: A Review. Education and Training in Developmental
Disabilities, 43, 3, 324-333.
Batool, I., and Ijaz, A. (2015). Effectiveness of speech and language therapy for autism
spectrum disorder. Journal of Pakistan Psychiatric Society. Retrieved on 10th february,
2017, from http://www.jpps.com.pk/article
Bax, M., Goldstein, M., & Rosenbaum, P. (2005). Proposed definition and classification of
cerebral palsy. Developmental Medicine and Child Neurology, 47, 571–76.
Beena, J. (2016). Early intervention in children with developmental disabilities. BMH
Medical Journal Editorial, 3,1, 1-4. Retrieved on 10th february, 2017, from
http://www.babymhospital.org/
BIBLIOGRAPHY
Alexander, G., Quigg, J., & Armstrong, A. P. (2005). The role of early intervention in
therapy. Retrieved on 11th february 2017, from http://www.leckey.com/pdfs/
American Association on Mental Retardation (1992). Mental Retardation: Definition,
Classification, and Systems of Support. 9th Edn. American Association on Mental
Retardation; Washington
American Occupational Therapy Association (1979). Minutes of the representative assembly,
59th annual conference. American Journal of Occupational Therapy, 33,11, 785.
Banda, D., and Grimmett, E. (2008). Enhancing social and transition behaviors of persons
with autism through activity schedules: A Review. Education and Training in Developmental
Disabilities, 43, 3, 324-333.
Batool, I., and Ijaz, A. (2015). Effectiveness of speech and language therapy for autism
spectrum disorder. Journal of Pakistan Psychiatric Society. Retrieved on 10th february,
2017, from http://www.jpps.com.pk/article
Bax, M., Goldstein, M., & Rosenbaum, P. (2005). Proposed definition and classification of
cerebral palsy. Developmental Medicine and Child Neurology, 47, 571–76.
Beena, J. (2016). Early intervention in children with developmental disabilities. BMH
Medical Journal Editorial, 3,1, 1-4. Retrieved on 10th february, 2017, from
http://www.babymhospital.org/
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
128
Bishop, D. V. M. (1993) Annotation: autism, executive functions and theory of mind: A
neuropsychological perspective, Journal of Child Psychology and Psychiatry 34, 3, 279–93.
Boyt Shell, B., Gillen, G., & Scaffa, M. (2014). Willard & Spackman's occupational therapy
(1st ed.). Philadelphia: Wolters Kluwer Health.
Bristol, M. M., and Gallagher, J. J. (1982). A family focus for intervention. In E. T. Ramey
& P. L. Trohanis (Eds.), Finding and educating high-risk and handicapped infants (pp. 137-
161). University Park Press : Baltimore, MD.
Brusnahan, L., and Klingenberg, L. (2010). Evidence-based practices for young children with
autism spectrum disorders: Guidelines and recommendations from the national resource
council and national professional development center on autism spectrum disorders.
Retrieved March 23, 2017, from http://www.int-jecse.net.
Bronfenbrenner, U. (1974). A report on longitudinal evaluations of preschool programs (Vol.
2): Is early intervention effective? : Office of Child Development. Department of Health,
Education and Welfare: Washington, DC.
Camarata, S. (2014). Early identification and early intervention in autism spectrum disorders:
accurate and effective?. International Journal of Speech-Language Pathology, 16,1 – 10.
Carta, J. J., and Kong, N. Y. (2007). Trends and issues in interventions for preschoolers with
developmental disabilities. In S. L. Odom, R. H. Horner, M. E. Snell, & J. Blacher (Ed.),
Handbook of developmental disabilities (pp. 181–198). Guilford Press: New York.
Bishop, D. V. M. (1993) Annotation: autism, executive functions and theory of mind: A
neuropsychological perspective, Journal of Child Psychology and Psychiatry 34, 3, 279–93.
Boyt Shell, B., Gillen, G., & Scaffa, M. (2014). Willard & Spackman's occupational therapy
(1st ed.). Philadelphia: Wolters Kluwer Health.
