Epidemiology Assignment: Public Health Study Designs and Data Analysis
VerifiedAdded on 2020/04/01
|9
|3198
|33
Homework Assignment
AI Summary
This epidemiology assignment explores two study designs: a cohort study on coronary heart disease (CHD) and a cross-sectional study on breast cancer. The CHD study investigates the relationship between physical activity and the incidence of CHD, analyzing data on incidence rates, relative risks, and the impact of physical activity levels. The assignment assesses the study's methodology, justifications, and potential biases. The breast cancer study examines the association between the drug Reserpine and breast cancer prevalence, including the creation of a 2x2 table and the calculation of the population attributable risk (PAF) to estimate the impact of banning Reserpine. The assignment highlights the importance of study design, data analysis, and the identification of risk factors in public health research.

Running head: EPIDEMIOLOGY 1
RESEARCH METHODOLOGIES IN EPIDEMIOLOGY
Student Name
Student ID
Date
RESEARCH METHODOLOGIES IN EPIDEMIOLOGY
Student Name
Student ID
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
EPIDEMIOLOGY 2
Question one
a) ``What study design does this study employ``? [1point]
The study uses a cohort study design. A cohort study depicts a clinical research
study in which individuals who currently have a particular condition or illness or get
a given treatment are followed over time. Normally, different study designs give
information of varied quality (Mark, 2013). This evidently implies that the choice
of the study design by any given researcher influences the quality of the information
generated in the particular study. As such, it is indispensable for any researcher to
be prudent when identifying the most appropriate study design to adequately
address all the necessary study elements.
b) ``Find the methodological aspects mentioned in the paper that convinced you
that is the type of study design, please use dot points`` [2points]
The data collection aspect. In the research paper, the data involving the national
random sample of 2,645 men and 2,551 women aged between 35 and 74 were
gathered in the years 1988 and 1989 respectively, after which they were perpetually
monitored concerning incident cases of CHD until December 31, 2000. As such,
the duration for data collection was continuous although it was done on the original
sample size.
The data analysis aspect. As vividly evident in the research paper, the data
collected in the study was analyzed after the completion of the follow-up on the
initial random sample subjects. This implies that the records from the responses to
the interview and questionnaires questions and the follow-up observations on the
study subjects were conclusively analyzed at the end of the study period on
December 31, 2000.
c) ``What justification do the authors give for conducting this study, please use dot
points`` [2points]
To adequately address the gap of the absence of holistic inclusivity of study subjects
from varied socioeconomic status in the sample in the previous researches. They
argue that in the previous research studies, there has been an overt lack of a
wholesome inclusivity when selecting the study sample. For instance, the authors
argue that a majority of the previous researches on the association between physical
inactivity and CHD have failed to include individuals with low socioeconomic status
(SES). As such, they are seeking to bridge this particular gap by including individuals
from the low socioeconomic status as well as those from other socioeconomic
statuses.
The need to include both genders, that is, both men and women in the study to counter
the lack of such inclusivity by the previous researchers. According to them, such an
inclusivity of the two genders would produce more reflective and reliable conclusions
in the study. For example, they point out the relative neglect of women in the studies
of CHD epidemiology. Evidently, including both men and women in their study is a
chief reason for motivating them to conduct this particular study.
Question one
a) ``What study design does this study employ``? [1point]
The study uses a cohort study design. A cohort study depicts a clinical research
study in which individuals who currently have a particular condition or illness or get
a given treatment are followed over time. Normally, different study designs give
information of varied quality (Mark, 2013). This evidently implies that the choice
of the study design by any given researcher influences the quality of the information
generated in the particular study. As such, it is indispensable for any researcher to
be prudent when identifying the most appropriate study design to adequately
address all the necessary study elements.
b) ``Find the methodological aspects mentioned in the paper that convinced you
that is the type of study design, please use dot points`` [2points]
The data collection aspect. In the research paper, the data involving the national
random sample of 2,645 men and 2,551 women aged between 35 and 74 were
gathered in the years 1988 and 1989 respectively, after which they were perpetually
monitored concerning incident cases of CHD until December 31, 2000. As such,
the duration for data collection was continuous although it was done on the original
sample size.
