Analyzing Poverty's Impact on Healthcare Access in South Africa
VerifiedAdded on 2020/11/23
|15
|4120
|439
Report
AI Summary
This report delves into the critical issue of poverty and its impact on healthcare access in South Africa. It begins by exploring the historical context, including the legacy of apartheid and its effect on socioeconomic disparities, which has led to significant health challenges. The report examines the current state of healthcare, highlighting the inequalities in access and resource allocation, and the influence of factors such as education and disease prevalence. It discusses key considerations, including the challenges faced by the public healthcare system, the impact of chronic diseases, and the financial burdens on patients. The report analyzes the shortcomings in leadership, primary healthcare, and the healthcare workforce, and also examines the current status, including government spending, legislative reforms, and the prevalence of diseases like HIV, cancer and diabetes. Finally, the report provides an overview of the current situation and suggests options for improvement. This report provides a detailed analysis of the issues and challenges facing South Africa's healthcare system and offers insights into potential solutions for improving access and health outcomes.

Poverty and Access to healthcare in South Africa
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Issue............................................................................................................................................................3
Background.................................................................................................................................................4
Current status...............................................................................................................................................6
Key considerations......................................................................................................................................9
Options......................................................................................................................................................10
Conclusion and recommendation...............................................................................................................11
References.................................................................................................................................................14
Appendix...................................................................................................................................................16
Issue............................................................................................................................................................3
Background.................................................................................................................................................4
Current status...............................................................................................................................................6
Key considerations......................................................................................................................................9
Options......................................................................................................................................................10
Conclusion and recommendation...............................................................................................................11
References.................................................................................................................................................14
Appendix...................................................................................................................................................16
Issue
Access to health care is all about the timely use of personal health services so that outcome
towards a better living can be attained (Khamisa and et.al., 2015). The present briefing paper has
been prepared on access to quality healthcare services within South Africa. This study is very
important for the reader as getting access to quality health care services is a basic right of all
people but this situation is not present in South Africa. It will further assist the local government
to assess the issues that are present in health care system so that proper steps can be taken by
them.
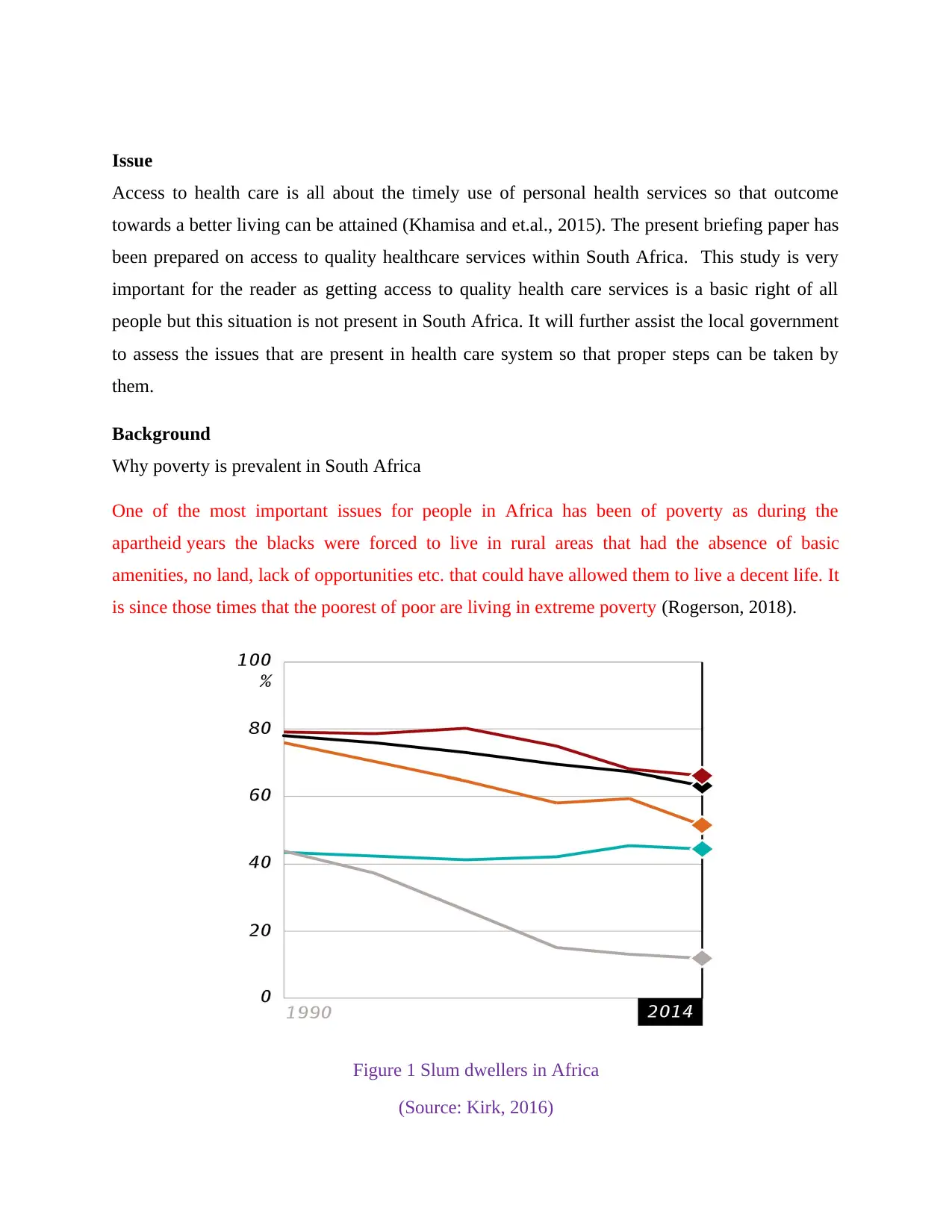
Background
Why poverty is prevalent in South Africa
One of the most important issues for people in Africa has been of poverty as during the
apartheid years the blacks were forced to live in rural areas that had the absence of basic
amenities, no land, lack of opportunities etc. that could have allowed them to live a decent life. It
is since those times that the poorest of poor are living in extreme poverty (Rogerson, 2018).
