Pathophysiology of Angina Assignment PDF
VerifiedAdded on 2021/01/02
|12
|2577
|112
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
CLINICAL SCENARIO
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
TABLE OF CONTENTS
MAIN BODY...................................................................................................................................1
Question 1. Explain the rationale for the ECG request................................................................1
Question 2....................................................................................................................................1
2a. Pathophysiology of angina.....................................................................................................1
2b. List two risk factors specific to Betsy....................................................................................2
Question 3. Interpretation of the ECG........................................................................................2
Question 4. Acute Coronary Syndrome central findings that potentially lead to a diagnosis of
Acute Coronary Syndrome..........................................................................................................3
Question 5. Discuss the following drugs: GTN, diltiazem and pravastatin.................................3
Question 6. Mechanism of action and use of aspirin and ticagrelor in cardiac patients..............4
Question 7. Use of morphine in ACS..........................................................................................5
Question 8. Use current research to link the increased risk of depression with chronic illness. .5
REFERENCES................................................................................................................................6
MAIN BODY...................................................................................................................................1
Question 1. Explain the rationale for the ECG request................................................................1
Question 2....................................................................................................................................1
2a. Pathophysiology of angina.....................................................................................................1
2b. List two risk factors specific to Betsy....................................................................................2
Question 3. Interpretation of the ECG........................................................................................2
Question 4. Acute Coronary Syndrome central findings that potentially lead to a diagnosis of
Acute Coronary Syndrome..........................................................................................................3
Question 5. Discuss the following drugs: GTN, diltiazem and pravastatin.................................3
Question 6. Mechanism of action and use of aspirin and ticagrelor in cardiac patients..............4
Question 7. Use of morphine in ACS..........................................................................................5
Question 8. Use current research to link the increased risk of depression with chronic illness. .5
REFERENCES................................................................................................................................6
MAIN BODY
Question 1. Explain the rationale for the ECG request
The rationale for ECG request is important to identify the issues related to heart such as
irregular heartbeats, irregularity in rhythm, inadequate supply of oxygen etc. It is based on the
patient's complaint of short of breathlessness and feeling giddy. Her medical history included
coronary heart disease, chronic obstructive pulmonary disease and thus, there might be
possibility of any dysfunctionality of Betsy health conditions (Dedic & et.al., 2016). Moreover,
Betsy who is an elderly and is following medication of heavy doses including diltiazem SR,
salbutamol, spiriva and aspirin. She looked pale and sweaty and these signs indicated some
hidden symptoms and thus the nurse requested for an Electrocardiogram.
Question 2
2a. Pathophysiology of angina
Stable angina is refereed as the chest pain that takes place due to poor blood vessels in
the heart. This is the most common type of angina and occurs mostly while performing any task
or activity and goes away by taking proper rest. The patient has stable angina due to the
symptoms including nausea, sweating, paleness and shortness of breath. However, this angina is
one of the triggering factors for coronary artery disease (Saric & et.al., 2016). Thus, its causes,
progression and outcomes must be examined from time to study the onset of this disease in
patients like Betsy. However, this also initiates the onset of any heart problem and takes gradual
time to grow. Mostly, the symptoms are overlooked and it starts developing gradually by
following a set pattern and impact the patient's well being. Here the patient, Betsy had past
medical history of heart issue in the form of COPD, CAGs and hypertension.
There are several causes which consists of nausea, pain in arms, neck, shoulder, chest
pain, release of pressure or burning sensation, fatigue, sweating etc. Additionally, the stable
angina lasts for shorter duration and disappears sooner (Carlton & et.al., 2016). This is developed
during the activity or performing any task like exercising, swimming etc. and makes the heart to
work harder. Here the pain occurs but with medication or rest, it gets treated instantly. Its impact
is not lasting and might lead towards the normal adoption of healthy living. Next is the medical
emergency type, which is called as unstable angina where the affected patient is expected to any
usual change and has more severe effects. The medication has the impact that is long standing
1
Question 1. Explain the rationale for the ECG request
The rationale for ECG request is important to identify the issues related to heart such as
irregular heartbeats, irregularity in rhythm, inadequate supply of oxygen etc. It is based on the
patient's complaint of short of breathlessness and feeling giddy. Her medical history included
coronary heart disease, chronic obstructive pulmonary disease and thus, there might be
possibility of any dysfunctionality of Betsy health conditions (Dedic & et.al., 2016). Moreover,
Betsy who is an elderly and is following medication of heavy doses including diltiazem SR,
salbutamol, spiriva and aspirin. She looked pale and sweaty and these signs indicated some
hidden symptoms and thus the nurse requested for an Electrocardiogram.
