SLE251 Project: Comparative Study of Infant Mortality in Two Countries
VerifiedAdded on 2023/03/30
|11
|1747
|186
Report
AI Summary
This SLE251 project report investigates the infant mortality rates in Australia and Bangladesh, examining the correlation between healthcare levels and infant survival. The study uses data from sources like the World Bank to compare mortality rates in both countries, employing statistical analysis via SPSS to test the hypothesis that mortality rates differ based on healthcare quality. Results from t-tests and ANOVA analyses suggest no significant difference in infant mortality rates related to healthcare levels between the two countries. The report discusses factors such as crude death rates, incidence rates of diseases like tuberculosis, and sanitation facilities, concluding that while both countries show improvements in healthcare, discrepancies exist due to differences in development, population aging, and technological advancements. The study concludes that based on the data analyzed, there is no significant difference in infant mortality rates based on the level of healthcare in Australia and Bangladesh.

Running head: SLE 251 PROJECT ASSIGNMENT 1
SLE 251 PROJECT ASSIGNMENT
By (Name of Student)
(Institutional Affiliation)
(Date of Submission)
SLE 251 PROJECT ASSIGNMENT
By (Name of Student)
(Institutional Affiliation)
(Date of Submission)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SLE 251 PROJECT ASSIGNMENT 2
INTRODUCTION
Infant mortality rate compares the number of deaths of infants under one year old in a given
year per 1,000 live births in the same year. This rate is often used as an indicator of the level
of health in a country. Research were carried out by a Medicare research group in 1992
concluded that health care system strongly influences the registration of infant deaths.
(Korbin Liu, 1992) The population of interest in this study are the infants/new born babies of
two countries which are Bangladesh and Australia respectively (The World Bank, 2019).
The current research was done to investigate if the mortality rate of infants is still dependent
on the level of health care of a country. The hypothesis of the research was that there is a
difference of mortality rate of infants, higher in low level of health care in a country and
lower in a higher level of heath care in a country.
Hypothesis Testing
To investigate whether mortality rate of infants is still dependent on the level of health care of
a country, it is important to conduct hypothesis testing based on the data obtained from the
survey. Two sample t-test based on the mortality rates of infants per 1000 live births in both
Australia and Bangladesh is performed. The null hypothesis and alternative hypothesis for
this study can be stated and formulated as follows;
Ho: There is no difference of mortality rate of infants, higher in low level of health care in a
country and lower in a higher level of heath care in a country.
H1: There is a difference of mortality rate of infants, higher in low level of health care in a
country and lower in a higher level of heath care in a country.
INTRODUCTION
Infant mortality rate compares the number of deaths of infants under one year old in a given
year per 1,000 live births in the same year. This rate is often used as an indicator of the level
of health in a country. Research were carried out by a Medicare research group in 1992
concluded that health care system strongly influences the registration of infant deaths.
(Korbin Liu, 1992) The population of interest in this study are the infants/new born babies of
two countries which are Bangladesh and Australia respectively (The World Bank, 2019).
The current research was done to investigate if the mortality rate of infants is still dependent
on the level of health care of a country. The hypothesis of the research was that there is a
difference of mortality rate of infants, higher in low level of health care in a country and
lower in a higher level of heath care in a country.
Hypothesis Testing
To investigate whether mortality rate of infants is still dependent on the level of health care of
a country, it is important to conduct hypothesis testing based on the data obtained from the
survey. Two sample t-test based on the mortality rates of infants per 1000 live births in both
Australia and Bangladesh is performed. The null hypothesis and alternative hypothesis for
this study can be stated and formulated as follows;
Ho: There is no difference of mortality rate of infants, higher in low level of health care in a
country and lower in a higher level of heath care in a country.
H1: There is a difference of mortality rate of infants, higher in low level of health care in a
country and lower in a higher level of heath care in a country.
SLE 251 PROJECT ASSIGNMENT 3
METHOD
Design
Systemically collecting data for mortality can be very hard. The data bank like World Bank
data might not have accurate data as they collect their data through governmental health care
surveys and Non-Governmental Organizations of that particular country. The data does not
imply as to how the death occurred and in what circumstances and also cross check the birth
certificate and death certificate to check if the birth of the infant is one year or less.
Data Analysis
The Statistical Packages for Social Sciences (SPSS Version 25.0) is used to analyze our
quantitative data. This will include the use of group means, frequencies, ANOVA and T-test.
Reliability test as well will be performed on the data to verify the biasness of the data.
RESULTS
The tables below displays the outputs of the findings based on the various analyses and test
performed in SPSS.
