Pathophysiology And Pharmacology - Case Study
VerifiedAdded on 2022/08/20
|16
|4661
|17
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Name of the Student:
Name of the University:
Author note:
PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Part 1: Pathophysiology
Upper Respiratory Tract Infection
From the given case study, one of the first observations which pave the way for
expounding upon the disease pathophysiology, is Benji’s recent preoccupation with an upper
respiratory tract infection. Upper respiratory tract infections (URTIs) are an acute form of
respiratory disorder which are characterized by both viral or bacterial infiltration and resultant
pathological transmission across the regions of the upper respiratory tract, mainly: the sinus, the
nose, the larynx or the pharynx (Aglipay et al., 2017). In the case of Benji, it is observed that he
has been diagnosed with URTI associated with bacterial etiology. Common bacterial strains
responsible for URTI pathophysiology, include: Streptococcus pyogenes, Staphylococcus
aureus, Haemophilus and Mycoplasma pneumoniae. Such bacterial strains generate URTI
disease pathophysiology via either the inhalation of droplets or via contact if droplets accumulate
upon the hands and the concerned individual uses the same to touch the nose or mouth (Gaarslev,
Yee, Chan, Fletcher-Lartey & Khan, 2016). Streptococcal sp. strains associated of the group A
type have been demonstrated to be transmitted via droplets in the surrounding coupled with
prolonged survival in environments which are dusty and dry (Lewnard et al., 2016). Considering
that Benji’s diagnosis and exacerbation of symptoms have been associated since the time he
caught a cold and specifically after playing soccer, thus demonstrating that the current URTI
pathogenesis is closely related to dust and infected droplet inhalation.
Childhood Asthma
Upon close examination of Benji’s current case presentation, it has been reported by his
mother that he received an asthma diagnosis during the 7 years of age. Childhood asthma is the
Part 1: Pathophysiology
Upper Respiratory Tract Infection
From the given case study, one of the first observations which pave the way for
expounding upon the disease pathophysiology, is Benji’s recent preoccupation with an upper
respiratory tract infection. Upper respiratory tract infections (URTIs) are an acute form of
respiratory disorder which are characterized by both viral or bacterial infiltration and resultant
pathological transmission across the regions of the upper respiratory tract, mainly: the sinus, the
nose, the larynx or the pharynx (Aglipay et al., 2017). In the case of Benji, it is observed that he
has been diagnosed with URTI associated with bacterial etiology. Common bacterial strains
responsible for URTI pathophysiology, include: Streptococcus pyogenes, Staphylococcus
aureus, Haemophilus and Mycoplasma pneumoniae. Such bacterial strains generate URTI
disease pathophysiology via either the inhalation of droplets or via contact if droplets accumulate
upon the hands and the concerned individual uses the same to touch the nose or mouth (Gaarslev,
Yee, Chan, Fletcher-Lartey & Khan, 2016). Streptococcal sp. strains associated of the group A
type have been demonstrated to be transmitted via droplets in the surrounding coupled with
prolonged survival in environments which are dusty and dry (Lewnard et al., 2016). Considering
that Benji’s diagnosis and exacerbation of symptoms have been associated since the time he
caught a cold and specifically after playing soccer, thus demonstrating that the current URTI
pathogenesis is closely related to dust and infected droplet inhalation.
Childhood Asthma
Upon close examination of Benji’s current case presentation, it has been reported by his
mother that he received an asthma diagnosis during the 7 years of age. Childhood asthma is the
2PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
name given to a chronic respiratory disorder associated with inflammatory mechanisms
contributing to an obstruction in the respiratory tract (King, James, Harkness & Wark, 2018).
Childhood asthmatic symptoms associated with the allergic type are largely contributed by
inhalation of common, potential allergens like pollen and dust – of which the latter seem to the
most relevant to Benji considering his symptom exacerbation in response to a cold, specifically
after playing soccer (McGeachie et al., 2016). The pathophysiology of atopic or allergic asthma
is facilitated by the inhalation of the above potential allergens which in turn, triggers the
asthmatic processes of pulmonary airway oedema, bronchoconstriction, airway remodelling and
airway hyper responsiveness across organs like the trachea, nasal passage, bronchial tree, lungs
and alveoli (Carpaij, Burgess, Kerstjens, Nawijn & van den Berge, 2019). Due to the inhalation
of allergens like dust by asthmatic children like Benji for a period of 2 hours or more, these
allergens are trapped by dendritic cells which in turn, facilitate antigen digestion in minute
particles followed by their transfer to the lamina propia. This facilitates the production of
immunoglobulin E (IgE) by plasma cells which in turn, causes bronchoconstriction, airway
narrowing and reduced air inhalation. This is due to the binding of IgE with smooth muscle cells
of the airways resulting in development of IgE muscle complex (King, Farrow & Chapman,
2019). Production of IgE characteristic of allergic asthma facilitates the production antigen
across the dendritic cells lining the upper respiratory tract which in turn paves the way for the
production of pro-inflammatory immunological cells like mast cell, eosinophil and lymphocyte
(Craft, Gordon, Huether, McCance & Brashers, 2015) – a key mechanism demonstrating
similarity to the URTI pathophysiology – Benji’s current symptomatic presentation and
associated fever. These cells, as a part of immunological defense response stimulate the
production of pro-inflammatory substances like interleukins and cytokines. Eosinophils
name given to a chronic respiratory disorder associated with inflammatory mechanisms
contributing to an obstruction in the respiratory tract (King, James, Harkness & Wark, 2018).
Childhood asthmatic symptoms associated with the allergic type are largely contributed by
inhalation of common, potential allergens like pollen and dust – of which the latter seem to the
most relevant to Benji considering his symptom exacerbation in response to a cold, specifically
after playing soccer (McGeachie et al., 2016). The pathophysiology of atopic or allergic asthma
is facilitated by the inhalation of the above potential allergens which in turn, triggers the
asthmatic processes of pulmonary airway oedema, bronchoconstriction, airway remodelling and
airway hyper responsiveness across organs like the trachea, nasal passage, bronchial tree, lungs
and alveoli (Carpaij, Burgess, Kerstjens, Nawijn & van den Berge, 2019). Due to the inhalation
of allergens like dust by asthmatic children like Benji for a period of 2 hours or more, these
allergens are trapped by dendritic cells which in turn, facilitate antigen digestion in minute
particles followed by their transfer to the lamina propia. This facilitates the production of
immunoglobulin E (IgE) by plasma cells which in turn, causes bronchoconstriction, airway
narrowing and reduced air inhalation. This is due to the binding of IgE with smooth muscle cells
of the airways resulting in development of IgE muscle complex (King, Farrow & Chapman,
2019). Production of IgE characteristic of allergic asthma facilitates the production antigen
across the dendritic cells lining the upper respiratory tract which in turn paves the way for the
production of pro-inflammatory immunological cells like mast cell, eosinophil and lymphocyte
(Craft, Gordon, Huether, McCance & Brashers, 2015) – a key mechanism demonstrating
similarity to the URTI pathophysiology – Benji’s current symptomatic presentation and
associated fever. These cells, as a part of immunological defense response stimulate the
production of pro-inflammatory substances like interleukins and cytokines. Eosinophils
3PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
specifically attack various sections of the lung to contribute to the secretion of leukotrienes and
resultant airway obstruction. This in turn contribute to secretion of pro-inflammatory bradykinin,
prostaglandins and histamines resulting in smooth muscle constriction and airway obstruction.
