Case Study of a Patient with Acute Pneumonia
VerifiedAdded on 2023/02/01
|10
|3123
|45
AI Summary
This case study report discusses the symptoms, causes, and treatment of a patient with acute pneumonia. It provides an in-depth analysis of the patient's condition and offers insights into the physiological changes associated with pneumonia. Find study material and solved assignments on Desklib.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Nursing
Student’s name:
Institutional:
Student’s name:
Institutional:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
A CASE STUDY REPORT OF A PATIENT WITH ACUTE PNEUMONIA
Introduction of the patient and the use of framework of practice thinking
This is a case study of a female patient aged 52 years old by the name Jenny who felt unwell
since two weeks ago with presentations of productive cough which was intermittent and
sometimes productive of green sputum. She has also been feeling the hotness of the body and
general body malaise for the last few days. On examination by the general practitioner, she
looked lethargic but oriented. On auscultations, she had coarse crackles on the right lower lobe
of the lungs. Specimen of green sputum was taken and for culturing which confirmed the
presence of infiltration of infections throughout her lungs and specifically the right lower lobe.
She has a past medical history of high blood pressure, obesity and hypercholesterolemia and she
is on the medication as; PO Atorvastatin drug that reduces cholesterol levels in the body, PO
Tenormin the antihypertensive drug, Tiotropium bromide inhaler, Ventolin inhaler as required.
Her vital signs were; BP- 135/85mmHg, PR- 104 beats/minute, RR-28 breaths/minute,
temperature-38.9^0c and SPO2 of 90% with no supplemental oxygen. In her social history, she
reports that she does smoke cigarettes about a pack per day. She has been doing so for the past
30 years. She stays with her husband and she does a part-time shift work as a cashier at a local
club. She has a well formed social network of friends centering close to her in the place of work.
From the clinical signs and symptoms, it is clear that she is ailing from bacterial pneumonia
which has affected the lower part of the respiratory tract. When the patient was done chest X-ray,
there were the areas of congestions within the bases and the patchy compaction at the right lung
base with the deprivation of coastal phrenic angle at the right side. The principal diagnosis,
therefore, was confirmed to be acute pneumonia.
Altered physiology and associated symptoms related to principal diagnosis
Pneumonia is an infection that causes inflammation of the air sacs in either one or both
lungs. The air sacs are filled with fluid or pus causing cough with phlegm or pus accompanied
with the feeling of chills and difficulty in breathing (Weinberger, Cockrill, & Mandel, 2017).
The extent of the effect of pneumonia infections vary in seriousness from mild to life-threatening
depending on the individual age and immunological status and also the type of agent causing the
disease. It is more serious in young children of less than five years of age and individuals of age
Introduction of the patient and the use of framework of practice thinking
This is a case study of a female patient aged 52 years old by the name Jenny who felt unwell
since two weeks ago with presentations of productive cough which was intermittent and
sometimes productive of green sputum. She has also been feeling the hotness of the body and
general body malaise for the last few days. On examination by the general practitioner, she
looked lethargic but oriented. On auscultations, she had coarse crackles on the right lower lobe
of the lungs. Specimen of green sputum was taken and for culturing which confirmed the
presence of infiltration of infections throughout her lungs and specifically the right lower lobe.
She has a past medical history of high blood pressure, obesity and hypercholesterolemia and she
is on the medication as; PO Atorvastatin drug that reduces cholesterol levels in the body, PO
Tenormin the antihypertensive drug, Tiotropium bromide inhaler, Ventolin inhaler as required.
Her vital signs were; BP- 135/85mmHg, PR- 104 beats/minute, RR-28 breaths/minute,
temperature-38.9^0c and SPO2 of 90% with no supplemental oxygen. In her social history, she
reports that she does smoke cigarettes about a pack per day. She has been doing so for the past
30 years. She stays with her husband and she does a part-time shift work as a cashier at a local
club. She has a well formed social network of friends centering close to her in the place of work.
From the clinical signs and symptoms, it is clear that she is ailing from bacterial pneumonia
which has affected the lower part of the respiratory tract. When the patient was done chest X-ray,
there were the areas of congestions within the bases and the patchy compaction at the right lung
base with the deprivation of coastal phrenic angle at the right side. The principal diagnosis,
therefore, was confirmed to be acute pneumonia.
Altered physiology and associated symptoms related to principal diagnosis
Pneumonia is an infection that causes inflammation of the air sacs in either one or both
lungs. The air sacs are filled with fluid or pus causing cough with phlegm or pus accompanied
with the feeling of chills and difficulty in breathing (Weinberger, Cockrill, & Mandel, 2017).
