Femoral Shaft Fracture Treatment & Complications
VerifiedAdded on 2020/02/23
|11
|3140
|52
AI Summary
This assignment delves into the complexities of treating femoral shaft fractures. It examines various surgical and non-surgical approaches, including intramedullary nailing, external fixation, and their impact on fracture healing. Additionally, it discusses potential complications such as compartment syndrome, heterotopic ossification, and pudendal neuralgia, highlighting their significance in patient care.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: INTEGRATED NURSING PRACTICE
Integrated nursing practice
Name of the Student
Name of the University
Author note
Integrated nursing practice
Name of the Student
Name of the University
Author note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1INTEGRATED NURSING PRACTICE
Surgical treatment options
The surgery for mid-shaft fractured femur depends on time. Mid-shaft femur fractures are
treated depending upon pattern of fracture. Femoral neck fractures, percutaneous pinning or
sliding of hip screw and anthroplasty is done for the elderly patients like in the given case study
of Mr.Brown. If the skin around the fracture is still not broken, then it is advisable to wait to
make it stable before surgery. If the fracture is open, it might be exposed to environment and so
need to be cleaned urgently to prevent infection before immediate surgery. The leg is placed in
skeletal fraction or long-leg splint between the period of initial emergency care and surgery. This
helps to keep the broken bones aligned and maintain length of leg. There are three surgical
treatment options available for the mid-shaft fractured femur.
External fixation is a type of operation where screws or metal pins are placed in bones
above and below the site of fracture. The screws and pins are attached to bar outside skin that act
as stabilizing frame for the holding bones in proper position for fast healing. It is a temporary
treatment where external fixators are applied which provide temporary and good stability until
the femur is healed (Kulshrestha, Roy, & Audige, 2011).
Intramedullary nailing is another surgical option where and currently in use for the mid-
shaft femoral fractures opted commonly by most surgeons. In this procedure, a specially
designed metal rod is inserted in femur marrow canal. The rod then passes across fracture that
helps to it in position. The intramedullary nail is inserted in the canal at the knee or hip in small
incision. There is crewing at the bones at both ends. This keeps the bone and nail in proper
position at the time of healing (Gelalis, et al., 2012).
Surgical treatment options
The surgery for mid-shaft fractured femur depends on time. Mid-shaft femur fractures are
treated depending upon pattern of fracture. Femoral neck fractures, percutaneous pinning or
sliding of hip screw and anthroplasty is done for the elderly patients like in the given case study
of Mr.Brown. If the skin around the fracture is still not broken, then it is advisable to wait to
make it stable before surgery. If the fracture is open, it might be exposed to environment and so
need to be cleaned urgently to prevent infection before immediate surgery. The leg is placed in
skeletal fraction or long-leg splint between the period of initial emergency care and surgery. This
helps to keep the broken bones aligned and maintain length of leg. There are three surgical
treatment options available for the mid-shaft fractured femur.
External fixation is a type of operation where screws or metal pins are placed in bones
above and below the site of fracture. The screws and pins are attached to bar outside skin that act
as stabilizing frame for the holding bones in proper position for fast healing. It is a temporary
treatment where external fixators are applied which provide temporary and good stability until
the femur is healed (Kulshrestha, Roy, & Audige, 2011).
Intramedullary nailing is another surgical option where and currently in use for the mid-
shaft femoral fractures opted commonly by most surgeons. In this procedure, a specially
designed metal rod is inserted in femur marrow canal. The rod then passes across fracture that
helps to it in position. The intramedullary nail is inserted in the canal at the knee or hip in small
incision. There is crewing at the bones at both ends. This keeps the bone and nail in proper
position at the time of healing (Gelalis, et al., 2012).
2INTEGRATED NURSING PRACTICE
Screws and plates are also done as a surgical operation when the bone segments are
reduced or first repositioned in their normal alignment. Metal plates and special screws are
attached to the bone outer surface. These screws and plates are often used during intramedulalry
nailing which is not possible for the fractures that are extended to knee or hip joints (Smith,
Parvizi, & Purtill, 2011).
Complications
Patients who sustain mid-line femur fracture after a traumatic accident like tractor
accident of Mr. Brown, encounter complications depending upon the severity of break or fracture
location. The complications include infection, bone healing problems, nerve damage,
compartment syndrome or surgical complications (Kong & Sabharwal, 2014). In fractured
femur, there can be bone breaking the skin and that increases the risk for infection. If there is
wrong alignment of bones or infection that causes irritation, the healing process is delayed and
there is requirement of further surgery. Nerve damage can also occur where there might be
weakness or numbness that is a rare complication. Compartment syndrome is also a rare
complication of femoral mid-shaft fractures where there is compression of blood vessels, nerves,
muscles inside compartment or closed space within the body. This generally occurs within the
thigh with bleeding or inflammation because of trauma that is associated with the fracture. In
case of this syndrome, immediate operation is required. Surgical complications can also occur
due to hardware failure that is required to stabilize bone or hardware piece that causes pain or
irritation. Nerve damage is the possible surgical complication in mid-shaft femoral fracture
(Park, Noh, & Kam, 2013).
Screws and plates are also done as a surgical operation when the bone segments are
reduced or first repositioned in their normal alignment. Metal plates and special screws are
attached to the bone outer surface. These screws and plates are often used during intramedulalry
nailing which is not possible for the fractures that are extended to knee or hip joints (Smith,
Parvizi, & Purtill, 2011).
