Parkinson's Disease and Dopamine Agonist: A Detailed Analysis
VerifiedAdded on 2022/08/23
|11
|2625
|17
Report
AI Summary
This report provides a comprehensive overview of Parkinson's Disease (PD), a neurodegenerative disorder characterized by motor and non-motor symptoms. It discusses the disease's pathophysiology, including the degeneration of dopamine-producing neurons in the substantia nigra and the accumulation of neurofibrillary tangles. The report delves into the primary and secondary motor symptoms, such as tremor, rigidity, bradykinesia, and balance issues. It also explores the role of dopamine agonists, like Ropinirole, in managing PD by mimicking the effects of dopamine and binding to dopamine receptors. The report covers the pharmacology of Ropinirole, its mechanism of action, and its advantages in treating PD. The conclusion emphasizes the importance of dopamine agonists in mitigating PD symptoms and the need for further research to develop more effective treatments.

Running head: PARKINSON’S DISEASE AND DOPAMINE AGONIST
Parkinson’s disease and Dopamine Agonist
Name of the Student
Name of the University
Author Note
Parkinson’s disease and Dopamine Agonist
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1PARKINSON’S DISEASE AND DOPAMINE AGONIST
Abstract
Introduction
The cases of Parkinson’s disease are enhancing 1 per 100 populations among the age group
of 60 years or more. Parkinson’s disease is a brain disorder that is characterized by the
presence of shaking, altered balance, stiffness, difficulty in walking. The patient may
experience mental and behavioural changes, sleeping problems, fatigue, depression,
difficulties in memory as well. This section is designed for the peers of the neurology wards
of the hospital care setting.
Discussion
The disease is characterized by primary motor symptoms and secondary motor symptoms.
The patients may experience shaking of hands, legs, arms, tongue, lips, jaws, rigidity of
muscles, joint pains and muscles. Moreover, cases of bradykinesia are also reported and as a
part of this, problems like reduced facial expression, lower rate of eye blinking, reduction in
the quality of hand writing due to shaky hand are observed. . Among the secondary motor
symptoms the main features are tendency to bend forward, impaired gross and fine motor
responses, dystonia, fatigue, akathisia, cramping, sexual dysfunction, drooling and problem
in chewing and swallowing of the foods. The main reason of this disease is associated with
the destruction of DA-neurons of SNpc and along with this accumulation of tau protein or
neurofibrillary tangles (NFT) can also promote onset of the disease. For managing the disease
condition, dopamine agonist such as Ropinirole can be used.
Abstract
Introduction
The cases of Parkinson’s disease are enhancing 1 per 100 populations among the age group
of 60 years or more. Parkinson’s disease is a brain disorder that is characterized by the
presence of shaking, altered balance, stiffness, difficulty in walking. The patient may
experience mental and behavioural changes, sleeping problems, fatigue, depression,
difficulties in memory as well. This section is designed for the peers of the neurology wards
of the hospital care setting.
Discussion
The disease is characterized by primary motor symptoms and secondary motor symptoms.
The patients may experience shaking of hands, legs, arms, tongue, lips, jaws, rigidity of
muscles, joint pains and muscles. Moreover, cases of bradykinesia are also reported and as a
part of this, problems like reduced facial expression, lower rate of eye blinking, reduction in
the quality of hand writing due to shaky hand are observed. . Among the secondary motor
symptoms the main features are tendency to bend forward, impaired gross and fine motor
responses, dystonia, fatigue, akathisia, cramping, sexual dysfunction, drooling and problem
in chewing and swallowing of the foods. The main reason of this disease is associated with
the destruction of DA-neurons of SNpc and along with this accumulation of tau protein or
neurofibrillary tangles (NFT) can also promote onset of the disease. For managing the disease
condition, dopamine agonist such as Ropinirole can be used.
2PARKINSON’S DISEASE AND DOPAMINE AGONIST
Conclusion
Therefore, it can be concluded that the low level of dopamine in PD is due to DA neuron
degeneration and accumulation of NFT. In order to prevent this dopamine agonists can be
prescribed.
Conclusion
Therefore, it can be concluded that the low level of dopamine in PD is due to DA neuron
degeneration and accumulation of NFT. In order to prevent this dopamine agonists can be
prescribed.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3PARKINSON’S DISEASE AND DOPAMINE AGONIST
Introduction
Around the world, a huge number of patients are suffering from a neurological
disorder named Parkinson’s disease and in case of Australia the condition is not all different.
In this context, it is very crucial to mention the fact that almost 4 out of 1000 people in
Australia are suffering from this disease condition. Along with this, it is also reported that the
cases of Parkinson’s disease are enhancing 1 per 100 populations among the age group of 60
years or more. Therefore, almost 80,000 people in the country is living with this problem and
only one out of five disease cases are diagnosed before the age of 50 years
(Betterhealth.vic.gov.au, 2020).
What is Parkinson’s Disease
As per the information of National Institute on Aging, it can be stated that the
Parkinson’s disease is a brain disorder that is characterized by the presence of shaking,
altered balance, stiffness, difficulty in walking. Therefore, it is observed that along with the
advancement of time, the symptoms and condition of the disease generally get worse.
Moreover, along with the progression of the disease, the patient may experience mental and
behavioural changes, sleeping problems, fatigue, depression, difficulties in memory as well.
