NRSG 355 : Clinical Integration
VerifiedAdded on 2021/10/31
|16
|4641
|29
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING PROFESSIONAL PRACTICE
NURSING PROFESSIONAL PRACTICE
Name of the Student:
Name of the University:
Author note:
NURSING PROFESSIONAL PRACTICE
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1NURSING PROFESSIONAL PRACTICE
NRSG355 WRITTEN ASSIGNMENT
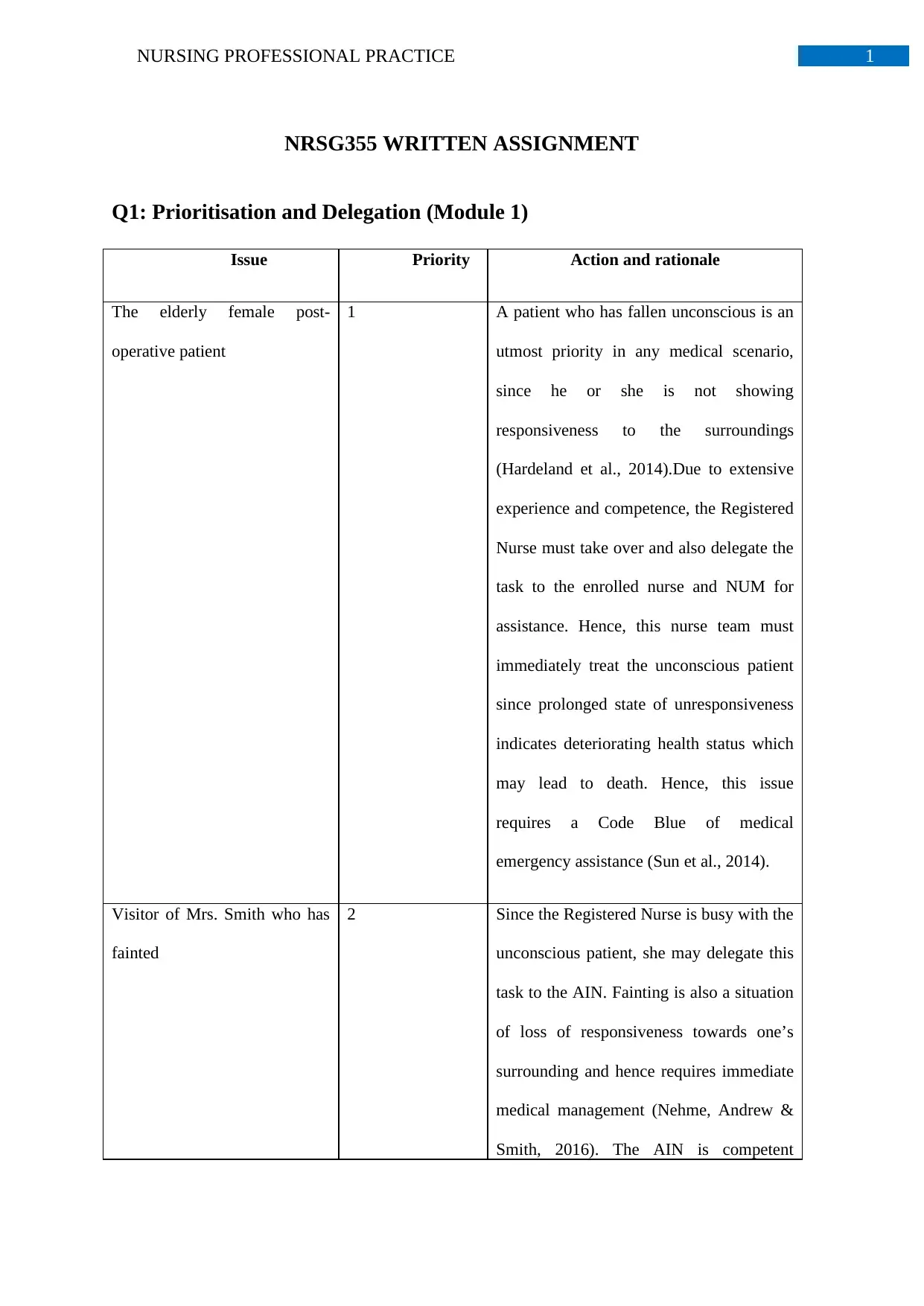
Q1: Prioritisation and Delegation (Module 1)
Issue Priority Action and rationale
The elderly female post-
operative patient
1 A patient who has fallen unconscious is an
utmost priority in any medical scenario,
since he or she is not showing
responsiveness to the surroundings
(Hardeland et al., 2014).Due to extensive
experience and competence, the Registered
Nurse must take over and also delegate the
task to the enrolled nurse and NUM for
assistance. Hence, this nurse team must
immediately treat the unconscious patient
since prolonged state of unresponsiveness
indicates deteriorating health status which
may lead to death. Hence, this issue
requires a Code Blue of medical
emergency assistance (Sun et al., 2014).
Visitor of Mrs. Smith who has
fainted
2 Since the Registered Nurse is busy with the
unconscious patient, she may delegate this
task to the AIN. Fainting is also a situation
of loss of responsiveness towards one’s
surrounding and hence requires immediate
medical management (Nehme, Andrew &
Smith, 2016). The AIN is competent
NRSG355 WRITTEN ASSIGNMENT
Q1: Prioritisation and Delegation (Module 1)
Issue Priority Action and rationale
The elderly female post-
operative patient
1 A patient who has fallen unconscious is an
utmost priority in any medical scenario,
since he or she is not showing
responsiveness to the surroundings
(Hardeland et al., 2014).Due to extensive
experience and competence, the Registered
Nurse must take over and also delegate the
task to the enrolled nurse and NUM for
assistance. Hence, this nurse team must
immediately treat the unconscious patient
since prolonged state of unresponsiveness
indicates deteriorating health status which
may lead to death. Hence, this issue
requires a Code Blue of medical
emergency assistance (Sun et al., 2014).
