Management of Neonatal Seizures: A Literature Review
VerifiedAdded on 2023/06/03
|39
|7091
|310
AI Summary
This literature review focuses on the management of neonatal seizures, which has proved challenging for both basic science researchers and clinicians. The aim of this research is to decide a better antidote for treating neonatal seizures by adopting a process of treatment method based on evidence-based algorithm to minimize the variation amongst providers.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
16260762 2
Declaration Form
Module title : Evidence-Based Nursing 2
Assessment title : Literature Review
Name : Divya S Nair
Student Number : 16269762
Date submitted : 10th May 2018
Word Count : 3382
I hereby declare this work is entirely my own and that I have acknowledged the writing
ideas, and work of others. Furthermore, I have not knowingly allowed another to copy my
work.
Signature: Divya S Nair Date: 10th May 2018
Declaration Form
Module title : Evidence-Based Nursing 2
Assessment title : Literature Review
Name : Divya S Nair
Student Number : 16269762
Date submitted : 10th May 2018
Word Count : 3382
I hereby declare this work is entirely my own and that I have acknowledged the writing
ideas, and work of others. Furthermore, I have not knowingly allowed another to copy my
work.
Signature: Divya S Nair Date: 10th May 2018
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

16260762 3
Management of Neonatal Seizures
Abstract
The neonatal seizure has proved challenging for both basic science researchers and clinicians
because of its distinct attributes. The new therapies of neonatal seizure used by physicians and
clinical experts are not performing as per the requirement of treating new-born infants. This is
the reason experts are giving continuous efforts in developing new and better techniques for
treatment and performing neonatal seizures. The new and advanced techniques are meant to
provide improved treatment. The aim of this research is to decide a better antidote for treating
neonatal seizures by adopting a process of treatment method based on evidence based algorithm
to minimize the variation amongst providers. This is done for the sake of future investigation on
the comparative effectiveness of antiepileptic in neonates the structure of this research is
designed in such a way. For examining the reported evidence related to pharmacological therapy
for neonatal seizures a literature review of related research papers on neonatal seizures has been
conducted. The research is date based and done on 22 articles initially within which seven
additional studies were identified. Limited information is found which is related to the best
pharmacologic treatment regarding the neonatal seizure. These data are conceived by treatment
methods based algorithm from available data. This research paper is designed as a comparative
study to investigate the effectiveness of antiepileptic in neonates. This will also serve as a
clinical reference for using neonatal antiepileptic. The research has effectiveness with capability
of offering better treatment process for neonatal seizures.
Management of Neonatal Seizures
Abstract
The neonatal seizure has proved challenging for both basic science researchers and clinicians
because of its distinct attributes. The new therapies of neonatal seizure used by physicians and
clinical experts are not performing as per the requirement of treating new-born infants. This is
the reason experts are giving continuous efforts in developing new and better techniques for
treatment and performing neonatal seizures. The new and advanced techniques are meant to
provide improved treatment. The aim of this research is to decide a better antidote for treating
neonatal seizures by adopting a process of treatment method based on evidence based algorithm
to minimize the variation amongst providers. This is done for the sake of future investigation on
the comparative effectiveness of antiepileptic in neonates the structure of this research is
designed in such a way. For examining the reported evidence related to pharmacological therapy
for neonatal seizures a literature review of related research papers on neonatal seizures has been
conducted. The research is date based and done on 22 articles initially within which seven
additional studies were identified. Limited information is found which is related to the best
pharmacologic treatment regarding the neonatal seizure. These data are conceived by treatment
methods based algorithm from available data. This research paper is designed as a comparative
study to investigate the effectiveness of antiepileptic in neonates. This will also serve as a
clinical reference for using neonatal antiepileptic. The research has effectiveness with capability
of offering better treatment process for neonatal seizures.
16260762 4
Contents
1. Introduction..............................................................................................................................5
2. Search Strategy.........................................................................................................................5
3. Main body.................................................................................................................................6
3.1 Pharmacological treatment................................................................................................6
3.2 Cooling Method..............................................................................................................10
3.3 Management of Underlying causes.................................................................................12
3.4 Antiepileptic Drug Therapy(AED)................................................................................13
4. Discussion..............................................................................................................................14
5. Conclusion and Recommendation.............................................................................................16
Appendix 1: Search Strategy Table...............................................................................................18
Appendix 2: Summary of Study Table..........................................................................................20
Contents
1. Introduction..............................................................................................................................5
2. Search Strategy.........................................................................................................................5
3. Main body.................................................................................................................................6
3.1 Pharmacological treatment................................................................................................6
3.2 Cooling Method..............................................................................................................10
3.3 Management of Underlying causes.................................................................................12
3.4 Antiepileptic Drug Therapy(AED)................................................................................13
4. Discussion..............................................................................................................................14
5. Conclusion and Recommendation.............................................................................................16
Appendix 1: Search Strategy Table...............................................................................................18
Appendix 2: Summary of Study Table..........................................................................................20
16260762 5
1. Introduction
The treatment processes for neonatal seizures are quite limited within 2 to 4/1000 in North
American births, which is not up to the level of expectancy of experts, and paediatric doctors
around the world as neonatal seizures are quite common. Nearly 19 to 58/1000 infants are born
with less than 1500 grams of birth weight (Slaughter Patel and Slaughter 2013). However,
different new antiepileptic medications are introduced almost every year to treat the infants. As
per the experts, besides new antiepileptic the necessity of treatment is also as important as the
process of treatment required for a certain newborn infant. The most common medication used
by experts are Phenobarbital and phenytoin/fosphenytoin which have efficiency of
approximately 50% which is way to less than required effectiveness. The main concerns related
to this medication process are the side effects, interaction of the medication with the patient
body, continuous monitoring of the blood flow level besides the consequences of potential
negative neurodevelopment. However, according to different reports, the increment in the usage
of antiepileptic medications is the result of these limitations of phenytoin and phenobarbital. As
per the research and analysis of different expert neurologists on the other hand, nearly 73% of
levetiracetam and/ or topiramete in the treatment of neo natal seizures are used in treatment of
neonatal seizures because of their less adverse effects and the easiness of usage.
2. Search Strategy
To develop the database for this research (see appendix 1) different databases like Medline,
PubMed Central, NCBI and Google Scholar are used. To complete the research, ample time is
important to ensure the significance of the work and the results obtained from this. 22 qualitative
research papers were approved which are summarized in Appendix 2. The study consists of
1. Introduction
The treatment processes for neonatal seizures are quite limited within 2 to 4/1000 in North
American births, which is not up to the level of expectancy of experts, and paediatric doctors
around the world as neonatal seizures are quite common. Nearly 19 to 58/1000 infants are born
with less than 1500 grams of birth weight (Slaughter Patel and Slaughter 2013). However,
different new antiepileptic medications are introduced almost every year to treat the infants. As
per the experts, besides new antiepileptic the necessity of treatment is also as important as the
process of treatment required for a certain newborn infant. The most common medication used
by experts are Phenobarbital and phenytoin/fosphenytoin which have efficiency of
approximately 50% which is way to less than required effectiveness. The main concerns related
to this medication process are the side effects, interaction of the medication with the patient
body, continuous monitoring of the blood flow level besides the consequences of potential
negative neurodevelopment. However, according to different reports, the increment in the usage
of antiepileptic medications is the result of these limitations of phenytoin and phenobarbital. As
per the research and analysis of different expert neurologists on the other hand, nearly 73% of
levetiracetam and/ or topiramete in the treatment of neo natal seizures are used in treatment of
neonatal seizures because of their less adverse effects and the easiness of usage.
2. Search Strategy
To develop the database for this research (see appendix 1) different databases like Medline,
PubMed Central, NCBI and Google Scholar are used. To complete the research, ample time is
important to ensure the significance of the work and the results obtained from this. 22 qualitative
research papers were approved which are summarized in Appendix 2. The study consists of
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16260762 6
systematic analysis and meta-synthesis review techniques. The three most predominant themes
immerged in the literature review in this paper have been formulated as the subdivisions of this
study paper to develop it. The three recurring themes will be debated in the next sections of this
paper.
3. Main body
3.1 Pharmacological treatment
To perform this research nearly 557 articles had been identified from the MEDLINE database by
the team of researchers. The whole texts of the rest of the 64 articles have been reviewed. During
this, the abstract and the titles of the manuscript are eliminated, as they do not serve the purpose
of paper analysis. After the analysis of these articles and the references involved with them 14
additional articles are taken to review. After the analysis of total 78 full texts with 16 research
papers involving investigations with EEG (electro encephalogram) to diagnose seizure and
treatment observations are taken in considerations as they are fulfilling the required criteria
(Slaughter Patel and Slaughter 2013).
Painter and his team focused on the phenobarbital and phenytoin and their research work
is the only one in this field in 1999. After this research study, a trail with 59 patients were
arranged. In this trail, patients were given a level of 25mg/l Phenobarbital and 3 mg/L of
phenytoin in addition to an alternative medication in case the process fails. EEG of the
patients were performed continuously. The effectiveness of the phenobarbital and
phenytoin were obtained as the seizures came in control of 43% for both matured and
premature infants. The results were obtained in both the cases with phenobarbital and
phenytoin (P=1) which is nearly 45% with a seizure ratio controlled by these medications
systematic analysis and meta-synthesis review techniques. The three most predominant themes
immerged in the literature review in this paper have been formulated as the subdivisions of this
study paper to develop it. The three recurring themes will be debated in the next sections of this
paper.
3. Main body
3.1 Pharmacological treatment
To perform this research nearly 557 articles had been identified from the MEDLINE database by
the team of researchers. The whole texts of the rest of the 64 articles have been reviewed. During
this, the abstract and the titles of the manuscript are eliminated, as they do not serve the purpose
of paper analysis. After the analysis of these articles and the references involved with them 14
additional articles are taken to review. After the analysis of total 78 full texts with 16 research
papers involving investigations with EEG (electro encephalogram) to diagnose seizure and
treatment observations are taken in considerations as they are fulfilling the required criteria
(Slaughter Patel and Slaughter 2013).
Painter and his team focused on the phenobarbital and phenytoin and their research work
is the only one in this field in 1999. After this research study, a trail with 59 patients were
arranged. In this trail, patients were given a level of 25mg/l Phenobarbital and 3 mg/L of
phenytoin in addition to an alternative medication in case the process fails. EEG of the
patients were performed continuously. The effectiveness of the phenobarbital and
phenytoin were obtained as the seizures came in control of 43% for both matured and
premature infants. The results were obtained in both the cases with phenobarbital and
phenytoin (P=1) which is nearly 45% with a seizure ratio controlled by these medications
16260762 7
is 57:62 respectively for P=0.67. Therefore, the results obtained shows that both of the
medications are equally effective with no adverse side effects for the infants. This
significant development is considered as the cause of seizure reduction up to 80% relative
to complete seizure cessation, this rate of efficiency improved to 80% and 72%
respectively. The observations of adverse effects are almost none. However, the patients
were shuffled for better research; still the research of Painter and his team consists of
some insignificant restraints. The research is carried on only single centre with expert
physicians, well aware EEG technicians to carry out the observation and research
method. The usage of disparity among groups and the only single-blinded regarding
baseline characteristics was present.
In 2004, boylan and his team had performed a research on randomised trial of lidocaine
versus a benzodiazepine dip after the failure of Phenobarbital. During the research, the
experts performed EEG of the patients continuously. Lidocaine was used at a dosage at a
rate of mg/kg then infused at a rate of 2 mg/kg/hr. 60 micrograms/kg of midazolam were
dozed after 150-300 micrograms/kg/hr infusion. In addition to this Clonazepam, dosing
has been used. The statistical analysis required for this research was prevented due to the
major restriction of its small size. There are certain cases, which were randomized
including five cases to lidocaine group, 6 to benzodiazepines (3 for midazolam, 3 for
clonazepam). The responses varied with each other. Benzodiazepine groups came up with
no responses and in case of lidocaine, 3 out of 5 patients responded to the treatment. In
the second case, among 3 patients one had 80% seizure reduction and two were seizure
free. It is clear that from the results that the neurodevelopment among patients were very
poor for over the period of a year for the research. However, no adverse effects were
is 57:62 respectively for P=0.67. Therefore, the results obtained shows that both of the
medications are equally effective with no adverse side effects for the infants. This
significant development is considered as the cause of seizure reduction up to 80% relative
to complete seizure cessation, this rate of efficiency improved to 80% and 72%
respectively. The observations of adverse effects are almost none. However, the patients
were shuffled for better research; still the research of Painter and his team consists of
some insignificant restraints. The research is carried on only single centre with expert
physicians, well aware EEG technicians to carry out the observation and research
method. The usage of disparity among groups and the only single-blinded regarding
baseline characteristics was present.
In 2004, boylan and his team had performed a research on randomised trial of lidocaine
versus a benzodiazepine dip after the failure of Phenobarbital. During the research, the
experts performed EEG of the patients continuously. Lidocaine was used at a dosage at a
rate of mg/kg then infused at a rate of 2 mg/kg/hr. 60 micrograms/kg of midazolam were
dozed after 150-300 micrograms/kg/hr infusion. In addition to this Clonazepam, dosing
has been used. The statistical analysis required for this research was prevented due to the
major restriction of its small size. There are certain cases, which were randomized
including five cases to lidocaine group, 6 to benzodiazepines (3 for midazolam, 3 for
clonazepam). The responses varied with each other. Benzodiazepine groups came up with
no responses and in case of lidocaine, 3 out of 5 patients responded to the treatment. In
the second case, among 3 patients one had 80% seizure reduction and two were seizure
free. It is clear that from the results that the neurodevelopment among patients were very
poor for over the period of a year for the research. However, no adverse effects were
16260762 8
noticed in a short period. Particularly the 50% of the patients under observation
responded to the phenobarbital, which is consistent with the reports of Painter and his
team.
A research on second-line midazolam usage after up to 40 mg/kg phenobarbital to a
historical phenobarbital and or phenytoin treated neonatal seizure patients by the team of
Castro-Condeet in 2005. Continuous EEG was done for multiple hours then intermittent
EEG at an interval of 24-hours was done to assure no seizure reversion occurs.
Midazolam was administered up to twice at a rate of 150 mg/kg when required at a rate
of 60-1080 mg/kg/hr injection. The dosage is way to higher than the dosage used by
Boylan and his team in 2004 or any other expert team for that matter. The midazolam rate
brought remarkable response of 100%. The seizures were totally controlled within an
hour for nearly 10 to 13 patients in the treatment group. However, no gap differences of
any year has been observed in case of neurodevelopmental results. If the results are
compared between group 1 with no responders (seizures continued even after
administration of phenobarbital or phenytoin) and the 2nd group which is treated with
midazolam, surprisingly the number of patients assessed as normal after treatment
showed significant differences in terms of percentage in favour of midazolam. As the
difference contains the previous troop, the results are considered to be biased as of the
changed practice between this time period which is not related to midazolam. In
numerical view, it has seen that in every 4 out of 13 infants have decreased consciousness
as side effects for nearly 10 to 15 minutes further leading to midazolam bolus
hypertension with multisystem organ failure because of acute hypoxic-ischemic injury
(HIE). Tin case of 2 infants the conditions are not related to midazolam administration.
noticed in a short period. Particularly the 50% of the patients under observation
responded to the phenobarbital, which is consistent with the reports of Painter and his
team.
A research on second-line midazolam usage after up to 40 mg/kg phenobarbital to a
historical phenobarbital and or phenytoin treated neonatal seizure patients by the team of
Castro-Condeet in 2005. Continuous EEG was done for multiple hours then intermittent
EEG at an interval of 24-hours was done to assure no seizure reversion occurs.
Midazolam was administered up to twice at a rate of 150 mg/kg when required at a rate
of 60-1080 mg/kg/hr injection. The dosage is way to higher than the dosage used by
Boylan and his team in 2004 or any other expert team for that matter. The midazolam rate
brought remarkable response of 100%. The seizures were totally controlled within an
hour for nearly 10 to 13 patients in the treatment group. However, no gap differences of
any year has been observed in case of neurodevelopmental results. If the results are
compared between group 1 with no responders (seizures continued even after
administration of phenobarbital or phenytoin) and the 2nd group which is treated with
midazolam, surprisingly the number of patients assessed as normal after treatment
showed significant differences in terms of percentage in favour of midazolam. As the
difference contains the previous troop, the results are considered to be biased as of the
changed practice between this time period which is not related to midazolam. In
numerical view, it has seen that in every 4 out of 13 infants have decreased consciousness
as side effects for nearly 10 to 15 minutes further leading to midazolam bolus
hypertension with multisystem organ failure because of acute hypoxic-ischemic injury
(HIE). Tin case of 2 infants the conditions are not related to midazolam administration.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
16260762 9
After dosage of 40mg/kg of phenobarbital and /or IV diazepam or lorazepam in a single
dosage, the comparison between second and third line treatment with lidocaine versus
midazolam for mature and premature babies with neonatal seizure cases has been
conducted by Shany and his team in 2007. The research also consists of the historical
cohort based on the hypoxic-ischemic encephalopathy of such cases. The Amplitude
based EEG has been conducted on the students continuously. The 2mg/kg of lidocaine
dosage was administered at a rate of 4-6 mg.kg.hr infusion. Midazolam was also injected
at a rate of 60-200 mg.kg/hr without loading as a dosage. This group of patients in the
first case responded up to 77% however, there were 50% cessation with the seizure
activity rate less than 6 hours. The second group showed 50% response with a seizure
activity rate also less than 6 hours of completion of cessation. The non-responders were
passed by the alternative medication agents leading towards the overall response consists
of 81% lidocaine and 67% of midazolam with no adverse effects in this short period. The
comparative investigation was limited due to the absence of midazolam loading dose.
After that about 20 infants were treated with lidocaine (dosing protocol: 2 mg.kg load,
6mg/kg/hour for 12 hours then 2 mg/kg/hours for again 12 hours.) prospectively.
Malingre and his team develop the process in 2006. The research work is significant after
the failure of phenobarbital and either midazolam or clonazepam. The reduction in the
seizures was noticed at 76% with 52% with seizure cessation. The aim of this research
was to minimize the cardiac effects with an optimal lidocaine dosing. The dose was
reduced following this research from 6 mg/kg/hour for 6 hours versus up to 12 hours.).
This gave a similar response rate of 78% affectivity with no adverse result notices.