According to the study of Kouli, Torsney and Kuan (2018), it is stated that, the disease
affects both men and women; however, men are more affected by this disease condition than
that of a women. The study also stated that the advancement of age is a major risk factor for
developing this disease condition.
Physiology of Parkinson’s disease
While discussing about the physiology of PD, it can be stated that the disease is
characterized by a few features and they can be divided into two categories- primary motor
Introduction
Around the world, a huge number of patients are suffering from a neurological
disorder named Parkinson’s disease and in case of Australia the condition is not all different.
In this context, it is very crucial to mention the fact that almost 4 out of 1000 people in
Australia are suffering from this disease condition. Along with this, it is also reported that the
cases of Parkinson’s disease are enhancing 1 per 100 populations among the age group of 60
years or more. Therefore, almost 80,000 people in the country is living with this problem and
only one out of five disease cases are diagnosed before the age of 50 years
(Betterhealth.vic.gov.au, 2020).
What is Parkinson’s Disease
As per the information of National Institute on Aging, it can be stated that the
Parkinson’s disease is a brain disorder that is characterized by the presence of shaking,
altered balance, stiffness, difficulty in walking. Therefore, it is observed that along with the
advancement of time, the symptoms and condition of the disease generally get worse.
Moreover, along with the progression of the disease, the patient may experience mental and
behavioural changes, sleeping problems, fatigue, depression, difficulties in memory as well.
According to the study of Kouli, Torsney and Kuan (2018), it is stated that, the disease
affects both men and women; however, men are more affected by this disease condition than
that of a women. The study also stated that the advancement of age is a major risk factor for
developing this disease condition.
Physiology of Parkinson’s disease
While discussing about the physiology of PD, it can be stated that the disease is
characterized by a few features and they can be divided into two categories- primary motor
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4PARKINSON’S DISEASE AND DOPAMINE AGONIST
symptoms and secondary motor symptoms. As a part of the primary motor symptoms the
patients of PD may experience resting tremor that is shaking of hands, legs, arms, tongue,
