Mechanical versus manual chest compressions for cardiac arrest: a systematic review and meta-analysis
VerifiedAdded on 2023/06/15
|10
|6758
|122
AI Summary
This paper is a systematic review and meta-analysis of the published literatures comparing the use of mechanical chest compression device and manual chest compression during cardiac arrest (CA) with respect to short-term survival outcomes and neurological function. The study found that the ability to achieve ROSC with mechanical devise was inferior to manual chest compression during resuscitation. The use of mechanical chest compression cannot be recommended as a replacement for manual CPR, but rather a supplemental treatment in an overall strategy for treating CA patients.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
O R I G I N A L R E S E A R C H Open Access
Mechanicalversus manualchest
compressions for cardiac arrest:a
systematic review and meta-analysis
HuiLi1†
, Dongping Wang2†
, Yi Yu1
, Xiang Zhao1 and XiaoliJing1*
Abstract
Background:The aim of this paper was to conduct a systematic review of the published literatures comparing the
use of mechanicalchest compression device and manualchest compression during cardiac arrest (CA) with respect
to short-term survivaloutcomes and neurologicalfunction.
Methods:Databases including MEDLINE,EMBASE,Web of Science and the ClinicalTrials.gov registry were
systematically searched.Further references were gathered from cross-references from articles by handsearch.The
inclusion criteria for this review must be human prospective controlled studies of adult CA.Random effects models
were used to assess the risk ratios and 95 % confidence intervals for return of spontaneous circulation (ROSC),
survivalto admission and discharge,and neurologicalfunction.
Results:Twelve trials (9 out-of-hospitaland 3 in-hospitalstudies),involving 11,162 participants,were included in
the review.The results of this meta-analysis indicated no differences were found in CerebralPerformance Category
(CPC) scores,survivalto hospitaladmission and survivalto discharge between manualcardiopulmonary
resuscitation (CPR) and mechanicalCPR for out-of-hospitalCA (OHCA) patients.The data on achieving ROSC in both
of in-hospitaland out-of-hospitalsetting suggested poor application of the mechanicaldevice (RR 0.71,[95 % CI,
0.53,0.97] and 0.87 [95 % CI,0.81,0.94],respectively).OHCA patients receiving manualresuscitation were more
likely to attain ROSC compared with load-distributing bands chest compression device (RR 0.88,[95 % CI,0.80,
0.96]).The in-hospitalstudies suggested increased relative harm with mechanicalcompressions for ratio of survival
to hospitaldischarge (RR 0.54,[95 % CI0.29,0.98]).However,the results were not statistically significant between
different kinds of mechanicalchest compression devices and manualresuscitation in survivalto admission,
discharge and CPC scores for OHCA patients and survivalto discharge for in-hospitalCA patients.
Conclusions:The ability to achieve ROSC with mechanicaldevise was inferior to manualchest compression during
resuscitation.The use of mechanicalchest compression cannot be recommended as a replacement for manualCPR,
but rather a supplementaltreatment in an overallstrategy for treating CA patients.
Keywords:Cardiac arrest,Cardiopulmonary resuscitation,Device,Meta-analysis
Li et al.Scandinavian Journalof Trauma,Resuscitation
and Emergency Medicine (2016) 24:10
DOI10.1186/s13049-016-0202-y
Mechanicalversus manualchest
compressions for cardiac arrest:a
systematic review and meta-analysis
HuiLi1†
, Dongping Wang2†
, Yi Yu1
, Xiang Zhao1 and XiaoliJing1*
Abstract
Background:The aim of this paper was to conduct a systematic review of the published literatures comparing the
use of mechanicalchest compression device and manualchest compression during cardiac arrest (CA) with respect
to short-term survivaloutcomes and neurologicalfunction.
Methods:Databases including MEDLINE,EMBASE,Web of Science and the ClinicalTrials.gov registry were
systematically searched.Further references were gathered from cross-references from articles by handsearch.The
inclusion criteria for this review must be human prospective controlled studies of adult CA.Random effects models
were used to assess the risk ratios and 95 % confidence intervals for return of spontaneous circulation (ROSC),
survivalto admission and discharge,and neurologicalfunction.
Results:Twelve trials (9 out-of-hospitaland 3 in-hospitalstudies),involving 11,162 participants,were included in
the review.The results of this meta-analysis indicated no differences were found in CerebralPerformance Category
(CPC) scores,survivalto hospitaladmission and survivalto discharge between manualcardiopulmonary
resuscitation (CPR) and mechanicalCPR for out-of-hospitalCA (OHCA) patients.The data on achieving ROSC in both
of in-hospitaland out-of-hospitalsetting suggested poor application of the mechanicaldevice (RR 0.71,[95 % CI,
0.53,0.97] and 0.87 [95 % CI,0.81,0.94],respectively).OHCA patients receiving manualresuscitation were more
likely to attain ROSC compared with load-distributing bands chest compression device (RR 0.88,[95 % CI,0.80,
0.96]).The in-hospitalstudies suggested increased relative harm with mechanicalcompressions for ratio of survival
to hospitaldischarge (RR 0.54,[95 % CI0.29,0.98]).However,the results were not statistically significant between
different kinds of mechanicalchest compression devices and manualresuscitation in survivalto admission,
discharge and CPC scores for OHCA patients and survivalto discharge for in-hospitalCA patients.
Conclusions:The ability to achieve ROSC with mechanicaldevise was inferior to manualchest compression during
resuscitation.The use of mechanicalchest compression cannot be recommended as a replacement for manualCPR,
but rather a supplementaltreatment in an overallstrategy for treating CA patients.
Keywords:Cardiac arrest,Cardiopulmonary resuscitation,Device,Meta-analysis
Li et al.Scandinavian Journalof Trauma,Resuscitation
and Emergency Medicine (2016) 24:10
DOI10.1186/s13049-016-0202-y
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Background
Sudden cardiacarrest(CA) occurs when someone’s
heart stops beating unexpectedly.Minimally interrupted,
regularand appropriatecardiopulmonaryresuscitation
(CPR) can keep blood flowing to the victim’s vitalorgans
while the heart is not pumping [1–4].Unfortunately,even
healthcareprofessionalshave difficultyin performing
effective CPR persistently,especially in a moving vehicle
and in situations of prolonged cardiac arrest [5–8].Chest-
compressions often are too shallow,hands-off time is too
long,chestcompression rate islessthan 90/min,and
rescuers fatigue over time [9–12].
Machines have been developed to take over this chest
pumping action using pneumatically driven or load-dis-
tributing bands (LDBs) mechanisms, because the machines
do not pause or get tired, and deliver uninterrupted chest-
compressions with a predefined depth and rate [13].Some
studies using those machines for chest compressions have
shown thatthey could achieveintrathoracicpressures
higher, improve coronary and systemic perfusion pressures
and flows compared with manualCPR in animalmodels
and in a smallnumber ofterminally illpatients [14–16].
Some data from human observationalstudies suggested
that mechanicalchest compressions might be superior to
manualchestcompressions in cardiac arrest[16–19].A
few recentmeta-analysescould not eliminateall the
doubts at this regards because of the paucity of data avail-
able and the presence of confounding factors [20–22].We
aimed to investigate which method ofchest compression
(applying the traditionalmanualcompression vs.using a
machine) would result in more lives saved.
Methods
Types of studies
A meta-analysis was performed to compare any type of
mechanicalchest compression device with manualchest
compression in themanagementof patientssuffered
from CA in out-of-hospital and in-hospitalsettings.
Human prospective randomized controlled studies com-
paring compressions delivered via any type ofpowered,
automatic mechanicalcompression device versus man-
ual compression were considered for inclusion.Studies
Electronic searches
A search strategy was pursued,using the following search
terms:“mechanical”,“manual”,“chestcompression” and
“cardiopulmonary resuscitation”. Searches were conducted
in MEDLINE (1946 to 31 August 2015),EMBASE (1950
to 31 August2015),Web of Science (including web of
science Core Collection,current content connect,BIOSIS
Previews,Chinese Science Citation Database and SciELO
Citation Index,from the start to 31 August 2015) and the
ClinicalTrials.gov registry (on 31 August 2015).We hand-
searched bibliographiesof included papers.The search
was inclusive of studies in any language.
Data collection and analysis
Data selectionand data extractedwere performed
among pairs ofindependentreviewers,and the results
were confirmed by a third review author.Discrepancies
were discussed and adjudicated by the team consensus.
In reporting the results of this systematic review,the au-
thors have followed the recommended guidelines from
the Quality ofReporting ofMeta-Analysis (QUOROM)
Statement.
Statistical analyses
Data were checked and entered into the Stata 12.0 (Stata
Corp.,College Station,TX) database for further analysis.
