disease management program PDF
VerifiedAdded on 2022/01/25
|13
|3123
|215
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
MATILDAH MOREMI
201700507 | BACHELOR OF PHARMACY
PHA 327
EXPERIENTIAL ATTACHMENT REPORT AT AFA (MANAGED CARE
ORGANISATION)
201700507 | BACHELOR OF PHARMACY
PHA 327
EXPERIENTIAL ATTACHMENT REPORT AT AFA (MANAGED CARE
ORGANISATION)
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Table of Contents
1.INTRODUCTION..................................................................................................................................2
1.1OBJECTIVES...................................................................................................................................2
2. DISEASE MANAGEMENT PROGRAM (DMP)...............................................................................2
2.1 Role of pharmacist in DMP.............................................................................................................2
2.2 Components of DMP.......................................................................................................................2
2.3 Activities undertaken in DMP........................................................................................................3
3.PHARMACEUTICAL BENEFIT MANAGEMENT..........................................................................3
3.1 Role of the pharmacist in PBM.......................................................................................................3
3.2 Components of PBM........................................................................................................................4
3.3 Activities undertaken in PBM.........................................................................................................4
4. SUCCESSES AND CHALLENGES....................................................................................................4
5. PERSONAL EXPERIENCE................................................................................................................5
REFERENCES..........................................................................................................................................6
APPENDICES...........................................................................................................................................7
Appendix 1 (Managed care organostructure).....................................................................................7
Appendix 2 (Managed care checklist)..................................................................................................8
Appendix 3 (Interview and observation tool)....................................................................................10
1 | P a g e
1.INTRODUCTION..................................................................................................................................2
1.1OBJECTIVES...................................................................................................................................2
2. DISEASE MANAGEMENT PROGRAM (DMP)...............................................................................2
2.1 Role of pharmacist in DMP.............................................................................................................2
2.2 Components of DMP.......................................................................................................................2
2.3 Activities undertaken in DMP........................................................................................................3
3.PHARMACEUTICAL BENEFIT MANAGEMENT..........................................................................3
3.1 Role of the pharmacist in PBM.......................................................................................................3
3.2 Components of PBM........................................................................................................................4
3.3 Activities undertaken in PBM.........................................................................................................4
4. SUCCESSES AND CHALLENGES....................................................................................................4
5. PERSONAL EXPERIENCE................................................................................................................5
REFERENCES..........................................................................................................................................6
APPENDICES...........................................................................................................................................7
Appendix 1 (Managed care organostructure).....................................................................................7
Appendix 2 (Managed care checklist)..................................................................................................8
Appendix 3 (Interview and observation tool)....................................................................................10
1 | P a g e
1.INTRODUCTION
The Associated Fund Administrators (AFA) was established in 1990. AFA offers medical aid
administration and disease management which is provided through the Managed Care Programme. AFA
by far is administering the government medical aid, Botswana Public Officers Medical Aid Scheme
(BPOMAS) and PULA Medical Aid Fund .The role of AFA in this instance is to manage the conditions
of members under the schemes to minimize the risk of waste, fraud and abuse of funds. The services
offered by AFA under Managed care includes Disease Management Programme (DMP), Pharmaceutical
Benefit Management (PBM), Hospital management and Benefit and Underwriting coordinator. It
comprises of a multidisciplinary team made up of pharmacists and pharmacy technicians, nurses, doctors
and IT personnel (See organostructure Appendix 1). For this report the focus will be on DMP and PBM.
1.1OBJECTIVES
To Discuss:
The roles and components under DMP and PBM
The activities undertaken under DMP and PBM
Personal experience, success and challenges encountered
2. DISEASE MANAGEMENT PROGRAM (DMP)
People living with chronic conditions tend to use more health care services that include many hospital and
physician visits as well as more use of prescription drugs. This on its own leads to massive health care
costs which puts a burden on the individuals, employers as well as the government. Here is where now
DMP fits in as it is a program that functions to improve the health of individuals living with chronic
conditions and to reduce the costs that can arise from preventable complications like hospitalizations. In
AFA (Managed Care Organisation) a full DMP is only done for HIV/AIDS and therefore the HIV form is
more detailed than for other conditions. But going forth AFA aims to carry out a full DMP for all the
other conditions.
2.1 Role of pharmacist in DMP
Assists in identifying suitable individuals for the program.
Conducts disease monitoring, for example monitoring of blood pressure in hypertensive patients.
Provides patient education like glucose monitoring even at home.
Assists with medication adherence
Evaluate outcomes of the program i.e. calculates adherence.
2.2 Components of DMP
Have a fully functional system to manage patients; there are at least two systems that are used
being AID for AIDS (to manage HIV patients) and the iMED system.
Population Identification Process: There is a process of what the target population is, how the
population is enrolled and which specific disease the people should have.
Evidence Based Practice Guidelines; to make an informed decision the pharmacist usually consult
a reference which could be for example the 2016 Botswana Integrated HIV Treatment Guideline
which can be used to guide on which dates the patient should go for the next laboratory
investigations such as CD4 count and Viral load.