After dosage of 40mg/kg of phenobarbital and /or IV diazepam or lorazepam in a single
dosage, the comparison between second and third line treatment with lidocaine versus
midazolam for mature and premature babies with neonatal seizure cases has been
conducted by Shany and his team in 2007. The research also consists of the historical
cohort based on the hypoxic-ischemic encephalopathy of such cases. The Amplitude
based EEG has been conducted on the students continuously. The 2mg/kg of lidocaine
dosage was administered at a rate of 4-6 mg.kg.hr infusion. Midazolam was also injected
at a rate of 60-200 mg.kg/hr without loading as a dosage. This group of patients in the
first case responded up to 77% however, there were 50% cessation with the seizure
activity rate less than 6 hours. The second group showed 50% response with a seizure
activity rate also less than 6 hours of completion of cessation. The non-responders were
passed by the alternative medication agents leading towards the overall response consists
of 81% lidocaine and 67% of midazolam with no adverse effects in this short period. The
comparative investigation was limited due to the absence of midazolam loading dose.
After that about 20 infants were treated with lidocaine (dosing protocol: 2 mg.kg load,
6mg/kg/hour for 12 hours then 2 mg/kg/hours for again 12 hours.) prospectively.
Malingre and his team develop the process in 2006. The research work is significant after
the failure of phenobarbital and either midazolam or clonazepam. The reduction in the
seizures was noticed at 76% with 52% with seizure cessation. The aim of this research
was to minimize the cardiac effects with an optimal lidocaine dosing. The dose was
reduced following this research from 6 mg/kg/hour for 6 hours versus up to 12 hours.).
This gave a similar response rate of 78% affectivity with no adverse result notices.
16260762 10
Another research is done on the usage of levetiracetam of 10-20 mg/kg load with a rate of
80 mg/kg/hour divided twice daily leading to 45mg/kg/hour everyday among 23 neonates
in comparison with phenobarbital and phenytoin. The research is conducted by Abend
and his team in 2011. Result of this research shows a reduction of 50% in the number of
seizures treated by levetiracetam recorded among 35% neonates. No adverse effects had
been noticed. It is stated in the discussion that with the passage of time some of the
seizures may have been secondary.
Another research is done by reviewing 22 patients acquiring first and second line
levetiracetam of 10-50 mg/kg intravenous load at an infusion rate of 50 mg/kg/hour. The
result of this research showed 86% reduction in seizure cessation. 100% improvement
was recorded in case of 7 patients among 22 which is 32% after the heavy dosage. The
side effect was noticed in one patient it was just an irritability, which was cured by
following pyridoxine supplement.
3.2 Cooling Method
Therapeutic hypothermia is a powerful and clinically accessible treatment for neonatal
hypoxic-ischemic encephalopathy or HIE. Various animal quantitative researches have
shown that this type of hypothermia treatment can diminish seizures and epilepsies action
in the setting of hypoxia-ischemia. However, recent clinical information in human babies
has been proving different from this. Three observational quantitative studies
demonstrated a diminished frequency and seriousness of seizures among neonates with
HIE who were treated with therapeutic hypothermia. Furthermore, two quantitative
research studies demonstrated a much lower burden for the electrographic seizures by
EEG observing: (1) among neonates with direct encephalopathy and (2) subsequent to
Another research is done on the usage of levetiracetam of 10-20 mg/kg load with a rate of
80 mg/kg/hour divided twice daily leading to 45mg/kg/hour everyday among 23 neonates
in comparison with phenobarbital and phenytoin. The research is conducted by Abend
and his team in 2011. Result of this research shows a reduction of 50% in the number of
seizures treated by levetiracetam recorded among 35% neonates. No adverse effects had
been noticed. It is stated in the discussion that with the passage of time some of the
seizures may have been secondary.
Another research is done by reviewing 22 patients acquiring first and second line
levetiracetam of 10-50 mg/kg intravenous load at an infusion rate of 50 mg/kg/hour. The
result of this research showed 86% reduction in seizure cessation. 100% improvement
was recorded in case of 7 patients among 22 which is 32% after the heavy dosage. The
side effect was noticed in one patient it was just an irritability, which was cured by
following pyridoxine supplement.
3.2 Cooling Method
Therapeutic hypothermia is a powerful and clinically accessible treatment for neonatal
hypoxic-ischemic encephalopathy or HIE. Various animal quantitative researches have
shown that this type of hypothermia treatment can diminish seizures and epilepsies action
in the setting of hypoxia-ischemia. However, recent clinical information in human babies
has been proving different from this. Three observational quantitative studies
demonstrated a diminished frequency and seriousness of seizures among neonates with
HIE who were treated with therapeutic hypothermia. Furthermore, two quantitative
research studies demonstrated a much lower burden for the electrographic seizures by
EEG observing: (1) among neonates with direct encephalopathy and (2) subsequent to
16260762 11
representing severe mind damage on MRI. In addition this, in cohort studies, neonates
were treated with therapeutic hypothermia and as a result it was found to have blood
vessel ischemic stroke on
MRI having a much lower probability of seizure when contrasted with those neonates
with stroke who were not given cooling treatment. Interestingly, meta-examinations of
randomized controlled trials of cooling therapy for neonatal HIE have neglected to
demonstrate a relationship between cooling therapy and diminished seizures. The
potential effects of epileptogenic impacts of cooling therapy possess critical clinical
ramifications. Since some of the seizure, medicines have restricted viability in infants and
hence, may prove harmful.
The connection between cooling therapy and the combined occurrence of seizures was
inspected by examining neonate's cohorts either with seizures who were admitted to
various health centers previously o rafter the start of the cooling treatment. Among the
enrolled infants incorporated into the study nearly 151 were getting treatment for
hypothermia. The seizure monitoring in study subjects who were born before the onset
of the cooling therapy were mainly at discreation of all appointed treating physician,
however, on the other hand, cooled newborns were having continuous monitoring both
with conventional video EEG as well as amplitude-integrated EEG. It was done from
time of admission until completion of the rewarming treatment after giving therapeutic
hypothermia. All the cooled infants suffering from direct encephalopathy substantially
were much less prone to suffer from either electrographic or clinical seizures compared
with the non-cooled babies (the cooled ones: 26 % vs. the non-cooled: 61%, P<0.001).
representing severe mind damage on MRI. In addition this, in cohort studies, neonates
were treated with therapeutic hypothermia and as a result it was found to have blood
vessel ischemic stroke on
MRI having a much lower probability of seizure when contrasted with those neonates
with stroke who were not given cooling treatment. Interestingly, meta-examinations of
randomized controlled trials of cooling therapy for neonatal HIE have neglected to
demonstrate a relationship between cooling therapy and diminished seizures. The
potential effects of epileptogenic impacts of cooling therapy possess critical clinical
ramifications. Since some of the seizure, medicines have restricted viability in infants and
hence, may prove harmful.
The connection between cooling therapy and the combined occurrence of seizures was
inspected by examining neonate's cohorts either with seizures who were admitted to
various health centers previously o rafter the start of the cooling treatment. Among the
enrolled infants incorporated into the study nearly 151 were getting treatment for
hypothermia. The seizure monitoring in study subjects who were born before the onset
of the cooling therapy were mainly at discreation of all appointed treating physician,
however, on the other hand, cooled newborns were having continuous monitoring both
with conventional video EEG as well as amplitude-integrated EEG. It was done from
time of admission until completion of the rewarming treatment after giving therapeutic
hypothermia. All the cooled infants suffering from direct encephalopathy substantially
were much less prone to suffer from either electrographic or clinical seizures compared
with the non-cooled babies (the cooled ones: 26 % vs. the non-cooled: 61%, P<0.001).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16260762 12
However, there was still no distinction in risks of seizures mainly among the infants
having extreme encephalopathy'
As the observation of ceaseless EEG was performed closely by hypothermia, it was most
probably possible that the recurrence of EEG seizure was more or less under-evaluated in
non-cooled amass whenever checking was more constrained and at the tact of the treating
doctor.
3.3 Management of Underlying causes
According to quantitative findings of - a study, neonatal period (the initial 28 days of life)
has the highest frequency of seizures over the life expectancy at 1.8 to 3.5 for every 1,000
live births. The most widely recognized reason for neonatal seizures is hypoxic-ischemic
Encephalopathy, which happens in around 1 to 2 for each 1,000-1ive births. In the
neonates, a wide scope of central nervous system and systematic disorders can give rise
to neonatal seizures. Evaluation of cause and treatment normally happens simultaneously.
The most basic need is distinguishing treatable reasons underlying seizures, including
metabolic disturbances (hypocalcaemia, hypo glycaemia and hypomagnesaemia) as well
as inflammation due to infection attack. The overwhelming reason is to some degree due
to the neonate basic setting. A detailed quantitative investigation from a tertiary care
referral neonatal ICU was done in which around 66% were found to be related to
hypoxic-ischemic encephalopathy and cerebrovascular disarranges
In spite of the fact that the term baby is at high hazard for seizures, it is progressively
perceived that seizures can be a major issue for the preterm newborn children. A recent
quantitative study of extremely low birth-weight children in Israel was analyzed showing
However, there was still no distinction in risks of seizures mainly among the infants
having extreme encephalopathy'
As the observation of ceaseless EEG was performed closely by hypothermia, it was most
probably possible that the recurrence of EEG seizure was more or less under-evaluated in
non-cooled amass whenever checking was more constrained and at the tact of the treating
doctor.
3.3 Management of Underlying causes
According to quantitative findings of - a study, neonatal period (the initial 28 days of life)
has the highest frequency of seizures over the life expectancy at 1.8 to 3.5 for every 1,000
live births. The most widely recognized reason for neonatal seizures is hypoxic-ischemic
Encephalopathy, which happens in around 1 to 2 for each 1,000-1ive births. In the
neonates, a wide scope of central nervous system and systematic disorders can give rise
to neonatal seizures. Evaluation of cause and treatment normally happens simultaneously.
The most basic need is distinguishing treatable reasons underlying seizures, including
metabolic disturbances (hypocalcaemia, hypo glycaemia and hypomagnesaemia) as well
as inflammation due to infection attack. The overwhelming reason is to some degree due
to the neonate basic setting. A detailed quantitative investigation from a tertiary care
referral neonatal ICU was done in which around 66% were found to be related to
hypoxic-ischemic encephalopathy and cerebrovascular disarranges
In spite of the fact that the term baby is at high hazard for seizures, it is progressively
perceived that seizures can be a major issue for the preterm newborn children. A recent
quantitative study of extremely low birth-weight children in Israel was analyzed showing
16260762 13
a general rate of neonatal seizures of around 5'6%' A much younger male sex, gestational
age, along with other major foundational (such as sepsis) and neurological comorbidities
(either intraventricular drain or periventricular (leukomalacia) were all considered as
autonomous indicators of neonatal seizures.
Newborn children with complex innate coronary illness are at high hazard for seizures in
the perioperative period. Different but less common reasons for neonatal seizures
incorporate formative irregularities, natural mistakes of digestion, and other hereditary
disorders that are examined in detail in reference studies
3.4 Antiepileptic Drug Therapy(AED)
Thorough assessment of the adequacy of antiepileptic drugs treatment in neonates is very
challenging. In perspective of the difficulties characteristic in behavioral findings,
incorporation of the constant EEG observing can be referred to as a quality level for
investigations of the therapeutic efficiency. A consensus exists that as of now the
anticonvulsants used are regularly ineffectual for the treatment of neonatal seizures
(Sanker and Painter 2005). Painter and associates' in 1999 quantitative investigation
revealed that in babies with EEG-affirmed seizures, the loading doses for both
phenobarbital and phenytoin were similar but deficiently viable, and that either of these
alone controlled seizures in less than the half. Moreover, variable viabilities has been
reported for midazolam as the second line of pharmaceutical.
Lidocaine is a viable treatment for neonatal seizures; however, issues related to the heart
danger have restricted broad reception of this in infants. A similarly imperative
quantitative finding regarding AED treatment in neonates was whether treatment as
fruitful method of treatment for seizures justified. In encephalopathy newbom children,
a general rate of neonatal seizures of around 5'6%' A much younger male sex, gestational
age, along with other major foundational (such as sepsis) and neurological comorbidities
(either intraventricular drain or periventricular (leukomalacia) were all considered as
autonomous indicators of neonatal seizures.
Newborn children with complex innate coronary illness are at high hazard for seizures in
the perioperative period. Different but less common reasons for neonatal seizures
incorporate formative irregularities, natural mistakes of digestion, and other hereditary
disorders that are examined in detail in reference studies
3.4 Antiepileptic Drug Therapy(AED)
Thorough assessment of the adequacy of antiepileptic drugs treatment in neonates is very
challenging. In perspective of the difficulties characteristic in behavioral findings,
incorporation of the constant EEG observing can be referred to as a quality level for
investigations of the therapeutic efficiency. A consensus exists that as of now the
anticonvulsants used are regularly ineffectual for the treatment of neonatal seizures
(Sanker and Painter 2005). Painter and associates' in 1999 quantitative investigation
revealed that in babies with EEG-affirmed seizures, the loading doses for both
phenobarbital and phenytoin were similar but deficiently viable, and that either of these
alone controlled seizures in less than the half. Moreover, variable viabilities has been
reported for midazolam as the second line of pharmaceutical.
Lidocaine is a viable treatment for neonatal seizures; however, issues related to the heart
danger have restricted broad reception of this in infants. A similarly imperative
quantitative finding regarding AED treatment in neonates was whether treatment as
fruitful method of treatment for seizures justified. In encephalopathy newbom children,
16260762 14
the seizures unexpectedly wind down before the finishing of first 7 days of life; in spite
of the fact that it is obscure whether continuation of AED treatment is of advantage, this
practice is very normal. Quantitative investigations of early-life anticonvulsant treatment
on both psychological as well as neurological improvement are constantly confounded by
numerous reasons for neonatal seizures, and it will be important to formulate thorough
methodologies for the generally homogeneous clinical populaces for such examinations.
4. Discussion
Proving a technique to be the best with 100% positive result in case of treating seizure is not
possible as a very few proof about the finest treatment for natural seizure in medicine is
available. One out of two scattered trails, which have been conducted for this research was
worthy and big enough to give numerical analysis. There are only few more researches available
with potential of non-scattered study by experiments and two legions of demonstrations done
before this research. Those papers also provide thorough study on effects of different types of
treatment methods for neonatal seizures. The description of the first exposure seizing infants
related to novel medications was revolutionary in terms of the historical cohort of neonatal
seizure treatment. However, hazards and advantages are very lesser known as per recent data
about anti-epileptic drugs comprising the scarcity of control or comparability group.
Even after different study suggesting against phenobarbital, it has been found from different
research papers that the first line of medication should be phenobarbital. This is because it is
included as RCT, which is the first line treatment of neonatal seizure. As in animals, it is the
most analyzed anti-epileptic drug, which makes it historically precedent for neonates. It has also
been found that the proof of the impact of phenobarbital on futuristic neonatal neurodevelopment
the seizures unexpectedly wind down before the finishing of first 7 days of life; in spite
of the fact that it is obscure whether continuation of AED treatment is of advantage, this
practice is very normal. Quantitative investigations of early-life anticonvulsant treatment
on both psychological as well as neurological improvement are constantly confounded by
numerous reasons for neonatal seizures, and it will be important to formulate thorough
methodologies for the generally homogeneous clinical populaces for such examinations.
4. Discussion
Proving a technique to be the best with 100% positive result in case of treating seizure is not
possible as a very few proof about the finest treatment for natural seizure in medicine is
available. One out of two scattered trails, which have been conducted for this research was
worthy and big enough to give numerical analysis. There are only few more researches available
with potential of non-scattered study by experiments and two legions of demonstrations done
before this research. Those papers also provide thorough study on effects of different types of
treatment methods for neonatal seizures. The description of the first exposure seizing infants
related to novel medications was revolutionary in terms of the historical cohort of neonatal
seizure treatment. However, hazards and advantages are very lesser known as per recent data
about anti-epileptic drugs comprising the scarcity of control or comparability group.
Even after different study suggesting against phenobarbital, it has been found from different
research papers that the first line of medication should be phenobarbital. This is because it is
included as RCT, which is the first line treatment of neonatal seizure. As in animals, it is the
most analyzed anti-epileptic drug, which makes it historically precedent for neonates. It has also
been found that the proof of the impact of phenobarbital on futuristic neonatal neurodevelopment
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
16260762 15
is very little. In addition, the U.S Food and Drug Administration (FDA) have put bindings on the
usage, which includes no approval of usage of such drugs in communities with large number of
patients. The reasons of such bindings is not clear. However, in other researches, Phenobarbital
was been considered as a better medication for neonatal antiepileptic, even though Painter and
his team gave equal importance to phenytoin. The probability of side effects, capricious
metabolism in neonates besides the requirement of continuous monitoring blood flow level are
the major reasons, which suggest the opposite of this.
There are treatments, which are not that much responsive to Phenobarbital for neonatal seizures
and can be used as second-line treatment includes Levetiracetam, Phenytoin/fosphenytoin, and
Lidocaine. Although there is no comparison within the same structural study in two different
studies. It has been observed that Levetiracetam has minimized the seizure. It is recommended
for all age groups and does not require any type of blood observations. Therefore, for this
research, as per the stipulations of Lidocaine and fosphenytoin/phenytoin, it has been considered
as the second line of medication. However, it is not recommended as there are not many
thorough studies done taken in regards to the first moth life cycle especially. If the usage is
compulsory at any circumstances, it is not recommended to use more than 40-50 mg/kg bolus in
line. This is also recommended by the team of Khan. It has been found from the study that this
measurement shows continuous progress.
In addition, neonatal seizures are related to the morbidity and mortality. Hypoxic-ischemic
encephalopathy (HIE) is a widely recognized cause behind seizures in beizuresabies. Neonatal
models using cooling therapies for animals show better results to diminish seizures and epileptic-
form among hypoxia-ischemia, however information from human examinations have poor
results. In this regard,discoveries of recent examinations exhibited a diminished seizure number
is very little. In addition, the U.S Food and Drug Administration (FDA) have put bindings on the
usage, which includes no approval of usage of such drugs in communities with large number of
patients. The reasons of such bindings is not clear. However, in other researches, Phenobarbital
was been considered as a better medication for neonatal antiepileptic, even though Painter and
his team gave equal importance to phenytoin. The probability of side effects, capricious
metabolism in neonates besides the requirement of continuous monitoring blood flow level are
the major reasons, which suggest the opposite of this.
There are treatments, which are not that much responsive to Phenobarbital for neonatal seizures
and can be used as second-line treatment includes Levetiracetam, Phenytoin/fosphenytoin, and
Lidocaine. Although there is no comparison within the same structural study in two different
studies. It has been observed that Levetiracetam has minimized the seizure. It is recommended
for all age groups and does not require any type of blood observations. Therefore, for this
research, as per the stipulations of Lidocaine and fosphenytoin/phenytoin, it has been considered
as the second line of medication. However, it is not recommended as there are not many
thorough studies done taken in regards to the first moth life cycle especially. If the usage is
compulsory at any circumstances, it is not recommended to use more than 40-50 mg/kg bolus in
line. This is also recommended by the team of Khan. It has been found from the study that this
measurement shows continuous progress.