Using a random-effectsmodel,we calculated the risk
ratios (RR) and 95 % confidence intervals (CI) for ROSC,
arrivalto hospitalwith a spontaneouspalpable pulse,
survivalat discharge and CPC score.The presence of
heterogeneity between trialswasassessed using the I2
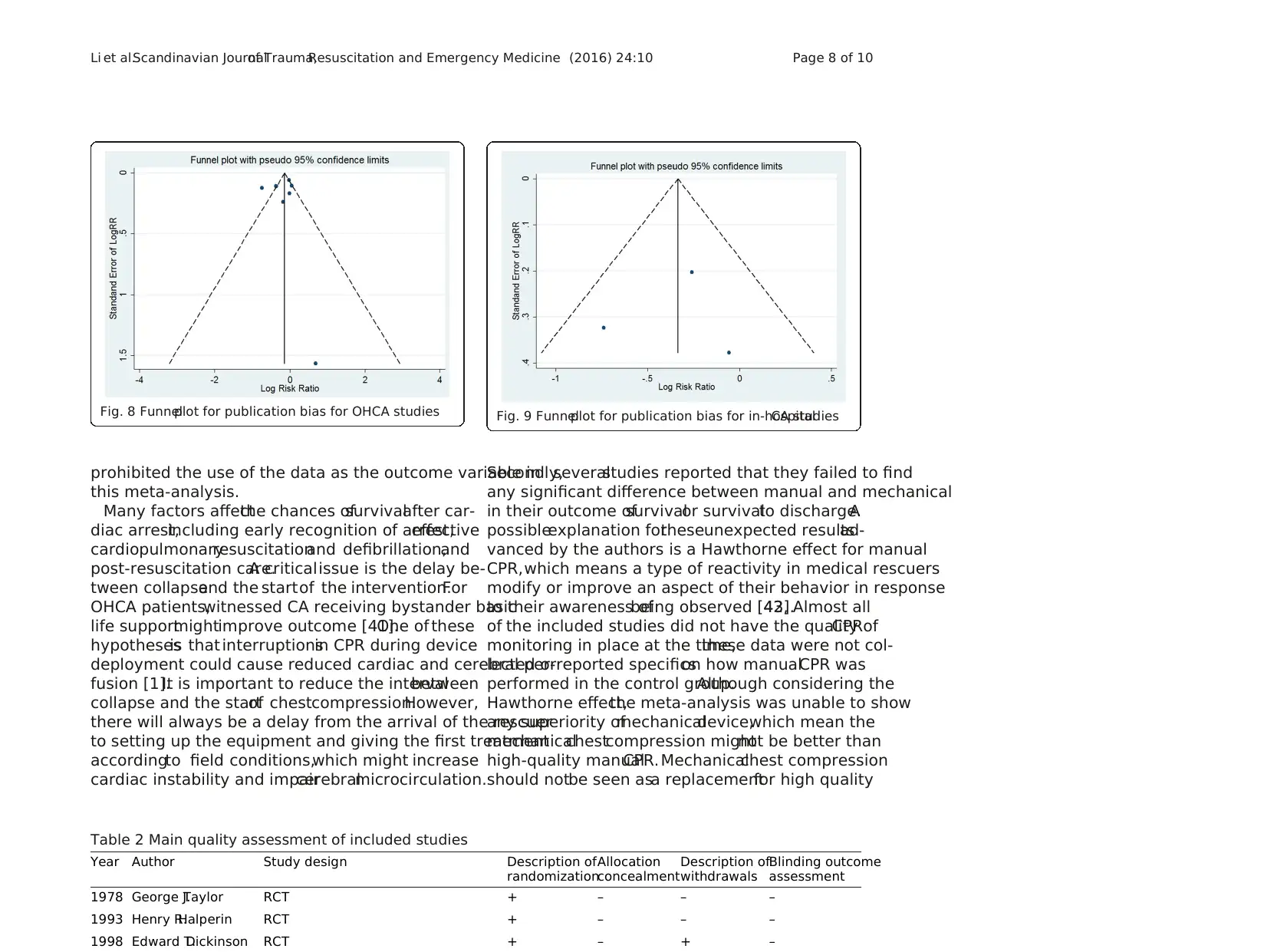
statistics.Funnelplots and Egger’s regression testwere
used to assess the potential for reporting bias.
Results
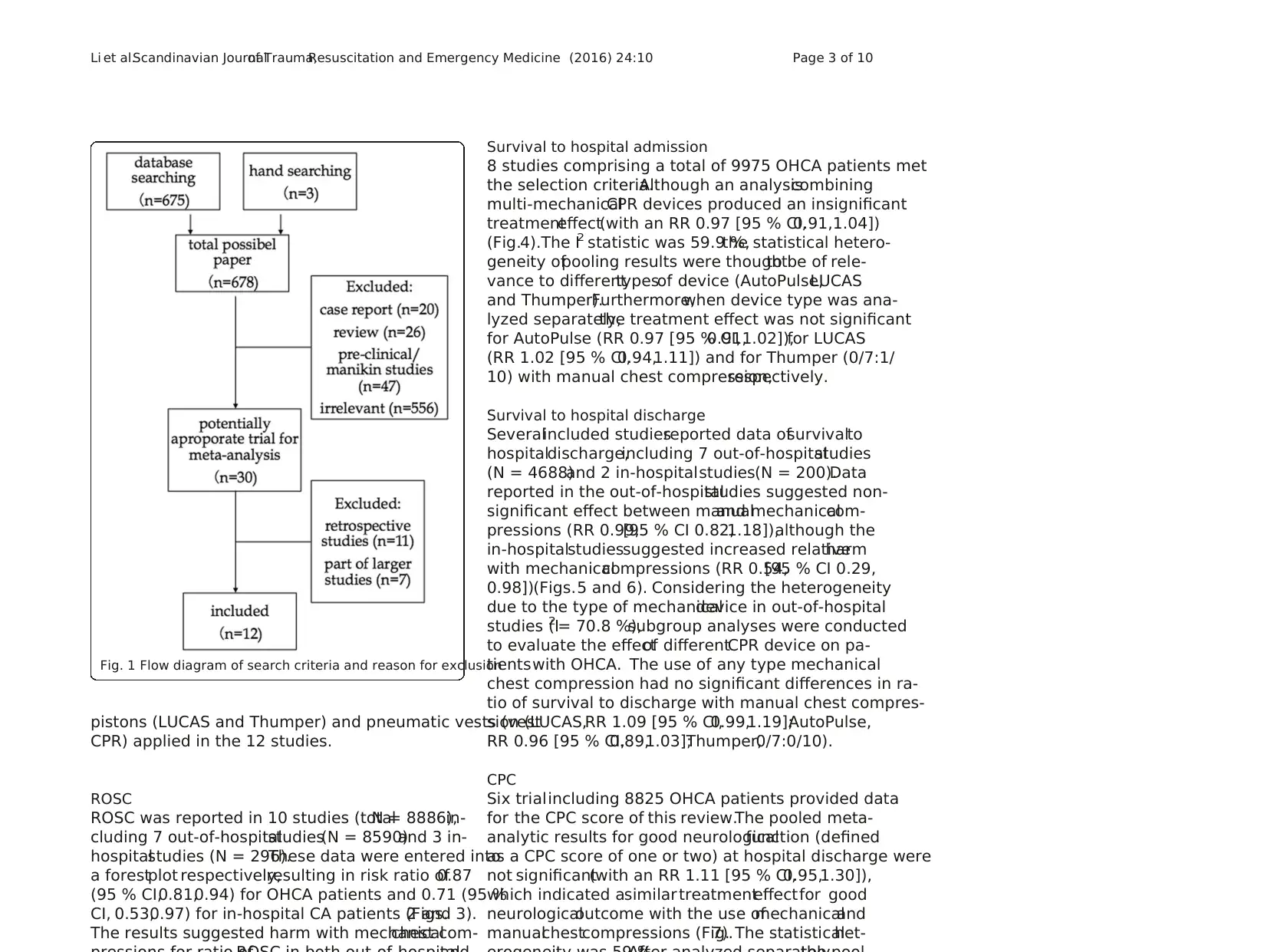
Results of the search
In the originalreview,the comprehensive search identi-
fied 678 citations (MEDLINE 118,EMBASE 94,Web of
Science 444,clinicaltrials.gov 19,handsearch of references
of included papers 3).Two independentreview authors
reviewed 678 citationsby titles;possible citations were
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 2 of 10
Sudden cardiacarrest(CA) occurs when someone’s
heart stops beating unexpectedly.Minimally interrupted,
regularand appropriatecardiopulmonaryresuscitation
(CPR) can keep blood flowing to the victim’s vitalorgans
while the heart is not pumping [1–4].Unfortunately,even
healthcareprofessionalshave difficultyin performing
effective CPR persistently,especially in a moving vehicle
and in situations of prolonged cardiac arrest [5–8].Chest-
compressions often are too shallow,hands-off time is too
long,chestcompression rate islessthan 90/min,and
rescuers fatigue over time [9–12].
Machines have been developed to take over this chest
pumping action using pneumatically driven or load-dis-
tributing bands (LDBs) mechanisms, because the machines
do not pause or get tired, and deliver uninterrupted chest-
compressions with a predefined depth and rate [13].Some
studies using those machines for chest compressions have
shown thatthey could achieveintrathoracicpressures
higher, improve coronary and systemic perfusion pressures
and flows compared with manualCPR in animalmodels
and in a smallnumber ofterminally illpatients [14–16].
Some data from human observationalstudies suggested
that mechanicalchest compressions might be superior to
manualchestcompressions in cardiac arrest[16–19].A
few recentmeta-analysescould not eliminateall the
doubts at this regards because of the paucity of data avail-
able and the presence of confounding factors [20–22].We
aimed to investigate which method ofchest compression
(applying the traditionalmanualcompression vs.using a
machine) would result in more lives saved.
Methods
Types of studies
A meta-analysis was performed to compare any type of
mechanicalchest compression device with manualchest
compression in themanagementof patientssuffered
from CA in out-of-hospital and in-hospitalsettings.
Human prospective randomized controlled studies com-
paring compressions delivered via any type ofpowered,
automatic mechanicalcompression device versus man-
ual compression were considered for inclusion.Studies
Electronic searches
A search strategy was pursued,using the following search
terms:“mechanical”,“manual”,“chestcompression” and
“cardiopulmonary resuscitation”. Searches were conducted
in MEDLINE (1946 to 31 August 2015),EMBASE (1950
to 31 August2015),Web of Science (including web of
science Core Collection,current content connect,BIOSIS
Previews,Chinese Science Citation Database and SciELO
Citation Index,from the start to 31 August 2015) and the
ClinicalTrials.gov registry (on 31 August 2015).We hand-
searched bibliographiesof included papers.The search
was inclusive of studies in any language.
Data collection and analysis
Data selectionand data extractedwere performed
among pairs ofindependentreviewers,and the results
were confirmed by a third review author.Discrepancies
were discussed and adjudicated by the team consensus.
In reporting the results of this systematic review,the au-
thors have followed the recommended guidelines from
the Quality ofReporting ofMeta-Analysis (QUOROM)
Statement.
Statistical analyses
Data were checked and entered into the Stata 12.0 (Stata
Corp.,College Station,TX) database for further analysis.
Using a random-effectsmodel,we calculated the risk
ratios (RR) and 95 % confidence intervals (CI) for ROSC,
arrivalto hospitalwith a spontaneouspalpable pulse,
survivalat discharge and CPC score.The presence of
heterogeneity between trialswasassessed using the I2
statistics.Funnelplots and Egger’s regression testwere
used to assess the potential for reporting bias.
Results
Results of the search
In the originalreview,the comprehensive search identi-
fied 678 citations (MEDLINE 118,EMBASE 94,Web of
Science 444,clinicaltrials.gov 19,handsearch of references
of included papers 3).Two independentreview authors
reviewed 678 citationsby titles;possible citations were
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 2 of 10
pistons (LUCAS and Thumper) and pneumatic vests (vest
CPR) applied in the 12 studies.
