Introduction to Epidemiology (401076) Assignment - Spring 2019
VerifiedAdded on 2022/11/07
|11
|2696
|365
Homework Assignment
AI Summary
This assignment analyzes a cross-sectional study examining the association between domestic violence (emotional, physical, and sexual) during pregnancy and preterm or low birthweight delivery in Ho Chi Minh City, Vietnam. The analysis includes calculating odds ratios, assessing the risk of selection bias, and interpreting the prevalence of physical violence. The assignment also covers a case-control study investigating the link between folic acid supplementation and birth defects, and a cohort study assessing the effect of a rare exposure on disease incidence, including the identification of confounders and calculation of attributable risk. Finally, the assignment discusses potential sources of error and bias in surveys related to weight and height, including recall bias and differential misclassification.

Running head: INTRODUCTION TO EPIDEMIOLOGY (401076) 1
Introduction to Epidemiology (401076)
Student Name
Institution
Introduction to Epidemiology (401076)
Student Name
Institution
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
INTRODUCTION TO EPIDEMIOLOGY 2
Introduction to Epidemiology (401076)
Question 1: [26]
“What study design does this study employ and identify from the paper methodological features
that support the design you just noted?” [2 mark]
This is a cross-section study design. The participants comprised of 1,099 women of age
18 to 49 who had delivered at least one kid in a period of 2 years from ten districts in Ho Chi
Minh City were. A cross section study analyses a subset of the population and observes them for
a period of time. This is satisfied by the fact that this was done for a sample of 10 districts in a
period of 2 years (Vo & Le, 2019).
(b) “What is/are the main exposure/s and what is/are the main outcome/s of this study in
operational terms (i.e., you answer should include how the measure was defined)?” [4 marks]
The main exposure is violence during pregnancy. The study examines the link between
various kinds of domestic violence such as emotional violence, physical violence and sexual
violence on pregnant term/birth weight (Laelago, Belachew, & Tamrat,2017). The study
concluded that domestic violence during pregnancy has about 1.44 times increased risk of a
pregnant mother delivering a preterm or low birthweight child.
(c) “Do you think the risk of selection bias is high or low? Your answer should be justified by no
more than 60 words!! Too long answer will be penalised ?” [4 marks]
The risk of selection bias is low. The criteria used for selection of participants is
probabilistic (Woodward,2013). Random sampling of districts and the subjects to be involved in
the study was done. The data collection method (questionnaire from WHO) is correct. The study
subjects willingly participated in the study increasing validity and accurateness (García-
Moreno,et al,2015)
(d) “Compute the crude OR for domestic violence (yes/no) and pre-term/low birthweight from
data presented in Table 4 and interpret this in your own words.” [4 mark]
Odds Ratio=Odds that a case was Exposed (A/C)/Odds that a Control was Exposed (B/D)
OR=AD/BC= [54/106]/[203/736]=1.84
Introduction to Epidemiology (401076)
Question 1: [26]
“What study design does this study employ and identify from the paper methodological features
that support the design you just noted?” [2 mark]
This is a cross-section study design. The participants comprised of 1,099 women of age
18 to 49 who had delivered at least one kid in a period of 2 years from ten districts in Ho Chi
Minh City were. A cross section study analyses a subset of the population and observes them for
a period of time. This is satisfied by the fact that this was done for a sample of 10 districts in a
period of 2 years (Vo & Le, 2019).
(b) “What is/are the main exposure/s and what is/are the main outcome/s of this study in
operational terms (i.e., you answer should include how the measure was defined)?” [4 marks]
The main exposure is violence during pregnancy. The study examines the link between
various kinds of domestic violence such as emotional violence, physical violence and sexual
violence on pregnant term/birth weight (Laelago, Belachew, & Tamrat,2017). The study
concluded that domestic violence during pregnancy has about 1.44 times increased risk of a
pregnant mother delivering a preterm or low birthweight child.