The data analysis aspect. As vividly evident in the research paper, the data
collected in the study was analyzed after the completion of the follow-up on the
initial random sample subjects. This implies that the records from the responses to
the interview and questionnaires questions and the follow-up observations on the
study subjects were conclusively analyzed at the end of the study period on
December 31, 2000.
c) ``What justification do the authors give for conducting this study, please use dot
points`` [2points]
To adequately address the gap of the absence of holistic inclusivity of study subjects
from varied socioeconomic status in the sample in the previous researches. They
argue that in the previous research studies, there has been an overt lack of a
wholesome inclusivity when selecting the study sample. For instance, the authors
argue that a majority of the previous researches on the association between physical
inactivity and CHD have failed to include individuals with low socioeconomic status
(SES). As such, they are seeking to bridge this particular gap by including individuals
from the low socioeconomic status as well as those from other socioeconomic
statuses.
The need to include both genders, that is, both men and women in the study to counter
the lack of such inclusivity by the previous researchers. According to them, such an
inclusivity of the two genders would produce more reflective and reliable conclusions
in the study. For example, they point out the relative neglect of women in the studies
of CHD epidemiology. Evidently, including both men and women in their study is a
chief reason for motivating them to conduct this particular study.
EPIDEMIOLOGY 3
d) ``What was the proportion of those who (i) do not do any physical activity (ii)
engaged in twice a week vigorous physical activity``? (You are not required to
report 95% confidence intervals) [2points]
The proportion of the individuals who do not perform any physical activity at all
according to the results table is 9.0%, which represents a sample size of 463 out of the
total sample size of 5191.
Based on the results table in the research, the proportion of those who took part in
twice a week vigorous physical activity was 10.9%, which reflects a sample size of
563 out of the overall sample size of 5191.
e) ``What is the crude incidence rate of CHD in inactive men and inactive
women``? [2points]
In this case, the crude incidence rate describes the number of new coronary heart
diseases in both the inactive men and women during a given period, expressed as the
number such cases per 10,000 population at risk. As such, the crude incident rate of
CHD in physically inactive men is 111.
For the case of women, the crude incident rate is 38.
f) ``What is the crude relative risk of being non-active versus being ``highly
active``(`vigorous physical activity at least twice a week) in men and` women``
[2points]
For men, it is 111:61
For women, it is 38:14
g) ``How would you interpret the relative risk in the above section f?`` [2points]
The relative risk in both the genders exhibits a similar trend. That is, the crude risk is
high for men and women who do not perform any active physical activity at all while,
on the other hand, those who engage in vigorous physical activity twice or more than
twice a week have a lower crude risk. This means that the highly physically active a
person is the higher the possibilities of not suffering from CHD conditions. Similarly,
the opposite is vividly true. Based on this observation, it is therefore advisable for
individuals to engage in physically active and if possible vigorous physical activities
two or more times in a week. This will lower the chances of them having such life-
threatening CHD conditions. This should be encouraged across the board, that is, in
both men and women of all ages.
h) ‘Looking at the sex and age-adjusted RR in Table 3 (the RR is measured by the
Hazard Ratio which is similar) (i) how would you describe the association
between physical activity and CHD” [4 points]
Men and women who were completely physically inactive have increased chances of
suffering from CHD. This is expressed in the HR=1 as shown in the table. This
implies that such people face a highly possible likelihood of contracting CHD
conditions and this is attributed to the absence of physical activities in their lives.
This illustration should quite serve as a warning to those people who are reluctant or
lazy about performing some active physical activities in their lives. They should see
it as an opportunity to avert such possible chances of getting CHD. Evidently, they
can achieve this by starting with simple regular physical exercises at their home or
work places if possible.
d) ``What was the proportion of those who (i) do not do any physical activity (ii)
engaged in twice a week vigorous physical activity``? (You are not required to
report 95% confidence intervals) [2points]
The proportion of the individuals who do not perform any physical activity at all
according to the results table is 9.0%, which represents a sample size of 463 out of the
total sample size of 5191.