2 | P a g e
The Associated Fund Administrators (AFA) was established in 1990. AFA offers medical aid
administration and disease management which is provided through the Managed Care Programme. AFA
by far is administering the government medical aid, Botswana Public Officers Medical Aid Scheme
(BPOMAS) and PULA Medical Aid Fund .The role of AFA in this instance is to manage the conditions
of members under the schemes to minimize the risk of waste, fraud and abuse of funds. The services
offered by AFA under Managed care includes Disease Management Programme (DMP), Pharmaceutical
Benefit Management (PBM), Hospital management and Benefit and Underwriting coordinator. It
comprises of a multidisciplinary team made up of pharmacists and pharmacy technicians, nurses, doctors
and IT personnel (See organostructure Appendix 1). For this report the focus will be on DMP and PBM.
1.1OBJECTIVES
To Discuss:
The roles and components under DMP and PBM
The activities undertaken under DMP and PBM
Personal experience, success and challenges encountered
2. DISEASE MANAGEMENT PROGRAM (DMP)
People living with chronic conditions tend to use more health care services that include many hospital and
physician visits as well as more use of prescription drugs. This on its own leads to massive health care
costs which puts a burden on the individuals, employers as well as the government. Here is where now
DMP fits in as it is a program that functions to improve the health of individuals living with chronic
conditions and to reduce the costs that can arise from preventable complications like hospitalizations. In
AFA (Managed Care Organisation) a full DMP is only done for HIV/AIDS and therefore the HIV form is
more detailed than for other conditions. But going forth AFA aims to carry out a full DMP for all the
other conditions.
2.1 Role of pharmacist in DMP
Assists in identifying suitable individuals for the program.
Conducts disease monitoring, for example monitoring of blood pressure in hypertensive patients.
Provides patient education like glucose monitoring even at home.
Assists with medication adherence
Evaluate outcomes of the program i.e. calculates adherence.
2.2 Components of DMP
Have a fully functional system to manage patients; there are at least two systems that are used
being AID for AIDS (to manage HIV patients) and the iMED system.
Population Identification Process: There is a process of what the target population is, how the
population is enrolled and which specific disease the people should have.
Evidence Based Practice Guidelines; to make an informed decision the pharmacist usually consult
a reference which could be for example the 2016 Botswana Integrated HIV Treatment Guideline
which can be used to guide on which dates the patient should go for the next laboratory
investigations such as CD4 count and Viral load.
2 | P a g e
Patient self-management education; individuals enrolled are educated and additional support is
also given in the form of adherence counselling and call consultations.
Process and outcomes measurement; there is a process for measuring outcomes such as health
care service use, expenditures and patient satisfaction. One way of doing this is by calculating
adherence, suppression (target is 95%) and coverage rates.
The above components were sourced from the Disease Management Association of America but upon
conducting a self-checklist the DMP in AFA was also found to be having all the components. (See
appendix 2 for the checklist)
2.3 Activities undertaken in DMP
The following are some of the activities that I managed to carry out.
Review one request for a chronic ex-formulary item. The request was for Empagliflozin
(Jardiance) to be given to a patient with uncontrolled Diabetes Mellitus who also has heart
problems. The other was for Rivaroxaban (Xarelto) to be considered for possible inclusion into
the formulary. In reviewing the requests, the focus was on finding convincing evidence-based
information that there is a great benefit that comes with adding the drug to the chronic basket not
only for one patient but for all patients that may present with similar conditions. Costs, side
effects, monitoring parameters and risks were also considered before reaching a decision. For
example, when doing a review for Xarelto it was considered that Xarelto has less pronounced side
effects than Warfarin, but it is also costly than Warfarin, but Warfarin also requires more
monitoring as compared to Xarelto which does not require monitoring.
Assess chronic benefit application plans; chronic benefit applications forms were given for
individuals with various conditions such as Hypertension, BPH. The requirement was to log into
the iMED system to see if the patient is eligible for being registered for that condition. The
medical aid scheme number was used to search for the patient in the system. Considerations were
made looking at the time of benefit the patient is under i.e., standard, flexi or deluxe, if the
condition is covered under that benefit and the amount of money available. After all had been
verified then the patient could then be enrolled and a letter sent to them.
Review of an ART application form. For this exercise the patient was being switched from
Atripla to Acriptega because the Efavirenz was causing acute liver injury which had however
resolved on stopping efavirenz. The laboratory results such as the Viral load, CD4, Creatine (for
Tenofovir) and dose were also assessed. The Botswana treatment guidelines were then used as
reference guide to determine on when the patients would need to go for lab examinations again.
An authorization of the treatment was then carried out. For this purpose, an intervention note had
to be written. After authorization, the patient would then be referred for Adherence counselling.
3.PHARMACEUTICAL BENEFIT MANAGEMENT
Services designed to help maximize drug effectiveness and contain drug costs by appropriately
influencing the behaviors of prescribing physicians, pharmacists, and members.
3.1 Role of the pharmacist in PBM
Perform drug utilization review
Processes claims
Negotiates rebates and discounts from manufacturing companies
3 | P a g e
also given in the form of adherence counselling and call consultations.
Process and outcomes measurement; there is a process for measuring outcomes such as health
care service use, expenditures and patient satisfaction. One way of doing this is by calculating
adherence, suppression (target is 95%) and coverage rates.