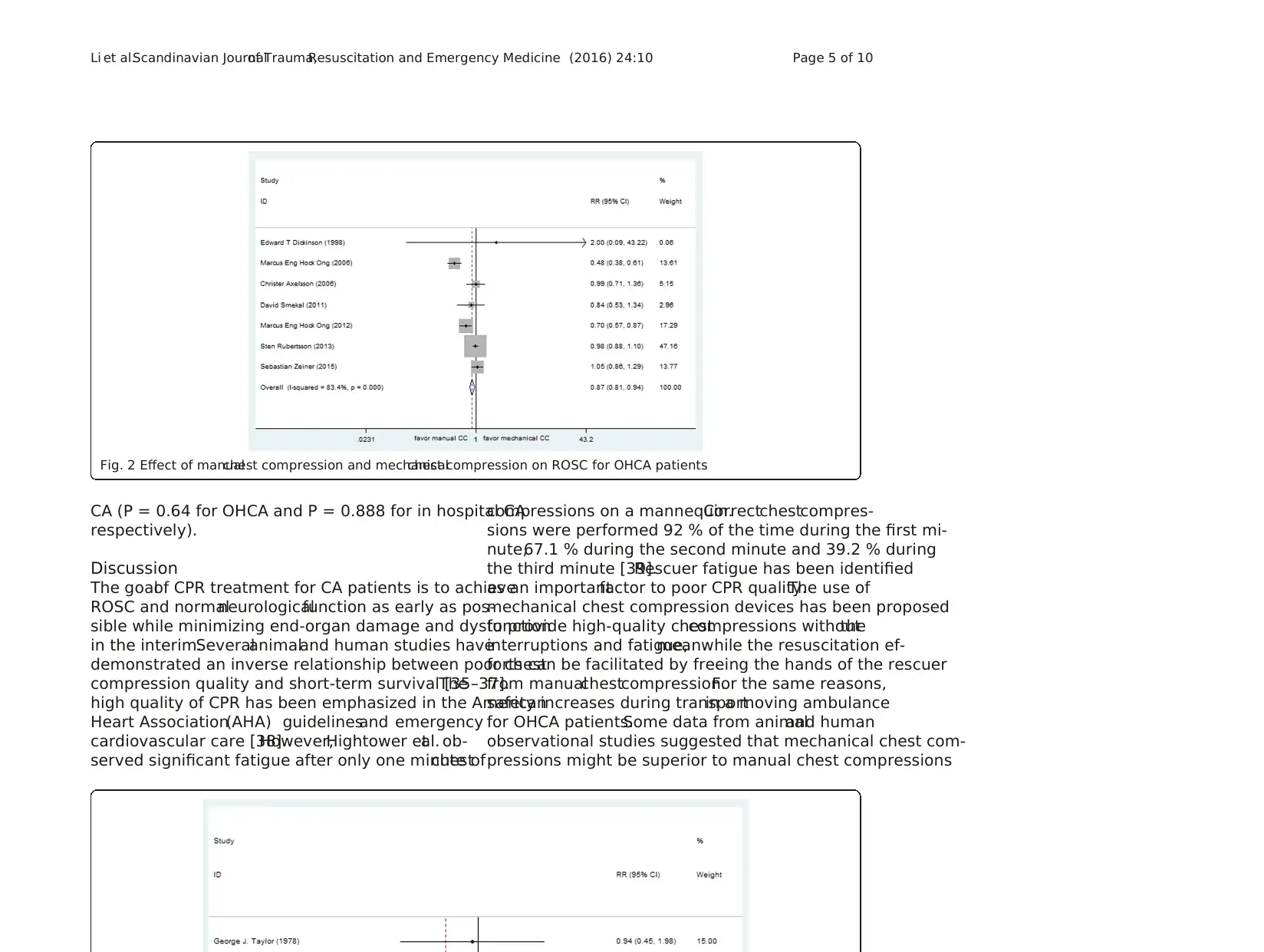
ROSC
ROSC was reported in 10 studies (totalN = 8886),in-
cluding 7 out-of-hospitalstudies(N = 8590)and 3 in-
hospitalstudies (N = 296).These data were entered into
a forestplot respectively,resulting in risk ratio of0.87
(95 % CI,0.81,0.94) for OHCA patients and 0.71 (95 %
CI, 0.53,0.97) for in-hospital CA patients (Figs.2 and 3).
The results suggested harm with mechanicalchest com-
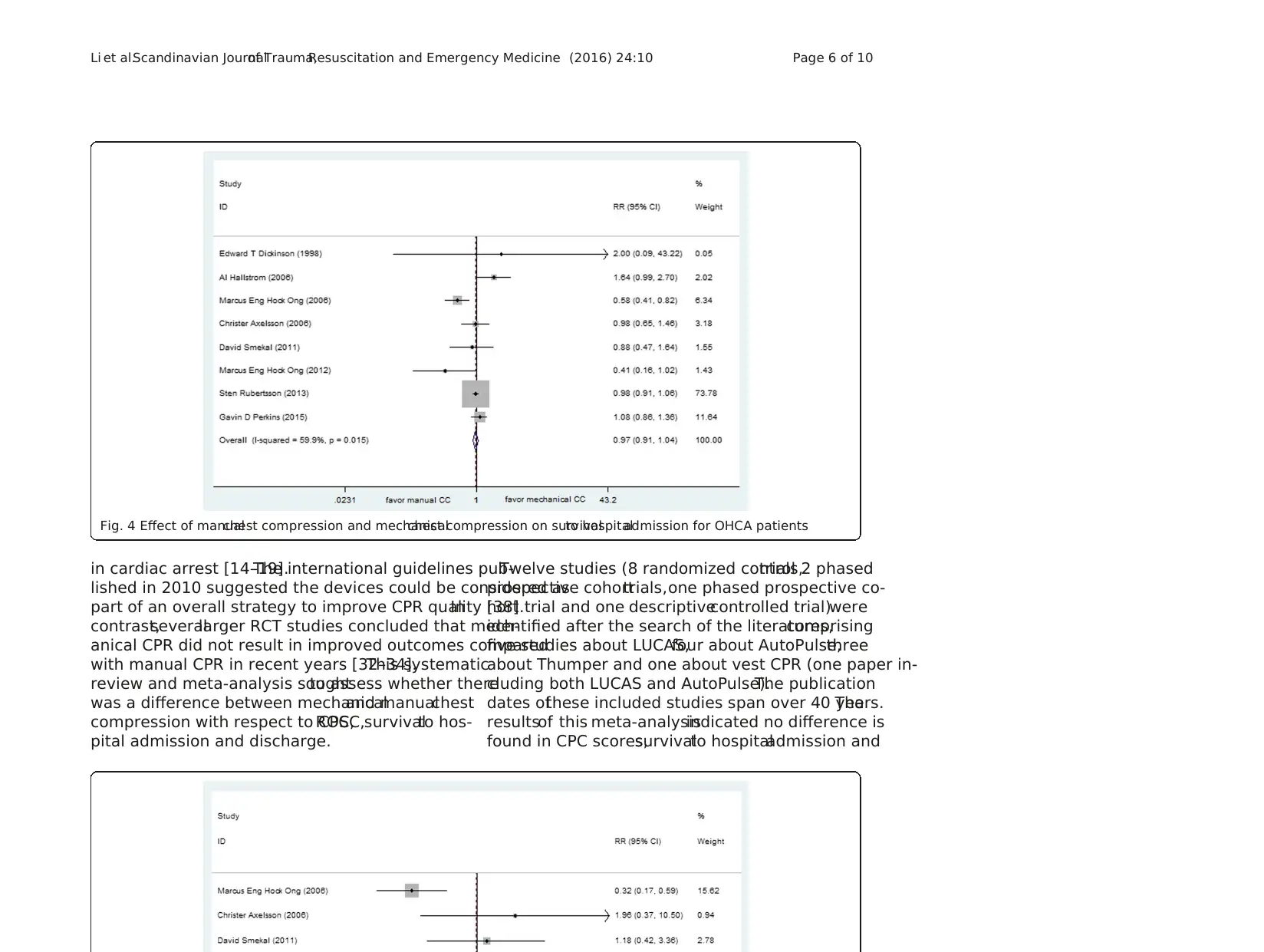
Survival to hospital admission
8 studies comprising a total of 9975 OHCA patients met
the selection criteria.Although an analysiscombining
multi-mechanicalCPR devices produced an insignificant
treatmenteffect(with an RR 0.97 [95 % CI,0.91,1.04])
(Fig.4).The I2 statistic was 59.9 %,the statistical hetero-
geneity ofpooling results were thoughtto be of rele-
vance to differenttypesof device (AutoPulse,LUCAS
and Thumper).Furthermore,when device type was ana-
lyzed separately,the treatment effect was not significant
for AutoPulse (RR 0.97 [95 % CI,0.91,1.02]),for LUCAS
(RR 1.02 [95 % CI,0.94,1.11]) and for Thumper (0/7:1/
10) with manual chest compression,respectively.