Visitor of Mrs. Smith who has
fainted
2 Since the Registered Nurse is busy with the
unconscious patient, she may delegate this
task to the AIN. Fainting is also a situation
of loss of responsiveness towards one’s
surrounding and hence requires immediate
medical management (Nehme, Andrew &
Smith, 2016). The AIN is competent
2NURSING PROFESSIONAL PRACTICE
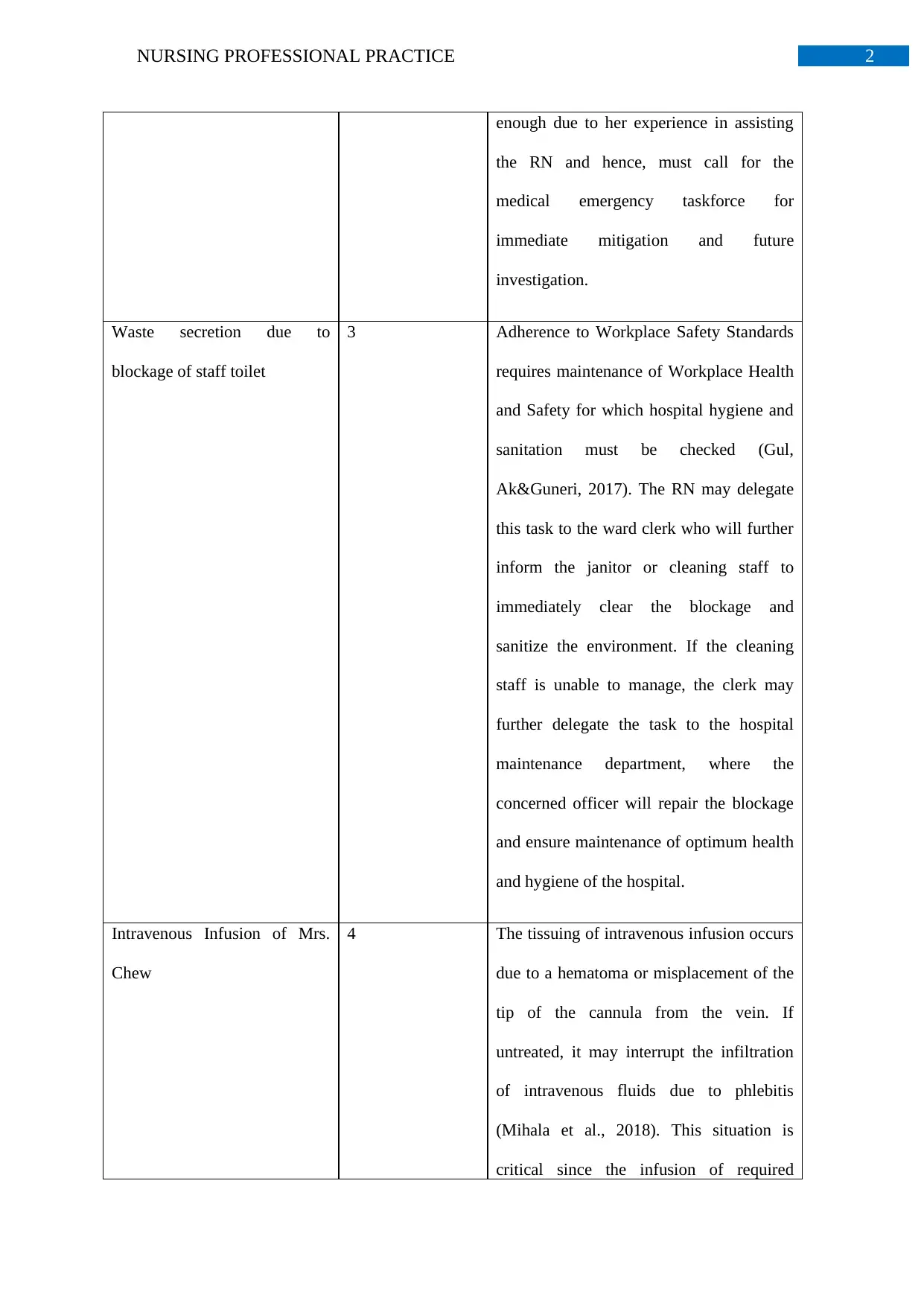
enough due to her experience in assisting
the RN and hence, must call for the
medical emergency taskforce for
immediate mitigation and future
investigation.
Waste secretion due to
blockage of staff toilet
3 Adherence to Workplace Safety Standards
requires maintenance of Workplace Health
and Safety for which hospital hygiene and
sanitation must be checked (Gul,
Ak&Guneri, 2017). The RN may delegate
this task to the ward clerk who will further
inform the janitor or cleaning staff to
immediately clear the blockage and
sanitize the environment. If the cleaning
staff is unable to manage, the clerk may
further delegate the task to the hospital
maintenance department, where the
concerned officer will repair the blockage
and ensure maintenance of optimum health
and hygiene of the hospital.
Intravenous Infusion of Mrs.
Chew
4 The tissuing of intravenous infusion occurs
due to a hematoma or misplacement of the
tip of the cannula from the vein. If
untreated, it may interrupt the infiltration
of intravenous fluids due to phlebitis
(Mihala et al., 2018). This situation is
critical since the infusion of required
enough due to her experience in assisting
the RN and hence, must call for the
medical emergency taskforce for
immediate mitigation and future
investigation.
Waste secretion due to
blockage of staff toilet
3 Adherence to Workplace Safety Standards
requires maintenance of Workplace Health
and Safety for which hospital hygiene and
sanitation must be checked (Gul,
Ak&Guneri, 2017). The RN may delegate
this task to the ward clerk who will further
inform the janitor or cleaning staff to
immediately clear the blockage and
sanitize the environment. If the cleaning
staff is unable to manage, the clerk may
further delegate the task to the hospital
maintenance department, where the
concerned officer will repair the blockage
and ensure maintenance of optimum health
and hygiene of the hospital.
Intravenous Infusion of Mrs.
Chew
4 The tissuing of intravenous infusion occurs
due to a hematoma or misplacement of the
tip of the cannula from the vein. If
untreated, it may interrupt the infiltration
of intravenous fluids due to phlebitis
(Mihala et al., 2018). This situation is
critical since the infusion of required
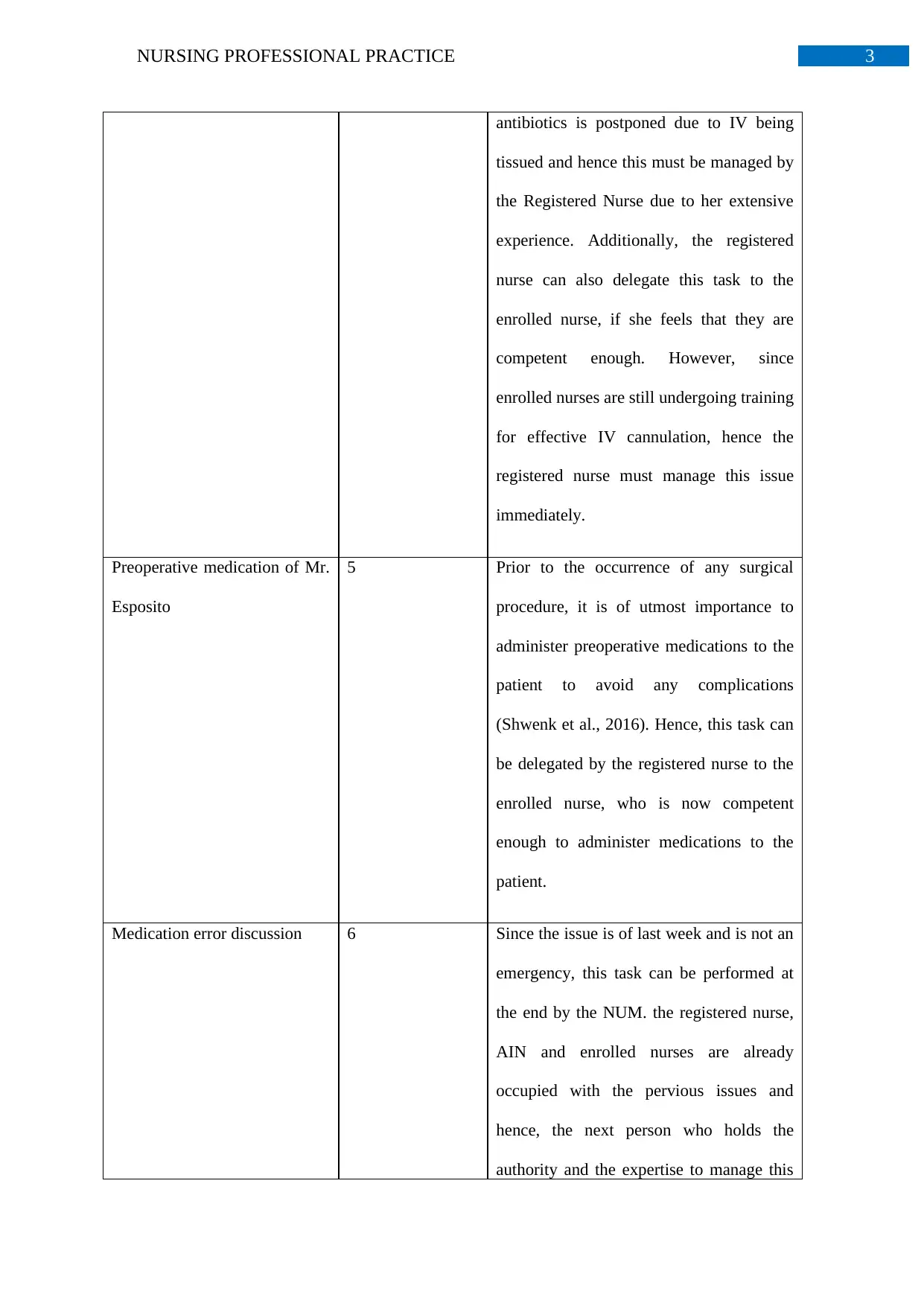
3NURSING PROFESSIONAL PRACTICE
antibiotics is postponed due to IV being
tissued and hence this must be managed by
the Registered Nurse due to her extensive
experience. Additionally, the registered
nurse can also delegate this task to the
enrolled nurse, if she feels that they are
competent enough. However, since
enrolled nurses are still undergoing training
for effective IV cannulation, hence the
registered nurse must manage this issue
immediately.