In addition, neonatal seizures are related to the morbidity and mortality. Hypoxic-ischemic
encephalopathy (HIE) is a widely recognized cause behind seizures in beizuresabies. Neonatal
models using cooling therapies for animals show better results to diminish seizures and epileptic-
form among hypoxia-ischemia, however information from human examinations have poor
results. In this regard,discoveries of recent examinations exhibited a diminished seizure number
16260762 16
in infants with direct HIE treated with hypothermia. This research also confirms to clinical trial
information that showed that infants with encephalopathy could benefit the most from
therapeutic hypothermia (Gano et al., 2014). Furthermore, more study is required to reveal the
components that underline the decreased risks of seizures related with cooling therapy in babies
with HIE, and the potential risks of epileptogenic for hypothermia in other clinical settings
(Silverstein and Jensen, 2007).
In spite of the fact that, many researches and innovations of procedures are now available for
neonatal seizures. Numerous functional difficulties must be routed to smoothen the clinical trials
of AEDs in neonates. Involving consistent EEG checking into clinical investigations of neonatal
seizure treatment is an overwhelming task. However, it will likewise be fundamental to survey
AED effectiveness with different treatments (such as instigated hypothermia) in newborn
children.
The criteria involved in this research do not include any articles as treatment options, which
comprise of Phenobarbital coma and status epileptics for infants. Resultantly it cannot be used as
reasons about the recommendation of the trail of phenobarbital in effected infants who have not
responded to our pharmacological therapies.
5. Conclusion and Recommendation
The research is conducted on the review of popular research works depicting different treatment
method for neonatal seizure with respect to antiepileptic medication. The aim of this research is
to bring out the most suitable method of them. The data used for this research is topiramate in
neonates is quite low. The adaptation of the futuristic approach includes the seizure diagnosis
in infants with direct HIE treated with hypothermia. This research also confirms to clinical trial
information that showed that infants with encephalopathy could benefit the most from
therapeutic hypothermia (Gano et al., 2014). Furthermore, more study is required to reveal the
components that underline the decreased risks of seizures related with cooling therapy in babies
with HIE, and the potential risks of epileptogenic for hypothermia in other clinical settings
(Silverstein and Jensen, 2007).
In spite of the fact that, many researches and innovations of procedures are now available for
neonatal seizures. Numerous functional difficulties must be routed to smoothen the clinical trials
of AEDs in neonates. Involving consistent EEG checking into clinical investigations of neonatal
seizure treatment is an overwhelming task. However, it will likewise be fundamental to survey
AED effectiveness with different treatments (such as instigated hypothermia) in newborn
children.
The criteria involved in this research do not include any articles as treatment options, which
comprise of Phenobarbital coma and status epileptics for infants. Resultantly it cannot be used as
reasons about the recommendation of the trail of phenobarbital in effected infants who have not
responded to our pharmacological therapies.
5. Conclusion and Recommendation
The research is conducted on the review of popular research works depicting different treatment
method for neonatal seizure with respect to antiepileptic medication. The aim of this research is
to bring out the most suitable method of them. The data used for this research is topiramate in
neonates is quite low. The adaptation of the futuristic approach includes the seizure diagnosis
16260762 17
and verification of cessation via amplitude-integrated EEG can be considered one of the most
effective of all. The focus of this method is on the condition of the patient and etiologist.
Irregular but controlled experimentation showed better results with medications without any side
effects. However financing such researches is a major concern for any researchers. The
collaboration of different neonatal care units of different hospitals is also necessary for such
researches, as this will help in financing of the projects. In addition to this, the collaboration will
ample the statistical power of data collection and help to cope with the difficulties of reports
related to the enrolled neonates in medical experiments of antiepileptic and offer a minimal
amount of protective means for treatment and randomization. A detailed group formation for
patients is necessary to enlist details of those infants whose parents have denied randomization
for different researches. This is why collaboration of different centres with networks to ensure
funding and permission to perform tests on neonatal seizure medication. On the other hand, this
will help the researchers to use large amount of statistical and medical reports and analyse more
data to ensure more accuracy of the research. The success rate of the research will be more than
conducting research on patients of a single centre.
and verification of cessation via amplitude-integrated EEG can be considered one of the most
effective of all. The focus of this method is on the condition of the patient and etiologist.
Irregular but controlled experimentation showed better results with medications without any side
effects. However financing such researches is a major concern for any researchers. The
collaboration of different neonatal care units of different hospitals is also necessary for such
researches, as this will help in financing of the projects. In addition to this, the collaboration will
ample the statistical power of data collection and help to cope with the difficulties of reports
related to the enrolled neonates in medical experiments of antiepileptic and offer a minimal
amount of protective means for treatment and randomization. A detailed group formation for
patients is necessary to enlist details of those infants whose parents have denied randomization
for different researches. This is why collaboration of different centres with networks to ensure
funding and permission to perform tests on neonatal seizure medication. On the other hand, this
will help the researchers to use large amount of statistical and medical reports and analyse more
data to ensure more accuracy of the research. The success rate of the research will be more than
conducting research on patients of a single centre.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16260762 18
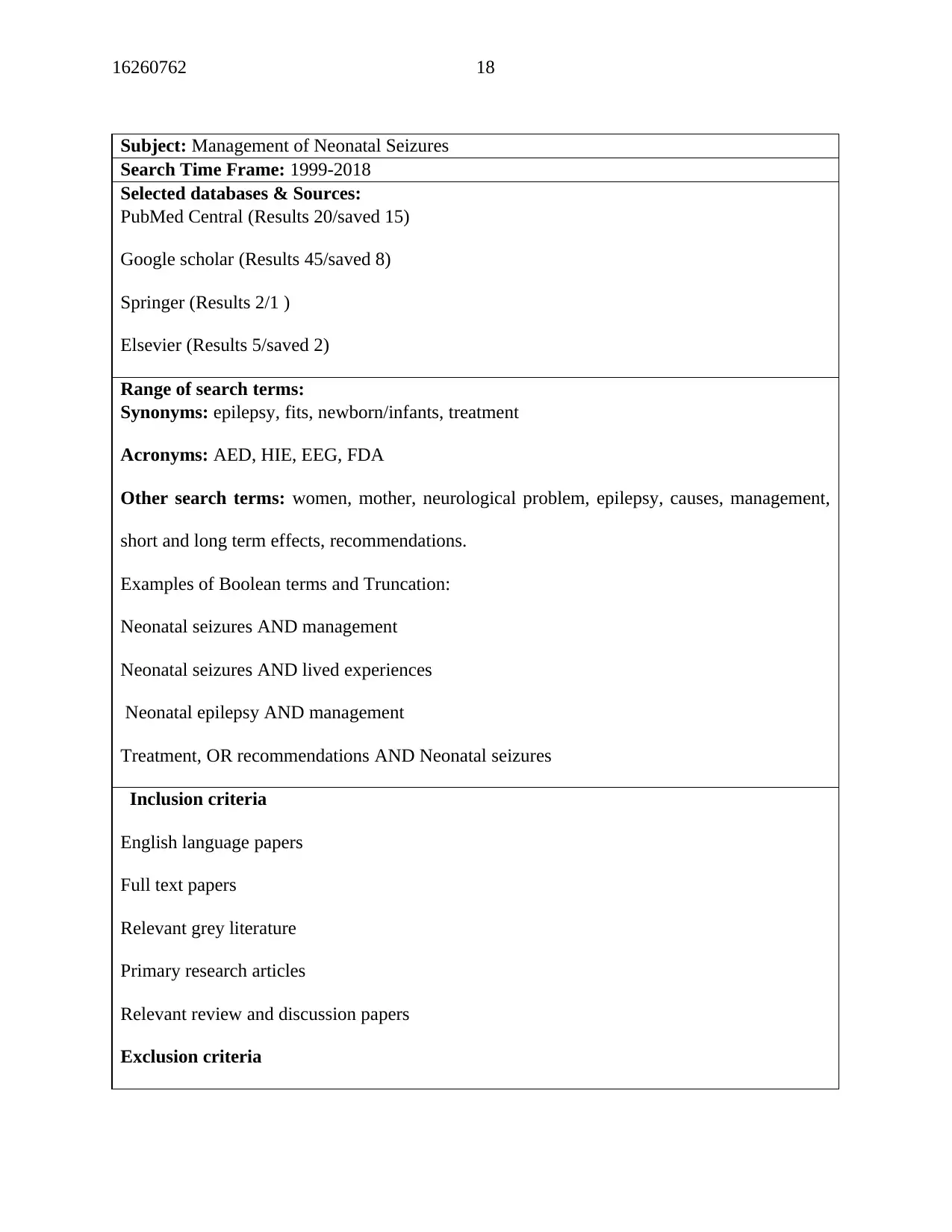
Subject: Management of Neonatal Seizures
Search Time Frame: 1999-2018
Selected databases & Sources:
PubMed Central (Results 20/saved 15)
Google scholar (Results 45/saved 8)
Springer (Results 2/1 )
Elsevier (Results 5/saved 2)
Range of search terms:
Synonyms: epilepsy, fits, newborn/infants, treatment
Acronyms: AED, HIE, EEG, FDA
Other search terms: women, mother, neurological problem, epilepsy, causes, management,
short and long term effects, recommendations.
Examples of Boolean terms and Truncation:
Neonatal seizures AND management
Neonatal seizures AND lived experiences
Neonatal epilepsy AND management
Treatment, OR recommendations AND Neonatal seizures
Inclusion criteria
English language papers
Full text papers
Relevant grey literature
Primary research articles
Relevant review and discussion papers
Exclusion criteria
Subject: Management of Neonatal Seizures
Search Time Frame: 1999-2018
Selected databases & Sources:
PubMed Central (Results 20/saved 15)
Google scholar (Results 45/saved 8)
Springer (Results 2/1 )
Elsevier (Results 5/saved 2)
Range of search terms:
Synonyms: epilepsy, fits, newborn/infants, treatment
Acronyms: AED, HIE, EEG, FDA
Other search terms: women, mother, neurological problem, epilepsy, causes, management,
short and long term effects, recommendations.
Examples of Boolean terms and Truncation:
Neonatal seizures AND management
Neonatal seizures AND lived experiences
Neonatal epilepsy AND management
Treatment, OR recommendations AND Neonatal seizures
Inclusion criteria
English language papers
Full text papers
Relevant grey literature
Primary research articles
Relevant review and discussion papers
Exclusion criteria
16260762 19
Research papers that require purchasing prior to viewing
Papers not available in full text
Unpublished studies
Appendix 1: Search Strategy Table
Research papers that require purchasing prior to viewing
Papers not available in full text
Unpublished studies
Appendix 1: Search Strategy Table

16260762 20
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
16260762 21
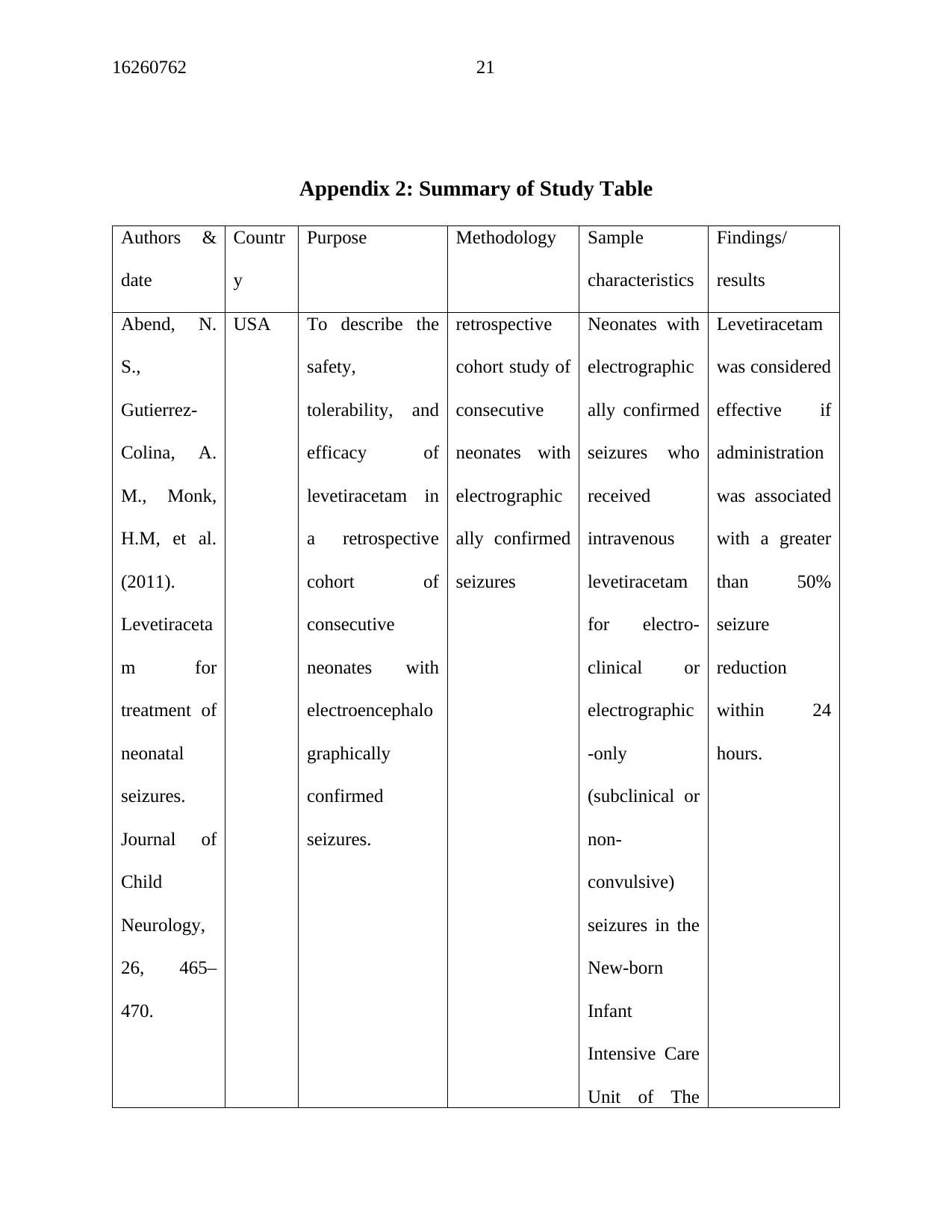
Appendix 2: Summary of Study Table
Authors &
date
Countr
y
Purpose Methodology Sample
characteristics
Findings/
results
Abend, N.
S.,
Gutierrez-
Colina, A.
M., Monk,
H.M, et al.
(2011).
Levetiraceta
m for
treatment of
neonatal
seizures.
Journal of
Child
Neurology,
26, 465–
470.
USA To describe the
safety,
tolerability, and
efficacy of
levetiracetam in
a retrospective
cohort of
consecutive
neonates with
electroencephalo
graphically
confirmed
seizures.
retrospective
cohort study of
consecutive
neonates with
electrographic
ally confirmed
seizures
Neonates with
electrographic
ally confirmed
seizures who
received
intravenous
levetiracetam
for electro-
clinical or
electrographic
-only
(subclinical or
non-
convulsive)
seizures in the
New-born
Infant
Intensive Care
Unit of The
Levetiracetam
was considered
effective if
administration
was associated
with a greater
than 50%
seizure
reduction
within 24
hours.
Appendix 2: Summary of Study Table
Authors &
date
Countr
y
Purpose Methodology Sample
characteristics
Findings/
results
Abend, N.
S.,
Gutierrez-
Colina, A.
M., Monk,
H.M, et al.
(2011).
Levetiraceta
m for
treatment of
neonatal
seizures.
Journal of
Child
Neurology,
26, 465–
470.
USA To describe the
safety,
tolerability, and
efficacy of
levetiracetam in
a retrospective
cohort of
consecutive
neonates with
electroencephalo
graphically
confirmed
seizures.
retrospective
cohort study of
consecutive
neonates with
electrographic
ally confirmed
seizures
Neonates with
electrographic
ally confirmed
seizures who
received
intravenous
levetiracetam
for electro-
clinical or
electrographic
-only
(subclinical or
non-
convulsive)
seizures in the
New-born
Infant
Intensive Care
Unit of The
Levetiracetam
was considered
effective if
administration
was associated
with a greater
than 50%
seizure
reduction
within 24
hours.
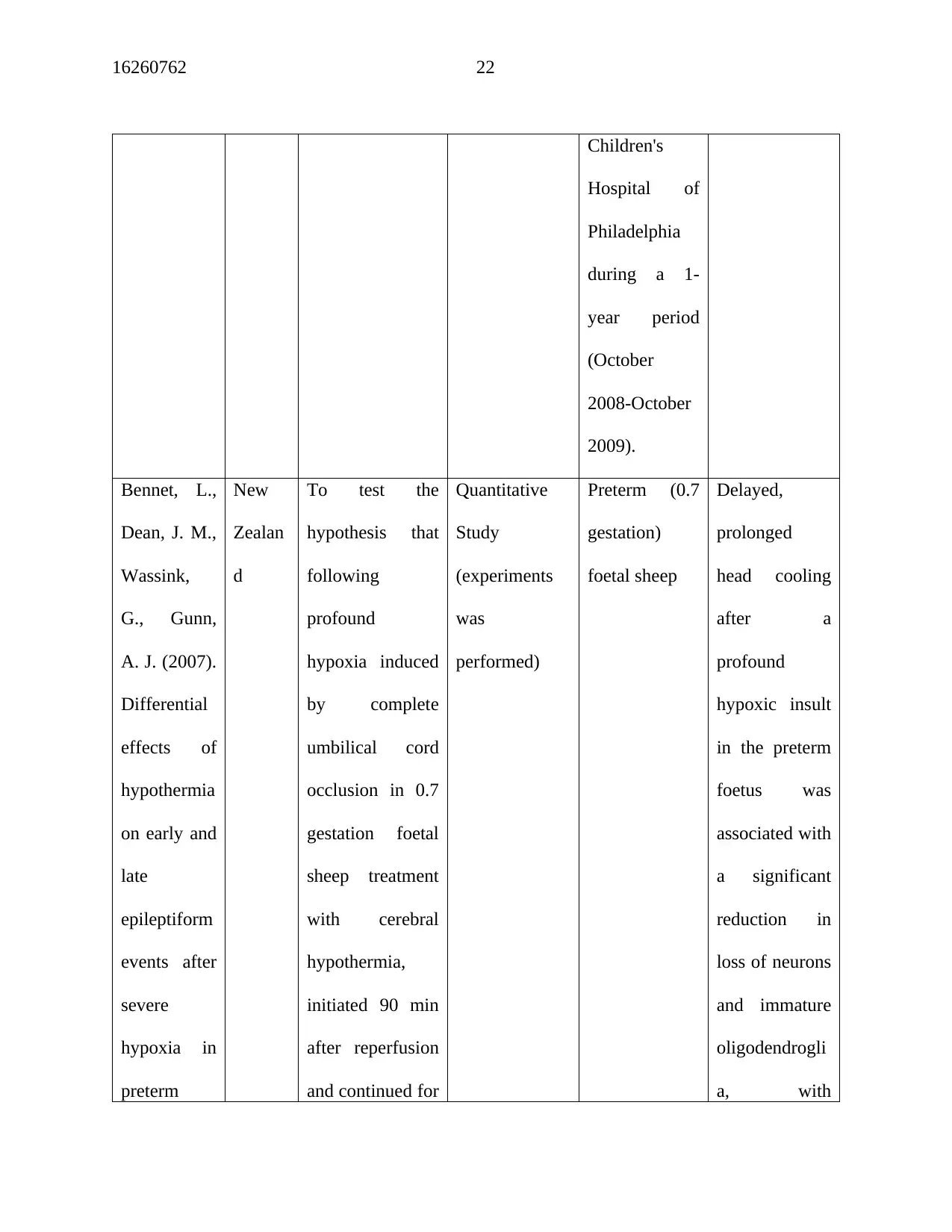
16260762 22
Children's
Hospital of
Philadelphia
during a 1-
year period
(October
2008-October
2009).