Complications
Patients who sustain mid-line femur fracture after a traumatic accident like tractor
accident of Mr. Brown, encounter complications depending upon the severity of break or fracture
location. The complications include infection, bone healing problems, nerve damage,
compartment syndrome or surgical complications (Kong & Sabharwal, 2014). In fractured
femur, there can be bone breaking the skin and that increases the risk for infection. If there is
wrong alignment of bones or infection that causes irritation, the healing process is delayed and
there is requirement of further surgery. Nerve damage can also occur where there might be
weakness or numbness that is a rare complication. Compartment syndrome is also a rare
complication of femoral mid-shaft fractures where there is compression of blood vessels, nerves,
muscles inside compartment or closed space within the body. This generally occurs within the
thigh with bleeding or inflammation because of trauma that is associated with the fracture. In
case of this syndrome, immediate operation is required. Surgical complications can also occur
due to hardware failure that is required to stabilize bone or hardware piece that causes pain or
irritation. Nerve damage is the possible surgical complication in mid-shaft femoral fracture
(Park, Noh, & Kam, 2013).
3INTEGRATED NURSING PRACTICE
Major complications, nursing interventions and monitoring
Depending on the femoral fracture, the major complications in mid shaft femoral fracture
affects the knee, however, in a different way. Femur movement when it breaks, there is ligament
damage in knee that demand immediate operation for repairing the damage. Heterotopic
ossification, pudendal nerve injury and Acute compartment syndrome are major complications
that might occur post-operation of fractured femur (Kaiser, et al., 2011).
Heterotopic ossification occurs with an incidence of 25% as a post-operative
complication after femur fracture surgery. In this, there is varying severity where bone debris
from endosteal canal reaming is deposited in soft tissues that surround the site of nail insertion in
Intramedullary nailing surgery (Botolin, Mauffrey, Hammerberg, Hak, & Stahel, 2013). These
debris are stimulate the heterotopic bone formation that decreases debris amount left in tissues
after the nailing leading to heterotopic ossification. This complication occurs at the proximal end
of reamed intramedullary femoral nail posing a complication after the procedure. The nursing
intervention is the physical therapy where the nurse keeps the patient with involved joint at rest
to maintain a functional position and perform Passive Range of Motion (PROM) where the body
parts are moved within the available range without muscle activation (Martinez de Albornoz,
Khanna, Longo, Forriol, & Maffulli, 2011). It is monitored by keeping into account the
movement range of the patient and pain management.
Pudendal nerve injury is another main complication that is associated with the fracture
surgery where there is static interlocking in the femur nailing. This neurologic injury is a
combination of direct compression and localized ischaemia of perineum against post fracture
countertraction. In this, there is branching of sensory terminals of pudendal nerve that appear
Major complications, nursing interventions and monitoring
Depending on the femoral fracture, the major complications in mid shaft femoral fracture
affects the knee, however, in a different way. Femur movement when it breaks, there is ligament
damage in knee that demand immediate operation for repairing the damage. Heterotopic
ossification, pudendal nerve injury and Acute compartment syndrome are major complications
that might occur post-operation of fractured femur (Kaiser, et al., 2011).
Heterotopic ossification occurs with an incidence of 25% as a post-operative
complication after femur fracture surgery. In this, there is varying severity where bone debris
from endosteal canal reaming is deposited in soft tissues that surround the site of nail insertion in
Intramedullary nailing surgery (Botolin, Mauffrey, Hammerberg, Hak, & Stahel, 2013). These
debris are stimulate the heterotopic bone formation that decreases debris amount left in tissues
after the nailing leading to heterotopic ossification. This complication occurs at the proximal end
of reamed intramedullary femoral nail posing a complication after the procedure. The nursing
intervention is the physical therapy where the nurse keeps the patient with involved joint at rest
to maintain a functional position and perform Passive Range of Motion (PROM) where the body
parts are moved within the available range without muscle activation (Martinez de Albornoz,
Khanna, Longo, Forriol, & Maffulli, 2011). It is monitored by keeping into account the
movement range of the patient and pain management.
Pudendal nerve injury is another main complication that is associated with the fracture
surgery where there is static interlocking in the femur nailing. This neurologic injury is a
combination of direct compression and localized ischaemia of perineum against post fracture
countertraction. In this, there is branching of sensory terminals of pudendal nerve that appear
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4INTEGRATED NURSING PRACTICE
susceptible to injury causing complications after the surgery. It is an important and common
complication after intramedullary femur nailing that might result in complete sensory loss. The
nursing intervention involves pain management and medical interventions. Nurses would reduce
the pudendal nerve irritability through lifestyle changes. They would perform sitting
modification, avoidance of physical activities that irritate nerves, bladder and bowel
management help to prevent straining of nerves and its compression that might cause nerve
irritation. Continuous monitoring and refereeing to a physiotherapist would help to relax the
muscles and decrease nerve irritation. Acupunture and psychotherapy can also be helpful for
reducing pain and irritation of nerve (Fisher & Lotze, 2011).
Acute compartment syndrome is a rare but important complication that takes place post
femur fracture. It is a highly painful condition when the muscle pressure builds to alarming
levels. This can decrease flow of blood preventing oxygen and nourishment from reaching
muscle and nerve cells. The pressure need to be released or else can cause permanent disability.