Figure 1 Slum dwellers in Africa
(Source: Kirk, 2016)
Access to health care is all about the timely use of personal health services so that outcome
towards a better living can be attained (Khamisa and et.al., 2015). The present briefing paper has
been prepared on access to quality healthcare services within South Africa. This study is very
important for the reader as getting access to quality health care services is a basic right of all
people but this situation is not present in South Africa. It will further assist the local government
to assess the issues that are present in health care system so that proper steps can be taken by
them.
Background
Why poverty is prevalent in South Africa
One of the most important issues for people in Africa has been of poverty as during the
apartheid years the blacks were forced to live in rural areas that had the absence of basic
amenities, no land, lack of opportunities etc. that could have allowed them to live a decent life. It
is since those times that the poorest of poor are living in extreme poverty (Rogerson, 2018).
Figure 1 Slum dwellers in Africa
(Source: Kirk, 2016)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
The figure given above further suggests that there are a large number of slum dwellers within
South Africa whose number has not decreased since the year 1990. Although other areas in
Africa has shown a huge decline in slum dwellers.
How poverty affects health care
It is beyond doubt that a huge relation exists between poverty and better access to health care
facilities. For 100s of years it has been found that people who belong to lowest socio-economic
levels in any nation have got higher death as well as illness rates (Mayosi and Benatar, 2014).
This correlation has been observed throughout the world regardless of whether death occurred on
account of infectious or non-infectious diseases and how the socio-economic position of the
person was measured. The impact of this relation is particular apparent in South Africa because
there is a presence of widespread poverty in the nation. The history of denial to proper health
care in South Africa goes back to early 1960s when the nation was grappled with apartheid
policies and had become quite isolated from the rest of the world (Marten and et.al. 2014).
There is also a presence of Social – cultural factors that have affected health care in South
Africa. Due to apartheid the black people in the nation were considered inferior in all contexts
and were not given a chance to come out of poverty issue. This forced them to live within
disorganized homes, made children homeless which then led to increased poverty cases thereby
leading to less access to health care facilities (Churchyard and et.al. 2014). There was also a
segregation of health care facilities during the time of 1880s on a racial basis. But then the health
act launched in 1919 gave responsibility of curative health care to 4 provinces while preventative
care to local bodies (Poku, 2017). Then came the Gluckman Commission during 1942 to 1944
which had made an attempt to redirect the health care system. The vision was to start a chain of
community health centers but then as soon as Nationalist Party came into power during 1948
there was a rejection of Gluckman recommendations entirely. Then came the collapse of the
Rand currency of South Africa in the year 1989 and a repeal against apartheid law started in all
parts of the nations followed by conduction of free election in 1994 (Khamisa and et.al., 2015).
This brought a change in the situation when first democratic elections were held and apartheid
system was brought to an end by African National Congress under the leadership of Dr Nelson
Mandela. The party established five main programs which focused on meeting the basic needs;
developing human resources; building economy; democratization of state and society as well as
South Africa whose number has not decreased since the year 1990. Although other areas in
Africa has shown a huge decline in slum dwellers.
How poverty affects health care
It is beyond doubt that a huge relation exists between poverty and better access to health care
facilities. For 100s of years it has been found that people who belong to lowest socio-economic
levels in any nation have got higher death as well as illness rates (Mayosi and Benatar, 2014).
This correlation has been observed throughout the world regardless of whether death occurred on
account of infectious or non-infectious diseases and how the socio-economic position of the
person was measured. The impact of this relation is particular apparent in South Africa because
there is a presence of widespread poverty in the nation. The history of denial to proper health
care in South Africa goes back to early 1960s when the nation was grappled with apartheid
policies and had become quite isolated from the rest of the world (Marten and et.al. 2014).
There is also a presence of Social – cultural factors that have affected health care in South
Africa. Due to apartheid the black people in the nation were considered inferior in all contexts
and were not given a chance to come out of poverty issue. This forced them to live within
disorganized homes, made children homeless which then led to increased poverty cases thereby
leading to less access to health care facilities (Churchyard and et.al. 2014). There was also a
segregation of health care facilities during the time of 1880s on a racial basis. But then the health
act launched in 1919 gave responsibility of curative health care to 4 provinces while preventative
care to local bodies (Poku, 2017). Then came the Gluckman Commission during 1942 to 1944
which had made an attempt to redirect the health care system. The vision was to start a chain of
community health centers but then as soon as Nationalist Party came into power during 1948
there was a rejection of Gluckman recommendations entirely. Then came the collapse of the
Rand currency of South Africa in the year 1989 and a repeal against apartheid law started in all
parts of the nations followed by conduction of free election in 1994 (Khamisa and et.al., 2015).
This brought a change in the situation when first democratic elections were held and apartheid
system was brought to an end by African National Congress under the leadership of Dr Nelson
Mandela. The party established five main programs which focused on meeting the basic needs;
developing human resources; building economy; democratization of state and society as well as
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
implementing the RDP. All the five programs were there to bring an improvement in the overall
level of poverty followed by health status of the country. Most importantly, the Reconstruction
and Development Programme started by Mr Mandela emphasized on the need to provide
affordable healthcare through introduction of primary health facilities so that overall health of
South African population can be maintained and improved. There was also a creation of a
fragmented health care system that had presence of separate public and private firms followed by
4 former provinces as well as 10 former homelands (Rogerson, 2018). Free health care services
were also provided to vulnerable population that included children, pregnant females as well as
old age population. Resources were redistributed in rural areas that were in high need of heath
care facilities. This also meant that health care staff were required to be retrained and encouraged
to work for rural people by serving the poorest in poor communities. There was further a
development of policy by Department of health which ensured to pay allowance to healthcare
workers who wanted to relocate (Churchyard and et.al., 2014). However, the above mentioned
changes had a set of their own challenges. One such was that although the public sector health
services were united into one but health facilities for black as well as homelands have been
lacking with respect to funding. Issues further arose as reconstruction of healthcare as well as
provision of free services led to immense burden on workers.