The extent of the effect of pneumonia infections vary in seriousness from mild to life-threatening
depending on the individual age and immunological status and also the type of agent causing the
disease. It is more serious in young children of less than five years of age and individuals of age
65 years and above. The common causes of pneumonia are bacteria that we inhale together with
the air we breathe and virus that is a presence in the lungs as normal flora and causes infections
when conditions are favorable like cold seasons in young children (Wojsyk-Banaszak, &
Bręborowicz, 2013). and when the immune system goes down. General Signs and symptoms of
pneumonia include; productive cough, chills, sweating, fever, general body malaise, shortness of
breath, decreased air entry, difficulty in breathing, wheezing, decreased oxygen saturation to less
than 90% and chest pains (Winland-Brown, & Klause, 2017).
Pneumonia can be classified in two ways, by the cause and as per the place it was acquired.
Classification by the place of acquisition includes; Community-acquired pneumonia. This is the
type of pneumonia acquired outside hospital settings (José, Periselneris, & Brown, 2015).
Another type according to acquisition is Hospital-acquired pneumonia where especially the
admitted patients in the hospitals acquire (Barbier, Andremont, Wolff, & Bouadma, 2013). This
one can be very much more serious than any other type since the bacteria involved may be more
resistant to several common antibiotics. Classification by the cause includes; bacterial
pneumonia and the common bacterium involved areas; streptococcus pneumonia. Other bacteria
that can cause pneumonia are Legionella pneumophila and Chlamydophila pneumonia
(Huijskens, et.al, 2013). Viral pneumonia; this one is not usually serious and last for a very short
period, unlike bacteria. It commonly affects young children, old people, and immune-suppressed
individuals. Mycoplasma pneumonia; mycoplasma is an organism that are neither bacteria nor
viral but has traits that are common to both. These organisms cause mild pneumonia, especially
on old age adults. Fungal pneumonia; fungi are mostly acquired through inhalation from the
environment, which they are a presence in animals and bird droppings and cause infections when
inhaled in large quantities and also when the immune system becomes weak. The common
fungus that causes pneumonia is Pneumocystis cariini pneumonia.
Bacterial pneumonia alters the physiology of the human body. The streptococcal pneumonia
bacterium leads to high fevers; this is due to the fact that the body adjusts in such a way that it
raises its temperature as a defense mechanism of the body aim at destroying the bacteria by high
temperatures (Fairbrother, & Taylor, 2014). The inflammation causes the production of phlegm
or mucus, which are secreted by the goblet cells in the respiratory tract when they are inflamed
just as a defense mechanism by these goblet cells. The body becomes generally weak due to the
the air we breathe and virus that is a presence in the lungs as normal flora and causes infections
when conditions are favorable like cold seasons in young children (Wojsyk-Banaszak, &
Bręborowicz, 2013). and when the immune system goes down. General Signs and symptoms of
pneumonia include; productive cough, chills, sweating, fever, general body malaise, shortness of
breath, decreased air entry, difficulty in breathing, wheezing, decreased oxygen saturation to less
than 90% and chest pains (Winland-Brown, & Klause, 2017).
Pneumonia can be classified in two ways, by the cause and as per the place it was acquired.
Classification by the place of acquisition includes; Community-acquired pneumonia. This is the
type of pneumonia acquired outside hospital settings (José, Periselneris, & Brown, 2015).
Another type according to acquisition is Hospital-acquired pneumonia where especially the
admitted patients in the hospitals acquire (Barbier, Andremont, Wolff, & Bouadma, 2013). This
one can be very much more serious than any other type since the bacteria involved may be more
resistant to several common antibiotics. Classification by the cause includes; bacterial
pneumonia and the common bacterium involved areas; streptococcus pneumonia. Other bacteria
that can cause pneumonia are Legionella pneumophila and Chlamydophila pneumonia
(Huijskens, et.al, 2013). Viral pneumonia; this one is not usually serious and last for a very short
period, unlike bacteria. It commonly affects young children, old people, and immune-suppressed
individuals. Mycoplasma pneumonia; mycoplasma is an organism that are neither bacteria nor
viral but has traits that are common to both. These organisms cause mild pneumonia, especially
on old age adults. Fungal pneumonia; fungi are mostly acquired through inhalation from the
environment, which they are a presence in animals and bird droppings and cause infections when
inhaled in large quantities and also when the immune system becomes weak. The common
fungus that causes pneumonia is Pneumocystis cariini pneumonia.
