Case Study: Nursing Practice and Management of Type 1 Diabetes
VerifiedAdded on 2022/10/17
|9
|1971
|11
Case Study
AI Summary
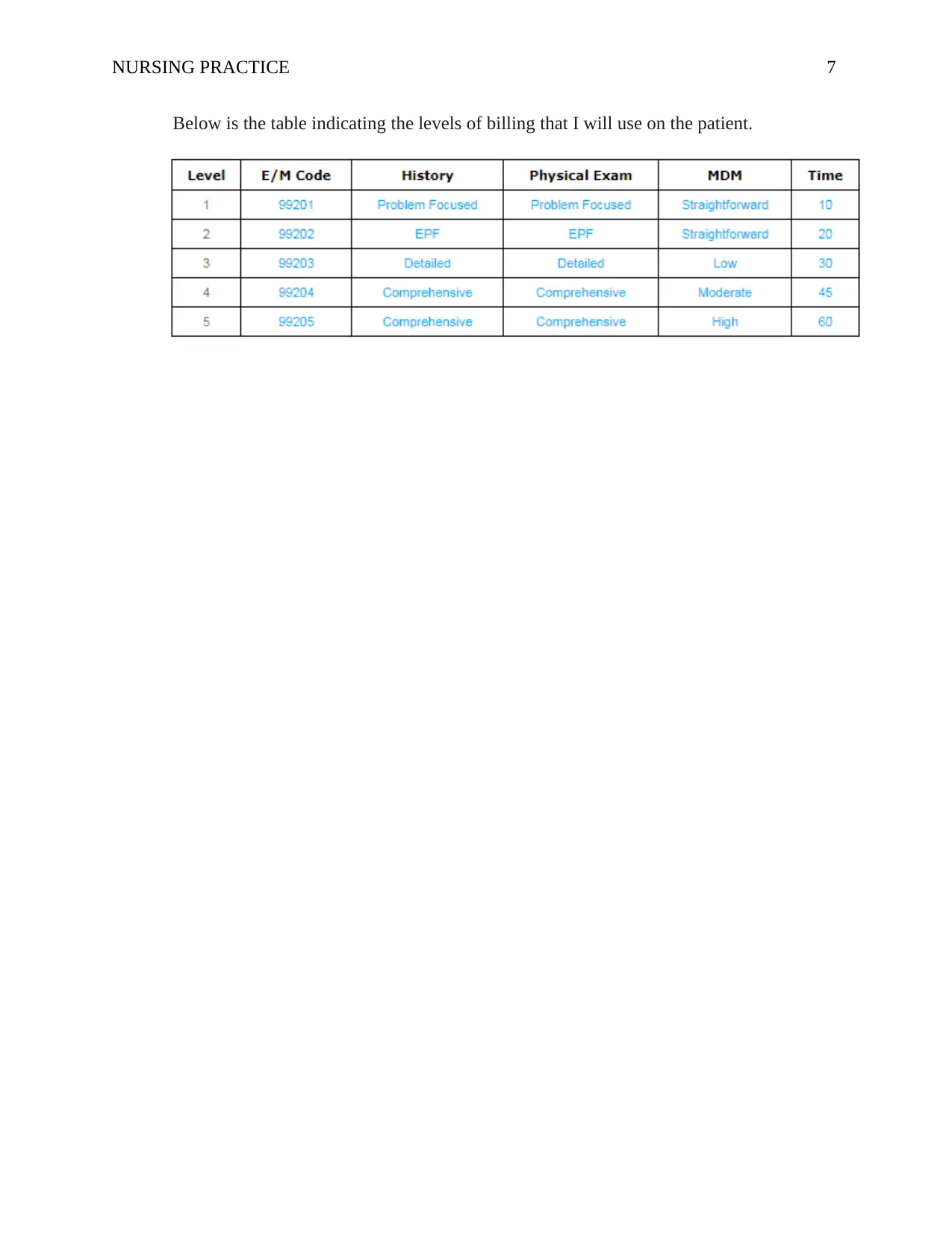
This case study presents the nursing practice related to a 50-year-old male, Mr. Kelvin, who was initially diagnosed with type 2 diabetes based on his fatigue, anxiety, family history, and initial blood tests. The case details the patient's history, including a physical exam, urinalysis, and BMI assessment. The initial treatment with metformin was followed by gliclazide. However, subsequent tests revealed the presence of glucose and ketones in the urine, leading to a diagnosis of type 1 diabetes. The paper discusses differential diagnoses, the characteristics of both type 1 and type 2 diabetes, and the diagnostic tests used, including fasting plasma glucose, oral glucose tolerance, random blood glucose, and Hemoglobin A1C tests. The treatment plan focuses on preventing infection, weight loss, and insulin deficiency, including dietary plans, medication, and monitoring of vital signs. Furthermore, the case highlights the importance of patient education, particularly regarding blood glucose monitoring and carbohydrate intake. The paper also includes references to support the nursing practice and treatment decisions.

1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.