Clinical Guidelines for Acute Coronary Syndrome
VerifiedAdded on 2022/12/21
|4
|1207
|89
AI Summary
This article focuses on the clinical practice relating to acute coronary syndrome in order to ensure improved outcomes for the patients suffering from chest pain or ACS. It discusses the adoption of a systematic approach and drawing interventions for ACS care.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Evidence Summary
Table
© Osborne, SR 2019 revised
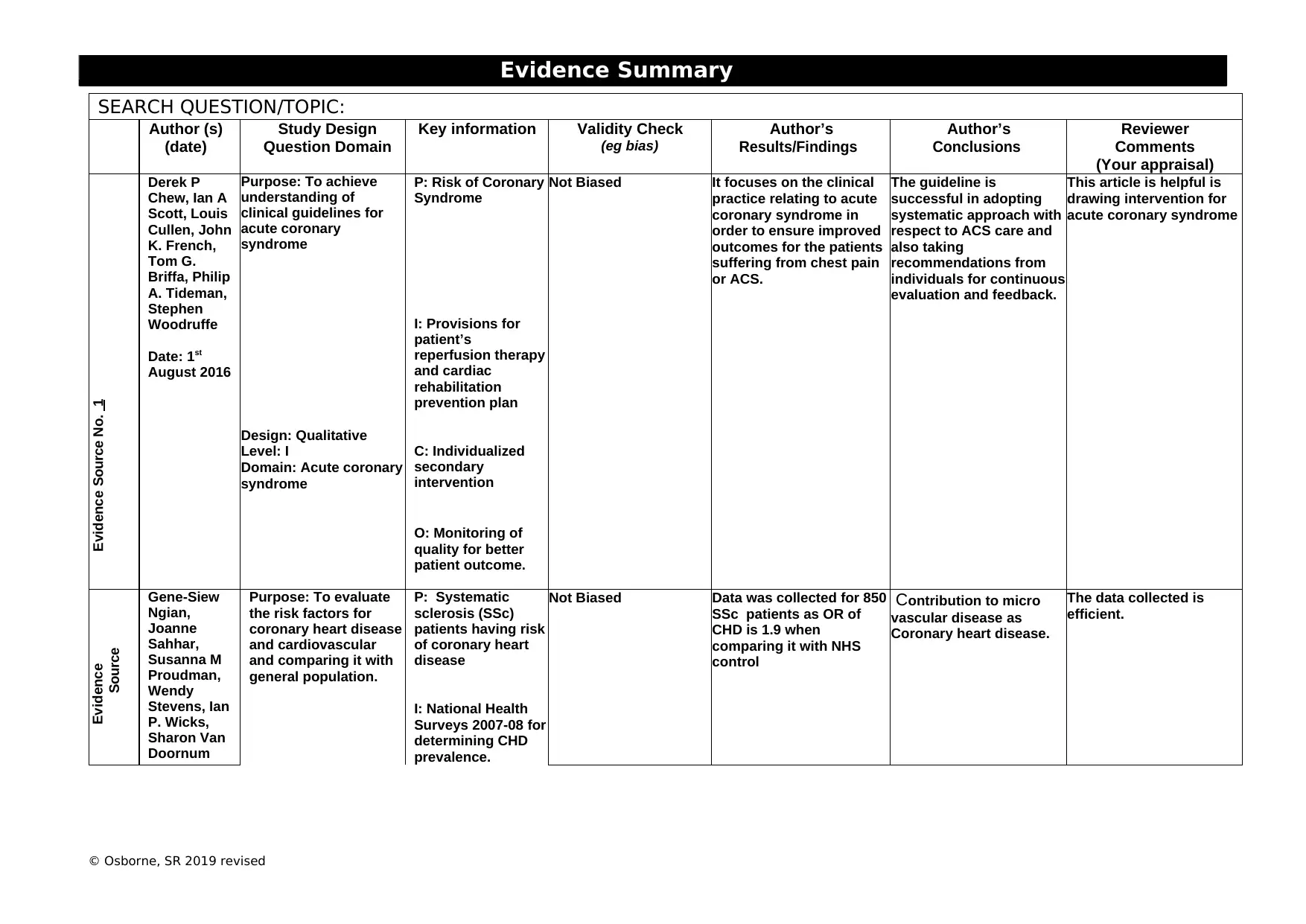
SEARCH QUESTION/TOPIC:
Author (s)
(date)
Study Design
Question Domain
Key information Validity Check
(eg bias)
Author’s
Results/Findings
Author’s
Conclusions
Reviewer
Comments
(Your appraisal)
Evidence Source No. 1
Derek P
Chew, Ian A
Scott, Louis
Cullen, John
K. French,
Tom G.