Bacterial pneumonia alters the physiology of the human body. The streptococcal pneumonia
bacterium leads to high fevers; this is due to the fact that the body adjusts in such a way that it
raises its temperature as a defense mechanism of the body aim at destroying the bacteria by high
temperatures (Fairbrother, & Taylor, 2014). The inflammation causes the production of phlegm
or mucus, which are secreted by the goblet cells in the respiratory tract when they are inflamed
just as a defense mechanism by these goblet cells. The body becomes generally weak due to the
fact that while the energy is concentrated on fighting the organism in the body. So the body is
left with a little amount of energy for normal basal metabolism. There is sometimes the
production of pus which is as a result of dead tissues and cells in the area of inflammation. The
smooth muscles of alveoli contract as a way of defense against the infections hence causing
narrowing of the airways leading to decrease in air entry and difficulty in breathing hence
labored breathing with the use of accessory muscles. Shortness of breath is also a result of
narrowed airways.
Health assessment
Coughing was due to the fact that the attempt of the patient to remove the products of
inflammation from the airway, that is to clear the airway. The body also develops chills which
are the shivering of the whole body. The muscles are made to contract and relax frequently in
order to generate heat that is needed to fight and kill the disease-causing microorganism in the
body. The patient also losses appetite due to little energy is available for use in the digestion of
foods taken since most of the energy is harnessed in the fight of the microorganism. Wheezing
comes as a result of the narrowed passageway of air. The air is forced out through the narrow
airways. The patient also becomes dehydrated as a result of the pneumonia infections. This is
because a lot of fluid is lost through the skin by sweating due to high temperature in the body.
Then sweating is due to the high temperatures in the body. The infections greatly influence the
lifestyle of the patient. She has to keep coughing, sweating, breath with difficult and to sleep
frequently.
Data Data analysis and linked to the assessment findings.
Subjective;
Cough, feeling generally
unwell, feeling hotness of the
body, smoker and general
body fatigue.
The patient has been having a cough due to the presence of
infections, and due to the inflammations in the respiratory
tract, the patient has to cough continuously. Cough has caused
the patient discomfort in sleeping hence has not been able to
sleep well. The patient felt increased body temperature as a
result of the inflammation due to infections. Smoking has
aggravated pneumonia infections. And the body fatigue is due
to the disease process of the body.
Objective; The patient lethargy is due to the presence of infections in the
left with a little amount of energy for normal basal metabolism. There is sometimes the
production of pus which is as a result of dead tissues and cells in the area of inflammation. The
smooth muscles of alveoli contract as a way of defense against the infections hence causing
narrowing of the airways leading to decrease in air entry and difficulty in breathing hence
labored breathing with the use of accessory muscles. Shortness of breath is also a result of
narrowed airways.
Health assessment
Coughing was due to the fact that the attempt of the patient to remove the products of
inflammation from the airway, that is to clear the airway. The body also develops chills which
are the shivering of the whole body. The muscles are made to contract and relax frequently in
order to generate heat that is needed to fight and kill the disease-causing microorganism in the
body. The patient also losses appetite due to little energy is available for use in the digestion of
foods taken since most of the energy is harnessed in the fight of the microorganism. Wheezing
comes as a result of the narrowed passageway of air. The air is forced out through the narrow
airways. The patient also becomes dehydrated as a result of the pneumonia infections. This is
because a lot of fluid is lost through the skin by sweating due to high temperature in the body.
Then sweating is due to the high temperatures in the body. The infections greatly influence the
lifestyle of the patient. She has to keep coughing, sweating, breath with difficult and to sleep
frequently.
Data Data analysis and linked to the assessment findings.
Subjective;
Cough, feeling generally
unwell, feeling hotness of the
body, smoker and general
body fatigue.
The patient has been having a cough due to the presence of
infections, and due to the inflammations in the respiratory
tract, the patient has to cough continuously. Cough has caused
the patient discomfort in sleeping hence has not been able to
sleep well. The patient felt increased body temperature as a
result of the inflammation due to infections. Smoking has
aggravated pneumonia infections. And the body fatigue is due
to the disease process of the body.