(c) “Do you think the risk of selection bias is high or low? Your answer should be justified by no
more than 60 words!! Too long answer will be penalised ?” [4 marks]
The risk of selection bias is low. The criteria used for selection of participants is
probabilistic (Woodward,2013). Random sampling of districts and the subjects to be involved in
the study was done. The data collection method (questionnaire from WHO) is correct. The study
subjects willingly participated in the study increasing validity and accurateness (García-
Moreno,et al,2015)
(d) “Compute the crude OR for domestic violence (yes/no) and pre-term/low birthweight from
data presented in Table 4 and interpret this in your own words.” [4 mark]
Odds Ratio=Odds that a case was Exposed (A/C)/Odds that a Control was Exposed (B/D)
OR=AD/BC= [54/106]/[203/736]=1.84
INTRODUCTION TO EPIDEMIOLOGY 3
Since OR>1, There is a strong association between domestic violence and the likelihood of
having a preterm/low birth weight child and the association is significant (p<.05).
This means that with the presence of domestic violence, one has 84% likelihood to have a
preterm/low birth weight child.
(e) “Was the crude OR differ from the adjusted and if yes why? if no why?” [4 marks]
The crude OR is not different from the adjusted OR since the presence of any type of
domestic violence was found to have a high association with preterm/low birth weight child. All
the exposure are equally likely to have similar effects on the dependent variable.
(f) “What was the prevalence of physical violence in this sample and what was the adjusted
prevalence odds ratio (POR-Table 5) between physical violence and pre term/low birthweight?
Interpret the association in your own words, could it be a result of some error?” [4 marks, no
more than 100 words]
The POR was found to be 1.44.This is a significant high value (POR>1) which implies
of presence of a strong positive association between domestic violence and preterm/low birth
weight child. The prevalence of physical violence can be computed as 54/257=0.210.This is a
21% prevalence rate.
(g) “What could be a source of measurement bias in this study and did the authors tried to
address this problem. Explain with evidence from the text.” [4 marks]
Recall bias would be one of the causes of bias in the study. This is where the study
subject answer questions about things that happened to them in the past. In such cases, the
accuracy of information depends on the participant’s memory. The selected subjects in this case
were less than 2 years since they gave birth to their child and can remember most of the
occurrences.
Selection bias-This occurs during sampling. To prevent this, probabilistic sampling
method was used in selection of subject such simple random sampling to get districts, use of
random numbers to select subjects (Flegal & Graubard,2017).
Since OR>1, There is a strong association between domestic violence and the likelihood of
having a preterm/low birth weight child and the association is significant (p<.05).
This means that with the presence of domestic violence, one has 84% likelihood to have a
preterm/low birth weight child.
(e) “Was the crude OR differ from the adjusted and if yes why? if no why?” [4 marks]
The crude OR is not different from the adjusted OR since the presence of any type of
domestic violence was found to have a high association with preterm/low birth weight child. All
the exposure are equally likely to have similar effects on the dependent variable.
(f) “What was the prevalence of physical violence in this sample and what was the adjusted
prevalence odds ratio (POR-Table 5) between physical violence and pre term/low birthweight?
Interpret the association in your own words, could it be a result of some error?” [4 marks, no
more than 100 words]
The POR was found to be 1.44.This is a significant high value (POR>1) which implies
of presence of a strong positive association between domestic violence and preterm/low birth
weight child. The prevalence of physical violence can be computed as 54/257=0.210.This is a
21% prevalence rate.
(g) “What could be a source of measurement bias in this study and did the authors tried to
address this problem. Explain with evidence from the text.” [4 marks]
Recall bias would be one of the causes of bias in the study. This is where the study
subject answer questions about things that happened to them in the past. In such cases, the
accuracy of information depends on the participant’s memory. The selected subjects in this case
were less than 2 years since they gave birth to their child and can remember most of the
occurrences.
Selection bias-This occurs during sampling. To prevent this, probabilistic sampling
method was used in selection of subject such simple random sampling to get districts, use of
random numbers to select subjects (Flegal & Graubard,2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION TO EPIDEMIOLOGY 4
Question 2 [12]
“In a case –control study researchers investigated the association between birth defect and
consuming folic acid supplements during pregnancy. There were 72 infants born with birth
defect and 55 of their mothers did not take folic supplementation during pregnancy. The authors
recruited for each case 3 mothers who gave birth to normal infant as control group. Among the
control group there were 70 mothers who did not use folic supplementation during pregnancy.”
(a) “Construct a 2x2 table with columns and rows headings and calculate an appropriate
measure of the strength of association between birth defect and folic acid supplements during
pregnancy.” [4 marks]
According to the description above, taking the55 mothers who had no folic supplement and
3mothers recruited for each case; 55*3=165-70=95.