lips, jaws and it is observed that almost 70 per cent of the individuals experience the issue of
resting tremor as a part of their PD. Another feature of this primary motor symptom is
rigidity that is enhancement of the tonicity or stiffness of the muscles (Maiti, Manna &
Dunbar, 2017). According to the study findings of Kouli, Torsney and Kuan (2018), it is
stated that the patients may feel weakness or pain in their muscles and as a consequence of
this the patient may feel joint pain as well. The study findings of Samà et al. (2017), reported
the problem of bradykinesia among the PD patients that is loss of spontaneous movements of
the body and this problem is characterized by the problems like reduced facial expression,
lower rate of eye blinking, reduction in the quality of hand writing due to shaky hands,
stopping of movements suddenly. The problem of coordination and balance is also associated
with the problem of PD among the patients. Among the secondary motor symptoms the main
features are tendency to bend forward, impaired gross and fine motor responses, dystonia,
fatigue, akathisia, cramping, sexual dysfunction, drooling and problem in chewing and
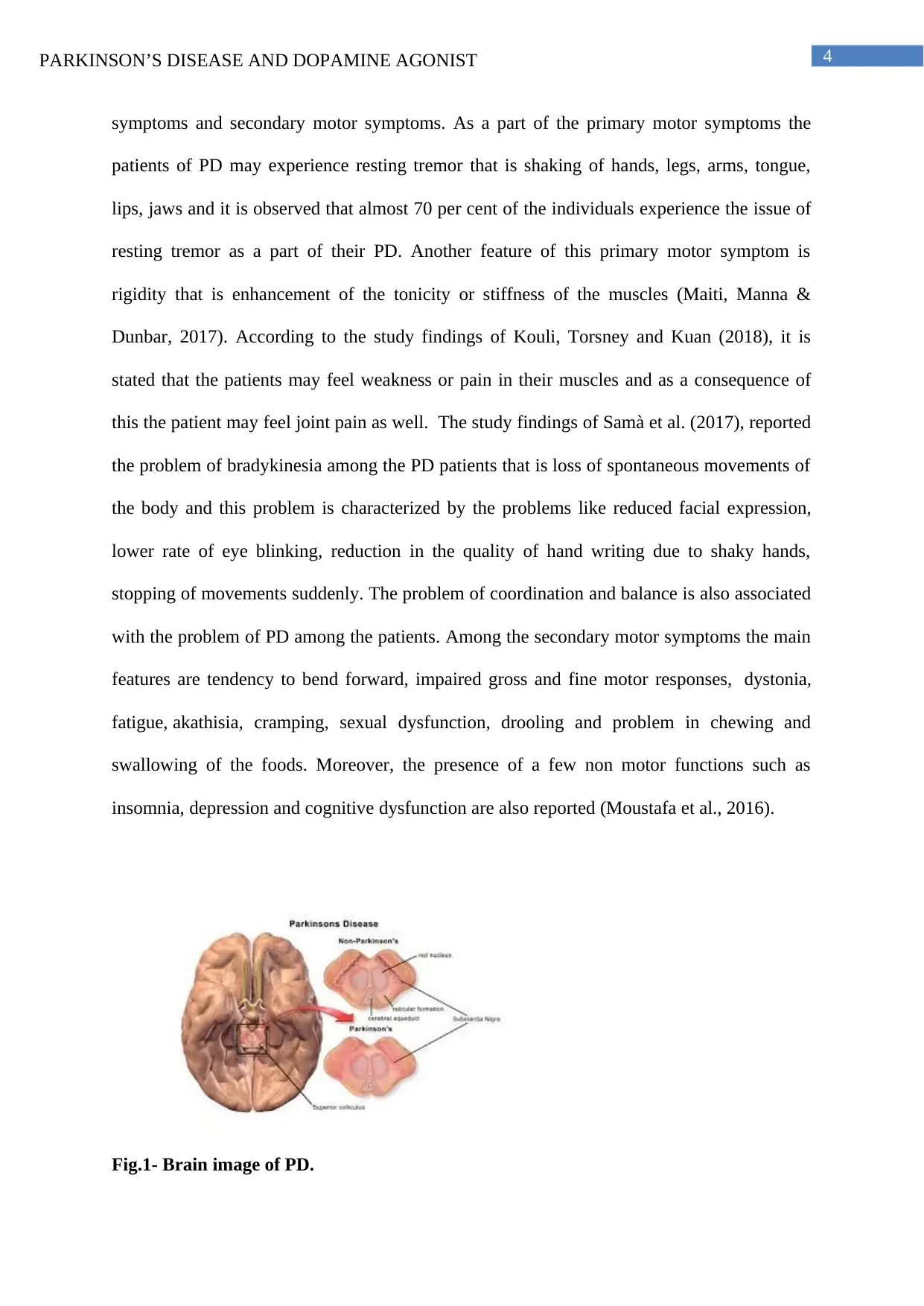
swallowing of the foods. Moreover, the presence of a few non motor functions such as
insomnia, depression and cognitive dysfunction are also reported (Moustafa et al., 2016).
Fig.1- Brain image of PD.
symptoms and secondary motor symptoms. As a part of the primary motor symptoms the
patients of PD may experience resting tremor that is shaking of hands, legs, arms, tongue,
lips, jaws and it is observed that almost 70 per cent of the individuals experience the issue of
resting tremor as a part of their PD. Another feature of this primary motor symptom is
rigidity that is enhancement of the tonicity or stiffness of the muscles (Maiti, Manna &
Dunbar, 2017). According to the study findings of Kouli, Torsney and Kuan (2018), it is
stated that the patients may feel weakness or pain in their muscles and as a consequence of
this the patient may feel joint pain as well. The study findings of Samà et al. (2017), reported
the problem of bradykinesia among the PD patients that is loss of spontaneous movements of
the body and this problem is characterized by the problems like reduced facial expression,
lower rate of eye blinking, reduction in the quality of hand writing due to shaky hands,
stopping of movements suddenly. The problem of coordination and balance is also associated
with the problem of PD among the patients. Among the secondary motor symptoms the main