Current status
The current times showcase that after the end of apartheid era, South Africa has a presence of
around 40 million citizens and the government spending on the health care services in terms of
GDP has also increased but still it is poorer in terms of meeting the health care needs in
comparison to other nations (Mayosi and Benatar, 2014). Education has also affected the overall
health care of the nation as on account of poverty most of the blacks are uneducated and thus
lack knowledge about health, less vaccinations in children, presence of malnutrition, under
nutrition as well as smoking and drinking habits (Wiley and Allen, 2016). They thus fall prey to
diseases like asthma, cancer, heart diseases, depression, teenage pregnancy among others (Poku,
2017).
A range of legislative reforms have been introduced within Africa in order to provide services to
the poor such as free care for pregnancy females and children; programs to build clinics on a
widespread basis; free primary healthcare services, program to build clinics as well as National
level of poverty followed by health status of the country. Most importantly, the Reconstruction
and Development Programme started by Mr Mandela emphasized on the need to provide
affordable healthcare through introduction of primary health facilities so that overall health of
South African population can be maintained and improved. There was also a creation of a
fragmented health care system that had presence of separate public and private firms followed by
4 former provinces as well as 10 former homelands (Rogerson, 2018). Free health care services
were also provided to vulnerable population that included children, pregnant females as well as
old age population. Resources were redistributed in rural areas that were in high need of heath
care facilities. This also meant that health care staff were required to be retrained and encouraged
to work for rural people by serving the poorest in poor communities. There was further a
development of policy by Department of health which ensured to pay allowance to healthcare
workers who wanted to relocate (Churchyard and et.al., 2014). However, the above mentioned
changes had a set of their own challenges. One such was that although the public sector health
services were united into one but health facilities for black as well as homelands have been
lacking with respect to funding. Issues further arose as reconstruction of healthcare as well as
provision of free services led to immense burden on workers.
Current status
The current times showcase that after the end of apartheid era, South Africa has a presence of
around 40 million citizens and the government spending on the health care services in terms of
GDP has also increased but still it is poorer in terms of meeting the health care needs in
comparison to other nations (Mayosi and Benatar, 2014). Education has also affected the overall
health care of the nation as on account of poverty most of the blacks are uneducated and thus
lack knowledge about health, less vaccinations in children, presence of malnutrition, under
nutrition as well as smoking and drinking habits (Wiley and Allen, 2016). They thus fall prey to
diseases like asthma, cancer, heart diseases, depression, teenage pregnancy among others (Poku,
2017).
A range of legislative reforms have been introduced within Africa in order to provide services to
the poor such as free care for pregnancy females and children; programs to build clinics on a
widespread basis; free primary healthcare services, program to build clinics as well as National
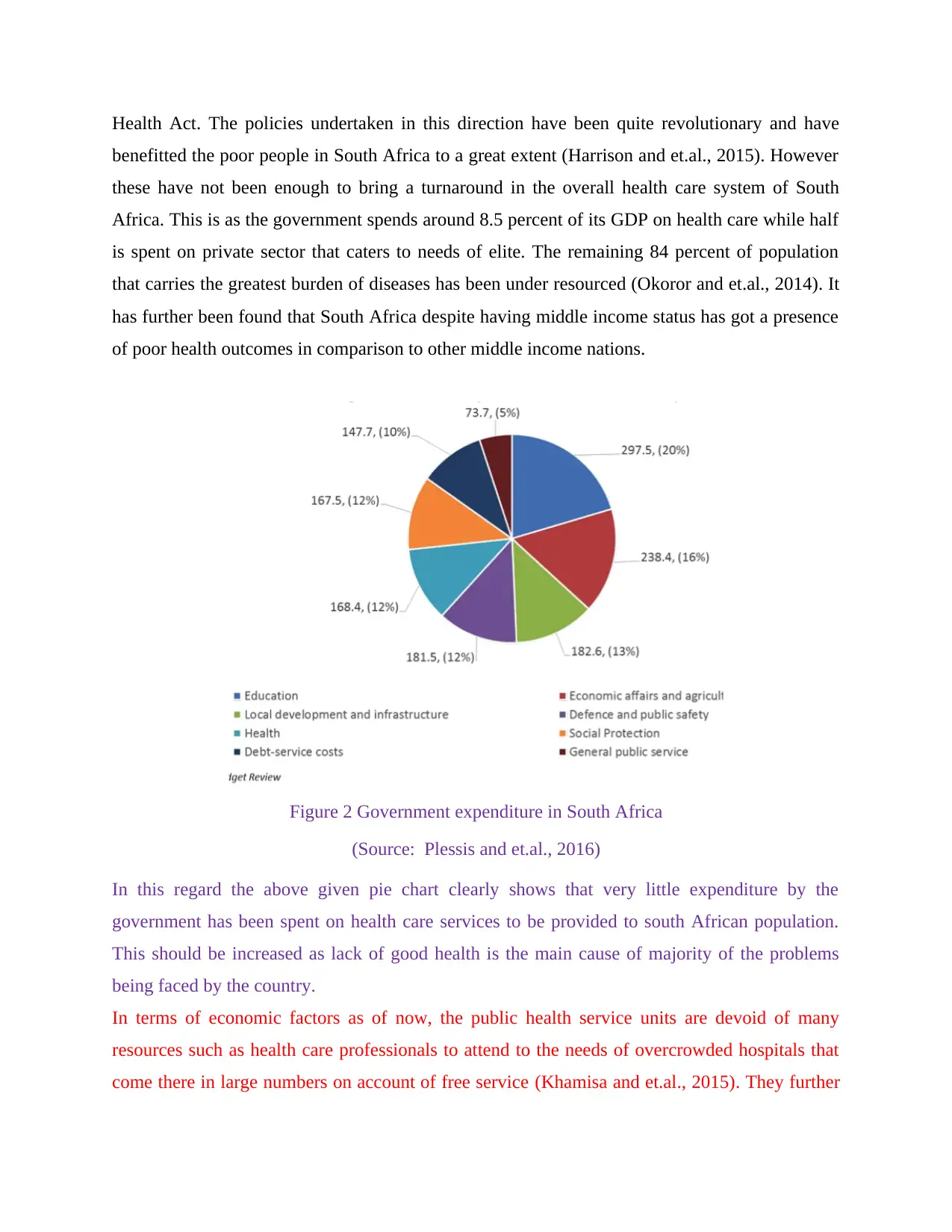
Health Act. The policies undertaken in this direction have been quite revolutionary and have
benefitted the poor people in South Africa to a great extent (Harrison and et.al., 2015). However
these have not been enough to bring a turnaround in the overall health care system of South
Africa. This is as the government spends around 8.5 percent of its GDP on health care while half
is spent on private sector that caters to needs of elite. The remaining 84 percent of population
that carries the greatest burden of diseases has been under resourced (Okoror and et.al., 2014). It
has further been found that South Africa despite having middle income status has got a presence
of poor health outcomes in comparison to other middle income nations.