Bennet, L.,
Dean, J. M.,
Wassink,
G., Gunn,
A. J. (2007).
Differential
effects of
hypothermia
on early and
late
epileptiform
events after
severe
hypoxia in
preterm
New
Zealan
d
To test the
hypothesis that
following
profound
hypoxia induced
by complete
umbilical cord
occlusion in 0.7
gestation foetal
sheep treatment
with cerebral
hypothermia,
initiated 90 min
after reperfusion
and continued for
Quantitative
Study
(experiments
was
performed)
Preterm (0.7
gestation)
foetal sheep
Delayed,
prolonged
head cooling
after a
profound
hypoxic insult
in the preterm
foetus was
associated with
a significant
reduction in
loss of neurons
and immature
oligodendrogli
a, with
Children's
Hospital of
Philadelphia
during a 1-
year period
(October
2008-October
2009).
Bennet, L.,
Dean, J. M.,
Wassink,
G., Gunn,
A. J. (2007).
Differential
effects of
hypothermia
on early and
late
epileptiform
events after
severe
hypoxia in
preterm
New
Zealan
d
To test the
hypothesis that
following
profound
hypoxia induced
by complete
umbilical cord
occlusion in 0.7
gestation foetal
sheep treatment
with cerebral
hypothermia,
initiated 90 min
after reperfusion
and continued for
Quantitative
Study
(experiments
was
performed)
Preterm (0.7
gestation)
foetal sheep
Delayed,
prolonged
head cooling
after a
profound
hypoxic insult
in the preterm
foetus was
associated with
a significant
reduction in
loss of neurons
and immature
oligodendrogli
a, with
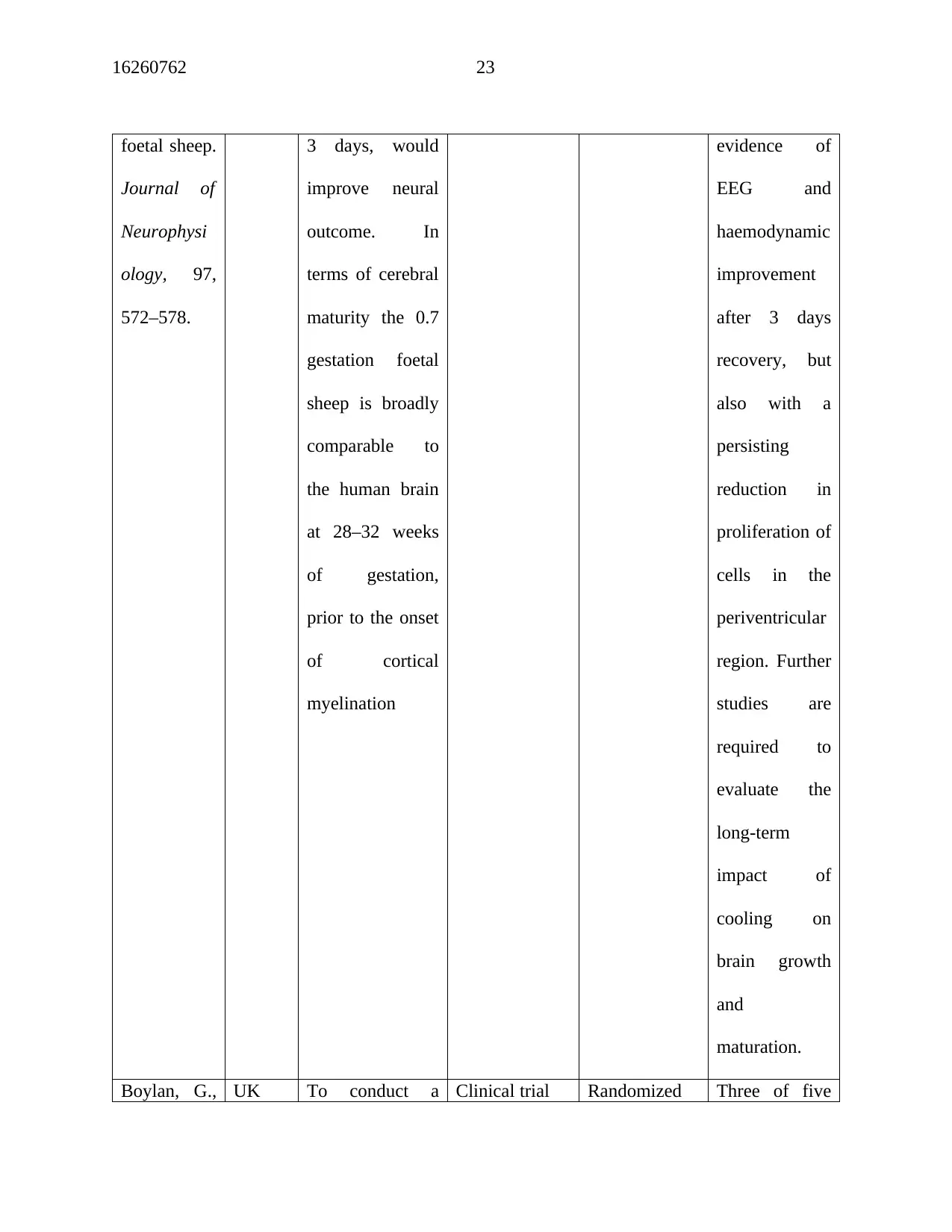
16260762 23
foetal sheep.
Journal of
Neurophysi
ology, 97,
572–578.
3 days, would
improve neural
outcome. In
terms of cerebral
maturity the 0.7
gestation foetal
sheep is broadly
comparable to
the human brain
at 28–32 weeks
of gestation,
prior to the onset
of cortical
myelination
evidence of
EEG and
haemodynamic
improvement
after 3 days
recovery, but
also with a
persisting
reduction in
proliferation of
cells in the
periventricular
region. Further
studies are
required to
evaluate the
long-term
impact of
cooling on
brain growth
and
maturation.
Boylan, G., UK To conduct a Clinical trial Randomized Three of five
foetal sheep.
Journal of
Neurophysi
ology, 97,
572–578.
3 days, would
improve neural
outcome. In
terms of cerebral
maturity the 0.7
gestation foetal
sheep is broadly
comparable to
the human brain
at 28–32 weeks
of gestation,
prior to the onset
of cortical
myelination
evidence of
EEG and
haemodynamic
improvement
after 3 days
recovery, but
also with a
persisting
reduction in
proliferation of
cells in the
periventricular
region. Further
studies are
required to
evaluate the
long-term
impact of
cooling on
brain growth
and
maturation.
Boylan, G., UK To conduct a Clinical trial Randomized Three of five
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16260762 24
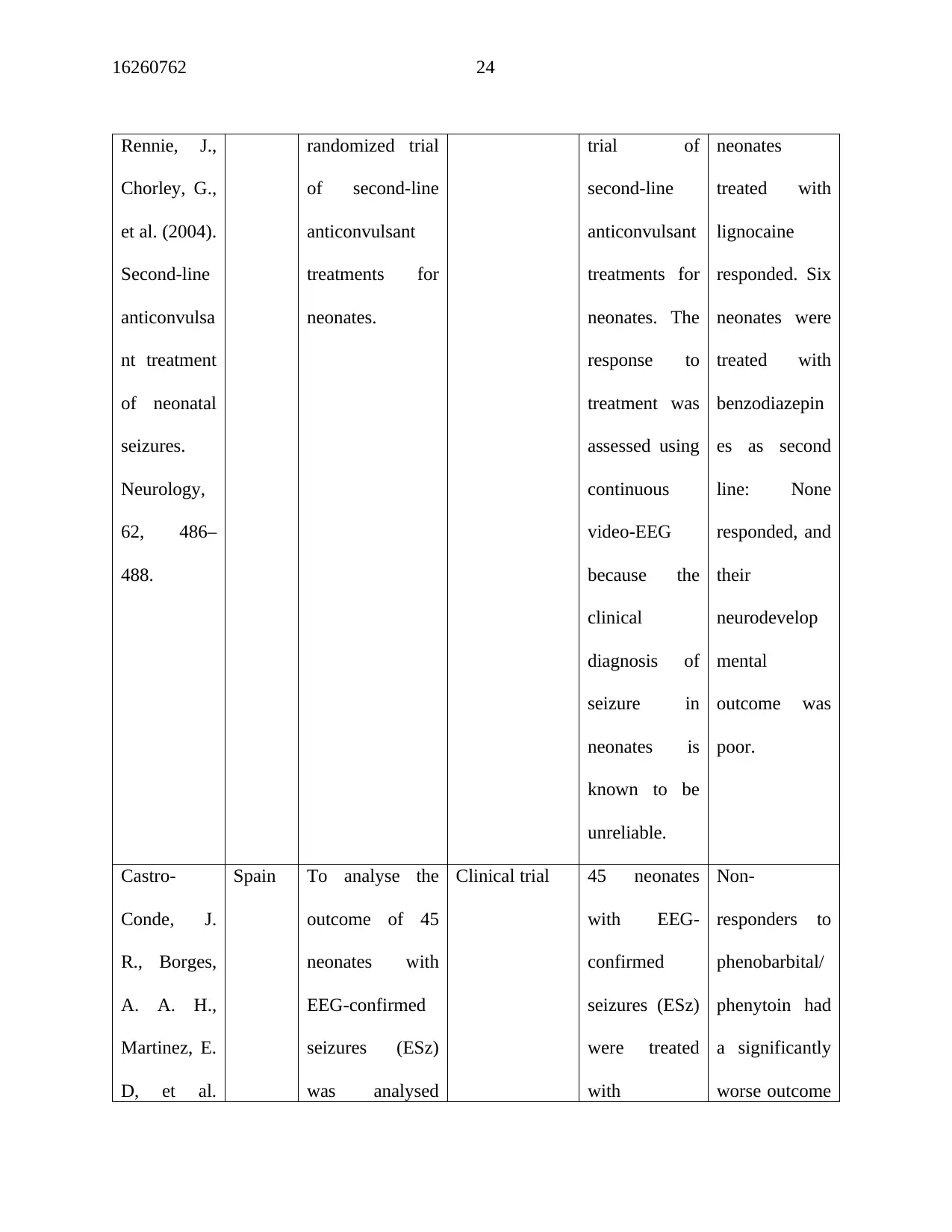
Rennie, J.,
Chorley, G.,
et al. (2004).
Second-line
anticonvulsa
nt treatment
of neonatal
seizures.
Neurology,
62, 486–
488.
randomized trial
of second-line
anticonvulsant
treatments for
neonates.
trial of
second-line
anticonvulsant
treatments for
neonates. The
response to
treatment was
assessed using
continuous
video-EEG
because the
clinical
diagnosis of
seizure in
neonates is
known to be
unreliable.
neonates
treated with
lignocaine
responded. Six
neonates were
treated with
benzodiazepin
es as second
line: None
responded, and
their
neurodevelop
mental
outcome was
poor.
Castro-
Conde, J.
R., Borges,
A. A. H.,
Martinez, E.
D, et al.
Spain To analyse the
outcome of 45
neonates with
EEG-confirmed
seizures (ESz)
was analysed
Clinical trial 45 neonates
with EEG-
confirmed
seizures (ESz)
were treated
with
Non-
responders to
phenobarbital/
phenytoin had
a significantly
worse outcome
Rennie, J.,
Chorley, G.,
et al. (2004).
Second-line
anticonvulsa
nt treatment
of neonatal
seizures.
Neurology,
62, 486–
488.
randomized trial
of second-line
anticonvulsant
treatments for
neonates.
trial of
second-line
anticonvulsant
treatments for
neonates. The
response to
treatment was
assessed using
continuous
video-EEG
because the
clinical
diagnosis of
seizure in
neonates is
known to be
unreliable.
neonates
treated with
lignocaine
responded. Six
neonates were
treated with
benzodiazepin
es as second
line: None
responded, and
their
neurodevelop
mental
outcome was
poor.
Castro-
Conde, J.
R., Borges,
A. A. H.,
Martinez, E.
D, et al.
Spain To analyse the
outcome of 45
neonates with
EEG-confirmed
seizures (ESz)
was analysed
Clinical trial 45 neonates
with EEG-
confirmed
seizures (ESz)
were treated
with
Non-
responders to
phenobarbital/
phenytoin had
a significantly
worse outcome
16260762 25
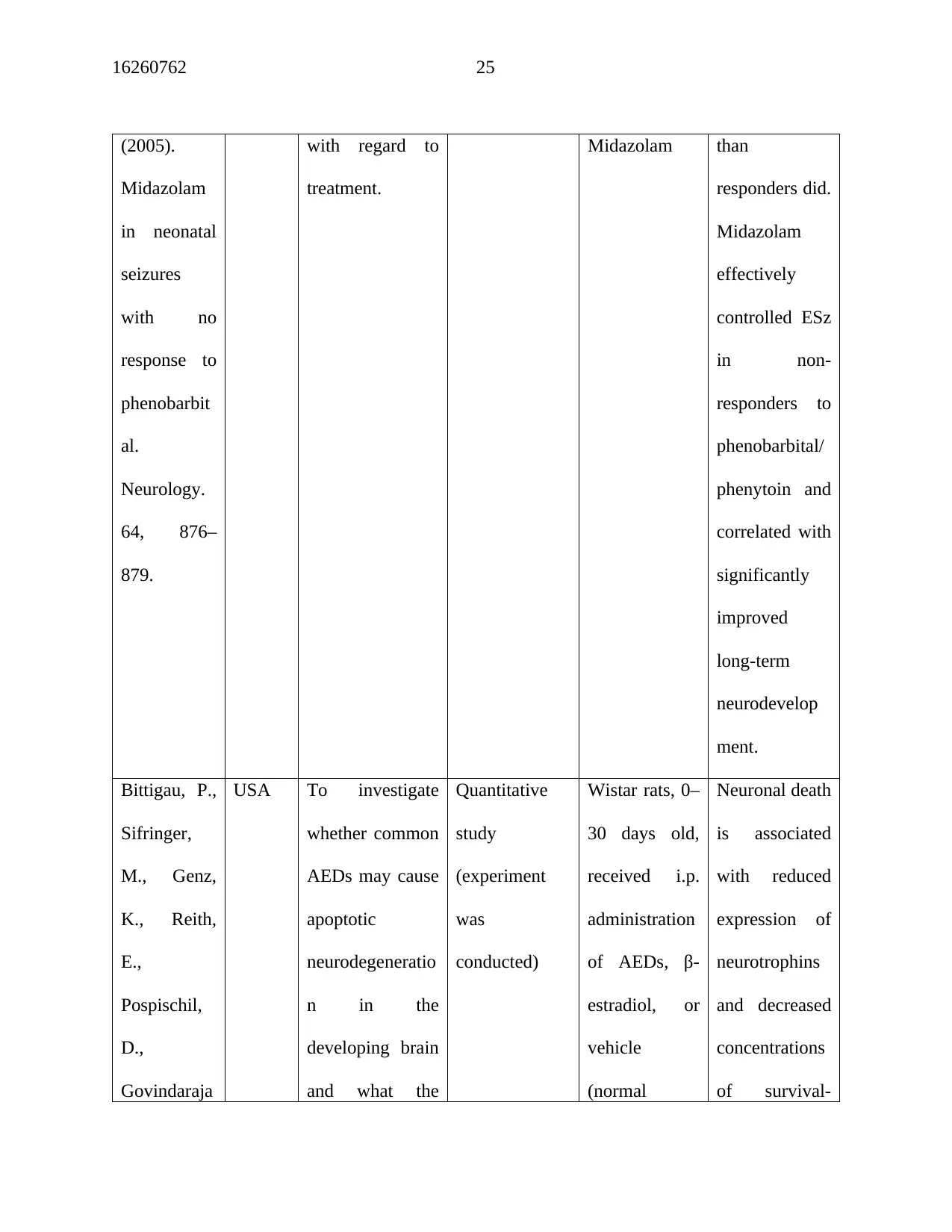
(2005).
Midazolam
in neonatal
seizures
with no
response to
phenobarbit
al.
Neurology.
64, 876–
879.
with regard to
treatment.
Midazolam than
responders did.
Midazolam
effectively
controlled ESz
in non-
responders to
phenobarbital/
phenytoin and
correlated with
significantly
improved
long-term
neurodevelop
ment.
Bittigau, P.,
Sifringer,
M., Genz,
K., Reith,
E.,
Pospischil,
D.,
Govindaraja
USA To investigate
whether common
AEDs may cause
apoptotic
neurodegeneratio
n in the
developing brain
and what the
Quantitative
study
(experiment
was
conducted)
Wistar rats, 0–
30 days old,
received i.p.
administration
of AEDs, β-
estradiol, or
vehicle
(normal
Neuronal death
is associated
with reduced
expression of
neurotrophins
and decreased
concentrations
of survival-
(2005).
Midazolam
in neonatal
seizures
with no
response to
phenobarbit
al.
Neurology.
64, 876–
879.
with regard to
treatment.
Midazolam than
responders did.