Objective; The patient lethargy is due to the presence of infections in the
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
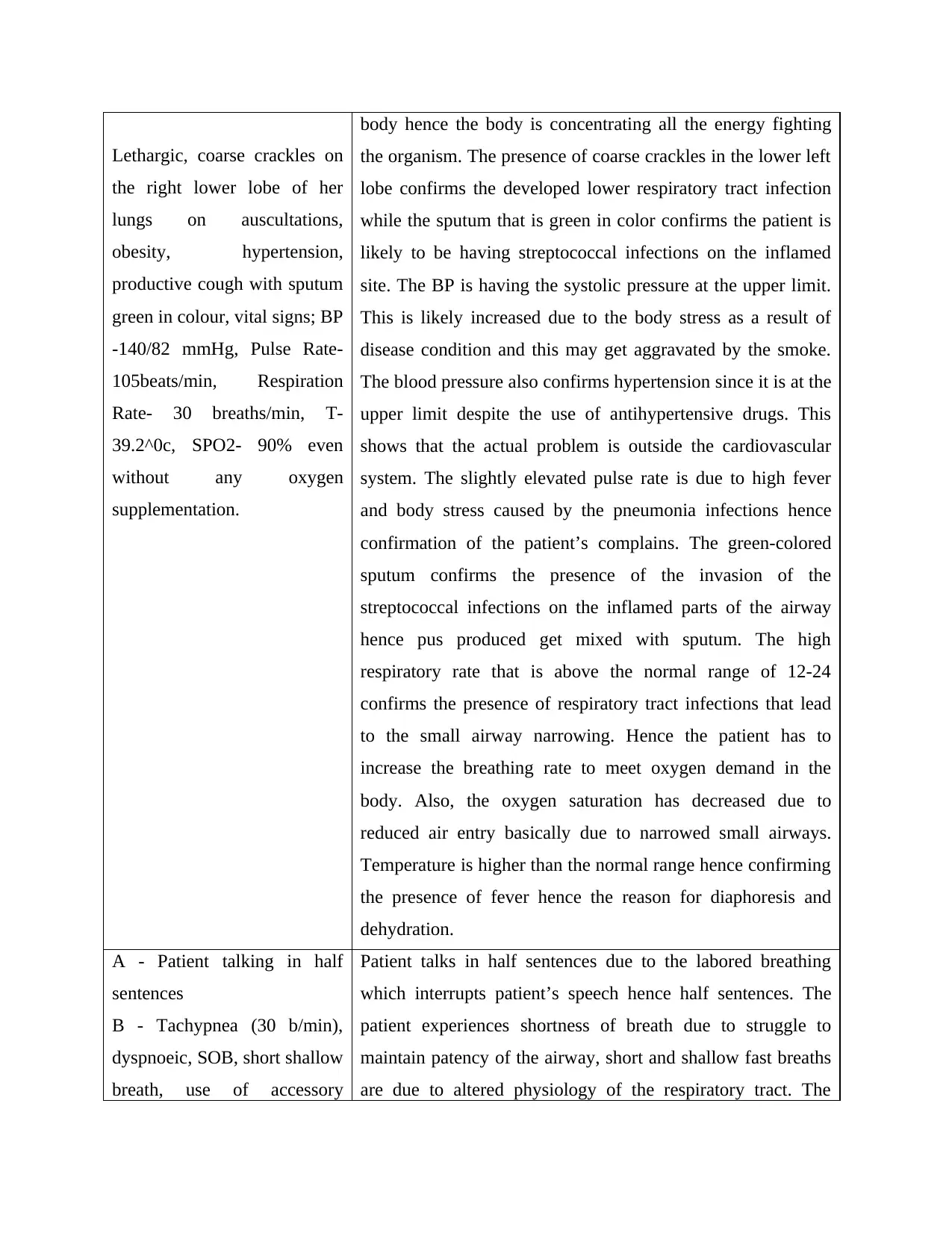
Lethargic, coarse crackles on
the right lower lobe of her
lungs on auscultations,
obesity, hypertension,
productive cough with sputum
green in colour, vital signs; BP
-140/82 mmHg, Pulse Rate-
105beats/min, Respiration
Rate- 30 breaths/min, T-
39.2^0c, SPO2- 90% even
without any oxygen
supplementation.
body hence the body is concentrating all the energy fighting
the organism. The presence of coarse crackles in the lower left
lobe confirms the developed lower respiratory tract infection
while the sputum that is green in color confirms the patient is
likely to be having streptococcal infections on the inflamed
site. The BP is having the systolic pressure at the upper limit.
This is likely increased due to the body stress as a result of
disease condition and this may get aggravated by the smoke.
The blood pressure also confirms hypertension since it is at the
upper limit despite the use of antihypertensive drugs. This
shows that the actual problem is outside the cardiovascular
system. The slightly elevated pulse rate is due to high fever
and body stress caused by the pneumonia infections hence
confirmation of the patient’s complains. The green-colored
sputum confirms the presence of the invasion of the
streptococcal infections on the inflamed parts of the airway
hence pus produced get mixed with sputum. The high
respiratory rate that is above the normal range of 12-24
confirms the presence of respiratory tract infections that lead
to the small airway narrowing. Hence the patient has to
increase the breathing rate to meet oxygen demand in the
body. Also, the oxygen saturation has decreased due to
reduced air entry basically due to narrowed small airways.
Temperature is higher than the normal range hence confirming
the presence of fever hence the reason for diaphoresis and
dehydration.