Asthma persisting for 12 to 24 hours facilitates interleukin-5 and eosinophil generation which
causes hyperplasia, thickness and vasodilation of airways resulting in mucous accumulation. The
accumulated mucous contributes to airway obstruction and airway epithelial damage (Pelaia et
al., 2019). Thus, the production of these substances, in turn contributes to respiratory tract
inflammation, excretion of mucosal exudate and possible edema and thus, progression of URTI
symptoms of bronchiole clogging, tightening and narrowing of the upper respiratory tract, and
resultant symptoms of wheezing coughing, fever and shortness of breath as observed in Benji
(Yamauchi & Ogasawara, 2019).
Part 2: Signs and Symptoms associated with Disease Pathophysiology
Fever
Upon entry, as evidenced by Regli, Becke and von Ungern-Sternberg (2017), the bacteria
strain undergoes invasion across the nasal mucosal lining and paves the way for destruction of
the lining of epithelial cells and resultant impairment of the ciliary functioning characteristic of
the sinuses present in the upper respiratory tract. The associated destruction facilitates the
immunological response comprising of pro-inflammatory cell funcionng such as lymphocytes,
macrophages and eosinophils which in turn, causes inflammation and redness of the upper
respiratory tract, increased internal temperatures as a consequence of the inflammatory response
and resultant fever – the first notable symptom which has been prevalently observed in Benji.
specifically attack various sections of the lung to contribute to the secretion of leukotrienes and
resultant airway obstruction. This in turn contribute to secretion of pro-inflammatory bradykinin,
prostaglandins and histamines resulting in smooth muscle constriction and airway obstruction.
Asthma persisting for 12 to 24 hours facilitates interleukin-5 and eosinophil generation which
causes hyperplasia, thickness and vasodilation of airways resulting in mucous accumulation. The
accumulated mucous contributes to airway obstruction and airway epithelial damage (Pelaia et
al., 2019). Thus, the production of these substances, in turn contributes to respiratory tract
inflammation, excretion of mucosal exudate and possible edema and thus, progression of URTI
symptoms of bronchiole clogging, tightening and narrowing of the upper respiratory tract, and
resultant symptoms of wheezing coughing, fever and shortness of breath as observed in Benji
(Yamauchi & Ogasawara, 2019).
Part 2: Signs and Symptoms associated with Disease Pathophysiology
Fever
Upon entry, as evidenced by Regli, Becke and von Ungern-Sternberg (2017), the bacteria
strain undergoes invasion across the nasal mucosal lining and paves the way for destruction of
the lining of epithelial cells and resultant impairment of the ciliary functioning characteristic of
the sinuses present in the upper respiratory tract. The associated destruction facilitates the
immunological response comprising of pro-inflammatory cell funcionng such as lymphocytes,
macrophages and eosinophils which in turn, causes inflammation and redness of the upper
respiratory tract, increased internal temperatures as a consequence of the inflammatory response
and resultant fever – the first notable symptom which has been prevalently observed in Benji.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Coughing and Wheezing
Additionally, such a pathogenic process contributes to excessive secretion of mucous,
impaired drainage of mucous and mucosal obstruction within the paranasal sinusal ostia. The
simultaneous prevalence of epithelial inflammation coupled with mucosal accumulation and
exudate secretion across sinuses contributes to narrowing of the upper respiratory tract and
mucosal clogging of the bronchi branches, gradually pave the way for blockage of the secondary
bronchus, tertiary bronchi and smaller airways or the bronchioles which ultimate are connected
to the pulmonary system via alveoli (Yuksel & Turkeli, 2017). Thus, the mucosal clogging of
bronchioles prompts coughing and wheezing, as a response to clear out mucous off the small
airways – which thus can be related well to the second notable symptoms of coughing and
wheezing demonstrated by Benji.
Shortness of Breath
Additionally, narrowing of bronchioles coupled with mucous and exudate accumulation
across the upper respiratory tract – which may often be associated with pulmonary edema due to
aggravation of inflammation - contributes to decreased air inhalation and resultant shortness of
breath - the third symptom of concern observed in Benji (Xu, Wischmeyer, Gonzalez &
Pichichero, 2017). It is thus evident, that the inflammatory response to URTI is the key
pathological mechanism responsible for contributing to Benji’s present symptoms of shortness of
breath, fever, and coughing and wheezing.
In the case of Benji, it can be observed that Benji’s history and exacerbation of asthma as
well as current URTI pathology is a resultant of a cold and possible inhalation of dust allergens
during soccer. Infections of the upper respiratory tract due to bacteria has been evidenced to be a
key causative factor underlying asthma exacerbation pathophysiology and one of the most
Coughing and Wheezing
Additionally, such a pathogenic process contributes to excessive secretion of mucous,
impaired drainage of mucous and mucosal obstruction within the paranasal sinusal ostia. The
simultaneous prevalence of epithelial inflammation coupled with mucosal accumulation and
exudate secretion across sinuses contributes to narrowing of the upper respiratory tract and
mucosal clogging of the bronchi branches, gradually pave the way for blockage of the secondary
bronchus, tertiary bronchi and smaller airways or the bronchioles which ultimate are connected
to the pulmonary system via alveoli (Yuksel & Turkeli, 2017). Thus, the mucosal clogging of
bronchioles prompts coughing and wheezing, as a response to clear out mucous off the small
airways – which thus can be related well to the second notable symptoms of coughing and
wheezing demonstrated by Benji.
Shortness of Breath
Additionally, narrowing of bronchioles coupled with mucous and exudate accumulation
across the upper respiratory tract – which may often be associated with pulmonary edema due to
aggravation of inflammation - contributes to decreased air inhalation and resultant shortness of
breath - the third symptom of concern observed in Benji (Xu, Wischmeyer, Gonzalez &
Pichichero, 2017). It is thus evident, that the inflammatory response to URTI is the key
pathological mechanism responsible for contributing to Benji’s present symptoms of shortness of
breath, fever, and coughing and wheezing.
In the case of Benji, it can be observed that Benji’s history and exacerbation of asthma as
well as current URTI pathology is a resultant of a cold and possible inhalation of dust allergens
during soccer. Infections of the upper respiratory tract due to bacteria has been evidenced to be a
key causative factor underlying asthma exacerbation pathophysiology and one of the most
5PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
prevalent causes of acute illness hospitalizations and school abstinence in school aged children
like Benji (Biezen et al., 2015). According to the cross sectional research conducted by Biezen et
al., (2015) published in the Medical Journal of Australia, approximately 6 million cases of
children cases of URTIs and asthma exacerbations are reported across general practitioner and
acute care units of Australia. Thus, Benji’s current aggravation of asthma symptoms may be a
result of URTI, considering that his asthma exacerbations have been found to relapse after
catching a cold and due to dust inhalation as a result of playing sport. Bacterial strain infiltration
within the upper respiratory tract demonstrates an inflammatory pathogenesis similar to asthma
comprising of a re-triggering of the immunological responses, the production of pro-
inflammatory substances and cells, inflammation of the respiratory tract and thus resultant
bronchiole narrowing, asthmatic exacerbation and symptoms of fever, wheezing and coughing
and shortness of breath (Depner et al., 2017). Thus, the simultaneous presence of URTI and
asthmatic pathologies can be observed and related to Benji’s case whose asthmatic symptoms of
fever, coughing, wheezing and fever and have presumably relapsed especially after encountering
a cold and after playing sport.