Midazolam
effectively
controlled ESz
in non-
responders to
phenobarbital/
phenytoin and
correlated with
significantly
improved
long-term
neurodevelop
ment.
Bittigau, P.,
Sifringer,
M., Genz,
K., Reith,
E.,
Pospischil,
D.,
Govindaraja
USA To investigate
whether common
AEDs may cause
apoptotic
neurodegeneratio
n in the
developing brain
and what the
Quantitative
study
(experiment
was
conducted)
Wistar rats, 0–
30 days old,
received i.p.
administration
of AEDs, β-
estradiol, or
vehicle
(normal
Neuronal death
is associated
with reduced
expression of
neurotrophins
and decreased
concentrations
of survival-
16260762 26
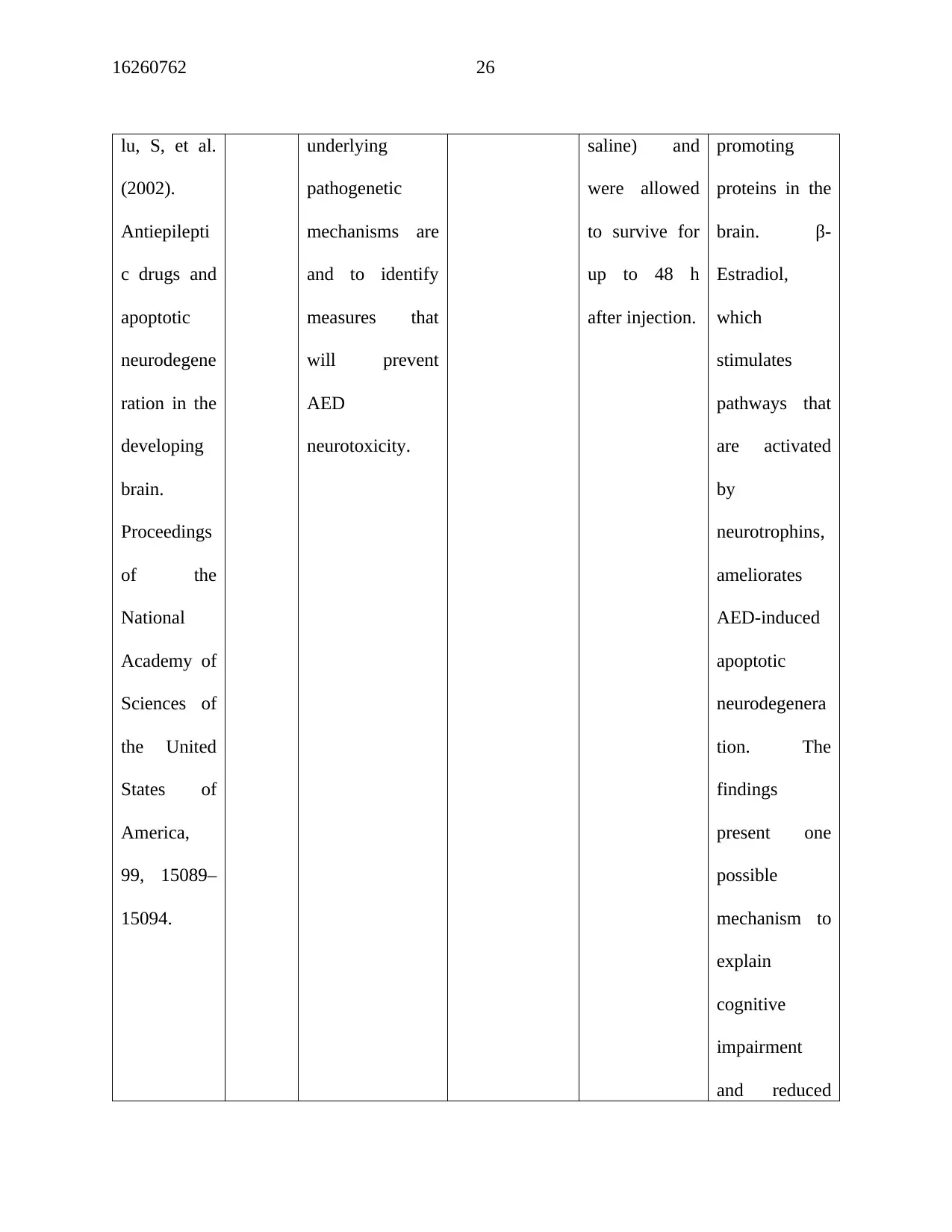
lu, S, et al.
(2002).
Antiepilepti
c drugs and
apoptotic
neurodegene
ration in the
developing
brain.
Proceedings
of the
National
Academy of
Sciences of
the United
States of
America,
99, 15089–
15094.
underlying
pathogenetic
mechanisms are
and to identify
measures that
will prevent
AED
neurotoxicity.
saline) and
were allowed
to survive for
up to 48 h
after injection.
promoting
proteins in the
brain. β-
Estradiol,
which
stimulates
pathways that
are activated
by
neurotrophins,
ameliorates
AED-induced
apoptotic
neurodegenera
tion. The
findings
present one
possible
mechanism to
explain
cognitive
impairment
and reduced
lu, S, et al.
(2002).
Antiepilepti
c drugs and
apoptotic
neurodegene
ration in the
developing
brain.
Proceedings
of the
National
Academy of
Sciences of
the United
States of
America,
99, 15089–
15094.
underlying
pathogenetic
mechanisms are
and to identify
measures that
will prevent
AED
neurotoxicity.
saline) and
were allowed
to survive for
up to 48 h
after injection.
promoting
proteins in the
brain. β-
Estradiol,
which
stimulates
pathways that
are activated
by
neurotrophins,
ameliorates
AED-induced
apoptotic
neurodegenera
tion. The
findings
present one
possible
mechanism to
explain
cognitive
impairment
and reduced
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
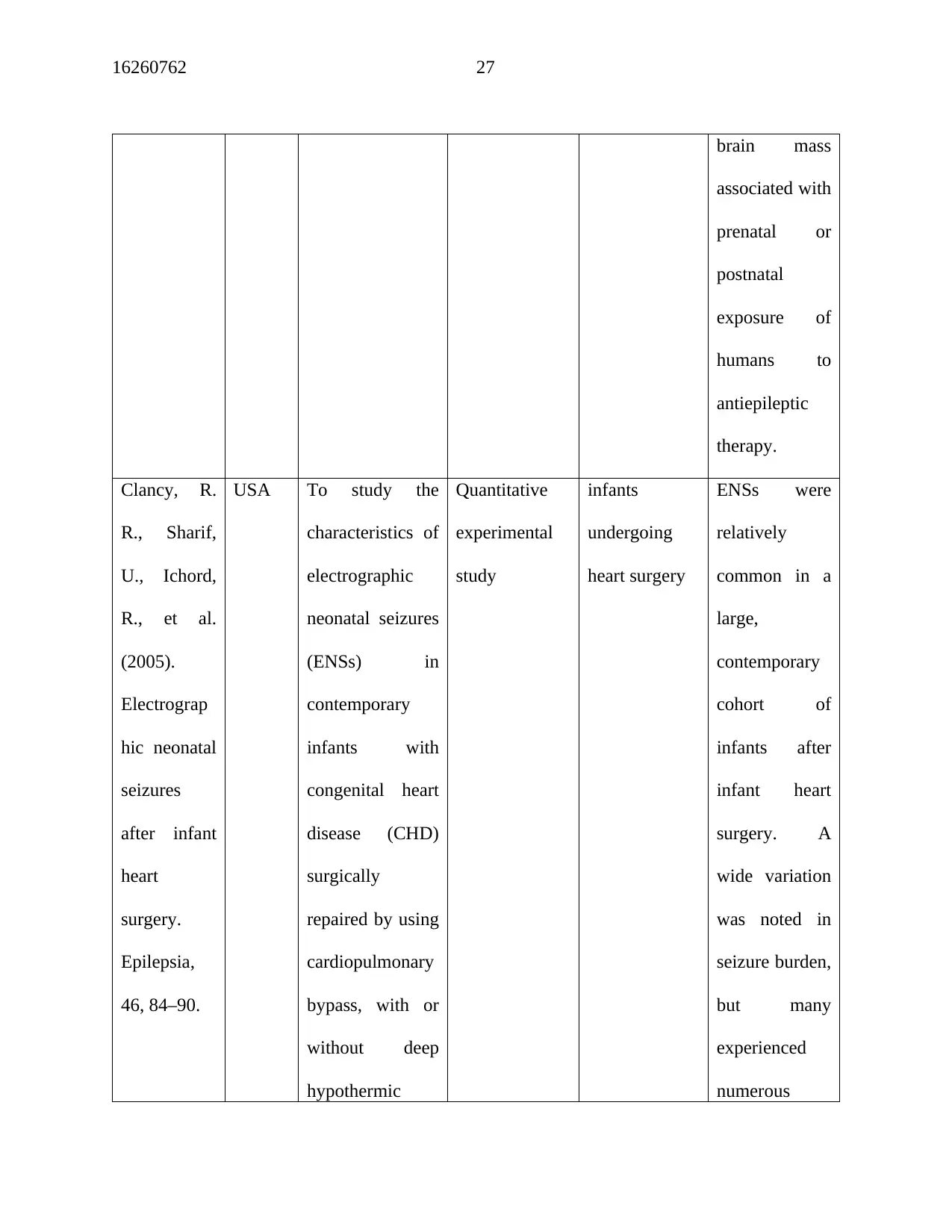
16260762 27
brain mass
associated with
prenatal or
postnatal
exposure of
humans to
antiepileptic
therapy.
Clancy, R.
R., Sharif,
U., Ichord,
R., et al.
(2005).
Electrograp
hic neonatal
seizures
after infant
heart
surgery.
Epilepsia,
46, 84–90.
USA To study the
characteristics of
electrographic
neonatal seizures
(ENSs) in
contemporary
infants with
congenital heart
disease (CHD)
surgically
repaired by using
cardiopulmonary
bypass, with or
without deep
hypothermic
Quantitative
experimental
study
infants
undergoing
heart surgery
ENSs were
relatively
common in a
large,
contemporary
cohort of
infants after
infant heart
surgery. A
wide variation
was noted in
seizure burden,
but many
experienced
numerous
brain mass
associated with
prenatal or
postnatal
exposure of
humans to
antiepileptic
therapy.
Clancy, R.
R., Sharif,
U., Ichord,
R., et al.
(2005).
Electrograp
hic neonatal
seizures
after infant
heart
surgery.
Epilepsia,
46, 84–90.
USA To study the
characteristics of
electrographic
neonatal seizures
(ENSs) in
contemporary
infants with
congenital heart
disease (CHD)
surgically
repaired by using
cardiopulmonary
bypass, with or
without deep
hypothermic
Quantitative
experimental
study
infants
undergoing
heart surgery
ENSs were
relatively
common in a
large,
contemporary
cohort of
infants after
infant heart
surgery. A
wide variation
was noted in
seizure burden,
but many
experienced
numerous
16260762 28
circulatory arrest. seizures.
Electrographic
neonatal
seizures are a
candidate
outcome end
in future
neuroprotectio
n trials in this
patient
population.
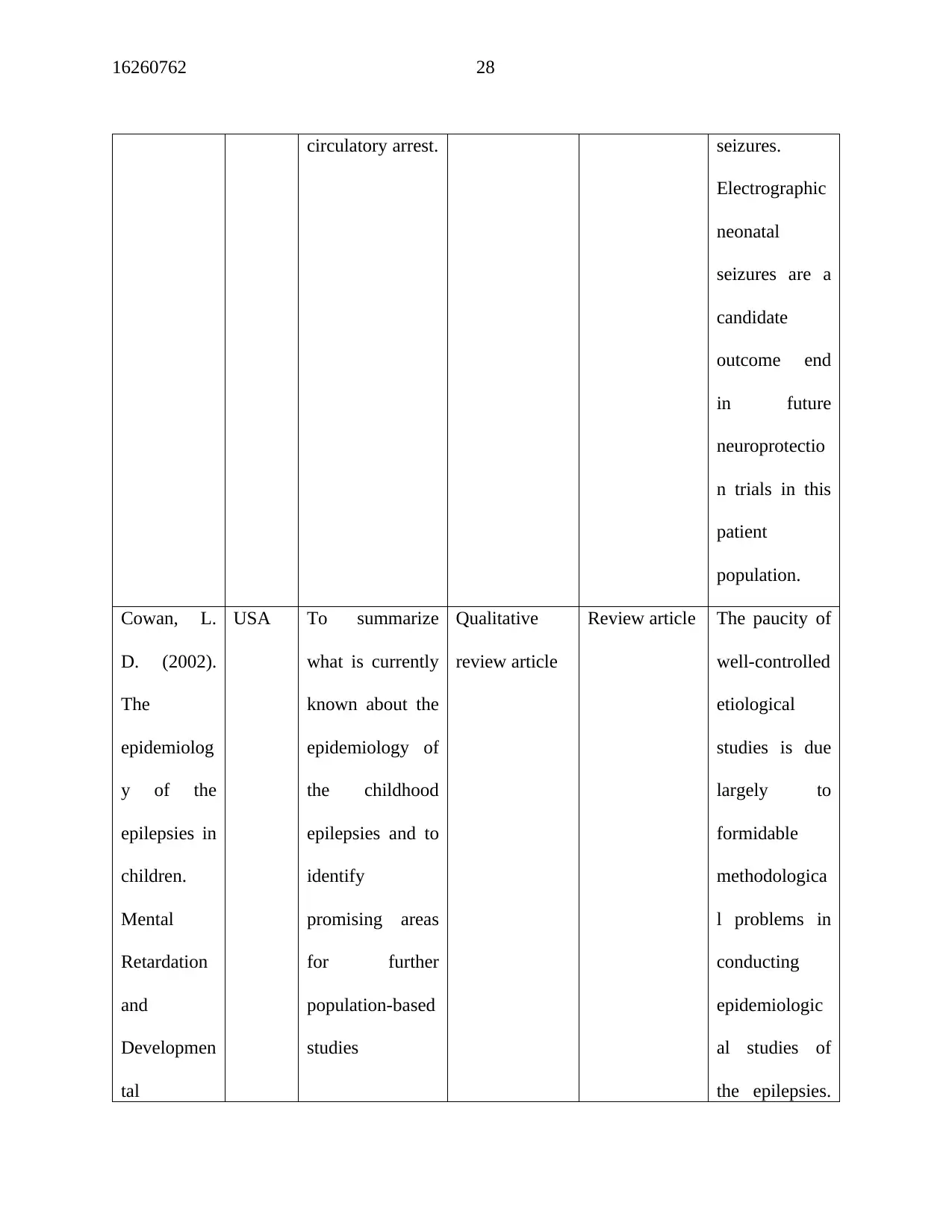
Cowan, L.
D. (2002).
The
epidemiolog
y of the
epilepsies in
children.
Mental
Retardation
and
Developmen
tal
USA To summarize
what is currently
known about the
epidemiology of
the childhood
epilepsies and to
identify
promising areas
for further
population-based
studies
Qualitative
review article
Review article The paucity of
well-controlled
etiological
studies is due
largely to
formidable
methodologica
l problems in
conducting
epidemiologic
al studies of
the epilepsies.
circulatory arrest. seizures.
Electrographic
neonatal
seizures are a
candidate
outcome end
in future
neuroprotectio
n trials in this
patient
population.
Cowan, L.
D. (2002).
The
epidemiolog
y of the
epilepsies in
children.
Mental
Retardation
and
Developmen
tal
USA To summarize
what is currently
known about the
epidemiology of
the childhood
epilepsies and to
identify
promising areas
for further
population-based
studies
Qualitative
review article
Review article The paucity of
well-controlled
etiological
studies is due
largely to
formidable
methodologica
l problems in
conducting
epidemiologic
al studies of
the epilepsies.
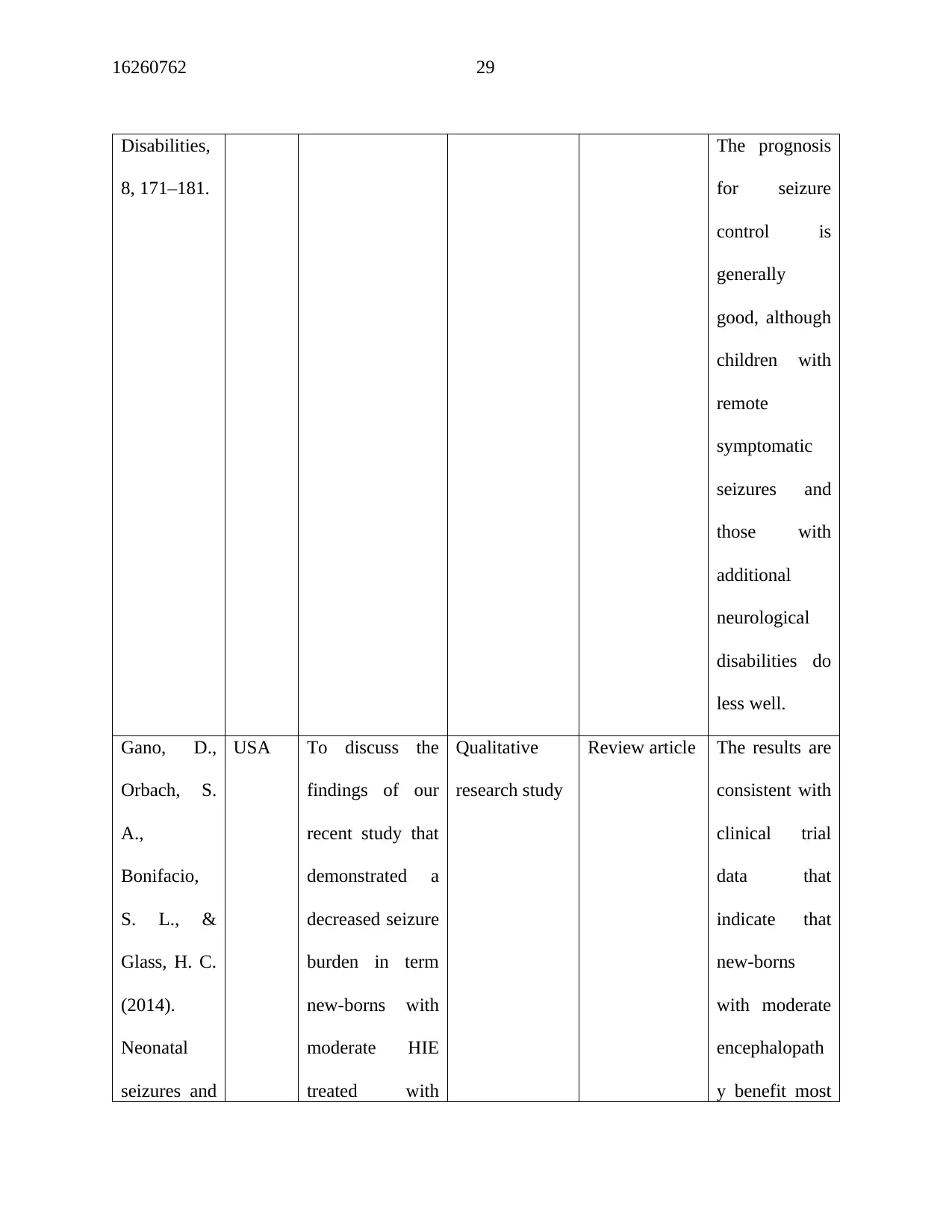
16260762 29
Disabilities,
8, 171–181.