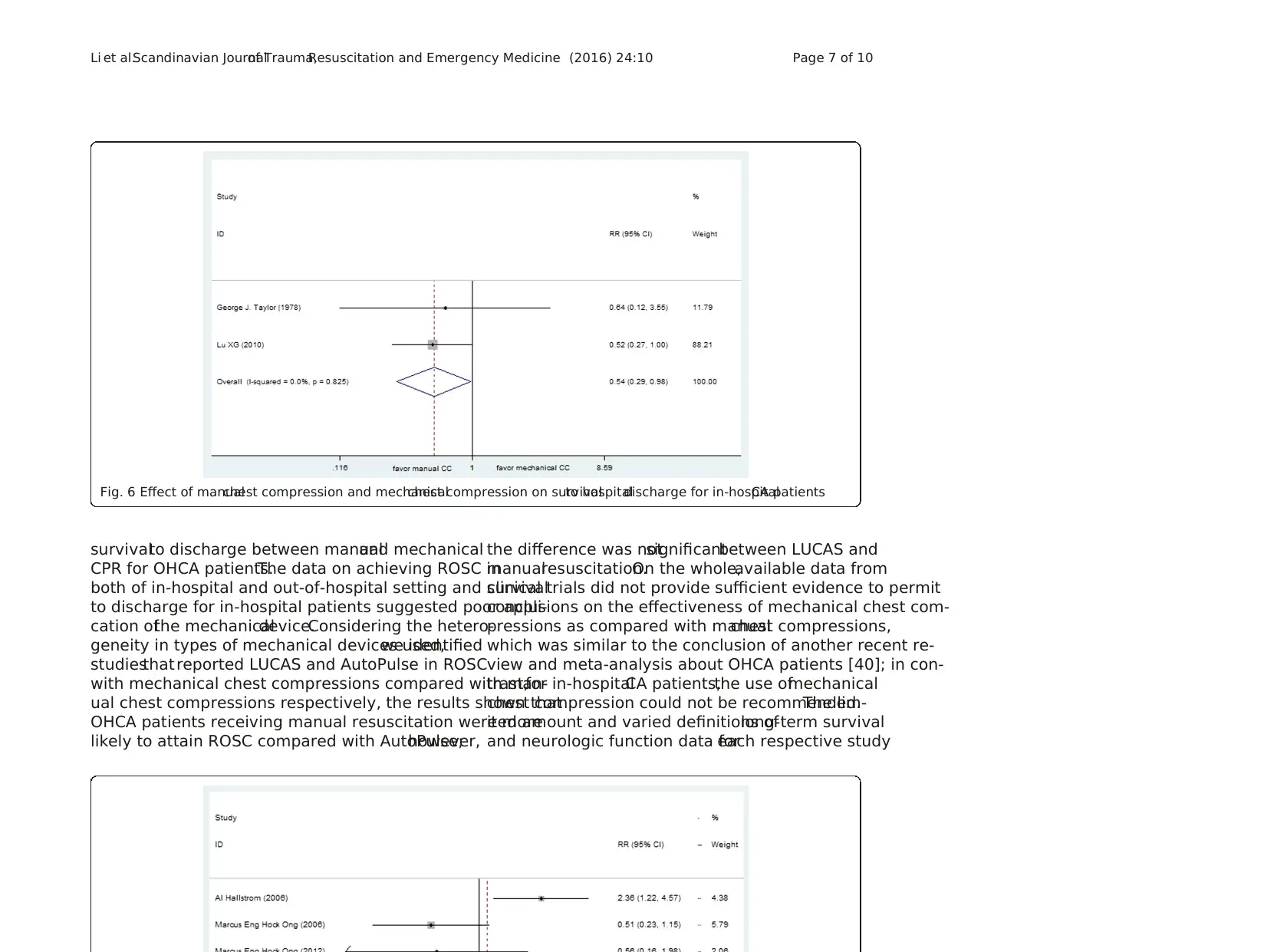
Survival to hospital discharge
Severalincluded studiesreported data ofsurvivalto
hospitaldischarge,including 7 out-of-hospitalstudies
(N = 4688)and 2 in-hospitalstudies(N = 200).Data
reported in the out-of-hospitalstudies suggested non-
significant effect between manualand mechanicalcom-
pressions (RR 0.99,[95 % CI 0.82,1.18]),although the
in-hospitalstudiessuggested increased relativeharm
with mechanicalcompressions (RR 0.54,[95 % CI 0.29,
0.98])(Figs.5 and 6). Considering the heterogeneity
due to the type of mechanicaldevice in out-of-hospital
studies (I2 = 70.8 %),subgroup analyses were conducted
to evaluate the effectof differentCPR device on pa-
tientswith OHCA. The use of any type mechanical
chest compression had no significant differences in ra-
tio of survival to discharge with manual chest compres-
sion (LUCAS,RR 1.09 [95 % CI,0.99,1.19];AutoPulse,
RR 0.96 [95 % CI,0.89,1.03];Thumper,0/7:0/10).
CPC
Six trialincluding 8825 OHCA patients provided data
for the CPC score of this review.The pooled meta-
analytic results for good neurologicalfunction (defined
as a CPC score of one or two) at hospital discharge were
not significant(with an RR 1.11 [95 % CI,0.95,1.30]),
which indicated asimilar treatmenteffectfor good
neurologicaloutcome with the use ofmechanicaland
manualchestcompressions (Fig.7). The statisticalhet-
Fig. 1 Flow diagram of search criteria and reason for exclusion
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 3 of 10
CPR) applied in the 12 studies.
ROSC
ROSC was reported in 10 studies (totalN = 8886),in-
cluding 7 out-of-hospitalstudies(N = 8590)and 3 in-
hospitalstudies (N = 296).These data were entered into
a forestplot respectively,resulting in risk ratio of0.87
(95 % CI,0.81,0.94) for OHCA patients and 0.71 (95 %
CI, 0.53,0.97) for in-hospital CA patients (Figs.2 and 3).
The results suggested harm with mechanicalchest com-
Survival to hospital admission
8 studies comprising a total of 9975 OHCA patients met
the selection criteria.Although an analysiscombining
multi-mechanicalCPR devices produced an insignificant
treatmenteffect(with an RR 0.97 [95 % CI,0.91,1.04])
(Fig.4).The I2 statistic was 59.9 %,the statistical hetero-
geneity ofpooling results were thoughtto be of rele-
vance to differenttypesof device (AutoPulse,LUCAS
and Thumper).Furthermore,when device type was ana-
lyzed separately,the treatment effect was not significant
for AutoPulse (RR 0.97 [95 % CI,0.91,1.02]),for LUCAS
(RR 1.02 [95 % CI,0.94,1.11]) and for Thumper (0/7:1/
10) with manual chest compression,respectively.
Survival to hospital discharge
Severalincluded studiesreported data ofsurvivalto
hospitaldischarge,including 7 out-of-hospitalstudies
(N = 4688)and 2 in-hospitalstudies(N = 200).Data
reported in the out-of-hospitalstudies suggested non-
significant effect between manualand mechanicalcom-
pressions (RR 0.99,[95 % CI 0.82,1.18]),although the
in-hospitalstudiessuggested increased relativeharm
with mechanicalcompressions (RR 0.54,[95 % CI 0.29,
0.98])(Figs.5 and 6). Considering the heterogeneity
due to the type of mechanicaldevice in out-of-hospital
studies (I2 = 70.8 %),subgroup analyses were conducted
to evaluate the effectof differentCPR device on pa-
tientswith OHCA. The use of any type mechanical
chest compression had no significant differences in ra-
tio of survival to discharge with manual chest compres-
sion (LUCAS,RR 1.09 [95 % CI,0.99,1.19];AutoPulse,
RR 0.96 [95 % CI,0.89,1.03];Thumper,0/7:0/10).
CPC
Six trialincluding 8825 OHCA patients provided data
for the CPC score of this review.The pooled meta-
analytic results for good neurologicalfunction (defined
as a CPC score of one or two) at hospital discharge were
not significant(with an RR 1.11 [95 % CI,0.95,1.30]),
which indicated asimilar treatmenteffectfor good
neurologicaloutcome with the use ofmechanicaland
manualchestcompressions (Fig.7). The statisticalhet-
Fig. 1 Flow diagram of search criteria and reason for exclusion
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 3 of 10
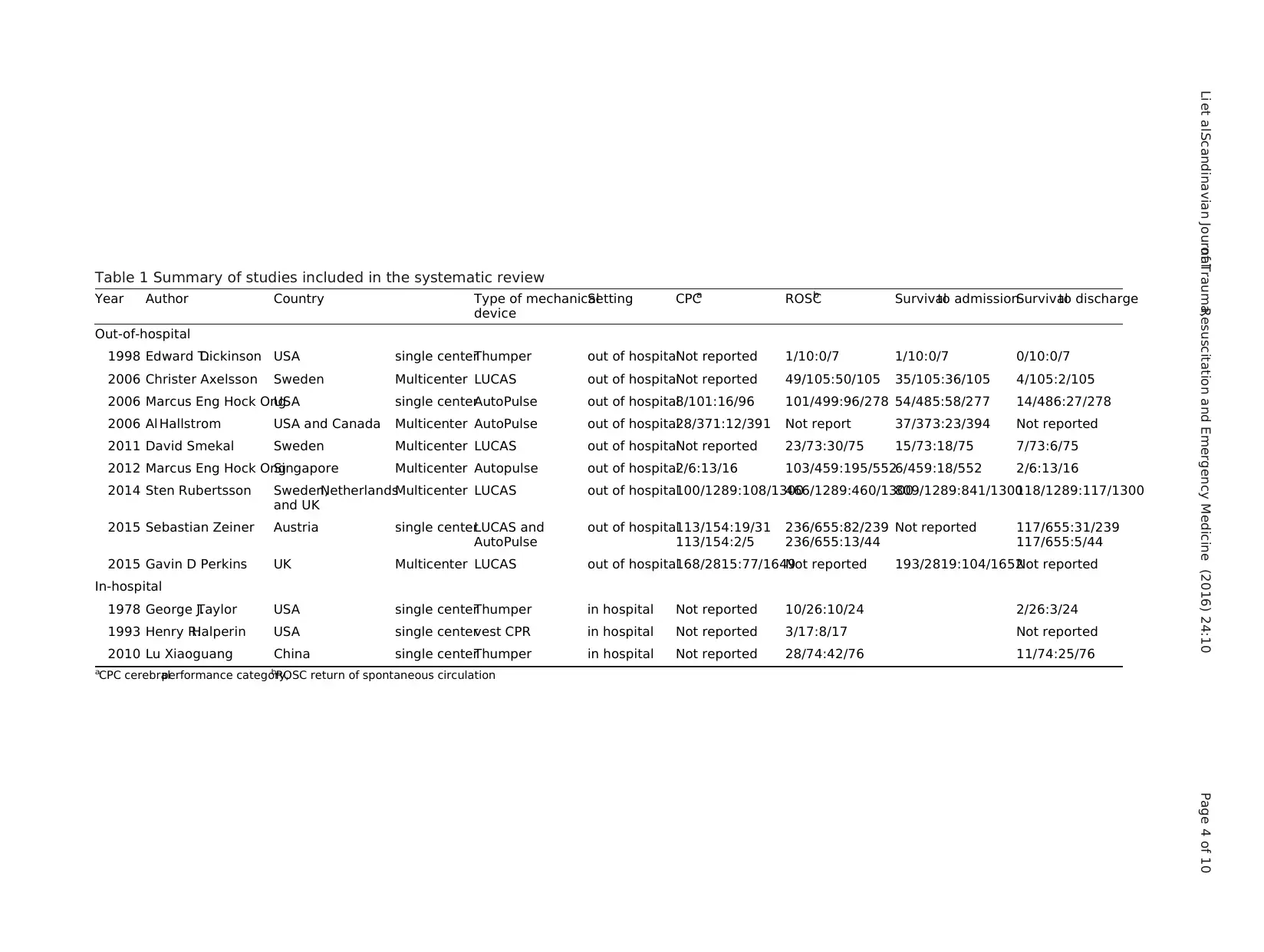
Table 1 Summary of studies included in the systematic review
Year Author Country Type of mechanical
device
Setting CPCa ROSCb Survivalto admissionSurvivalto discharge
Out-of-hospital
1998 Edward T.Dickinson USA single centerThumper out of hospitalNot reported 1/10:0/7 1/10:0/7 0/10:0/7
2006 Christer Axelsson Sweden Multicenter LUCAS out of hospitalNot reported 49/105:50/105 35/105:36/105 4/105:2/105
2006 Marcus Eng Hock OngUSA single centerAutoPulse out of hospital8/101:16/96 101/499:96/278 54/485:58/277 14/486:27/278
2006 Al Hallstrom USA and Canada Multicenter AutoPulse out of hospital28/371:12/391 Not report 37/373:23/394 Not reported
2011 David Smekal Sweden Multicenter LUCAS out of hospitalNot reported 23/73:30/75 15/73:18/75 7/73:6/75
2012 Marcus Eng Hock OngSingapore Multicenter Autopulse out of hospital2/6:13/16 103/459:195/5526/459:18/552 2/6:13/16
2014 Sten Rubertsson Sweden,Netherlands
and UK
Multicenter LUCAS out of hospital100/1289:108/1300466/1289:460/1300809/1289:841/1300118/1289:117/1300
2015 Sebastian Zeiner Austria single centerLUCAS and
AutoPulse
out of hospital113/154:19/31
113/154:2/5
236/655:82/239
236/655:13/44
Not reported 117/655:31/239
117/655:5/44
2015 Gavin D Perkins UK Multicenter LUCAS out of hospital168/2815:77/1649Not reported 193/2819:104/1652Not reported
In-hospital
1978 George J.Taylor USA single centerThumper in hospital Not reported 10/26:10/24 2/26:3/24
1993 Henry R.Halperin USA single centervest CPR in hospital Not reported 3/17:8/17 Not reported
2010 Lu Xiaoguang China single centerThumper in hospital Not reported 28/74:42/76 11/74:25/76
aCPC cerebralperformance category,bROSC return of spontaneous circulation
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 4 of 10
Year Author Country Type of mechanical
device
Setting CPCa ROSCb Survivalto admissionSurvivalto discharge
Out-of-hospital
1998 Edward T.Dickinson USA single centerThumper out of hospitalNot reported 1/10:0/7 1/10:0/7 0/10:0/7
2006 Christer Axelsson Sweden Multicenter LUCAS out of hospitalNot reported 49/105:50/105 35/105:36/105 4/105:2/105