Descriptive Analysis
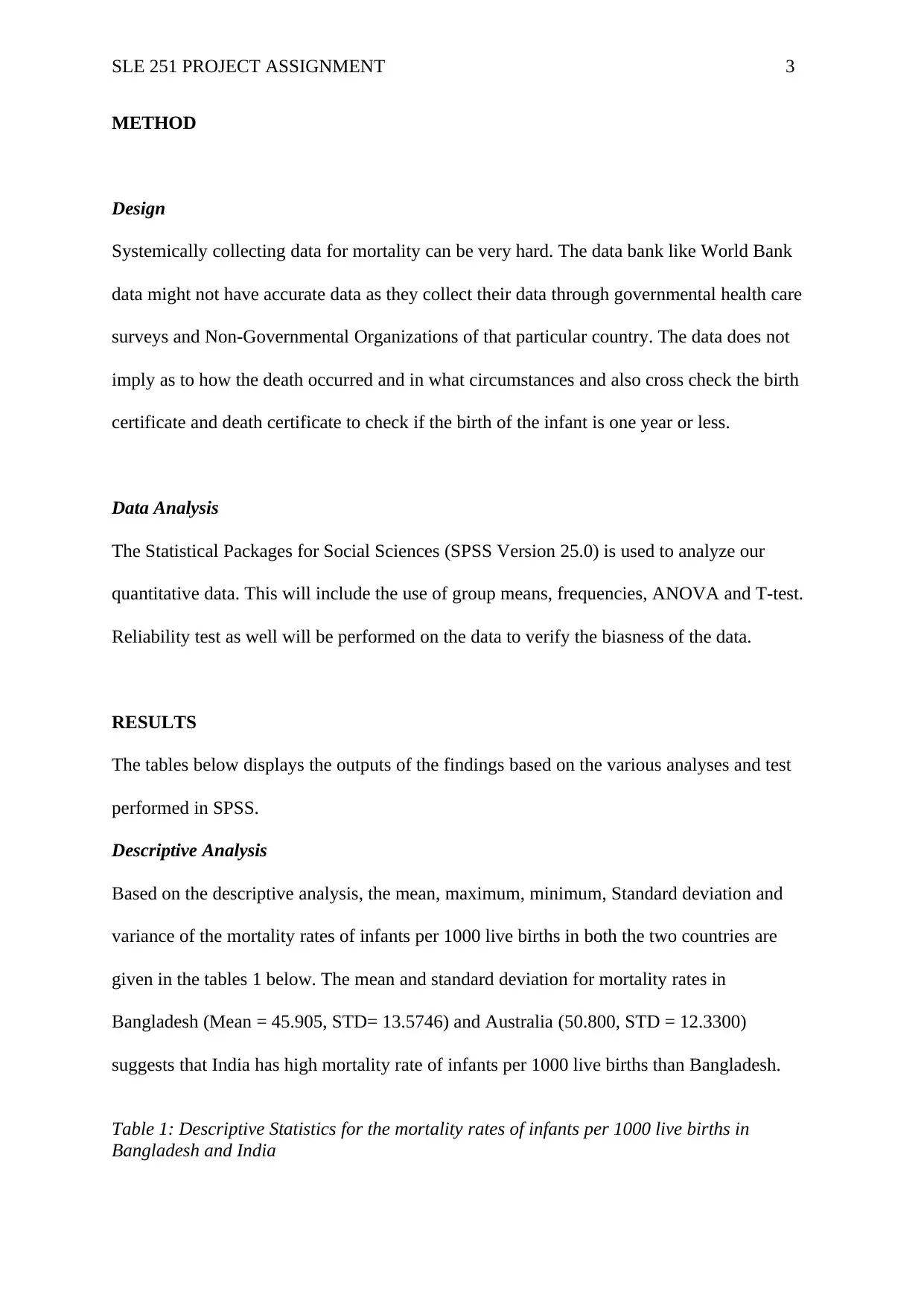
Based on the descriptive analysis, the mean, maximum, minimum, Standard deviation and
variance of the mortality rates of infants per 1000 live births in both the two countries are
given in the tables 1 below. The mean and standard deviation for mortality rates in
Bangladesh (Mean = 45.905, STD= 13.5746) and Australia (50.800, STD = 12.3300)
suggests that India has high mortality rate of infants per 1000 live births than Bangladesh.
Table 1: Descriptive Statistics for the mortality rates of infants per 1000 live births in
Bangladesh and India
METHOD
Design
Systemically collecting data for mortality can be very hard. The data bank like World Bank
data might not have accurate data as they collect their data through governmental health care
surveys and Non-Governmental Organizations of that particular country. The data does not
imply as to how the death occurred and in what circumstances and also cross check the birth
certificate and death certificate to check if the birth of the infant is one year or less.
Data Analysis
The Statistical Packages for Social Sciences (SPSS Version 25.0) is used to analyze our
quantitative data. This will include the use of group means, frequencies, ANOVA and T-test.
Reliability test as well will be performed on the data to verify the biasness of the data.
RESULTS
The tables below displays the outputs of the findings based on the various analyses and test
performed in SPSS.
Descriptive Analysis
Based on the descriptive analysis, the mean, maximum, minimum, Standard deviation and
variance of the mortality rates of infants per 1000 live births in both the two countries are
given in the tables 1 below. The mean and standard deviation for mortality rates in
Bangladesh (Mean = 45.905, STD= 13.5746) and Australia (50.800, STD = 12.3300)
suggests that India has high mortality rate of infants per 1000 live births than Bangladesh.