This requires surgery when the surgeon makes incisions in the muscle coverings and skin to
relieve pressure (Kalyani, Fisher, Roberts, & Giannoudis, 2011). The nursing intervention
involves pain management by medications like epidural analgesia to relieve pain. Multimodal
approach that includes use of non-steroidal anti-inflammatory drug (NSAID) and paracetamol
along with an opioid considered best after pressure release through surgery. Patient education is
also required before discharge after pressure release surgery by nurses for predisposition to this
syndrome. The monitoring involves evaluation of any medication side effects and compartment
pressure that should be less than 15mmHg via single pressure readings or continuous pressure
monitoring.
susceptible to injury causing complications after the surgery. It is an important and common
complication after intramedullary femur nailing that might result in complete sensory loss. The
nursing intervention involves pain management and medical interventions. Nurses would reduce
the pudendal nerve irritability through lifestyle changes. They would perform sitting
modification, avoidance of physical activities that irritate nerves, bladder and bowel
management help to prevent straining of nerves and its compression that might cause nerve
irritation. Continuous monitoring and refereeing to a physiotherapist would help to relax the
muscles and decrease nerve irritation. Acupunture and psychotherapy can also be helpful for
reducing pain and irritation of nerve (Fisher & Lotze, 2011).
Acute compartment syndrome is a rare but important complication that takes place post
femur fracture. It is a highly painful condition when the muscle pressure builds to alarming
levels. This can decrease flow of blood preventing oxygen and nourishment from reaching
muscle and nerve cells. The pressure need to be released or else can cause permanent disability.
This requires surgery when the surgeon makes incisions in the muscle coverings and skin to
relieve pressure (Kalyani, Fisher, Roberts, & Giannoudis, 2011). The nursing intervention
involves pain management by medications like epidural analgesia to relieve pain. Multimodal
approach that includes use of non-steroidal anti-inflammatory drug (NSAID) and paracetamol
along with an opioid considered best after pressure release through surgery. Patient education is
also required before discharge after pressure release surgery by nurses for predisposition to this
syndrome. The monitoring involves evaluation of any medication side effects and compartment
pressure that should be less than 15mmHg via single pressure readings or continuous pressure
monitoring.
5INTEGRATED NURSING PRACTICE
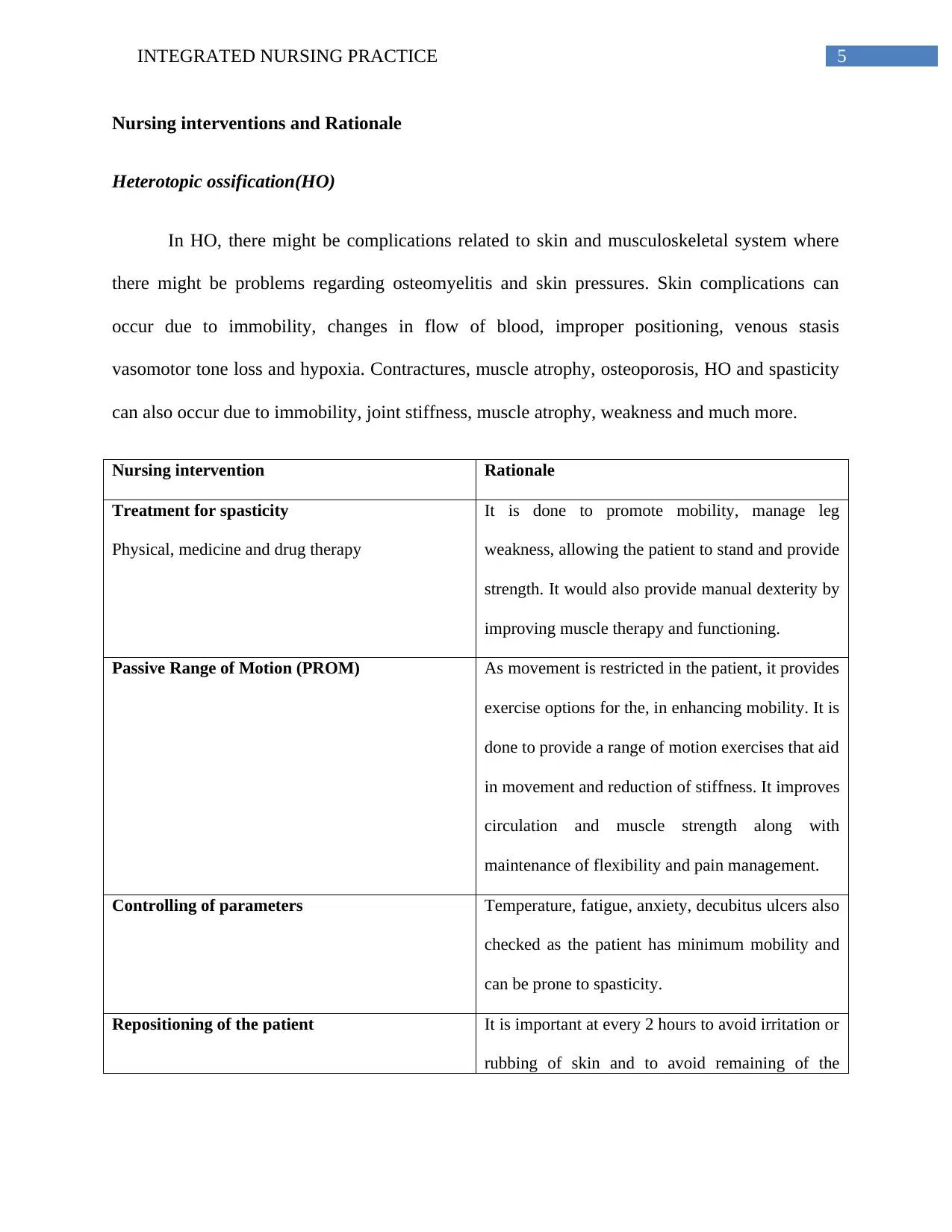
Nursing interventions and Rationale
Heterotopic ossification(HO)
In HO, there might be complications related to skin and musculoskeletal system where
there might be problems regarding osteomyelitis and skin pressures. Skin complications can
occur due to immobility, changes in flow of blood, improper positioning, venous stasis
vasomotor tone loss and hypoxia. Contractures, muscle atrophy, osteoporosis, HO and spasticity
can also occur due to immobility, joint stiffness, muscle atrophy, weakness and much more.