Based on the results table in the research, the proportion of those who took part in
twice a week vigorous physical activity was 10.9%, which reflects a sample size of
563 out of the overall sample size of 5191.
e) ``What is the crude incidence rate of CHD in inactive men and inactive
women``? [2points]
In this case, the crude incidence rate describes the number of new coronary heart
diseases in both the inactive men and women during a given period, expressed as the
number such cases per 10,000 population at risk. As such, the crude incident rate of
CHD in physically inactive men is 111.
For the case of women, the crude incident rate is 38.
f) ``What is the crude relative risk of being non-active versus being ``highly
active``(`vigorous physical activity at least twice a week) in men and` women``
[2points]
For men, it is 111:61
For women, it is 38:14
g) ``How would you interpret the relative risk in the above section f?`` [2points]
The relative risk in both the genders exhibits a similar trend. That is, the crude risk is
high for men and women who do not perform any active physical activity at all while,
on the other hand, those who engage in vigorous physical activity twice or more than
twice a week have a lower crude risk. This means that the highly physically active a
person is the higher the possibilities of not suffering from CHD conditions. Similarly,
the opposite is vividly true. Based on this observation, it is therefore advisable for
individuals to engage in physically active and if possible vigorous physical activities
two or more times in a week. This will lower the chances of them having such life-
threatening CHD conditions. This should be encouraged across the board, that is, in
both men and women of all ages.
h) ‘Looking at the sex and age-adjusted RR in Table 3 (the RR is measured by the
Hazard Ratio which is similar) (i) how would you describe the association
between physical activity and CHD” [4 points]
Men and women who were completely physically inactive have increased chances of
suffering from CHD. This is expressed in the HR=1 as shown in the table. This
implies that such people face a highly possible likelihood of contracting CHD
conditions and this is attributed to the absence of physical activities in their lives.
This illustration should quite serve as a warning to those people who are reluctant or
lazy about performing some active physical activities in their lives. They should see
it as an opportunity to avert such possible chances of getting CHD. Evidently, they
can achieve this by starting with simple regular physical exercises at their home or
work places if possible.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
EPIDEMIOLOGY 4
Women and men who engaged in occasional physical activities have relatively
reduced risks of having CHD compared to those who did not perform any physical
activity at all. There HR=0.72. This is slightly lower than the HR=1 of those who did
not engage in any physical activity totally. As such, at this level, the individuals in
this category are at better placed regarding susceptibility to CHD compared to their
counterparts in the above-mentioned group.
The men and women who performed physical activities once to twice a week had
quite lower possibility of getting CHD relative to their counterparts who did
occasional physical activities. This is exhibited in their HR=0.64. Evidently, there is
an overt reduction from the HR of 0.72 faced by those who do occasional physical
exercises to an HR of 0.64 in those who engaged in physical activities once or twice
in every week.
`There was a significantly lower risk of developing` CHD for men and women who
performed vigorous physical activities at least twice each week. This is indicated by
their HD=0.46 in the illustration table in the research study. As such, this cadre of
people have a reduced risk of 0.54 relative to the risk faced by those who did not
perform any physical activity at all of contracting CHD. As a result, this statistic
should serve as a key motivator to those men and women who would wish or desire to
have higher chances of averting CHD conditions in their lives regardless of their age.
However, this should be a great motivator to the young people who are normally
energetic and vibrant. This will enable them to live a healthy life devoid of CHD
conditions throughout their lives.
i) ‘The authors removed from the analysis any person who self-rated their health
as “bad” or “anywhere between good and bad” why? (one sentence [2 points]
The authors wanted only those respondents who had good self-rated health which
provided the possibility of such individuals having good health.
j) “`What possible bias could have changed the estimate for the association
between physical activity and CHD` – mention at least one, and explain why” [2
points]
The high non-response rate of 21.8% in the study. This nonresponse rate was quite
high in such a study. As such, this could lead to possible bias in the association
results. This may imply that people with CHD conditions were either particularly
reluctant or anxious in taking part in that particular study. This nonresponse rate
could imply that those who responded to the comprehensive interview questions were
possibly those who are open about their health status. On the other hand, the
individuals who did not give their responses may be those who felt that concealing
their health status is the best thing to do. As such, there exist the possibility of bias in
the conclusively analyzed results of the study on the relationship between physical
activity and CHD.