Table 1: Descriptive Statistics for the mortality rates of infants per 1000 live births in
Bangladesh and India
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SLE 251 PROJECT ASSIGNMENT 4
Descriptive Statistics
N Minimum Maximum Mean Std. Deviation Variance
Mortality rates of infants per 1000
live births(BANGLADESH)
20 26.9 70.4 45.905 13.5746 184.271
Mortality rates of infants per 1000
live births(AUSTRALIA)
20 32.0 71.2 50.800 12.3300 152.029
Valid N (listwise) 20
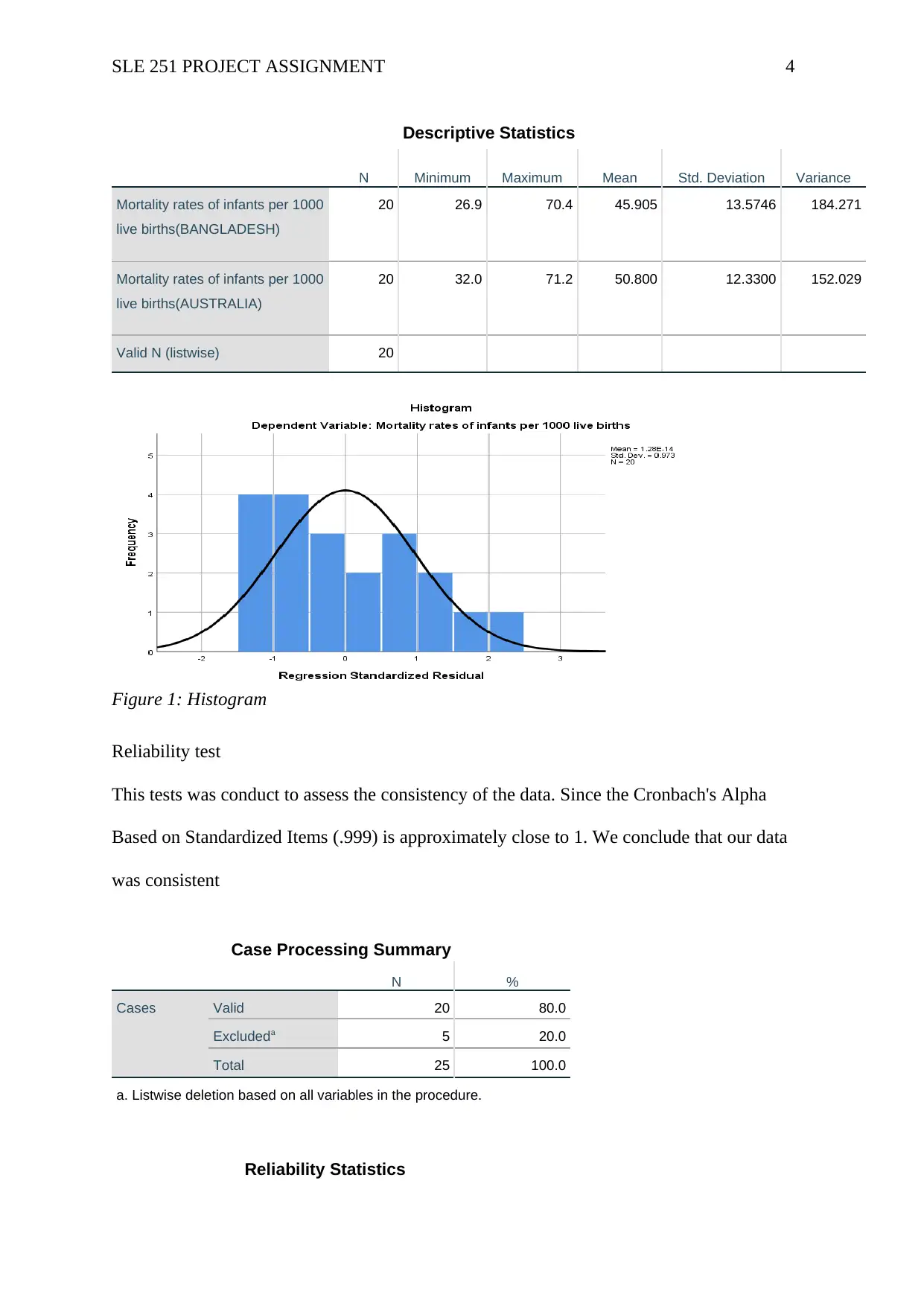
Figure 1: Histogram
Reliability test
This tests was conduct to assess the consistency of the data. Since the Cronbach's Alpha
Based on Standardized Items (.999) is approximately close to 1. We conclude that our data
was consistent
Case Processing Summary
N %
Cases Valid 20 80.0
Excludeda 5 20.0
Total 25 100.0
a. Listwise deletion based on all variables in the procedure.
Reliability Statistics
Descriptive Statistics
N Minimum Maximum Mean Std. Deviation Variance
Mortality rates of infants per 1000
live births(BANGLADESH)
20 26.9 70.4 45.905 13.5746 184.271
Mortality rates of infants per 1000
live births(AUSTRALIA)
20 32.0 71.2 50.800 12.3300 152.029
Valid N (listwise) 20
Figure 1: Histogram
Reliability test
This tests was conduct to assess the consistency of the data. Since the Cronbach's Alpha
Based on Standardized Items (.999) is approximately close to 1. We conclude that our data
was consistent
Case Processing Summary
N %
Cases Valid 20 80.0
Excludeda 5 20.0
Total 25 100.0
a. Listwise deletion based on all variables in the procedure.