FOLIC SUPPLEMENT
YES NO TOTAL
DEFECT 17 55 72
NO DEFECT 95 70 165
TOTAL 112 125 237
To measure the strength of association the relative risk or odd ratio can be used (Wassertheil &
Smoller,2015).
In a case control study, the incidence cannot be calculated .In such case therefore the Odds ratio
is used instead of the relative risk (Oakes & Kaufman,2017)
Odd Ratio= Odds that a case was exposed/Odds that a Control was Exposed
Odds Ratio=Odds that a case was Exposed (A/C)/Odds that a Control was Exposed (B/D)
Question 2 [12]
“In a case –control study researchers investigated the association between birth defect and
consuming folic acid supplements during pregnancy. There were 72 infants born with birth
defect and 55 of their mothers did not take folic supplementation during pregnancy. The authors
recruited for each case 3 mothers who gave birth to normal infant as control group. Among the
control group there were 70 mothers who did not use folic supplementation during pregnancy.”
(a) “Construct a 2x2 table with columns and rows headings and calculate an appropriate
measure of the strength of association between birth defect and folic acid supplements during
pregnancy.” [4 marks]
According to the description above, taking the55 mothers who had no folic supplement and
3mothers recruited for each case; 55*3=165-70=95.
FOLIC SUPPLEMENT
YES NO TOTAL
DEFECT 17 55 72
NO DEFECT 95 70 165
TOTAL 112 125 237
To measure the strength of association the relative risk or odd ratio can be used (Wassertheil &
Smoller,2015).
In a case control study, the incidence cannot be calculated .In such case therefore the Odds ratio
is used instead of the relative risk (Oakes & Kaufman,2017)
Odd Ratio= Odds that a case was exposed/Odds that a Control was Exposed
Odds Ratio=Odds that a case was Exposed (A/C)/Odds that a Control was Exposed (B/D)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
INTRODUCTION TO EPIDEMIOLOGY 5
OR=AD/BC= [17/95]/[55/70]=17*70/55*95=1190/5225=0.228
b) “What the name of this measure and how you interpret the findings in (a) in your own words.”
[4 marks]
In this case we used the Odds Ratio since this is a case control study. If the Odds Ratio
<1 it implies that the exposure has a negative association with the defect
In this case OR=0.228 which is less than 1 hence implying that a negative association between
mothers having birth defect and folic acid supplements during pregnancy (Purdue,et al,2015))
c) “What proportion of birth defect in the population is potentially preventable, assuming a
causal association between folic acid supplement.”[4 marks] explain in words your findings
From the whole population, the birth defect that has potential to be prevented is
55/237.This consist of 23.2% of the total population assuming that the sample selected was
representative of the total population.
Question 3: [16]
“In a cohort study investigating the effect of a rare exposure (E) on a disease , the following
results were obtained.”
Table: Incidence the disease by exposure status, stratified by age group (young /old)
Cases of D Persons-years/1000
Total
Exposed 51 3116
Not exposed 345 31787
Young adults <65
Exposed 19 1168
Not exposed 177 13,177
Old adults
Exposed 33 1948
Not exposed 167 18560
OR=AD/BC= [17/95]/[55/70]=17*70/55*95=1190/5225=0.228
b) “What the name of this measure and how you interpret the findings in (a) in your own words.”
[4 marks]
In this case we used the Odds Ratio since this is a case control study. If the Odds Ratio
<1 it implies that the exposure has a negative association with the defect
In this case OR=0.228 which is less than 1 hence implying that a negative association between
mothers having birth defect and folic acid supplements during pregnancy (Purdue,et al,2015))
c) “What proportion of birth defect in the population is potentially preventable, assuming a
causal association between folic acid supplement.”[4 marks] explain in words your findings
From the whole population, the birth defect that has potential to be prevented is
55/237.This consist of 23.2% of the total population assuming that the sample selected was
representative of the total population.
Question 3: [16]
“In a cohort study investigating the effect of a rare exposure (E) on a disease , the following
results were obtained.”