Briffa, Philip
A. Tideman,
Stephen
Woodruffe
Date: 1st
August 2016
Purpose: To achieve
understanding of
clinical guidelines for
acute coronary
syndrome
P: Risk of Coronary
Syndrome
Not Biased It focuses on the clinical
practice relating to acute
coronary syndrome in
order to ensure improved
outcomes for the patients
suffering from chest pain
or ACS.
The guideline is
successful in adopting
systematic approach with
respect to ACS care and
also taking
recommendations from
individuals for continuous
evaluation and feedback.
This article is helpful is
drawing intervention for
acute coronary syndrome
I: Provisions for
patient’s
reperfusion therapy
and cardiac
rehabilitation
prevention plan
Design: Qualitative
Level: I
Domain: Acute coronary
syndrome
C: Individualized
secondary
intervention
O: Monitoring of
quality for better
patient outcome.
Evidence
Source
Gene-Siew
Ngian,
Joanne
Sahhar,
Susanna M
Proudman,
Wendy
Stevens, Ian
P. Wicks,
Sharon Van
Doornum
Purpose: To evaluate
the risk factors for
coronary heart disease
and cardiovascular
and comparing it with
general population.
P: Systematic
sclerosis (SSc)
patients having risk
of coronary heart
disease
Not Biased Data was collected for 850
SSc patients as OR of
CHD is 1.9 when
comparing it with NHS
control
Contribution to micro
vascular disease as
Coronary heart disease.
The data collected is
efficient.
I: National Health
Surveys 2007-08 for
determining CHD
prevalence.
Table
© Osborne, SR 2019 revised
SEARCH QUESTION/TOPIC:
Author (s)
(date)
Study Design
Question Domain
Key information Validity Check
(eg bias)
Author’s
Results/Findings
Author’s
Conclusions
Reviewer
Comments
(Your appraisal)
Evidence Source No. 1
Derek P
Chew, Ian A
Scott, Louis
Cullen, John
K. French,
Tom G.
Briffa, Philip
A. Tideman,
Stephen
Woodruffe
Date: 1st
August 2016
Purpose: To achieve
understanding of
clinical guidelines for
acute coronary
syndrome
P: Risk of Coronary
Syndrome
Not Biased It focuses on the clinical
practice relating to acute
coronary syndrome in
order to ensure improved
outcomes for the patients
suffering from chest pain
or ACS.
The guideline is
successful in adopting
systematic approach with
respect to ACS care and
also taking
recommendations from
individuals for continuous
evaluation and feedback.
This article is helpful is
drawing intervention for
acute coronary syndrome
I: Provisions for
patient’s
reperfusion therapy
and cardiac
rehabilitation
prevention plan
Design: Qualitative
Level: I
Domain: Acute coronary
syndrome
C: Individualized
secondary
intervention
O: Monitoring of
quality for better
patient outcome.
Evidence
Source
Gene-Siew
Ngian,
Joanne
Sahhar,
Susanna M
Proudman,
Wendy
Stevens, Ian
P. Wicks,
Sharon Van
Doornum
Purpose: To evaluate
the risk factors for
coronary heart disease
and cardiovascular
and comparing it with
general population.
P: Systematic
sclerosis (SSc)
patients having risk
of coronary heart
disease
Not Biased Data was collected for 850
SSc patients as OR of
CHD is 1.9 when
comparing it with NHS
control
Contribution to micro
vascular disease as
Coronary heart disease.
The data collected is
efficient.