A - Patient talking in half
sentences
B - Tachypnea (30 b/min),
dyspnoeic, SOB, short shallow
breath, use of accessory
Patient talks in half sentences due to the labored breathing
which interrupts patient’s speech hence half sentences. The
patient experiences shortness of breath due to struggle to
maintain patency of the airway, short and shallow fast breaths
are due to altered physiology of the respiratory tract. The
the right lower lobe of her
lungs on auscultations,
obesity, hypertension,
productive cough with sputum
green in colour, vital signs; BP
-140/82 mmHg, Pulse Rate-
105beats/min, Respiration
Rate- 30 breaths/min, T-
39.2^0c, SPO2- 90% even
without any oxygen
supplementation.
body hence the body is concentrating all the energy fighting
the organism. The presence of coarse crackles in the lower left
lobe confirms the developed lower respiratory tract infection
while the sputum that is green in color confirms the patient is
likely to be having streptococcal infections on the inflamed
site. The BP is having the systolic pressure at the upper limit.
This is likely increased due to the body stress as a result of
disease condition and this may get aggravated by the smoke.
The blood pressure also confirms hypertension since it is at the
upper limit despite the use of antihypertensive drugs. This
shows that the actual problem is outside the cardiovascular
system. The slightly elevated pulse rate is due to high fever
and body stress caused by the pneumonia infections hence
confirmation of the patient’s complains. The green-colored
sputum confirms the presence of the invasion of the
streptococcal infections on the inflamed parts of the airway
hence pus produced get mixed with sputum. The high
respiratory rate that is above the normal range of 12-24
confirms the presence of respiratory tract infections that lead
to the small airway narrowing. Hence the patient has to
increase the breathing rate to meet oxygen demand in the
body. Also, the oxygen saturation has decreased due to
reduced air entry basically due to narrowed small airways.
Temperature is higher than the normal range hence confirming
the presence of fever hence the reason for diaphoresis and
dehydration.
A - Patient talking in half
sentences
B - Tachypnea (30 b/min),
dyspnoeic, SOB, short shallow
breath, use of accessory
Patient talks in half sentences due to the labored breathing
which interrupts patient’s speech hence half sentences. The
patient experiences shortness of breath due to struggle to
maintain patency of the airway, short and shallow fast breaths
are due to altered physiology of the respiratory tract. The
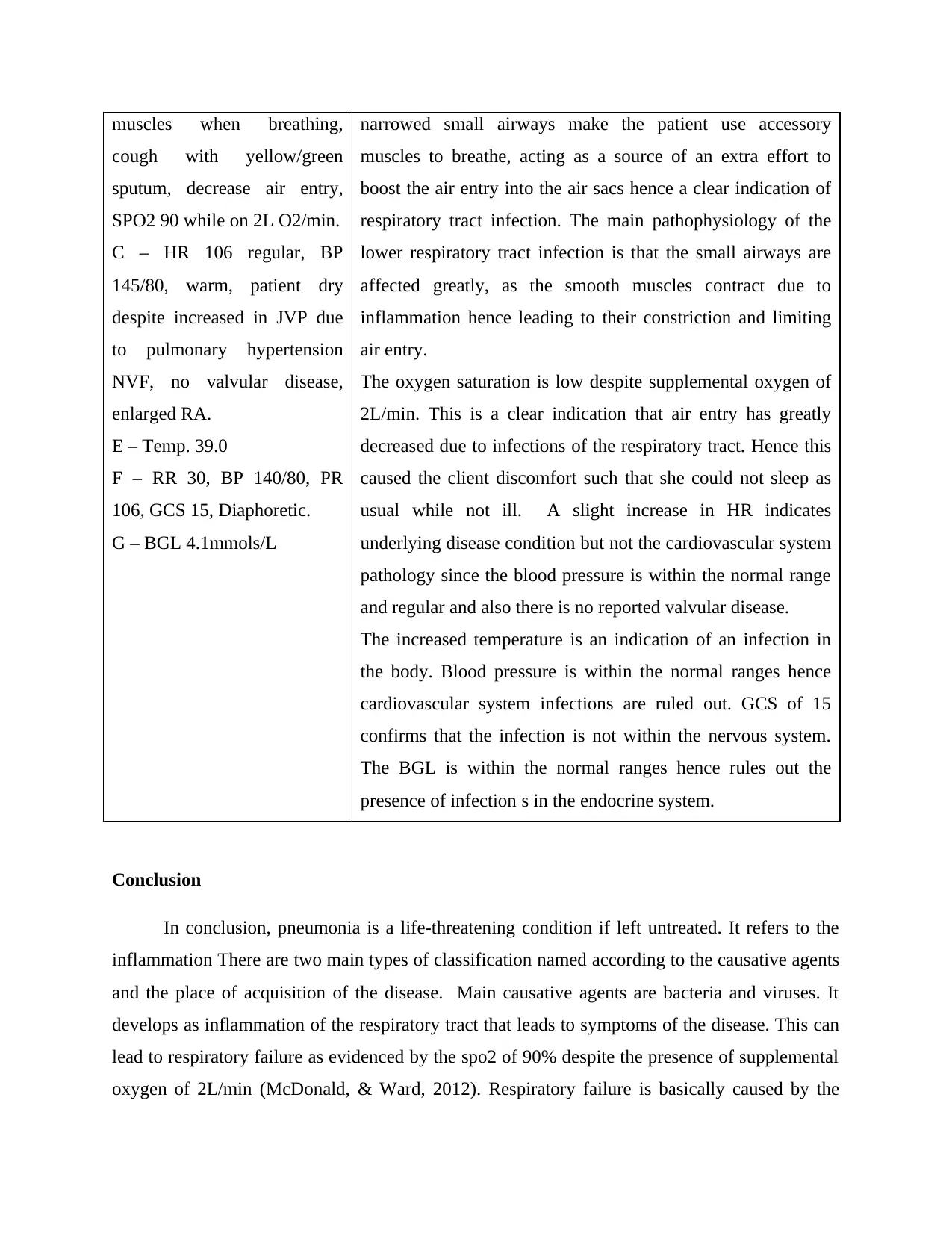
muscles when breathing,
cough with yellow/green
sputum, decrease air entry,
SPO2 90 while on 2L O2/min.
C – HR 106 regular, BP
145/80, warm, patient dry
despite increased in JVP due
to pulmonary hypertension
NVF, no valvular disease,
enlarged RA.
E – Temp. 39.0
F – RR 30, BP 140/80, PR
106, GCS 15, Diaphoretic.
G – BGL 4.1mmols/L
narrowed small airways make the patient use accessory
muscles to breathe, acting as a source of an extra effort to
boost the air entry into the air sacs hence a clear indication of
respiratory tract infection. The main pathophysiology of the
