Evaluating Vitamin D's Impact on Diabetes in Saudi Children
VerifiedAdded on 2023/06/11
|12
|4038
|92
Project
AI Summary
This research proposal aims to investigate the relationship between vitamin D deficiency in pregnant women and the subsequent development of type 1 diabetes mellitus (T1DM) in their children aged 1-4 years in the Kingdom of Saudi Arabia. The study employs a cohort design, recruiting 100 pregnant women and their children, to assess the impact of vitamin D supplementation on reducing the occurrence of T1DM. Data collection involves gathering information on vitamin D levels (25OHD) and supplementation details from hospital records, as well as measuring HbA1c and glucose levels in the children using HPLC and glucose strips, respectively. Statistical analysis will be conducted using SPSS to determine the correlation between vitamin D levels, supplementation, and T1DM incidence, while also considering socioeconomic factors and gender. The study seeks to establish a clear exposure-outcome relationship, providing evidence for the role of vitamin D in preventing T1DM in children and informing public health interventions in Saudi Arabia. Ethical considerations, including informed consent and confidentiality, are prioritized throughout the research process.
Epidemiology of Non-Communicable Diseases
1
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Title: Evaluation of outcome of vitamin D supplementation in vitamin D deficient
pregnant women on the incidence of Diabetes Mellitus type 1 in children of age between
1 to 4 years in Kingdom of Saudi Aribia
Synopsis:
This study will be planned to find association among vitamin deficiency, vitamin
supplementation and T1DM. It is very necessary to carry out this intervention because fewer
studies are existing for association among vitamin deficiency, vitamin supplementation and
T1DM. In this cohort study 100 women and 100 children will be recruited. This cohort study
will be helpful in identifying exposure-outcome relationship. Influence of socioeconomic
factors and gender on outcome of study will be assessed. Confidentiality will be maintained
for identity of women and children. This study will be carried out in two stages. In first stage,
data will be collected for vitamin D in pregnant women. In second stage, their children will
be assessed for the occurrence of T1DM. Data related to 25OHD levels and vitamin D
supplementation will be gathered from records of hospitals. HPLC and glucose strips will be
used for estimation of HbA1c and glucose levels in children respectively. SPSS statistical
software package version 18.0. will be used for statistical analysis. Potential bias, limitations
and confounding factors will be assessed and proper attention will be given to eliminate these
factors. This cohort study will establish effect of vitamin D deficiency and vitamin D
supplementation on occurrence of TIDM in their children.
2
pregnant women on the incidence of Diabetes Mellitus type 1 in children of age between
1 to 4 years in Kingdom of Saudi Aribia
Synopsis:
This study will be planned to find association among vitamin deficiency, vitamin
supplementation and T1DM. It is very necessary to carry out this intervention because fewer
studies are existing for association among vitamin deficiency, vitamin supplementation and
T1DM. In this cohort study 100 women and 100 children will be recruited. This cohort study
will be helpful in identifying exposure-outcome relationship. Influence of socioeconomic
factors and gender on outcome of study will be assessed. Confidentiality will be maintained
for identity of women and children. This study will be carried out in two stages. In first stage,
data will be collected for vitamin D in pregnant women. In second stage, their children will
be assessed for the occurrence of T1DM. Data related to 25OHD levels and vitamin D
supplementation will be gathered from records of hospitals. HPLC and glucose strips will be
used for estimation of HbA1c and glucose levels in children respectively. SPSS statistical
software package version 18.0. will be used for statistical analysis. Potential bias, limitations
and confounding factors will be assessed and proper attention will be given to eliminate these
factors. This cohort study will establish effect of vitamin D deficiency and vitamin D
supplementation on occurrence of TIDM in their children.
2
Background:
Vitamin D plays important role in bone health. Deficiency of vitamin D lead to development
of rickets in children and osteomalacia in adults. Deficiency of vitamin D also lead to
development of disease like cardiovascular disease, cancer, autoimmune diseases and type 1
and type 2 diabetes mellitus. In the blood samples, vitamin D can be estimated as 25-
hydroxy vitamin D (25OHD) which is its metabolite. Hypovitaminosis is a condition
associated with vitamin deficiency and it occurs in both pregnant and non-pregnant women.