I: National Health
Surveys 2007-08 for
determining CHD
prevalence.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Evidence Summary
Table
© Osborne, SR 2019 revised
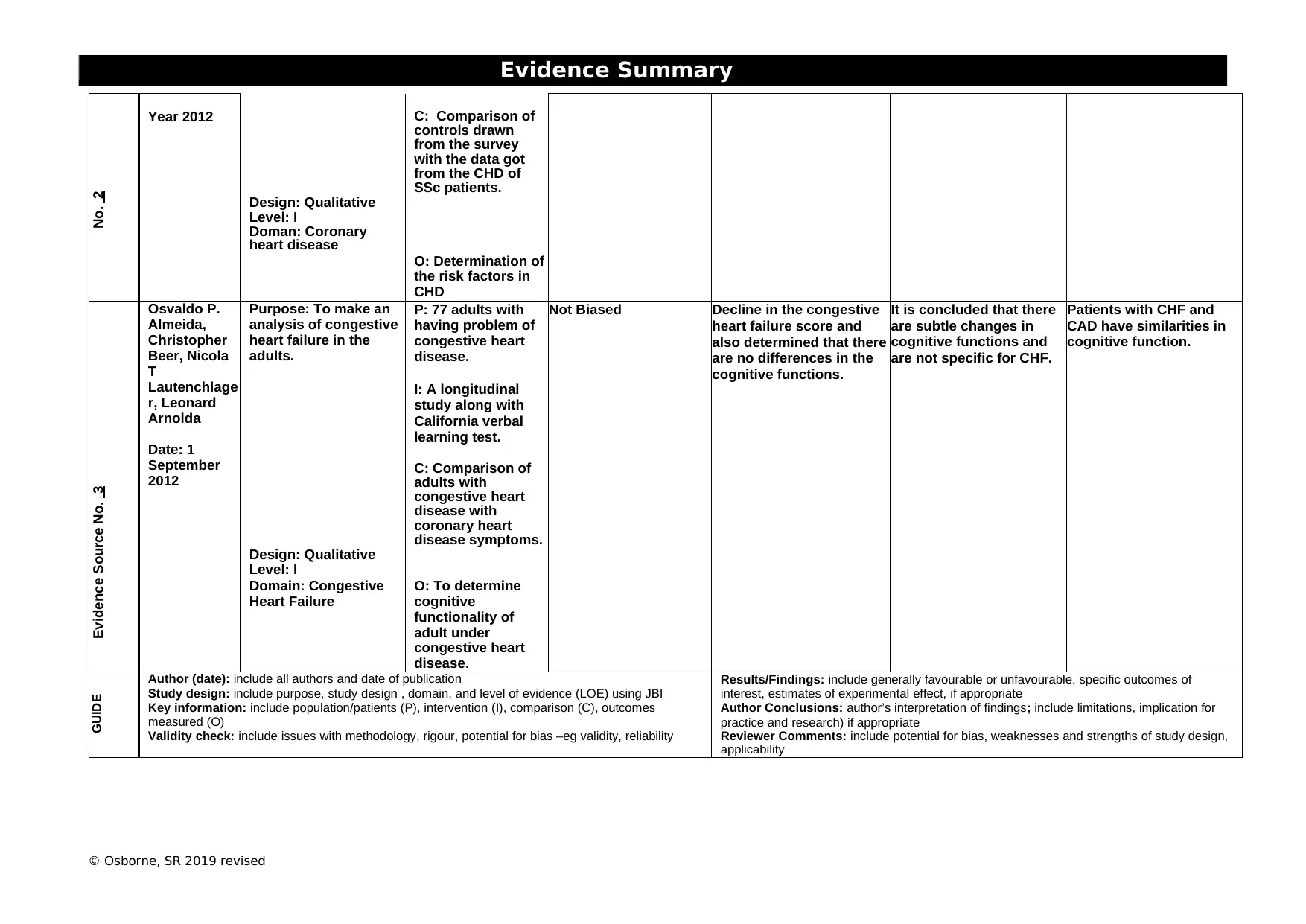
No. 2
Year 2012 C: Comparison of
controls drawn
from the survey
with the data got
from the CHD of
SSc patients.
Design: Qualitative
Level: I
Doman: Coronary
heart disease
O: Determination of
the risk factors in
CHD
Evidence Source No. 3
Osvaldo P.
Almeida,
Christopher
Beer, Nicola
T
Lautenchlage
r, Leonard
Arnolda
Date: 1
September
2012
Purpose: To make an
analysis of congestive
heart failure in the
adults.
P: 77 adults with
having problem of
congestive heart
disease.
Not Biased Decline in the congestive
heart failure score and
also determined that there
are no differences in the
cognitive functions.