The prognosis
for seizure
control is
generally
good, although
children with
remote
symptomatic
seizures and
those with
additional
neurological
disabilities do
less well.
Gano, D.,
Orbach, S.
A.,
Bonifacio,
S. L., &
Glass, H. C.
(2014).
Neonatal
seizures and
USA To discuss the
findings of our
recent study that
demonstrated a
decreased seizure
burden in term
new-borns with
moderate HIE
treated with
Qualitative
research study
Review article The results are
consistent with
clinical trial
data that
indicate that
new-borns
with moderate
encephalopath
y benefit most
Disabilities,
8, 171–181.
The prognosis
for seizure
control is
generally
good, although
children with
remote
symptomatic
seizures and
those with
additional
neurological
disabilities do
less well.
Gano, D.,
Orbach, S.
A.,
Bonifacio,
S. L., &
Glass, H. C.
(2014).
Neonatal
seizures and
USA To discuss the
findings of our
recent study that
demonstrated a
decreased seizure
burden in term
new-borns with
moderate HIE
treated with
Qualitative
research study
Review article The results are
consistent with
clinical trial
data that
indicate that
new-borns
with moderate
encephalopath
y benefit most
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
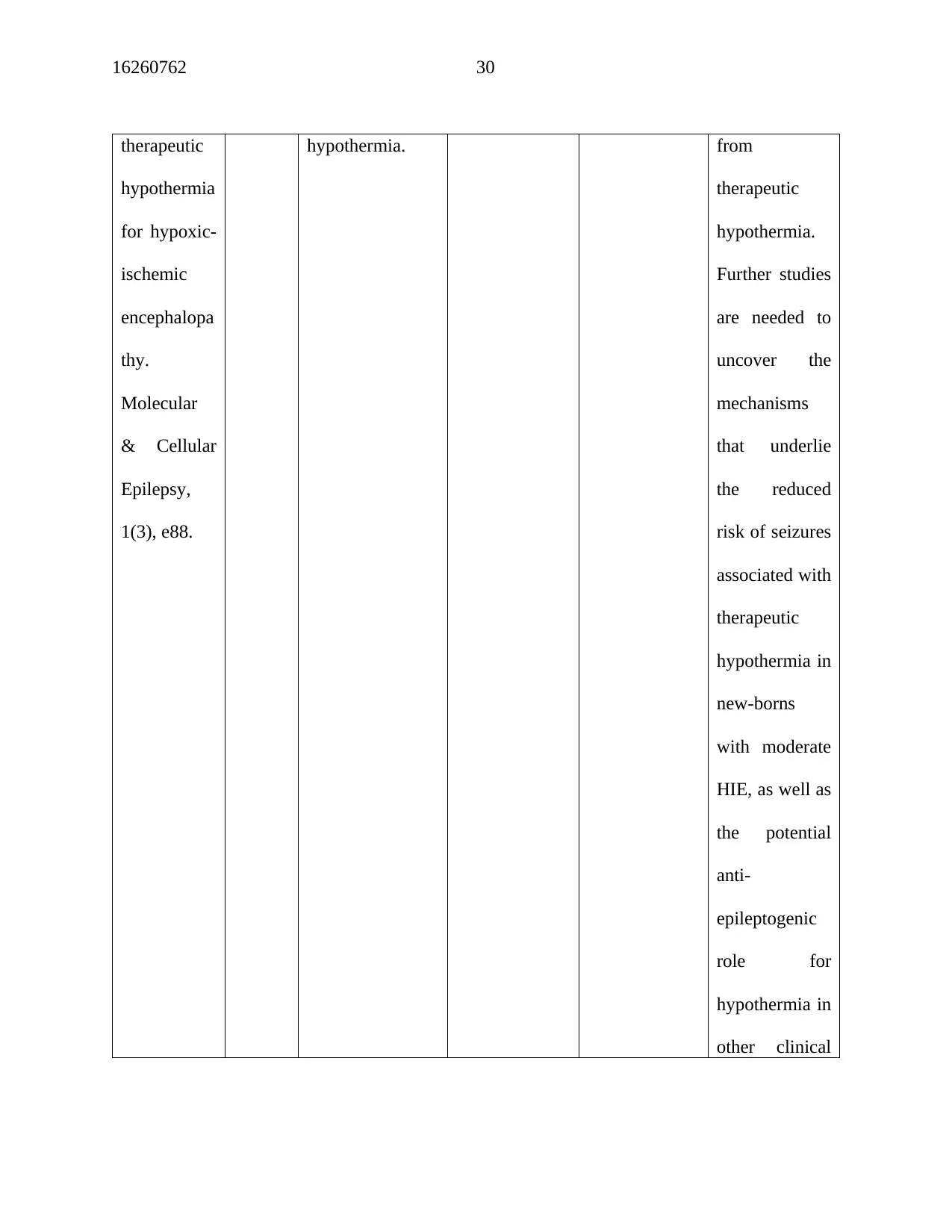
16260762 30
therapeutic
hypothermia
for hypoxic-
ischemic
encephalopa
thy.
Molecular
& Cellular
Epilepsy,
1(3), e88.
hypothermia. from
therapeutic
hypothermia.
Further studies
are needed to
uncover the
mechanisms
that underlie
the reduced
risk of seizures
associated with
therapeutic
hypothermia in
new-borns
with moderate
HIE, as well as
the potential
anti-
epileptogenic
role for
hypothermia in
other clinical
therapeutic
hypothermia
for hypoxic-
ischemic
encephalopa
thy.
Molecular
& Cellular
Epilepsy,
1(3), e88.
hypothermia. from
therapeutic
hypothermia.
Further studies
are needed to
uncover the
mechanisms
that underlie
the reduced
risk of seizures
associated with
therapeutic
hypothermia in
new-borns
with moderate
HIE, as well as
the potential
anti-
epileptogenic
role for
hypothermia in
other clinical
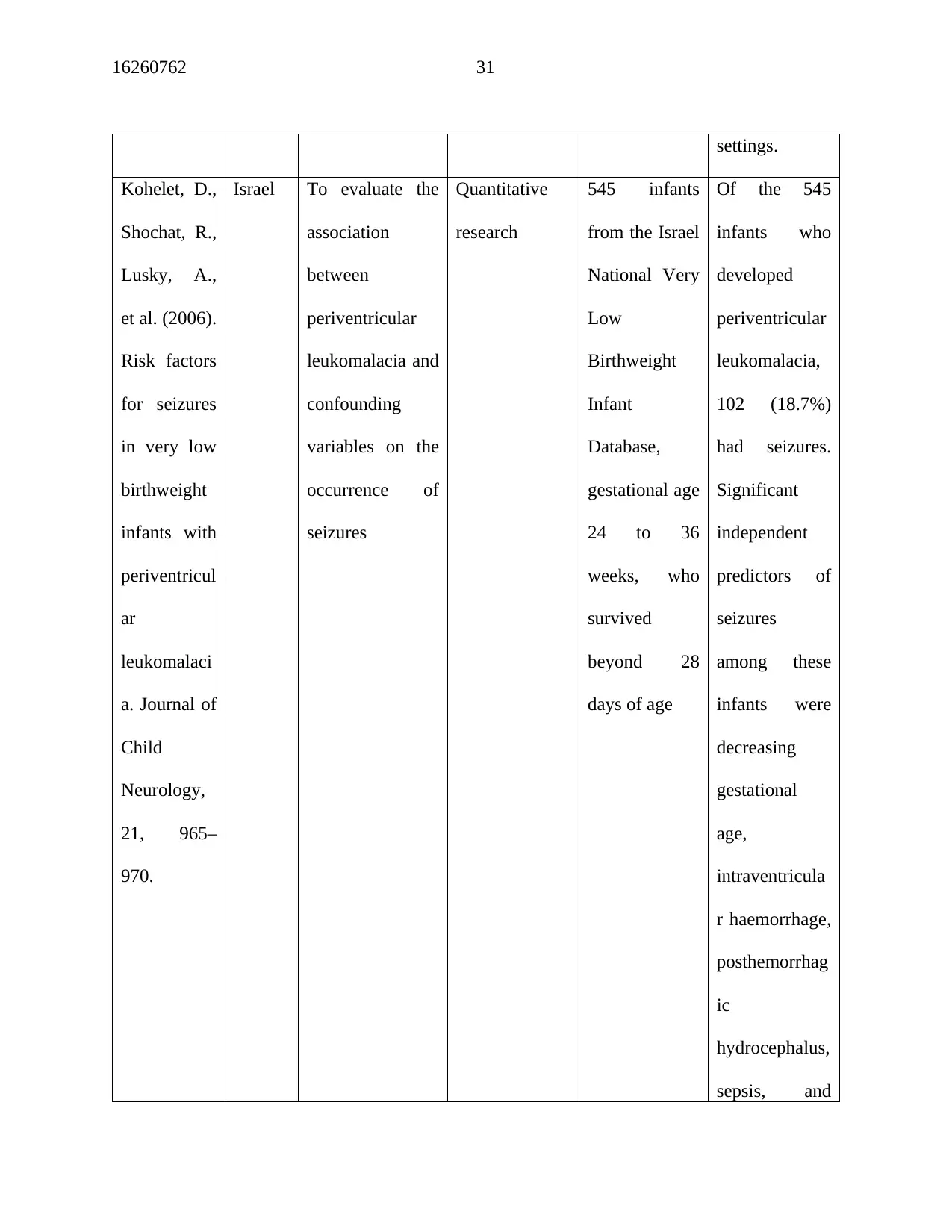
16260762 31
settings.
Kohelet, D.,
Shochat, R.,
Lusky, A.,
et al. (2006).
Risk factors
for seizures
in very low
birthweight
infants with
periventricul
ar
leukomalaci
a. Journal of
Child
Neurology,
21, 965–
970.
Israel To evaluate the
association
between
periventricular
leukomalacia and
confounding
variables on the
occurrence of
seizures
Quantitative
research
545 infants
from the Israel
National Very
Low
Birthweight
Infant
Database,
gestational age
24 to 36
weeks, who
survived
beyond 28
days of age
Of the 545
infants who
developed
periventricular
leukomalacia,
102 (18.7%)
had seizures.
Significant
independent
predictors of
seizures
among these
infants were
decreasing
gestational
age,
intraventricula
r haemorrhage,
posthemorrhag
ic
hydrocephalus,
sepsis, and
settings.
Kohelet, D.,
Shochat, R.,
Lusky, A.,
et al. (2006).
Risk factors
for seizures
in very low
birthweight
infants with
periventricul
ar
leukomalaci
a. Journal of
Child
Neurology,
21, 965–
970.
Israel To evaluate the
association
between
periventricular
leukomalacia and
confounding
variables on the
occurrence of
seizures
Quantitative
research
545 infants
from the Israel
National Very
Low
Birthweight
Infant
Database,
gestational age
24 to 36
weeks, who
survived
beyond 28
days of age
Of the 545
infants who
developed
periventricular
leukomalacia,
102 (18.7%)
had seizures.
Significant
independent
predictors of
seizures
among these
infants were
decreasing
gestational
age,
intraventricula
r haemorrhage,
posthemorrhag
ic
hydrocephalus,
sepsis, and
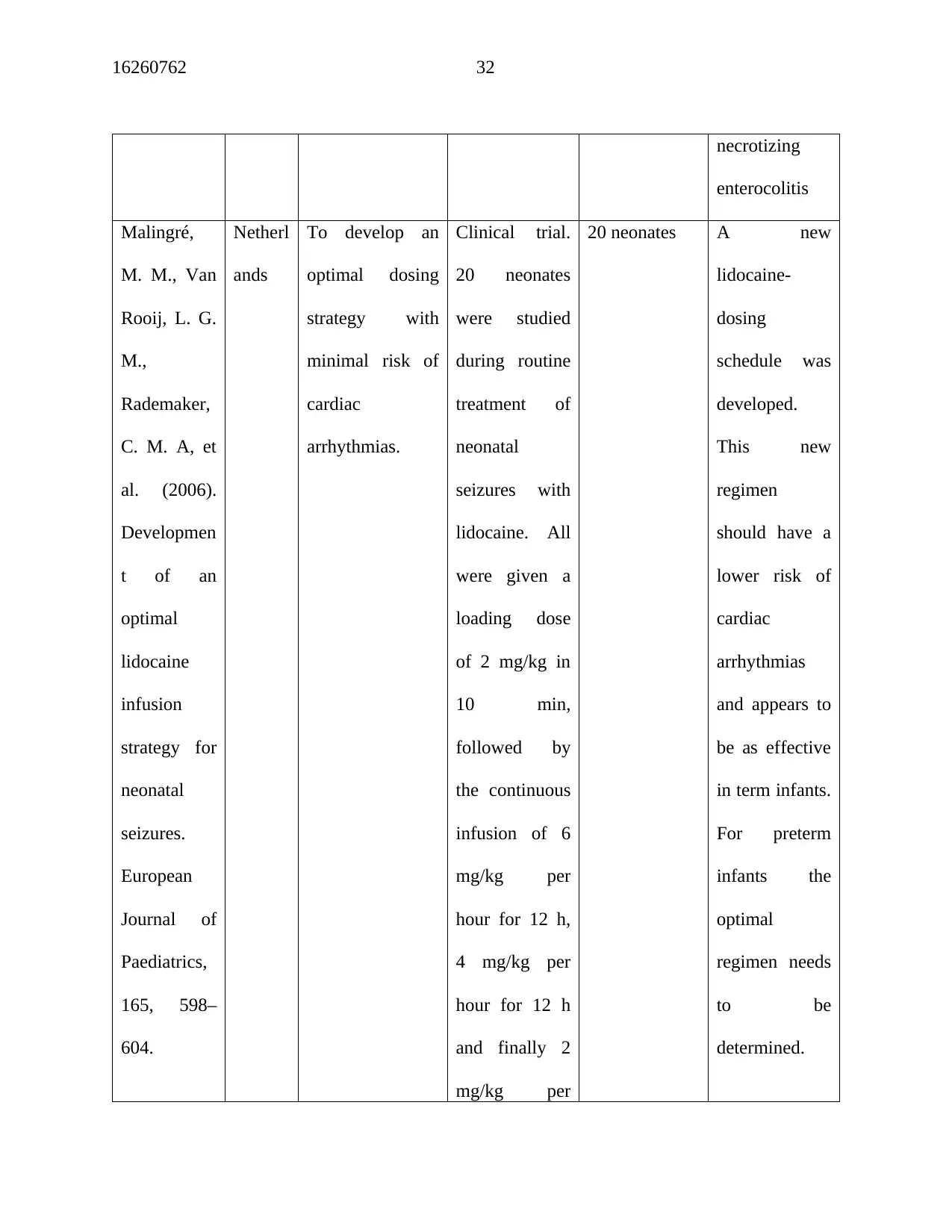
16260762 32
necrotizing
enterocolitis
Malingré,
M. M., Van
Rooij, L. G.
M.,
Rademaker,
C. M. A, et
al. (2006).
Developmen
t of an
optimal
lidocaine
infusion
strategy for
neonatal
seizures.
European
Journal of
Paediatrics,
165, 598–
604.
Netherl
ands
To develop an
optimal dosing
strategy with
minimal risk of
cardiac
arrhythmias.
Clinical trial.
20 neonates
were studied
during routine
treatment of
neonatal
seizures with
lidocaine. All
were given a
loading dose
of 2 mg/kg in
10 min,
followed by
the continuous
infusion of 6
mg/kg per
hour for 12 h,
4 mg/kg per
hour for 12 h
and finally 2
mg/kg per
20 neonates A new
lidocaine-
dosing
schedule was
developed.
This new
regimen
should have a
lower risk of
cardiac
arrhythmias
and appears to
be as effective
in term infants.
For preterm
infants the
optimal
regimen needs
to be
determined.
necrotizing
enterocolitis
Malingré,
M. M., Van
Rooij, L. G.
M.,
Rademaker,
C. M. A, et
al. (2006).
Developmen
t of an
optimal
lidocaine
infusion
strategy for
neonatal
seizures.
European
Journal of
Paediatrics,
165, 598–
604.
Netherl
ands
To develop an
optimal dosing
strategy with
minimal risk of
cardiac
arrhythmias.
Clinical trial.
20 neonates
were studied
during routine
treatment of
neonatal
seizures with
lidocaine. All
were given a
loading dose
of 2 mg/kg in
10 min,
followed by
the continuous
infusion of 6
mg/kg per
hour for 12 h,
4 mg/kg per
hour for 12 h
and finally 2
mg/kg per
20 neonates A new
lidocaine-
dosing
schedule was
developed.
This new
regimen
should have a
lower risk of
cardiac
arrhythmias
and appears to
be as effective
in term infants.