Table: Incidence the disease by exposure status, stratified by age group (young /old)
Cases of D Persons-years/1000
Total
Exposed 51 3116
Not exposed 345 31787
Young adults <65
Exposed 19 1168
Not exposed 177 13,177
Old adults
Exposed 33 1948
Not exposed 167 18560
INTRODUCTION TO EPIDEMIOLOGY 6
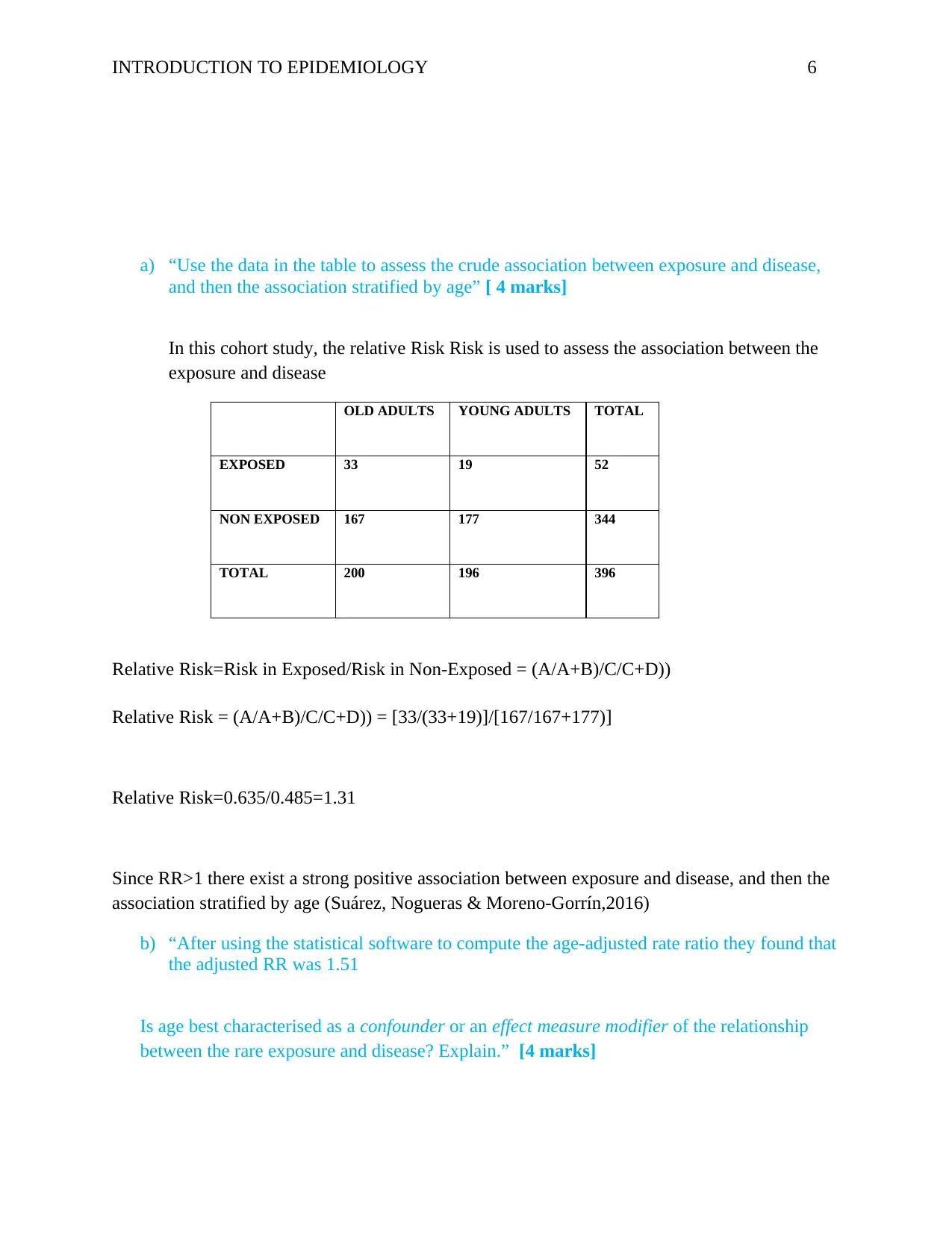
a) “Use the data in the table to assess the crude association between exposure and disease,
and then the association stratified by age” [ 4 marks]
In this cohort study, the relative Risk Risk is used to assess the association between the
exposure and disease
OLD ADULTS YOUNG ADULTS TOTAL
EXPOSED 33 19 52
NON EXPOSED 167 177 344
TOTAL 200 196 396
Relative Risk=Risk in Exposed/Risk in Non-Exposed = (A/A+B)/C/C+D))
Relative Risk = (A/A+B)/C/C+D)) = [33/(33+19)]/[167/167+177)]
Relative Risk=0.635/0.485=1.31
Since RR>1 there exist a strong positive association between exposure and disease, and then the
association stratified by age (Suárez, Nogueras & Moreno-Gorrín,2016)
b) “After using the statistical software to compute the age-adjusted rate ratio they found that
the adjusted RR was 1.51
Is age best characterised as a confounder or an effect measure modifier of the relationship
between the rare exposure and disease? Explain.” [4 marks]
a) “Use the data in the table to assess the crude association between exposure and disease,
and then the association stratified by age” [ 4 marks]
In this cohort study, the relative Risk Risk is used to assess the association between the
exposure and disease
OLD ADULTS YOUNG ADULTS TOTAL
EXPOSED 33 19 52
NON EXPOSED 167 177 344
TOTAL 200 196 396
Relative Risk=Risk in Exposed/Risk in Non-Exposed = (A/A+B)/C/C+D))
Relative Risk = (A/A+B)/C/C+D)) = [33/(33+19)]/[167/167+177)]
Relative Risk=0.635/0.485=1.31
Since RR>1 there exist a strong positive association between exposure and disease, and then the
association stratified by age (Suárez, Nogueras & Moreno-Gorrín,2016)
b) “After using the statistical software to compute the age-adjusted rate ratio they found that
the adjusted RR was 1.51
Is age best characterised as a confounder or an effect measure modifier of the relationship
between the rare exposure and disease? Explain.” [4 marks]
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION TO EPIDEMIOLOGY 7
A cofounder is a kind of a risk factor for the disease under scrutiny (Thrusfield, 2018). For
this study to measure the association between rare exposure and disease, age is a confounder
since it is a big contributor to the exposure to the disease (Corraini,Pedersen & Vandenbroucke,
2017).