features are tendency to bend forward, impaired gross and fine motor responses, dystonia,
fatigue, akathisia, cramping, sexual dysfunction, drooling and problem in chewing and
swallowing of the foods. Moreover, the presence of a few non motor functions such as
insomnia, depression and cognitive dysfunction are also reported (Moustafa et al., 2016).
Fig.1- Brain image of PD.
5PARKINSON’S DISEASE AND DOPAMINE AGONIST
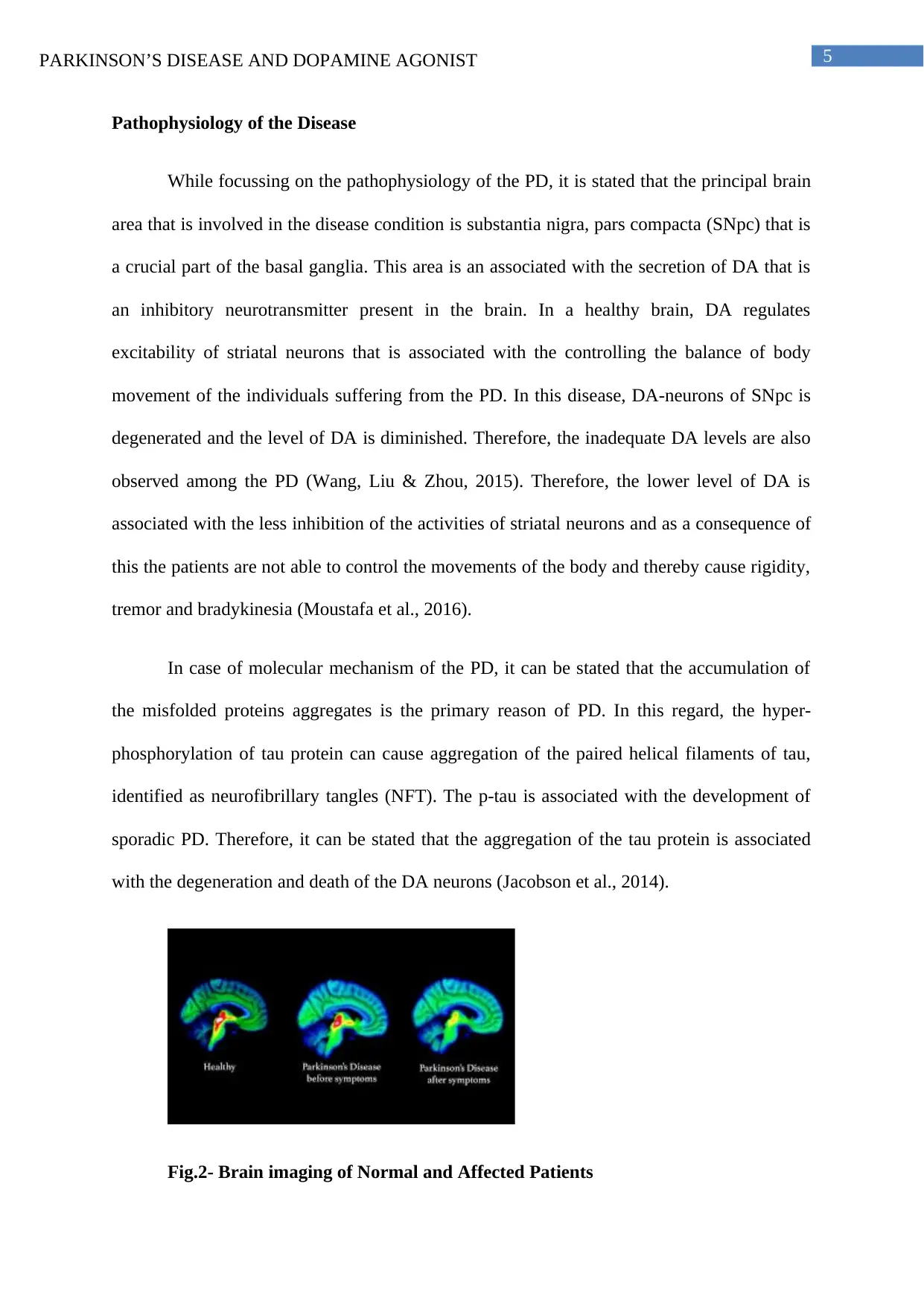
Pathophysiology of the Disease
While focussing on the pathophysiology of the PD, it is stated that the principal brain
area that is involved in the disease condition is substantia nigra, pars compacta (SNpc) that is
a crucial part of the basal ganglia. This area is an associated with the secretion of DA that is
an inhibitory neurotransmitter present in the brain. In a healthy brain, DA regulates
excitability of striatal neurons that is associated with the controlling the balance of body
movement of the individuals suffering from the PD. In this disease, DA-neurons of SNpc is
degenerated and the level of DA is diminished. Therefore, the inadequate DA levels are also
observed among the PD (Wang, Liu & Zhou, 2015). Therefore, the lower level of DA is
associated with the less inhibition of the activities of striatal neurons and as a consequence of
this the patients are not able to control the movements of the body and thereby cause rigidity,
tremor and bradykinesia (Moustafa et al., 2016).
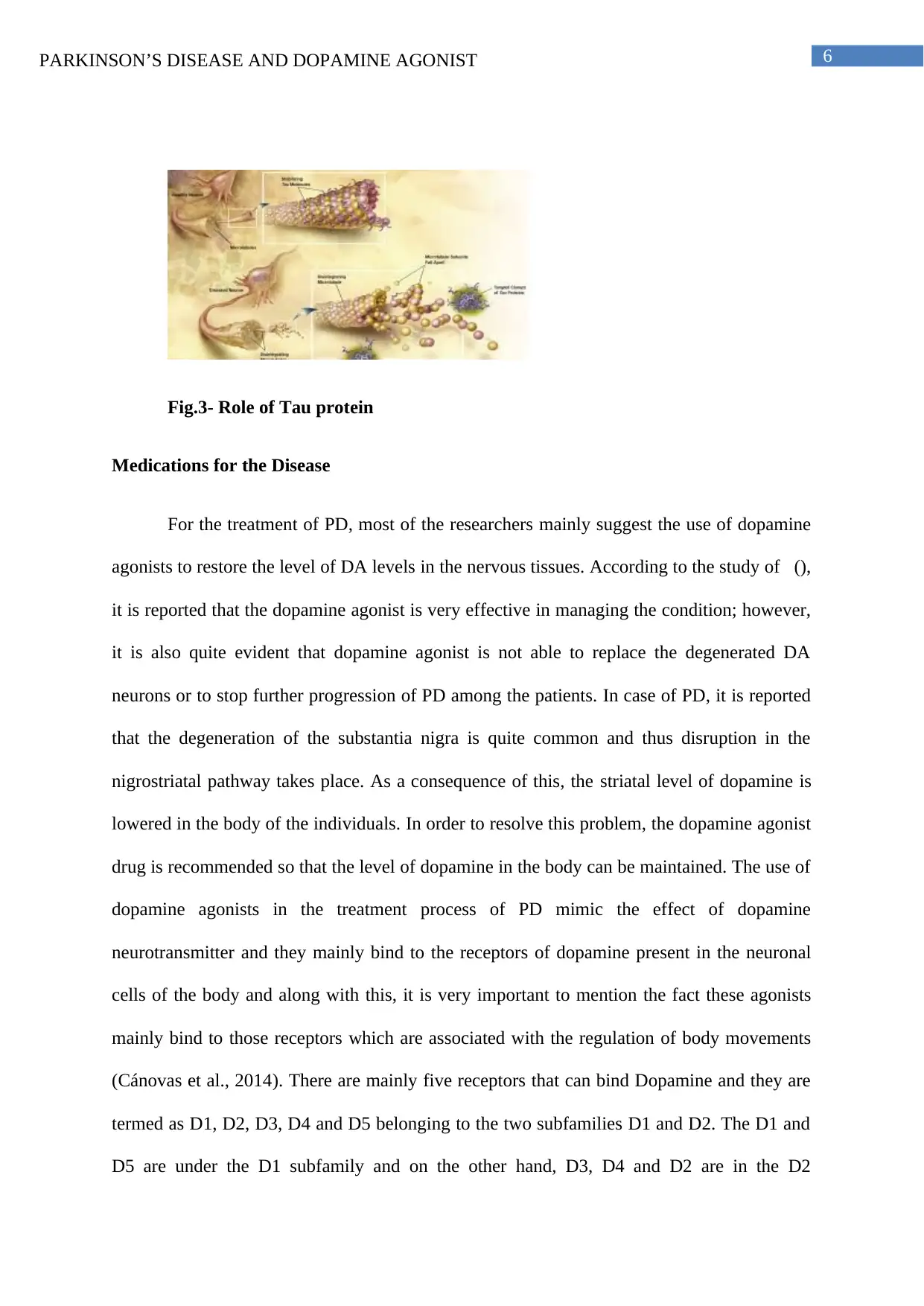
In case of molecular mechanism of the PD, it can be stated that the accumulation of
the misfolded proteins aggregates is the primary reason of PD. In this regard, the hyper-
phosphorylation of tau protein can cause aggregation of the paired helical filaments of tau,
identified as neurofibrillary tangles (NFT). The p-tau is associated with the development of
sporadic PD. Therefore, it can be stated that the aggregation of the tau protein is associated
with the degeneration and death of the DA neurons (Jacobson et al., 2014).
Fig.2- Brain imaging of Normal and Affected Patients
Pathophysiology of the Disease
While focussing on the pathophysiology of the PD, it is stated that the principal brain
area that is involved in the disease condition is substantia nigra, pars compacta (SNpc) that is
a crucial part of the basal ganglia. This area is an associated with the secretion of DA that is
an inhibitory neurotransmitter present in the brain. In a healthy brain, DA regulates
excitability of striatal neurons that is associated with the controlling the balance of body