Preoperative medication of Mr.
Esposito
5 Prior to the occurrence of any surgical
procedure, it is of utmost importance to
administer preoperative medications to the
patient to avoid any complications
(Shwenk et al., 2016). Hence, this task can
be delegated by the registered nurse to the
enrolled nurse, who is now competent
enough to administer medications to the
patient.
Medication error discussion 6 Since the issue is of last week and is not an
emergency, this task can be performed at
the end by the NUM. the registered nurse,
AIN and enrolled nurses are already
occupied with the pervious issues and
hence, the next person who holds the
authority and the expertise to manage this
antibiotics is postponed due to IV being
tissued and hence this must be managed by
the Registered Nurse due to her extensive
experience. Additionally, the registered
nurse can also delegate this task to the
enrolled nurse, if she feels that they are
competent enough. However, since
enrolled nurses are still undergoing training
for effective IV cannulation, hence the
registered nurse must manage this issue
immediately.
Preoperative medication of Mr.
Esposito
5 Prior to the occurrence of any surgical
procedure, it is of utmost importance to
administer preoperative medications to the
patient to avoid any complications
(Shwenk et al., 2016). Hence, this task can
be delegated by the registered nurse to the
enrolled nurse, who is now competent
enough to administer medications to the
patient.
Medication error discussion 6 Since the issue is of last week and is not an
emergency, this task can be performed at
the end by the NUM. the registered nurse,
AIN and enrolled nurses are already
occupied with the pervious issues and
hence, the next person who holds the
authority and the expertise to manage this
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING PROFESSIONAL PRACTICE
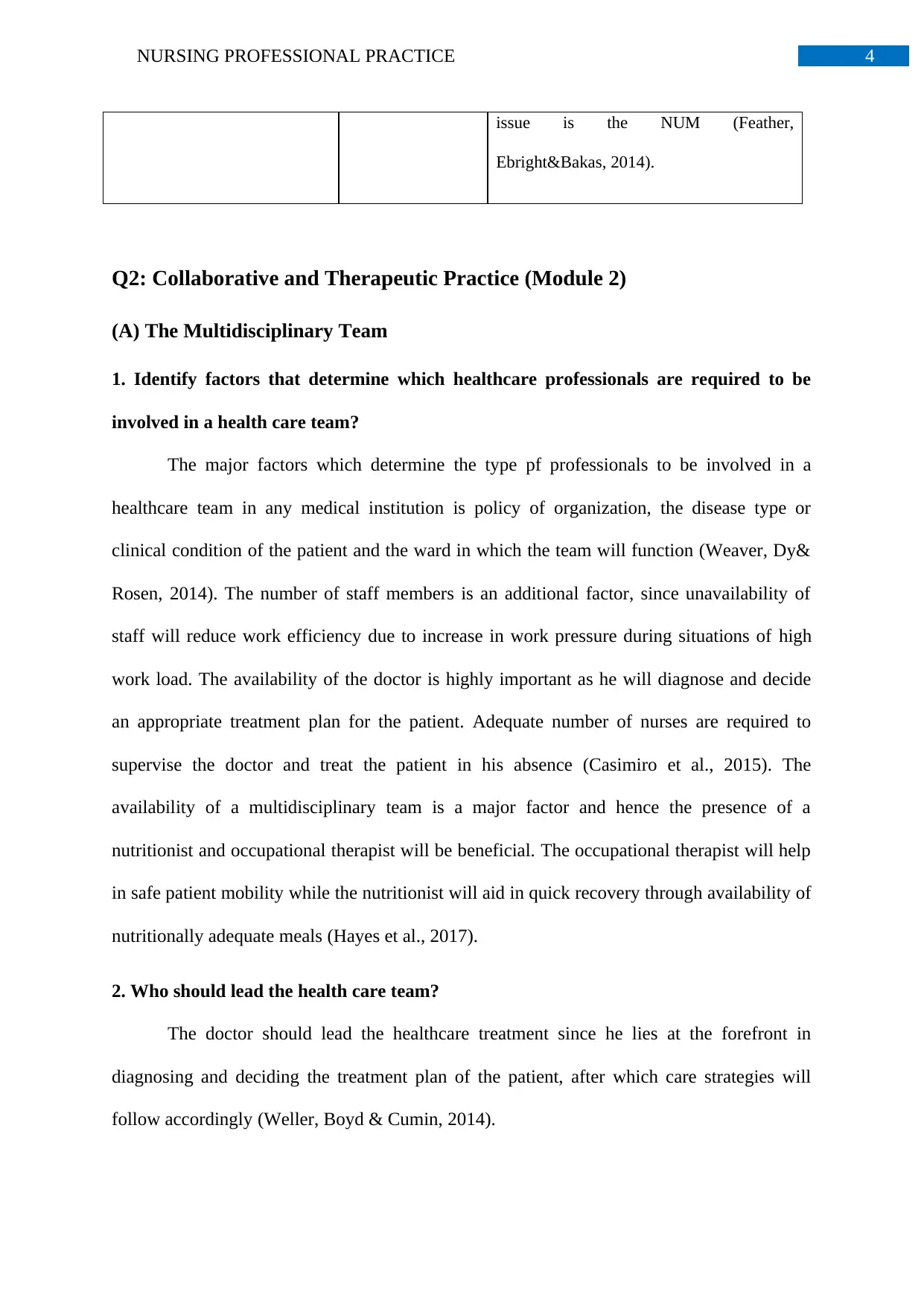
issue is the NUM (Feather,
Ebright&Bakas, 2014).