The above components were sourced from the Disease Management Association of America but upon
conducting a self-checklist the DMP in AFA was also found to be having all the components. (See
appendix 2 for the checklist)
2.3 Activities undertaken in DMP
The following are some of the activities that I managed to carry out.
Review one request for a chronic ex-formulary item. The request was for Empagliflozin
(Jardiance) to be given to a patient with uncontrolled Diabetes Mellitus who also has heart
problems. The other was for Rivaroxaban (Xarelto) to be considered for possible inclusion into
the formulary. In reviewing the requests, the focus was on finding convincing evidence-based
information that there is a great benefit that comes with adding the drug to the chronic basket not
only for one patient but for all patients that may present with similar conditions. Costs, side
effects, monitoring parameters and risks were also considered before reaching a decision. For
example, when doing a review for Xarelto it was considered that Xarelto has less pronounced side
effects than Warfarin, but it is also costly than Warfarin, but Warfarin also requires more
monitoring as compared to Xarelto which does not require monitoring.
Assess chronic benefit application plans; chronic benefit applications forms were given for
individuals with various conditions such as Hypertension, BPH. The requirement was to log into
the iMED system to see if the patient is eligible for being registered for that condition. The
medical aid scheme number was used to search for the patient in the system. Considerations were
made looking at the time of benefit the patient is under i.e., standard, flexi or deluxe, if the
condition is covered under that benefit and the amount of money available. After all had been
verified then the patient could then be enrolled and a letter sent to them.
Review of an ART application form. For this exercise the patient was being switched from
Atripla to Acriptega because the Efavirenz was causing acute liver injury which had however
resolved on stopping efavirenz. The laboratory results such as the Viral load, CD4, Creatine (for
Tenofovir) and dose were also assessed. The Botswana treatment guidelines were then used as
reference guide to determine on when the patients would need to go for lab examinations again.
An authorization of the treatment was then carried out. For this purpose, an intervention note had
to be written. After authorization, the patient would then be referred for Adherence counselling.
3.PHARMACEUTICAL BENEFIT MANAGEMENT
Services designed to help maximize drug effectiveness and contain drug costs by appropriately
influencing the behaviors of prescribing physicians, pharmacists, and members.
3.1 Role of the pharmacist in PBM
Perform drug utilization review
Processes claims
Negotiates rebates and discounts from manufacturing companies
3 | P a g e
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Develop and maintain lists, or formularies, of covered medications on behalf of health insurers,
which influence which drugs individuals use and determine out-of-pocket costs
contract directly with individual pharmacies to reimburse for drugs dispensed to beneficiaries.
Prior authorization.
3.2 Components of PBM
Medicine benefit plans;
-Acute medicines benefit. It comprises of the OTC benefit for which the limit is P1000.00
and the Non-dispensing Doctor for which the limit is P750.00. The reason for having limits
on the OTC medicines is to minimize the risk of abuse by customers and for the non-
dispensing doctor the limit is set to minimize medicine errors that can result from doctors
prescribing and also dispensing again
-chronic medicines benefit made up of general, psych and HIV benefit.
-Pharmaceutical and Related Substances benefit
-Appliances benefit; only pay for appliances that have been scientifically proven to be useful
at home. Examples include aero chambers and glucometers.
Reimbursement of medicines (reference pricing); deals with how much money will be paid to
whom and from which benefit will the money be paid from.
Regulation of prices i.e., Single Exit Price (Manufacture’s price). Controls how much prices
can be increased or reduced by. For Brands there is a 10% markup allowed for wholesale and
35% for pharmacies. For generics there is 10% markup for wholesale and 52% for
pharmacies. A higher percentage is allowed as generics are generally cheaper. Pa
Drug utilization review.
3.3 Activities undertaken in PBM
Drug utilization review: logged on the iMED system and audited claims to assess suitability of
patients taking the same medication again that they took less than 14 days. It was taken into
consideration was the type of medication, age, reason for taking the medication. Usually for
chronic conditions such as Hypertension the claims were rejected as most medications are given
as 1 month supply so it cannot be finished in less than 14 days.
Prior authorization: this was done for medicines which are not included in the formulary for
them to be paid for particular patients. Doctors usually send motivation letters explaining
condition of patient so that they can be considered. On site I had an opportunity to go through
request for the drugs; Goserelin which in Botswana is indicated for cancer but was requested for
endometriosis. To authorize it was taken into consideration if the drug can be used for what it is
requested for, the cost and from which benefit it would pay from.
4. SUCCESSES AND CHALLENGES
Success: being able to do and complete on time all the activities I was assigned to do such as
processing of audits for patients taking acute medicines, prior authorization, drug utilization
review and reviewing at least one request for chronic ex-formulary items.
Challenge; due to limited time I was not able to do some activities that were expected by the
school such as selecting one patient for whom medication therapy management will be applied
to. The other issue was that of using the iMED system. As it was the first time I at times missed
4 | P a g e
which influence which drugs individuals use and determine out-of-pocket costs
contract directly with individual pharmacies to reimburse for drugs dispensed to beneficiaries.
Prior authorization.