movement of the individuals suffering from the PD. In this disease, DA-neurons of SNpc is
degenerated and the level of DA is diminished. Therefore, the inadequate DA levels are also
observed among the PD (Wang, Liu & Zhou, 2015). Therefore, the lower level of DA is
associated with the less inhibition of the activities of striatal neurons and as a consequence of
this the patients are not able to control the movements of the body and thereby cause rigidity,
tremor and bradykinesia (Moustafa et al., 2016).
In case of molecular mechanism of the PD, it can be stated that the accumulation of
the misfolded proteins aggregates is the primary reason of PD. In this regard, the hyper-
phosphorylation of tau protein can cause aggregation of the paired helical filaments of tau,
identified as neurofibrillary tangles (NFT). The p-tau is associated with the development of
sporadic PD. Therefore, it can be stated that the aggregation of the tau protein is associated
with the degeneration and death of the DA neurons (Jacobson et al., 2014).
Fig.2- Brain imaging of Normal and Affected Patients
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6PARKINSON’S DISEASE AND DOPAMINE AGONIST
Fig.3- Role of Tau protein
Medications for the Disease
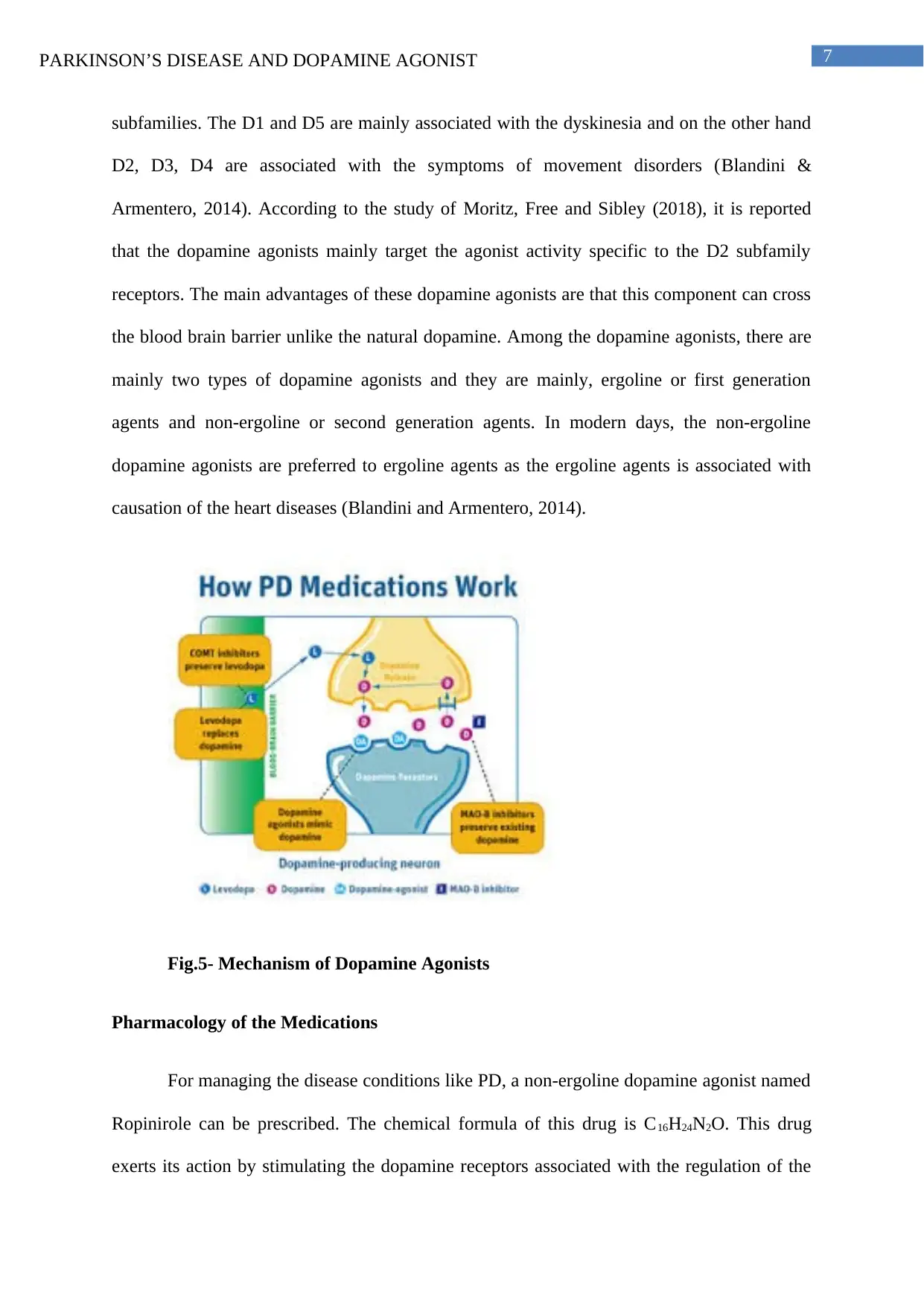
For the treatment of PD, most of the researchers mainly suggest the use of dopamine
agonists to restore the level of DA levels in the nervous tissues. According to the study of (),
it is reported that the dopamine agonist is very effective in managing the condition; however,
it is also quite evident that dopamine agonist is not able to replace the degenerated DA
neurons or to stop further progression of PD among the patients. In case of PD, it is reported
that the degeneration of the substantia nigra is quite common and thus disruption in the
nigrostriatal pathway takes place. As a consequence of this, the striatal level of dopamine is
lowered in the body of the individuals. In order to resolve this problem, the dopamine agonist
drug is recommended so that the level of dopamine in the body can be maintained. The use of
dopamine agonists in the treatment process of PD mimic the effect of dopamine
neurotransmitter and they mainly bind to the receptors of dopamine present in the neuronal
cells of the body and along with this, it is very important to mention the fact these agonists
mainly bind to those receptors which are associated with the regulation of body movements
(Cánovas et al., 2014). There are mainly five receptors that can bind Dopamine and they are
termed as D1, D2, D3, D4 and D5 belonging to the two subfamilies D1 and D2. The D1 and