Bristol, M. M., and Gallagher, J. J. (1982). A family focus for intervention. In E. T. Ramey
& P. L. Trohanis (Eds.), Finding and educating high-risk and handicapped infants (pp. 137-
161). University Park Press : Baltimore, MD.
Brusnahan, L., and Klingenberg, L. (2010). Evidence-based practices for young children with
autism spectrum disorders: Guidelines and recommendations from the national resource
council and national professional development center on autism spectrum disorders.
Retrieved March 23, 2017, from http://www.int-jecse.net.
Bronfenbrenner, U. (1974). A report on longitudinal evaluations of preschool programs (Vol.
2): Is early intervention effective? : Office of Child Development. Department of Health,
Education and Welfare: Washington, DC.
Camarata, S. (2014). Early identification and early intervention in autism spectrum disorders:
accurate and effective?. International Journal of Speech-Language Pathology, 16,1 – 10.
Carta, J. J., and Kong, N. Y. (2007). Trends and issues in interventions for preschoolers with
developmental disabilities. In S. L. Odom, R. H. Horner, M. E. Snell, & J. Blacher (Ed.),
Handbook of developmental disabilities (pp. 181–198). Guilford Press: New York.
129
Chippett, D.C. (2017). Early home based intervention with developmentally delayed young
children. Memorial University Research Repository. Research.library.mun.ca. Retrieved on
March 24, 2017, from http://research.library.mun.ca/view/creator_az/
Corsello, C. (2005). Early intervention in autism. Infants & Young Children, 18, 2, 74-85.
Derrington, T., Shapiro, B., & Smith, B (2003). The effectiveness of early intervention
services. Retrieved on 5th february 2017 from http://www.seek.hawaii.edu/
Dunst, C. J. (2007). Early intervention for infants and toddlers with developmental
disabilities. In S. L. Odom, R. H. Homer, M. Snell, & J. Blacher (Ed.). Handbook of
developmental disabilities (pp. 161- 180). Guilford Press: New York.
Fabiennet, B., Naber, A., Bakermans-Kranenburg, M. J., Van Ijzendorn, M. H., Swinkels,
S.H.N., Buitelaar, J. K., Dietz, C., Van Daalen, E. & Van Engeland, H. (2008). Play behavior
and attachment in toddlers with autism. Journal of Autism and Developmental Disorders, 38,
5, 857–866, doi: 10.1007/s10803-007-0454-5.
Gilkerson, L., Hillard, G. A., Schrag, E., & Shonkoff, J. P. (1987). Report accompanying the
education of the handicapped act amendments of 1986 (House Report No. 99-860). National
Center for Clinical Infant Programs. Washington, DC.
Goldstein, H. (2002). Communication intervention for children with autism: A review of
treatment efficacy. Journal of Autism and Developmental Disorders, 32, 5, 373–396.
doi:10.1023/a:1020589821992
Chippett, D.C. (2017). Early home based intervention with developmentally delayed young
children. Memorial University Research Repository. Research.library.mun.ca. Retrieved on
March 24, 2017, from http://research.library.mun.ca/view/creator_az/
Corsello, C. (2005). Early intervention in autism. Infants & Young Children, 18, 2, 74-85.
Derrington, T., Shapiro, B., & Smith, B (2003). The effectiveness of early intervention
services. Retrieved on 5th february 2017 from http://www.seek.hawaii.edu/
Dunst, C. J. (2007). Early intervention for infants and toddlers with developmental
disabilities. In S. L. Odom, R. H. Homer, M. Snell, & J. Blacher (Ed.). Handbook of
developmental disabilities (pp. 161- 180). Guilford Press: New York.
Fabiennet, B., Naber, A., Bakermans-Kranenburg, M. J., Van Ijzendorn, M. H., Swinkels,
S.H.N., Buitelaar, J. K., Dietz, C., Van Daalen, E. & Van Engeland, H. (2008). Play behavior
and attachment in toddlers with autism. Journal of Autism and Developmental Disorders, 38,
5, 857–866, doi: 10.1007/s10803-007-0454-5.
Gilkerson, L., Hillard, G. A., Schrag, E., & Shonkoff, J. P. (1987). Report accompanying the
education of the handicapped act amendments of 1986 (House Report No. 99-860). National
Center for Clinical Infant Programs. Washington, DC.