lower respiratory tract infection is that the small airways are
affected greatly, as the smooth muscles contract due to
inflammation hence leading to their constriction and limiting
air entry.
The oxygen saturation is low despite supplemental oxygen of
2L/min. This is a clear indication that air entry has greatly
decreased due to infections of the respiratory tract. Hence this
caused the client discomfort such that she could not sleep as
usual while not ill. A slight increase in HR indicates
underlying disease condition but not the cardiovascular system
pathology since the blood pressure is within the normal range
and regular and also there is no reported valvular disease.
The increased temperature is an indication of an infection in
the body. Blood pressure is within the normal ranges hence
cardiovascular system infections are ruled out. GCS of 15
confirms that the infection is not within the nervous system.
The BGL is within the normal ranges hence rules out the
presence of infection s in the endocrine system.
Conclusion
In conclusion, pneumonia is a life-threatening condition if left untreated. It refers to the
inflammation There are two main types of classification named according to the causative agents
and the place of acquisition of the disease. Main causative agents are bacteria and viruses. It
develops as inflammation of the respiratory tract that leads to symptoms of the disease. This can
lead to respiratory failure as evidenced by the spo2 of 90% despite the presence of supplemental
oxygen of 2L/min (McDonald, & Ward, 2012). Respiratory failure is basically caused by the
cough with yellow/green
sputum, decrease air entry,
SPO2 90 while on 2L O2/min.
C – HR 106 regular, BP
145/80, warm, patient dry
despite increased in JVP due
to pulmonary hypertension
NVF, no valvular disease,
enlarged RA.
E – Temp. 39.0
F – RR 30, BP 140/80, PR
106, GCS 15, Diaphoretic.
G – BGL 4.1mmols/L
narrowed small airways make the patient use accessory
muscles to breathe, acting as a source of an extra effort to
boost the air entry into the air sacs hence a clear indication of
respiratory tract infection. The main pathophysiology of the
lower respiratory tract infection is that the small airways are
affected greatly, as the smooth muscles contract due to
inflammation hence leading to their constriction and limiting
air entry.
The oxygen saturation is low despite supplemental oxygen of
2L/min. This is a clear indication that air entry has greatly
decreased due to infections of the respiratory tract. Hence this
caused the client discomfort such that she could not sleep as
usual while not ill. A slight increase in HR indicates
underlying disease condition but not the cardiovascular system
pathology since the blood pressure is within the normal range
and regular and also there is no reported valvular disease.
The increased temperature is an indication of an infection in
the body. Blood pressure is within the normal ranges hence
cardiovascular system infections are ruled out. GCS of 15
confirms that the infection is not within the nervous system.
The BGL is within the normal ranges hence rules out the
presence of infection s in the endocrine system.