2006 Marcus Eng Hock OngUSA single centerAutoPulse out of hospital8/101:16/96 101/499:96/278 54/485:58/277 14/486:27/278
2006 Al Hallstrom USA and Canada Multicenter AutoPulse out of hospital28/371:12/391 Not report 37/373:23/394 Not reported
2011 David Smekal Sweden Multicenter LUCAS out of hospitalNot reported 23/73:30/75 15/73:18/75 7/73:6/75
2012 Marcus Eng Hock OngSingapore Multicenter Autopulse out of hospital2/6:13/16 103/459:195/5526/459:18/552 2/6:13/16
2014 Sten Rubertsson Sweden,Netherlands
and UK
Multicenter LUCAS out of hospital100/1289:108/1300466/1289:460/1300809/1289:841/1300118/1289:117/1300
2015 Sebastian Zeiner Austria single centerLUCAS and
AutoPulse
out of hospital113/154:19/31
113/154:2/5
236/655:82/239
236/655:13/44
Not reported 117/655:31/239
117/655:5/44
2015 Gavin D Perkins UK Multicenter LUCAS out of hospital168/2815:77/1649Not reported 193/2819:104/1652Not reported
In-hospital
1978 George J.Taylor USA single centerThumper in hospital Not reported 10/26:10/24 2/26:3/24
1993 Henry R.Halperin USA single centervest CPR in hospital Not reported 3/17:8/17 Not reported
2010 Lu Xiaoguang China single centerThumper in hospital Not reported 28/74:42/76 11/74:25/76
aCPC cerebralperformance category,bROSC return of spontaneous circulation
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 4 of 10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CA (P = 0.64 for OHCA and P = 0.888 for in hospital CA
respectively).
Discussion
The goalof CPR treatment for CA patients is to achieve
ROSC and normalneurologicalfunction as early as pos-
sible while minimizing end-organ damage and dysfunction
in the interim.Severalanimaland human studies have
demonstrated an inverse relationship between poor chest
compression quality and short-term survival [35–37].The
high quality of CPR has been emphasized in the American
Heart Association(AHA) guidelinesand emergency
cardiovascular care [38].However,Hightower etal. ob-
served significant fatigue after only one minute ofchest
compressions on a mannequin.Correctchestcompres-
sions were performed 92 % of the time during the first mi-
nute,67.1 % during the second minute and 39.2 % during
the third minute [39].Rescuer fatigue has been identified
as an importantfactor to poor CPR quality.The use of
mechanical chest compression devices has been proposed
to provide high-quality chestcompressions withoutthe
interruptions and fatigue,meanwhile the resuscitation ef-
forts can be facilitated by freeing the hands of the rescuer
from manualchestcompression.For the same reasons,
safety increases during transportin a moving ambulance
for OHCA patients.Some data from animaland human
observational studies suggested that mechanical chest com-
pressions might be superior to manual chest compressions
Fig. 2 Effect of manualchest compression and mechanicalchest compression on ROSC for OHCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 5 of 10
respectively).
Discussion
The goalof CPR treatment for CA patients is to achieve
ROSC and normalneurologicalfunction as early as pos-
sible while minimizing end-organ damage and dysfunction
in the interim.Severalanimaland human studies have
demonstrated an inverse relationship between poor chest
compression quality and short-term survival [35–37].The
high quality of CPR has been emphasized in the American
Heart Association(AHA) guidelinesand emergency
cardiovascular care [38].However,Hightower etal. ob-
served significant fatigue after only one minute ofchest
compressions on a mannequin.Correctchestcompres-
sions were performed 92 % of the time during the first mi-
nute,67.1 % during the second minute and 39.2 % during
the third minute [39].Rescuer fatigue has been identified
as an importantfactor to poor CPR quality.The use of
mechanical chest compression devices has been proposed
to provide high-quality chestcompressions withoutthe
interruptions and fatigue,meanwhile the resuscitation ef-
forts can be facilitated by freeing the hands of the rescuer
from manualchestcompression.For the same reasons,
safety increases during transportin a moving ambulance
for OHCA patients.Some data from animaland human
observational studies suggested that mechanical chest com-
pressions might be superior to manual chest compressions
Fig. 2 Effect of manualchest compression and mechanicalchest compression on ROSC for OHCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 5 of 10
in cardiac arrest [14–19].The international guidelines pub-
lished in 2010 suggested the devices could be considered as
part of an overall strategy to improve CPR quality [38].In
contrast,severallarger RCT studies concluded that mech-
anical CPR did not result in improved outcomes compared
with manual CPR in recent years [32–34].This systematic
review and meta-analysis soughtto assess whether there
was a difference between mechanicaland manualchest
compression with respect to CPC,ROSC,survivalto hos-
pital admission and discharge.
Twelve studies (8 randomized controltrials,2 phased
prospective cohorttrials,one phased prospective co-
hort trial and one descriptivecontrolled trial)were
identified after the search of the literatures,comprising
five studies about LUCAS,four about AutoPulse,three
about Thumper and one about vest CPR (one paper in-
cluding both LUCAS and AutoPulse).The publication
dates ofthese included studies span over 40 years.The
resultsof this meta-analysisindicated no difference is
found in CPC scores,survivalto hospitaladmission and
Fig. 4 Effect of manualchest compression and mechanicalchest compression on survivalto hospitaladmission for OHCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 6 of 10
lished in 2010 suggested the devices could be considered as
part of an overall strategy to improve CPR quality [38].In
contrast,severallarger RCT studies concluded that mech-
anical CPR did not result in improved outcomes compared
with manual CPR in recent years [32–34].This systematic
review and meta-analysis soughtto assess whether there
was a difference between mechanicaland manualchest
compression with respect to CPC,ROSC,survivalto hos-
pital admission and discharge.