Factors responsible for the occurrence of hypovitaminosis in children are impaired sunlight
exposure, obesity and latitude (Holick, 2007). Decline in the 25OHD levels in pregnant
women occur with the advanced stages of gestation. Placental barrier is the only delivery
source for supply of vitamin D to foetus. It indicates foetus particularly dependent on mother
for vitamin D. Vitamin D deficiency in mother can result in different conditions in mothers
like pre-eclampsia, gestational diabetes, bacterial vaginosis, pre-term delivery and caesarean
section (Ginde et al., 2010). Moreover, vitamin D deficiency in pregnant women can lead to
development of conditions such as multiple sclerosis, cardiovascular disease, schizophrenia,
certain cancers and other autoimmune diseases such as type 1 diabetes mellitus (T1DM) and
lupus in children. It is evident that vitamin D deficiency can occur between 24 – 28 weeks of
gestation in women with gestational diabetes. 83 % and 29 % of women with gestational
diabetes exhibit 25OHD levels <50 nmol/L and 15 nmol/L respectively (Soheilykhah et al.,
2010; Hossein-Nezhad et al., 2007).
Deficiency of vitamin D can lead to impaired metabolism of glucose and insulin. It can lead
to reduced energy availability to the foetus. Few of the studies indicated that vitamin D lead
to improved insulin sensitivity. However, valid and robust evidence is not available for role
of vitamin D in insulin sensitivity. Most likely reason for the development of TIDM in
children might be due to reduced levels if vitamin D in the children. Hence, pregnant women
should be supplemented with vitamin D. Vitamin D supplementation can lead to improved
insulin sensitivity and it can reach to its optimum level due to vitamin D supplementation on
the regular basis (Alvarez and Ashraf, 2010)
Vitamin D analysis and its correlation with the different health issues is a challenging task.
Challenges associated with the vitamin D are variable actions of vitamin D, ubiquity of
vitamin D receptors in the body and predominant nature of vitamin D deficiency. Hence, it is
necessity to establish robust relationship among these factors. To establish this relationship
3
Vitamin D plays important role in bone health. Deficiency of vitamin D lead to development
of rickets in children and osteomalacia in adults. Deficiency of vitamin D also lead to
development of disease like cardiovascular disease, cancer, autoimmune diseases and type 1
and type 2 diabetes mellitus. In the blood samples, vitamin D can be estimated as 25-
hydroxy vitamin D (25OHD) which is its metabolite. Hypovitaminosis is a condition
associated with vitamin deficiency and it occurs in both pregnant and non-pregnant women.
Factors responsible for the occurrence of hypovitaminosis in children are impaired sunlight
exposure, obesity and latitude (Holick, 2007). Decline in the 25OHD levels in pregnant
women occur with the advanced stages of gestation. Placental barrier is the only delivery
source for supply of vitamin D to foetus. It indicates foetus particularly dependent on mother
for vitamin D. Vitamin D deficiency in mother can result in different conditions in mothers
like pre-eclampsia, gestational diabetes, bacterial vaginosis, pre-term delivery and caesarean
section (Ginde et al., 2010). Moreover, vitamin D deficiency in pregnant women can lead to
development of conditions such as multiple sclerosis, cardiovascular disease, schizophrenia,
certain cancers and other autoimmune diseases such as type 1 diabetes mellitus (T1DM) and
lupus in children. It is evident that vitamin D deficiency can occur between 24 – 28 weeks of
gestation in women with gestational diabetes. 83 % and 29 % of women with gestational
diabetes exhibit 25OHD levels <50 nmol/L and 15 nmol/L respectively (Soheilykhah et al.,
2010; Hossein-Nezhad et al., 2007).
Deficiency of vitamin D can lead to impaired metabolism of glucose and insulin. It can lead
to reduced energy availability to the foetus. Few of the studies indicated that vitamin D lead
to improved insulin sensitivity. However, valid and robust evidence is not available for role
of vitamin D in insulin sensitivity. Most likely reason for the development of TIDM in
children might be due to reduced levels if vitamin D in the children. Hence, pregnant women
should be supplemented with vitamin D. Vitamin D supplementation can lead to improved
insulin sensitivity and it can reach to its optimum level due to vitamin D supplementation on
the regular basis (Alvarez and Ashraf, 2010)
Vitamin D analysis and its correlation with the different health issues is a challenging task.