Also, the risk ratio obtained was for the age stratified is 1.3 which and less than the crude risk
ratio of 1.5 hence age is a cofounder.
c) “What is the attributable risk of the exposure in older people?” [4 marks]
According to Pagano & Gauvreau(2018),Attributable risk=risk for non-exposed group-risk for
exposed group
AR=p1-p2
P1=a/a+b=proportion of old =33/(33+19)= 0.635
P2=c/c+d =proportion of young =167/167+177=0.485
AR=0.635-0.485=0.15
d) “How would you interpret the finding in 3 (c)?” [4 marks]
Measuring the attributable risk as a percentage will be;
AR% =(0.635-0.485/.635)*100=23.62%
This implies that about 23.62% of the participants with the rare disease can be attributed to the
participant’s old age.( Ahlbom,2017).
Question 4 [12]
“In a survey of the prevalence of overweight and obese participants were measured once for their
weight and once for their height in the same lab”
a) “What source of error/bias, if at all, it can introduce to the estimated prevalence? (explain
briefly)” [4 marks]
A cofounder is a kind of a risk factor for the disease under scrutiny (Thrusfield, 2018). For
this study to measure the association between rare exposure and disease, age is a confounder
since it is a big contributor to the exposure to the disease (Corraini,Pedersen & Vandenbroucke,
2017).
Also, the risk ratio obtained was for the age stratified is 1.3 which and less than the crude risk
ratio of 1.5 hence age is a cofounder.
c) “What is the attributable risk of the exposure in older people?” [4 marks]
According to Pagano & Gauvreau(2018),Attributable risk=risk for non-exposed group-risk for
exposed group
AR=p1-p2
P1=a/a+b=proportion of old =33/(33+19)= 0.635
P2=c/c+d =proportion of young =167/167+177=0.485
AR=0.635-0.485=0.15
d) “How would you interpret the finding in 3 (c)?” [4 marks]
Measuring the attributable risk as a percentage will be;
AR% =(0.635-0.485/.635)*100=23.62%
This implies that about 23.62% of the participants with the rare disease can be attributed to the
participant’s old age.( Ahlbom,2017).
Question 4 [12]
“In a survey of the prevalence of overweight and obese participants were measured once for their
weight and once for their height in the same lab”
a) “What source of error/bias, if at all, it can introduce to the estimated prevalence? (explain
briefly)” [4 marks]
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
INTRODUCTION TO EPIDEMIOLOGY 8
In this scenario, the weight and heights of participants were taken from a common instrument
which minimizes errors. There could have been some errors in designing of the experiment since
there is no mention of randomness in selection of the subjects to be selected to the sample.