Goldstein, H. (2002). Communication intervention for children with autism: A review of
treatment efficacy. Journal of Autism and Developmental Disorders, 32, 5, 373–396.
doi:10.1023/a:1020589821992
130
Greenough, W., Black, J., & Wallace, C. (1987). Experience and brain development. Child
development., 58, 3, 539–59. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/3038480
Grover, D. (2005). The young child in the family: Promoting synergies between survival,
growth and development in early childhood. Presentation at the CARK MCH Forum.
Dushambe, Tajikistan, September 20-22, 2005
Guralnick, M. J. (2005). Early intervention for children with intellectual disabilities: Current
knowledge and future prospects. Journal of Applied Research in Intellectual Disabilities, 18,
313–324.
Haley, S. M., Stephens, T. E., & Larsen, A. M. (1988). Patterns of physical and occupational
therapy implementation in early motor intervention. Topics in Early Childhood Special
Education, 7, 4, 46–63. doi:10.1177/027112148800700406
Herskind, A., Greisen, G., & Nielsen, J. (2014). Early identification and intervention in
cerebral palsy. Developmental Medicine & Child Neurology, 57, 1 , 29-36.
Individuals with Disabilities Education Improvement Act of 2004, Pub. L. 108-446, 118 Stat.
2647, 2004 Enacted H.R. 1350; 108 Enacted H.R. 1350. To be codified at 20 U.S.C. 1400 et
seq.
Jain, R., Juneja, M., & Sairam, S. (2013). Children with developmental disabilities in india.
Journal of Child Neurology, 28, 4, 455-460.
Greenough, W., Black, J., & Wallace, C. (1987). Experience and brain development. Child
development., 58, 3, 539–59. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/3038480
Grover, D. (2005). The young child in the family: Promoting synergies between survival,
growth and development in early childhood. Presentation at the CARK MCH Forum.
Dushambe, Tajikistan, September 20-22, 2005
Guralnick, M. J. (2005). Early intervention for children with intellectual disabilities: Current
knowledge and future prospects. Journal of Applied Research in Intellectual Disabilities, 18,
313–324.
Haley, S. M., Stephens, T. E., & Larsen, A. M. (1988). Patterns of physical and occupational
therapy implementation in early motor intervention. Topics in Early Childhood Special
Education, 7, 4, 46–63. doi:10.1177/027112148800700406
Herskind, A., Greisen, G., & Nielsen, J. (2014). Early identification and intervention in
cerebral palsy. Developmental Medicine & Child Neurology, 57, 1 , 29-36.
Individuals with Disabilities Education Improvement Act of 2004, Pub. L. 108-446, 118 Stat.
2647, 2004 Enacted H.R. 1350; 108 Enacted H.R. 1350. To be codified at 20 U.S.C. 1400 et
seq.
Jain, R., Juneja, M., & Sairam, S. (2013). Children with developmental disabilities in india.
Journal of Child Neurology, 28, 4, 455-460.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
131
Joubish, M. F., Farooq, M., & Khurram, M. A. (2015). Early intervention in developmental
disabilities. World Applied Sciences Journal, 11,12, 1590–1596. Retrieved from
https://www.idosi.org/wasj/wasj11(12)/18.pdf
Karande, S., Patil, S., & Kulkarni, M. (2008). Impact of an educational program on parental
knowledge of cerebral palsy. The Indian Journal of Pediatrics, 75, 9, 901–906.
doi:10.1007/s12098-008-0160-0
Koegel, L. K., Koegel, R. L., Ashbaugh, K., & Bradshaw, J. (2013). The importance of early
identification and intervention for children with or at risk for autism spectrum
disorders. International Journal of Speech-Language Pathology, 16, 1, 50–56.
doi:10.3109/17549507.2013.861511
Kurani, D., Nerurka, A., Miranda, L., Jawadwala, F., & Prabhulkar, D. (2009). Impact of
parents’ involvement and engagement in a learning readiness programme for children with
severe and profound intellectual disability and complex needs in India. Journal of Intellectual
Disabilities, 13, 4, 269–289. doi:10.1177/1744629509355751
Lai, D., Chiang, C., Hou, Y., Liu, J., Yao, S., Guo, H., & Tseng, Y. (2014). Predictors of
effectiveness of early intervention on children with intellectual disability: a retrospective
cohort study. BMC Pediatrics, 14, 1.