Question 2
2a. Pathophysiology of angina
Stable angina is refereed as the chest pain that takes place due to poor blood vessels in
the heart. This is the most common type of angina and occurs mostly while performing any task
or activity and goes away by taking proper rest. The patient has stable angina due to the
symptoms including nausea, sweating, paleness and shortness of breath. However, this angina is
one of the triggering factors for coronary artery disease (Saric & et.al., 2016). Thus, its causes,
progression and outcomes must be examined from time to study the onset of this disease in
patients like Betsy. However, this also initiates the onset of any heart problem and takes gradual
time to grow. Mostly, the symptoms are overlooked and it starts developing gradually by
following a set pattern and impact the patient's well being. Here the patient, Betsy had past
medical history of heart issue in the form of COPD, CAGs and hypertension.
There are several causes which consists of nausea, pain in arms, neck, shoulder, chest
pain, release of pressure or burning sensation, fatigue, sweating etc. Additionally, the stable
angina lasts for shorter duration and disappears sooner (Carlton & et.al., 2016). This is developed
during the activity or performing any task like exercising, swimming etc. and makes the heart to
work harder. Here the pain occurs but with medication or rest, it gets treated instantly. Its impact
is not lasting and might lead towards the normal adoption of healthy living. Next is the medical
emergency type, which is called as unstable angina where the affected patient is expected to any
usual change and has more severe effects. The medication has the impact that is long standing
1
and might signal towards the occurrence of heart attack. This unstable angina is exactly like its
name which reflects upon the uncertainties and irregularities in terms of future impact.
STEMI is an acronym used for ST Elevation Myocardial Infarction which refers a serious
type of heart attack and is mostly treated with angioplasty or stenting via using thrombolytic or
PCI (percutaneous coronary intervention). For this, the individual is suffering from abnormalities
in the arteries gets blocked and this results in inconsistent flow of blood. Nevertheless, the
people misjudged it by dismissing it as symptoms of indigestion or heartburn. In rare cases like
Betsy who already has hypertension and undergo heavy does of medication on daily basis, the
scenario might be under controlled but with chances of getting a heart attack (Nishiguchi &
et.al., 2016). On the other hand, Non-ST Elevation Myocardial Infarction is considered as less
common than the STEMI. It has been evident that this is an intermediate form of Acute Coronary
Syndrome and is mainly due to onset of unstable angina. Here the patient takes additional
pressure that leads to damage on the muscles of the heart and might leads to tightness in the
chest, hooting pains in the arm and leg and more. Here, this is curable when treated under
supervision of professional help.
2b. List two risk factors specific to Betsy
The two risk factors that might impact Betsy with increasing risks of Acute Coronary
Syndrome are as follows. Firstly, her medication dosage which is based on daily basis and the
additional pressure on her body due to lack of physical activity (Pape & et.al., 2015). There is
past records of hypertension and past medical history of Chronic Obstructive Pulmonary
Disease. Secondly, the history of coronary heart disease and Type 2 Diabetes Mellitus also
proved another factor that risks her towards ACI. The additional signs were the symptoms of
nauseous feeling and patterns of heavy breathing which also hindered her well being.
Question 3. Interpretation of the ECG
An Electro Cardiogram is the combination of P waves, T waves and QRS complex. The
rhyme is inconsistent forms and the rate is present but shows irregularities in the p waves. This
infers that Betsy has stable angina which focuses on minute levels of abnormalities in her heart
rate despite showing fluctuations. Moreover, the sensors attached are useful in detecting the
electrical signals by the heart.