It is concluded that there
are subtle changes in
cognitive functions and
are not specific for CHF.
Patients with CHF and
CAD have similarities in
cognitive function.
I: A longitudinal
study along with
California verbal
learning test.
C: Comparison of
adults with
congestive heart
disease with
coronary heart
disease symptoms.
Design: Qualitative
Level: I
Domain: Congestive
Heart Failure
O: To determine
cognitive
functionality of
adult under
congestive heart
disease.
GUIDE Author (date): include all authors and date of publication
Study design: include purpose, study design , domain, and level of evidence (LOE) using JBI
Key information: include population/patients (P), intervention (I), comparison (C), outcomes
measured (O)
Validity check: include issues with methodology, rigour, potential for bias –eg validity, reliability
Results/Findings: include generally favourable or unfavourable, specific outcomes of
interest, estimates of experimental effect, if appropriate
Author Conclusions: author’s interpretation of findings; include limitations, implication for
practice and research) if appropriate
Reviewer Comments: include potential for bias, weaknesses and strengths of study design,
applicability
Table
© Osborne, SR 2019 revised
No. 2
Year 2012 C: Comparison of
controls drawn
from the survey
with the data got
from the CHD of
SSc patients.
Design: Qualitative
Level: I
Doman: Coronary
heart disease
O: Determination of
the risk factors in
CHD
Evidence Source No. 3
Osvaldo P.
Almeida,
Christopher
Beer, Nicola
T
Lautenchlage
r, Leonard
Arnolda
Date: 1
September
2012
Purpose: To make an
analysis of congestive
heart failure in the
adults.
P: 77 adults with
having problem of
congestive heart
disease.
Not Biased Decline in the congestive
heart failure score and
also determined that there
are no differences in the
cognitive functions.
It is concluded that there
are subtle changes in
cognitive functions and
are not specific for CHF.
Patients with CHF and
CAD have similarities in
cognitive function.
I: A longitudinal
study along with
California verbal
learning test.
C: Comparison of
adults with
congestive heart
disease with
coronary heart
disease symptoms.
Design: Qualitative
Level: I
Domain: Congestive
Heart Failure
O: To determine
cognitive
functionality of
adult under
congestive heart