Landesman R. S.,and Ramey, C. (1999). Early experience and early intervention for children
at risk for developmental delay and mental retardation. Mental Retardation and
Developmental Disabilities Research Reviews, 5,1, 1-10.
Joubish, M. F., Farooq, M., & Khurram, M. A. (2015). Early intervention in developmental
disabilities. World Applied Sciences Journal, 11,12, 1590–1596. Retrieved from
https://www.idosi.org/wasj/wasj11(12)/18.pdf
Karande, S., Patil, S., & Kulkarni, M. (2008). Impact of an educational program on parental
knowledge of cerebral palsy. The Indian Journal of Pediatrics, 75, 9, 901–906.
doi:10.1007/s12098-008-0160-0
Koegel, L. K., Koegel, R. L., Ashbaugh, K., & Bradshaw, J. (2013). The importance of early
identification and intervention for children with or at risk for autism spectrum
disorders. International Journal of Speech-Language Pathology, 16, 1, 50–56.
doi:10.3109/17549507.2013.861511
Kurani, D., Nerurka, A., Miranda, L., Jawadwala, F., & Prabhulkar, D. (2009). Impact of
parents’ involvement and engagement in a learning readiness programme for children with
severe and profound intellectual disability and complex needs in India. Journal of Intellectual
Disabilities, 13, 4, 269–289. doi:10.1177/1744629509355751
Lai, D., Chiang, C., Hou, Y., Liu, J., Yao, S., Guo, H., & Tseng, Y. (2014). Predictors of
effectiveness of early intervention on children with intellectual disability: a retrospective
cohort study. BMC Pediatrics, 14, 1.
Landesman R. S.,and Ramey, C. (1999). Early experience and early intervention for children
at risk for developmental delay and mental retardation. Mental Retardation and
Developmental Disabilities Research Reviews, 5,1, 1-10.
132
Levy, F. (2007). Theories of autism. Australian & New Zealand Journal of Psychiatry, 41, 11,
859-868.
Mahoney, G., Boyce, G., Fewell, R., Spiker, D. & Wheeden, C. (1998). The relationship of
parent-child interaction to the effectiveness of early intervention services for at-risk children
and children with disabilities. Topics in Early Childhood Special Education, 18, 1, 5-17
Majnemer, A. (1998). Benefits of early intervention for children with developmental
disabilities. Seminars in Pediatric Neurology, 5,1, 62–69. doi:10.1016/s1071-9091(98)80020-
Mather, J., and Weinstein, E. (1988). Teachers and therapists: Evolution of a partnership in
early intervention. Topics in Early Childhood Special Education, 7, 4, 1–9.
doi:10.1177/027112148800700402
Menon, L. (2012). Autism spectrum disorders (ASD) (1st ed.). Kanishka Publishers,
Distributors :New Delhi.
McConachie, H. (1986). Parents and young mentally handicapped children: A review of
research issues. Brookline Books : Cambridge
McWilliam, R. A., Young, H. J., & Harville, K. (1996). Therapy services in early
intervention: Current status, barriers, and recommendations. Topics in Early Childhood
Special Education, 16, 3, 348–374. doi:10.1177/027112149601600306
Medical Research Council (MRC) (2000) Review of Autism Research: Epidemiology and
Causes. MRC: London
Levy, F. (2007). Theories of autism. Australian & New Zealand Journal of Psychiatry, 41, 11,
859-868.