The reliance on patients treated at the hospitals. Patients attended to at the hospitals
for CHD conditions are not representative of the entire patients with this condition.
This is because the patients with mild CHD conditions or extremely severe ones (so
severe that there exist immense chances of them dying before arriving at the hospital)
will normally tend to be excluded from the research or study. It is not certainly
Women and men who engaged in occasional physical activities have relatively
reduced risks of having CHD compared to those who did not perform any physical
activity at all. There HR=0.72. This is slightly lower than the HR=1 of those who did
not engage in any physical activity totally. As such, at this level, the individuals in
this category are at better placed regarding susceptibility to CHD compared to their
counterparts in the above-mentioned group.
The men and women who performed physical activities once to twice a week had
quite lower possibility of getting CHD relative to their counterparts who did
occasional physical activities. This is exhibited in their HR=0.64. Evidently, there is
an overt reduction from the HR of 0.72 faced by those who do occasional physical
exercises to an HR of 0.64 in those who engaged in physical activities once or twice
in every week.
`There was a significantly lower risk of developing` CHD for men and women who
performed vigorous physical activities at least twice each week. This is indicated by
their HD=0.46 in the illustration table in the research study. As such, this cadre of
people have a reduced risk of 0.54 relative to the risk faced by those who did not
perform any physical activity at all of contracting CHD. As a result, this statistic
should serve as a key motivator to those men and women who would wish or desire to
have higher chances of averting CHD conditions in their lives regardless of their age.
However, this should be a great motivator to the young people who are normally
energetic and vibrant. This will enable them to live a healthy life devoid of CHD
conditions throughout their lives.
i) ‘The authors removed from the analysis any person who self-rated their health
as “bad” or “anywhere between good and bad” why? (one sentence [2 points]
The authors wanted only those respondents who had good self-rated health which
provided the possibility of such individuals having good health.
j) “`What possible bias could have changed the estimate for the association
between physical activity and CHD` – mention at least one, and explain why” [2
points]
The high non-response rate of 21.8% in the study. This nonresponse rate was quite
high in such a study. As such, this could lead to possible bias in the association
results. This may imply that people with CHD conditions were either particularly
reluctant or anxious in taking part in that particular study. This nonresponse rate
could imply that those who responded to the comprehensive interview questions were
possibly those who are open about their health status. On the other hand, the
individuals who did not give their responses may be those who felt that concealing
their health status is the best thing to do. As such, there exist the possibility of bias in
the conclusively analyzed results of the study on the relationship between physical
activity and CHD.
The reliance on patients treated at the hospitals. Patients attended to at the hospitals
for CHD conditions are not representative of the entire patients with this condition.
This is because the patients with mild CHD conditions or extremely severe ones (so
severe that there exist immense chances of them dying before arriving at the hospital)
will normally tend to be excluded from the research or study. It is not certainly
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
EPIDEMIOLOGY 5
possible to establish whether an individual is mildly suffering from CHD particularly
when interviewing them. As a result, such a crucial group of people perhaps end up
being not considered in the research. Essentially, both those with mild CHD
conditions and those suffering from extreme CHD conditions can remarkably account
for the reliability, accuracy, and validity of the study results. This is because
including such people will holistically give a representative sample that reflects the
entire target population or rather the population under study.
k) “Do you think this research adequately addressed `confounders`? `Justify your
answers` `{no more than 60 words}” [2 points]`
Yes, it has quite satisfactorily addressed the necessary confounders. It has evidently
employed age as a confounder in a complete manner. The age distribution in the
study is different in the exposure categories being compared. It has shown its
association with exposure and outcome. Additionally, BMI has been addressed. It
impacts both physical activity and CHD conditions.