Twelve studies (8 randomized controltrials,2 phased
prospective cohorttrials,one phased prospective co-
hort trial and one descriptivecontrolled trial)were
identified after the search of the literatures,comprising
five studies about LUCAS,four about AutoPulse,three
about Thumper and one about vest CPR (one paper in-
cluding both LUCAS and AutoPulse).The publication
dates ofthese included studies span over 40 years.The
resultsof this meta-analysisindicated no difference is
found in CPC scores,survivalto hospitaladmission and
Fig. 4 Effect of manualchest compression and mechanicalchest compression on survivalto hospitaladmission for OHCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 6 of 10
survivalto discharge between manualand mechanical
CPR for OHCA patients.The data on achieving ROSC in
both of in-hospital and out-of-hospital setting and survival
to discharge for in-hospital patients suggested poor appli-
cation ofthe mechanicaldevice.Considering the hetero-
geneity in types of mechanical devices used,we identified
studiesthatreported LUCAS and AutoPulse in ROSC
with mechanical chest compressions compared with man-
ual chest compressions respectively, the results shown that
OHCA patients receiving manual resuscitation were more
likely to attain ROSC compared with AutoPulse;however,
the difference was notsignificantbetween LUCAS and
manualresuscitation.On the whole,available data from
clinical trials did not provide sufficient evidence to permit
conclusions on the effectiveness of mechanical chest com-
pressions as compared with manualchest compressions,
which was similar to the conclusion of another recent re-
view and meta-analysis about OHCA patients [40]; in con-
trast,for in-hospitalCA patients,the use ofmechanical
chest compression could not be recommended.The lim-
ited amount and varied definitions oflong-term survival
and neurologic function data foreach respective study
Fig. 6 Effect of manualchest compression and mechanicalchest compression on survivalto hospitaldischarge for in-hospitalCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 7 of 10
CPR for OHCA patients.The data on achieving ROSC in
both of in-hospital and out-of-hospital setting and survival
to discharge for in-hospital patients suggested poor appli-
cation ofthe mechanicaldevice.Considering the hetero-
geneity in types of mechanical devices used,we identified
studiesthatreported LUCAS and AutoPulse in ROSC
with mechanical chest compressions compared with man-
ual chest compressions respectively, the results shown that
OHCA patients receiving manual resuscitation were more
likely to attain ROSC compared with AutoPulse;however,
the difference was notsignificantbetween LUCAS and
manualresuscitation.On the whole,available data from
clinical trials did not provide sufficient evidence to permit
conclusions on the effectiveness of mechanical chest com-
pressions as compared with manualchest compressions,
which was similar to the conclusion of another recent re-
view and meta-analysis about OHCA patients [40]; in con-
trast,for in-hospitalCA patients,the use ofmechanical
chest compression could not be recommended.The lim-
ited amount and varied definitions oflong-term survival
and neurologic function data foreach respective study
Fig. 6 Effect of manualchest compression and mechanicalchest compression on survivalto hospitaldischarge for in-hospitalCA patients
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 7 of 10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
prohibited the use of the data as the outcome variable in
this meta-analysis.
Many factors affectthe chances ofsurvivalafter car-
diac arrest,including early recognition of arrest,effective
cardiopulmonaryresuscitationand defibrillation,and
post-resuscitation care.A criticalissue is the delay be-
tween collapseand the startof the intervention.For
OHCA patients,witnessed CA receiving bystander basic
life supportmightimprove outcome [41].One of these
hypothesesis that interruptionsin CPR during device
deployment could cause reduced cardiac and cerebral per-
fusion [1].It is important to reduce the intervalbetween
collapse and the startof chestcompression.However,
there will always be a delay from the arrival of the rescuer
to setting up the equipment and giving the first treatment
accordingto field conditions,which might increase
cardiac instability and impaircerebralmicrocirculation.
Secondly,severalstudies reported that they failed to find
any significant difference between manual and mechanical
in their outcome ofsurvivalor survivalto discharge.A
possibleexplanation fortheseunexpected resultsad-
vanced by the authors is a Hawthorne effect for manual
CPR,which means a type of reactivity in medical rescuers
modify or improve an aspect of their behavior in response
to their awareness ofbeing observed [42,43].Almost all
of the included studies did not have the quality ofCPR
monitoring in place at the time,these data were not col-
lected orreported specificson how manualCPR was
performed in the control group.Although considering the
Hawthorne effect,the meta-analysis was unable to show
any superiority ofmechanicaldevice,which mean the
mechanicalchestcompression mightnot be better than
high-quality manualCPR. Mechanicalchest compression
should notbe seen asa replacementfor high quality
Table 2 Main quality assessment of included studies
Year Author Study design Description of
randomization
Allocation
concealment
Description of
withdrawals
Blinding outcome
assessment
1978 George J.Taylor RCT + – – –
1993 Henry R.Halperin RCT + – – –
1998 Edward T.Dickinson RCT + – + –
Fig. 9 Funnelplot for publication bias for in-hospitalCA studiesFig. 8 Funnelplot for publication bias for OHCA studies
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 8 of 10
this meta-analysis.
Many factors affectthe chances ofsurvivalafter car-
diac arrest,including early recognition of arrest,effective
cardiopulmonaryresuscitationand defibrillation,and
post-resuscitation care.A criticalissue is the delay be-
tween collapseand the startof the intervention.For
OHCA patients,witnessed CA receiving bystander basic
life supportmightimprove outcome [41].One of these
hypothesesis that interruptionsin CPR during device
deployment could cause reduced cardiac and cerebral per-
fusion [1].It is important to reduce the intervalbetween
collapse and the startof chestcompression.However,
there will always be a delay from the arrival of the rescuer
to setting up the equipment and giving the first treatment
accordingto field conditions,which might increase
cardiac instability and impaircerebralmicrocirculation.
Secondly,severalstudies reported that they failed to find
any significant difference between manual and mechanical
in their outcome ofsurvivalor survivalto discharge.A
possibleexplanation fortheseunexpected resultsad-
vanced by the authors is a Hawthorne effect for manual
CPR,which means a type of reactivity in medical rescuers
modify or improve an aspect of their behavior in response
to their awareness ofbeing observed [42,43].Almost all
of the included studies did not have the quality ofCPR
monitoring in place at the time,these data were not col-
lected orreported specificson how manualCPR was
performed in the control group.Although considering the
Hawthorne effect,the meta-analysis was unable to show
any superiority ofmechanicaldevice,which mean the
mechanicalchestcompression mightnot be better than
high-quality manualCPR. Mechanicalchest compression
should notbe seen asa replacementfor high quality
Table 2 Main quality assessment of included studies
Year Author Study design Description of
randomization
Allocation
concealment
Description of
withdrawals
Blinding outcome
assessment
1978 George J.Taylor RCT + – – –
1993 Henry R.Halperin RCT + – – –
1998 Edward T.Dickinson RCT + – + –
Fig. 9 Funnelplot for publication bias for in-hospitalCA studiesFig. 8 Funnelplot for publication bias for OHCA studies
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 8 of 10
manualCPR, but rather a supplementaltreatment in an
overall strategy for treating CA patients.Thirdly,it is also
increasingly recognized that although defibrillation is the
definitive treatment for ventricular fibrillation,its success
is also dependent on adequate circulation [44].Thus,ef-
fective CPR is often a prerequisite for effective defibrilla-
tion. Patientspresenting in ventricularfibrillation have
relatively high survivability with early defibrillation [45]. In
practice,the device is usually applied in patients who do
not respond to initial defibrillation and require prolonged
CPR. Patients in prolonged cardiac arrest who are success-
fully resuscitated would beexpected to havepoorer
neurologicalstatus on discharge compared to those who
respond immediately.Finally,managementof patients
following resuscitation from CA is complex and requires
specialized institutions capable of providing advanced care
therapies.Patientswith ROSC are treated with mild
hypothermia to 32 ~ 34 °C for 24 h,if no contraindica-
tions are present.Acute coronary angiography is consid-
ered during the first 48 h and, if indicated, a percutaneous
coronary intervention is performed.Managing these pa-
tients achieving ROSC is challenging and requires a struc-
tured approach.Clinical recommendationsfor CPR,
including the nature ofmanualchest compression,have
changed drastically over the past 10 to 15 years [38].The
dates ofthese included studies span over four decades,
strategy of post-resuscitation care for ROSC patients has
improved.Those might influence the survival of discharge
and neurological function over years.
In this meta-analysis,there were some limitations.The
first limitation wasthat some ofthe included studies
were prospectiveobservationaltrials or phased con-
trolled trials.It was possible that selection bias could be
introduced thatthe paramedics tended to have a lower
threshold for initiation of resuscitation.A second limita-
tion was that none of studies were blinded.Because the
rescuerswho decided when to initiate CPR were not
blinded,introducing the possibility of rescuers preferen-
tialapplication of a device to patients thought to have a
very poor prognosis in the hope thatuse ofthe device
might lead to better outcomes than attained with stand-
ard care.Thirdly,these included studies were conducted
Conclusions
In this systematic review,the combined meta-analysis of
mechanicalchestcompression devicescompared with
manualchestcompressionsshown a betterresultwith
manual chest compression in ROSC rates for both out-of-
hospitaland in-hospitalCA patients and survivalof
discharge for in-hospital CA patients. When analyzed sep-
arately, only AutoPulse was found to be inferior to manual
chest compressions with ratio of ROSC.We believed that
the mechanical chest compression should not be seen as a
replacement for manualCPR, but rather a supplemental
treatment in an overall strategy for treating CA patients.
Abbreviations
CA:cardiac arrest;ROSC:return of spontaneous circulation;
CPR:cardiopulmonary resuscitation;CPC:CerebralPerformance Category;
LDBs:load-distributing bands;RR:risk ratio;CI:confidence interval.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
JX and LH conceived the study,designed the trial,and obtained research
funding;WD and YY collected and analyses the data;JX supervised the
project with the advise of ZX;JX,LH and WD edited the manuscript;JX took
responsibility for the paper as a whole.Allauthors discussed the results and
implications and commented on the manuscript at allstages.JX is the
corresponding author of this paper.Allauthors read and approved the final
manuscript.
Acknowledgments
This study was supported by grant from the NSFC (81372022) and Medical
Scientific Research Foundation of Guangdong Province,China (B2014112).
The funders had no role in the study design,data collection,analysis,
decision to publish,or the preparation of the manuscript.
Author details
1Department of Emergency,The First Affiliated Hospitalof Sun Yat-Sen
University,58 Zhongshan 2nd Road,Guangzhou,Guangdong 510080,China.
2Department of Organ Transplantation,The First Affiliated Hospitalof Sun
Yat-Sen University,Guangzhou 510080,China.
Received:12 November 2015 Accepted:21 January 2016
References
1. Ewy GA.Cardiocerebralresuscitation:the new cardiopulmonary
resuscitation.Circulation.2005;111(16):2134–42.