Mahoney, G., Boyce, G., Fewell, R., Spiker, D. & Wheeden, C. (1998). The relationship of
parent-child interaction to the effectiveness of early intervention services for at-risk children
and children with disabilities. Topics in Early Childhood Special Education, 18, 1, 5-17
Majnemer, A. (1998). Benefits of early intervention for children with developmental
disabilities. Seminars in Pediatric Neurology, 5,1, 62–69. doi:10.1016/s1071-9091(98)80020-
Mather, J., and Weinstein, E. (1988). Teachers and therapists: Evolution of a partnership in
early intervention. Topics in Early Childhood Special Education, 7, 4, 1–9.
doi:10.1177/027112148800700402
Menon, L. (2012). Autism spectrum disorders (ASD) (1st ed.). Kanishka Publishers,
Distributors :New Delhi.
McConachie, H. (1986). Parents and young mentally handicapped children: A review of
research issues. Brookline Books : Cambridge
McWilliam, R. A., Young, H. J., & Harville, K. (1996). Therapy services in early
intervention: Current status, barriers, and recommendations. Topics in Early Childhood
Special Education, 16, 3, 348–374. doi:10.1177/027112149601600306
Medical Research Council (MRC) (2000) Review of Autism Research: Epidemiology and
Causes. MRC: London
133
Meisels, S.,and Shonkoff, P. (2000). Early childhood intervention: A continuing evolution. In
J. E Shonkoff & S. J Meisels (Ed.), Handbook of Early Childhood Intervention. Cambridge
University Press: New York.
Naletilić, M., Tomic, V., Tabic, M., & Vlak, T. (2009). Cerebral Palsy: Early diagnosis,
intervention and risk factors. Collegium antropologicum, 33, 2, 59-65.
Nelson, Kaylee A. (2013). Parental Involvement in early intervention programs for children
with autism. Master of Social Work Clinical Research Papers. Paper 239.
http://sophia.stkate.edu/msw_papers/239
NIMH (2008). Organization of Early Intervention Services. National Institute for the
Mentally Handicapped: Secunderabad.
Opp, G. and Thurmair, M. (1993). Early intervention for children with developmental delays
and children with disabilities: the bavarian concept. Topics in Early Childhood Special
Education, 13, 4, 488-507.
Panteliadis, C., Hagel, C., Karch, D., & Heinemann, K. (2015). Cerebral Palsy: A Lifelong
challenge asks for early intervention. The Open Neurology Journal, 9, 45-52.
Peterson, N. L. (1987). Early intervention for handicapped and at-risk children: An
introduction to early childhood-special education. Denver: Love.
Pihlar, Z. (2013). From activity to participation – occupational therapy intervention for CP
children. Eastern Journal of Medicine, 17, 4, 198–201. Retrieved on January 10th 2017, from
http://edergi.yyu.edu.tr/article/view/1049000454
Meisels, S.,and Shonkoff, P. (2000). Early childhood intervention: A continuing evolution. In
J. E Shonkoff & S. J Meisels (Ed.), Handbook of Early Childhood Intervention. Cambridge
University Press: New York.
Naletilić, M., Tomic, V., Tabic, M., & Vlak, T. (2009). Cerebral Palsy: Early diagnosis,
intervention and risk factors. Collegium antropologicum, 33, 2, 59-65.
Nelson, Kaylee A. (2013). Parental Involvement in early intervention programs for children
with autism. Master of Social Work Clinical Research Papers. Paper 239.
http://sophia.stkate.edu/msw_papers/239
NIMH (2008). Organization of Early Intervention Services. National Institute for the
Mentally Handicapped: Secunderabad.
Opp, G. and Thurmair, M. (1993). Early intervention for children with developmental delays
and children with disabilities: the bavarian concept. Topics in Early Childhood Special
Education, 13, 4, 488-507.
Panteliadis, C., Hagel, C., Karch, D., & Heinemann, K. (2015). Cerebral Palsy: A Lifelong
challenge asks for early intervention. The Open Neurology Journal, 9, 45-52.
Peterson, N. L. (1987). Early intervention for handicapped and at-risk children: An
introduction to early childhood-special education. Denver: Love.
Pihlar, Z. (2013). From activity to participation – occupational therapy intervention for CP
children. Eastern Journal of Medicine, 17, 4, 198–201. Retrieved on January 10th 2017, from
http://edergi.yyu.edu.tr/article/view/1049000454
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
134
Rutter, M., Bailey, A., Bolton, P. and Le Couteur, A. (1994) Autism and known medical
conditions: myth and substance, Journal of Child Psychology and Psychiatry 35, 2: 311–22
Sacrey, L., Bennett, J., & Zwaigenbaum, L. (2015). Early infant development and
intervention for autism spectrum disorder. Journal of Child Neurology, 30, 14, 1921-1929.