2
name which reflects upon the uncertainties and irregularities in terms of future impact.
STEMI is an acronym used for ST Elevation Myocardial Infarction which refers a serious
type of heart attack and is mostly treated with angioplasty or stenting via using thrombolytic or
PCI (percutaneous coronary intervention). For this, the individual is suffering from abnormalities
in the arteries gets blocked and this results in inconsistent flow of blood. Nevertheless, the
people misjudged it by dismissing it as symptoms of indigestion or heartburn. In rare cases like
Betsy who already has hypertension and undergo heavy does of medication on daily basis, the
scenario might be under controlled but with chances of getting a heart attack (Nishiguchi &
et.al., 2016). On the other hand, Non-ST Elevation Myocardial Infarction is considered as less
common than the STEMI. It has been evident that this is an intermediate form of Acute Coronary
Syndrome and is mainly due to onset of unstable angina. Here the patient takes additional
pressure that leads to damage on the muscles of the heart and might leads to tightness in the
chest, hooting pains in the arm and leg and more. Here, this is curable when treated under
supervision of professional help.
2b. List two risk factors specific to Betsy
The two risk factors that might impact Betsy with increasing risks of Acute Coronary
Syndrome are as follows. Firstly, her medication dosage which is based on daily basis and the
additional pressure on her body due to lack of physical activity (Pape & et.al., 2015). There is
past records of hypertension and past medical history of Chronic Obstructive Pulmonary
Disease. Secondly, the history of coronary heart disease and Type 2 Diabetes Mellitus also
proved another factor that risks her towards ACI. The additional signs were the symptoms of
nauseous feeling and patterns of heavy breathing which also hindered her well being.
Question 3. Interpretation of the ECG
An Electro Cardiogram is the combination of P waves, T waves and QRS complex. The
rhyme is inconsistent forms and the rate is present but shows irregularities in the p waves. This
infers that Betsy has stable angina which focuses on minute levels of abnormalities in her heart
rate despite showing fluctuations. Moreover, the sensors attached are useful in detecting the
electrical signals by the heart.
2
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Question 4. Acute Coronary Syndrome central findings that potentially lead to a diagnosis of
Acute Coronary Syndrome
There are several findings that shed light on the onset of acute coronary syndrome that
administered the diagnosis. This is mainly looked into by reading the ECG in detailed manner
and by observing the chest pain centres to understand the symptoms or signs in the patient.
Moreover, the influxes in the left arm, jaw or leg also gives signs of ACI and might be relatable
to nausea and sweating (Sanchis-Gomar & et.al., 2016). Herein, Betsy demonstrated signs like
nausea, sweating, paleness which shows signs of fatigue and led to the onset of ACI. In addition
to this, coronary angiogram procedure might be used to see the progression whether any
blockage or narrowing might take place. Here, the catheter is used to find out the extensive
outcomes on the affected patient. Next findings include about the unstable angina which also
leads to aggressive modes of acute coronary syndrome. Here its impact is in the coronary arteries
which is crucial for blood flow. The discomfort in chest or muscles of the heart led to worsening
impact and might result to shift to an Emergency and increasing the chances of cardiac arrest or
arrhythmias.