Challenges associated with the vitamin D are variable actions of vitamin D, ubiquity of
vitamin D receptors in the body and predominant nature of vitamin D deficiency. Hence, it is
necessity to establish robust relationship among these factors. To establish this relationship
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
cohort study will be planned. Exposure-outcome relationship will be established in this
cohort study in women from the Kingdom of Saudi Arabia.
Aim:
To reduce occurrence of TIDM in children by supplementation of vitamin D in pregnant
women.
To collect data related to vitamin D deficiency in pregnant women.
To collect data related to vitamin D supplementation in pregnant with vitamin D deficiency.
To estimate HbA1c and glucose levels in children.
To establish relationship between vitamin D supplementation and TIDM in the children.
Hypothesis:
Hypothesis can be stated as :
Vitamin D deficiency in pregnant women can lead to development of T1DM in their children.
Optimum level of supplementation of vitamin D in pregnant women can be helpful in
managing TIDM in their children.
Study design:
In this research, cohort study design will be employed. In this type of study desgn,
participants with the same features are being recruited. In this study, both the current and
historical cohorts will be recruited. This type of cohort studies can be considered as true
prospective studies because in this study data can be collected before the information of the
development of disease (Kung, 2007; Stephen et al., 2013). In the proposed study, vitamin D
deficiency data in the pregnant women will be collected prior to assessment of TIDM in their
children. Common characteristics shared by the participants include pregnant women with
vitamin D deficiency and vitamin D supplementation to these women. In the evaluation
phase, children int the age group 1 – 4 years will be evaluated and these children will be of
the same selected mothers.
4
cohort study in women from the Kingdom of Saudi Arabia.
Aim:
To reduce occurrence of TIDM in children by supplementation of vitamin D in pregnant
women.
To collect data related to vitamin D deficiency in pregnant women.
To collect data related to vitamin D supplementation in pregnant with vitamin D deficiency.
To estimate HbA1c and glucose levels in children.
To establish relationship between vitamin D supplementation and TIDM in the children.
Hypothesis:
Hypothesis can be stated as :
Vitamin D deficiency in pregnant women can lead to development of T1DM in their children.
Optimum level of supplementation of vitamin D in pregnant women can be helpful in
managing TIDM in their children.