Pharmacology related to Case Patient
Salbutamol: ADME and Pharmacology
From the case study, one of medications given to Benji is Salbutamol. Salbutamol is a
selective agonist of beta 2 adrenergic receptor of the short acting type, which used prevalently
for the purpose of mitigating asthmatic symptoms specifically shortness of breath and
bronchoconstriction which have been presented by Benji. After being inhaled, Salbutamol is
prevalent causes of acute illness hospitalizations and school abstinence in school aged children
like Benji (Biezen et al., 2015). According to the cross sectional research conducted by Biezen et
al., (2015) published in the Medical Journal of Australia, approximately 6 million cases of
children cases of URTIs and asthma exacerbations are reported across general practitioner and
acute care units of Australia. Thus, Benji’s current aggravation of asthma symptoms may be a
result of URTI, considering that his asthma exacerbations have been found to relapse after
catching a cold and due to dust inhalation as a result of playing sport. Bacterial strain infiltration
within the upper respiratory tract demonstrates an inflammatory pathogenesis similar to asthma
comprising of a re-triggering of the immunological responses, the production of pro-
inflammatory substances and cells, inflammation of the respiratory tract and thus resultant
bronchiole narrowing, asthmatic exacerbation and symptoms of fever, wheezing and coughing
and shortness of breath (Depner et al., 2017). Thus, the simultaneous presence of URTI and
asthmatic pathologies can be observed and related to Benji’s case whose asthmatic symptoms of
fever, coughing, wheezing and fever and have presumably relapsed especially after encountering
a cold and after playing sport.
Pharmacology related to Case Patient
Salbutamol: ADME and Pharmacology
From the case study, one of medications given to Benji is Salbutamol. Salbutamol is a
selective agonist of beta 2 adrenergic receptor of the short acting type, which used prevalently
for the purpose of mitigating asthmatic symptoms specifically shortness of breath and
bronchoconstriction which have been presented by Benji. After being inhaled, Salbutamol is
6PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
absorbed topically by the smooth muscles lining the bronchioles and is prevalently undetected in
systemic circulation (Zhou, Wang, Zhang, Ji & Yang, 2017). Minute concentrations may
however be found in the blood after approximately 3 hours as a result of a minor amount of
dosage which undergoes swallowing during inhalation, thus resulting in absorption by the gut.
Upon absorption, salbutamol has been evidenced to undergo distribution across the body via
binding loosely to the proteins in the blood plasma. Intravenous administration of salbutamol has
been evidenced to record a distribution volume of approximately 156 +/- 38 L. This medication
undergoes metabolism via hepatic conversion to its ester form, salbutamol 4’-O-sulfate which is
associated with negligible pharmacological functioning (Moore et al., 2019). Salbutamol may
also undergo metabolism via conjugation or oxidative deamination with glucuronide.
Approximately 80% of the drug undergoes urinary excretion within 24 hours of oral intake, a
majority of which comprises of metabolites. Fecal excretion may occur with trace amounts of the
drug. The half-life of elimination of salbutamol has been found to range from approximately 3 to
7 hours (Louis et al., 2020).
Salbutamol has been found to excrete its pharmacological mechanism of action by
exerting an agonistic effect on beta 2 adrenergic receptors which are present across the smooth
muscles lining the bronchioles and upper respiratory tract. This results in the stimulation of the
enzyme adenyl cyclase which in turn results in the rise of concentration of cyclic-3′, 5′-adenosine
monophosphate or cyclic AMP at the intracellular level. Activation of cyclic AMP contributes to
the facilitation of protein kinase A which in turn, inhibits myosin phosphorylation and resultant
reduced intracellular concentration of calcium ions (Gonem, Cumella & Richardson, 2019). This
pharmacological mechanism results in the relaxation of all the smooth muscles lining the
bronchioles as well as the trachea of the upper respiratory tract resulting in dilation of
absorbed topically by the smooth muscles lining the bronchioles and is prevalently undetected in
systemic circulation (Zhou, Wang, Zhang, Ji & Yang, 2017). Minute concentrations may
however be found in the blood after approximately 3 hours as a result of a minor amount of
dosage which undergoes swallowing during inhalation, thus resulting in absorption by the gut.
Upon absorption, salbutamol has been evidenced to undergo distribution across the body via
binding loosely to the proteins in the blood plasma. Intravenous administration of salbutamol has
been evidenced to record a distribution volume of approximately 156 +/- 38 L. This medication
undergoes metabolism via hepatic conversion to its ester form, salbutamol 4’-O-sulfate which is
associated with negligible pharmacological functioning (Moore et al., 2019). Salbutamol may
also undergo metabolism via conjugation or oxidative deamination with glucuronide.
Approximately 80% of the drug undergoes urinary excretion within 24 hours of oral intake, a
majority of which comprises of metabolites. Fecal excretion may occur with trace amounts of the
drug. The half-life of elimination of salbutamol has been found to range from approximately 3 to
7 hours (Louis et al., 2020).
Salbutamol has been found to excrete its pharmacological mechanism of action by
exerting an agonistic effect on beta 2 adrenergic receptors which are present across the smooth
muscles lining the bronchioles and upper respiratory tract. This results in the stimulation of the
enzyme adenyl cyclase which in turn results in the rise of concentration of cyclic-3′, 5′-adenosine
monophosphate or cyclic AMP at the intracellular level. Activation of cyclic AMP contributes to
the facilitation of protein kinase A which in turn, inhibits myosin phosphorylation and resultant
reduced intracellular concentration of calcium ions (Gonem, Cumella & Richardson, 2019). This
pharmacological mechanism results in the relaxation of all the smooth muscles lining the
bronchioles as well as the trachea of the upper respiratory tract resulting in dilation of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
bronchioles, prevention of bronchiole narrowing and enhanced air inhalation resulting in
mitigation of asthmatic and URTI symptoms of coughing and wheezing and shortness of breath.
Thus, bronchodilator-associated mechanisms of Salbutamol are likely to provide relief to Benji’s
current symptoms of coughing and wheezing and shortness of breath by counteracting asthmatic
symptoms of bronchiole narrowing and constriction (Ozer et al., 2018).