Nursing intervention Rationale
Treatment for spasticity
Physical, medicine and drug therapy
It is done to promote mobility, manage leg
weakness, allowing the patient to stand and provide
strength. It would also provide manual dexterity by
improving muscle therapy and functioning.
Passive Range of Motion (PROM) As movement is restricted in the patient, it provides
exercise options for the, in enhancing mobility. It is
done to provide a range of motion exercises that aid
in movement and reduction of stiffness. It improves
circulation and muscle strength along with
maintenance of flexibility and pain management.
Controlling of parameters Temperature, fatigue, anxiety, decubitus ulcers also
checked as the patient has minimum mobility and
can be prone to spasticity.
Repositioning of the patient It is important at every 2 hours to avoid irritation or
rubbing of skin and to avoid remaining of the
Nursing interventions and Rationale
Heterotopic ossification(HO)
In HO, there might be complications related to skin and musculoskeletal system where
there might be problems regarding osteomyelitis and skin pressures. Skin complications can
occur due to immobility, changes in flow of blood, improper positioning, venous stasis
vasomotor tone loss and hypoxia. Contractures, muscle atrophy, osteoporosis, HO and spasticity
can also occur due to immobility, joint stiffness, muscle atrophy, weakness and much more.
Nursing intervention Rationale
Treatment for spasticity
Physical, medicine and drug therapy
It is done to promote mobility, manage leg
weakness, allowing the patient to stand and provide
strength. It would also provide manual dexterity by
improving muscle therapy and functioning.
Passive Range of Motion (PROM) As movement is restricted in the patient, it provides
exercise options for the, in enhancing mobility. It is
done to provide a range of motion exercises that aid
in movement and reduction of stiffness. It improves
circulation and muscle strength along with
maintenance of flexibility and pain management.
Controlling of parameters Temperature, fatigue, anxiety, decubitus ulcers also
checked as the patient has minimum mobility and
can be prone to spasticity.
Repositioning of the patient It is important at every 2 hours to avoid irritation or
rubbing of skin and to avoid remaining of the
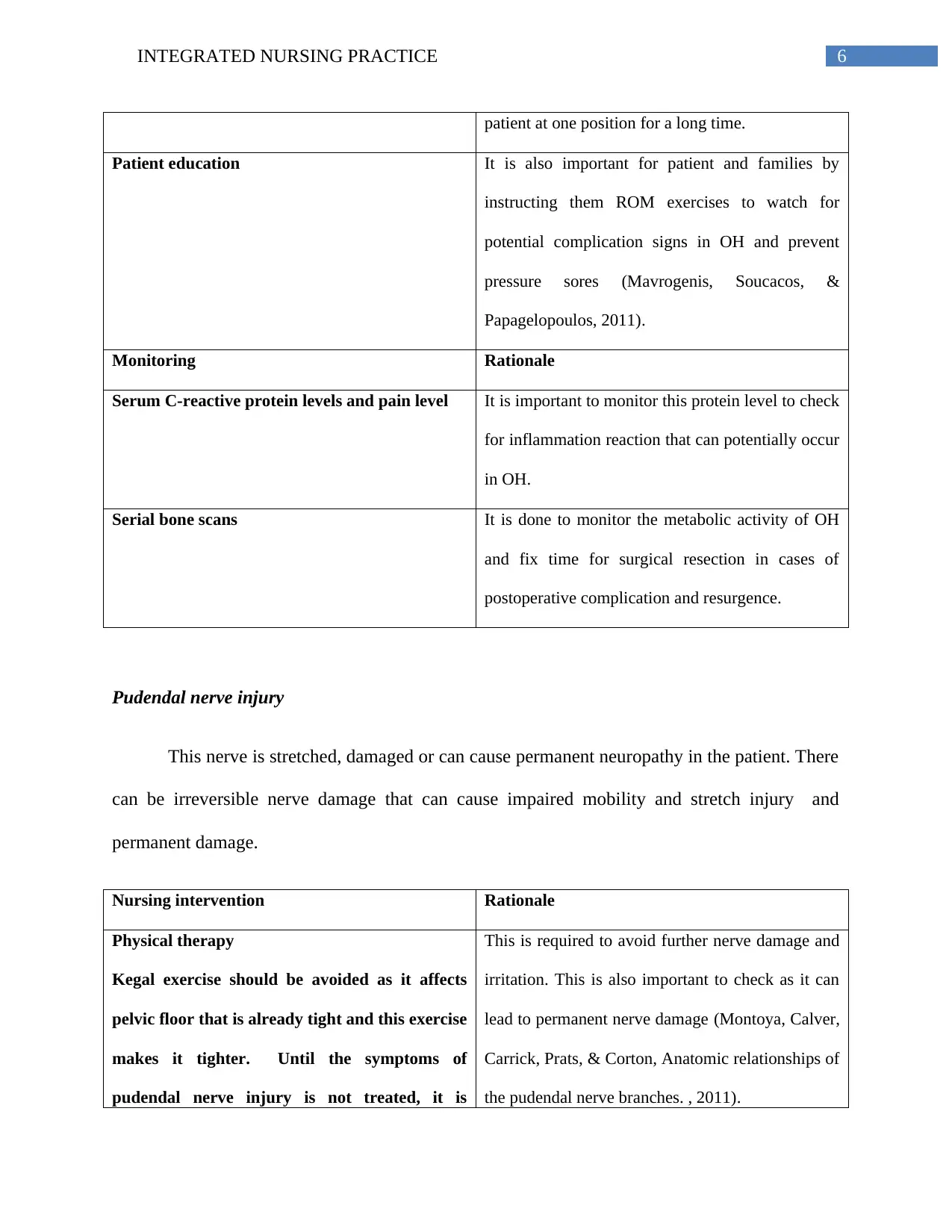
6INTEGRATED NURSING PRACTICE
patient at one position for a long time.