Study design:
In this research, cohort study design will be employed. In this type of study desgn,
participants with the same features are being recruited. In this study, both the current and
historical cohorts will be recruited. This type of cohort studies can be considered as true
prospective studies because in this study data can be collected before the information of the
development of disease (Kung, 2007; Stephen et al., 2013). In the proposed study, vitamin D
deficiency data in the pregnant women will be collected prior to assessment of TIDM in their
children. Common characteristics shared by the participants include pregnant women with
vitamin D deficiency and vitamin D supplementation to these women. In the evaluation
phase, children int the age group 1 – 4 years will be evaluated and these children will be of
the same selected mothers.
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
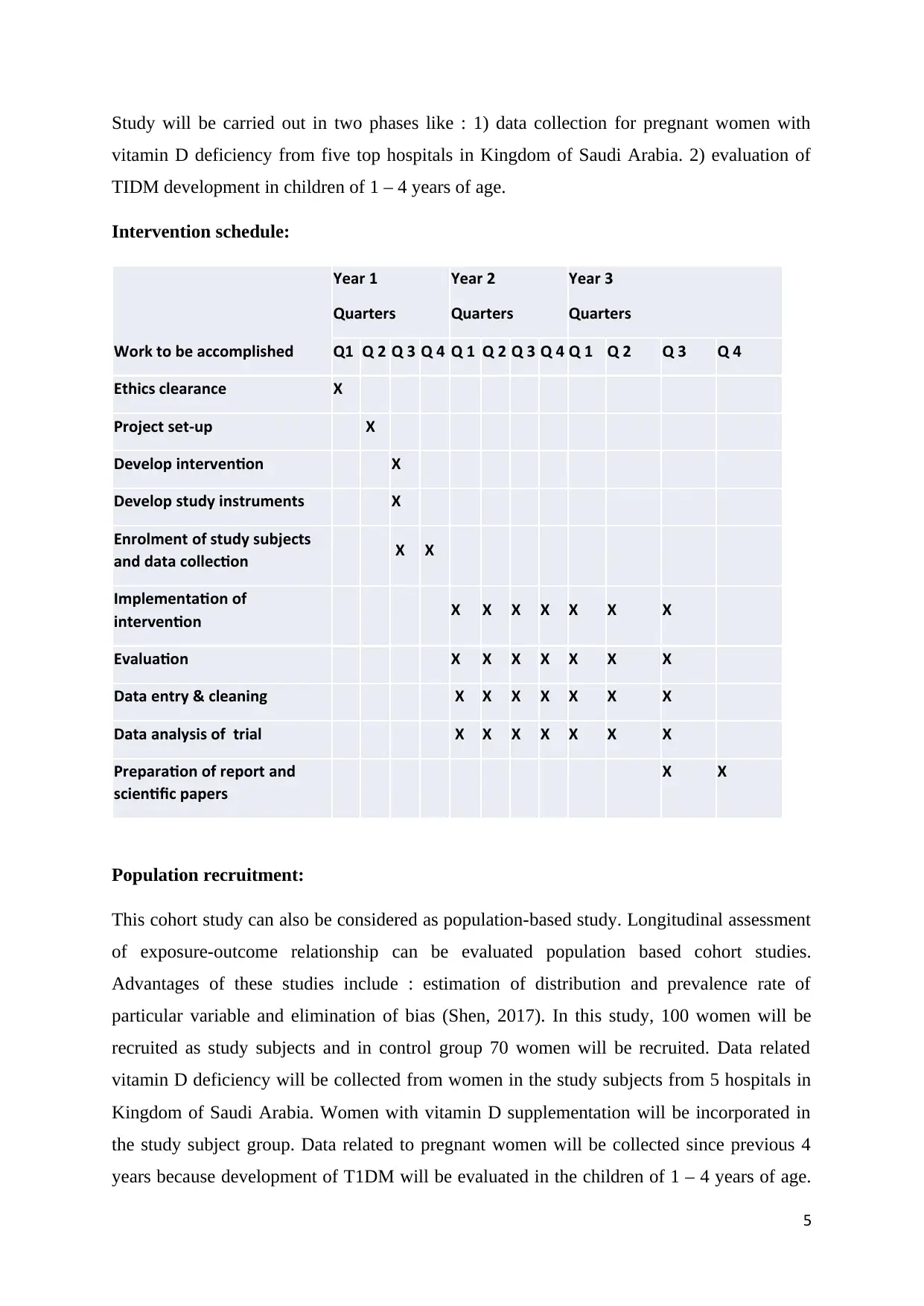
Study will be carried out in two phases like : 1) data collection for pregnant women with
vitamin D deficiency from five top hospitals in Kingdom of Saudi Arabia. 2) evaluation of
TIDM development in children of 1 – 4 years of age.
Intervention schedule:
Work to be accomplished
Year 1
Quarters
Year 2
Quarters
Year 3
Quarters
Q1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q 4
Ethics clearance X
Project set-up X
Develop intervention X
Develop study instruments X
Enrolment of study subjects
and data collection X X
Implementation of
intervention X X X X X X X
Evaluation X X X X X X X
Data entry & cleaning X X X X X X X
Data analysis of trial X X X X X X X
Preparation of report and
scientific papers
X X
Population recruitment:
This cohort study can also be considered as population-based study. Longitudinal assessment
of exposure-outcome relationship can be evaluated population based cohort studies.
Advantages of these studies include : estimation of distribution and prevalence rate of
particular variable and elimination of bias (Shen, 2017). In this study, 100 women will be
recruited as study subjects and in control group 70 women will be recruited. Data related
vitamin D deficiency will be collected from women in the study subjects from 5 hospitals in
Kingdom of Saudi Arabia. Women with vitamin D supplementation will be incorporated in
the study subject group. Data related to pregnant women will be collected since previous 4
years because development of T1DM will be evaluated in the children of 1 – 4 years of age.
5
vitamin D deficiency from five top hospitals in Kingdom of Saudi Arabia. 2) evaluation of
TIDM development in children of 1 – 4 years of age.