Prednisolone: ADME and Pharmacology
Prednisolone is a glucocorticoid medication with a pharmacological mechanism of action
similar to glucocorticoids. It is prevalently known for its pharmacological functions of anti-
inflammation, immunosuppression, vasoconstriction and anti-neoplasm. In addition to the
treatment of endocrinal, hematological, ophthalmological, dermatological, gastrointestinal and
rheumatoid conditions, prednisolone is prevalently used for the mitigation of symptoms related
to respiratory diseases, allergies – which can be well related to Benji’s present condition of
asthma, dust allergy and possible risk of pulmonary edema (Bryant & Knights, 2014; Agarwal et
al., 2018). Upon intake, prednisolone undergoes rapid absorption by the gut resulting in peak
values of concentration associated with 70% bioavailability in the blood within approximately 3
hours of its consumption. Prednisolone undergoes distribution in the body via binding with
plasma proteins, with a variation of approximately 60 to 90% (Sneeboer et al., 2016). Upon
consumption of prednisolone dosages ranging from 0.15 to 0.30 grams/kg of dosage, it has been
evidenced to contribute to a distribution in volumes ranging from 30 to 45 L approximately.
Prednisolone undergoes metabolism to prednisone followed by metabolism to a range of
metabolites like 6α-hydroxy-prednisone, 17α, 21-dihydroxy-pregnan-1, 4, 6-trien-3, 11, 30-
trione or 20α-dihydro-prednisone. These metabolites and approximately 99% of prednisolone
bronchioles, prevention of bronchiole narrowing and enhanced air inhalation resulting in
mitigation of asthmatic and URTI symptoms of coughing and wheezing and shortness of breath.
Thus, bronchodilator-associated mechanisms of Salbutamol are likely to provide relief to Benji’s
current symptoms of coughing and wheezing and shortness of breath by counteracting asthmatic
symptoms of bronchiole narrowing and constriction (Ozer et al., 2018).
Prednisolone: ADME and Pharmacology
Prednisolone is a glucocorticoid medication with a pharmacological mechanism of action
similar to glucocorticoids. It is prevalently known for its pharmacological functions of anti-
inflammation, immunosuppression, vasoconstriction and anti-neoplasm. In addition to the
treatment of endocrinal, hematological, ophthalmological, dermatological, gastrointestinal and
rheumatoid conditions, prednisolone is prevalently used for the mitigation of symptoms related
to respiratory diseases, allergies – which can be well related to Benji’s present condition of
asthma, dust allergy and possible risk of pulmonary edema (Bryant & Knights, 2014; Agarwal et
al., 2018). Upon intake, prednisolone undergoes rapid absorption by the gut resulting in peak
values of concentration associated with 70% bioavailability in the blood within approximately 3
hours of its consumption. Prednisolone undergoes distribution in the body via binding with
plasma proteins, with a variation of approximately 60 to 90% (Sneeboer et al., 2016). Upon
consumption of prednisolone dosages ranging from 0.15 to 0.30 grams/kg of dosage, it has been
evidenced to contribute to a distribution in volumes ranging from 30 to 45 L approximately.
Prednisolone undergoes metabolism to prednisone followed by metabolism to a range of
metabolites like 6α-hydroxy-prednisone, 17α, 21-dihydroxy-pregnan-1, 4, 6-trien-3, 11, 30-
trione or 20α-dihydro-prednisone. These metabolites and approximately 99% of prednisolone
8PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
undergo urinary excretion, with a half-life approximately 4 hours in the plasma (Sousa et al.,
2017).
Prednisolone exerts its pharmacological mechanism of action via binding to the receptors
of glucocorticoids, which in turn, contributes to the promotion of anti-inflammation and
restriction of pro-inflammatory mechanisms which are prevalently observed in asthma and URTI
as discussed in Benji’s case (Bryant & Knights, 2014; Cronin et al., 2016). These
pharmacological mechanisms contribute to the restricted migration of pro-inflammatory
leukocytes to inflammation and inhibition of the apoptosis of neutrophils sites across the upper
respiratory tract. Reduction of pro-inflammatory mechanisms will hence contribute to
improvement in children like Benji, since it will pave the way for decreased inflammation of the
respiratory tract and resultant reduced mucosal blockage and exudate secretion across
bronchioles, a decrease bronchiole narrowing and increased temperature and thus, alleviation of
symptoms of fever, coughing wheezing due to constriction (Agarwal et al., 2018).
Ipratropium: ADME and Pharmacology
Ipratropium is a commonly prescribed therapeutic drug with anticholinergic based
pharmacological mechanisms. It is used prevalently for acute asthma exacerbations treatment
and local reduction of symptoms associated with rhinitis, nasal congestion and bronchospasm
and thus, will prove to be useful for combating the acute respiratory distress he experiences due
to dust and allergic response of asthma (Wongwaree, 2017). Upon inhalation, ipratropium
demonstrates negligible gut absorption and active topic absorption via the presence of 5 valent
nitrogen ions across the mucosal lining of the upper respiratory tract. Upon inhalation,
ipratropium attains peak levels of absorption by approximately 2 hours of 2% of the dosage
administered. Low concentrations thus demonstrate low levels of protein binding and
undergo urinary excretion, with a half-life approximately 4 hours in the plasma (Sousa et al.,
2017).
Prednisolone exerts its pharmacological mechanism of action via binding to the receptors
of glucocorticoids, which in turn, contributes to the promotion of anti-inflammation and
restriction of pro-inflammatory mechanisms which are prevalently observed in asthma and URTI
as discussed in Benji’s case (Bryant & Knights, 2014; Cronin et al., 2016). These
pharmacological mechanisms contribute to the restricted migration of pro-inflammatory
leukocytes to inflammation and inhibition of the apoptosis of neutrophils sites across the upper
respiratory tract. Reduction of pro-inflammatory mechanisms will hence contribute to
improvement in children like Benji, since it will pave the way for decreased inflammation of the
respiratory tract and resultant reduced mucosal blockage and exudate secretion across
bronchioles, a decrease bronchiole narrowing and increased temperature and thus, alleviation of
symptoms of fever, coughing wheezing due to constriction (Agarwal et al., 2018).