2. Kern KB,Carter AB,Showen RL,Voorhees 3rd WD,Babbs CF,Tacker WA,et al.
Twenty-four hour survival in a canine model of cardiac arrest comparing three
methods of manual cardiopulmonary resuscitation.J Am Coll Cardiol.1986;7:
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 9 of 10
overall strategy for treating CA patients.Thirdly,it is also
increasingly recognized that although defibrillation is the
definitive treatment for ventricular fibrillation,its success
is also dependent on adequate circulation [44].Thus,ef-
fective CPR is often a prerequisite for effective defibrilla-
tion. Patientspresenting in ventricularfibrillation have
relatively high survivability with early defibrillation [45]. In
practice,the device is usually applied in patients who do
not respond to initial defibrillation and require prolonged
CPR. Patients in prolonged cardiac arrest who are success-
fully resuscitated would beexpected to havepoorer
neurologicalstatus on discharge compared to those who
respond immediately.Finally,managementof patients
following resuscitation from CA is complex and requires
specialized institutions capable of providing advanced care
therapies.Patientswith ROSC are treated with mild
hypothermia to 32 ~ 34 °C for 24 h,if no contraindica-
tions are present.Acute coronary angiography is consid-
ered during the first 48 h and, if indicated, a percutaneous
coronary intervention is performed.Managing these pa-
tients achieving ROSC is challenging and requires a struc-
tured approach.Clinical recommendationsfor CPR,
including the nature ofmanualchest compression,have
changed drastically over the past 10 to 15 years [38].The
dates ofthese included studies span over four decades,
strategy of post-resuscitation care for ROSC patients has
improved.Those might influence the survival of discharge
and neurological function over years.
In this meta-analysis,there were some limitations.The
first limitation wasthat some ofthe included studies
were prospectiveobservationaltrials or phased con-
trolled trials.It was possible that selection bias could be
introduced thatthe paramedics tended to have a lower
threshold for initiation of resuscitation.A second limita-
tion was that none of studies were blinded.Because the
rescuerswho decided when to initiate CPR were not
blinded,introducing the possibility of rescuers preferen-
tialapplication of a device to patients thought to have a
very poor prognosis in the hope thatuse ofthe device
might lead to better outcomes than attained with stand-
ard care.Thirdly,these included studies were conducted
Conclusions
In this systematic review,the combined meta-analysis of
mechanicalchestcompression devicescompared with
manualchestcompressionsshown a betterresultwith
manual chest compression in ROSC rates for both out-of-
hospitaland in-hospitalCA patients and survivalof
discharge for in-hospital CA patients. When analyzed sep-
arately, only AutoPulse was found to be inferior to manual
chest compressions with ratio of ROSC.We believed that
the mechanical chest compression should not be seen as a
replacement for manualCPR, but rather a supplemental
treatment in an overall strategy for treating CA patients.
Abbreviations
CA:cardiac arrest;ROSC:return of spontaneous circulation;
CPR:cardiopulmonary resuscitation;CPC:CerebralPerformance Category;
LDBs:load-distributing bands;RR:risk ratio;CI:confidence interval.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
JX and LH conceived the study,designed the trial,and obtained research
funding;WD and YY collected and analyses the data;JX supervised the
project with the advise of ZX;JX,LH and WD edited the manuscript;JX took
responsibility for the paper as a whole.Allauthors discussed the results and
implications and commented on the manuscript at allstages.JX is the
corresponding author of this paper.Allauthors read and approved the final
manuscript.
Acknowledgments
This study was supported by grant from the NSFC (81372022) and Medical
Scientific Research Foundation of Guangdong Province,China (B2014112).
The funders had no role in the study design,data collection,analysis,
decision to publish,or the preparation of the manuscript.
Author details
1Department of Emergency,The First Affiliated Hospitalof Sun Yat-Sen
University,58 Zhongshan 2nd Road,Guangzhou,Guangdong 510080,China.
2Department of Organ Transplantation,The First Affiliated Hospitalof Sun
Yat-Sen University,Guangzhou 510080,China.
Received:12 November 2015 Accepted:21 January 2016
References
1. Ewy GA.Cardiocerebralresuscitation:the new cardiopulmonary
resuscitation.Circulation.2005;111(16):2134–42.
2. Kern KB,Carter AB,Showen RL,Voorhees 3rd WD,Babbs CF,Tacker WA,et al.
Twenty-four hour survival in a canine model of cardiac arrest comparing three
methods of manual cardiopulmonary resuscitation.J Am Coll Cardiol.1986;7:
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 9 of 10
8. Foo NP,Chang JH,Su SB,Lin HJ,Chen KT,Cheng CF,et al.A stabilization
device to improve the quality of cardiopulmonary resuscitation during
ambulance transportation:a randomized crossover trial.Resuscitation.2013;
84:1579–84.
9. Abella BS,Alvarado JP,Myklebust H,Edelson DP,Barry A,O’Hearn N,et al.
Quality of cardiopulmonary resuscitation during in-hospitalcardiac arrest.J
Am Med Assoc.2005;293(3):305–10.
10. Abella BS,Sandbo N,Vassilatos P,Alvarado JP,O’Hearn N,Wigder HN,et al.
Chest compression rates during cardiopulmonary resuscitation are
suboptimal:a prospective study during in-hospitalcardiac arrest.Circulation.
2005;111(4):428–34.
11. Ko PC,Chen WJ,Lin CH,Ma MH,Lin FY.Evaluating the quality of
prehospitalcardiopulmonary resuscitation by reviewing automated external
defibrillator records and survivalfor out-of-hospitalwitnessed arrests.
Resuscitation.2005;64(2):163–9.
12. Wik L,Kramer-Johansen J,Myklebust H,Sørebø H,Svensson L,Fellows B,
et al.Quality of cardiopulmonary resuscitation during out-of-hospitalcardiac
arrest.J Am Med Assoc.2005;293(3):299–304.
13. Lurie K.Mechanicaldevices for cardiopulmonary resuscitation:an update.
Emerg Med Clin North Am.2002;20(4):771–84.
14. Ikeno F,Kaneda H,Hongo Y,Sakanoue Y,Nolasco C,EmamiS,et al.
Augmentation of tissue perfusion by a novelcompression device increases
neurologicalintact survivalin porcine modelof prolonged cardiac arrest.
Resuscitation.2006;68:109–18.
15. Halperin H,Paradis N,Ornato J.Cardiopulmonary resuscitation with a novel
chest compression device in a porcine modelof cardiac arrest:improved
hemodynamics and mechanisms.J Am CollCardiol.2004;44:2214–20.
16. Casner M,Andersen D,Isaacs SM.The impact of a new CPR assist device on
rate of return of spontaneous circulation in out-of-hospitalcardiac arrest.
Prehosp Emerg Care.2005;9:61–7.
17. Lewis RJ,Niemann JT.Manualvs device-assisted CPR:reconciling apparently
contradictory results.J Am Med Assoc.2006;295(22):2661–4.
18. Swanson M,PoniatowskiM,O’Keefe M,Shedd JG.Effect of a CPR assist
device on survivalto emergency department arrivalin out of hospital
cardiac arrest.Circulation.2005;112(17):U1186.
19. Swanson M,PoniatowskiM,O’Keefe M,Springer P.A CPR assist device
increased emergency department admission and end tidalcarbon dioxide
partialpressures during treatment of out of hospitalcardiac arrest.
Circulation.2006;114(18):554.
20. WestfallM,Krantz S,Mullin C,Kaufman C.Mechanicalversus manualchest
compressions in out-of-hospitalcardiac arrest:a meta-analysis.Crit Care
Med.2013;41(7):1782–9.
21. Ong ME,Mackey KE,Zhang ZC,Tanaka H,Ma MH,Swor R.MechanicalCPR
devices compared to manualCPR during out-of-hospitalcardiac arrest and
ambulance transport:a systematic review.Scand J Trauma Resusc Emerg
Med.2012;20:39.
22. Brooks SC,Hassan N,Bigham BL,Morrison LJ.Mechanicalversus manual
chest compressions for cardiac arrest.Cochrane Database Syst Rev.
2014;2:CD007260.
23. Dickinson ET,Verdile VP,Schneider RM,Salluzzo RF.Effectiveness of
mechanicalversus manualchest compressions in out-of-hospitalcardiac
arrest resuscitation:a pilot study.Am J Emerg Med.1998;16(3):289–92.
24. Halperin HR,Tsitlik JE,Gelfand M,Weisfeldt ML,Gruben KG,Levin HR.A
preliminary study of cardiopulmonary resuscitation by circumferential
compression of the chest with use of a pneumatic vest.N EnglJ Med.
1993;329(11):762–8.
EMS system for treatment of out-of-hospitalcardiac arrest-a pilot study.
Resuscitation.2006;71(1):47–55.
30. Hock Ong ME,Fook-Chong S,AnnathuraiA,Ang SH,Tiah L,Yong KL.
Improved neurologically intact survivalwith the use of an automated,load-
distributing band chest compression device for cardiac arrest presenting to
the emergency department.Crit Care.2012;16:R144.
31. Ong ME,Ornato JP,Edwards DP,Dhindsa HS,Best AM,Ines CS.Use of an
automated,load-distributing band chest compression device for out-of-
hospitalcardiac arrest resuscitation.J Am Med Assoc.2006;295(22):2629–37.
32. Zeiner S,Sulzgruber P,Datler P,Keferböck M,Poppe M,Lobmeyr E,et al.
Chest compression does not seem to improve outcome after out-of
hospitalcardiac arrest.A single center observationaltrial.Resuscitation.
2015;96:220–5.
33. Rubertsson S,Lindgren E,SmekalD,Ostlund O,Silfverstolpe J,Robert A,
et al.Mechanicalchest compressions and simultaneous defibrillation vs
conventionalcardiopulmonary resuscitation in out-of-hospitalcardiac arrest.
J Am Med Assoc.2014;311(1):53–61.
34. Perkins GD,LallR,Quinn T,Deakin CD,Cooke MW,Horton J,et al.
Mechanicalversus manualchest compression for out-of-hospitalcardiac
arrest (PARAMEDIC):a pragmatic,cluster randomised controlled trial.Lancet.
2015;385:947–55.
35. Kern KB,Hilwig RW,Berg RA,Sanders AB,Ewy GA.Importance of
continuous chest compressions during cardiopulmonary resuscitation:
improved outcome during a simulated single lay-rescuer scenario.
Circulation.2002;105(5):645–9.
36. Yu T,WeilMH,Tang W,Sun S,Klouche K,Povoas H,et al.Adverse
outcomes of interrupted precordialcompression during automated
defibrillation.Circulation.2002;106(3):368–72.
37. EftestolT,Sunde K,Steen PA.Effects of interrupting precordial
compressions on the calculated probability of defibrillation success during
out-of-hospitalcardiac arrest.Circulation.2002;105(19):2270–3.