Shonkoff, J., Hauser-Cram, P., Krauss, M., & Upshur, C. (1986). Early intervention for
disabled infants and their families : A quantitative analysis of program impacts. Journal of
Developmental & Behavioral Pediatrics, 7, 3, 199.
Shore, R. (1997). Rethinking the brain: New insights into early development. Families and
Work Institute: New York.
Stephens, L.C. and Tauber, S.K. (2001). Occupational Therapy for Children, Sixth Edition -
Case-Smith, O'Brien (2001). Retrieved on 21st March 2017, from
https://www.scribd.com/doc/299665914/
The royal Australasian college of physician’s early intervention for children with
developmental disabilities. (2013). Retrieved on 1st February 2017, from
https://www.racp.edu.au/docs/default-source/advocacy-library/
Turnbull, A. P.and Turnbull, H. R. (1986). Families and professionals: Creating an
exceptional partnership. Columbus.Merrill: OH
Watts Pappas, N., McAllister, L., & McLeod, S. (2015). Parental beliefs and experiences
regarding involvement in intervention for their child with speech sound disorder. Child
Language Teaching and Therapy, 32, 2, 223–239. doi:10.1177/0265659015615925
Rutter, M., Bailey, A., Bolton, P. and Le Couteur, A. (1994) Autism and known medical
conditions: myth and substance, Journal of Child Psychology and Psychiatry 35, 2: 311–22
Sacrey, L., Bennett, J., & Zwaigenbaum, L. (2015). Early infant development and
intervention for autism spectrum disorder. Journal of Child Neurology, 30, 14, 1921-1929.
Shonkoff, J., Hauser-Cram, P., Krauss, M., & Upshur, C. (1986). Early intervention for
disabled infants and their families : A quantitative analysis of program impacts. Journal of
Developmental & Behavioral Pediatrics, 7, 3, 199.
Shore, R. (1997). Rethinking the brain: New insights into early development. Families and
Work Institute: New York.
Stephens, L.C. and Tauber, S.K. (2001). Occupational Therapy for Children, Sixth Edition -
Case-Smith, O'Brien (2001). Retrieved on 21st March 2017, from
https://www.scribd.com/doc/299665914/
The royal Australasian college of physician’s early intervention for children with
developmental disabilities. (2013). Retrieved on 1st February 2017, from
https://www.racp.edu.au/docs/default-source/advocacy-library/
Turnbull, A. P.and Turnbull, H. R. (1986). Families and professionals: Creating an
exceptional partnership. Columbus.Merrill: OH
Watts Pappas, N., McAllister, L., & McLeod, S. (2015). Parental beliefs and experiences
regarding involvement in intervention for their child with speech sound disorder. Child
Language Teaching and Therapy, 32, 2, 223–239. doi:10.1177/0265659015615925
135
Webster, A., Feiler, A., Webster, V., & Lovell, C. (2004). Parental perspectives on early
intensive intervention for children diagnosed with autistic spectrum disorder. Journal of Early
Childhood Research, 2, 1, 25–49. doi:10.1177/1476718x0421002
White, K. R., Taylor, M. J., & Moss, V. D. (1992). Does research support claims about the
benefits of involving parents in early intervention programs? Review of Educational
Research, 62, 1, 91–125. doi:10.3102/00346543062001091
Webster, A., Feiler, A., Webster, V., & Lovell, C. (2004). Parental perspectives on early
intensive intervention for children diagnosed with autistic spectrum disorder. Journal of Early
Childhood Research, 2, 1, 25–49. doi:10.1177/1476718x0421002
White, K. R., Taylor, M. J., & Moss, V. D. (1992). Does research support claims about the
benefits of involving parents in early intervention programs? Review of Educational
Research, 62, 1, 91–125. doi:10.3102/00346543062001091
1 out of 135
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.