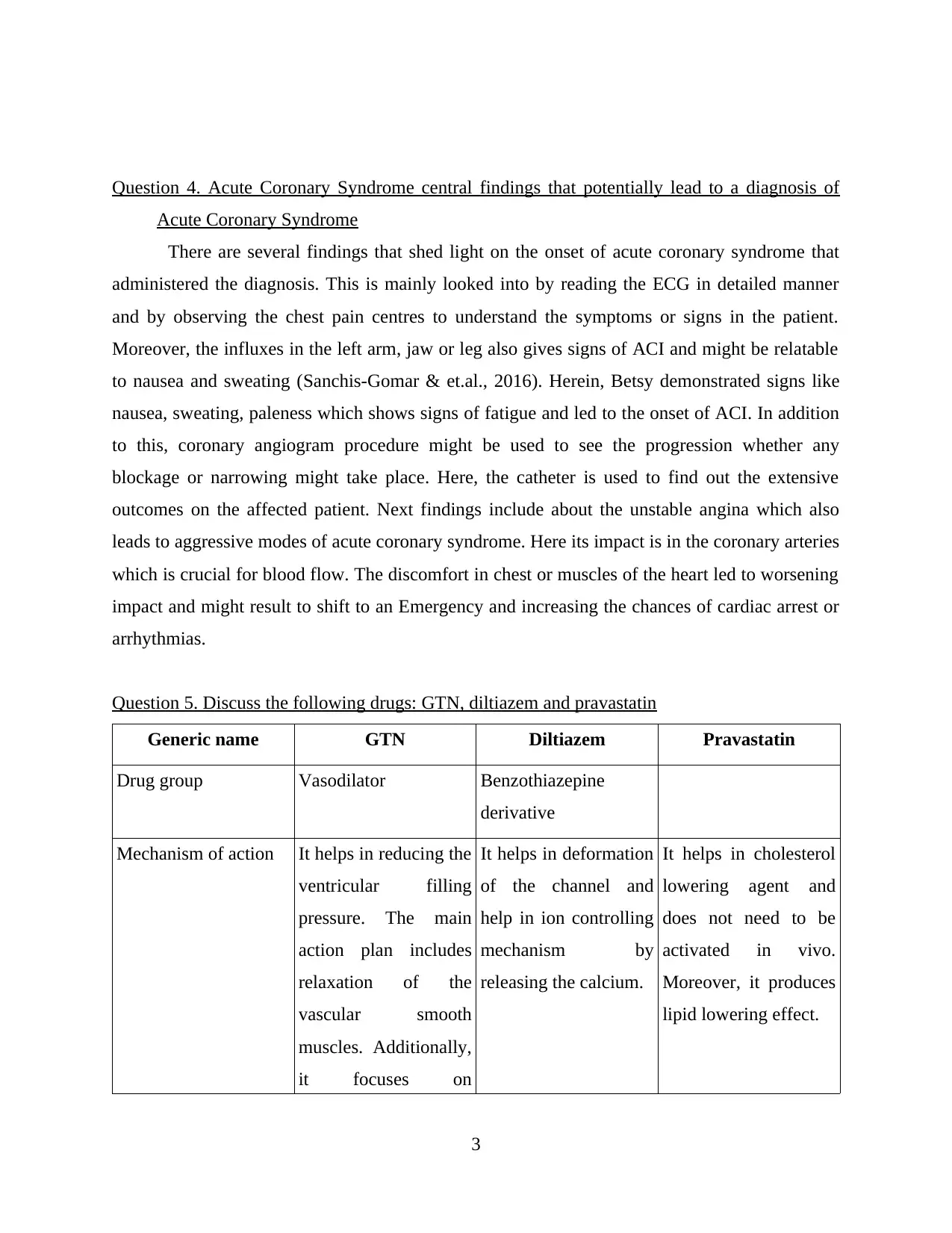
Question 5. Discuss the following drugs: GTN, diltiazem and pravastatin
Generic name GTN Diltiazem Pravastatin
Drug group Vasodilator Benzothiazepine
derivative
Mechanism of action It helps in reducing the
ventricular filling
pressure. The main
action plan includes
relaxation of the
vascular smooth
muscles. Additionally,
it focuses on
It helps in deformation
of the channel and
help in ion controlling
mechanism by
releasing the calcium.
It helps in cholesterol
lowering agent and
does not need to be
activated in vivo.
Moreover, it produces
lipid lowering effect.
3
Acute Coronary Syndrome
There are several findings that shed light on the onset of acute coronary syndrome that
administered the diagnosis. This is mainly looked into by reading the ECG in detailed manner
and by observing the chest pain centres to understand the symptoms or signs in the patient.