Question two
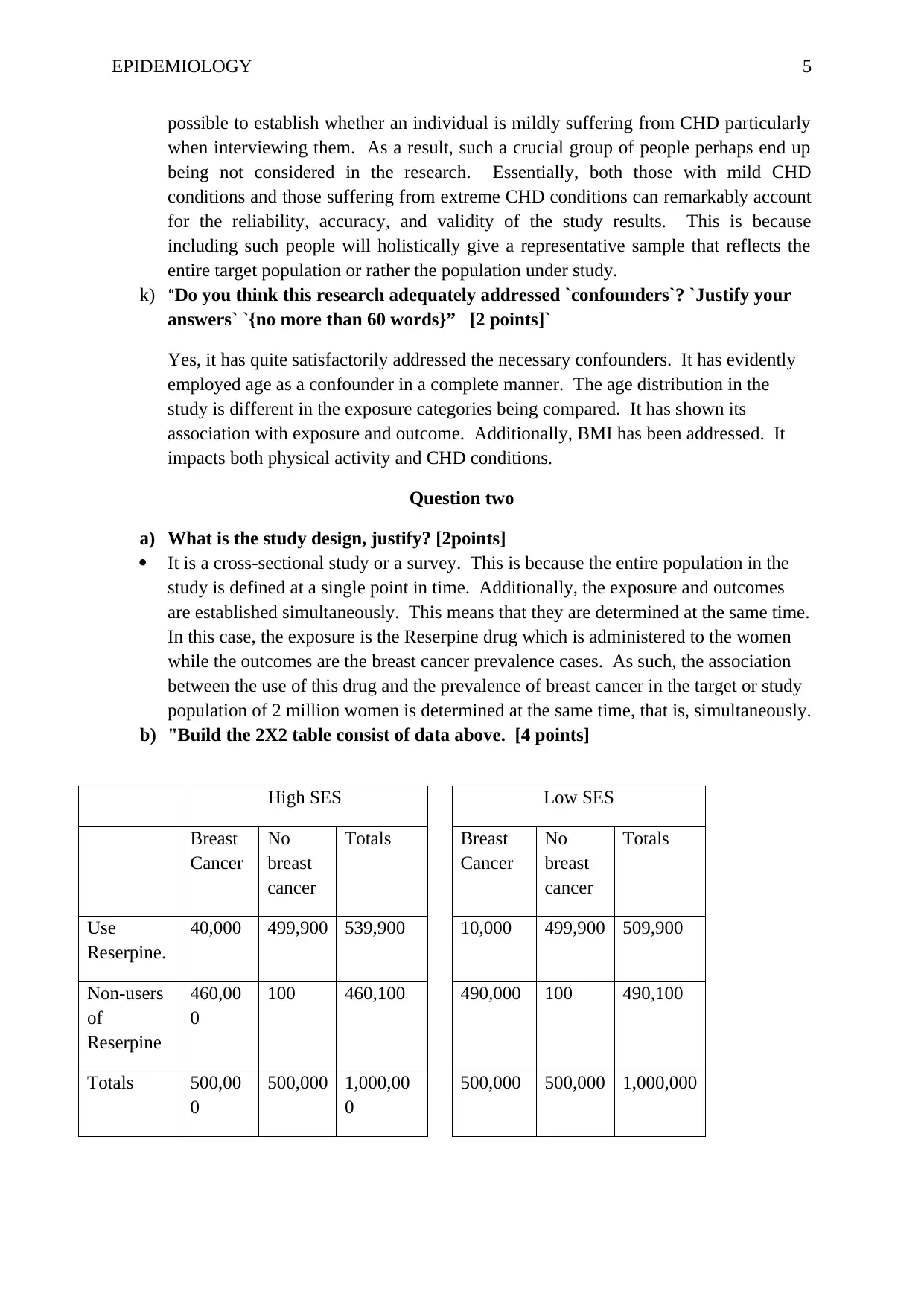
a) What is the study design, justify? [2points]
It is a cross-sectional study or a survey. This is because the entire population in the
study is defined at a single point in time. Additionally, the exposure and outcomes
are established simultaneously. This means that they are determined at the same time.