Ipratropium: ADME and Pharmacology
Ipratropium is a commonly prescribed therapeutic drug with anticholinergic based
pharmacological mechanisms. It is used prevalently for acute asthma exacerbations treatment
and local reduction of symptoms associated with rhinitis, nasal congestion and bronchospasm
and thus, will prove to be useful for combating the acute respiratory distress he experiences due
to dust and allergic response of asthma (Wongwaree, 2017). Upon inhalation, ipratropium
demonstrates negligible gut absorption and active topic absorption via the presence of 5 valent
nitrogen ions across the mucosal lining of the upper respiratory tract. Upon inhalation,
ipratropium attains peak levels of absorption by approximately 2 hours of 2% of the dosage
administered. Low concentrations thus demonstrate low levels of protein binding and
9PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
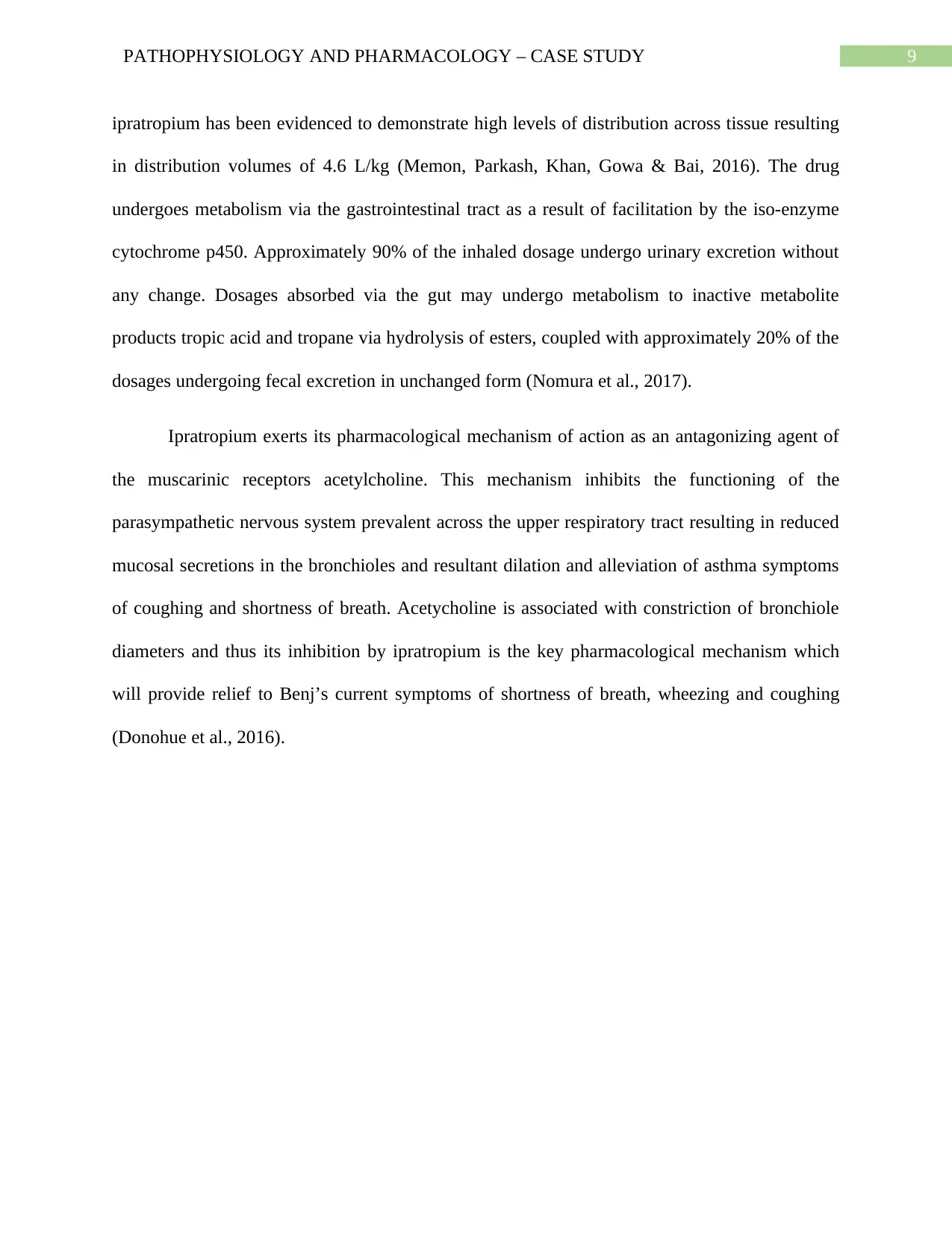
ipratropium has been evidenced to demonstrate high levels of distribution across tissue resulting
in distribution volumes of 4.6 L/kg (Memon, Parkash, Khan, Gowa & Bai, 2016). The drug
undergoes metabolism via the gastrointestinal tract as a result of facilitation by the iso-enzyme
cytochrome p450. Approximately 90% of the inhaled dosage undergo urinary excretion without
any change. Dosages absorbed via the gut may undergo metabolism to inactive metabolite
products tropic acid and tropane via hydrolysis of esters, coupled with approximately 20% of the
dosages undergoing fecal excretion in unchanged form (Nomura et al., 2017).
Ipratropium exerts its pharmacological mechanism of action as an antagonizing agent of
the muscarinic receptors acetylcholine. This mechanism inhibits the functioning of the
parasympathetic nervous system prevalent across the upper respiratory tract resulting in reduced
mucosal secretions in the bronchioles and resultant dilation and alleviation of asthma symptoms
of coughing and shortness of breath. Acetycholine is associated with constriction of bronchiole
diameters and thus its inhibition by ipratropium is the key pharmacological mechanism which
will provide relief to Benj’s current symptoms of shortness of breath, wheezing and coughing
(Donohue et al., 2016).
ipratropium has been evidenced to demonstrate high levels of distribution across tissue resulting
in distribution volumes of 4.6 L/kg (Memon, Parkash, Khan, Gowa & Bai, 2016). The drug
undergoes metabolism via the gastrointestinal tract as a result of facilitation by the iso-enzyme
cytochrome p450. Approximately 90% of the inhaled dosage undergo urinary excretion without
any change. Dosages absorbed via the gut may undergo metabolism to inactive metabolite
products tropic acid and tropane via hydrolysis of esters, coupled with approximately 20% of the
dosages undergoing fecal excretion in unchanged form (Nomura et al., 2017).
Ipratropium exerts its pharmacological mechanism of action as an antagonizing agent of
the muscarinic receptors acetylcholine. This mechanism inhibits the functioning of the
parasympathetic nervous system prevalent across the upper respiratory tract resulting in reduced
mucosal secretions in the bronchioles and resultant dilation and alleviation of asthma symptoms
of coughing and shortness of breath. Acetycholine is associated with constriction of bronchiole
diameters and thus its inhibition by ipratropium is the key pharmacological mechanism which
will provide relief to Benj’s current symptoms of shortness of breath, wheezing and coughing
(Donohue et al., 2016).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
References
Agarwal, R., Dhooria, S., Sehgal, I. S., Aggarwal, A. N., Garg, M., Saikia, B., ... & Chakrabarti,
A. (2018). A randomized trial of itraconazole vs prednisolone in acute-stage allergic
bronchopulmonary aspergillosis complicating asthma. Chest, 153(3), 656-664. doi:
https://doi.org/10.1016/j.chest.2018.01.005.
Agarwal, R., Dhooria, S., Sehgal, I. S., Aggarwal, A. N., Garg, M., Saikia, B., & Chakrabarti, A.
(2018). A randomised trial of voriconazole and prednisolone monotherapy in acute-stage
allergic bronchopulmonary aspergillosis complicating asthma. European Respiratory
Journal, 52(3), 1801159. doi: 10.1183/13993003.01159-2018.
Aglipay, M., Birken, C. S., Parkin, P. C., Loeb, M. B., Thorpe, K., Chen, Y., ... & Mazzulli, T.
(2017). Effect of high-dose vs standard-dose wintertime vitamin D supplementation on
viral upper respiratory tract infections in young healthy children. Jama, 318(3), 245-254.
doi: 10.1001/jama.2017.8708.
Biezen, R., Pollack, A. J., Harrison, C., Brijnath, B., Grando, D., Britt, H. C., & Mazza, D.
