Reflective Journal: Insulin Administration in Patient 7
VerifiedAdded on 2020/05/11
|9
|2430
|4515
Journal and Reflective Writing
AI Summary
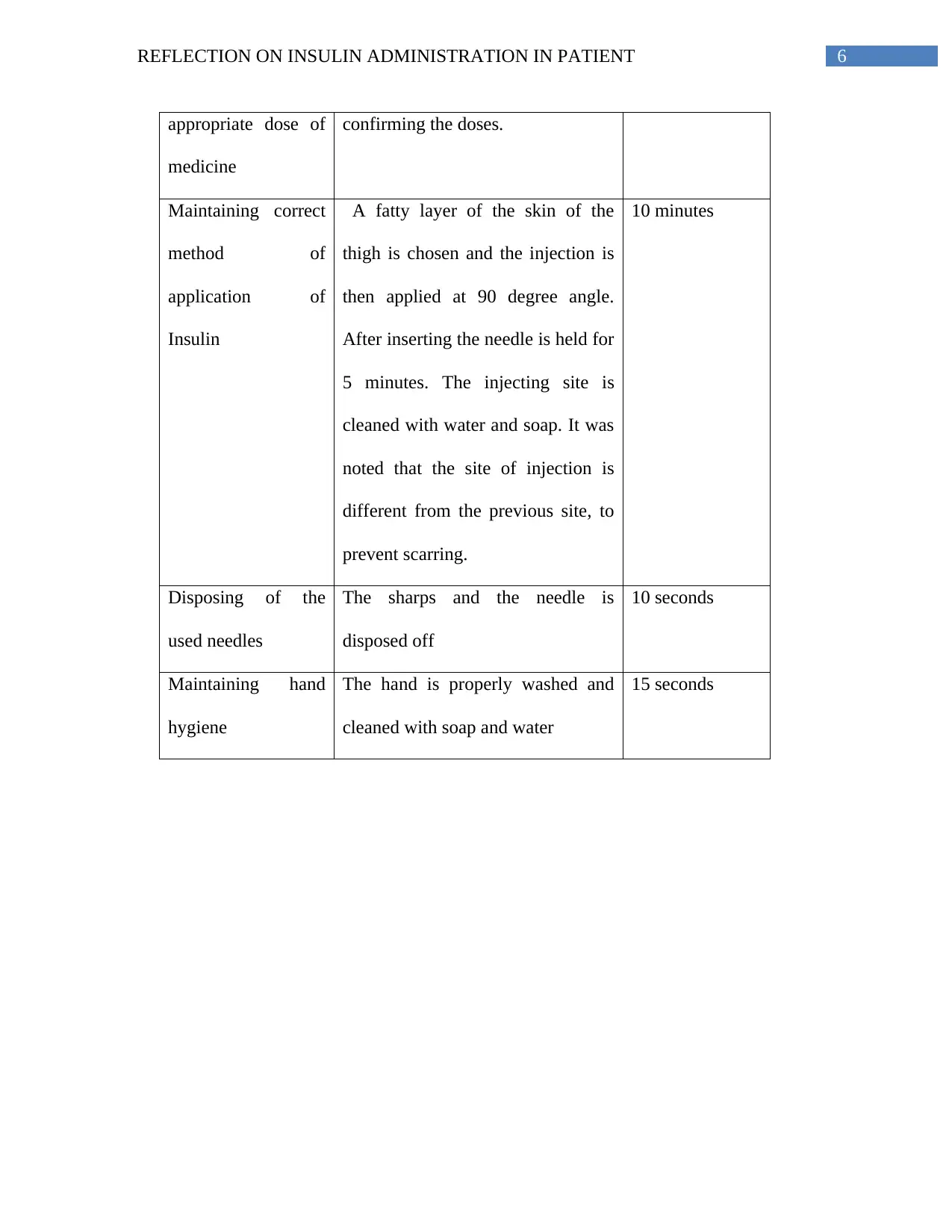
This reflective journal details a nursing student's experience administering subcutaneous insulin to a patient with type 1 diabetes post-surgery. The student discusses the assessment of vital signs, the importance of safe medication practices, and the challenges encountered, such as selecting the appropriate injection site due to the patient's recent umbilical hernia surgery. The reflection covers the student's feelings, evaluation of the process, and analysis of relevant factors like insulin types, injection techniques, and the importance of aseptic conditions. The student identifies areas for improvement, including gaining more confidence and proficiency, and outlines an action plan to enhance skills in medication administration, site selection, and maintaining an aseptic environment. The document also references key nursing principles and research related to insulin administration and patient safety, including the six rights of medication administration and the importance of hand hygiene.



1 out of 9
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.