Q2: Collaborative and Therapeutic Practice (Module 2)
(A) The Multidisciplinary Team
1. Identify factors that determine which healthcare professionals are required to be
involved in a health care team?
The major factors which determine the type pf professionals to be involved in a
healthcare team in any medical institution is policy of organization, the disease type or
clinical condition of the patient and the ward in which the team will function (Weaver, Dy&
Rosen, 2014). The number of staff members is an additional factor, since unavailability of
staff will reduce work efficiency due to increase in work pressure during situations of high
work load. The availability of the doctor is highly important as he will diagnose and decide
an appropriate treatment plan for the patient. Adequate number of nurses are required to
supervise the doctor and treat the patient in his absence (Casimiro et al., 2015). The
availability of a multidisciplinary team is a major factor and hence the presence of a
nutritionist and occupational therapist will be beneficial. The occupational therapist will help
in safe patient mobility while the nutritionist will aid in quick recovery through availability of
nutritionally adequate meals (Hayes et al., 2017).
2. Who should lead the health care team?
The doctor should lead the healthcare treatment since he lies at the forefront in
diagnosing and deciding the treatment plan of the patient, after which care strategies will
follow accordingly (Weller, Boyd & Cumin, 2014).
issue is the NUM (Feather,
Ebright&Bakas, 2014).
Q2: Collaborative and Therapeutic Practice (Module 2)
(A) The Multidisciplinary Team
1. Identify factors that determine which healthcare professionals are required to be
involved in a health care team?
The major factors which determine the type pf professionals to be involved in a
healthcare team in any medical institution is policy of organization, the disease type or
clinical condition of the patient and the ward in which the team will function (Weaver, Dy&
Rosen, 2014). The number of staff members is an additional factor, since unavailability of
staff will reduce work efficiency due to increase in work pressure during situations of high
work load. The availability of the doctor is highly important as he will diagnose and decide
an appropriate treatment plan for the patient. Adequate number of nurses are required to
supervise the doctor and treat the patient in his absence (Casimiro et al., 2015). The
availability of a multidisciplinary team is a major factor and hence the presence of a
nutritionist and occupational therapist will be beneficial. The occupational therapist will help
in safe patient mobility while the nutritionist will aid in quick recovery through availability of
nutritionally adequate meals (Hayes et al., 2017).
2. Who should lead the health care team?
The doctor should lead the healthcare treatment since he lies at the forefront in
diagnosing and deciding the treatment plan of the patient, after which care strategies will
follow accordingly (Weller, Boyd & Cumin, 2014).
5NURSING PROFESSIONAL PRACTICE
3. Who is the most important member of the health care team?
The most important member of the healthcare team is the patient whose consent is of
utmost priority before commencement of the treatment procedure. Hence, every healthcare
team must adopt a patient-centred approach for efficient performance and continuously
inform the patient about the selected treatment plan and update him regarding his progress or
deterioration. Additionally, the doctor and the nurses are equally important members, since
the final and best treatment plan is decided by the doctor based on his expert diagnosis and
the nurses are involved in supervising and caring for the patient in his absence (Carayon et
al., 2014).
(B) Case Study
1. What are the key issues in this dilemma?
As per the case study, the outcome of patient medical choices seems to be the ethical
dilemma. This dilemma occurs due to the importance of valuing patient’s decision and
consent, during conductance of patient centred approach in treatment and medical decision-
making (Monrouxe et al., 2015). Despite the requirement of further treatment of Grant due to
his medical condition, his wife’s Georgina’s eagerness to have him home as well as Grant’s
grief of being away from his family also has to be considered since patient demands are also
important for quality treatment.
2. What outcomes would be best for Grant and his family?
Family involvement and family therapy has been documented to quicken the recovery
of the patient (Fox & Reeves, 2015). As evident, from the case study, Grant as well as his
family are exhibiting considerable disinterest in treatment due to their separation from each
other. Hence the best outcome for Grant would involve shifting to the outpatient department
which would reunite with his family.
3. Who is the most important member of the health care team?
The most important member of the healthcare team is the patient whose consent is of
utmost priority before commencement of the treatment procedure. Hence, every healthcare
team must adopt a patient-centred approach for efficient performance and continuously
inform the patient about the selected treatment plan and update him regarding his progress or
deterioration. Additionally, the doctor and the nurses are equally important members, since
the final and best treatment plan is decided by the doctor based on his expert diagnosis and
the nurses are involved in supervising and caring for the patient in his absence (Carayon et
al., 2014).
(B) Case Study
1. What are the key issues in this dilemma?
As per the case study, the outcome of patient medical choices seems to be the ethical
dilemma. This dilemma occurs due to the importance of valuing patient’s decision and
consent, during conductance of patient centred approach in treatment and medical decision-
making (Monrouxe et al., 2015). Despite the requirement of further treatment of Grant due to
his medical condition, his wife’s Georgina’s eagerness to have him home as well as Grant’s
grief of being away from his family also has to be considered since patient demands are also
important for quality treatment.
2. What outcomes would be best for Grant and his family?
Family involvement and family therapy has been documented to quicken the recovery
of the patient (Fox & Reeves, 2015). As evident, from the case study, Grant as well as his
family are exhibiting considerable disinterest in treatment due to their separation from each
other. Hence the best outcome for Grant would involve shifting to the outpatient department
which would reunite with his family.
6NURSING PROFESSIONAL PRACTICE
3. How would you guide the group in achieving this best outcome?
As a team leader, I will adopt a family centred approach to treatment, which involves
placing the opinion and consent of the family of the patient at the highest regard, especially
during the decision-making process of diagnosis, care and treatment (Coyne, 2015). Hence,
during the meeting of the healthcare team, I would also involve Grant and Georgina in the
discussion in order to receive their feedback. Adequate occupational and physiotherapy by
professionals enhances the mobility of the patient. Hence, I would clearly explain Georgina
this information as Grant still requires further treatment as per the expert opinions of the
professional team. I would also instruct my team to consider Grant and Georgina’s interest
since for ensuring patient satisfaction, a healthcare team must always prioritise the patient
and his family through adoption of patient-centred and family-centred approach (Rankin,
2015).
Q3: Provision and Coordination of Care (Module 3)
1. What further questions will you need to ask the nurse?
According to the Australian Medical Association, obtaining an effective handover is
of utmost importance for the deliverance of optimum treatment to the patient, as it provides
vital information about the clinical signs and symptoms of the patient, his family background
as well as past medical history (Whitty et al., 2017).
In accordance to the handover, the nurse did not seem to ask about the vital signs of
the patient. Hence, for an appropriate handover, we must ask about the vital signs of the
patients, which indicates the how efficiently the basic functions of the body are being
conducted which includes, pulse rate, rate of respiration, blood pressure and body
temperature. If such an assessment produces abnormal values, it would indicate a critical fatal
3. How would you guide the group in achieving this best outcome?
As a team leader, I will adopt a family centred approach to treatment, which involves
placing the opinion and consent of the family of the patient at the highest regard, especially
during the decision-making process of diagnosis, care and treatment (Coyne, 2015). Hence,
during the meeting of the healthcare team, I would also involve Grant and Georgina in the
discussion in order to receive their feedback. Adequate occupational and physiotherapy by
professionals enhances the mobility of the patient. Hence, I would clearly explain Georgina
this information as Grant still requires further treatment as per the expert opinions of the
professional team. I would also instruct my team to consider Grant and Georgina’s interest
since for ensuring patient satisfaction, a healthcare team must always prioritise the patient
and his family through adoption of patient-centred and family-centred approach (Rankin,
2015).