Intervention schedule:
Work to be accomplished
Year 1
Quarters
Year 2
Quarters
Year 3
Quarters
Q1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q 4 Q 1 Q 2 Q 3 Q 4
Ethics clearance X
Project set-up X
Develop intervention X
Develop study instruments X
Enrolment of study subjects
and data collection X X
Implementation of
intervention X X X X X X X
Evaluation X X X X X X X
Data entry & cleaning X X X X X X X
Data analysis of trial X X X X X X X
Preparation of report and
scientific papers
X X
Population recruitment:
This cohort study can also be considered as population-based study. Longitudinal assessment
of exposure-outcome relationship can be evaluated population based cohort studies.
Advantages of these studies include : estimation of distribution and prevalence rate of
particular variable and elimination of bias (Shen, 2017). In this study, 100 women will be
recruited as study subjects and in control group 70 women will be recruited. Data related
vitamin D deficiency will be collected from women in the study subjects from 5 hospitals in
Kingdom of Saudi Arabia. Women with vitamin D supplementation will be incorporated in
the study subject group. Data related to pregnant women will be collected since previous 4
years because development of T1DM will be evaluated in the children of 1 – 4 years of age.
5
Women in the subject group and control group will be between 20 – 35 years of age. In the
second phase of the study, 100 children will be selected for the evaluation of development of
T1DM. Selected children for assessment of T1DM will be between 1 – 4 years of age.
Selected 100 children will be again separated into boys and girls.
Ethical consideration:
Ethical approval is necessary for human based studies and it will be taken from the institute
ethical committee. Approval for collection of vitamin D deficiency data will be taken from
the dean of selected hospitals. Approval will also be taken from dean of each hospital for data
collection for women with vitamin D deficiency. Selected women will be asked to give
written informed consent. Confidentiality will be maintained for identity of the women.
Children and their parents will be asked to give written informed consent for assessment of
T1DM. Children will be allowed to withdraw from the study at their will and such provision
will be made at the initiation of the study.
Measurement of outcomes:
Data related to vitamin D levels from the hospital will be collected as 25OHD levels. 24 – 28
weeks of gestation will be selected as period for the collection of 25OHD levels data in the
recruited pregnant women. Data related to vitamin D supplementation will be categorised
with respect to dose, frequency and duration of vitamin D supplementation. Data related to
development of T1DM in children will be collected by evaluating blood levels of HbA1c in
selected children. HbA1c blood levels will be evaluated and processed using validated
methods. Collected blood samples from the children will be processed immediately after
collection. HbA1c levels with 6.5 % will be considered as the normal levels. HbA1c levels
will be evaluated on regular basis with interval of 3 months for upto 1 year. Estimation of
HbA1c will be performed by using standardised method. This method include analysis using
high-performance liquid chromatography; auto A1c HA 8140 analyzer. Prior to use of this
method for HbA1c analysis, this method will be validated at our research centre (Bennett et
a., 2013).
Since, HbA1c estimation give accumulated glucose levels, it is not required to estimate
HbA1c levels frequently. In addition to the estimation of HbA1c level, fasting and fed
conditions glucose levels will be estimated. Glucose strips will be used for the estimation of
glucose levels. Pin-prick blood sampling will be used for the estimation of glucose levels
(Mukherjee, 2013).
6
second phase of the study, 100 children will be selected for the evaluation of development of
T1DM. Selected children for assessment of T1DM will be between 1 – 4 years of age.
Selected 100 children will be again separated into boys and girls.
Ethical consideration:
Ethical approval is necessary for human based studies and it will be taken from the institute
ethical committee. Approval for collection of vitamin D deficiency data will be taken from
the dean of selected hospitals. Approval will also be taken from dean of each hospital for data
collection for women with vitamin D deficiency. Selected women will be asked to give
written informed consent. Confidentiality will be maintained for identity of the women.
Children and their parents will be asked to give written informed consent for assessment of
T1DM. Children will be allowed to withdraw from the study at their will and such provision
will be made at the initiation of the study.