disease.
GUIDE Author (date): include all authors and date of publication
Study design: include purpose, study design , domain, and level of evidence (LOE) using JBI
Key information: include population/patients (P), intervention (I), comparison (C), outcomes
measured (O)
Validity check: include issues with methodology, rigour, potential for bias –eg validity, reliability
Results/Findings: include generally favourable or unfavourable, specific outcomes of
interest, estimates of experimental effect, if appropriate
Author Conclusions: author’s interpretation of findings; include limitations, implication for
practice and research) if appropriate
Reviewer Comments: include potential for bias, weaknesses and strengths of study design,
applicability
Evidence Summary
Table
© Osborne, SR 2019 revised
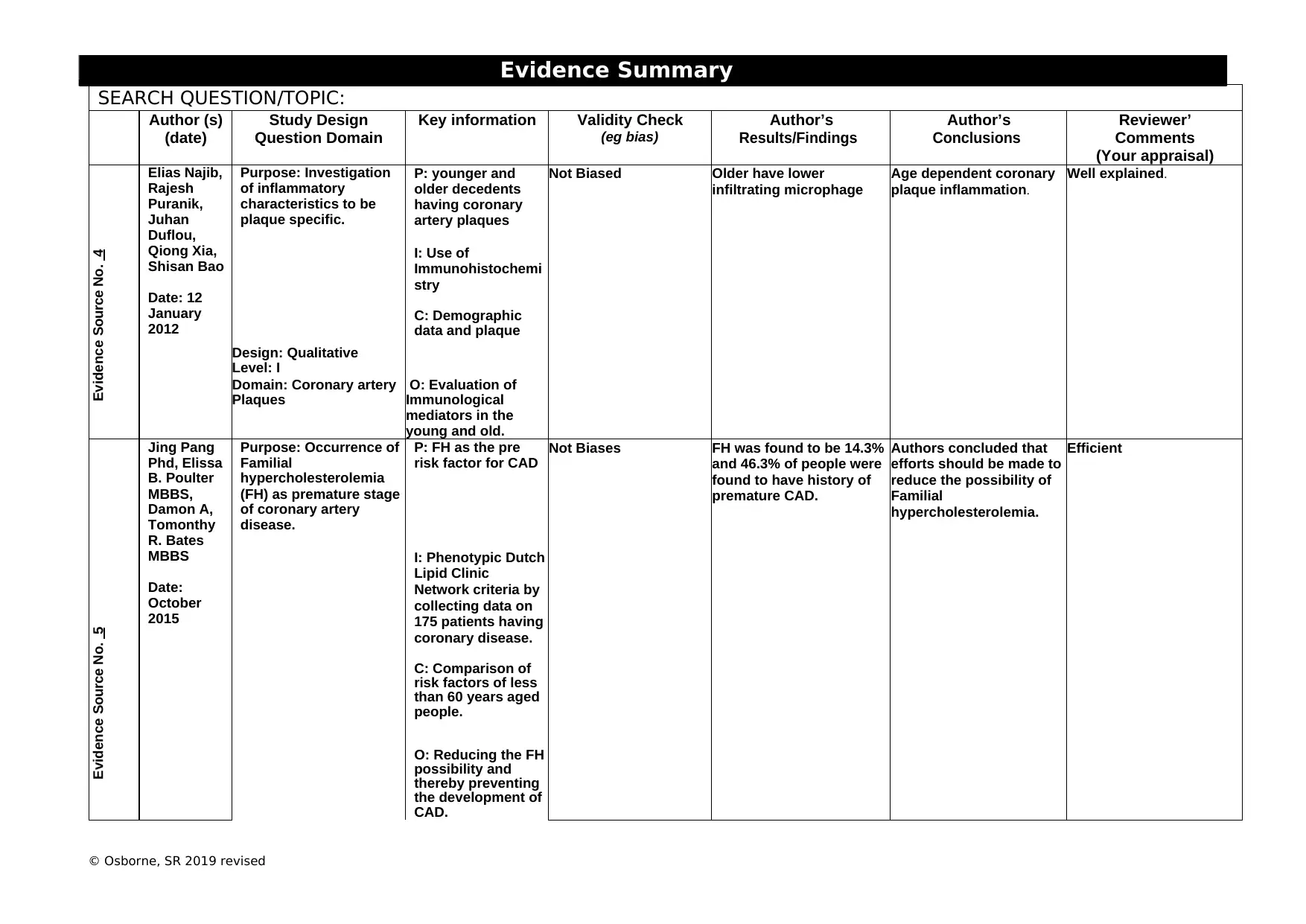
SEARCH QUESTION/TOPIC:
Author (s)
(date)
Study Design
Question Domain
Key information Validity Check
(eg bias)
Author’s
Results/Findings
Author’s
Conclusions
Reviewer’
Comments
(Your appraisal)
Evidence Source No. 4
Elias Najib,
Rajesh
Puranik,
Juhan
Duflou,
Qiong Xia,
Shisan Bao
Date: 12
January
2012
Purpose: Investigation
of inflammatory
characteristics to be
plaque specific.
P: younger and
older decedents
having coronary
artery plaques
Not Biased Older have lower
infiltrating microphage
Age dependent coronary
plaque inflammation.
Well explained.
I: Use of
Immunohistochemi
stry
C: Demographic
data and plaque
Design: Qualitative
Level: I
Domain: Coronary artery
Plaques
O: Evaluation of
Immunological
mediators in the
young and old.
Evidence Source No. 5
Jing Pang
Phd, Elissa
B. Poulter
MBBS,
Damon A,
Tomonthy
R. Bates
MBBS
Date:
October
2015
Purpose: Occurrence of
Familial
hypercholesterolemia
(FH) as premature stage
of coronary artery
disease.
P: FH as the pre
risk factor for CAD
Not Biases FH was found to be 14.3%
and 46.3% of people were
found to have history of
premature CAD.
Authors concluded that
efforts should be made to
reduce the possibility of
Familial
hypercholesterolemia.
Efficient
I: Phenotypic Dutch
Lipid Clinic
Network criteria by
collecting data on
175 patients having
coronary disease.
C: Comparison of
risk factors of less
than 60 years aged
people.
O: Reducing the FH
possibility and
thereby preventing
the development of
CAD.