In this case, the exposure is the Reserpine drug which is administered to the women
while the outcomes are the breast cancer prevalence cases. As such, the association
between the use of this drug and the prevalence of breast cancer in the target or study
population of 2 million women is determined at the same time, that is, simultaneously.
b) "Build the 2X2 table consist of data above. [4 points]
High SES Low SES
Breast
Cancer
No
breast
cancer
Totals Breast
Cancer
No
breast
cancer
Totals
Use
Reserpine.
40,000 499,900 539,900 10,000 499,900 509,900
Non-users
of
Reserpine
460,00
0
100 460,100 490,000 100 490,100
Totals 500,00
0
500,000 1,000,00
0
500,000 500,000 1,000,000
possible to establish whether an individual is mildly suffering from CHD particularly
when interviewing them. As a result, such a crucial group of people perhaps end up
being not considered in the research. Essentially, both those with mild CHD
conditions and those suffering from extreme CHD conditions can remarkably account
for the reliability, accuracy, and validity of the study results. This is because
including such people will holistically give a representative sample that reflects the
entire target population or rather the population under study.
k) “Do you think this research adequately addressed `confounders`? `Justify your
answers` `{no more than 60 words}” [2 points]`
Yes, it has quite satisfactorily addressed the necessary confounders. It has evidently
employed age as a confounder in a complete manner. The age distribution in the
study is different in the exposure categories being compared. It has shown its
association with exposure and outcome. Additionally, BMI has been addressed. It
impacts both physical activity and CHD conditions.
Question two
a) What is the study design, justify? [2points]
It is a cross-sectional study or a survey. This is because the entire population in the
study is defined at a single point in time. Additionally, the exposure and outcomes
are established simultaneously. This means that they are determined at the same time.
In this case, the exposure is the Reserpine drug which is administered to the women
while the outcomes are the breast cancer prevalence cases. As such, the association
between the use of this drug and the prevalence of breast cancer in the target or study
population of 2 million women is determined at the same time, that is, simultaneously.
b) "Build the 2X2 table consist of data above. [4 points]
High SES Low SES
Breast
Cancer
No
breast
cancer
Totals Breast
Cancer
No
breast
cancer
Totals
Use
Reserpine.
40,000 499,900 539,900 10,000 499,900 509,900
Non-users
of
Reserpine
460,00
0
100 460,100 490,000 100 490,100
Totals 500,00
0
500,000 1,000,00
0
500,000 500,000 1,000,000
EPIDEMIOLOGY 6
`If `Reserpine `is causally related to breast`, `how `many cases of `breast-cancer` could
be avoided in the `high SES` and `Low SES`, had `Reserpine` been banned` from being
in the market?` (`in other words, what is the PAF?`)`` [3 points]``
Population attributable risk fraction (PAF) describes the proportion of all the cases
comprised in the entire study population (both the unexposed and the exposed) which can be
attributed to the exposure. PAR is normally computed by subtracting the incidence within
the unexposed from the incidence in the sum population which includes both the exposed and
the unexposed. It is employed in measuring the likely effect of control measures within a
given population and hence indispensable in public health decisions. Its formula is shown
below:
PAF= Population Attributable Risk (PAR) ÷ Overall population rate
That is, PAF=PAR/r
i) For the high SES, the PAF calculation is shown below:
Incidence rate =3 Non-incidence rate=1
Incidence of the unexposed is 3/4×460,000= 345,000
Incidence in the total population is 3/4×1,000,000= 750,000
Hence, PAR= 750,000-345,000= 405,000
Percentage of PAR= 405,000/705,000×100= 57%, cases to be possibly avoided are
57/100×1000000= 570,000 cases
ii) For the low SES, the PAF calculation is illustrated below:
Incidence of the unexposed is 3/4×490,000= 367,500
Incidence in the total population is 3/4×1,000,000= 750,000
Hence, PAR= 750,000-367,500= 382500
Percentage of PAR= 382,500/750,000×100= 51%, cases to be possibly averted are
51/100×1000000= 510,000 cases
Question three