Measurement of outcomes:
Data related to vitamin D levels from the hospital will be collected as 25OHD levels. 24 – 28
weeks of gestation will be selected as period for the collection of 25OHD levels data in the
recruited pregnant women. Data related to vitamin D supplementation will be categorised
with respect to dose, frequency and duration of vitamin D supplementation. Data related to
development of T1DM in children will be collected by evaluating blood levels of HbA1c in
selected children. HbA1c blood levels will be evaluated and processed using validated
methods. Collected blood samples from the children will be processed immediately after
collection. HbA1c levels with 6.5 % will be considered as the normal levels. HbA1c levels
will be evaluated on regular basis with interval of 3 months for upto 1 year. Estimation of
HbA1c will be performed by using standardised method. This method include analysis using
high-performance liquid chromatography; auto A1c HA 8140 analyzer. Prior to use of this
method for HbA1c analysis, this method will be validated at our research centre (Bennett et
a., 2013).
Since, HbA1c estimation give accumulated glucose levels, it is not required to estimate
HbA1c levels frequently. In addition to the estimation of HbA1c level, fasting and fed
conditions glucose levels will be estimated. Glucose strips will be used for the estimation of
glucose levels. Pin-prick blood sampling will be used for the estimation of glucose levels
(Mukherjee, 2013).
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Biological estimations are prone to variability; hence there might be variations in estimation
of HbA1c and glucose levels. Hence, for estimation of HbA1c and glucose levels average of
three readings will be taken.
Analysis:
Effective analysis and interpretation of data will be achieved by arranging data in both tabular
and graphical format. Collected data will be entered in the excel sheet. Collected data will be
segregated into respective groups such as study subjects and control participants and male
and female children. Data will also be segregated with respect to different time points. Mean
and standard deviation will be calculated separately for different groups. Statistical analysis
will be performed for each group separately. Statistical data will be presented along with the
respective data. This type of the presentation of the data will be helpful in improving clarity
of the data and variation can be effectively assessed.
Statistical analysis:
100 women in the study subject group and 70 women in the control group will be optimum
for power calculation and statistical analysis. Mean difference in 25OHD in mol/L between
study subject group and control will be estimated. This analysis will be helpful in assessing
vitamin deficiency. Mean difference in HbAC1 level and glucose level will be estimated
between intervention and control group. This analysis will aid assessment of vitamin
deficiency and vitamin supplementation on the occurrence of T1DM. SPSS statistical
software package version 18.0 (SPSS Inc., Chicago, IL, USA) will be used for statistical
analysis. Comparisons among different groups will be carried out by using t test and one-way
repeated measures ANOVA whichever is appropriate. Tukey test will be used for post hoc
comparisons. Correlations among different variables will be established using Pearson’s
coefficients for correlations (Petrie, 2009).
Analytic strategy to evaluate impact:
Glucose estimation can be performed by self-monitoring of glucose. Probability of biasness is
high in self-monitoring of glucose. Hence, blood glucose determination in children will not
be performed by their parents; rather will be performed by healthcare professional.
7
of HbA1c and glucose levels. Hence, for estimation of HbA1c and glucose levels average of
three readings will be taken.
Analysis:
Effective analysis and interpretation of data will be achieved by arranging data in both tabular
and graphical format. Collected data will be entered in the excel sheet. Collected data will be
segregated into respective groups such as study subjects and control participants and male
and female children. Data will also be segregated with respect to different time points. Mean
and standard deviation will be calculated separately for different groups. Statistical analysis
will be performed for each group separately. Statistical data will be presented along with the
respective data. This type of the presentation of the data will be helpful in improving clarity
of the data and variation can be effectively assessed.
Statistical analysis:
100 women in the study subject group and 70 women in the control group will be optimum
for power calculation and statistical analysis. Mean difference in 25OHD in mol/L between
study subject group and control will be estimated. This analysis will be helpful in assessing
vitamin deficiency. Mean difference in HbAC1 level and glucose level will be estimated
between intervention and control group. This analysis will aid assessment of vitamin
deficiency and vitamin supplementation on the occurrence of T1DM. SPSS statistical
software package version 18.0 (SPSS Inc., Chicago, IL, USA) will be used for statistical
analysis. Comparisons among different groups will be carried out by using t test and one-way
repeated measures ANOVA whichever is appropriate. Tukey test will be used for post hoc
comparisons. Correlations among different variables will be established using Pearson’s
coefficients for correlations (Petrie, 2009).
Analytic strategy to evaluate impact:
Glucose estimation can be performed by self-monitoring of glucose. Probability of biasness is
high in self-monitoring of glucose. Hence, blood glucose determination in children will not
be performed by their parents; rather will be performed by healthcare professional.