Otherwise, the experiment considers the weight and height variables to enable the researcher to
measure the participants Body Mass Index (BMI).This is important in showing if a participant is
normal, overweight or obese (Kestenbaum & Weiss, 2019).
“In another survey to estimate the prevalence of overweight and obesity participants were
asked to report on their weight and height from their head ”
b) What source of error/bias, if at all, in can introduce to the estimated prevalence? Explain
(you can use reference here) [4 marks]
This is an information or measurement bias of the study variable. This arises from
inaccurately classifying and measuring the study variables (Merrill, 2019). Asking the
participants to report their weights and height from their heads will result to errors. A participant
could have measured his/her weight / height a long period ago. This participant will have lost or
gained weight from that time. Also, the scales used to measure weight and height could be
different from one source to another. These will results to measurement error hence wrong
results.
c) “if you were told that women were more likely to underestimate their weight and men
accurately report their weight what source of bias it is : [4 marks]
i) Differential misclassification.
ii) Non-differential misclassification.
iii) Recall bias.
iv) Confounding.”
Explain your answer briefly
In this scenario, the weight and heights of participants were taken from a common instrument
which minimizes errors. There could have been some errors in designing of the experiment since
there is no mention of randomness in selection of the subjects to be selected to the sample.
Otherwise, the experiment considers the weight and height variables to enable the researcher to
measure the participants Body Mass Index (BMI).This is important in showing if a participant is
normal, overweight or obese (Kestenbaum & Weiss, 2019).
“In another survey to estimate the prevalence of overweight and obesity participants were
asked to report on their weight and height from their head ”
b) What source of error/bias, if at all, in can introduce to the estimated prevalence? Explain
(you can use reference here) [4 marks]
This is an information or measurement bias of the study variable. This arises from
inaccurately classifying and measuring the study variables (Merrill, 2019). Asking the
participants to report their weights and height from their heads will result to errors. A participant
could have measured his/her weight / height a long period ago. This participant will have lost or
gained weight from that time. Also, the scales used to measure weight and height could be
different from one source to another. These will results to measurement error hence wrong
results.
c) “if you were told that women were more likely to underestimate their weight and men
accurately report their weight what source of bias it is : [4 marks]
i) Differential misclassification.
ii) Non-differential misclassification.
iii) Recall bias.
iv) Confounding.”
Explain your answer briefly
INTRODUCTION TO EPIDEMIOLOGY 9
This can be classified as being a recall bias. According to Porta et al. (2014) his is a
systematic error that occurs when the study subjects are less likely to relate some information on
a given exposure in accordance to the outcome. The systematic differences in how the subject
report outcome. This kind of bias is mainly found in case control studies (Giesecke, J. (2017).
On the gender variable, most women tend to consider less weight fashionable and more
attractive. From those reports and suggestions one could lead to making a reporting or recall
bias. This then lead to differential classification.
This can be classified as being a recall bias. According to Porta et al. (2014) his is a
systematic error that occurs when the study subjects are less likely to relate some information on
a given exposure in accordance to the outcome. The systematic differences in how the subject
report outcome. This kind of bias is mainly found in case control studies (Giesecke, J. (2017).
On the gender variable, most women tend to consider less weight fashionable and more
attractive. From those reports and suggestions one could lead to making a reporting or recall
bias. This then lead to differential classification.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION TO EPIDEMIOLOGY 10
References
1. Corraini, P., Olsen, M., Pedersen, L., Dekkers, O. M., & Vandenbroucke, J. P. (2017). Effect
modification, interaction and mediation: an overview of theoretical insights for clinical
investigators. Clinical epidemiology, 9, 331.
2. Flegal, K. M., Kit, B. K., & Graubard, B. I. (2017). Bias in hazard ratios arising from
misclassification according to self-reported weight and height in observational studies of
body mass index and mortality. American journal of epidemiology, 187(1), 125-134.
3. García-Moreno, C., Hegarty, K., d'Oliveira, A. F. L., Koziol-McLain, J., Colombini, M., &
Feder, G. (2015). The health-systems response to violence against women. The Lancet,
385(9977), 1567-1579.
4. Giesecke, J. (2017). Modern infectious disease epidemiology. CRC Press.
5. Kestenbaum, B., & Weiss, N. S. (2019). Epidemiology and biostatistics: an introduction to
clinical research. Springer.