3.2 Components of PBM
Medicine benefit plans;
-Acute medicines benefit. It comprises of the OTC benefit for which the limit is P1000.00
and the Non-dispensing Doctor for which the limit is P750.00. The reason for having limits
on the OTC medicines is to minimize the risk of abuse by customers and for the non-
dispensing doctor the limit is set to minimize medicine errors that can result from doctors
prescribing and also dispensing again
-chronic medicines benefit made up of general, psych and HIV benefit.
-Pharmaceutical and Related Substances benefit
-Appliances benefit; only pay for appliances that have been scientifically proven to be useful
at home. Examples include aero chambers and glucometers.
Reimbursement of medicines (reference pricing); deals with how much money will be paid to
whom and from which benefit will the money be paid from.
Regulation of prices i.e., Single Exit Price (Manufacture’s price). Controls how much prices
can be increased or reduced by. For Brands there is a 10% markup allowed for wholesale and
35% for pharmacies. For generics there is 10% markup for wholesale and 52% for
pharmacies. A higher percentage is allowed as generics are generally cheaper. Pa
Drug utilization review.
3.3 Activities undertaken in PBM
Drug utilization review: logged on the iMED system and audited claims to assess suitability of
patients taking the same medication again that they took less than 14 days. It was taken into
consideration was the type of medication, age, reason for taking the medication. Usually for
chronic conditions such as Hypertension the claims were rejected as most medications are given
as 1 month supply so it cannot be finished in less than 14 days.
Prior authorization: this was done for medicines which are not included in the formulary for
them to be paid for particular patients. Doctors usually send motivation letters explaining
condition of patient so that they can be considered. On site I had an opportunity to go through
request for the drugs; Goserelin which in Botswana is indicated for cancer but was requested for
endometriosis. To authorize it was taken into consideration if the drug can be used for what it is
requested for, the cost and from which benefit it would pay from.
4. SUCCESSES AND CHALLENGES
Success: being able to do and complete on time all the activities I was assigned to do such as
processing of audits for patients taking acute medicines, prior authorization, drug utilization
review and reviewing at least one request for chronic ex-formulary items.
Challenge; due to limited time I was not able to do some activities that were expected by the
school such as selecting one patient for whom medication therapy management will be applied
to. The other issue was that of using the iMED system. As it was the first time I at times missed
4 | P a g e
some steps which meant I would have to ask for help from the supervisor or start again which
caused me to take more time on the assignments than I would have.
5. PERSONAL EXPERIENCE
Personally, this is the first experiential attachment that has made me to realize and appreciate other crucial
roles that pharmacists play other than their primary role of dispensing. Having a chance to see a
pharmacists have on call consultations with patients and doctors was also a great experience because it is
not something that I see every day, but it is rather what I mostly hear in class that pharmacists should
always make a follow up. This has helped me to know the importance of making follow ups as it gives
patients assurance and ensures that as the pharmacist, I always have correct information instead of
making assumption. Doing the exercises has helped me to realize that I need to always have reference
standards such as treatment guidelines and the national formularies, have up-to date information about the
medicines and their uses and always make decisions that I can back up by evidence. It has taught me that
in the future I should always be cautious of the decisions I make, always be in a position to account for
my actions as not being able to do so may result in serious repercussions such as being sued. I should
always be confident and stand for what I believe in as I am on the receiving end and should therefore not
be intimidated by other colleagues, especially doctors. Dealing with real life cases was such a great
experience as it gave me an essence of how the real workplace will be like soon. Helped me to know what
approaches I can take when I am presented with a particular case. Overall, this was a wonderful
experience, the staff were very friendly and always willing to help. I wish we had more time there and not
just a week and I would recommend that I the future we go there for more than a week and that all the
students get a chance to go to an MCO.
5 | P a g e
caused me to take more time on the assignments than I would have.
5. PERSONAL EXPERIENCE
Personally, this is the first experiential attachment that has made me to realize and appreciate other crucial
roles that pharmacists play other than their primary role of dispensing. Having a chance to see a
pharmacists have on call consultations with patients and doctors was also a great experience because it is
not something that I see every day, but it is rather what I mostly hear in class that pharmacists should
always make a follow up. This has helped me to know the importance of making follow ups as it gives
patients assurance and ensures that as the pharmacist, I always have correct information instead of
making assumption. Doing the exercises has helped me to realize that I need to always have reference
standards such as treatment guidelines and the national formularies, have up-to date information about the
medicines and their uses and always make decisions that I can back up by evidence. It has taught me that
in the future I should always be cautious of the decisions I make, always be in a position to account for
my actions as not being able to do so may result in serious repercussions such as being sued. I should
always be confident and stand for what I believe in as I am on the receiving end and should therefore not
be intimidated by other colleagues, especially doctors. Dealing with real life cases was such a great
experience as it gave me an essence of how the real workplace will be like soon. Helped me to know what
approaches I can take when I am presented with a particular case. Overall, this was a wonderful
experience, the staff were very friendly and always willing to help. I wish we had more time there and not
just a week and I would recommend that I the future we go there for more than a week and that all the
students get a chance to go to an MCO.