Moreover, the influxes in the left arm, jaw or leg also gives signs of ACI and might be relatable
to nausea and sweating (Sanchis-Gomar & et.al., 2016). Herein, Betsy demonstrated signs like
nausea, sweating, paleness which shows signs of fatigue and led to the onset of ACI. In addition
to this, coronary angiogram procedure might be used to see the progression whether any
blockage or narrowing might take place. Here, the catheter is used to find out the extensive
outcomes on the affected patient. Next findings include about the unstable angina which also
leads to aggressive modes of acute coronary syndrome. Here its impact is in the coronary arteries
which is crucial for blood flow. The discomfort in chest or muscles of the heart led to worsening
impact and might result to shift to an Emergency and increasing the chances of cardiac arrest or
arrhythmias.
Question 5. Discuss the following drugs: GTN, diltiazem and pravastatin
Generic name GTN Diltiazem Pravastatin
Drug group Vasodilator Benzothiazepine
derivative
Mechanism of action It helps in reducing the
ventricular filling
pressure. The main
action plan includes
relaxation of the
vascular smooth
muscles. Additionally,
it focuses on
It helps in deformation
of the channel and
help in ion controlling
mechanism by
releasing the calcium.
It helps in cholesterol
lowering agent and
does not need to be
activated in vivo.
Moreover, it produces
lipid lowering effect.
3
decreasing the effects
in both arterial and
venous parts.
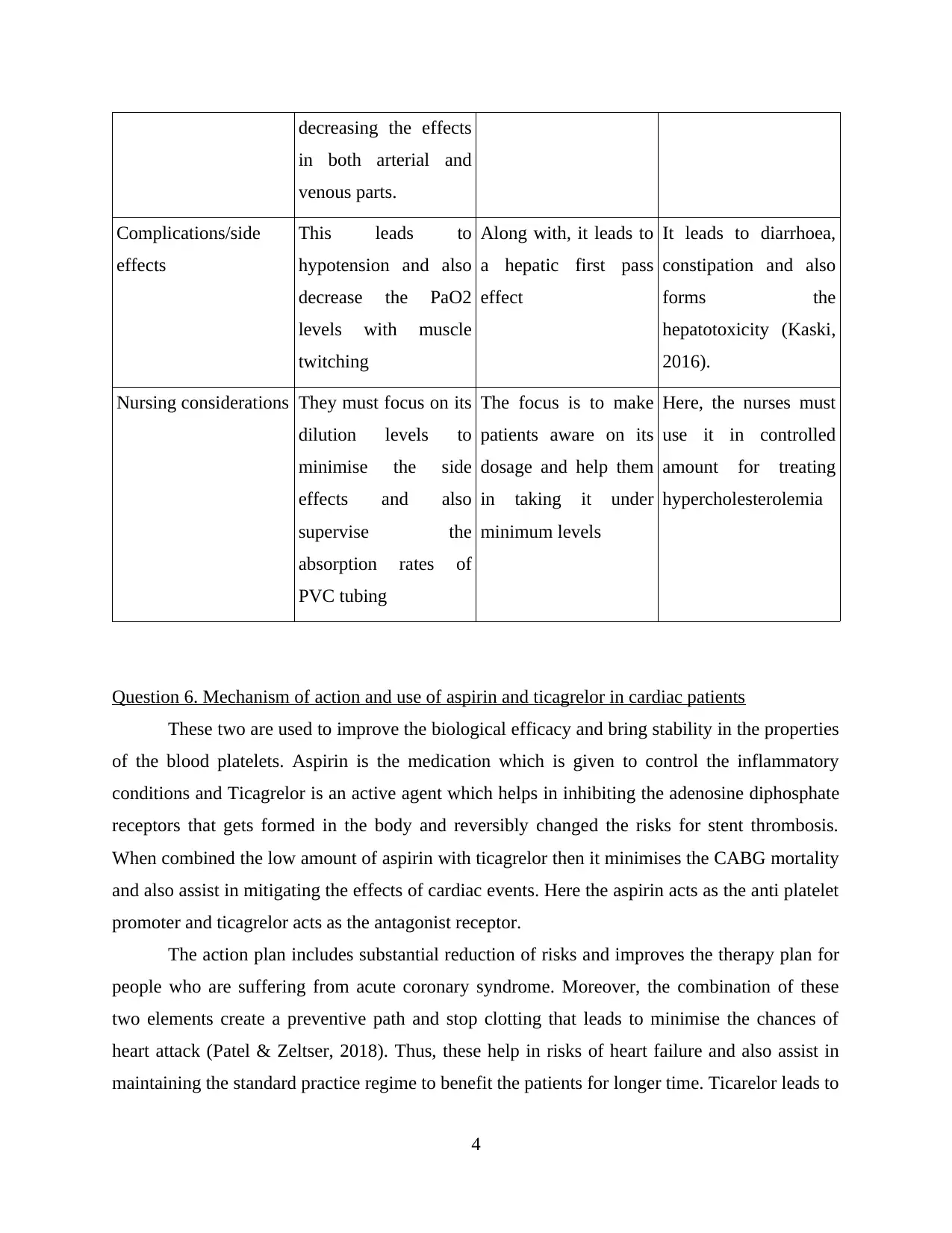
Complications/side
effects
This leads to
hypotension and also
decrease the PaO2
levels with muscle
twitching
Along with, it leads to
a hepatic first pass
effect
It leads to diarrhoea,
constipation and also
forms the
hepatotoxicity (Kaski,
2016).