Patient education It is also important for patient and families by
instructing them ROM exercises to watch for
potential complication signs in OH and prevent
pressure sores (Mavrogenis, Soucacos, &
Papagelopoulos, 2011).
Monitoring Rationale
Serum C-reactive protein levels and pain level It is important to monitor this protein level to check
for inflammation reaction that can potentially occur
in OH.
Serial bone scans It is done to monitor the metabolic activity of OH
and fix time for surgical resection in cases of
postoperative complication and resurgence.
Pudendal nerve injury
This nerve is stretched, damaged or can cause permanent neuropathy in the patient. There
can be irreversible nerve damage that can cause impaired mobility and stretch injury and
permanent damage.
Nursing intervention Rationale
Physical therapy
Kegal exercise should be avoided as it affects
pelvic floor that is already tight and this exercise
makes it tighter. Until the symptoms of
pudendal nerve injury is not treated, it is
This is required to avoid further nerve damage and
irritation. This is also important to check as it can
lead to permanent nerve damage (Montoya, Calver,
Carrick, Prats, & Corton, Anatomic relationships of
the pudendal nerve branches. , 2011).
patient at one position for a long time.
Patient education It is also important for patient and families by
instructing them ROM exercises to watch for
potential complication signs in OH and prevent
pressure sores (Mavrogenis, Soucacos, &
Papagelopoulos, 2011).
Monitoring Rationale
Serum C-reactive protein levels and pain level It is important to monitor this protein level to check
for inflammation reaction that can potentially occur
in OH.
Serial bone scans It is done to monitor the metabolic activity of OH
and fix time for surgical resection in cases of
postoperative complication and resurgence.
Pudendal nerve injury
This nerve is stretched, damaged or can cause permanent neuropathy in the patient. There
can be irreversible nerve damage that can cause impaired mobility and stretch injury and
permanent damage.
Nursing intervention Rationale
Physical therapy
Kegal exercise should be avoided as it affects
pelvic floor that is already tight and this exercise
makes it tighter. Until the symptoms of
pudendal nerve injury is not treated, it is
This is required to avoid further nerve damage and
irritation. This is also important to check as it can
lead to permanent nerve damage (Montoya, Calver,
Carrick, Prats, & Corton, Anatomic relationships of
the pudendal nerve branches. , 2011).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
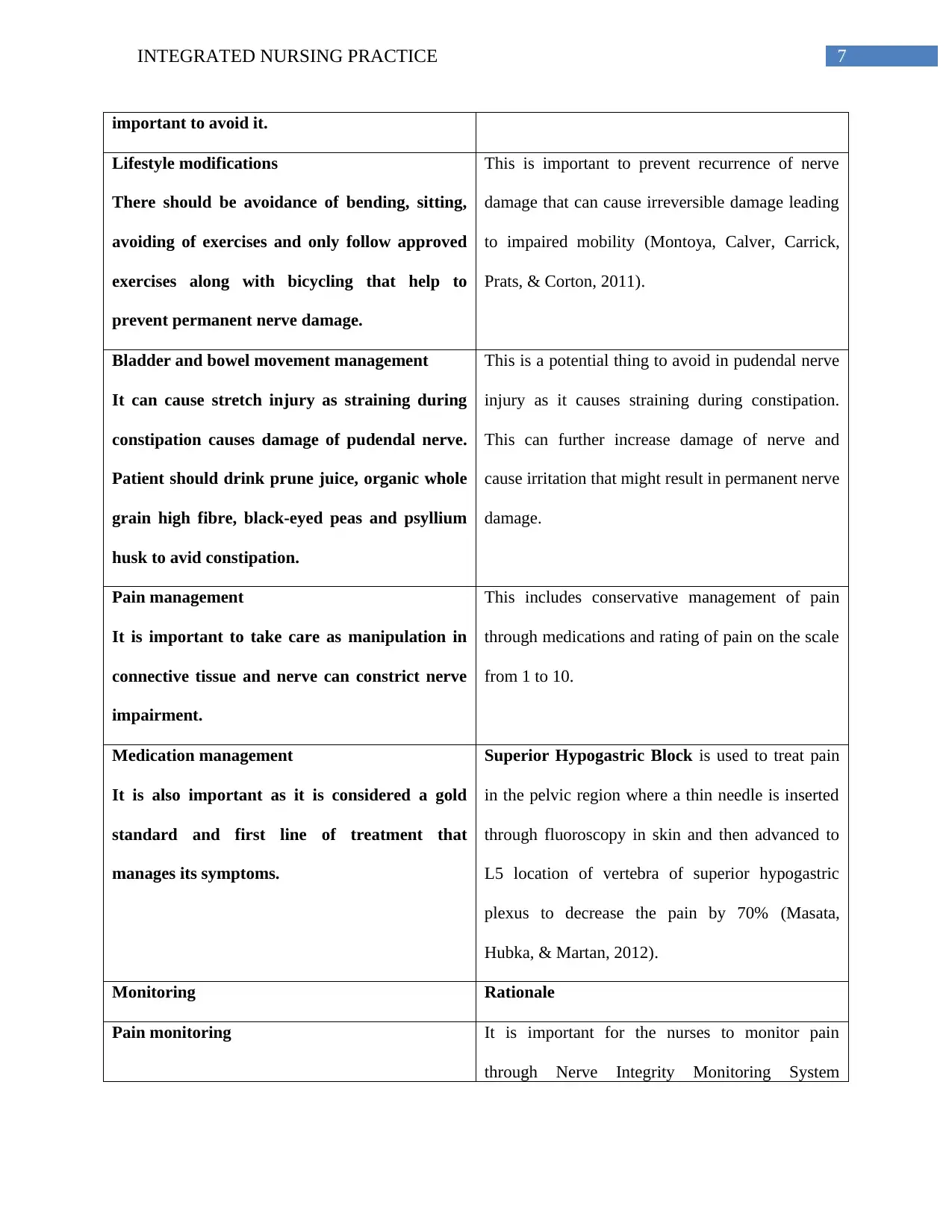
7INTEGRATED NURSING PRACTICE
important to avoid it.
Lifestyle modifications
There should be avoidance of bending, sitting,
avoiding of exercises and only follow approved
exercises along with bicycling that help to
prevent permanent nerve damage.