`If `Reserpine `is causally related to breast`, `how `many cases of `breast-cancer` could
be avoided in the `high SES` and `Low SES`, had `Reserpine` been banned` from being
in the market?` (`in other words, what is the PAF?`)`` [3 points]``
Population attributable risk fraction (PAF) describes the proportion of all the cases
comprised in the entire study population (both the unexposed and the exposed) which can be
attributed to the exposure. PAR is normally computed by subtracting the incidence within
the unexposed from the incidence in the sum population which includes both the exposed and
the unexposed. It is employed in measuring the likely effect of control measures within a
given population and hence indispensable in public health decisions. Its formula is shown
below:
PAF= Population Attributable Risk (PAR) ÷ Overall population rate
That is, PAF=PAR/r
i) For the high SES, the PAF calculation is shown below:
Incidence rate =3 Non-incidence rate=1
Incidence of the unexposed is 3/4×460,000= 345,000
Incidence in the total population is 3/4×1,000,000= 750,000
Hence, PAR= 750,000-345,000= 405,000
Percentage of PAR= 405,000/705,000×100= 57%, cases to be possibly avoided are
57/100×1000000= 570,000 cases
ii) For the low SES, the PAF calculation is illustrated below:
Incidence of the unexposed is 3/4×490,000= 367,500
Incidence in the total population is 3/4×1,000,000= 750,000
Hence, PAR= 750,000-367,500= 382500
Percentage of PAR= 382,500/750,000×100= 51%, cases to be possibly averted are
51/100×1000000= 510,000 cases
Question three
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
EPIDEMIOLOGY 7
a) `Compute the crude measure of association between the drug and blood pressure
[2 points]`
The crude ratio is given as follows:
Crude ratio; (70/100) ÷ (40/100) = 0.7/0.4 = 1.75
b) "Calculate the stratum-specific association between the drug and blood pressure
[2 points]"
The stratum-specific ratios are illustrated below:
Among those whose BMI>=25, the risk ratio is calculated as follows;
RR= (30/50) ÷ (20/50) = (0.6/0.4) = 1.5
Among those individuals whose BMI <25, the risk ratio is determined as shown in the
below illustration:
RR= (40/50) ÷ (20/50) = 0.8/0.4 = 2.0
c) “Interpret your findings [2 points]”
From the above calculations, the crude analysis proposed an association between drug
use and lowered BP frequency. This implies that there exists an overt relationship
between the consumption of the new drug and the recorded blood pressure levels
among individuals with different BMI. Nevertheless, if this is stratified based on
BMI, one can see a robust association with drug use in subjects with a BMI<25
compared to subjects with a BMI>=25. Possibly the drug was more effective in
individuals whose BMI is less than 25 than in their counterparts.
Question four
``Could this difference induce a bias?`` `Explain your answer`. ``What would be a
practical way to avoid such differences in case-control studies?`` [4 points]
Yes, the difference can bring about quite a noticeable bias.
The most likely type of bias is selection bias. According to (Mark, 2013), selection bias is
more likely to happen in case-control studies. Usually, this type of study takes place when
participation in the study is differential based on the disease status. For instance, the people
who participated as controls were half less when compared to those who participated as cases
in reporting similar disorder particularly breathing. As a result, this may lead to bias or error
in estimating the relationship between the type 2 diabetes conditions and sleeping disorders.
This is evidenced in the non-comparability exhibited between the cases and the controls.
First, the sole aim of case-control studies is to select study controls that are reflective of the
population that from which the cases were produced. As such, the percentage discrepancy
between the men in the cases and those in control is bound to induce a bias. This is because
the less number of controls relative to the number of cases is likely to provide a poor estimate
of the exposure rate in the study population.
A possible efficacious way to avert such discrepancies in a case-control study is by
ensuring that the number of controls matches the number of cases (Richard, 2005). This can
be achieved by ensuring that when you select one control, you also select one case.