(2015). Respiratory tract infections among children younger than 5 years: current
management in Australian general practice. Medical Journal of Australia, 202(5), 262-
265. doi: 10.5694/mja14.00090.
Bosch, A. A., Levin, E., van Houten, M. A., Hasrat, R., Kalkman, G., Biesbroek, G., ... &
Sanders, E. A. (2016). Development of upper respiratory tract microbiota in infancy is
affected by mode of delivery. EBioMedicine, 9, 336-345. doi:
https://doi.org/10.1016/j.ebiom.2016.05.031.
References
Agarwal, R., Dhooria, S., Sehgal, I. S., Aggarwal, A. N., Garg, M., Saikia, B., ... & Chakrabarti,
A. (2018). A randomized trial of itraconazole vs prednisolone in acute-stage allergic
bronchopulmonary aspergillosis complicating asthma. Chest, 153(3), 656-664. doi:
https://doi.org/10.1016/j.chest.2018.01.005.
Agarwal, R., Dhooria, S., Sehgal, I. S., Aggarwal, A. N., Garg, M., Saikia, B., & Chakrabarti, A.
(2018). A randomised trial of voriconazole and prednisolone monotherapy in acute-stage
allergic bronchopulmonary aspergillosis complicating asthma. European Respiratory
Journal, 52(3), 1801159. doi: 10.1183/13993003.01159-2018.
Aglipay, M., Birken, C. S., Parkin, P. C., Loeb, M. B., Thorpe, K., Chen, Y., ... & Mazzulli, T.
(2017). Effect of high-dose vs standard-dose wintertime vitamin D supplementation on
viral upper respiratory tract infections in young healthy children. Jama, 318(3), 245-254.
doi: 10.1001/jama.2017.8708.
Biezen, R., Pollack, A. J., Harrison, C., Brijnath, B., Grando, D., Britt, H. C., & Mazza, D.
(2015). Respiratory tract infections among children younger than 5 years: current
management in Australian general practice. Medical Journal of Australia, 202(5), 262-
265. doi: 10.5694/mja14.00090.
Bosch, A. A., Levin, E., van Houten, M. A., Hasrat, R., Kalkman, G., Biesbroek, G., ... &
Sanders, E. A. (2016). Development of upper respiratory tract microbiota in infancy is
affected by mode of delivery. EBioMedicine, 9, 336-345. doi:
https://doi.org/10.1016/j.ebiom.2016.05.031.
11PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Bryant, B., & Knights, K. (2014). Pharmacology for Health Professionals Ebook. Elsevier
Health Sciences. Retrieved from: https://www.elsevier.com/books/pharmacology-for-
health-professionals/bryant/978-0-7295-4275-3.
Carpaij, O. A., Burgess, J. K., Kerstjens, H. A., Nawijn, M. C., & van den Berge, M. (2019). A
review on the pathophysiology of asthma remission. Pharmacology & therapeutics, 201,
8-24. doi: https://doi.org/10.1016/j.pharmthera.2019.05.002.
Craft, J., Gordon, C., Huether, S. E., McCance, K. L., & Brashers, V. L. (2015). Understanding
pathophysiology-ANZ adaptation. Elsevier Health Sciences. Retrieved from:
https://www.elsevier.com/books/understanding-pathophysiology-anz/craft/978-0-7295-
4264-7.
Cronin, J. J., McCoy, S., Kennedy, U., an Fhailí, S. N., Wakai, A., Hayden, J., ... & O’Sullivan,
R. (2016). A randomized trial of single-dose oral dexamethasone versus multidose
prednisolone for acute exacerbations of asthma in children who attend the emergency
department. Annals of emergency medicine, 67(5), 593-601. doi:
https://doi.org/10.1016/j.annemergmed.2015.08.001.
DeMuri, G. P., Gern, J. E., Eickhoff, J. C., Lynch, S. V., & Wald, E. R. (2018). Dynamics of
bacterial colonization with Streptococcus pneumoniae, Haemophilus influenzae, and
Moraxella catarrhalis during symptomatic and asymptomatic viral upper respiratory tract
infection. Clinical Infectious Diseases, 66(7), 1045-1053. doi:
https://doi.org/10.1093/cid/cix941.
Depner, M., Ege, M. J., Cox, M. J., Dwyer, S., Walker, A. W., Birzele, L. T., ... & Maier, R. M.
(2017). Bacterial microbiota of the upper respiratory tract and childhood asthma. Journal
Bryant, B., & Knights, K. (2014). Pharmacology for Health Professionals Ebook. Elsevier
Health Sciences. Retrieved from: https://www.elsevier.com/books/pharmacology-for-
health-professionals/bryant/978-0-7295-4275-3.
Carpaij, O. A., Burgess, J. K., Kerstjens, H. A., Nawijn, M. C., & van den Berge, M. (2019). A
review on the pathophysiology of asthma remission. Pharmacology & therapeutics, 201,
8-24. doi: https://doi.org/10.1016/j.pharmthera.2019.05.002.
Craft, J., Gordon, C., Huether, S. E., McCance, K. L., & Brashers, V. L. (2015). Understanding
pathophysiology-ANZ adaptation. Elsevier Health Sciences. Retrieved from:
https://www.elsevier.com/books/understanding-pathophysiology-anz/craft/978-0-7295-
4264-7.
Cronin, J. J., McCoy, S., Kennedy, U., an Fhailí, S. N., Wakai, A., Hayden, J., ... & O’Sullivan,
R. (2016). A randomized trial of single-dose oral dexamethasone versus multidose
prednisolone for acute exacerbations of asthma in children who attend the emergency
department. Annals of emergency medicine, 67(5), 593-601. doi:
https://doi.org/10.1016/j.annemergmed.2015.08.001.
DeMuri, G. P., Gern, J. E., Eickhoff, J. C., Lynch, S. V., & Wald, E. R. (2018). Dynamics of
bacterial colonization with Streptococcus pneumoniae, Haemophilus influenzae, and
Moraxella catarrhalis during symptomatic and asymptomatic viral upper respiratory tract
infection. Clinical Infectious Diseases, 66(7), 1045-1053. doi:
https://doi.org/10.1093/cid/cix941.
Depner, M., Ege, M. J., Cox, M. J., Dwyer, S., Walker, A. W., Birzele, L. T., ... & Maier, R. M.
(2017). Bacterial microbiota of the upper respiratory tract and childhood asthma. Journal
12PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
of Allergy and Clinical Immunology, 139(3), 826-834. doi:
https://doi.org/10.1016/j.jaci.2016.05.050.
Donohue, J. F., Wise, R., Busse, W. W., Garfinkel, S., Zubek, V. B., Ghafouri, M., ... &
Bleecker, E. R. (2016). Efficacy and safety of ipratropium bromide/albuterol compared
with albuterol in patients with moderate-to-severe asthma: a randomized controlled
trial. BMC pulmonary medicine, 16(1), 65. doi: https://doi.org/10.1186/s12890-016-0223-
3.
Gaarslev, C., Yee, M., Chan, G., Fletcher-Lartey, S., & Khan, R. (2016). A mixed methods study
to understand patient expectations for antibiotics for an upper respiratory tract
infection. Antimicrobial Resistance & Infection Control, 5(1), 39. doi:
https://doi.org/10.1186/s13756-016-0134-3.