Q3: Provision and Coordination of Care (Module 3)
1. What further questions will you need to ask the nurse?
According to the Australian Medical Association, obtaining an effective handover is
of utmost importance for the deliverance of optimum treatment to the patient, as it provides
vital information about the clinical signs and symptoms of the patient, his family background
as well as past medical history (Whitty et al., 2017).
In accordance to the handover, the nurse did not seem to ask about the vital signs of
the patient. Hence, for an appropriate handover, we must ask about the vital signs of the
patients, which indicates the how efficiently the basic functions of the body are being
conducted which includes, pulse rate, rate of respiration, blood pressure and body
temperature. If such an assessment produces abnormal values, it would indicate a critical fatal
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING PROFESSIONAL PRACTICE
situation, where the patient would require immediate medical emergency treatment
(Dominguez et al., 2015).
There is no mention by the emergency nurse about the measurement and assessment
of pain and its treatment. Hence, the nurse must be asked about the data associated with the
pain, since it has an impact on the level of anxiety, ability to cope and vital signs of the
patient. For this, the conductance of PQRST pain assessment tool is important (Fink & Brant,
2018).
Despite being admitted for an abdominal pain, the nurse did not mention about an
abdominal pain assessment, which would be indicative about the presence of any fluids,
palpations or protrusions in the abdominal area through auditory and visual inspection (Hall,
2017).
The nurse did not mention about fluid balance chart. The fluid balance chart of the
patient will indicate electrolyte status and hydration of the patient through documentation of
the amount of fluid consumed as well as excretion. Hence it is required to ask about the fluid
balance chart since this will determine which medicines and treatments are required to be
given to the patient (McGloin, 2015).
Other information which is missing in the handover is the medications taken by the
patient currently, since they may indicate presence of any disease or comorbidity. Other
missing information is the family details and social status since according to family centred
care, patient’s family must be contacted during treatment and emergency (Pucher et al.,
2015).
situation, where the patient would require immediate medical emergency treatment
(Dominguez et al., 2015).
There is no mention by the emergency nurse about the measurement and assessment
of pain and its treatment. Hence, the nurse must be asked about the data associated with the
pain, since it has an impact on the level of anxiety, ability to cope and vital signs of the
patient. For this, the conductance of PQRST pain assessment tool is important (Fink & Brant,
2018).
Despite being admitted for an abdominal pain, the nurse did not mention about an
abdominal pain assessment, which would be indicative about the presence of any fluids,
palpations or protrusions in the abdominal area through auditory and visual inspection (Hall,
2017).
The nurse did not mention about fluid balance chart. The fluid balance chart of the
patient will indicate electrolyte status and hydration of the patient through documentation of
the amount of fluid consumed as well as excretion. Hence it is required to ask about the fluid
balance chart since this will determine which medicines and treatments are required to be
given to the patient (McGloin, 2015).
Other information which is missing in the handover is the medications taken by the
patient currently, since they may indicate presence of any disease or comorbidity. Other
missing information is the family details and social status since according to family centred
care, patient’s family must be contacted during treatment and emergency (Pucher et al.,
2015).
8NURSING PROFESSIONAL PRACTICE
2. List specifically what further assessments you would complete when the
patient arrives onto the ward?
An ABCDE assessment which is used to assess airway, breathing, circulation,
disability and exposure. The rationale behind this is to indicate whether the health
status of the patient is at a critical detrimental condition which may lead to death if
left untreated (Steele, Greenwood & Desai, 2017).
Vital signs: The purpose of this assessment is to understand basic body functioning, as
a deteriorating vital signs means the patient needs immediate treatment and may
succumb to his injuries. This requires assessment of blood pressure, heart rate,
temperature of the body and rate of respiration and hence, evaluation of efficacy of
basic body function is the rationale behind its conductance (Middleton, Fritz &
Lusardi, 2015).
Cardiac assessment: The purpose behind this is to uncover if the patient has the risk of
developing any cardiovascular problem or has any existing shortcoming in
cardiovascular functioning. It measures previous patient history of strokes,
hypertension, hyperlipidemia and cardiovascular disorders. Identification of any
pathological disease of the heart is the rationale behind this assessment, especially if
there is chest pain in the patient (DeKoninck et al., 2014).
Respiratory assessment: The rationale and purpose of this is to identify any
pathological condition of the patient’s pulmonary system, such as pneumonia through
observation of breathing and presence of wheezing in the patient. Abnormal sounds of
bubbling, crackling and rumbling are produced during breathing if lungs are affected
by pneumonia (Kalu et al., 2016).
Pain assessment: The purpose behind this is to obtain data about pain history faced by
the patient. Evaluation of nature of pain and its severity, through assessment of
2. List specifically what further assessments you would complete when the
patient arrives onto the ward?
An ABCDE assessment which is used to assess airway, breathing, circulation,
disability and exposure. The rationale behind this is to indicate whether the health
status of the patient is at a critical detrimental condition which may lead to death if
left untreated (Steele, Greenwood & Desai, 2017).
Vital signs: The purpose of this assessment is to understand basic body functioning, as
a deteriorating vital signs means the patient needs immediate treatment and may
succumb to his injuries. This requires assessment of blood pressure, heart rate,
temperature of the body and rate of respiration and hence, evaluation of efficacy of
basic body function is the rationale behind its conductance (Middleton, Fritz &
Lusardi, 2015).
Cardiac assessment: The purpose behind this is to uncover if the patient has the risk of
developing any cardiovascular problem or has any existing shortcoming in
cardiovascular functioning. It measures previous patient history of strokes,
hypertension, hyperlipidemia and cardiovascular disorders. Identification of any
pathological disease of the heart is the rationale behind this assessment, especially if
there is chest pain in the patient (DeKoninck et al., 2014).
Respiratory assessment: The rationale and purpose of this is to identify any
pathological condition of the patient’s pulmonary system, such as pneumonia through
observation of breathing and presence of wheezing in the patient. Abnormal sounds of
bubbling, crackling and rumbling are produced during breathing if lungs are affected
by pneumonia (Kalu et al., 2016).
Pain assessment: The purpose behind this is to obtain data about pain history faced by
the patient. Evaluation of nature of pain and its severity, through assessment of
9NURSING PROFESSIONAL PRACTICE
provocation or palliation, quality or quantity, radiation and region, severity and pain
occurrence timings is the rationale behind this tool (Young, 2017).
Abdominal assessment: The purpose behind this is to identify excessive fluid
deposition or oedema in the patient which may cause kidney diseases in the future.
Inspection of abdominal protrusions, abdominal palpations and abnormal abdominal
sounds to monitor nature of patient abdominal functioning is the rationale behind this
assessment (Markiet et al., 2017).