Figure 2 Government expenditure in South Africa
(Source: Plessis and et.al., 2016)
In this regard the above given pie chart clearly shows that very little expenditure by the
government has been spent on health care services to be provided to south African population.
This should be increased as lack of good health is the main cause of majority of the problems
being faced by the country.
In terms of economic factors as of now, the public health service units are devoid of many
resources such as health care professionals to attend to the needs of overcrowded hospitals that
come there in large numbers on account of free service (Khamisa and et.al., 2015). They further
benefitted the poor people in South Africa to a great extent (Harrison and et.al., 2015). However
these have not been enough to bring a turnaround in the overall health care system of South
Africa. This is as the government spends around 8.5 percent of its GDP on health care while half
is spent on private sector that caters to needs of elite. The remaining 84 percent of population
that carries the greatest burden of diseases has been under resourced (Okoror and et.al., 2014). It
has further been found that South Africa despite having middle income status has got a presence
of poor health outcomes in comparison to other middle income nations.
Figure 2 Government expenditure in South Africa
(Source: Plessis and et.al., 2016)
In this regard the above given pie chart clearly shows that very little expenditure by the
government has been spent on health care services to be provided to south African population.
This should be increased as lack of good health is the main cause of majority of the problems
being faced by the country.
In terms of economic factors as of now, the public health service units are devoid of many
resources such as health care professionals to attend to the needs of overcrowded hospitals that
come there in large numbers on account of free service (Khamisa and et.al., 2015). They further
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
have a presence of limited resources in form of equipment, protective masks, syringes, medicines
etc to perform their activities. They are thus left with no option but to look for jobs in developed
nations such as UK, Australia and USA. There is also a marked differences in rates of diseases as
well as mortality between the different races. For example, the prevalence of HIV in the nation
showcase that white men and women have a very low diseases prevalence being 0.6 percent and
1.9 percent respectively whereas the highest relevance of the disease has been found in blacks
being 13.3 percent (Stoops, Williamson and Braa, 2018).
South African health care system suffers from three basic faultiness that are as follows. First
fault is in the lack of leadership by Health Minister of the nation being Aaron Motsoaledi. There
is also an issue with respect to commitment to be received from competent healthcare managers
and doctors that has led to a major failure of the healthcare system. The overall performance of
health departments was found to be compromised by the presence of fragment health care
planning; lack of proper coordination between national as well as provincial departments; and
absence of a single as well as strong health care system (Churchyard and et.al., 2014). Other than
this, corruption has also played a key role in aggreviaating the issue as the provincial health
funds of 24 billion given between 2009 and 2013 were regarded as irregular spending
(Tomlinson and et.al., 2014). It is however not known as to how much money was involved in
corruption but showcases the incompetence of public servants and presence of an inefficient
management. The second fault is with respect to compromised primary health care as the nation
still does not have a presence of district health system that is fully functional. If this is worked
upon in the right manner and at right time then proper quality and equitable health care facilities
can be ensured to people of South Africa including the poor (Poku, 2017). The third fault is with
respect to health workforce crisis in terms of maldistribution of healthcare workers amongst
urban and rural areas and also between public and private health sectors. Then there is further an
issue of Moonlighting and agency nursing that is prevalent among nurses. A cross sectional
survey was also carried out on the prevalence of agency nursing as well as moonlighting and
overtime in South Africa on around 3784 nurses of 80 hospitals (Poku, 2017). The nurses have
been found to work in critical care units, emergency firms, operation theatre etc. and they were
asked to fill up a questionnaire. The study found that more than 70 percent of the nurses were
involved either in moonlighting, overtime or agency service while one third of them did all the
three (Rispel, 2015). There is also an existence of out of the pocket system in health care sector
etc to perform their activities. They are thus left with no option but to look for jobs in developed
nations such as UK, Australia and USA. There is also a marked differences in rates of diseases as
well as mortality between the different races. For example, the prevalence of HIV in the nation
showcase that white men and women have a very low diseases prevalence being 0.6 percent and
1.9 percent respectively whereas the highest relevance of the disease has been found in blacks
being 13.3 percent (Stoops, Williamson and Braa, 2018).