6. Laelago, T., Belachew, T., & Tamrat, M. (2017). Effect of intimate partner violence on birth
outcomes. African health sciences, 17(3), 681-689.
7. Merrill, R. M. (2019). Introduction to epidemiology. Jones & Bartlett Publishers.
8. Oakes, J. M., & Kaufman, J. S. (Eds.). (2017). Methods in social epidemiology. John Wiley
& Sons.
9. Pagano, M., & Gauvreau, K. (2018). Principles of biostatistics. Chapman and Hall/CRC.
10. Porta, M. (Ed.). (2014). A dictionary of epidemiology. Oxford university press.
11. Purdue, M. P., Hutchings, S. J., Rushton, L., & Silverman, D. T. (2015). The proportion of
cancer attributable to occupational exposures. Annals of epidemiology, 25(3), 188-192.
12. Suárez, E. L., Pérez, C. M., Nogueras, G. M., & Moreno-Gorrín, C. (2016). Biostatistics in
Public Health Using STATA. CRC Press.
13. Thrusfield, M. (2018). Veterinary epidemiology. John Wiley & Sons.
14. Vo, T. M., Tran, V. T., Cuu, T. N., Do, T. T., & Le, T. M. (2019). Domestic violence and its
association with pre-term or low birthweight delivery in Vietnam. International Journal of
Women's Health, 11, 501-510.
15. Wassertheil-Smoller, S., & Smoller, J. (2015). Biostatistics and epidemiology: a primer for
health and biomedical professionals. Springer.
References
1. Corraini, P., Olsen, M., Pedersen, L., Dekkers, O. M., & Vandenbroucke, J. P. (2017). Effect
modification, interaction and mediation: an overview of theoretical insights for clinical
investigators. Clinical epidemiology, 9, 331.
2. Flegal, K. M., Kit, B. K., & Graubard, B. I. (2017). Bias in hazard ratios arising from
misclassification according to self-reported weight and height in observational studies of
body mass index and mortality. American journal of epidemiology, 187(1), 125-134.
3. García-Moreno, C., Hegarty, K., d'Oliveira, A. F. L., Koziol-McLain, J., Colombini, M., &
Feder, G. (2015). The health-systems response to violence against women. The Lancet,
385(9977), 1567-1579.
4. Giesecke, J. (2017). Modern infectious disease epidemiology. CRC Press.
5. Kestenbaum, B., & Weiss, N. S. (2019). Epidemiology and biostatistics: an introduction to
clinical research. Springer.
6. Laelago, T., Belachew, T., & Tamrat, M. (2017). Effect of intimate partner violence on birth
outcomes. African health sciences, 17(3), 681-689.
7. Merrill, R. M. (2019). Introduction to epidemiology. Jones & Bartlett Publishers.
8. Oakes, J. M., & Kaufman, J. S. (Eds.). (2017). Methods in social epidemiology. John Wiley
& Sons.
9. Pagano, M., & Gauvreau, K. (2018). Principles of biostatistics. Chapman and Hall/CRC.
10. Porta, M. (Ed.). (2014). A dictionary of epidemiology. Oxford university press.
11. Purdue, M. P., Hutchings, S. J., Rushton, L., & Silverman, D. T. (2015). The proportion of
cancer attributable to occupational exposures. Annals of epidemiology, 25(3), 188-192.
12. Suárez, E. L., Pérez, C. M., Nogueras, G. M., & Moreno-Gorrín, C. (2016). Biostatistics in
Public Health Using STATA. CRC Press.
13. Thrusfield, M. (2018). Veterinary epidemiology. John Wiley & Sons.
14. Vo, T. M., Tran, V. T., Cuu, T. N., Do, T. T., & Le, T. M. (2019). Domestic violence and its
association with pre-term or low birthweight delivery in Vietnam. International Journal of
Women's Health, 11, 501-510.
15. Wassertheil-Smoller, S., & Smoller, J. (2015). Biostatistics and epidemiology: a primer for
health and biomedical professionals. Springer.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
INTRODUCTION TO EPIDEMIOLOGY 11
16. Woodward, M. (2013). Epidemiology: study design and data analysis. Chapman and
Hall/CRC.
16. Woodward, M. (2013). Epidemiology: study design and data analysis. Chapman and
Hall/CRC.
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.