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Information related to HbA1c and glucose levels might influence food consumption and
lifestyle habits. Alteration in the food consumption and lifestyle can influence HbA1c and
glucose levels estimations (Sanghani et al., 2013). Biasness in the data collection will be
avoided by not displaying the data to the children and their parents.
It is evident that environmental and behavioural factors have significant impact on 25OHD
levels in the pregnant women (Christesen et al., 2012). However, these factors will be
considered while selecting pregnant women for incorporating in the study. If this data is not
available with the hospitals; these women will be excluded from the study. It has been well
established that 25OHD levels remains stable without influence of environmental and
behavioural aspects. 25OHD should pass through placental barrier to enter foetus; hence,
cord concentration of 25OHD will be considered for the selection of pregnant with vitamin D
deficiency (Brannon and Picciano, 2011). It is highly possible that, pregnant women with
optimum levels of 25OHD, can supply reduced levels of 25OHD to their foetus. Such women
will also be included in the study subjects group. Women from different hospitals will be
selected. In such scenario, women in the different hospitals might have been administered
with vitamin D with different brands. Different brands of vitamin D can produce different
levels of efficacy for maintaining optimum levels of vitamin D. This variable efficiency of
vitamin D might produce different effect of occurrence of T1DM in children. This varied
effect of vitamin D can lead to variability in the outcome of the study. This variability will be
reduced by normalising vitamin D supplements data. It will be helpful in getting robust
outcome of the study. It will be achieved by analysis and interpreting data separately for
different hospitals. It will be helpful in accurate estimation of the vitamin D supplementation
on T1DM occurrence.
In cohort study design, confounding factors can be responsible to disturb exposure and
outcome relationship (Bookwala et al., 2011). While selecting children for the assessment of
occurrence of T1DM, factors like anti-diabetic medication and insulin will be considered.
Glucose and HbA1c levels in the children can be significantly affected by administration of
anti-diabetic medication and insulin (Seung-Hyun et al., 2016). Hence, children consuming
anti-diabetic medications and insulin will be excluded because these children might have
demonstrated reduced levels of glucose and HbA1c. For eliminating this cofounding factor,
data related to consumption of medications will be collected for the selected children. After
collecting data for medication consumption, data will be again reanalysed and will be
incorporated in the original data. T1DM is a complex disease and it can be associated with
8
lifestyle habits. Alteration in the food consumption and lifestyle can influence HbA1c and
glucose levels estimations (Sanghani et al., 2013). Biasness in the data collection will be
avoided by not displaying the data to the children and their parents.
It is evident that environmental and behavioural factors have significant impact on 25OHD
levels in the pregnant women (Christesen et al., 2012). However, these factors will be
considered while selecting pregnant women for incorporating in the study. If this data is not
available with the hospitals; these women will be excluded from the study. It has been well
established that 25OHD levels remains stable without influence of environmental and
behavioural aspects. 25OHD should pass through placental barrier to enter foetus; hence,
cord concentration of 25OHD will be considered for the selection of pregnant with vitamin D
deficiency (Brannon and Picciano, 2011). It is highly possible that, pregnant women with
optimum levels of 25OHD, can supply reduced levels of 25OHD to their foetus. Such women
will also be included in the study subjects group. Women from different hospitals will be
selected. In such scenario, women in the different hospitals might have been administered
with vitamin D with different brands. Different brands of vitamin D can produce different
levels of efficacy for maintaining optimum levels of vitamin D. This variable efficiency of
vitamin D might produce different effect of occurrence of T1DM in children. This varied
effect of vitamin D can lead to variability in the outcome of the study. This variability will be
reduced by normalising vitamin D supplements data. It will be helpful in getting robust
outcome of the study. It will be achieved by analysis and interpreting data separately for
different hospitals. It will be helpful in accurate estimation of the vitamin D supplementation
on T1DM occurrence.
In cohort study design, confounding factors can be responsible to disturb exposure and
outcome relationship (Bookwala et al., 2011). While selecting children for the assessment of
occurrence of T1DM, factors like anti-diabetic medication and insulin will be considered.