5 | P a g e
REFERENCES
AFA . (n.d.). Retrieved from https://afa.co.bw
Health Policy Institute . (2020, Jul 05). Retrieved from https://hpi.georgetown.edu/management/
The CommonWealth Fund. (2019, April 22). Retrieved from
https://www.commonwealthfund.org/publications/explainer/2019/apr/pharmacy-benefit-
managers-and-their-role-drug-spending
6 | P a g e
AFA . (n.d.). Retrieved from https://afa.co.bw
Health Policy Institute . (2020, Jul 05). Retrieved from https://hpi.georgetown.edu/management/
The CommonWealth Fund. (2019, April 22). Retrieved from
https://www.commonwealthfund.org/publications/explainer/2019/apr/pharmacy-benefit-
managers-and-their-role-drug-spending
6 | P a g e
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
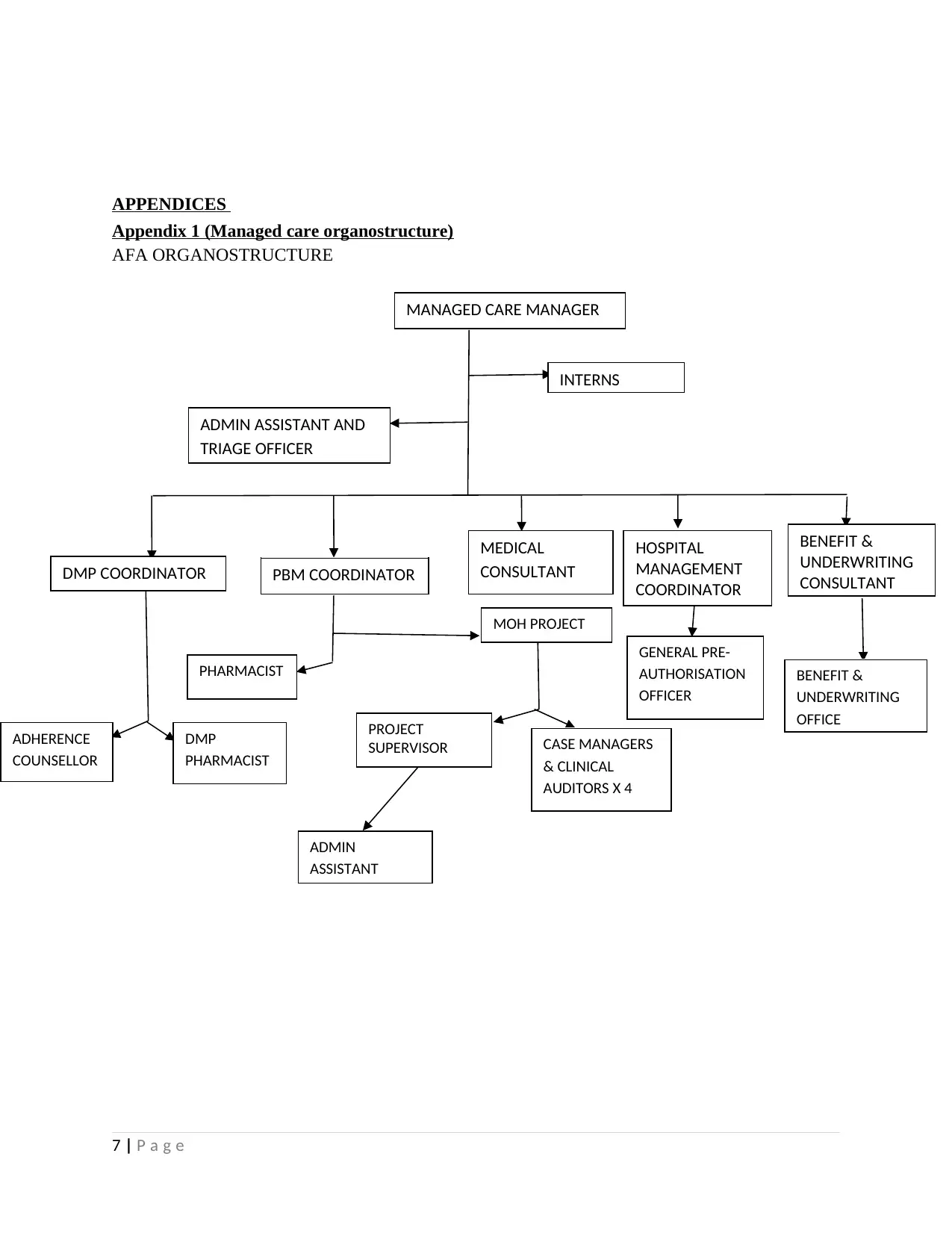
APPENDICES
Appendix 1 (Managed care organostructure)
AFA ORGANOSTRUCTURE
7 | P a g e
MANAGED CARE MANAGER
INTERNS
ADMIN ASSISTANT AND
TRIAGE OFFICER
DMP COORDINATOR PBM COORDINATOR
MEDICAL
CONSULTANT
HOSPITAL
MANAGEMENT
COORDINATOR