South African health care system suffers from three basic faultiness that are as follows. First
fault is in the lack of leadership by Health Minister of the nation being Aaron Motsoaledi. There
is also an issue with respect to commitment to be received from competent healthcare managers
and doctors that has led to a major failure of the healthcare system. The overall performance of
health departments was found to be compromised by the presence of fragment health care
planning; lack of proper coordination between national as well as provincial departments; and
absence of a single as well as strong health care system (Churchyard and et.al., 2014). Other than
this, corruption has also played a key role in aggreviaating the issue as the provincial health
funds of 24 billion given between 2009 and 2013 were regarded as irregular spending
(Tomlinson and et.al., 2014). It is however not known as to how much money was involved in
corruption but showcases the incompetence of public servants and presence of an inefficient
management. The second fault is with respect to compromised primary health care as the nation
still does not have a presence of district health system that is fully functional. If this is worked
upon in the right manner and at right time then proper quality and equitable health care facilities
can be ensured to people of South Africa including the poor (Poku, 2017). The third fault is with
respect to health workforce crisis in terms of maldistribution of healthcare workers amongst
urban and rural areas and also between public and private health sectors. Then there is further an
issue of Moonlighting and agency nursing that is prevalent among nurses. A cross sectional
survey was also carried out on the prevalence of agency nursing as well as moonlighting and
overtime in South Africa on around 3784 nurses of 80 hospitals (Poku, 2017). The nurses have
been found to work in critical care units, emergency firms, operation theatre etc. and they were
asked to fill up a questionnaire. The study found that more than 70 percent of the nurses were
involved either in moonlighting, overtime or agency service while one third of them did all the
three (Rispel, 2015). There is also an existence of out of the pocket system in health care sector
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

of South Africa which is draining the disposable income of South Africans at high rates. The
patients in the nation are exposed to three types of pocket payments being that have to pay cash
when they approach public or private health sector. Secondly, Additional payments are also to be
done by the ones on medical scheme as it does not cover all cost. Cash payment is required to be
done by those on medical schemes whose benefit exhaust by the end of year (NATIONAL
HEALTH INSURANCE, 2018).
Key considerations
As per latest report by AnalytixBI’s on Healthcare Landscape of South Africa in 2016 it has been
found that there exists a large number of chronic diseases within the nation the highest among
them are HIV; high BP; diabetes; cancer etc. The nation has the fastest growing diabetes
epidemic in the world. There is a huge prevalence of cancer within the nation as well. For
example, a report by world bank has depicted that in the year 2012 there were 645000 new cases
of cancer and 456000 deaths on account of the disease within South Africa (Khamisa and et.al.,