This is important to prevent recurrence of nerve
damage that can cause irreversible damage leading
to impaired mobility (Montoya, Calver, Carrick,
Prats, & Corton, 2011).
Bladder and bowel movement management
It can cause stretch injury as straining during
constipation causes damage of pudendal nerve.
Patient should drink prune juice, organic whole
grain high fibre, black-eyed peas and psyllium
husk to avid constipation.
This is a potential thing to avoid in pudendal nerve
injury as it causes straining during constipation.
This can further increase damage of nerve and
cause irritation that might result in permanent nerve
damage.
Pain management
It is important to take care as manipulation in
connective tissue and nerve can constrict nerve
impairment.
This includes conservative management of pain
through medications and rating of pain on the scale
from 1 to 10.
Medication management
It is also important as it is considered a gold
standard and first line of treatment that
manages its symptoms.
Superior Hypogastric Block is used to treat pain
in the pelvic region where a thin needle is inserted
through fluoroscopy in skin and then advanced to
L5 location of vertebra of superior hypogastric
plexus to decrease the pain by 70% (Masata,
Hubka, & Martan, 2012).
Monitoring Rationale
Pain monitoring It is important for the nurses to monitor pain
through Nerve Integrity Monitoring System
important to avoid it.
Lifestyle modifications
There should be avoidance of bending, sitting,
avoiding of exercises and only follow approved
exercises along with bicycling that help to
prevent permanent nerve damage.
This is important to prevent recurrence of nerve
damage that can cause irreversible damage leading
to impaired mobility (Montoya, Calver, Carrick,
Prats, & Corton, 2011).
Bladder and bowel movement management
It can cause stretch injury as straining during
constipation causes damage of pudendal nerve.
Patient should drink prune juice, organic whole
grain high fibre, black-eyed peas and psyllium
husk to avid constipation.
This is a potential thing to avoid in pudendal nerve
injury as it causes straining during constipation.
This can further increase damage of nerve and
cause irritation that might result in permanent nerve
damage.
Pain management
It is important to take care as manipulation in
connective tissue and nerve can constrict nerve
impairment.
This includes conservative management of pain
through medications and rating of pain on the scale
from 1 to 10.
Medication management
It is also important as it is considered a gold
standard and first line of treatment that
manages its symptoms.
Superior Hypogastric Block is used to treat pain
in the pelvic region where a thin needle is inserted
through fluoroscopy in skin and then advanced to
L5 location of vertebra of superior hypogastric
plexus to decrease the pain by 70% (Masata,
Hubka, & Martan, 2012).