BENEFIT &
UNDERWRITING
CONSULTANT
ADHERENCE
COUNSELLOR
DMP
PHARMACIST
PHARMACIST
MOH PROJECT
PROJECT
SUPERVISOR CASE MANAGERS
& CLINICAL
AUDITORS X 4
ADMIN
ASSISTANT
GENERAL PRE-
AUTHORISATION
OFFICER
BENEFIT &
UNDERWRITING
OFFICE
Appendix 1 (Managed care organostructure)
AFA ORGANOSTRUCTURE
7 | P a g e
MANAGED CARE MANAGER
INTERNS
ADMIN ASSISTANT AND
TRIAGE OFFICER
DMP COORDINATOR PBM COORDINATOR
MEDICAL
CONSULTANT
HOSPITAL
MANAGEMENT
COORDINATOR
BENEFIT &
UNDERWRITING
CONSULTANT
ADHERENCE
COUNSELLOR
DMP
PHARMACIST
PHARMACIST
MOH PROJECT
PROJECT
SUPERVISOR CASE MANAGERS
& CLINICAL
AUDITORS X 4
ADMIN
ASSISTANT
GENERAL PRE-
AUTHORISATION
OFFICER
BENEFIT &
UNDERWRITING
OFFICE
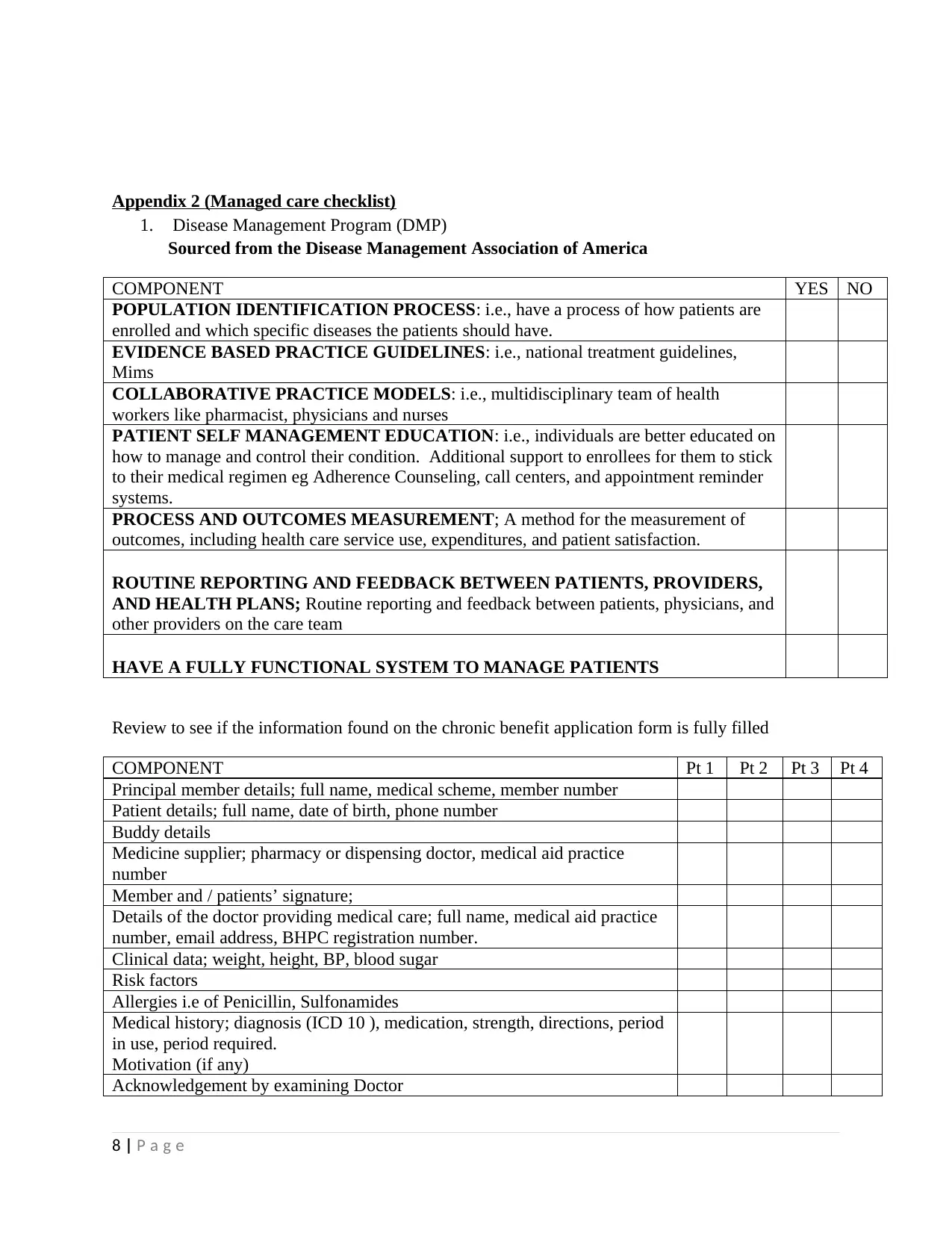
Appendix 2 (Managed care checklist)
1. Disease Management Program (DMP)
Sourced from the Disease Management Association of America
COMPONENT YES NO
POPULATION IDENTIFICATION PROCESS: i.e., have a process of how patients are
enrolled and which specific diseases the patients should have.