Conclusion
In conclusion, pneumonia is a life-threatening condition if left untreated. It refers to the
inflammation There are two main types of classification named according to the causative agents
and the place of acquisition of the disease. Main causative agents are bacteria and viruses. It
develops as inflammation of the respiratory tract that leads to symptoms of the disease. This can
lead to respiratory failure as evidenced by the spo2 of 90% despite the presence of supplemental
oxygen of 2L/min (McDonald, & Ward, 2012). Respiratory failure is basically caused by the
mechanical changes in the lungs resulting from pneumonia. Alveoli secretions fill the alveoli at
slightly lower than their normal functional capacity leading to loss of volume almost
proportional to the extent of the pulmonary infiltrate. There is also evidence that the dynamic
compliance of the remaining ventilated lungs is decreased in pneumococcal pneumonia possibly
by a reduction in surfactant activity hence leading to more increase in the work of breathing.
Signs and symptoms of the disease manifest differently as according to the causative agents. The
main symptoms are; fevers, a cough that is productive, difficulty in breathing, shortness of
breath, increased respiratory rate, feeling exhausted and chills. Objective data should include
visible obvious respiratory distress. On auscultation, there is the presence of coarse crackles in
the lungs. The main laboratory investigation to be done is the ASOT test to confirm the presence
of the Streptococcus species in the cultured specimen. Another investigation is the chest x-ray to
confirm the pathophysiological changes in the alveoli. Complications of bacterial pneumonia
include; bacteremia leading to septic shock, lung abscesses, acute respiratory distress syndrome,
pleural effusion, and even death. The main route of transmission of bacterial pneumonia
infections is by air droplets (Hawker, et.al, 2018). Hence it can be prevented by vaccination,
avoiding smoking and maintaining a high level of hygiene.
Academic honesty policy
This work has never been done before by any other student and therefore not a recycling of
the already work done. The plagiarism level is within the accepted level as it has been passed
through a plagiarism checker. I have personally done and research the work as adequately as per
the academic honestly policy 2015 Sidney University. I have not engaged any of my classmates
in the doing of this assignment nor paid for anyone to do the assignment on my behalf. Also, this
work has been personally researched by use of several books sources, journals, and therefore was
never copied from any student whatsoever. Also, this work was not done collaboratively.
Furthermore, no one was asked to complete the assignment as I surely did myself to the end.
Concerning plagiarism levels, plagiarism means presenting another person’s work as one’s own
work by presenting, copying or reproducing it without appropriate acknowledgment of the
source. The policy states that Plagiarism is unacceptable in academic work, even where it is not
intended to deceive the examiner into believing that the work is original to the student, but
instead arises from, for example, poor referencing; error; inability to paraphrase; or inhibition
slightly lower than their normal functional capacity leading to loss of volume almost
proportional to the extent of the pulmonary infiltrate. There is also evidence that the dynamic
compliance of the remaining ventilated lungs is decreased in pneumococcal pneumonia possibly
by a reduction in surfactant activity hence leading to more increase in the work of breathing.
Signs and symptoms of the disease manifest differently as according to the causative agents. The
main symptoms are; fevers, a cough that is productive, difficulty in breathing, shortness of
breath, increased respiratory rate, feeling exhausted and chills. Objective data should include
visible obvious respiratory distress. On auscultation, there is the presence of coarse crackles in
the lungs. The main laboratory investigation to be done is the ASOT test to confirm the presence
of the Streptococcus species in the cultured specimen. Another investigation is the chest x-ray to
confirm the pathophysiological changes in the alveoli. Complications of bacterial pneumonia
include; bacteremia leading to septic shock, lung abscesses, acute respiratory distress syndrome,
pleural effusion, and even death. The main route of transmission of bacterial pneumonia
infections is by air droplets (Hawker, et.al, 2018). Hence it can be prevented by vaccination,
avoiding smoking and maintaining a high level of hygiene.
Academic honesty policy
This work has never been done before by any other student and therefore not a recycling of
the already work done. The plagiarism level is within the accepted level as it has been passed
through a plagiarism checker. I have personally done and research the work as adequately as per
the academic honestly policy 2015 Sidney University. I have not engaged any of my classmates
in the doing of this assignment nor paid for anyone to do the assignment on my behalf. Also, this
work has been personally researched by use of several books sources, journals, and therefore was
never copied from any student whatsoever. Also, this work was not done collaboratively.
Furthermore, no one was asked to complete the assignment as I surely did myself to the end.