Table
© Osborne, SR 2019 revised
SEARCH QUESTION/TOPIC:
Author (s)
(date)
Study Design
Question Domain
Key information Validity Check
(eg bias)
Author’s
Results/Findings
Author’s
Conclusions
Reviewer’
Comments
(Your appraisal)
Evidence Source No. 4
Elias Najib,
Rajesh
Puranik,
Juhan
Duflou,
Qiong Xia,
Shisan Bao
Date: 12
January
2012
Purpose: Investigation
of inflammatory
characteristics to be
plaque specific.
P: younger and
older decedents
having coronary
artery plaques
Not Biased Older have lower
infiltrating microphage
Age dependent coronary
plaque inflammation.
Well explained.
I: Use of
Immunohistochemi
stry
C: Demographic
data and plaque
Design: Qualitative
Level: I
Domain: Coronary artery
Plaques
O: Evaluation of
Immunological
mediators in the
young and old.
Evidence Source No. 5
Jing Pang
Phd, Elissa
B. Poulter
MBBS,
Damon A,
Tomonthy
R. Bates
MBBS
Date:
October
2015
Purpose: Occurrence of
Familial
hypercholesterolemia
(FH) as premature stage
of coronary artery
disease.
P: FH as the pre
risk factor for CAD
Not Biases FH was found to be 14.3%
and 46.3% of people were
found to have history of
premature CAD.
Authors concluded that
efforts should be made to
reduce the possibility of
Familial
hypercholesterolemia.
Efficient
I: Phenotypic Dutch
Lipid Clinic
Network criteria by
collecting data on
175 patients having
coronary disease.
C: Comparison of
risk factors of less
than 60 years aged
people.
O: Reducing the FH
possibility and
thereby preventing
the development of
CAD.
Evidence Summary
Table
© Osborne, SR 2019 revised
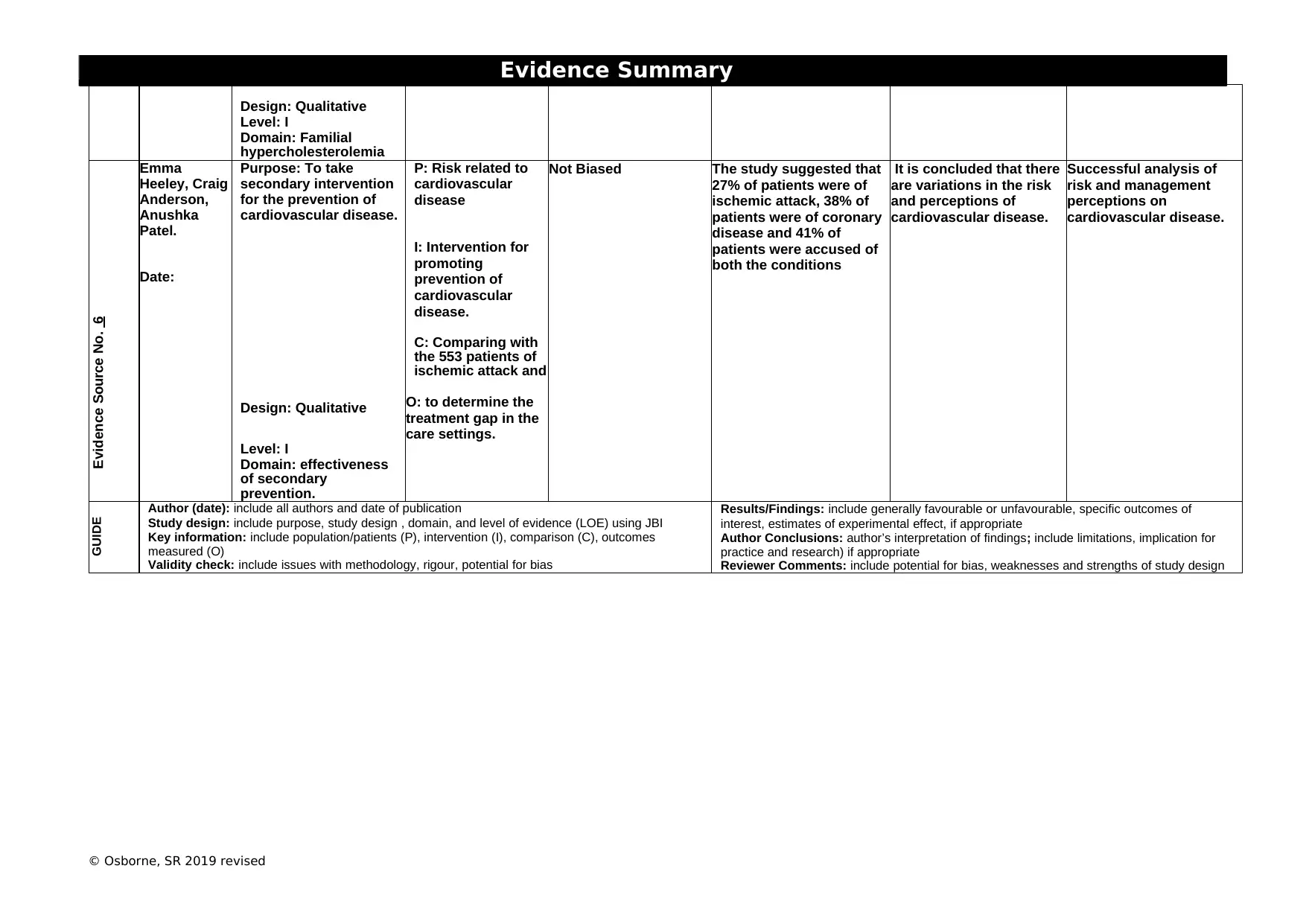
Design: Qualitative
Level: I
Domain: Familial
hypercholesterolemia
Evidence Source No. 6
Emma
Heeley, Craig
Anderson,
Anushka
Patel.
Date:
Purpose: To take
secondary intervention
for the prevention of
cardiovascular disease.
P: Risk related to
cardiovascular
disease
Not Biased The study suggested that
27% of patients were of
ischemic attack, 38% of
patients were of coronary
disease and 41% of
patients were accused of
both the conditions
It is concluded that there
are variations in the risk
and perceptions of
cardiovascular disease.
Successful analysis of
risk and management
perceptions on
cardiovascular disease.
I: Intervention for
promoting
prevention of
cardiovascular
disease.
C: Comparing with
the 553 patients of
ischemic attack and
Design: Qualitative O: to determine the
treatment gap in the
care settings.
Level: I