For preterm
infants the
optimal
regimen needs
to be
determined.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
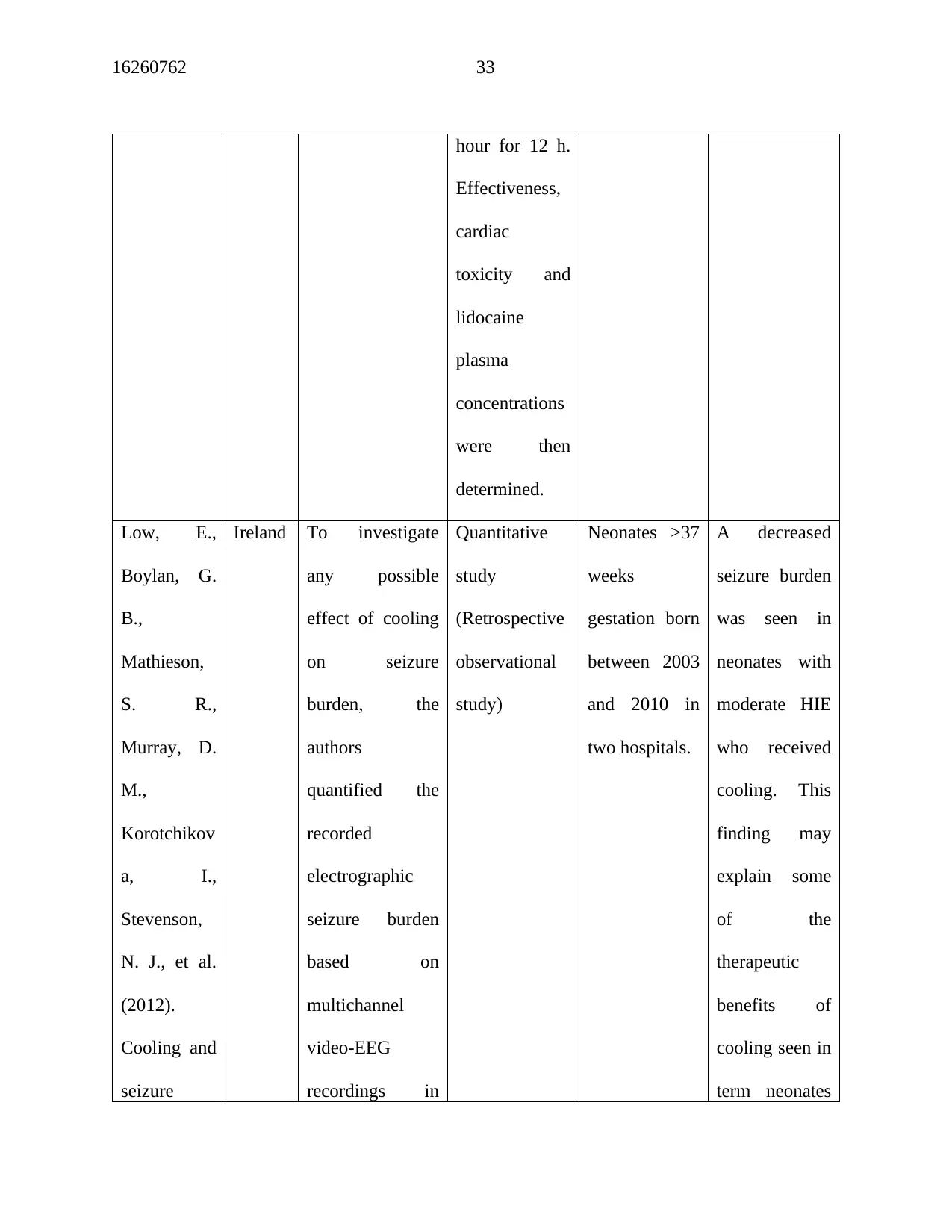
16260762 33
hour for 12 h.
Effectiveness,
cardiac
toxicity and
lidocaine
plasma
concentrations
were then
determined.
Low, E.,
Boylan, G.
B.,
Mathieson,
S. R.,
Murray, D.
M.,
Korotchikov
a, I.,
Stevenson,
N. J., et al.
(2012).
Cooling and
seizure
Ireland To investigate
any possible
effect of cooling
on seizure
burden, the
authors
quantified the
recorded
electrographic
seizure burden
based on
multichannel
video-EEG
recordings in
Quantitative
study
(Retrospective
observational
study)
Neonates >37
weeks
gestation born
between 2003
and 2010 in
two hospitals.
A decreased
seizure burden
was seen in
neonates with
moderate HIE
who received
cooling. This
finding may
explain some
of the
therapeutic
benefits of
cooling seen in
term neonates
hour for 12 h.
Effectiveness,
cardiac
toxicity and
lidocaine
plasma
concentrations
were then
determined.
Low, E.,
Boylan, G.
B.,
Mathieson,
S. R.,
Murray, D.
M.,
Korotchikov
a, I.,
Stevenson,
N. J., et al.
(2012).
Cooling and
seizure
Ireland To investigate
any possible
effect of cooling
on seizure
burden, the
authors
quantified the
recorded
electrographic
seizure burden
based on
multichannel
video-EEG
recordings in
Quantitative
study
(Retrospective
observational
study)
Neonates >37
weeks
gestation born
between 2003
and 2010 in
two hospitals.
A decreased
seizure burden
was seen in
neonates with
moderate HIE
who received
cooling. This
finding may
explain some
of the
therapeutic
benefits of
cooling seen in
term neonates
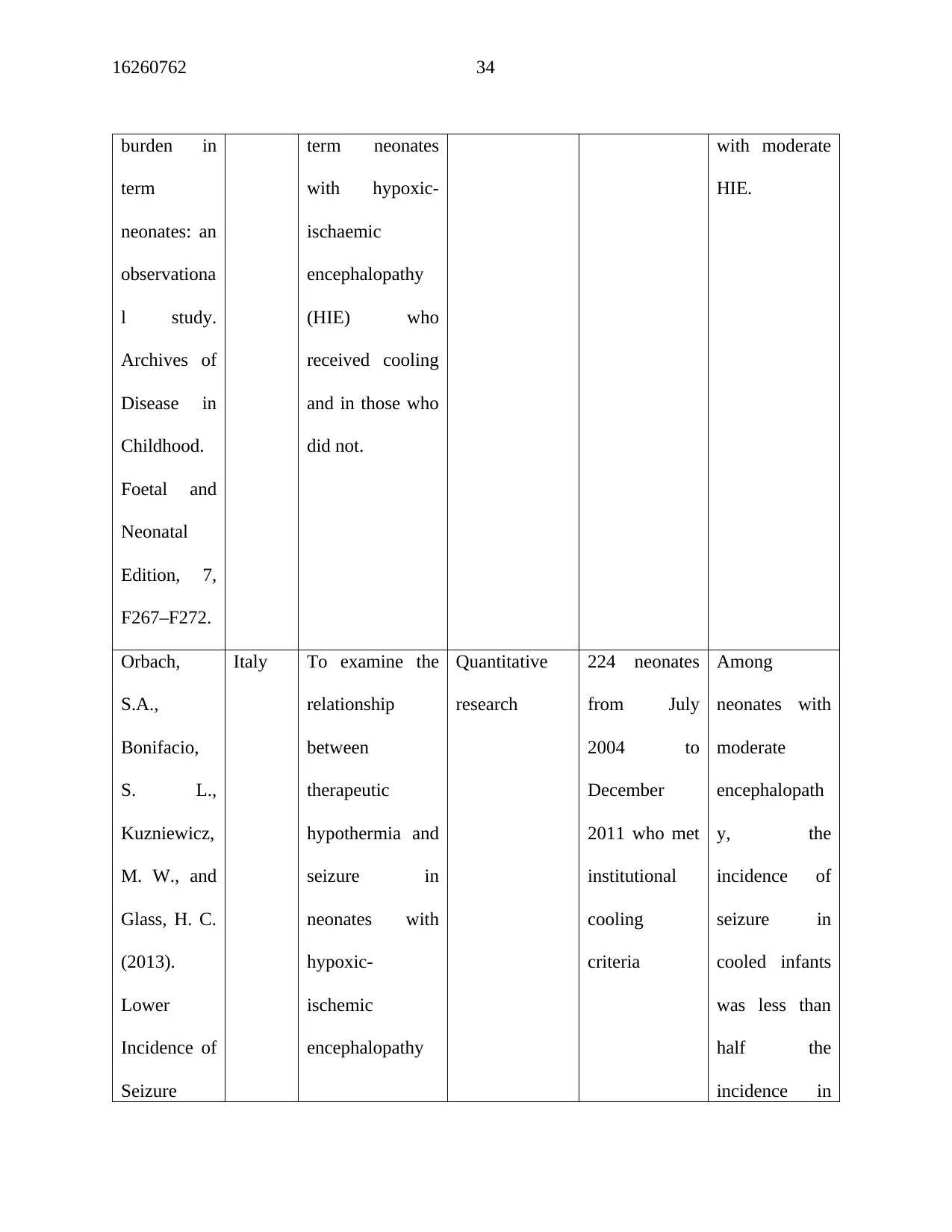
16260762 34
burden in
term
neonates: an
observationa
l study.
Archives of
Disease in
Childhood.
Foetal and
Neonatal
Edition, 7,
F267–F272.
term neonates
with hypoxic-
ischaemic
encephalopathy
(HIE) who
received cooling
and in those who
did not.
with moderate
HIE.
Orbach,
S.A.,
Bonifacio,
S. L.,
Kuzniewicz,
M. W., and
Glass, H. C.
(2013).
Lower
Incidence of
Seizure
Italy To examine the
relationship
between
therapeutic
hypothermia and
seizure in
neonates with
hypoxic-
ischemic
encephalopathy
Quantitative
research
224 neonates
from July
2004 to
December
2011 who met
institutional
cooling
criteria
Among
neonates with
moderate
encephalopath
y, the
incidence of
seizure in
cooled infants
was less than
half the
incidence in
burden in
term
neonates: an
observationa
l study.
Archives of
Disease in
Childhood.
Foetal and
Neonatal
Edition, 7,
F267–F272.
term neonates
with hypoxic-
ischaemic
encephalopathy
(HIE) who
received cooling
and in those who
did not.
with moderate
HIE.
Orbach,
S.A.,
Bonifacio,
S. L.,
Kuzniewicz,
M. W., and
Glass, H. C.
(2013).
Lower
Incidence of
Seizure
Italy To examine the
relationship
between
therapeutic
hypothermia and
seizure in
neonates with
hypoxic-
ischemic
encephalopathy
Quantitative
research
224 neonates
from July
2004 to
December
2011 who met
institutional
cooling
criteria
Among
neonates with
moderate
encephalopath
y, the
incidence of
seizure in
cooled infants
was less than
half the
incidence in
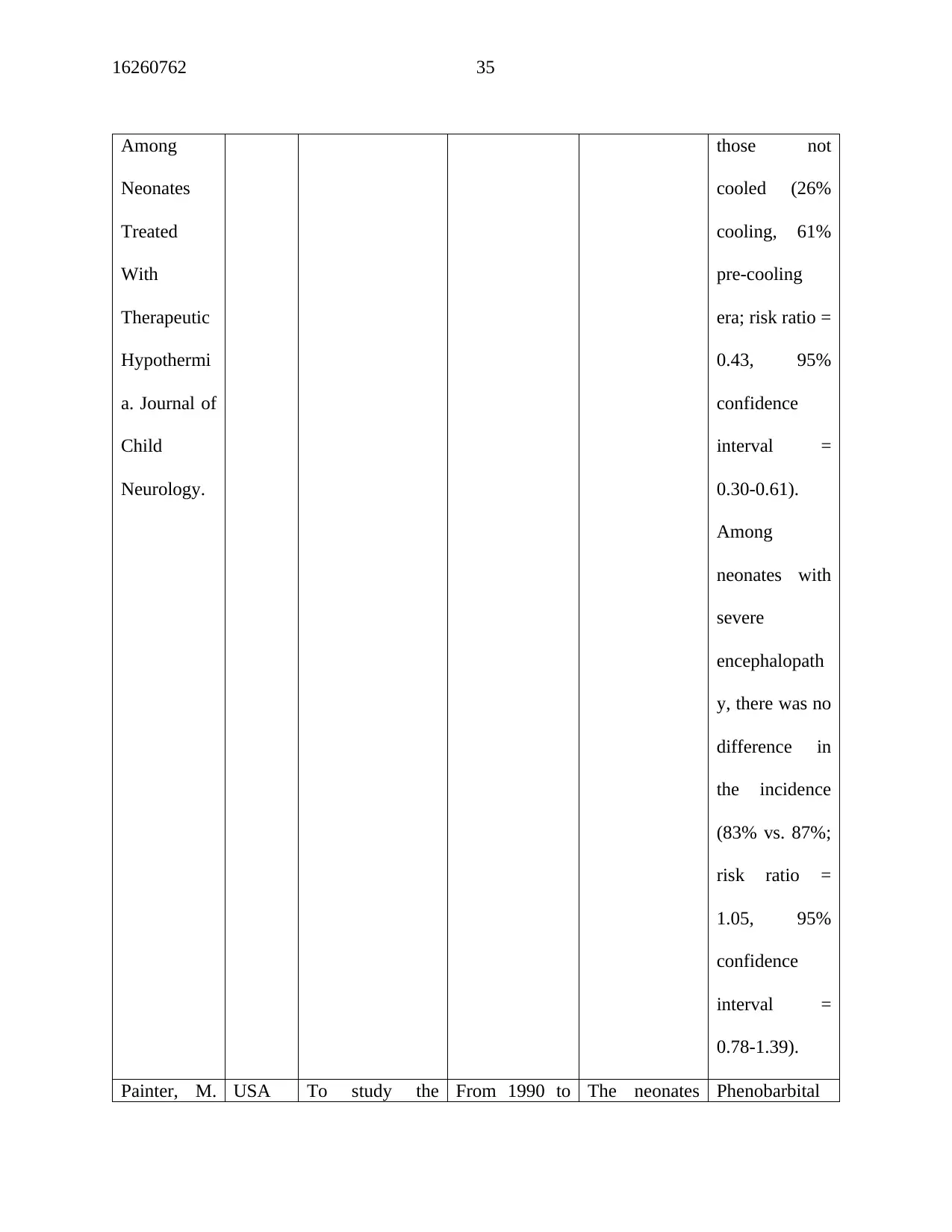
16260762 35
Among
Neonates
Treated
With
Therapeutic
Hypothermi
a. Journal of
Child
Neurology.
those not
cooled (26%
cooling, 61%
pre-cooling
era; risk ratio =
0.43, 95%
confidence
interval =
0.30-0.61).
Among
neonates with
severe
encephalopath
y, there was no
difference in
the incidence
(83% vs. 87%;
risk ratio =
1.05, 95%
confidence
interval =
0.78-1.39).
Painter, M. USA To study the From 1990 to The neonates Phenobarbital
Among
Neonates
Treated
With
Therapeutic
Hypothermi
a. Journal of
Child
Neurology.
those not
cooled (26%
cooling, 61%
pre-cooling
era; risk ratio =
0.43, 95%
confidence
interval =
0.30-0.61).
Among
neonates with
severe
encephalopath
y, there was no
difference in
the incidence
(83% vs. 87%;
risk ratio =
1.05, 95%
confidence
interval =
0.78-1.39).
Painter, M. USA To study the From 1990 to The neonates Phenobarbital
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
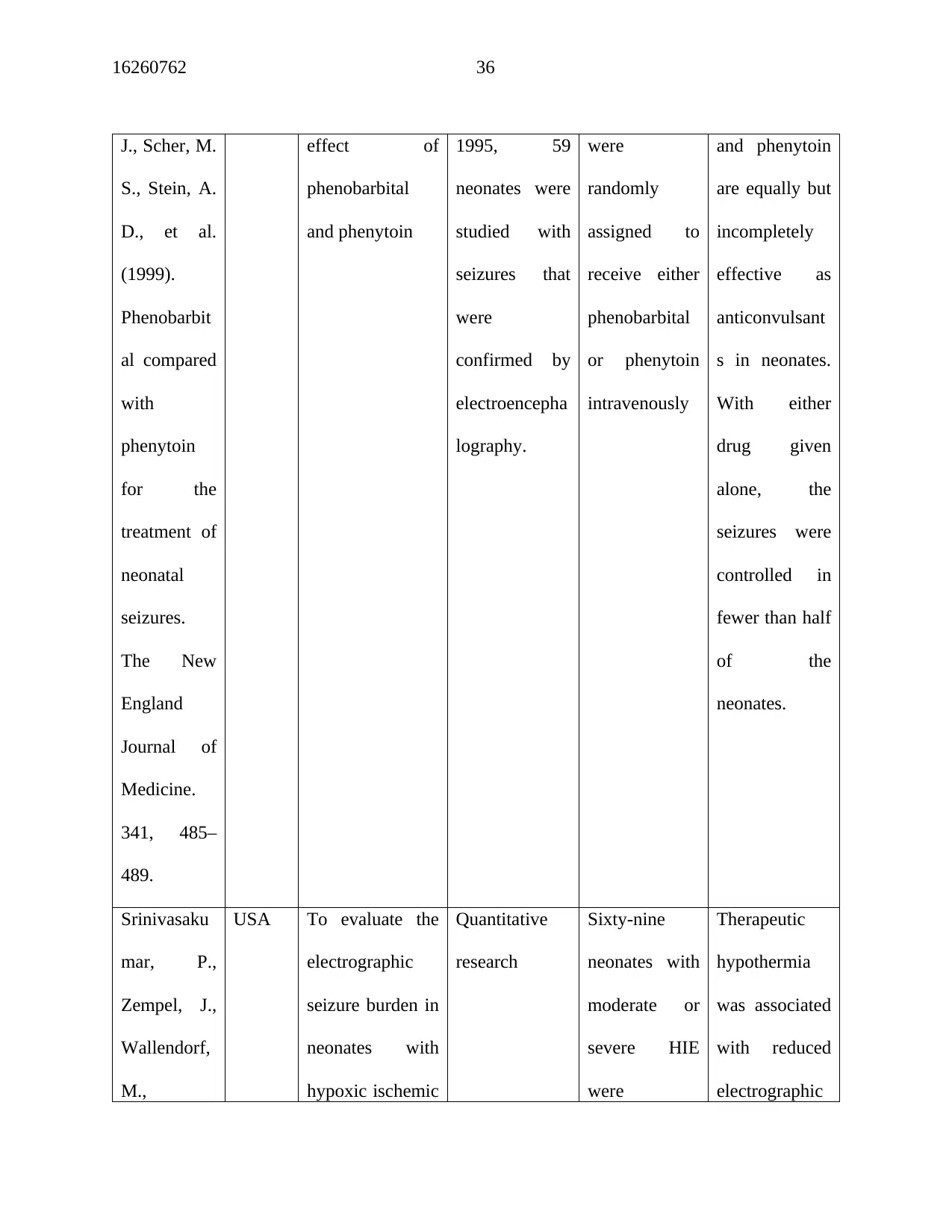
16260762 36
J., Scher, M.
S., Stein, A.
D., et al.
(1999).
Phenobarbit
al compared
with
phenytoin
for the
treatment of
neonatal
seizures.
The New
England
Journal of
Medicine.
341, 485–
489.
effect of
phenobarbital
and phenytoin
1995, 59
neonates were
studied with
seizures that
were
confirmed by
electroencepha
lography.
were
randomly
assigned to
receive either
phenobarbital
or phenytoin
intravenously
and phenytoin
are equally but
incompletely
effective as
anticonvulsant
s in neonates.
With either
drug given
alone, the
seizures were
controlled in
fewer than half
of the
neonates.