Reliability Statistics
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SLE 251 PROJECT ASSIGNMENT 5
Cronbach's Alpha
Cronbach's Alpha
Based on
Standardized Items N of Items
.996 .999 2
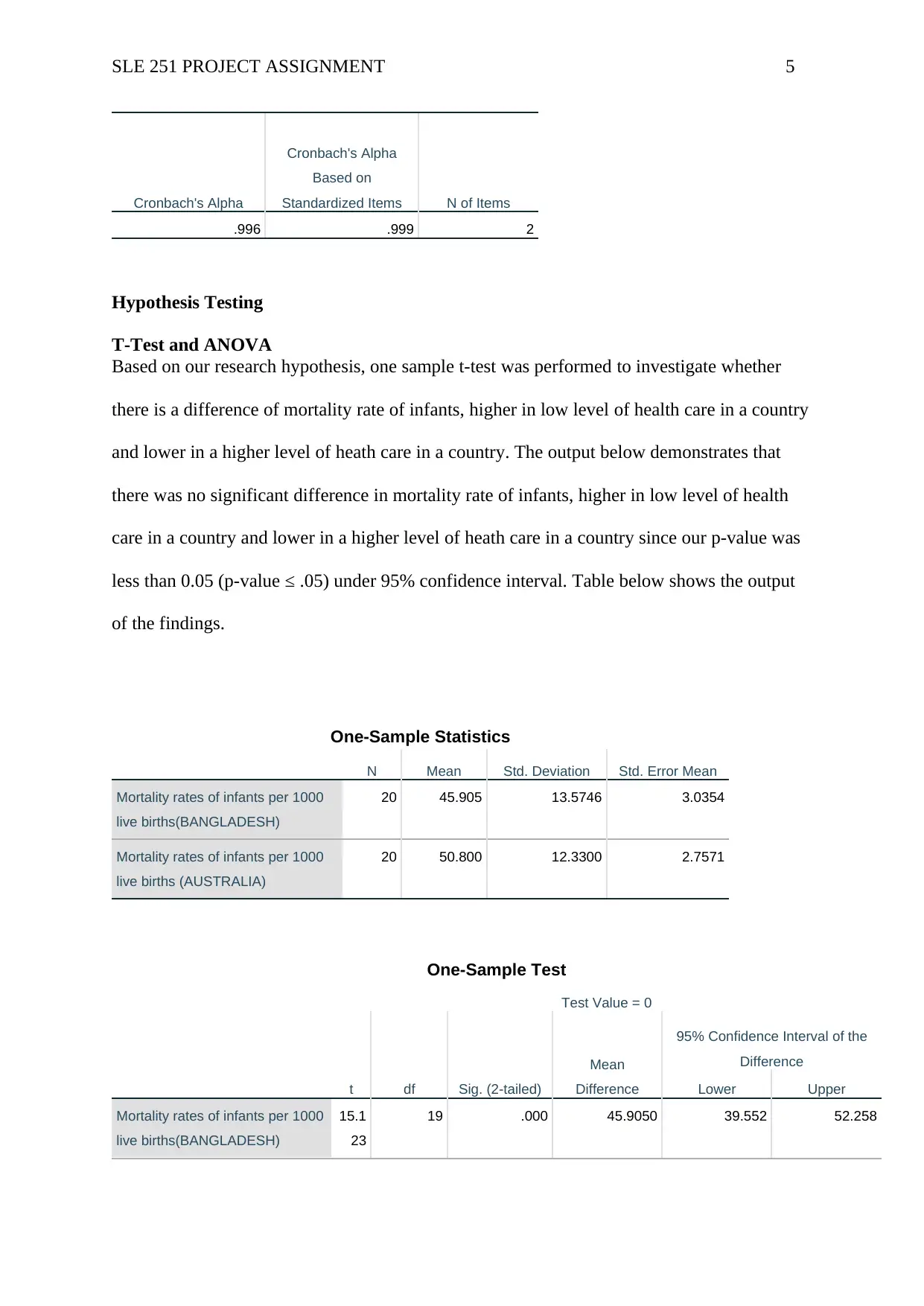
Hypothesis Testing
T-Test and ANOVA
Based on our research hypothesis, one sample t-test was performed to investigate whether
there is a difference of mortality rate of infants, higher in low level of health care in a country
and lower in a higher level of heath care in a country. The output below demonstrates that
there was no significant difference in mortality rate of infants, higher in low level of health
care in a country and lower in a higher level of heath care in a country since our p-value was
less than 0.05 (p-value ≤ .05) under 95% confidence interval. Table below shows the output
of the findings.
One-Sample Statistics
N Mean Std. Deviation Std. Error Mean
Mortality rates of infants per 1000
live births(BANGLADESH)
20 45.905 13.5746 3.0354
Mortality rates of infants per 1000
live births (AUSTRALIA)
20 50.800 12.3300 2.7571
One-Sample Test
Test Value = 0
t df Sig. (2-tailed)
Mean
Difference
95% Confidence Interval of the
Difference
Lower Upper
Mortality rates of infants per 1000
live births(BANGLADESH)
15.1
23
19 .000 45.9050 39.552 52.258
Cronbach's Alpha
Cronbach's Alpha
Based on
Standardized Items N of Items
.996 .999 2
Hypothesis Testing
T-Test and ANOVA
Based on our research hypothesis, one sample t-test was performed to investigate whether
there is a difference of mortality rate of infants, higher in low level of health care in a country
and lower in a higher level of heath care in a country. The output below demonstrates that
there was no significant difference in mortality rate of infants, higher in low level of health
care in a country and lower in a higher level of heath care in a country since our p-value was
less than 0.05 (p-value ≤ .05) under 95% confidence interval. Table below shows the output
of the findings.