D5 are under the D1 subfamily and on the other hand, D3, D4 and D2 are in the D2
Fig.3- Role of Tau protein
Medications for the Disease
For the treatment of PD, most of the researchers mainly suggest the use of dopamine
agonists to restore the level of DA levels in the nervous tissues. According to the study of (),
it is reported that the dopamine agonist is very effective in managing the condition; however,
it is also quite evident that dopamine agonist is not able to replace the degenerated DA
neurons or to stop further progression of PD among the patients. In case of PD, it is reported
that the degeneration of the substantia nigra is quite common and thus disruption in the
nigrostriatal pathway takes place. As a consequence of this, the striatal level of dopamine is
lowered in the body of the individuals. In order to resolve this problem, the dopamine agonist
drug is recommended so that the level of dopamine in the body can be maintained. The use of
dopamine agonists in the treatment process of PD mimic the effect of dopamine
neurotransmitter and they mainly bind to the receptors of dopamine present in the neuronal
cells of the body and along with this, it is very important to mention the fact these agonists
mainly bind to those receptors which are associated with the regulation of body movements
(Cánovas et al., 2014). There are mainly five receptors that can bind Dopamine and they are
termed as D1, D2, D3, D4 and D5 belonging to the two subfamilies D1 and D2. The D1 and
D5 are under the D1 subfamily and on the other hand, D3, D4 and D2 are in the D2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7PARKINSON’S DISEASE AND DOPAMINE AGONIST
subfamilies. The D1 and D5 are mainly associated with the dyskinesia and on the other hand
D2, D3, D4 are associated with the symptoms of movement disorders (Blandini &
Armentero, 2014). According to the study of Moritz, Free and Sibley (2018), it is reported
that the dopamine agonists mainly target the agonist activity specific to the D2 subfamily
receptors. The main advantages of these dopamine agonists are that this component can cross
the blood brain barrier unlike the natural dopamine. Among the dopamine agonists, there are
mainly two types of dopamine agonists and they are mainly, ergoline or first generation
agents and non-ergoline or second generation agents. In modern days, the non-ergoline
dopamine agonists are preferred to ergoline agents as the ergoline agents is associated with
causation of the heart diseases (Blandini and Armentero, 2014).