Q4: Time Management and Delegation (Module 4)
Five nursing allocation models are present, as stated by the government of New South
Wales. These are task, team, primary nursing, allocation and modular models. Delegation of a
single registered nurse to only one patient is the primary care model. Nursing involving
delegation and allocation based on level of competency is the task allocation model.
Delegation of a single, competent nurse to multiple patients is the feature of allocation model.
Team leaders are present in team nursing model, as they are solely responsible for staff
functioning by delegating work according to expertise. In modular approach, a group of
patients – or modules, determine the nature of work to be performed by the medical team
(Zlotnik et al., 2015).
In the case study, out of a total of 22 patients, 14 patients have faced surgery. While 4
patients have encountered treatment intravenously, remaining 8 have encountered
conventional care. There is 1 enrolled nurse, 1 NUM and 3 AINs. For this case, usage of team
nursing model would be useful for providing efficiently, quality treatment to the patients
which will lead to their quick recovery and positive outcomes in health. This approach
requires a team leader who will ensure unity and collaborative functioning of the medical
team which will help to meet the clinical objectives of the organization. This model is
provocation or palliation, quality or quantity, radiation and region, severity and pain
occurrence timings is the rationale behind this tool (Young, 2017).
Abdominal assessment: The purpose behind this is to identify excessive fluid
deposition or oedema in the patient which may cause kidney diseases in the future.
Inspection of abdominal protrusions, abdominal palpations and abnormal abdominal
sounds to monitor nature of patient abdominal functioning is the rationale behind this
assessment (Markiet et al., 2017).
Q4: Time Management and Delegation (Module 4)
Five nursing allocation models are present, as stated by the government of New South
Wales. These are task, team, primary nursing, allocation and modular models. Delegation of a
single registered nurse to only one patient is the primary care model. Nursing involving
delegation and allocation based on level of competency is the task allocation model.
Delegation of a single, competent nurse to multiple patients is the feature of allocation model.
Team leaders are present in team nursing model, as they are solely responsible for staff
functioning by delegating work according to expertise. In modular approach, a group of
patients – or modules, determine the nature of work to be performed by the medical team
(Zlotnik et al., 2015).
In the case study, out of a total of 22 patients, 14 patients have faced surgery. While 4
patients have encountered treatment intravenously, remaining 8 have encountered
conventional care. There is 1 enrolled nurse, 1 NUM and 3 AINs. For this case, usage of team
nursing model would be useful for providing efficiently, quality treatment to the patients
which will lead to their quick recovery and positive outcomes in health. This approach
requires a team leader who will ensure unity and collaborative functioning of the medical
team which will help to meet the clinical objectives of the organization. This model is
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING PROFESSIONAL PRACTICE
advantageous since it has been documented to improve satisfaction amongst nurses, provide a
supportive occupational surrounding and improvement in the interaction between members
which results in patients receiving safe and high quality treatment (Deravin et al., 2017).
Hence, for the team nursing approach model of allocation, the registered nurse must adopt the
role of the team leader. For this, she must recognize the scope of practice and competency of
each nursing staff member.
What is delegation? When the registered nurse delegate, what you have to be
aware to other healthcare professional’s competencies?
Delegation is a process of task allocation or instruction to the team members, which is
followed by team leaders such as registered nurse. Delegation must be performed based on
the level of experience and competence possessed by each team member, which the
registered nurse must consider before allocating a task.
For appropriate delegation which considers the expertise of the nursing workforce, the
registered nurse of team leader must adopt a team nursing approach (Yoon, Kim & Shin,
2016). Hence, the registered nurse should be aware of the low level of competency presented
by the enrolled nurses since they are undergoing training and are new to critical medical
emergencies. Hence, being the team leader, the registered nurse should attend to the surgical
patients herself. This is due to the fact that she has vast scope of exhibiting her expertise and
skills since she possesses extensive experience and competency to manage critical health
situations. The registered nurse can delegate the enrolled nurse to manage conventional care
patients. This is due to the fact that the scope of practice of enrolled nurses is low, since they
are still undergoing training, are relatively new to the surrounding, have reduced experience
and present low levels of competency. The AIN can be delegated to assist the enrolled nurse
for patients receiving intravenous treatment this is due to the fact that the AIN’s scope of
functioning lies at assisting the registered nurse. Due to acquiring this scope of practice by
advantageous since it has been documented to improve satisfaction amongst nurses, provide a
supportive occupational surrounding and improvement in the interaction between members
which results in patients receiving safe and high quality treatment (Deravin et al., 2017).
Hence, for the team nursing approach model of allocation, the registered nurse must adopt the
role of the team leader. For this, she must recognize the scope of practice and competency of
each nursing staff member.
What is delegation? When the registered nurse delegate, what you have to be
aware to other healthcare professional’s competencies?
Delegation is a process of task allocation or instruction to the team members, which is
followed by team leaders such as registered nurse. Delegation must be performed based on
the level of experience and competence possessed by each team member, which the
registered nurse must consider before allocating a task.
For appropriate delegation which considers the expertise of the nursing workforce, the
registered nurse of team leader must adopt a team nursing approach (Yoon, Kim & Shin,
2016). Hence, the registered nurse should be aware of the low level of competency presented
by the enrolled nurses since they are undergoing training and are new to critical medical
emergencies. Hence, being the team leader, the registered nurse should attend to the surgical
patients herself. This is due to the fact that she has vast scope of exhibiting her expertise and
skills since she possesses extensive experience and competency to manage critical health
situations. The registered nurse can delegate the enrolled nurse to manage conventional care
patients. This is due to the fact that the scope of practice of enrolled nurses is low, since they
are still undergoing training, are relatively new to the surrounding, have reduced experience
and present low levels of competency. The AIN can be delegated to assist the enrolled nurse
for patients receiving intravenous treatment this is due to the fact that the AIN’s scope of
functioning lies at assisting the registered nurse. Due to acquiring this scope of practice by
11NURSING PROFESSIONAL PRACTICE
working with a highly competent nurse member, AIN will have enough experience to assist
as well as teach the enrolled nurses in the management of patients receiving intravenous
infusion.
working with a highly competent nurse member, AIN will have enough experience to assist
as well as teach the enrolled nurses in the management of patients receiving intravenous
infusion.
12NURSING PROFESSIONAL PRACTICE
References
Carayon, P., Wetterneck, T. B., Rivera-Rodriguez, A. J., Hundt, A. S., Hoonakker, P.,
Holden, R., &Gurses, A. P. (2014). Human factors systems approach to healthcare
quality and patient safety. Applied ergonomics, 45(1), 14-25.doi:
https://doi.org/10.1016/j.apergo.2013.04.023.
Casimiro, L. M., Hall, P., Kuziemsky, C., O'Connor, M., &Varpio, L. (2015). Enhancing
patient-engaged teamwork in healthcare: An observational case study. Journal of
interprofessional care, 29(1), 55-61.doi:
https://doi.org/10.3109/13561820.2014.940038.
Coyne, I. (2015). Families and health‐care professionals' perspectives and expectations of
family‐centred care: hidden expectations and unclear roles. Health expectations,
18(5), 796-808.doi: https://doi.org/10.1111/hex.12104.