EVIDENCE BASED PRACTICE GUIDELINES: i.e., national treatment guidelines,
Mims
COLLABORATIVE PRACTICE MODELS: i.e., multidisciplinary team of health
workers like pharmacist, physicians and nurses
PATIENT SELF MANAGEMENT EDUCATION: i.e., individuals are better educated on
how to manage and control their condition. Additional support to enrollees for them to stick
to their medical regimen eg Adherence Counseling, call centers, and appointment reminder
systems.
PROCESS AND OUTCOMES MEASUREMENT; A method for the measurement of
outcomes, including health care service use, expenditures, and patient satisfaction.
ROUTINE REPORTING AND FEEDBACK BETWEEN PATIENTS, PROVIDERS,
AND HEALTH PLANS; Routine reporting and feedback between patients, physicians, and
other providers on the care team
HAVE A FULLY FUNCTIONAL SYSTEM TO MANAGE PATIENTS
Review to see if the information found on the chronic benefit application form is fully filled
COMPONENT Pt 1 Pt 2 Pt 3 Pt 4
Principal member details; full name, medical scheme, member number
Patient details; full name, date of birth, phone number
Buddy details
Medicine supplier; pharmacy or dispensing doctor, medical aid practice
number
Member and / patients’ signature;
Details of the doctor providing medical care; full name, medical aid practice
number, email address, BHPC registration number.
Clinical data; weight, height, BP, blood sugar
Risk factors
Allergies i.e of Penicillin, Sulfonamides
Medical history; diagnosis (ICD 10 ), medication, strength, directions, period
in use, period required.
Motivation (if any)
Acknowledgement by examining Doctor
8 | P a g e
1. Disease Management Program (DMP)
Sourced from the Disease Management Association of America
COMPONENT YES NO
POPULATION IDENTIFICATION PROCESS: i.e., have a process of how patients are
enrolled and which specific diseases the patients should have.
EVIDENCE BASED PRACTICE GUIDELINES: i.e., national treatment guidelines,
Mims
COLLABORATIVE PRACTICE MODELS: i.e., multidisciplinary team of health
workers like pharmacist, physicians and nurses
PATIENT SELF MANAGEMENT EDUCATION: i.e., individuals are better educated on
how to manage and control their condition. Additional support to enrollees for them to stick
to their medical regimen eg Adherence Counseling, call centers, and appointment reminder
systems.
PROCESS AND OUTCOMES MEASUREMENT; A method for the measurement of
outcomes, including health care service use, expenditures, and patient satisfaction.
ROUTINE REPORTING AND FEEDBACK BETWEEN PATIENTS, PROVIDERS,
AND HEALTH PLANS; Routine reporting and feedback between patients, physicians, and
other providers on the care team
HAVE A FULLY FUNCTIONAL SYSTEM TO MANAGE PATIENTS
Review to see if the information found on the chronic benefit application form is fully filled
COMPONENT Pt 1 Pt 2 Pt 3 Pt 4
Principal member details; full name, medical scheme, member number
Patient details; full name, date of birth, phone number
Buddy details
Medicine supplier; pharmacy or dispensing doctor, medical aid practice
number
Member and / patients’ signature;
Details of the doctor providing medical care; full name, medical aid practice
number, email address, BHPC registration number.
Clinical data; weight, height, BP, blood sugar
Risk factors
Allergies i.e of Penicillin, Sulfonamides
Medical history; diagnosis (ICD 10 ), medication, strength, directions, period
in use, period required.
Motivation (if any)
Acknowledgement by examining Doctor
8 | P a g e
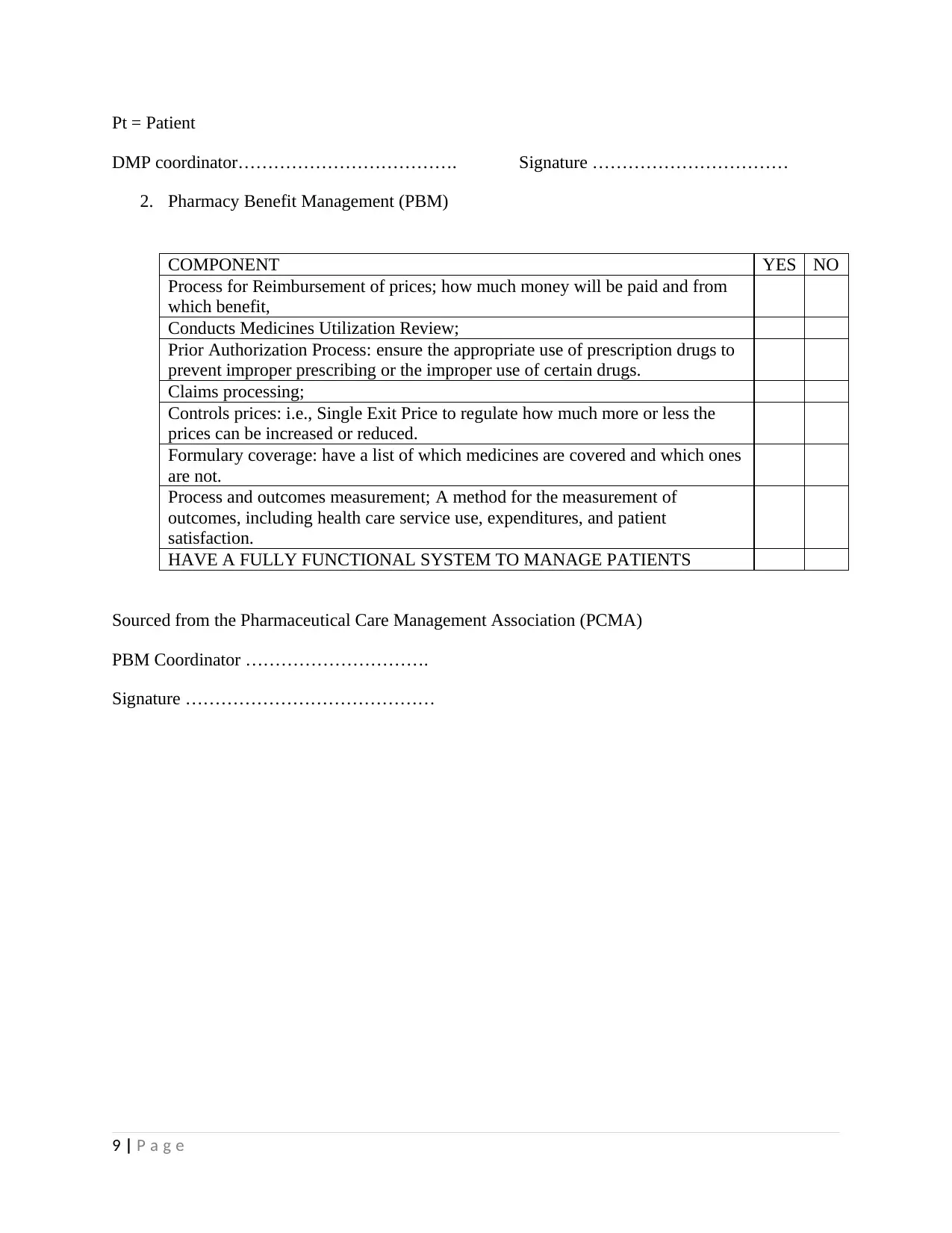
Pt = Patient
DMP coordinator………………………………. Signature ……………………………
2. Pharmacy Benefit Management (PBM)
COMPONENT YES NO
Process for Reimbursement of prices; how much money will be paid and from
which benefit,
Conducts Medicines Utilization Review;
Prior Authorization Process: ensure the appropriate use of prescription drugs to
prevent improper prescribing or the improper use of certain drugs.
Claims processing;
Controls prices: i.e., Single Exit Price to regulate how much more or less the