Monitoring Rationale
Pain monitoring It is important for the nurses to monitor pain
through Nerve Integrity Monitoring System
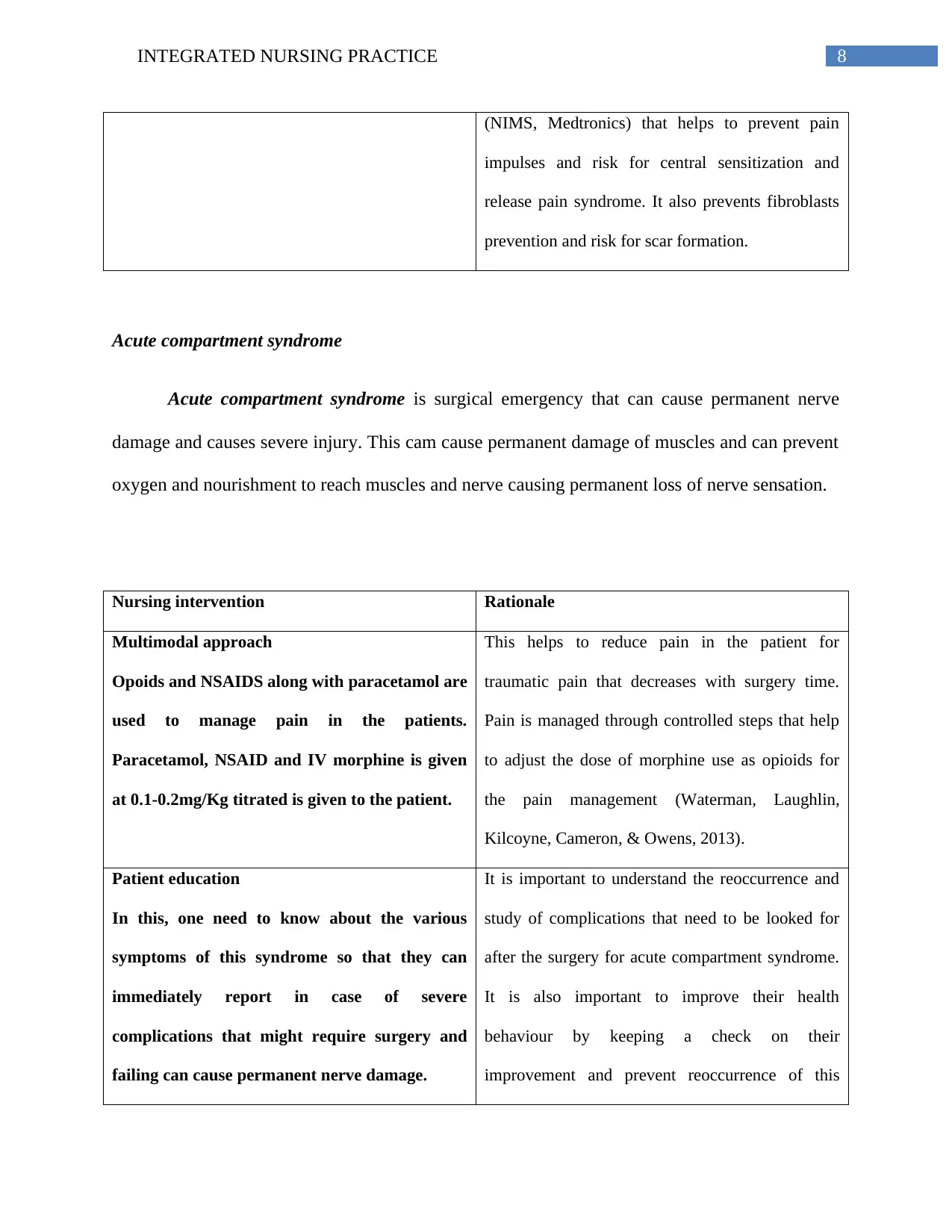
8INTEGRATED NURSING PRACTICE
(NIMS, Medtronics) that helps to prevent pain
impulses and risk for central sensitization and
release pain syndrome. It also prevents fibroblasts
prevention and risk for scar formation.
Acute compartment syndrome
Acute compartment syndrome is surgical emergency that can cause permanent nerve
damage and causes severe injury. This cam cause permanent damage of muscles and can prevent
oxygen and nourishment to reach muscles and nerve causing permanent loss of nerve sensation.
Nursing intervention Rationale
Multimodal approach
Opoids and NSAIDS along with paracetamol are
used to manage pain in the patients.
Paracetamol, NSAID and IV morphine is given
at 0.1-0.2mg/Kg titrated is given to the patient.
This helps to reduce pain in the patient for
traumatic pain that decreases with surgery time.
Pain is managed through controlled steps that help
to adjust the dose of morphine use as opioids for
the pain management (Waterman, Laughlin,
Kilcoyne, Cameron, & Owens, 2013).
Patient education
In this, one need to know about the various
symptoms of this syndrome so that they can
immediately report in case of severe
complications that might require surgery and
failing can cause permanent nerve damage.
It is important to understand the reoccurrence and
study of complications that need to be looked for
after the surgery for acute compartment syndrome.
It is also important to improve their health
behaviour by keeping a check on their
improvement and prevent reoccurrence of this
(NIMS, Medtronics) that helps to prevent pain
impulses and risk for central sensitization and
release pain syndrome. It also prevents fibroblasts
prevention and risk for scar formation.
Acute compartment syndrome
Acute compartment syndrome is surgical emergency that can cause permanent nerve
damage and causes severe injury. This cam cause permanent damage of muscles and can prevent
oxygen and nourishment to reach muscles and nerve causing permanent loss of nerve sensation.
Nursing intervention Rationale
Multimodal approach
Opoids and NSAIDS along with paracetamol are
used to manage pain in the patients.
Paracetamol, NSAID and IV morphine is given
at 0.1-0.2mg/Kg titrated is given to the patient.
This helps to reduce pain in the patient for
traumatic pain that decreases with surgery time.
Pain is managed through controlled steps that help
to adjust the dose of morphine use as opioids for
the pain management (Waterman, Laughlin,
Kilcoyne, Cameron, & Owens, 2013).
Patient education
In this, one need to know about the various
symptoms of this syndrome so that they can
immediately report in case of severe
complications that might require surgery and
failing can cause permanent nerve damage.
It is important to understand the reoccurrence and
study of complications that need to be looked for
after the surgery for acute compartment syndrome.
It is also important to improve their health
behaviour by keeping a check on their
improvement and prevent reoccurrence of this
9INTEGRATED NURSING PRACTICE
complication.