DeKoninck, P., Richter, J., Van Mieghem, T., Van Schoubroeck, D., Allegaert, K., De Catte,
L., &Deprest, J. A. (2014). Cardiac assessment in fetuses with right‐sided congenital
diaphragmatic hernia: case–control study. Ultrasound in Obstetrics &Gynecology,
43(4), 432-436.doi: https://doi.org/10.1002/uog.12561.
Deravin, L., Francis, K., Nielsen, S., & Anderson, J. (2017). Nursing stress and satisfaction
outcomes resulting from implementing a team nursing model of care in a rural setting.
Journal of Hospital Administration, 6(1), 60.doi: https://doi.org/10.5430/jha.v6n1p60.
Dominguez, K., Penman-Aguilar, A., Chang, M. H., Moonesinghe, R., Castellanos, T.,
Rodriguez-Lainz, A., & Schieber, R. (2015). Vital signs: leading causes of death,
prevalence of diseases and risk factors, and use of health services among Hispanics in
the United States—2009–2013. MMWR. Morbidity and mortality weekly
References
Carayon, P., Wetterneck, T. B., Rivera-Rodriguez, A. J., Hundt, A. S., Hoonakker, P.,
Holden, R., &Gurses, A. P. (2014). Human factors systems approach to healthcare
quality and patient safety. Applied ergonomics, 45(1), 14-25.doi:
https://doi.org/10.1016/j.apergo.2013.04.023.
Casimiro, L. M., Hall, P., Kuziemsky, C., O'Connor, M., &Varpio, L. (2015). Enhancing
patient-engaged teamwork in healthcare: An observational case study. Journal of
interprofessional care, 29(1), 55-61.doi:
https://doi.org/10.3109/13561820.2014.940038.
Coyne, I. (2015). Families and health‐care professionals' perspectives and expectations of
family‐centred care: hidden expectations and unclear roles. Health expectations,
18(5), 796-808.doi: https://doi.org/10.1111/hex.12104.
DeKoninck, P., Richter, J., Van Mieghem, T., Van Schoubroeck, D., Allegaert, K., De Catte,
L., &Deprest, J. A. (2014). Cardiac assessment in fetuses with right‐sided congenital
diaphragmatic hernia: case–control study. Ultrasound in Obstetrics &Gynecology,
43(4), 432-436.doi: https://doi.org/10.1002/uog.12561.
Deravin, L., Francis, K., Nielsen, S., & Anderson, J. (2017). Nursing stress and satisfaction
outcomes resulting from implementing a team nursing model of care in a rural setting.
Journal of Hospital Administration, 6(1), 60.doi: https://doi.org/10.5430/jha.v6n1p60.
Dominguez, K., Penman-Aguilar, A., Chang, M. H., Moonesinghe, R., Castellanos, T.,
Rodriguez-Lainz, A., & Schieber, R. (2015). Vital signs: leading causes of death,
prevalence of diseases and risk factors, and use of health services among Hispanics in
the United States—2009–2013. MMWR. Morbidity and mortality weekly
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13NURSING PROFESSIONAL PRACTICE
report, 64(17), 469. Retrieved from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4584552/pdf/469-478.pdf.
Feather, R. A., Ebright, P., &Bakas, T. (2015, April). Nurse Manager Behaviors That RN s
Perceive to Affect Their Job Satisfaction. In Nursing forum (Vol. 50, No. 2, pp. 125-
136).doi: https://doi.org/10.1111/nuf.12086.
Fox, A., & Reeves, S. (2015). Interprofessional collaborative patient-centred care: a critical
exploration of two related discourses. Journal of Interprofessional Care, 29(2), 113-
118.doi: https://doi.org/10.3109/13561820.2014.954284.
Gul, M., Ak, M. F., &Guneri, A. F. (2017). Occupational health and safety risk assessment in
hospitals: A case study using two-stage fuzzy multi-criteria approach. Human and
Ecological Risk Assessment: An International Journal, 23(2), 187-202.doi:
https://doi.org/10.1080/10807039.2016.1234363.
Hall, C. (2017). Back to basics: Abdominal assessments. Australian Midwifery News, 17(2),
17. Doi:
https://search.informit.com.au/documentSummary;dn=929839608457890;res=IELHE
A.
Hardeland, C., Olasveengen, T. M., Lawrence, R., Garrison, D., Lorem, T., Farstad, G.,
&Wik, L. (2014). Comparison of Medical Priority Dispatch (MPD) and Criteria
Based Dispatch (CBD) relating to cardiac arrest calls. Resuscitation, 85(5), 612-
616.doi: https://doi.org/10.1016/j.resuscitation.2014.01.029.
Hayes, S., Wolf, C., Labbé, S., Peterson, E., & Murray, S. (2017). Primary health care
providers' roles and responsibilities: A qualitative exploration of ‘who does what’in
the treatment and management of persons affected by obesity. Journal of
report, 64(17), 469. Retrieved from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4584552/pdf/469-478.pdf.
Feather, R. A., Ebright, P., &Bakas, T. (2015, April). Nurse Manager Behaviors That RN s
Perceive to Affect Their Job Satisfaction. In Nursing forum (Vol. 50, No. 2, pp. 125-
136).doi: https://doi.org/10.1111/nuf.12086.
Fox, A., & Reeves, S. (2015). Interprofessional collaborative patient-centred care: a critical
exploration of two related discourses. Journal of Interprofessional Care, 29(2), 113-
118.doi: https://doi.org/10.3109/13561820.2014.954284.
Gul, M., Ak, M. F., &Guneri, A. F. (2017). Occupational health and safety risk assessment in
hospitals: A case study using two-stage fuzzy multi-criteria approach. Human and
Ecological Risk Assessment: An International Journal, 23(2), 187-202.doi:
https://doi.org/10.1080/10807039.2016.1234363.
Hall, C. (2017). Back to basics: Abdominal assessments. Australian Midwifery News, 17(2),
17. Doi:
https://search.informit.com.au/documentSummary;dn=929839608457890;res=IELHE
A.
Hardeland, C., Olasveengen, T. M., Lawrence, R., Garrison, D., Lorem, T., Farstad, G.,
&Wik, L. (2014). Comparison of Medical Priority Dispatch (MPD) and Criteria
Based Dispatch (CBD) relating to cardiac arrest calls. Resuscitation, 85(5), 612-
616.doi: https://doi.org/10.1016/j.resuscitation.2014.01.029.
Hayes, S., Wolf, C., Labbé, S., Peterson, E., & Murray, S. (2017). Primary health care
providers' roles and responsibilities: A qualitative exploration of ‘who does what’in
the treatment and management of persons affected by obesity. Journal of
14NURSING PROFESSIONAL PRACTICE
Communication in Healthcare, 10(1), 47-54.doi:
https://doi.org/10.1080/17538068.2016.1270874.
Kalu, N. O., Lufesi, N., Havens, D., & Mortimer, K. (2016). B26 UPDATES IN PEDIATRIC
LUNG INFECTIONS: The Practical Implementation Of The Who Integrated
Management Of Childhood Illnesses (imci) Guidelines In The Assessment Of
Pneumonia In The Under 5s In Malawi. American Journal of Respiratory and Critical
Care Medicine, 193, 1. Retrieved
from:https://search.proquest.com/openview/46295391e0398320c48c1dda459462bb/
1?pq-origsite=gscholar&cbl=40575.