Gonem, S., Cumella, A., & Richardson, M. (2019). Asthma admission rates and patterns of
salbutamol and inhaled corticosteroid prescribing in England from 2013 to
2017. Thorax, 74(7), 705-706. doi: http://dx.doi.org/10.1136/thoraxjnl-2018-212723.
King, G. G., Farrow, C. E., & Chapman, D. G. (2019). Dismantling the pathophysiology of
asthma using imaging. European Respiratory Review, 28(152). doi:
10.1183/16000617.0111-2018.
King, G. G., James, A., Harkness, L., & Wark, P. A. (2018). Pathophysiology of severe asthma:
We’ve only just started. Respirology, 23(3), 262-271. doi:
https://doi.org/10.1111/resp.13251.
Lewnard, J. A., Givon-Lavi, N., Huppert, A., Pettigrew, M. M., Regev-Yochay, G., Dagan, R., &
Weinberger, D. M. (2016). Epidemiological markers for interactions among
of Allergy and Clinical Immunology, 139(3), 826-834. doi:
https://doi.org/10.1016/j.jaci.2016.05.050.
Donohue, J. F., Wise, R., Busse, W. W., Garfinkel, S., Zubek, V. B., Ghafouri, M., ... &
Bleecker, E. R. (2016). Efficacy and safety of ipratropium bromide/albuterol compared
with albuterol in patients with moderate-to-severe asthma: a randomized controlled
trial. BMC pulmonary medicine, 16(1), 65. doi: https://doi.org/10.1186/s12890-016-0223-
3.
Gaarslev, C., Yee, M., Chan, G., Fletcher-Lartey, S., & Khan, R. (2016). A mixed methods study
to understand patient expectations for antibiotics for an upper respiratory tract
infection. Antimicrobial Resistance & Infection Control, 5(1), 39. doi:
https://doi.org/10.1186/s13756-016-0134-3.
Gonem, S., Cumella, A., & Richardson, M. (2019). Asthma admission rates and patterns of
salbutamol and inhaled corticosteroid prescribing in England from 2013 to
2017. Thorax, 74(7), 705-706. doi: http://dx.doi.org/10.1136/thoraxjnl-2018-212723.
King, G. G., Farrow, C. E., & Chapman, D. G. (2019). Dismantling the pathophysiology of
asthma using imaging. European Respiratory Review, 28(152). doi:
10.1183/16000617.0111-2018.
King, G. G., James, A., Harkness, L., & Wark, P. A. (2018). Pathophysiology of severe asthma:
We’ve only just started. Respirology, 23(3), 262-271. doi:
https://doi.org/10.1111/resp.13251.
Lewnard, J. A., Givon-Lavi, N., Huppert, A., Pettigrew, M. M., Regev-Yochay, G., Dagan, R., &
Weinberger, D. M. (2016). Epidemiological markers for interactions among
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus in upper
respiratory tract carriage. The Journal of infectious diseases, 213(10), 1596-1605. doi:
https://doi.org/10.1093/infdis/jiv761.
Louis, R., Bougard, N., Guissard, F., Paulus, V., Henket, M., & Schleich, F. (2020).
Bronchodilation Test with Inhaled Salbutamol Versus Bronchial Methacholine Challenge
to Make an Asthma Diagnosis: Do They Provide the Same Information?. The Journal of
Allergy and Clinical Immunology: In Practice, 8(2), 618-625. doi:
https://doi.org/10.1016/j.jaip.2019.09.007.
McGeachie, M. J., Yates, K. P., Zhou, X., Guo, F., Sternberg, A. L., Van Natta, M. L., ... & Cho,
M. H. (2016). Patterns of growth and decline in lung function in persistent childhood
asthma. New England Journal of Medicine, 374(19), 1842-1852. doi:
10.1056/NEJMoa1513737.
Memon, B. N., Parkash, A., Khan, K. M. A., Gowa, M. A., & Bai, C. (2016). Response to
nebulized salbutamol versus combination with ipratropium bromide in children with
acute severe asthma. JPMA. The Journal of the Pakistan Medical Association, 66(3),
243-6. Retrieved from:
https://www.researchgate.net/profile/Arit_Parkash/publication/296485202_Response_to_
nebulized_salbutamol_versus_combination_with_ipratropium_bromide_in_children_with
_acute_severe_asthma/links/56d5d2bd08aee73df6c05335.pdf.
Moore, L. E., Kapoor, K., Byers, B. W., Brotto, A. R., Ghods-Esfahani, D., Henry, S. L., ... &
Stickland, M. K. (2019). Acute effects of salbutamol on systemic vascular function in
Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus in upper
respiratory tract carriage. The Journal of infectious diseases, 213(10), 1596-1605. doi:
https://doi.org/10.1093/infdis/jiv761.
Louis, R., Bougard, N., Guissard, F., Paulus, V., Henket, M., & Schleich, F. (2020).
Bronchodilation Test with Inhaled Salbutamol Versus Bronchial Methacholine Challenge
to Make an Asthma Diagnosis: Do They Provide the Same Information?. The Journal of
Allergy and Clinical Immunology: In Practice, 8(2), 618-625. doi:
https://doi.org/10.1016/j.jaip.2019.09.007.
McGeachie, M. J., Yates, K. P., Zhou, X., Guo, F., Sternberg, A. L., Van Natta, M. L., ... & Cho,
M. H. (2016). Patterns of growth and decline in lung function in persistent childhood
asthma. New England Journal of Medicine, 374(19), 1842-1852. doi:
10.1056/NEJMoa1513737.
Memon, B. N., Parkash, A., Khan, K. M. A., Gowa, M. A., & Bai, C. (2016). Response to
nebulized salbutamol versus combination with ipratropium bromide in children with
acute severe asthma. JPMA. The Journal of the Pakistan Medical Association, 66(3),
243-6. Retrieved from:
https://www.researchgate.net/profile/Arit_Parkash/publication/296485202_Response_to_
nebulized_salbutamol_versus_combination_with_ipratropium_bromide_in_children_with
_acute_severe_asthma/links/56d5d2bd08aee73df6c05335.pdf.
Moore, L. E., Kapoor, K., Byers, B. W., Brotto, A. R., Ghods-Esfahani, D., Henry, S. L., ... &
Stickland, M. K. (2019). Acute effects of salbutamol on systemic vascular function in
14PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
people with asthma. Respiratory medicine, 155, 133-140. doi:
https://doi.org/10.1016/j.rmed.2019.07.018.
Nomura, O., Morikawa, Y., Hagiwara, Y., Ihara, T., Inoue, N., Sakakibara, H., & Akasawa, A.
(2017). Ipratropium bromide for acute asthma in children: A retrospective trial.
Allergy, 66(7), 945-952. doi: https://doi.org/10.15036/arerugi.66.945.