Fig.5- Mechanism of Dopamine Agonists
Pharmacology of the Medications
For managing the disease conditions like PD, a non-ergoline dopamine agonist named
Ropinirole can be prescribed. The chemical formula of this drug is C16H24N2O. This drug
exerts its action by stimulating the dopamine receptors associated with the regulation of the
subfamilies. The D1 and D5 are mainly associated with the dyskinesia and on the other hand
D2, D3, D4 are associated with the symptoms of movement disorders (Blandini &
Armentero, 2014). According to the study of Moritz, Free and Sibley (2018), it is reported
that the dopamine agonists mainly target the agonist activity specific to the D2 subfamily
receptors. The main advantages of these dopamine agonists are that this component can cross
the blood brain barrier unlike the natural dopamine. Among the dopamine agonists, there are
mainly two types of dopamine agonists and they are mainly, ergoline or first generation
agents and non-ergoline or second generation agents. In modern days, the non-ergoline
dopamine agonists are preferred to ergoline agents as the ergoline agents is associated with
causation of the heart diseases (Blandini and Armentero, 2014).
Fig.5- Mechanism of Dopamine Agonists
Pharmacology of the Medications
For managing the disease conditions like PD, a non-ergoline dopamine agonist named
Ropinirole can be prescribed. The chemical formula of this drug is C16H24N2O. This drug
exerts its action by stimulating the dopamine receptors associated with the regulation of the
8PARKINSON’S DISEASE AND DOPAMINE AGONIST
bodily movements. According to the information from the Drugbank, it is reported that the
Ropinirole shows highest affinity towards the D3 receptor which is present in high numbers
in the limbic areas of the brain and it is believed that they are responsible for exerting various
neuropsychiatric effects. Although the exact mechanism of action of Ropinirole is still not
very clear (Drugbank, 2020). Therefore, it is assumed that the action of this drug is exerted
through the selective stimulation of D2 receptors present in the caudate-putamen region in the
brain. It is believed that this system can affect the body movements and so positive
stimulation to that region can help in controlling the symptoms of PD. Along with this, it
should also be mentioned that this drug has almost no affinity to the D1 like receptor, α2
adrenoreceptors in the periphery GABA receptor and 5HT-1 receptor. Therefore, it should be
mentioned that this drug is associated with the onset of orthostatic hypotension. However, it
is stated that the overdose symptoms of this drug are mainly agitation, drowsiness, chest pain,
nausea, confusion, facial muscle movements, grogginess, vomiting and enhanced jerkiness of
movement. However, in a study conducting in rat showed that this drug can cause disruption
regarding the implantation of the embryo and it is believed that this effect may be due to the
prolactin-lowering effects of Ropinirole (Drugbank, 2020).
Conclusion
Hence, it can be concluded that, issue of PD is serious for the older adults and it
should be managed properly by the help of dopamine agonists. In this context, it can be stated
that the use of Ropinirole is very effective in treating the PD as it has more effective than that
of the first generation drugs.
bodily movements. According to the information from the Drugbank, it is reported that the
Ropinirole shows highest affinity towards the D3 receptor which is present in high numbers
in the limbic areas of the brain and it is believed that they are responsible for exerting various
neuropsychiatric effects. Although the exact mechanism of action of Ropinirole is still not
very clear (Drugbank, 2020). Therefore, it is assumed that the action of this drug is exerted
through the selective stimulation of D2 receptors present in the caudate-putamen region in the
brain. It is believed that this system can affect the body movements and so positive
stimulation to that region can help in controlling the symptoms of PD. Along with this, it
should also be mentioned that this drug has almost no affinity to the D1 like receptor, α2
adrenoreceptors in the periphery GABA receptor and 5HT-1 receptor. Therefore, it should be
mentioned that this drug is associated with the onset of orthostatic hypotension. However, it
is stated that the overdose symptoms of this drug are mainly agitation, drowsiness, chest pain,
nausea, confusion, facial muscle movements, grogginess, vomiting and enhanced jerkiness of
movement. However, in a study conducting in rat showed that this drug can cause disruption
regarding the implantation of the embryo and it is believed that this effect may be due to the
prolactin-lowering effects of Ropinirole (Drugbank, 2020).
Conclusion
Hence, it can be concluded that, issue of PD is serious for the older adults and it
should be managed properly by the help of dopamine agonists. In this context, it can be stated
that the use of Ropinirole is very effective in treating the PD as it has more effective than that
of the first generation drugs.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9PARKINSON’S DISEASE AND DOPAMINE AGONIST
References
Betterhealth.vic.gov.au (2020). Parkinson’s Disease. Betterhealth.vic.gov.au. Retrieved from-
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/parkinsons-disease
[Accessed on 29th March 2020]
Blandini, F., & Armentero, M. T. (2014). Dopamine receptor agonists for Parkinson's
disease. Expert opinion on investigational drugs, 23(3), 387-410.
Cánovas, A. A., Piudo, R. L., Ruiz-Espiga, P. G., Burguera, J. A., Arillo, V. C., Castro, A., ...
& Castrillo, J. M. (2014). Dopaminergic agonists in Parkinson's disease. Neurología
(English Edition), 29(4), 230-241.