Srinivasaku
mar, P.,
Zempel, J.,
Wallendorf,
M.,
USA To evaluate the
electrographic
seizure burden in
neonates with
hypoxic ischemic
Quantitative
research
Sixty-nine
neonates with
moderate or
severe HIE
were
Therapeutic
hypothermia
was associated
with reduced
electrographic
J., Scher, M.
S., Stein, A.
D., et al.
(1999).
Phenobarbit
al compared
with
phenytoin
for the
treatment of
neonatal
seizures.
The New
England
Journal of
Medicine.
341, 485–
489.
effect of
phenobarbital
and phenytoin
1995, 59
neonates were
studied with
seizures that
were
confirmed by
electroencepha
lography.
were
randomly
assigned to
receive either
phenobarbital
or phenytoin
intravenously
and phenytoin
are equally but
incompletely
effective as
anticonvulsant
s in neonates.
With either
drug given
alone, the
seizures were
controlled in
fewer than half
of the
neonates.
Srinivasaku
mar, P.,
Zempel, J.,
Wallendorf,
M.,
USA To evaluate the
electrographic
seizure burden in
neonates with
hypoxic ischemic
Quantitative
research
Sixty-nine
neonates with
moderate or
severe HIE
were
Therapeutic
hypothermia
was associated
with reduced
electrographic
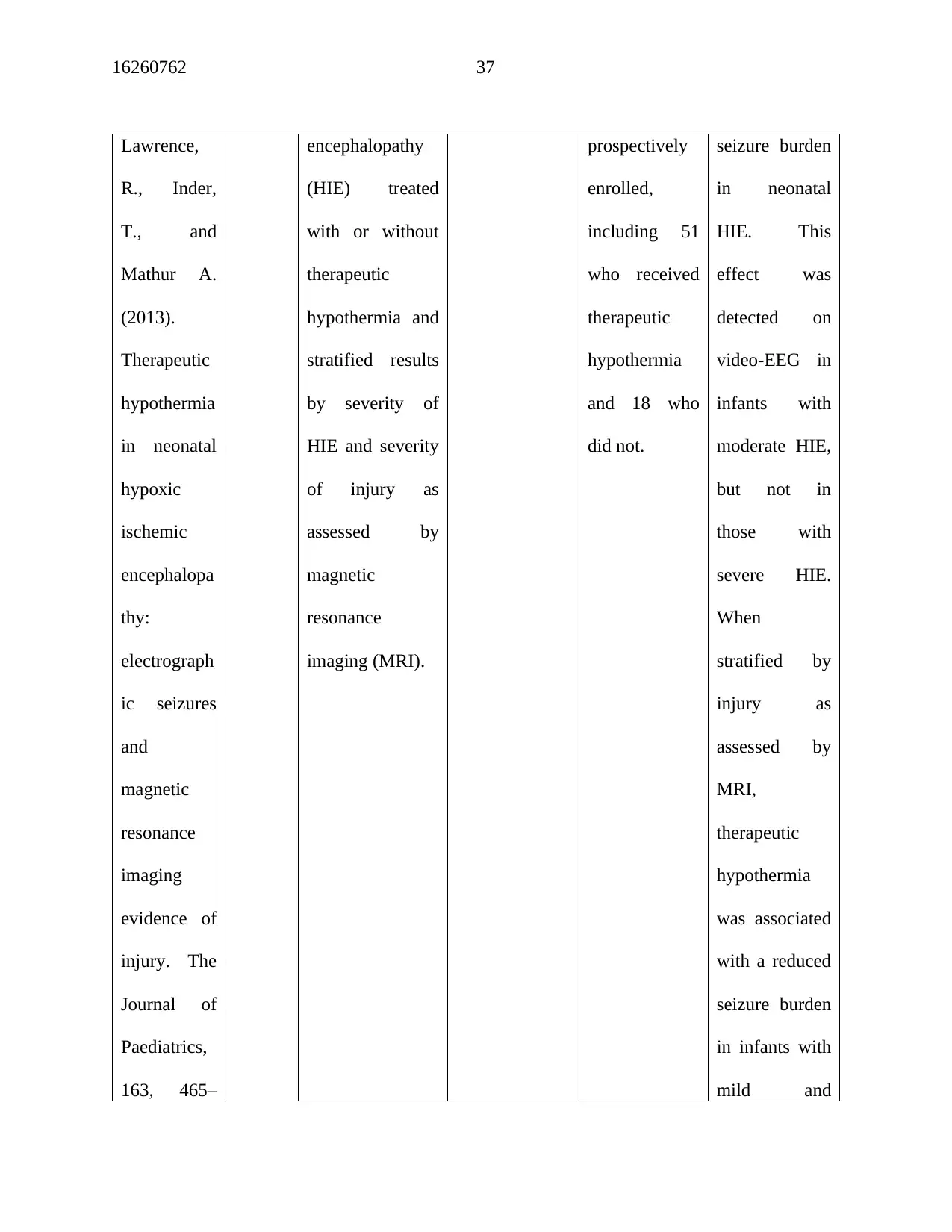
16260762 37
Lawrence,
R., Inder,
T., and
Mathur A.
(2013).
Therapeutic
hypothermia
in neonatal
hypoxic
ischemic
encephalopa
thy:
electrograph
ic seizures
and
magnetic
resonance
imaging
evidence of
injury. The
Journal of
Paediatrics,
163, 465–
encephalopathy
(HIE) treated
with or without
therapeutic
hypothermia and
stratified results
by severity of
HIE and severity
of injury as
assessed by
magnetic
resonance
imaging (MRI).
prospectively
enrolled,
including 51
who received
therapeutic
hypothermia
and 18 who
did not.
seizure burden
in neonatal
HIE. This
effect was
detected on
video-EEG in
infants with
moderate HIE,
but not in
those with
severe HIE.
When
stratified by
injury as
assessed by
MRI,
therapeutic
hypothermia
was associated
with a reduced
seizure burden
in infants with
mild and
Lawrence,
R., Inder,
T., and
Mathur A.
(2013).
Therapeutic
hypothermia
in neonatal
hypoxic
ischemic
encephalopa
thy:
electrograph
ic seizures
and
magnetic
resonance
imaging
evidence of
injury. The
Journal of
Paediatrics,
163, 465–
encephalopathy
(HIE) treated
with or without
therapeutic
hypothermia and
stratified results
by severity of
HIE and severity
of injury as
assessed by
magnetic
resonance
imaging (MRI).
prospectively
enrolled,
including 51
who received
therapeutic
hypothermia
and 18 who
did not.
seizure burden
in neonatal
HIE. This
effect was
detected on
video-EEG in
infants with
moderate HIE,
but not in
those with
severe HIE.
When
stratified by
injury as
assessed by
MRI,
therapeutic
hypothermia
was associated
with a reduced
seizure burden
in infants with
mild and
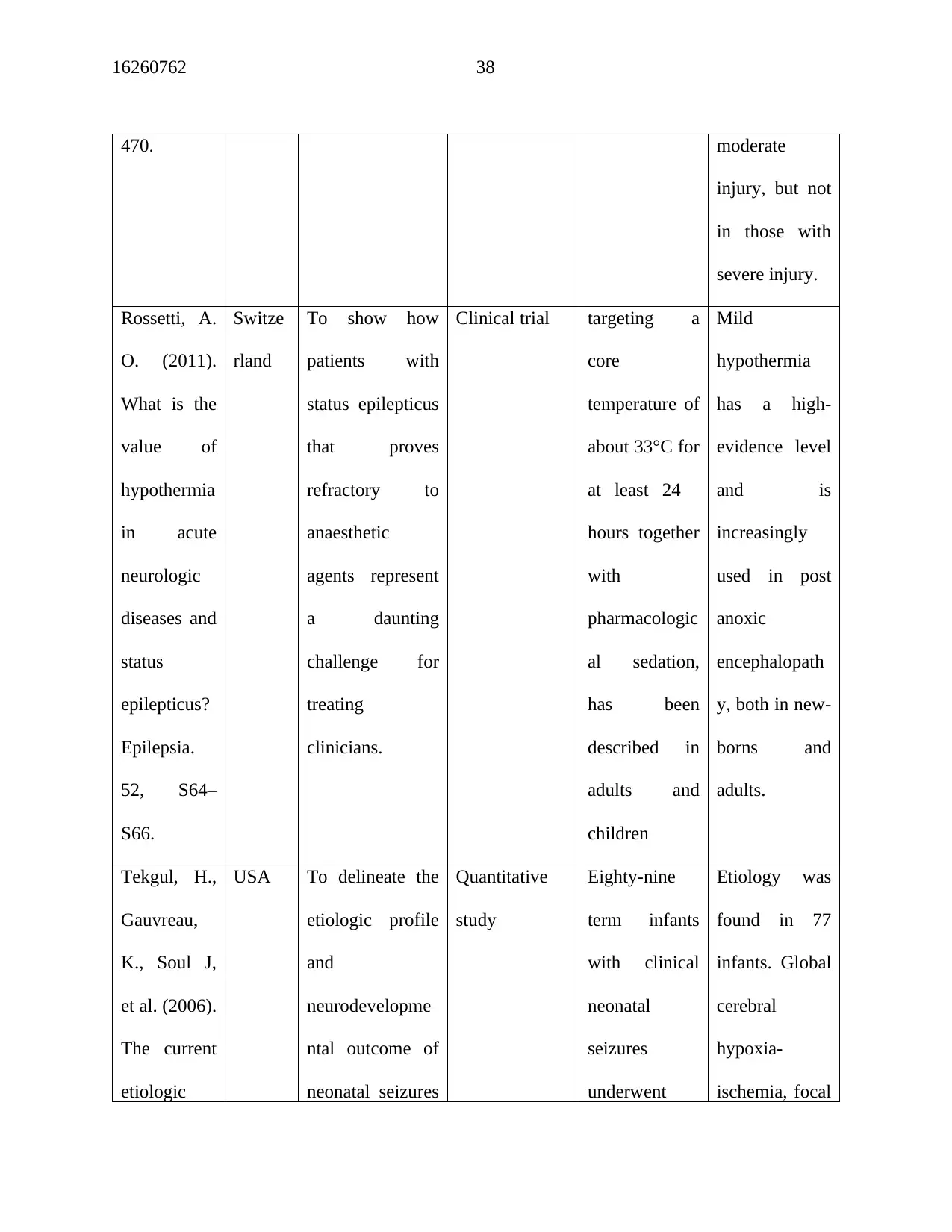
16260762 38
470. moderate
injury, but not
in those with
severe injury.
Rossetti, A.
O. (2011).
What is the
value of
hypothermia
in acute
neurologic
diseases and
status
epilepticus?
Epilepsia.
52, S64–
S66.
Switze
rland
To show how
patients with
status epilepticus
that proves
refractory to
anaesthetic
agents represent
a daunting
challenge for
treating
clinicians.
Clinical trial targeting a
core
temperature of
about 33°C for
at least 24
hours together
with
pharmacologic
al sedation,
has been
described in
adults and
children
Mild
hypothermia
has a high‐
evidence level
and is
increasingly
used in post
anoxic
encephalopath
y, both in new-
borns and
adults.
Tekgul, H.,
Gauvreau,
K., Soul J,
et al. (2006).
The current
etiologic
USA To delineate the
etiologic profile
and
neurodevelopme
ntal outcome of
neonatal seizures
Quantitative
study
Eighty-nine
term infants
with clinical
neonatal
seizures
underwent
Etiology was
found in 77
infants. Global
cerebral
hypoxia-
ischemia, focal
470. moderate
injury, but not
in those with
severe injury.
Rossetti, A.
O. (2011).
What is the
value of
hypothermia
in acute
neurologic
diseases and
status
epilepticus?
Epilepsia.
52, S64–
S66.
Switze
rland
To show how
patients with
status epilepticus
that proves
refractory to
anaesthetic
agents represent
a daunting
challenge for
treating
clinicians.
Clinical trial targeting a
core
temperature of
about 33°C for
at least 24
hours together
with
pharmacologic
al sedation,
has been
described in
adults and
children
Mild
hypothermia
has a high‐
evidence level
and is
increasingly
used in post
anoxic
encephalopath
y, both in new-
borns and
adults.
Tekgul, H.,
Gauvreau,
K., Soul J,
et al. (2006).
The current
etiologic
USA To delineate the
etiologic profile
and
neurodevelopme
ntal outcome of
neonatal seizures
Quantitative
study
Eighty-nine
term infants
with clinical
neonatal
seizures
underwent
Etiology was
found in 77
infants. Global
cerebral
hypoxia-
ischemia, focal
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
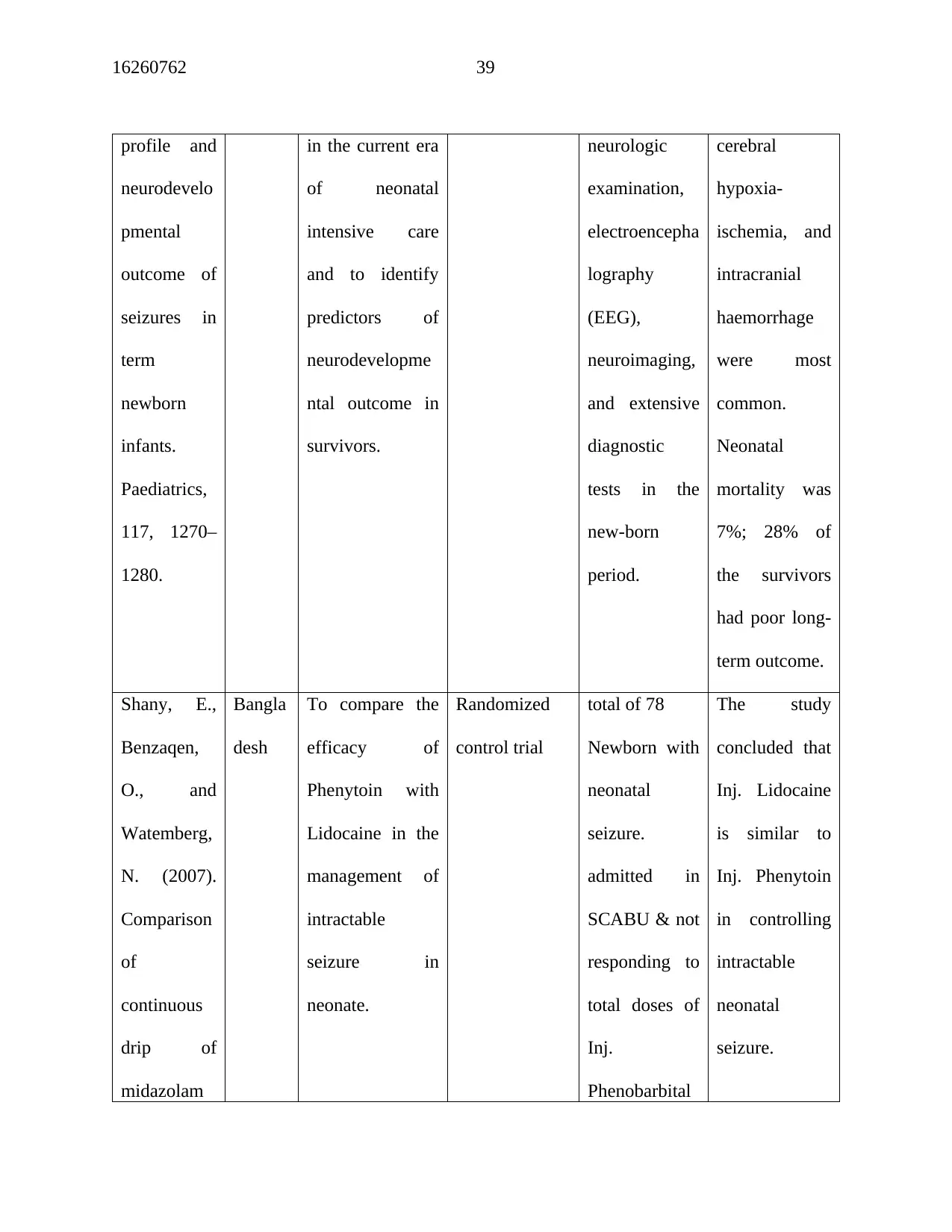
16260762 39
profile and
neurodevelo
pmental
outcome of
seizures in
term
newborn
infants.
Paediatrics,
117, 1270–
1280.
in the current era
of neonatal
intensive care
and to identify
predictors of
neurodevelopme
ntal outcome in
survivors.
neurologic
examination,
electroencepha
lography
(EEG),
neuroimaging,
and extensive
diagnostic
tests in the
new-born
period.
cerebral
hypoxia-
ischemia, and
intracranial
haemorrhage
were most
common.
Neonatal
mortality was
7%; 28% of
the survivors
had poor long-
term outcome.
Shany, E.,
Benzaqen,
O., and
Watemberg,
N. (2007).
Comparison
of
continuous
drip of
midazolam
Bangla
desh
To compare the
efficacy of
Phenytoin with
Lidocaine in the
management of
intractable
seizure in
neonate.
Randomized
control trial
total of 78
Newborn with
neonatal
seizure.
admitted in
SCABU & not
responding to
total doses of
Inj.
Phenobarbital
The study
concluded that
Inj. Lidocaine
is similar to
Inj. Phenytoin
in controlling
intractable
neonatal
seizure.
profile and
neurodevelo
pmental
outcome of
seizures in
term
newborn
infants.
Paediatrics,
117, 1270–
1280.
in the current era
of neonatal
intensive care
and to identify
predictors of
neurodevelopme
ntal outcome in
survivors.
neurologic
examination,
electroencepha
lography
(EEG),
neuroimaging,
and extensive
diagnostic
tests in the
new-born
period.
cerebral
hypoxia-
ischemia, and
intracranial
haemorrhage
were most
common.
Neonatal
mortality was
7%; 28% of
the survivors
had poor long-
term outcome.
Shany, E.,
Benzaqen,
O., and
Watemberg,
N. (2007).
Comparison
of
continuous
drip of
midazolam
Bangla
desh
To compare the
efficacy of
Phenytoin with
Lidocaine in the
management of
intractable
seizure in
neonate.
Randomized
control trial
total of 78
Newborn with
neonatal
seizure.
admitted in
SCABU & not
responding to
total doses of
Inj.
Phenobarbital
The study
concluded that
Inj. Lidocaine
is similar to
Inj. Phenytoin
in controlling
intractable
neonatal
seizure.
16260762 40
or lidocaine
in the
treatment of
intractable
neonatal
seizures.
Journal of
Child
Neurology,
22, 255–
259.
(40 mg/kg)
were included
or lidocaine
in the
treatment of
intractable
neonatal
seizures.
Journal of
Child
Neurology,
22, 255–
259.
(40 mg/kg)
were included
1 out of 39

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.