Question five
a) `Compute the crude measure of association between the drug and blood pressure
[2 points]`
The crude ratio is given as follows:
Crude ratio; (70/100) ÷ (40/100) = 0.7/0.4 = 1.75
b) "Calculate the stratum-specific association between the drug and blood pressure
[2 points]"
The stratum-specific ratios are illustrated below:
Among those whose BMI>=25, the risk ratio is calculated as follows;
RR= (30/50) ÷ (20/50) = (0.6/0.4) = 1.5
Among those individuals whose BMI <25, the risk ratio is determined as shown in the
below illustration:
RR= (40/50) ÷ (20/50) = 0.8/0.4 = 2.0
c) “Interpret your findings [2 points]”
From the above calculations, the crude analysis proposed an association between drug
use and lowered BP frequency. This implies that there exists an overt relationship
between the consumption of the new drug and the recorded blood pressure levels
among individuals with different BMI. Nevertheless, if this is stratified based on
BMI, one can see a robust association with drug use in subjects with a BMI<25
compared to subjects with a BMI>=25. Possibly the drug was more effective in
individuals whose BMI is less than 25 than in their counterparts.
Question four
``Could this difference induce a bias?`` `Explain your answer`. ``What would be a
practical way to avoid such differences in case-control studies?`` [4 points]
Yes, the difference can bring about quite a noticeable bias.
The most likely type of bias is selection bias. According to (Mark, 2013), selection bias is
more likely to happen in case-control studies. Usually, this type of study takes place when
participation in the study is differential based on the disease status. For instance, the people
who participated as controls were half less when compared to those who participated as cases
in reporting similar disorder particularly breathing. As a result, this may lead to bias or error
in estimating the relationship between the type 2 diabetes conditions and sleeping disorders.
This is evidenced in the non-comparability exhibited between the cases and the controls.
First, the sole aim of case-control studies is to select study controls that are reflective of the
population that from which the cases were produced. As such, the percentage discrepancy
between the men in the cases and those in control is bound to induce a bias. This is because
the less number of controls relative to the number of cases is likely to provide a poor estimate
of the exposure rate in the study population.
A possible efficacious way to avert such discrepancies in a case-control study is by
ensuring that the number of controls matches the number of cases (Richard, 2005). This can
be achieved by ensuring that when you select one control, you also select one case.
Question five
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

EPIDEMIOLOGY 8
“Which of the following terms is associated with selection bias? [2 points]”
The response rate is one of the terms closely related to selection bias.
This is because, for instance, the selected study subjects in research about the prevalence of
alcohol use among college students may show different response rates to the questionnaire or
interview questions.
Question six
`Which of the following term is associated with measurement bias?` [2 points]`
Validity is related to measurement bias.
The measurement error or bias normally impacts the validity of the measured exposure or
disease for instance.
Question seven
``What biases would you suspect in a survey of the prevalence of drug use among
`young ``people using a representative sample of students attending high school justify``
(``not enough to name the biases`` (``No more than` 60` words)" [4 points]
The most likely biases are;
Students attending high school are not representative of the young population outside
the institution. This means that the sample of high school students selected does not
reflect the entire population of young people who are not high school students.
There may be a high nonresponse rate among the students in the selected sample.
“Which of the following terms is associated with selection bias? [2 points]”
The response rate is one of the terms closely related to selection bias.
This is because, for instance, the selected study subjects in research about the prevalence of
alcohol use among college students may show different response rates to the questionnaire or
interview questions.
Question six
`Which of the following term is associated with measurement bias?` [2 points]`
Validity is related to measurement bias.
The measurement error or bias normally impacts the validity of the measured exposure or
disease for instance.
Question seven
``What biases would you suspect in a survey of the prevalence of drug use among
`young ``people using a representative sample of students attending high school justify``
(``not enough to name the biases`` (``No more than` 60` words)" [4 points]
The most likely biases are;
Students attending high school are not representative of the young population outside
the institution. This means that the sample of high school students selected does not
reflect the entire population of young people who are not high school students.
There may be a high nonresponse rate among the students in the selected sample.

EPIDEMIOLOGY 9
References
Mark, W. (2013). Epidemiology: Studt Design and Data Analysis. CRC Press.
Richard, R. (2005). `Studying a Study and Testing a Test: How to Read the Medical
Evidence`. Lippincott Williams & Wilkins.
References
Mark, W. (2013). Epidemiology: Studt Design and Data Analysis. CRC Press.
Richard, R. (2005). `Studying a Study and Testing a Test: How to Read the Medical
Evidence`. Lippincott Williams & Wilkins.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.