Domain: effectiveness
of secondary
prevention.
GUIDE Author (date): include all authors and date of publication
Study design: include purpose, study design , domain, and level of evidence (LOE) using JBI
Key information: include population/patients (P), intervention (I), comparison (C), outcomes
measured (O)
Validity check: include issues with methodology, rigour, potential for bias
Results/Findings: include generally favourable or unfavourable, specific outcomes of
interest, estimates of experimental effect, if appropriate
Author Conclusions: author’s interpretation of findings; include limitations, implication for
practice and research) if appropriate
Reviewer Comments: include potential for bias, weaknesses and strengths of study design
Table
© Osborne, SR 2019 revised
Design: Qualitative
Level: I
Domain: Familial
hypercholesterolemia
Evidence Source No. 6
Emma
Heeley, Craig
Anderson,
Anushka
Patel.
Date:
Purpose: To take
secondary intervention
for the prevention of
cardiovascular disease.
P: Risk related to
cardiovascular
disease
Not Biased The study suggested that
27% of patients were of
ischemic attack, 38% of
patients were of coronary
disease and 41% of
patients were accused of
both the conditions
It is concluded that there
are variations in the risk
and perceptions of
cardiovascular disease.
Successful analysis of
risk and management
perceptions on
cardiovascular disease.
I: Intervention for
promoting
prevention of
cardiovascular
disease.
C: Comparing with
the 553 patients of
ischemic attack and
Design: Qualitative O: to determine the
treatment gap in the
care settings.
Level: I
Domain: effectiveness
of secondary
prevention.
GUIDE Author (date): include all authors and date of publication
Study design: include purpose, study design , domain, and level of evidence (LOE) using JBI
Key information: include population/patients (P), intervention (I), comparison (C), outcomes
measured (O)
Validity check: include issues with methodology, rigour, potential for bias
Results/Findings: include generally favourable or unfavourable, specific outcomes of
interest, estimates of experimental effect, if appropriate
Author Conclusions: author’s interpretation of findings; include limitations, implication for
practice and research) if appropriate
Reviewer Comments: include potential for bias, weaknesses and strengths of study design
1 out of 4



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.