2015). This is more prevalent in poor on account of less knowledge and awareness about the
disease which makes the patient reach at health care in advanced stages of the disease. The
poverty has grappled them so much that that they have to travel long distances, make financial
sacrifices so as to get a cure. Cancer in people with low socioeconomic status is more as the
white population has access to private health care which has good presence of diagnostic and
screening facilities. This is not much in case of public healthcare facilities. Asthma cases in
South Africa are more than any other continent in the world and approximately 20 percent of
school going children suffer firm it (Okoror and et.al., 2014). Out of them only 2 percent are able
to receive proper treatment and that too at the right time.
patients in the nation are exposed to three types of pocket payments being that have to pay cash
when they approach public or private health sector. Secondly, Additional payments are also to be
done by the ones on medical scheme as it does not cover all cost. Cash payment is required to be
done by those on medical schemes whose benefit exhaust by the end of year (NATIONAL
HEALTH INSURANCE, 2018).
Key considerations
As per latest report by AnalytixBI’s on Healthcare Landscape of South Africa in 2016 it has been
found that there exists a large number of chronic diseases within the nation the highest among
them are HIV; high BP; diabetes; cancer etc. The nation has the fastest growing diabetes
epidemic in the world. There is a huge prevalence of cancer within the nation as well. For
example, a report by world bank has depicted that in the year 2012 there were 645000 new cases
of cancer and 456000 deaths on account of the disease within South Africa (Khamisa and et.al.,
2015). This is more prevalent in poor on account of less knowledge and awareness about the
disease which makes the patient reach at health care in advanced stages of the disease. The
poverty has grappled them so much that that they have to travel long distances, make financial
sacrifices so as to get a cure. Cancer in people with low socioeconomic status is more as the
white population has access to private health care which has good presence of diagnostic and
screening facilities. This is not much in case of public healthcare facilities. Asthma cases in
South Africa are more than any other continent in the world and approximately 20 percent of
school going children suffer firm it (Okoror and et.al., 2014). Out of them only 2 percent are able
to receive proper treatment and that too at the right time.
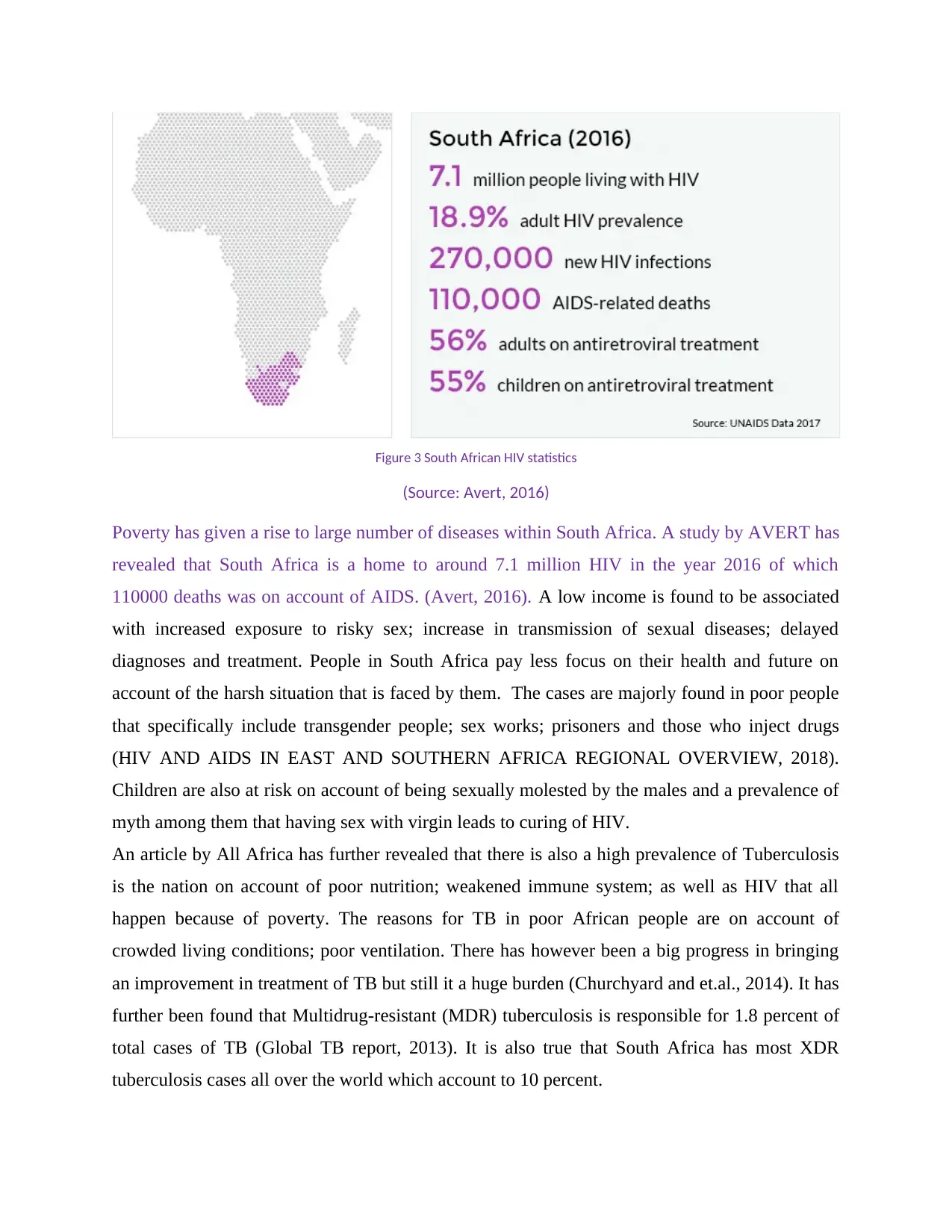
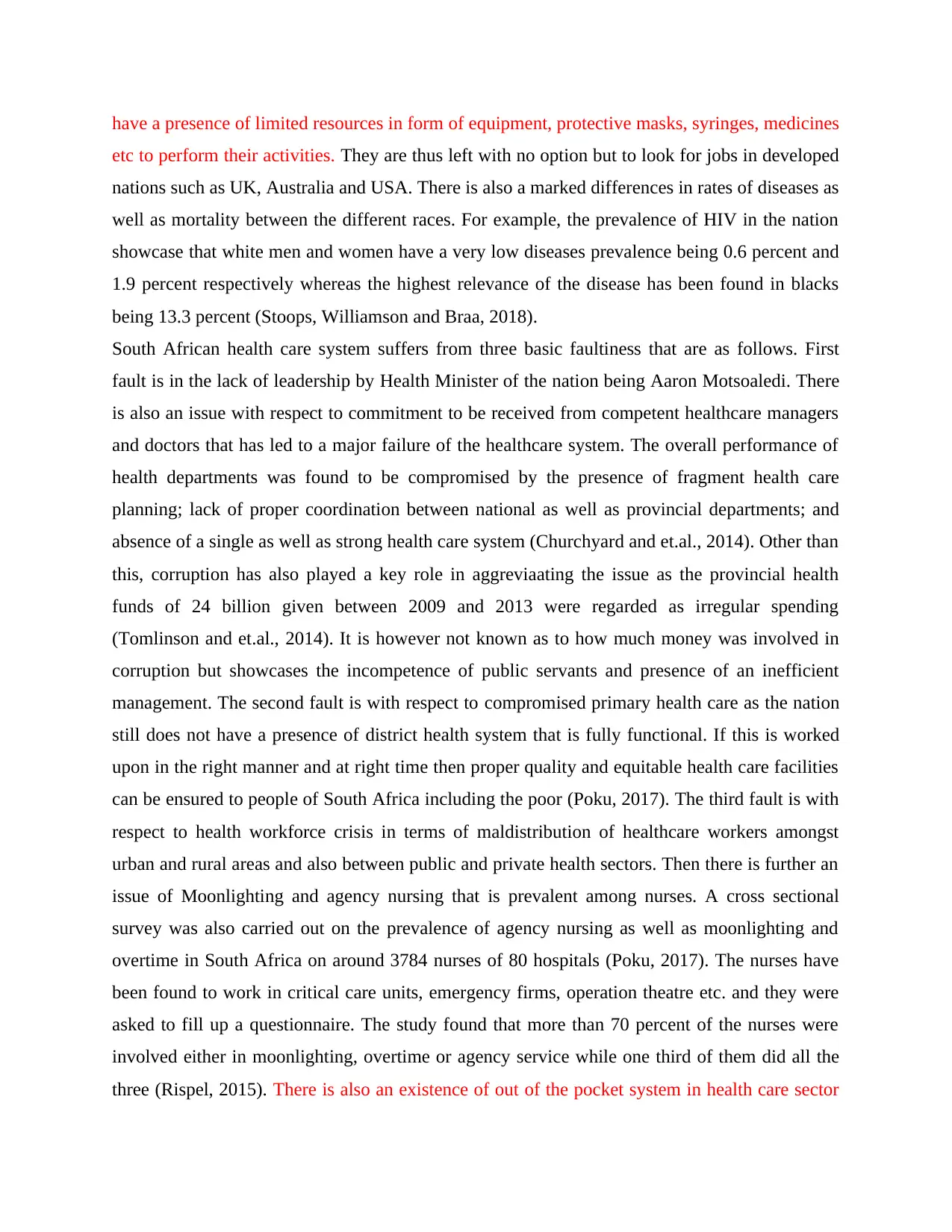
Figure 3 South African HIV statistics
(Source: Avert, 2016)
Poverty has given a rise to large number of diseases within South Africa. A study by AVERT has
revealed that South Africa is a home to around 7.1 million HIV in the year 2016 of which
110000 deaths was on account of AIDS. (Avert, 2016). A low income is found to be associated
with increased exposure to risky sex; increase in transmission of sexual diseases; delayed
diagnoses and treatment. People in South Africa pay less focus on their health and future on
account of the harsh situation that is faced by them. The cases are majorly found in poor people
that specifically include transgender people; sex works; prisoners and those who inject drugs
(HIV AND AIDS IN EAST AND SOUTHERN AFRICA REGIONAL OVERVIEW, 2018).