One-Sample Statistics
N Mean Std. Deviation Std. Error Mean
Mortality rates of infants per 1000
live births(BANGLADESH)
20 45.905 13.5746 3.0354
Mortality rates of infants per 1000
live births (AUSTRALIA)
20 50.800 12.3300 2.7571
One-Sample Test
Test Value = 0
t df Sig. (2-tailed)
Mean
Difference
95% Confidence Interval of the
Difference
Lower Upper
Mortality rates of infants per 1000
live births(BANGLADESH)
15.1
23
19 .000 45.9050 39.552 52.258
SLE 251 PROJECT ASSIGNMENT 6
Mortality rates of infants per 1000
live births(AUSTRALIA)
18.4
25
19 .000 50.8000 45.029 56.571
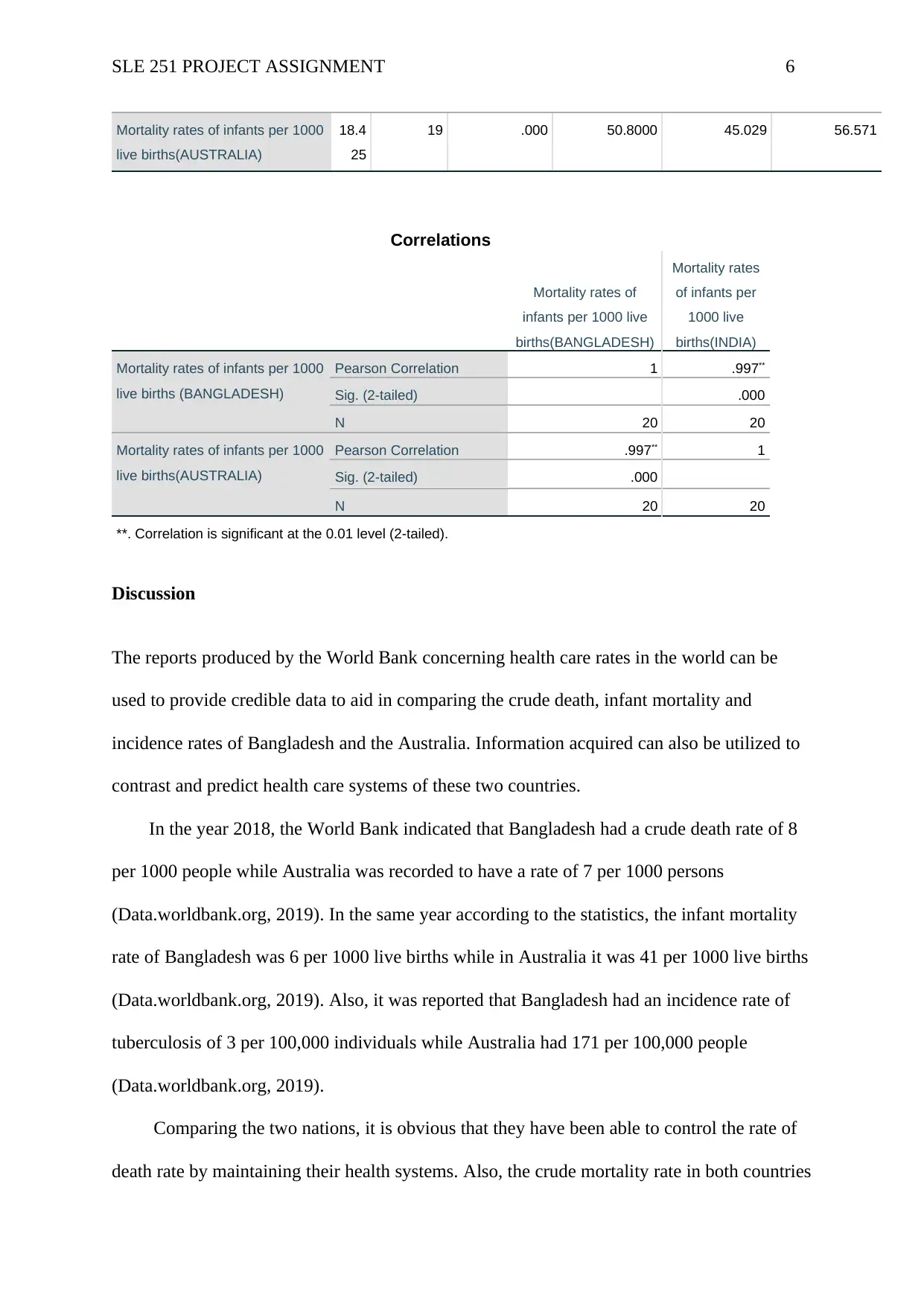
Correlations
Mortality rates of
infants per 1000 live
births(BANGLADESH)
Mortality rates
of infants per
1000 live
births(INDIA)
Mortality rates of infants per 1000
live births (BANGLADESH)
Pearson Correlation 1 .997**
Sig. (2-tailed) .000
N 20 20
Mortality rates of infants per 1000
live births(AUSTRALIA)
Pearson Correlation .997** 1
Sig. (2-tailed) .000
N 20 20
**. Correlation is significant at the 0.01 level (2-tailed).
Discussion
The reports produced by the World Bank concerning health care rates in the world can be
used to provide credible data to aid in comparing the crude death, infant mortality and
incidence rates of Bangladesh and the Australia. Information acquired can also be utilized to
contrast and predict health care systems of these two countries.
In the year 2018, the World Bank indicated that Bangladesh had a crude death rate of 8
per 1000 people while Australia was recorded to have a rate of 7 per 1000 persons
(Data.worldbank.org, 2019). In the same year according to the statistics, the infant mortality
rate of Bangladesh was 6 per 1000 live births while in Australia it was 41 per 1000 live births
(Data.worldbank.org, 2019). Also, it was reported that Bangladesh had an incidence rate of
tuberculosis of 3 per 100,000 individuals while Australia had 171 per 100,000 people
(Data.worldbank.org, 2019).