Nursing considerations They must focus on its
dilution levels to
minimise the side
effects and also
supervise the
absorption rates of
PVC tubing
The focus is to make
patients aware on its
dosage and help them
in taking it under
minimum levels
Here, the nurses must
use it in controlled
amount for treating
hypercholesterolemia
Question 6. Mechanism of action and use of aspirin and ticagrelor in cardiac patients
These two are used to improve the biological efficacy and bring stability in the properties
of the blood platelets. Aspirin is the medication which is given to control the inflammatory
conditions and Ticagrelor is an active agent which helps in inhibiting the adenosine diphosphate
receptors that gets formed in the body and reversibly changed the risks for stent thrombosis.
When combined the low amount of aspirin with ticagrelor then it minimises the CABG mortality
and also assist in mitigating the effects of cardiac events. Here the aspirin acts as the anti platelet
promoter and ticagrelor acts as the antagonist receptor.
The action plan includes substantial reduction of risks and improves the therapy plan for
people who are suffering from acute coronary syndrome. Moreover, the combination of these
two elements create a preventive path and stop clotting that leads to minimise the chances of
heart attack (Patel & Zeltser, 2018). Thus, these help in risks of heart failure and also assist in
maintaining the standard practice regime to benefit the patients for longer time. Ticarelor leads to
4
in both arterial and
venous parts.
Complications/side
effects
This leads to
hypotension and also
decrease the PaO2
levels with muscle
twitching
Along with, it leads to
a hepatic first pass
effect
It leads to diarrhoea,
constipation and also
forms the
hepatotoxicity (Kaski,
2016).
Nursing considerations They must focus on its
dilution levels to
minimise the side
effects and also
supervise the
absorption rates of
PVC tubing
The focus is to make
patients aware on its
dosage and help them
in taking it under
minimum levels
Here, the nurses must
use it in controlled
amount for treating
hypercholesterolemia
Question 6. Mechanism of action and use of aspirin and ticagrelor in cardiac patients
These two are used to improve the biological efficacy and bring stability in the properties
of the blood platelets. Aspirin is the medication which is given to control the inflammatory
conditions and Ticagrelor is an active agent which helps in inhibiting the adenosine diphosphate
receptors that gets formed in the body and reversibly changed the risks for stent thrombosis.
When combined the low amount of aspirin with ticagrelor then it minimises the CABG mortality
and also assist in mitigating the effects of cardiac events. Here the aspirin acts as the anti platelet
promoter and ticagrelor acts as the antagonist receptor.
The action plan includes substantial reduction of risks and improves the therapy plan for
people who are suffering from acute coronary syndrome. Moreover, the combination of these
two elements create a preventive path and stop clotting that leads to minimise the chances of
heart attack (Patel & Zeltser, 2018). Thus, these help in risks of heart failure and also assist in
maintaining the standard practice regime to benefit the patients for longer time. Ticarelor leads to
4
bleeding due to the blood thinning process. However, aspirin inhibit the risk of bleeding and led
to onset of dyspnea.