Ozer, M., Buyuktiryaki, B., Sahiner, U. M., Teksam, O., Karaatmaca, B., Soyer, O., & Sekerel,
B. E. (2018). Repeated doses of salbutamol and aeroallergen sensitisation both increased
salbutamol‐induced hypoxia in children and adolescents with acute asthma. Acta
Paediatrica, 107(4), 647-652. doi: https://doi.org/10.1111/apa.14202.
Pelaia, C., Paoletti, G., Puggioni, F., Racca, F., Pelaia, G., Canonica, G. W., & Heffler, E.
(2019). Interleukin-5 in the Pathophysiology of Severe Asthma. Frontiers in
Physiology, 10, 1514. doi: https://doi.org/10.3389/fphys.2019.01514.
Regli, A., Becke, K., & von Ungern-Sternberg, B. S. (2017). An update on the perioperative
management of children with upper respiratory tract infections. Current Opinion in
Anesthesiology, 30(3), 362-367. doi: 10.1097/ACO.0000000000000460.
Sneeboer, M. M., Majoor, C. J., de Kievit, A., Meijers, J. C., van der Poll, T., Kamphuisen, P.
W., & Bel, E. H. (2016). Prothrombotic state in patients with severe and prednisolone-
dependent asthma. Journal of Allergy and Clinical Immunology, 137(6), 1727-1732. doi:
https://doi.org/10.1016/j.jaci.2015.10.038.
Sousa, A. R., Marshall, R. P., Warnock, L. C., Bolton, S., Hastie, A., Symon, F., ... & Haldar, P.
(2017). Responsiveness to oral prednisolone in severe asthma is related to the degree of
people with asthma. Respiratory medicine, 155, 133-140. doi:
https://doi.org/10.1016/j.rmed.2019.07.018.
Nomura, O., Morikawa, Y., Hagiwara, Y., Ihara, T., Inoue, N., Sakakibara, H., & Akasawa, A.
(2017). Ipratropium bromide for acute asthma in children: A retrospective trial.
Allergy, 66(7), 945-952. doi: https://doi.org/10.15036/arerugi.66.945.
Ozer, M., Buyuktiryaki, B., Sahiner, U. M., Teksam, O., Karaatmaca, B., Soyer, O., & Sekerel,
B. E. (2018). Repeated doses of salbutamol and aeroallergen sensitisation both increased
salbutamol‐induced hypoxia in children and adolescents with acute asthma. Acta
Paediatrica, 107(4), 647-652. doi: https://doi.org/10.1111/apa.14202.
Pelaia, C., Paoletti, G., Puggioni, F., Racca, F., Pelaia, G., Canonica, G. W., & Heffler, E.
(2019). Interleukin-5 in the Pathophysiology of Severe Asthma. Frontiers in
Physiology, 10, 1514. doi: https://doi.org/10.3389/fphys.2019.01514.
Regli, A., Becke, K., & von Ungern-Sternberg, B. S. (2017). An update on the perioperative
management of children with upper respiratory tract infections. Current Opinion in
Anesthesiology, 30(3), 362-367. doi: 10.1097/ACO.0000000000000460.
Sneeboer, M. M., Majoor, C. J., de Kievit, A., Meijers, J. C., van der Poll, T., Kamphuisen, P.
W., & Bel, E. H. (2016). Prothrombotic state in patients with severe and prednisolone-
dependent asthma. Journal of Allergy and Clinical Immunology, 137(6), 1727-1732. doi:
https://doi.org/10.1016/j.jaci.2015.10.038.
Sousa, A. R., Marshall, R. P., Warnock, L. C., Bolton, S., Hastie, A., Symon, F., ... & Haldar, P.
(2017). Responsiveness to oral prednisolone in severe asthma is related to the degree of
15PATHOPHYSIOLOGY AND PHARMACOLOGY – CASE STUDY
eosinophilic airway inflammation. Clinical & Experimental Allergy, 47(7), 890-899. doi:
https://doi.org/10.1111/cea.12954.
Wongwaree, S. (2017). Comparison Efficacy of Randomized Nebulized Magnesium Sulfate and
Ipratropium Bromide/Fenoterol in Children with Severe Asthma Exacerbation. Journal
of Allergy and Clinical Immunology, 139(2), AB94. doi:
https://doi.org/10.1016/j.jaci.2016.12.307.
Xu, Q., Wischmeyer, J., Gonzalez, E., & Pichichero, M. E. (2017). Nasopharyngeal
polymicrobial colonization during health, viral upper respiratory infection and upper
respiratory bacterial infection. Journal of Infection, 75(1), 26-34. doi:
https://doi.org/10.1016/j.jinf.2017.04.003.
Yamauchi, K., & Ogasawara, M. (2019). The Role of Histamine in the Pathophysiology of
Asthma and the Clinical Efficacy of Antihistamines in Asthma Therapy. International
journal of molecular sciences, 20(7), 1733. doi: https://doi.org/10.3390/ijms20071733.
Yuksel, H., & Turkeli, A. (2017). Airway epithelial barrier dysfunction in the pathogenesis and
prognosis of respiratory tract diseases in childhood and adulthood. Tissue barriers, 5(4),
e1367458. doi: https://doi.org/10.1080/21688370.2017.1367458.
Zhou, L., Wang, Q., Zhang, Y., Ji, Y., & Yang, X. (2017). Aquatic photolysis of β2-agonist
salbutamol: kinetics and mechanism studies. Environmental Science and Pollution
Research, 24(6), 5544-5553. doi: https://doi.org/10.1007/s11356-016-8207-7.
eosinophilic airway inflammation. Clinical & Experimental Allergy, 47(7), 890-899. doi:
https://doi.org/10.1111/cea.12954.
Wongwaree, S. (2017). Comparison Efficacy of Randomized Nebulized Magnesium Sulfate and
Ipratropium Bromide/Fenoterol in Children with Severe Asthma Exacerbation. Journal
of Allergy and Clinical Immunology, 139(2), AB94. doi:
https://doi.org/10.1016/j.jaci.2016.12.307.
Xu, Q., Wischmeyer, J., Gonzalez, E., & Pichichero, M. E. (2017). Nasopharyngeal
polymicrobial colonization during health, viral upper respiratory infection and upper
respiratory bacterial infection. Journal of Infection, 75(1), 26-34. doi:
https://doi.org/10.1016/j.jinf.2017.04.003.
Yamauchi, K., & Ogasawara, M. (2019). The Role of Histamine in the Pathophysiology of
Asthma and the Clinical Efficacy of Antihistamines in Asthma Therapy. International
journal of molecular sciences, 20(7), 1733. doi: https://doi.org/10.3390/ijms20071733.
Yuksel, H., & Turkeli, A. (2017). Airway epithelial barrier dysfunction in the pathogenesis and
prognosis of respiratory tract diseases in childhood and adulthood. Tissue barriers, 5(4),
e1367458. doi: https://doi.org/10.1080/21688370.2017.1367458.
Zhou, L., Wang, Q., Zhang, Y., Ji, Y., & Yang, X. (2017). Aquatic photolysis of β2-agonist
salbutamol: kinetics and mechanism studies. Environmental Science and Pollution
Research, 24(6), 5544-5553. doi: https://doi.org/10.1007/s11356-016-8207-7.
1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.