Concerning plagiarism levels, plagiarism means presenting another person’s work as one’s own
work by presenting, copying or reproducing it without appropriate acknowledgment of the
source. The policy states that Plagiarism is unacceptable in academic work, even where it is not
intended to deceive the examiner into believing that the work is original to the student, but
instead arises from, for example, poor referencing; error; inability to paraphrase; or inhibition
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

about writing in the student’s own words. Therefore, I confidently report that this work is
absolutely free of plagiarism since it complies with the academic honesty policy of the
University of Sidney, concerning plagiarism.
absolutely free of plagiarism since it complies with the academic honesty policy of the
University of Sidney, concerning plagiarism.
Bibliography
Barbier, F., Andremont, A., Wolff, M., & Bouadma, L. (2013). Hospital-acquired pneumonia
and ventilator-associated pneumonia: recent advances in epidemiology and
management. Current opinion in pulmonary medicine, 19(3), 216-228.
Craig, J. C., Williams, G. J., Jones, M., Codarini, M., Macaskill, P., Hayen, A., ... & McCaskill,
M. (2010). The accuracy of clinical symptoms and signs for the diagnosis of serious
bacterial infection in young febrile children: prospective cohort study of 15 781 febrile
illnesses. Bmj, 340, c1594.
Deranek, J., & Parnther, C. (2015). Academic honesty and the new technological frontier. The
Hilltop Review, 8(1), 4.
Fairbrother, R. W., & Taylor, G. A. (2014). A Text-book of Bacteriology. Butterworth-
Heinemann.
Hawker, J., Begg, N., Reintjes, R., Ekdahl, K., Edeghere, O., & Van Steenbergen, J. E.
(2018). Communicable disease control and health protection handbook. John Wiley &
Sons.
Huijskens, E. G., van Erkel, A. J., Palmen, F. M., Buiting, A. G., Kluytmans, J. A., & Rossen, J.
W. (2013). Viral and bacterial aetiology of community‐acquired pneumonia in
adults. Influenza and other respiratory viruses, 7(4), 567-573.
José, R. J., Periselneris, J. N., & Brown, J. S. (2015). Community-acquired pneumonia. Current
opinion in pulmonary medicine, 21(3), 212-218.
McDonald, C., & Ward, J. (2012). Oxygen and airflow. Supportive Care in Respiratory Disease,
123.
Weinberger, S. E., Cockrill, B. A., & Mandel, J. (2017). Principles of Pulmonary Medicine E-
Book. Elsevier Health Sciences.
Barbier, F., Andremont, A., Wolff, M., & Bouadma, L. (2013). Hospital-acquired pneumonia
and ventilator-associated pneumonia: recent advances in epidemiology and
management. Current opinion in pulmonary medicine, 19(3), 216-228.
Craig, J. C., Williams, G. J., Jones, M., Codarini, M., Macaskill, P., Hayen, A., ... & McCaskill,
M. (2010). The accuracy of clinical symptoms and signs for the diagnosis of serious
bacterial infection in young febrile children: prospective cohort study of 15 781 febrile
illnesses. Bmj, 340, c1594.
Deranek, J., & Parnther, C. (2015). Academic honesty and the new technological frontier. The
Hilltop Review, 8(1), 4.
Fairbrother, R. W., & Taylor, G. A. (2014). A Text-book of Bacteriology. Butterworth-
Heinemann.
Hawker, J., Begg, N., Reintjes, R., Ekdahl, K., Edeghere, O., & Van Steenbergen, J. E.
(2018). Communicable disease control and health protection handbook. John Wiley &
Sons.
Huijskens, E. G., van Erkel, A. J., Palmen, F. M., Buiting, A. G., Kluytmans, J. A., & Rossen, J.
W. (2013). Viral and bacterial aetiology of community‐acquired pneumonia in
adults. Influenza and other respiratory viruses, 7(4), 567-573.
José, R. J., Periselneris, J. N., & Brown, J. S. (2015). Community-acquired pneumonia. Current
opinion in pulmonary medicine, 21(3), 212-218.
McDonald, C., & Ward, J. (2012). Oxygen and airflow. Supportive Care in Respiratory Disease,
123.
Weinberger, S. E., Cockrill, B. A., & Mandel, J. (2017). Principles of Pulmonary Medicine E-
Book. Elsevier Health Sciences.
Winland-Brown, J. E., & Klause, K. T. (2017). Respiratory problems. Family practice and adult-
gerontology primary care nurse practitioner certification examination review questions
and strategies, 239.
Wojsyk-Banaszak, I., & Bręborowicz, A. (2013). Pneumonia in children. In Respiratory Disease
and Infection-A New Insight. IntechOpen.
gerontology primary care nurse practitioner certification examination review questions
and strategies, 239.
Wojsyk-Banaszak, I., & Bręborowicz, A. (2013). Pneumonia in children. In Respiratory Disease
and Infection-A New Insight. IntechOpen.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.