Comparing the two nations, it is obvious that they have been able to control the rate of
death rate by maintaining their health systems. Also, the crude mortality rate in both countries
Mortality rates of infants per 1000
live births(AUSTRALIA)
18.4
25
19 .000 50.8000 45.029 56.571
Correlations
Mortality rates of
infants per 1000 live
births(BANGLADESH)
Mortality rates
of infants per
1000 live
births(INDIA)
Mortality rates of infants per 1000
live births (BANGLADESH)
Pearson Correlation 1 .997**
Sig. (2-tailed) .000
N 20 20
Mortality rates of infants per 1000
live births(AUSTRALIA)
Pearson Correlation .997** 1
Sig. (2-tailed) .000
N 20 20
**. Correlation is significant at the 0.01 level (2-tailed).
Discussion
The reports produced by the World Bank concerning health care rates in the world can be
used to provide credible data to aid in comparing the crude death, infant mortality and
incidence rates of Bangladesh and the Australia. Information acquired can also be utilized to
contrast and predict health care systems of these two countries.
In the year 2018, the World Bank indicated that Bangladesh had a crude death rate of 8
per 1000 people while Australia was recorded to have a rate of 7 per 1000 persons
(Data.worldbank.org, 2019). In the same year according to the statistics, the infant mortality
rate of Bangladesh was 6 per 1000 live births while in Australia it was 41 per 1000 live births
(Data.worldbank.org, 2019). Also, it was reported that Bangladesh had an incidence rate of
tuberculosis of 3 per 100,000 individuals while Australia had 171 per 100,000 people
(Data.worldbank.org, 2019).
Comparing the two nations, it is obvious that they have been able to control the rate of
death rate by maintaining their health systems. Also, the crude mortality rate in both countries
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SLE 251 PROJECT ASSIGNMENT 7
is almost the same but Bangladesh records higher than Australia due to transitions such as
industrialization; hence, increased death causes as compared to India. However, from the data
provided it is evident that Bangladesh has more improved health system than Australia.
Bangladesh has a low infant mortality rate while that of Australia is a bit high. Also,
tuberculosis is a health challenge in Australia as it is a cause of many deaths as compared to
Bangladesh. The wide gaps between the two countries regarding infant mortality rate and
incidence rate can be attributed to the difference in the level of development and population
ageing. The Bangladesh can efficiently provide adequate sanitation facilities to the
community and also enhance its health expenditure since it’s more developed than India and
less populated; hence, the improved health in the former than in the later.
According to the yearly reports produced by the World Bank in both countries, it is
evident that the performance is impressive as there is a reduction in the rates. By this, it
indicates that the population of the two countries will have a more improved health than the
current state due to the continued globalization. However, it might be impossible for India to
reach the same health care standards as Bangladesh due to the difference in technological
advances. Therefore, despite there being evidence to indicate improved future health in the
two nations; Bangladesh has more potentials of exceling than Australia.
CONCLUSION
Based on the hypothesis testing and ANOVA tests, we can thus assert that there is no
difference of mortality rate of infants, higher in low level of health care in a country and
lower in a higher level of heath care in a country.
is almost the same but Bangladesh records higher than Australia due to transitions such as
industrialization; hence, increased death causes as compared to India. However, from the data
provided it is evident that Bangladesh has more improved health system than Australia.
Bangladesh has a low infant mortality rate while that of Australia is a bit high. Also,
tuberculosis is a health challenge in Australia as it is a cause of many deaths as compared to
Bangladesh. The wide gaps between the two countries regarding infant mortality rate and
incidence rate can be attributed to the difference in the level of development and population
ageing. The Bangladesh can efficiently provide adequate sanitation facilities to the
community and also enhance its health expenditure since it’s more developed than India and
less populated; hence, the improved health in the former than in the later.
According to the yearly reports produced by the World Bank in both countries, it is
evident that the performance is impressive as there is a reduction in the rates. By this, it
indicates that the population of the two countries will have a more improved health than the
current state due to the continued globalization. However, it might be impossible for India to
reach the same health care standards as Bangladesh due to the difference in technological
advances. Therefore, despite there being evidence to indicate improved future health in the
two nations; Bangladesh has more potentials of exceling than Australia.
CONCLUSION
Based on the hypothesis testing and ANOVA tests, we can thus assert that there is no
difference of mortality rate of infants, higher in low level of health care in a country and
lower in a higher level of heath care in a country.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SLE 251 PROJECT ASSIGNMENT 8
References
Korbin Liu, M. M. (1992). International infant mortality rankings: A look behind the
numbers. Health Care Financ Rev, 13(4): 105–118. .
The World Bank. (2019, May 26). Mortality rate, infant (per 1,000 live births). Retrieved
from The World Bank IBRD IDA Data:
https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?
end=2017&locations=BD&start=1960&view=chart
Byington, C. L., Wilkes, J., Korgenski, K., & Sheng, X. (2015). Respiratory syncytial virus–
associated mortality in hospitalized infants and young children. Pediatrics, 135(1),
e24.
Mathews, T. J., MacDorman, M. F., & Thoma, M. E. (2015). Infant mortality statistics from
the 2013 period linked birth/infant death data set.
Panigrahi, P., Parida, S., Nanda, N. C., Satpathy, R., Pradhan, L., Chandel, D. S. ... &
Chaudhry, R. (2017). A randomized synbiotic trial to prevent sepsis among infants in
rural India. Nature, 548(7668), 407.
Sahu, D., Nair, S., Singh, L., Gulati, B. K., & Pandey, A. (2015). Levels, trends & predictors
of infant & child mortality among Scheduled Tribes in rural Australia. The Indian
journal of medical research, 141(5), 709.
References
Korbin Liu, M. M. (1992). International infant mortality rankings: A look behind the
numbers. Health Care Financ Rev, 13(4): 105–118. .
The World Bank. (2019, May 26). Mortality rate, infant (per 1,000 live births). Retrieved
from The World Bank IBRD IDA Data:
https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?
end=2017&locations=BD&start=1960&view=chart
Byington, C. L., Wilkes, J., Korgenski, K., & Sheng, X. (2015). Respiratory syncytial virus–
associated mortality in hospitalized infants and young children. Pediatrics, 135(1),
e24.