prices can be increased or reduced.
Formulary coverage: have a list of which medicines are covered and which ones
are not.
Process and outcomes measurement; A method for the measurement of
outcomes, including health care service use, expenditures, and patient
satisfaction.
HAVE A FULLY FUNCTIONAL SYSTEM TO MANAGE PATIENTS
Sourced from the Pharmaceutical Care Management Association (PCMA)
PBM Coordinator ………………………….
Signature ……………………………………
9 | P a g e
DMP coordinator………………………………. Signature ……………………………
2. Pharmacy Benefit Management (PBM)
COMPONENT YES NO
Process for Reimbursement of prices; how much money will be paid and from
which benefit,
Conducts Medicines Utilization Review;
Prior Authorization Process: ensure the appropriate use of prescription drugs to
prevent improper prescribing or the improper use of certain drugs.
Claims processing;
Controls prices: i.e., Single Exit Price to regulate how much more or less the
prices can be increased or reduced.
Formulary coverage: have a list of which medicines are covered and which ones
are not.
Process and outcomes measurement; A method for the measurement of
outcomes, including health care service use, expenditures, and patient
satisfaction.
HAVE A FULLY FUNCTIONAL SYSTEM TO MANAGE PATIENTS
Sourced from the Pharmaceutical Care Management Association (PCMA)
PBM Coordinator ………………………….
Signature ……………………………………
9 | P a g e
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Appendix 3 (Interview and observation tool)
Interview and observational tool for managed care
1. What is the role of the managed care in the health system financing?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
2. How is health care financed?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………………………………………….
3. How are the risks mitigated by the MCO?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
4. Who are the customers and stakeholders of the MCO?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
5. Explain the process of monitoring for effectiveness of the managed care interventions.
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………….
6. What are the roles of the pharmacists and pharmacy technicians ?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
10 | P a g e
Interview and observational tool for managed care
1. What is the role of the managed care in the health system financing?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
2. How is health care financed?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………………………………………….
3. How are the risks mitigated by the MCO?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
4. Who are the customers and stakeholders of the MCO?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
5. Explain the process of monitoring for effectiveness of the managed care interventions.
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………….
6. What are the roles of the pharmacists and pharmacy technicians ?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
10 | P a g e
7. What are the various activities in the MCO?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………….
8. Please list the medicine benefit plans?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
9. How are prices reimbursed?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
10. Briefly explain the medication use review process
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
OBSERVATIONS
11 | P a g e
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………………………………………………….
8. Please list the medicine benefit plans?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
9. How are prices reimbursed?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
……………….
10. Briefly explain the medication use review process
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
…………………………………………………………………………………
OBSERVATIONS
11 | P a g e

THANK YOU!
12 | P a g e
12 | P a g e
1 out of 13
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.