Monitoring Rationale
Side effects of medication
This multimodal approach causes many
potential side effects that can affect the patient
and adverse the complicated situation. Side
effects are renal toxicity, gastric ulceration,
platelet aggregation inhibition that can cause
hemorrhagic complications. This can aggravate
the complication of acute compartment
syndrome.
Nurses have to monitor the potential side effects of
multimodal approach to avoid high risk for further
trauma injuries, increased risk for potential side
effects of medication therapy that might affect the
patient and deteriorate the condition.
Pressure monitoring
It is an invasive procedure that has an huge
impact on the patient having acute compartment
syndrome following fracture surgery. The
pressure should be below 15 mmHg to avoid
complications. It is done through single pressure
readings, fibreoptic transducer (camino-
catheter) which is simple and reliable.
Nurses have to keep monitoring the compartment
pressure as it can cause complications like
inflammation, swelling, and blood supply loss in
muscles, muscle scarring, loss of function and
contracture. Therefore, it is important to monitor
the pressure levels.
complication.
Monitoring Rationale
Side effects of medication
This multimodal approach causes many
potential side effects that can affect the patient
and adverse the complicated situation. Side
effects are renal toxicity, gastric ulceration,
platelet aggregation inhibition that can cause
hemorrhagic complications. This can aggravate
the complication of acute compartment
syndrome.
Nurses have to monitor the potential side effects of
multimodal approach to avoid high risk for further
trauma injuries, increased risk for potential side
effects of medication therapy that might affect the
patient and deteriorate the condition.
Pressure monitoring
It is an invasive procedure that has an huge
impact on the patient having acute compartment
syndrome following fracture surgery. The
pressure should be below 15 mmHg to avoid
complications. It is done through single pressure
readings, fibreoptic transducer (camino-
catheter) which is simple and reliable.
Nurses have to keep monitoring the compartment
pressure as it can cause complications like
inflammation, swelling, and blood supply loss in
muscles, muscle scarring, loss of function and
contracture. Therefore, it is important to monitor
the pressure levels.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10INTEGRATED NURSING PRACTICE
Bibliography
Aubut, J. A., Mehta, S., Cullen, N., Teasell, R. W., & Team, G. t. (2011). A comparison of
heterotopic ossification treatment within the traumatic brain and spinal cord injured
population: an evidence based systematic review. NeuroRehabilitation, 151-160.
Botolin, S., Mauffrey, C., Hammerberg, E. M., Hak, D. J., & Stahel, P. F. (2013). Heterotopic
ossification in the reaming tract of a percutaneous antegrade femoral nail: a case report.
Journal of medical case reports, 90.
Fisher, H. W., & Lotze, P. M. (2011). Nerve injury locations during retropubic sling
procedures. . International urogynecology journal, 439-441.
Gelalis, I. D., Politis, A. N., Arnaoutoglou, C. M., Korompilias, A. V., E., P. E., Vekris, M. D.,
& ... & Xenakis, T. A. (2012). Diagnostic and treatment modalities in nonunions of the
femoral shaft. A review. Injury, 980-988.
Kaiser, M. M., Wessel, L. M., Zachert, G., Stratmann, C., Eggert, R., Gros, N., & ... & Rapp, M.
(2011). Biomechanical analysis of a synthetic femur spiral fracture model: influence of
different materials on the stiffness in flexible intramedullary nailing. . Clinical
Biomechanics, 592-597.
Kalyani, B. S., Fisher, B. E., Roberts, C. S., & Giannoudis, P. V. (2011). Compartment
syndrome of the forearm: a systematic review. The Journal of hand surgery, 535-543.
Kong, H., & Sabharwal, S. (2014). External fixation for closed pediatric femoral shaft fractures:
where are we now?. Clinical Orthopaedics and Related Research, 3814-3822.
Bibliography
Aubut, J. A., Mehta, S., Cullen, N., Teasell, R. W., & Team, G. t. (2011). A comparison of
heterotopic ossification treatment within the traumatic brain and spinal cord injured
population: an evidence based systematic review. NeuroRehabilitation, 151-160.
Botolin, S., Mauffrey, C., Hammerberg, E. M., Hak, D. J., & Stahel, P. F. (2013). Heterotopic
ossification in the reaming tract of a percutaneous antegrade femoral nail: a case report.
Journal of medical case reports, 90.
Fisher, H. W., & Lotze, P. M. (2011). Nerve injury locations during retropubic sling
procedures. . International urogynecology journal, 439-441.
Gelalis, I. D., Politis, A. N., Arnaoutoglou, C. M., Korompilias, A. V., E., P. E., Vekris, M. D.,
& ... & Xenakis, T. A. (2012). Diagnostic and treatment modalities in nonunions of the
femoral shaft. A review. Injury, 980-988.
Kaiser, M. M., Wessel, L. M., Zachert, G., Stratmann, C., Eggert, R., Gros, N., & ... & Rapp, M.
(2011). Biomechanical analysis of a synthetic femur spiral fracture model: influence of
different materials on the stiffness in flexible intramedullary nailing. . Clinical
Biomechanics, 592-597.
Kalyani, B. S., Fisher, B. E., Roberts, C. S., & Giannoudis, P. V. (2011). Compartment
syndrome of the forearm: a systematic review. The Journal of hand surgery, 535-543.
Kong, H., & Sabharwal, S. (2014). External fixation for closed pediatric femoral shaft fractures:
where are we now?. Clinical Orthopaedics and Related Research, 3814-3822.
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.