Mathews, T. J., MacDorman, M. F., & Thoma, M. E. (2015). Infant mortality statistics from
the 2013 period linked birth/infant death data set.
Panigrahi, P., Parida, S., Nanda, N. C., Satpathy, R., Pradhan, L., Chandel, D. S. ... &
Chaudhry, R. (2017). A randomized synbiotic trial to prevent sepsis among infants in
rural India. Nature, 548(7668), 407.
Sahu, D., Nair, S., Singh, L., Gulati, B. K., & Pandey, A. (2015). Levels, trends & predictors
of infant & child mortality among Scheduled Tribes in rural Australia. The Indian
journal of medical research, 141(5), 709.

SLE 251 PROJECT ASSIGNMENT 9
Subramaniam, P., Ho, J. J., & Davis, P. G. (2016). Prophylactic nasal continuous positive
airway pressure for preventing morbidity and mortality in very preterm
infants. Cochrane Database of Systematic Reviews, (6).
Venkatesh, V., Rai, A., Sykes, T. A., & Aljafari, R. (2016). Combating Infant Mortality in
Rural Australia: Evidence from a Field Study of eHealth Kiosk Imlementations. Mis
Quarterly, 40(2), 353-380.
Subramaniam, P., Ho, J. J., & Davis, P. G. (2016). Prophylactic nasal continuous positive
airway pressure for preventing morbidity and mortality in very preterm
infants. Cochrane Database of Systematic Reviews, (6).
Venkatesh, V., Rai, A., Sykes, T. A., & Aljafari, R. (2016). Combating Infant Mortality in