Question 7. Use of morphine in ACS
According to Ferrari, Pavasini & Balla (2019) morphine has become essential in treating
acute coronary syndrome. People with non ST segment myocardial infraction has been benefited
to use it and it is beneficial in decreasing the pain levels. This is considered as the ideal analgesic
and has haemodynamic effects. It stimulates the processes and assist in reducing the demand of
oxygen that leads to inhibit the growth of seizures. In addition to this, it supports in delaying the
oral type of anti platelet drug absorption. This is pain reliever and is refereed as valuable agent
while conducting medical procedures. However, there are several limitations that has seen that
morphine has adverse impact and act as supplementary burden on the cardiac load. This
sometimes led to low rate and blood pressure as well in the patients which might lead to risk of
heart failure. Thus, this morphine has both advantages and disadvantages and has an impact on
the acute coronary syndrome related cases.
Question 8. Use current research to link the increased risk of depression with chronic illness
From the case study, it is evident that Betsy is an elderly who is 72 years and is devoid of
physical activity with a long medical history. She has been diagnosed with stable angina and led
to effects in her conditions. Moreover, the focus is on gaining knowledge on dealing with such
onset of heart diseases without any signs or symptoms. Although she showed few symptoms but
ignored it which is normal among the public (Santos & et.al., 2015). This entire phase of long list
of diseases like COPD, Type 2 diabetes, Hypertension and more led to a type of depression
where the patients like Betsy find it difficult to curb the negative feelings and has an anxiety
feeling all the time.
Furthermore, depression has negative effects on the human's heart and includes a more
probable risk of heart disease. This affects the cognitive and biological symptoms where it leads
to disturbances in the overall health of the involved patients. There is a need to understand that
psychological stress affects the nervous system and leads to elevated levels of risks that might
trigger the factors affecting the acute coronary syndrome or any chronic ailment. Thus,
depression must be treated with well structured medical planning to minimise the ill effects it has
on the mind and body of the patients. Alongside, this leads to a comprehensive treatment plan to
minimise the risks and optimise the effectiveness of the surroundings of the patients like Betsy.
5
to onset of dyspnea.
Question 7. Use of morphine in ACS
According to Ferrari, Pavasini & Balla (2019) morphine has become essential in treating
acute coronary syndrome. People with non ST segment myocardial infraction has been benefited
to use it and it is beneficial in decreasing the pain levels. This is considered as the ideal analgesic
and has haemodynamic effects. It stimulates the processes and assist in reducing the demand of
oxygen that leads to inhibit the growth of seizures. In addition to this, it supports in delaying the
oral type of anti platelet drug absorption. This is pain reliever and is refereed as valuable agent
while conducting medical procedures. However, there are several limitations that has seen that
morphine has adverse impact and act as supplementary burden on the cardiac load. This
sometimes led to low rate and blood pressure as well in the patients which might lead to risk of
heart failure. Thus, this morphine has both advantages and disadvantages and has an impact on
the acute coronary syndrome related cases.
Question 8. Use current research to link the increased risk of depression with chronic illness
From the case study, it is evident that Betsy is an elderly who is 72 years and is devoid of
physical activity with a long medical history. She has been diagnosed with stable angina and led
to effects in her conditions. Moreover, the focus is on gaining knowledge on dealing with such
onset of heart diseases without any signs or symptoms. Although she showed few symptoms but
ignored it which is normal among the public (Santos & et.al., 2015). This entire phase of long list
of diseases like COPD, Type 2 diabetes, Hypertension and more led to a type of depression
where the patients like Betsy find it difficult to curb the negative feelings and has an anxiety
feeling all the time.