Drugbank (2020). Ropinirole. Drugbank. Retrieved from-
https://www.drugbank.ca/drugs/DB00268#reference-A35711 [Accessed on 29th March
2020]
Jacobson, S. A., Morshed, T., Dugger, B. N., Beach, T. G., Hentz, J. G., Adler, C. H., ... &
Caviness, J. N. (2014). Plaques and tangles as well as Lewy-type alpha synucleinopathy
are associated with formed visual hallucinations. Parkinsonism & related
disorders, 20(9), 1009-1014.
Kouli, A., Torsney, K. M., & Kuan, W. L. (2018). Parkinson’s disease: etiology,
neuropathology, and pathogenesis. In Parkinson’s Disease: Pathogenesis and Clinical
Aspects [Internet]. Codon Publications.
Maiti, P., Manna, J., & Dunbar, G. L. (2017). Current understanding of the molecular
mechanisms in Parkinson's disease: targets for potential treatments. Translational
neurodegeneration, 6(1), 28.
References
Betterhealth.vic.gov.au (2020). Parkinson’s Disease. Betterhealth.vic.gov.au. Retrieved from-
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/parkinsons-disease
[Accessed on 29th March 2020]
Blandini, F., & Armentero, M. T. (2014). Dopamine receptor agonists for Parkinson's
disease. Expert opinion on investigational drugs, 23(3), 387-410.
Cánovas, A. A., Piudo, R. L., Ruiz-Espiga, P. G., Burguera, J. A., Arillo, V. C., Castro, A., ...
& Castrillo, J. M. (2014). Dopaminergic agonists in Parkinson's disease. Neurología
(English Edition), 29(4), 230-241.
Drugbank (2020). Ropinirole. Drugbank. Retrieved from-
https://www.drugbank.ca/drugs/DB00268#reference-A35711 [Accessed on 29th March
2020]
Jacobson, S. A., Morshed, T., Dugger, B. N., Beach, T. G., Hentz, J. G., Adler, C. H., ... &
Caviness, J. N. (2014). Plaques and tangles as well as Lewy-type alpha synucleinopathy
are associated with formed visual hallucinations. Parkinsonism & related
disorders, 20(9), 1009-1014.
Kouli, A., Torsney, K. M., & Kuan, W. L. (2018). Parkinson’s disease: etiology,
neuropathology, and pathogenesis. In Parkinson’s Disease: Pathogenesis and Clinical
Aspects [Internet]. Codon Publications.
Maiti, P., Manna, J., & Dunbar, G. L. (2017). Current understanding of the molecular
mechanisms in Parkinson's disease: targets for potential treatments. Translational
neurodegeneration, 6(1), 28.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10PARKINSON’S DISEASE AND DOPAMINE AGONIST
Moritz, A. E., Free, R. B., & Sibley, D. R. (2018). Advances and challenges in the search for
D2 and D3 dopamine receptor-selective compounds. Cellular signalling, 41, 75-81.
Moustafa, A. A., Chakravarthy, S., Phillips, J. R., Gupta, A., Keri, S., Polner, B., ... &
Jahanshahi, M. (2016). Motor symptoms in Parkinson’s disease: A unified
framework. Neuroscience & Biobehavioral Reviews, 68, 727-740.
National Institute on Ageing (2020). Parkinson’s Disease. Department of Health & Human
Service. Retrieved from- https://www.nia.nih.gov/health/parkinsons-disease [Accessed on
29th March 2020]
Samà, A., Pérez-López, C., Rodríguez-Martín, D., Català, A., Moreno-Aróstegui, J. M.,
Cabestany, J., ... & Rodríguez-Molinero, A. (2017). Estimating bradykinesia severity in
Parkinson's disease by analysing gait through a waist-worn sensor. Computers in biology
and medicine, 84, 114-123.
Wang, Q., Liu, Y., & Zhou, J. (2015). Neuroinflammation in Parkinson’s disease and its
potential as therapeutic target. Translational Neurodegeneration, 4(1), 19.
Moritz, A. E., Free, R. B., & Sibley, D. R. (2018). Advances and challenges in the search for
D2 and D3 dopamine receptor-selective compounds. Cellular signalling, 41, 75-81.
Moustafa, A. A., Chakravarthy, S., Phillips, J. R., Gupta, A., Keri, S., Polner, B., ... &
Jahanshahi, M. (2016). Motor symptoms in Parkinson’s disease: A unified
framework. Neuroscience & Biobehavioral Reviews, 68, 727-740.
National Institute on Ageing (2020). Parkinson’s Disease. Department of Health & Human
Service. Retrieved from- https://www.nia.nih.gov/health/parkinsons-disease [Accessed on
29th March 2020]
Samà, A., Pérez-López, C., Rodríguez-Martín, D., Català, A., Moreno-Aróstegui, J. M.,
Cabestany, J., ... & Rodríguez-Molinero, A. (2017). Estimating bradykinesia severity in
Parkinson's disease by analysing gait through a waist-worn sensor. Computers in biology
and medicine, 84, 114-123.
Wang, Q., Liu, Y., & Zhou, J. (2015). Neuroinflammation in Parkinson’s disease and its
potential as therapeutic target. Translational Neurodegeneration, 4(1), 19.
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.