Rural Australia: Evidence from a Field Study of eHealth Kiosk Imlementations. Mis
Quarterly, 40(2), 353-380.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
SLE 251 PROJECT ASSIGNMENT 10
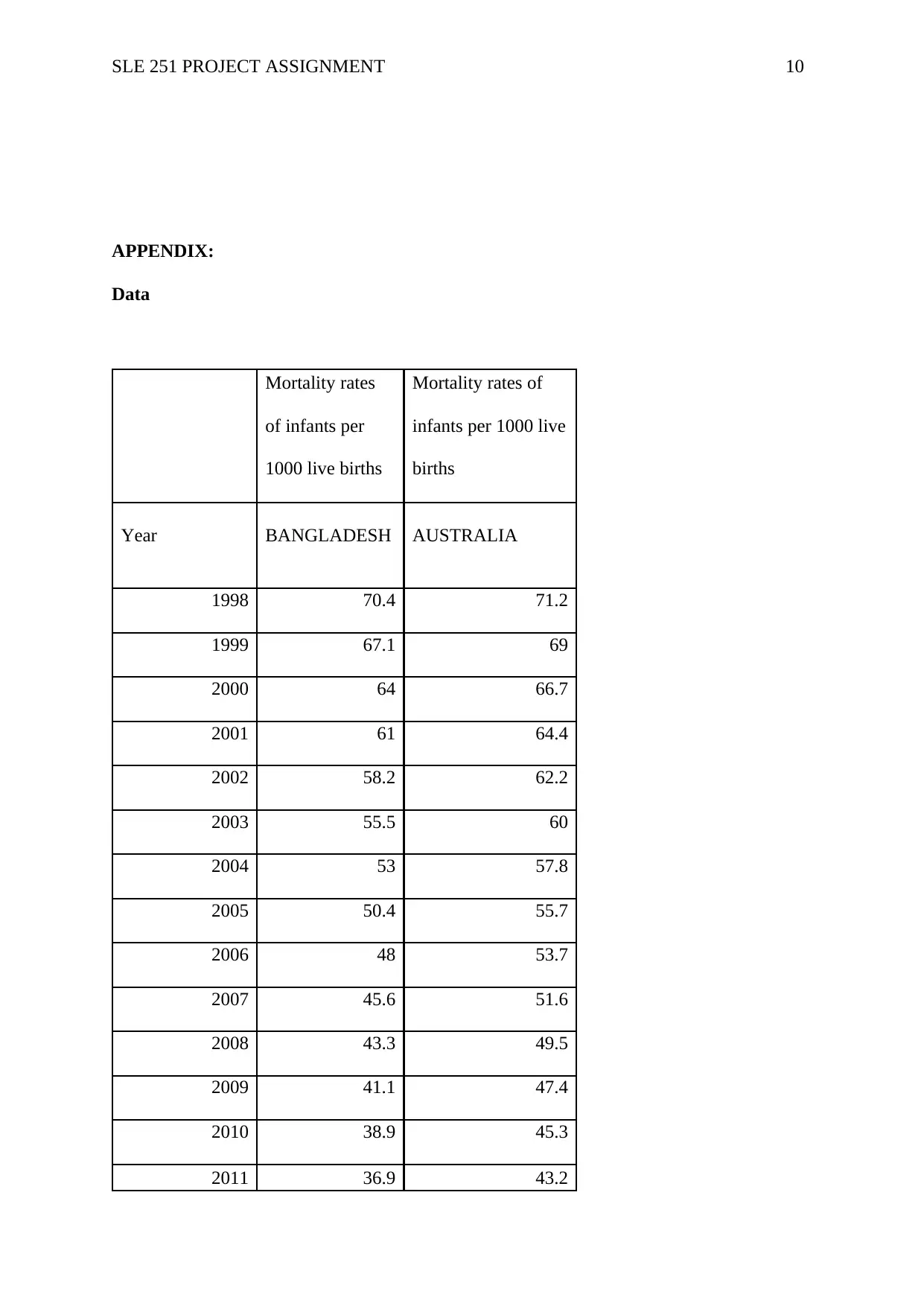
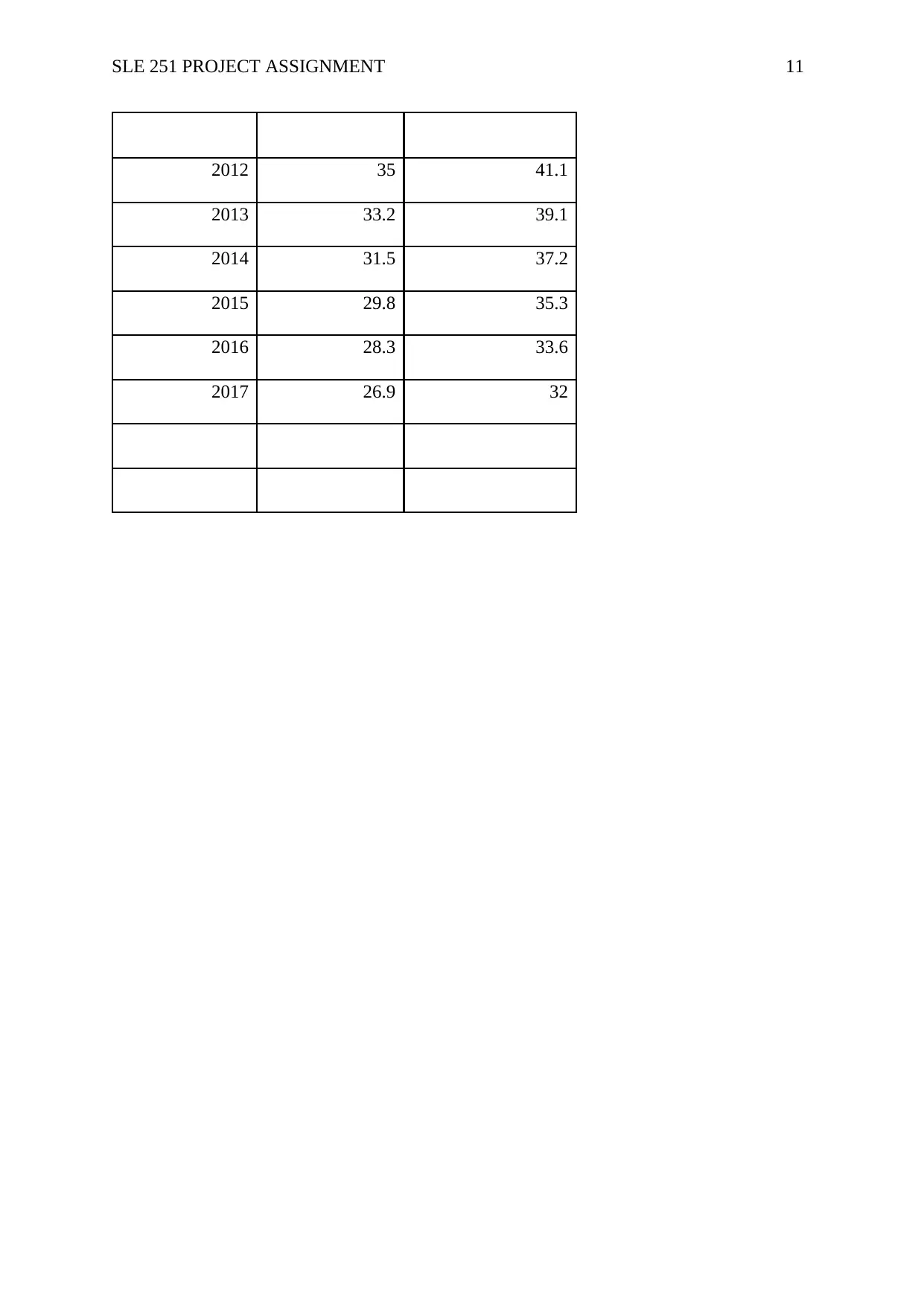
APPENDIX:
Data
Mortality rates
of infants per
1000 live births
Mortality rates of
infants per 1000 live
births
Year BANGLADESH AUSTRALIA
1998 70.4 71.2
1999 67.1 69
2000 64 66.7
2001 61 64.4
2002 58.2 62.2
2003 55.5 60
2004 53 57.8
2005 50.4 55.7
2006 48 53.7
2007 45.6 51.6
2008 43.3 49.5
2009 41.1 47.4
2010 38.9 45.3
2011 36.9 43.2
APPENDIX:
Data
Mortality rates
of infants per
1000 live births
Mortality rates of
infants per 1000 live
births
Year BANGLADESH AUSTRALIA
1998 70.4 71.2
1999 67.1 69
2000 64 66.7
2001 61 64.4
2002 58.2 62.2
2003 55.5 60
2004 53 57.8
2005 50.4 55.7
2006 48 53.7
2007 45.6 51.6
2008 43.3 49.5
2009 41.1 47.4
2010 38.9 45.3
2011 36.9 43.2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
SLE 251 PROJECT ASSIGNMENT 11
2012 35 41.1
2013 33.2 39.1
2014 31.5 37.2
2015 29.8 35.3
2016 28.3 33.6
2017 26.9 32
2012 35 41.1
2013 33.2 39.1
2014 31.5 37.2
2015 29.8 35.3
2016 28.3 33.6
2017 26.9 32
1 out of 11


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.