Furthermore, depression has negative effects on the human's heart and includes a more
probable risk of heart disease. This affects the cognitive and biological symptoms where it leads
to disturbances in the overall health of the involved patients. There is a need to understand that
psychological stress affects the nervous system and leads to elevated levels of risks that might
trigger the factors affecting the acute coronary syndrome or any chronic ailment. Thus,
depression must be treated with well structured medical planning to minimise the ill effects it has
on the mind and body of the patients. Alongside, this leads to a comprehensive treatment plan to
minimise the risks and optimise the effectiveness of the surroundings of the patients like Betsy.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REFERENCES
Carlton, E. & et.al. (2016). Evaluation of high-sensitivity cardiac troponin I levels in patients
with suspected acute coronary syndrome. JAMA cardiology.1(4). 405-412.
Dedic, A. & et.al. (2016). Coronary CT angiography for suspected ACS in the era of high-
sensitivity troponins: randomized multicenter study. Journal of the American College of
Cardiology.67(1). 16-26.
Ferrari, R., Pavasini, R., & Balla, C. (2019). The multifaceted angina. European Heart Journal
Supplements, 21(Supplement_C), C1-C5.
Kaski, J. C. (2016). Stable Angina Pectoris: Definition, Clinical Presentation and
Pathophysiologic Mechanisms. In Essentials in Stable Angina Pectoris (pp. 15-35).
Springer, Cham.
Nishiguchi, T. & et.al. (2016). Prevalence of spontaneous coronary artery dissection in patients
with acute coronary syndrome. European Heart Journal: Acute Cardiovascular Care.5(3).
263-270.
Pape, L. A. & et.al. (2015). Presentation, diagnosis, and outcomes of acute aortic dissection: 17-
year trends from the International Registry of Acute Aortic Dissection. Journal of the
American College of Cardiology. 66(4). 350-358.
Patel, N. B., & Zeltser, R. (2018). Angina, Unstable. In StatPearls [Internet]. StatPearls
Publishing.
Sanchis-Gomar, F. & et.al. (2016). Epidemiology of coronary heart disease and acute coronary
syndrome. Annals of translational medicine, 4(13).
Santos, P. & et.al. (2015). Motives for requesting an electrocardiogram in primary health
care. Ciencia & saude coletiva.20. 1549-1554.
Saric, M. & et.al. (2016). Guidelines for the use of echocardiography in the evaluation of a
cardiac source of embolism. Journal of the American Society of Echocardiography.29(1).
1-42.
6
Carlton, E. & et.al. (2016). Evaluation of high-sensitivity cardiac troponin I levels in patients
with suspected acute coronary syndrome. JAMA cardiology.1(4). 405-412.
Dedic, A. & et.al. (2016). Coronary CT angiography for suspected ACS in the era of high-
sensitivity troponins: randomized multicenter study. Journal of the American College of
Cardiology.67(1). 16-26.
Ferrari, R., Pavasini, R., & Balla, C. (2019). The multifaceted angina. European Heart Journal
Supplements, 21(Supplement_C), C1-C5.
Kaski, J. C. (2016). Stable Angina Pectoris: Definition, Clinical Presentation and
Pathophysiologic Mechanisms. In Essentials in Stable Angina Pectoris (pp. 15-35).
Springer, Cham.
Nishiguchi, T. & et.al. (2016). Prevalence of spontaneous coronary artery dissection in patients
with acute coronary syndrome. European Heart Journal: Acute Cardiovascular Care.5(3).
263-270.
Pape, L. A. & et.al. (2015). Presentation, diagnosis, and outcomes of acute aortic dissection: 17-
year trends from the International Registry of Acute Aortic Dissection. Journal of the
American College of Cardiology. 66(4). 350-358.
Patel, N. B., & Zeltser, R. (2018). Angina, Unstable. In StatPearls [Internet]. StatPearls
Publishing.
Sanchis-Gomar, F. & et.al. (2016). Epidemiology of coronary heart disease and acute coronary
syndrome. Annals of translational medicine, 4(13).
Santos, P. & et.al. (2015). Motives for requesting an electrocardiogram in primary health
care. Ciencia & saude coletiva.20. 1549-1554.
Saric, M. & et.al. (2016). Guidelines for the use of echocardiography in the evaluation of a
cardiac source of embolism. Journal of the American Society of Echocardiography.29(1).
1-42.
6

7

8
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
9

10
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.