Children are also at risk on account of being sexually molested by the males and a prevalence of
myth among them that having sex with virgin leads to curing of HIV.
An article by All Africa has further revealed that there is also a high prevalence of Tuberculosis
is the nation on account of poor nutrition; weakened immune system; as well as HIV that all
happen because of poverty. The reasons for TB in poor African people are on account of
crowded living conditions; poor ventilation. There has however been a big progress in bringing
an improvement in treatment of TB but still it a huge burden (Churchyard and et.al., 2014). It has
further been found that Multidrug-resistant (MDR) tuberculosis is responsible for 1.8 percent of
total cases of TB (Global TB report, 2013). It is also true that South Africa has most XDR
tuberculosis cases all over the world which account to 10 percent.
(Source: Avert, 2016)
Poverty has given a rise to large number of diseases within South Africa. A study by AVERT has
revealed that South Africa is a home to around 7.1 million HIV in the year 2016 of which
110000 deaths was on account of AIDS. (Avert, 2016). A low income is found to be associated
with increased exposure to risky sex; increase in transmission of sexual diseases; delayed
diagnoses and treatment. People in South Africa pay less focus on their health and future on
account of the harsh situation that is faced by them. The cases are majorly found in poor people
that specifically include transgender people; sex works; prisoners and those who inject drugs
(HIV AND AIDS IN EAST AND SOUTHERN AFRICA REGIONAL OVERVIEW, 2018).
Children are also at risk on account of being sexually molested by the males and a prevalence of
myth among them that having sex with virgin leads to curing of HIV.
An article by All Africa has further revealed that there is also a high prevalence of Tuberculosis
is the nation on account of poor nutrition; weakened immune system; as well as HIV that all
happen because of poverty. The reasons for TB in poor African people are on account of
crowded living conditions; poor ventilation. There has however been a big progress in bringing
an improvement in treatment of TB but still it a huge burden (Churchyard and et.al., 2014). It has
further been found that Multidrug-resistant (MDR) tuberculosis is responsible for 1.8 percent of
total cases of TB (Global TB report, 2013). It is also true that South Africa has most XDR
tuberculosis cases all over the world which account to 10 percent.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Options
Health care changes for the good of people are constantly taking place in South Africa but
history is constantly trying to show on surface through present situations. For example, apartheid
is marked so heavily in the minds of African population that discrimination in health care figures
for white and blacks can still be observed. In this regard, in order to reduce poverty as well as
promote health in South African nation there is a need for economy to take a growth path. It is
important for the policy makers within South Africa to focus on human capital and try to attain
sustainable socioeconomic development. Economic growth that leads to poverty alleviation and
improved health of people can only be fuelled through creative and physical capabilities of
people.
It is a huge requirement that the attention is diverted on crucial factors that influence of the
overall health status of South African population. This is because overall health of the population
has already been compromised on the grounds of colonial past, apartheid, economic disparities,
corruption, incompetence as well as a delay in applying bwbwigrs of medical advances to all the
people.
In this regard, there is a need to work on dysfunctional public health sector by increasing the
overall efficiency as well as effectiveness of managerial practices. Priorities are further required
to be set for the usage and supply of resources for public health care sector in South Africa which
should be utilized in an efficient manner. There is also a need to train and motivate health care
workers from time to time so that there number and efficiency increases to meet the needs of
widespread population in the nation.
Conclusion and recommendation
From the above report it can be concluded that the South African continent since a long time was
grappled with poverty and issue of apartheid that led to decrease in health care facilities provided
to the masses. The blacks were forced to live in disorganized homes, had lack of sanitation
facilities followed by absence of any proper health care facilities for them. Situation however
improved after the end of apartheid in 1994 when several legal policies and programs were
brought in place to provide health care facilities to the masses. But the current times still
showcase that although there has been a substantial increase in the government spending on
health care but still the nation stands to poor in terms of meeting the health care needs in
Health care changes for the good of people are constantly taking place in South Africa but
history is constantly trying to show on surface through present situations. For example, apartheid
is marked so heavily in the minds of African population that discrimination in health care figures
for white and blacks can still be observed. In this regard, in order to reduce poverty as well as
promote health in South African nation there is a need for economy to take a growth path. It is
important for the policy makers within South Africa to focus on human capital and try to attain
sustainable socioeconomic development. Economic growth that leads to poverty alleviation and
improved health of people can only be fuelled through creative and physical capabilities of
people.
It is a huge requirement that the attention is diverted on crucial factors that influence of the
overall health status of South African population. This is because overall health of the population
has already been compromised on the grounds of colonial past, apartheid, economic disparities,
corruption, incompetence as well as a delay in applying bwbwigrs of medical advances to all the
people.
In this regard, there is a need to work on dysfunctional public health sector by increasing the
overall efficiency as well as effectiveness of managerial practices. Priorities are further required
to be set for the usage and supply of resources for public health care sector in South Africa which
should be utilized in an efficient manner. There is also a need to train and motivate health care
workers from time to time so that there number and efficiency increases to meet the needs of
widespread population in the nation.