Markiet, K., Szymanska-Dubowik, A., Janczewska, I., Domazalska-Popadiuk, I., Zawadzka-
Kepczynska, A., &Bianek-Bodzak, A. (2017). Agreement and reproducibility of
radiological signs in NEC using The Duke Abdominal Assessment Scale (DAAS).
Pediatric surgery international, 33(3), 335-340.doi: https://doi.org/10.1007/s00383-
016-4022-y.
McGloin, S. (2015). The ins and outs of fluid balance in the acutely ill patient. British
Journal of Nursing, 24(1), 14-18.doi: https://doi.org/10.12968/bjon.2015.24.1.14.
Middleton, A., Fritz, S. L., & Lusardi, M. (2015). Walking speed: the functional vital sign.
Journal of aging and physical activity, 23(2), 314-322.doi:
https://doi.org/10.1123/japa.2013-0236.
Mihala, G., Ray-Barruel, G., Chopra, V., Webster, J., Wallis, M., Marsh, N., ...& Rickard, C.
M. (2018). Phlebitis Signs and Symptoms With Peripheral Intravenous Catheters:
Incidence and Correlation Study. Journal of Infusion Nursing, 41(4), 260-263.doi:
10.1097/NAN.0000000000000288.
Communication in Healthcare, 10(1), 47-54.doi:
https://doi.org/10.1080/17538068.2016.1270874.
Kalu, N. O., Lufesi, N., Havens, D., & Mortimer, K. (2016). B26 UPDATES IN PEDIATRIC
LUNG INFECTIONS: The Practical Implementation Of The Who Integrated
Management Of Childhood Illnesses (imci) Guidelines In The Assessment Of
Pneumonia In The Under 5s In Malawi. American Journal of Respiratory and Critical
Care Medicine, 193, 1. Retrieved
from:https://search.proquest.com/openview/46295391e0398320c48c1dda459462bb/
1?pq-origsite=gscholar&cbl=40575.
Markiet, K., Szymanska-Dubowik, A., Janczewska, I., Domazalska-Popadiuk, I., Zawadzka-
Kepczynska, A., &Bianek-Bodzak, A. (2017). Agreement and reproducibility of
radiological signs in NEC using The Duke Abdominal Assessment Scale (DAAS).
Pediatric surgery international, 33(3), 335-340.doi: https://doi.org/10.1007/s00383-
016-4022-y.
McGloin, S. (2015). The ins and outs of fluid balance in the acutely ill patient. British
Journal of Nursing, 24(1), 14-18.doi: https://doi.org/10.12968/bjon.2015.24.1.14.
Middleton, A., Fritz, S. L., & Lusardi, M. (2015). Walking speed: the functional vital sign.
Journal of aging and physical activity, 23(2), 314-322.doi:
https://doi.org/10.1123/japa.2013-0236.
Mihala, G., Ray-Barruel, G., Chopra, V., Webster, J., Wallis, M., Marsh, N., ...& Rickard, C.
M. (2018). Phlebitis Signs and Symptoms With Peripheral Intravenous Catheters:
Incidence and Correlation Study. Journal of Infusion Nursing, 41(4), 260-263.doi:
10.1097/NAN.0000000000000288.
15NURSING PROFESSIONAL PRACTICE
Monrouxe, L. V., Rees, C. E., Dennis, I., & Wells, S. E. (2015). Professionalism dilemmas,
moral distress and the healthcare student: insights from two online UK-wide
questionnaire studies. BMJ open, 5(5), e007518.doi: 10.1136/bmjopen-2014-007518.
Nehme, Z., Andrew, E., & Smith, K. (2016). Factors influencing the timeliness of emergency
medical service response to time critical emergencies. Prehospital emergency care,
20(6), 783-791.doi: https://doi.org/10.3109/10903127.2016.1164776.
Pucher, P. H., Johnston, M. J., Aggarwal, R., Arora, S., &Darzi, A. (2015). Effectiveness of
interventions to improve patient handover in surgery: a systematic review. Surgery,
158(1), 85-95.doi: https://doi.org/10.1016/j.surg.2015.02.017.
Rankin, J. M. (2015). The rhetoric of patient and family centred care: an institutional
ethnography into what actually happens. Journal of advanced nursing, 71(3), 526-
534.doi: https://doi.org/10.1111/jan.12575.
Reith, F. C., Brennan, P. M., Maas, A. I., & Teasdale, G. M. (2016). Lack of standardization
in the use of the glasgow coma scale: results of international surveys. Journal of
neurotrauma, 33(1), 89-94.doi: https://doi.org/10.1089/neu.2014.3843.
Reith, F. C., Van den Brande, R., Synnot, A., Gruen, R., & Maas, A. I. (2016). The reliability
of the Glasgow Coma Scale: a systematic review. Intensive care medicine, 42(1), 3-
15.doi: https://doi.org/10.1007/s00134-015-4124-3.
Schwenk, E. S., Goldberg, S. F., Patel, R. D., Zhou, J., Adams, D. R., Baratta, J. L., ... &
Epstein, R. H. (2016). Adverse drug effects and preoperative medication factors
related to perioperative low-dose ketamine infusions. Regional anesthesia and pain
medicine, 41(4), 482-487.doi: 10.1097/AAP.0000000000000416.
Monrouxe, L. V., Rees, C. E., Dennis, I., & Wells, S. E. (2015). Professionalism dilemmas,
moral distress and the healthcare student: insights from two online UK-wide
questionnaire studies. BMJ open, 5(5), e007518.doi: 10.1136/bmjopen-2014-007518.
Nehme, Z., Andrew, E., & Smith, K. (2016). Factors influencing the timeliness of emergency
medical service response to time critical emergencies. Prehospital emergency care,
20(6), 783-791.doi: https://doi.org/10.3109/10903127.2016.1164776.
Pucher, P. H., Johnston, M. J., Aggarwal, R., Arora, S., &Darzi, A. (2015). Effectiveness of
interventions to improve patient handover in surgery: a systematic review. Surgery,
158(1), 85-95.doi: https://doi.org/10.1016/j.surg.2015.02.017.
Rankin, J. M. (2015). The rhetoric of patient and family centred care: an institutional
ethnography into what actually happens. Journal of advanced nursing, 71(3), 526-
534.doi: https://doi.org/10.1111/jan.12575.
Reith, F. C., Brennan, P. M., Maas, A. I., & Teasdale, G. M. (2016). Lack of standardization
in the use of the glasgow coma scale: results of international surveys. Journal of
neurotrauma, 33(1), 89-94.doi: https://doi.org/10.1089/neu.2014.3843.
Reith, F. C., Van den Brande, R., Synnot, A., Gruen, R., & Maas, A. I. (2016). The reliability
of the Glasgow Coma Scale: a systematic review. Intensive care medicine, 42(1), 3-
15.doi: https://doi.org/10.1007/s00134-015-4124-3.
Schwenk, E. S., Goldberg, S. F., Patel, R. D., Zhou, J., Adams, D. R., Baratta, J. L., ... &
Epstein, R. H. (2016). Adverse drug effects and preoperative medication factors
related to perioperative low-dose ketamine infusions. Regional anesthesia and pain
medicine, 41(4), 482-487.doi: 10.1097/AAP.0000000000000416.
1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.