38. Berg MD,Schexnayder SM,Chameides L,Terry M,Donoghue A,Hickey RW,
et al.Part 5:Adult Basic Life Support:2010 American Heart Association
guidelines for cardiopulmonary resuscitation and emergency cardiovascular
care.Circulation.2010;122 Suppl3:S685–705.
39. Hightower D,Thomas SH,Stone CK,Dunn K,March JA.Decay in quality of
closed-chest compressions over time.Ann Emerg Med.1995;26(3):300–3.
40. Gatesa S,Quinnb T,Deakinc CD,Blaire L,Coupera K,Perkins GD.Mechanical
chest compression for out of hospitalcardiac arrest:systematic review and
meta-analysis.Resuscitation.2015;94:91–7.
41. Herlitz J,Ekstrom L,Wennerblom B,Axelsson A,Bang A,Holmberg S.Effect
of bystander initiated cardiopulmonary resuscitation on ventricular
fibrillation and survivalafter witnessed cardiac arrest outside hospital.Br
Heart J.1994;72(5):408–12.
42. McCarney R,Warner J,Iliffe S,van Haselen R,Griffin M,Fisher P.The
Hawthorne Effect:a randomised,controlled trial.BMC Med Res Methodol.
2007;7:30.
43. Fox NS,Brennan JS,Chasen ST.Clinicalestimation of fetalweight and the
Hawthorne effect.Eur J Obstet GynecolReprod Biol.2008;141(2):111–4.
44. Valenzuela TD,Roe DJ,Cretin S,Spaite DW,Larsen MP.Estimating
effectiveness of cardiac arrest interventions:a logistic regression survival
model.Circulation.1997;96(10):3308–13.
45. Wik L,Hansen TB,Fylling F,Steen T,Vaagenes P,Auestad BH,et al.Delaying
defibrillation to give basic cardiopulmonary resuscitation to patients with
out-of-hospitalventricular fibrillation:a randomized trial.J Am Med Assoc.
2003;289:1389–95.
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 10 of 10
device to improve the quality of cardiopulmonary resuscitation during
ambulance transportation:a randomized crossover trial.Resuscitation.2013;
84:1579–84.
9. Abella BS,Alvarado JP,Myklebust H,Edelson DP,Barry A,O’Hearn N,et al.
Quality of cardiopulmonary resuscitation during in-hospitalcardiac arrest.J
Am Med Assoc.2005;293(3):305–10.
10. Abella BS,Sandbo N,Vassilatos P,Alvarado JP,O’Hearn N,Wigder HN,et al.
Chest compression rates during cardiopulmonary resuscitation are
suboptimal:a prospective study during in-hospitalcardiac arrest.Circulation.
2005;111(4):428–34.
11. Ko PC,Chen WJ,Lin CH,Ma MH,Lin FY.Evaluating the quality of
prehospitalcardiopulmonary resuscitation by reviewing automated external
defibrillator records and survivalfor out-of-hospitalwitnessed arrests.
Resuscitation.2005;64(2):163–9.
12. Wik L,Kramer-Johansen J,Myklebust H,Sørebø H,Svensson L,Fellows B,
et al.Quality of cardiopulmonary resuscitation during out-of-hospitalcardiac
arrest.J Am Med Assoc.2005;293(3):299–304.
13. Lurie K.Mechanicaldevices for cardiopulmonary resuscitation:an update.
Emerg Med Clin North Am.2002;20(4):771–84.
14. Ikeno F,Kaneda H,Hongo Y,Sakanoue Y,Nolasco C,EmamiS,et al.
Augmentation of tissue perfusion by a novelcompression device increases
neurologicalintact survivalin porcine modelof prolonged cardiac arrest.
Resuscitation.2006;68:109–18.
15. Halperin H,Paradis N,Ornato J.Cardiopulmonary resuscitation with a novel
chest compression device in a porcine modelof cardiac arrest:improved
hemodynamics and mechanisms.J Am CollCardiol.2004;44:2214–20.
16. Casner M,Andersen D,Isaacs SM.The impact of a new CPR assist device on
rate of return of spontaneous circulation in out-of-hospitalcardiac arrest.
Prehosp Emerg Care.2005;9:61–7.
17. Lewis RJ,Niemann JT.Manualvs device-assisted CPR:reconciling apparently
contradictory results.J Am Med Assoc.2006;295(22):2661–4.
18. Swanson M,PoniatowskiM,O’Keefe M,Shedd JG.Effect of a CPR assist
device on survivalto emergency department arrivalin out of hospital
cardiac arrest.Circulation.2005;112(17):U1186.
19. Swanson M,PoniatowskiM,O’Keefe M,Springer P.A CPR assist device
increased emergency department admission and end tidalcarbon dioxide
partialpressures during treatment of out of hospitalcardiac arrest.
Circulation.2006;114(18):554.
20. WestfallM,Krantz S,Mullin C,Kaufman C.Mechanicalversus manualchest
compressions in out-of-hospitalcardiac arrest:a meta-analysis.Crit Care
Med.2013;41(7):1782–9.
21. Ong ME,Mackey KE,Zhang ZC,Tanaka H,Ma MH,Swor R.MechanicalCPR
devices compared to manualCPR during out-of-hospitalcardiac arrest and
ambulance transport:a systematic review.Scand J Trauma Resusc Emerg
Med.2012;20:39.
22. Brooks SC,Hassan N,Bigham BL,Morrison LJ.Mechanicalversus manual
chest compressions for cardiac arrest.Cochrane Database Syst Rev.
2014;2:CD007260.
23. Dickinson ET,Verdile VP,Schneider RM,Salluzzo RF.Effectiveness of
mechanicalversus manualchest compressions in out-of-hospitalcardiac
arrest resuscitation:a pilot study.Am J Emerg Med.1998;16(3):289–92.
24. Halperin HR,Tsitlik JE,Gelfand M,Weisfeldt ML,Gruben KG,Levin HR.A
preliminary study of cardiopulmonary resuscitation by circumferential
compression of the chest with use of a pneumatic vest.N EnglJ Med.
1993;329(11):762–8.
EMS system for treatment of out-of-hospitalcardiac arrest-a pilot study.
Resuscitation.2006;71(1):47–55.
30. Hock Ong ME,Fook-Chong S,AnnathuraiA,Ang SH,Tiah L,Yong KL.
Improved neurologically intact survivalwith the use of an automated,load-
distributing band chest compression device for cardiac arrest presenting to
the emergency department.Crit Care.2012;16:R144.
31. Ong ME,Ornato JP,Edwards DP,Dhindsa HS,Best AM,Ines CS.Use of an
automated,load-distributing band chest compression device for out-of-
hospitalcardiac arrest resuscitation.J Am Med Assoc.2006;295(22):2629–37.
32. Zeiner S,Sulzgruber P,Datler P,Keferböck M,Poppe M,Lobmeyr E,et al.
Chest compression does not seem to improve outcome after out-of
hospitalcardiac arrest.A single center observationaltrial.Resuscitation.
2015;96:220–5.
33. Rubertsson S,Lindgren E,SmekalD,Ostlund O,Silfverstolpe J,Robert A,
et al.Mechanicalchest compressions and simultaneous defibrillation vs
conventionalcardiopulmonary resuscitation in out-of-hospitalcardiac arrest.
J Am Med Assoc.2014;311(1):53–61.
34. Perkins GD,LallR,Quinn T,Deakin CD,Cooke MW,Horton J,et al.
Mechanicalversus manualchest compression for out-of-hospitalcardiac
arrest (PARAMEDIC):a pragmatic,cluster randomised controlled trial.Lancet.
2015;385:947–55.
35. Kern KB,Hilwig RW,Berg RA,Sanders AB,Ewy GA.Importance of
continuous chest compressions during cardiopulmonary resuscitation:
improved outcome during a simulated single lay-rescuer scenario.
Circulation.2002;105(5):645–9.
36. Yu T,WeilMH,Tang W,Sun S,Klouche K,Povoas H,et al.Adverse
outcomes of interrupted precordialcompression during automated
defibrillation.Circulation.2002;106(3):368–72.
37. EftestolT,Sunde K,Steen PA.Effects of interrupting precordial
compressions on the calculated probability of defibrillation success during
out-of-hospitalcardiac arrest.Circulation.2002;105(19):2270–3.
38. Berg MD,Schexnayder SM,Chameides L,Terry M,Donoghue A,Hickey RW,
et al.Part 5:Adult Basic Life Support:2010 American Heart Association
guidelines for cardiopulmonary resuscitation and emergency cardiovascular
care.Circulation.2010;122 Suppl3:S685–705.
39. Hightower D,Thomas SH,Stone CK,Dunn K,March JA.Decay in quality of
closed-chest compressions over time.Ann Emerg Med.1995;26(3):300–3.
40. Gatesa S,Quinnb T,Deakinc CD,Blaire L,Coupera K,Perkins GD.Mechanical
chest compression for out of hospitalcardiac arrest:systematic review and
meta-analysis.Resuscitation.2015;94:91–7.
41. Herlitz J,Ekstrom L,Wennerblom B,Axelsson A,Bang A,Holmberg S.Effect
of bystander initiated cardiopulmonary resuscitation on ventricular
fibrillation and survivalafter witnessed cardiac arrest outside hospital.Br
Heart J.1994;72(5):408–12.
42. McCarney R,Warner J,Iliffe S,van Haselen R,Griffin M,Fisher P.The
Hawthorne Effect:a randomised,controlled trial.BMC Med Res Methodol.
2007;7:30.
43. Fox NS,Brennan JS,Chasen ST.Clinicalestimation of fetalweight and the
Hawthorne effect.Eur J Obstet GynecolReprod Biol.2008;141(2):111–4.
44. Valenzuela TD,Roe DJ,Cretin S,Spaite DW,Larsen MP.Estimating
effectiveness of cardiac arrest interventions:a logistic regression survival
model.Circulation.1997;96(10):3308–13.
45. Wik L,Hansen TB,Fylling F,Steen T,Vaagenes P,Auestad BH,et al.Delaying
defibrillation to give basic cardiopulmonary resuscitation to patients with
out-of-hospitalventricular fibrillation:a randomized trial.J Am Med Assoc.
2003;289:1389–95.
Li et al.Scandinavian Journalof Trauma,Resuscitation and Emergency Medicine (2016) 24:10 Page 10 of 10
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.