Conclusion and recommendation
From the above report it can be concluded that the South African continent since a long time was
grappled with poverty and issue of apartheid that led to decrease in health care facilities provided
to the masses. The blacks were forced to live in disorganized homes, had lack of sanitation
facilities followed by absence of any proper health care facilities for them. Situation however
improved after the end of apartheid in 1994 when several legal policies and programs were
brought in place to provide health care facilities to the masses. But the current times still
showcase that although there has been a substantial increase in the government spending on
health care but still the nation stands to poor in terms of meeting the health care needs in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

comparison to other nations. The health care system has further been divided into private sector
that caters to need of elite while public sector which is there for general population. However a
huge amount of disparity exists between the two on account of under sourced public health
sector; overcrowded units; overworked and underpaid doctors; lack of commitment from
competent healthcare managers and doctors; corruption; Moonlighting and agency nursing
among others. In short, the public health sector is not enough to meet the needs of 84 percent of
population that have high incidences of diseases as compared to rest of the population. Al this
has resulted in the creation of many chronic diseases such as cancer, diabetes, tuberculosis that is
taking the life of people in large numbers. In this regard, various steps are required to be taken by
the South African government that is as follows;
The nation should strengthen the overall leadership as well as governance of public as
well as private health care firms in order to gain the confidence of the stakeholders. This
can be done by investing heavily in the district and community health systems.
Government is required to follow innovative strategies to raise the revenue for domestic
heath care sources so that essential services can be provided to the entire population.
There is further a need to develop adequate infrastructure so that high quality medicines;
vaccines and innovative therapies can be provided to the patients.
Teleconsultation centers should further be established in the remote villages through the
usage of mobile technology where health workers should speak with staff on phone to
make treatment decisions. This can be done through use of programs carried out through
public and private partnerships where government can work on infrastructure support
while private sector can take care of funding.
that caters to need of elite while public sector which is there for general population. However a
huge amount of disparity exists between the two on account of under sourced public health
sector; overcrowded units; overworked and underpaid doctors; lack of commitment from
competent healthcare managers and doctors; corruption; Moonlighting and agency nursing
among others. In short, the public health sector is not enough to meet the needs of 84 percent of
population that have high incidences of diseases as compared to rest of the population. Al this
has resulted in the creation of many chronic diseases such as cancer, diabetes, tuberculosis that is
taking the life of people in large numbers. In this regard, various steps are required to be taken by
the South African government that is as follows;
The nation should strengthen the overall leadership as well as governance of public as
well as private health care firms in order to gain the confidence of the stakeholders. This
can be done by investing heavily in the district and community health systems.
Government is required to follow innovative strategies to raise the revenue for domestic
heath care sources so that essential services can be provided to the entire population.
There is further a need to develop adequate infrastructure so that high quality medicines;
vaccines and innovative therapies can be provided to the patients.
Teleconsultation centers should further be established in the remote villages through the
usage of mobile technology where health workers should speak with staff on phone to
make treatment decisions. This can be done through use of programs carried out through
public and private partnerships where government can work on infrastructure support
while private sector can take care of funding.
References
Avert, 2016. HIV and AIDS in South Africa. [Online]. Available through:
<https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/south-africa/>
[Accessed on 13th May 2018].
Churchyard, G.J. and et.al., 2014. Tuberculosis control in South Africa: Successes, challenges
and recommendations. SAMJ: South African Medical Journal. 104(3). pp.234-248.
Global tuberculosis report. Geneva: World Health Organization, 2013 [Online]. Available
through: <http://www.who.int/tb/publications/global_report/en. /> [Accessed on 26th
April 2018].
Harrison, A. and et.al., 2015. Sustained high HIV incidence in young women in Southern Africa:
social, behavioral, and structural factors and emerging intervention approaches. Current
HIV/AIDS Reports. 12(2). pp.207-215.
HIV AND AIDS IN EAST AND SOUTHERN AFRICA REGIONAL OVERVIEW. 2018. [Online].
Available through: <HTTPS://WWW.AVERT.ORG/PROFESSIONALS/HIV-
AROUND-WORLD/SUB-SAHARAN-AFRICA/OVERVIEW/> [Accessed on 26th April
2018].
Khamisa, N. and et.al., 2015. Work related stress, burnout, job satisfaction and general health of
nurses. International journal of environmental research and public health. 12(1). pp.652-
666.
Kirk, A., 2016. What Africa will look like in 100 years. [Online]. Available through:
<https://s.telegraph.co.uk/graphics/projects/Africa-in-100-years//> [Accessed on 13th May
2018].
Marten, R., McIntyre, D., Travassos, C., Shishkin, S., Longde, W., Reddy, S. and Vega, J., 2014.
An assessment of progress towards universal health coverage in Brazil, Russia, India,
China, and South Africa (BRICS). The Lancet. 384(9960). pp.2164-2171.
Avert, 2016. HIV and AIDS in South Africa. [Online]. Available through:
<https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/south-africa/>
[Accessed on 13th May 2018].
Churchyard, G.J. and et.al., 2014. Tuberculosis control in South Africa: Successes, challenges
and recommendations. SAMJ: South African Medical Journal. 104(3). pp.234-248.
Global tuberculosis report. Geneva: World Health Organization, 2013 [Online]. Available
through: <http://www.who.int/tb/publications/global_report/en. /> [Accessed on 26th
April 2018].
Harrison, A. and et.al., 2015. Sustained high HIV incidence in young women in Southern Africa:
social, behavioral, and structural factors and emerging intervention approaches. Current
HIV/AIDS Reports. 12(2). pp.207-215.
HIV AND AIDS IN EAST AND SOUTHERN AFRICA REGIONAL OVERVIEW. 2018. [Online].
Available through: <HTTPS://WWW.AVERT.ORG/PROFESSIONALS/HIV-
AROUND-WORLD/SUB-SAHARAN-AFRICA/OVERVIEW/> [Accessed on 26th April
2018].
Khamisa, N. and et.al., 2015. Work related stress, burnout, job satisfaction and general health of
nurses. International journal of environmental research and public health. 12(1). pp.652-
666.
Kirk, A., 2016. What Africa will look like in 100 years. [Online]. Available through:
<https://s.telegraph.co.uk/graphics/projects/Africa-in-100-years//> [Accessed on 13th May
2018].
Marten, R., McIntyre, D., Travassos, C., Shishkin, S., Longde, W., Reddy, S. and Vega, J., 2014.
An assessment of progress towards universal health coverage in Brazil, Russia, India,
China, and South Africa (BRICS). The Lancet. 384(9960). pp.2164-2171.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.