Glucose and HbA1c levels in the children can be significantly affected by administration of
anti-diabetic medication and insulin (Seung-Hyun et al., 2016). Hence, children consuming
anti-diabetic medications and insulin will be excluded because these children might have
demonstrated reduced levels of glucose and HbA1c. For eliminating this cofounding factor,
data related to consumption of medications will be collected for the selected children. After
collecting data for medication consumption, data will be again reanalysed and will be
incorporated in the original data. T1DM is a complex disease and it can be associated with
8
the other metabolic disorders. It can lead to altered levels of glucose. Hence, this factor will
also be considered while analysing and interpreting data (Chillarón et l., 2014). Information
about occurrence of other metabolic disease will be collected from the parents. In case of
increased levels of glucose and HbA1c in children with other metabolic diseases, these results
will be excluded from the study. Exercise and eating habits can also affect significantly
glucose levels. Hence, these factors will be considered while analysing and interpreting the
data. Severity of T1DM in children will be assessed by observing polyuria, polydipsia, and
polyphagia in the children (Kharroubi and Darwish, 2015).
Prior to execution of the study, this protocol will be discussed with other healthcare
professionals. People with different experience and expertise can have different opinions on
the same subject. Hence, questions might be raised during presentation to these healthcare
professionals. These questions will be considered and will be incorporated in the protocol.
Anticipated outcomes of study:
It is evident form the literature that there is existence of confounding relationship between
vitamin D deficiency and T1DM. However, insulin sensitivity can be significantly improved
and effective glycaemic control in T2DM patients by vitamin D supplementation (Chih-
Chien et al., 2012). However, there is scarcity of evidence for improvement in T1DM
condition after supplementation with vitamin D (Svoren et al., 2009). This study will play
significant role for validation of vitamin D deficiency for the development of T1DM in
children. This study can be useful in validating role of vitamin D deficiency on HbA1c levels
on children. It will also be establish role of vitamin D supplements in pregnant women on the
development of T1DM in their respective children.
This study will establish difference in glucose and HbA1c levels between the children in the
control group and T1DM group. Studies established that little variation exists between the
women in vitamin D deficient and non-deficient group for the development of T1DM. It will
be interesting to explore whether mother’s trend of T1DM will be translated in their children.
Effect of other factors like socioeconomic factors on the occurrence of T1DM will be
established in this study. From, the literature it is evident that occurrence of T1DM is more
prevalent in low socioeconomic class children as compared to the children of high
socioeconomic class children. This difference might be due to less knowledge and awareness
of T1DM among low socioeconomic class people. This study will also establish difference
between male and female children on the occurrence of T1DM.
9
also be considered while analysing and interpreting data (Chillarón et l., 2014). Information
about occurrence of other metabolic disease will be collected from the parents. In case of
increased levels of glucose and HbA1c in children with other metabolic diseases, these results
will be excluded from the study. Exercise and eating habits can also affect significantly
glucose levels. Hence, these factors will be considered while analysing and interpreting the
data. Severity of T1DM in children will be assessed by observing polyuria, polydipsia, and
polyphagia in the children (Kharroubi and Darwish, 2015).
Prior to execution of the study, this protocol will be discussed with other healthcare
professionals. People with different experience and expertise can have different opinions on
the same subject. Hence, questions might be raised during presentation to these healthcare
professionals. These questions will be considered and will be incorporated in the protocol.
Anticipated outcomes of study:
It is evident form the literature that there is existence of confounding relationship between
vitamin D deficiency and T1DM. However, insulin sensitivity can be significantly improved
and effective glycaemic control in T2DM patients by vitamin D supplementation (Chih-
Chien et al., 2012). However, there is scarcity of evidence for improvement in T1DM
condition after supplementation with vitamin D (Svoren et al., 2009). This study will play
significant role for validation of vitamin D deficiency for the development of T1DM in
children. This study can be useful in validating role of vitamin D deficiency on HbA1c levels
on children. It will also be establish role of vitamin D supplements in pregnant women on the
development of T1DM in their respective children.
This study will establish difference in glucose and HbA1c levels between the children in the
control group and T1DM group. Studies established that little variation exists between the
women in vitamin D deficient and non-deficient group for the development of T1DM. It will
be interesting to explore whether mother’s trend of T1DM will be translated in their children.
Effect of other factors like socioeconomic factors on the occurrence of T1DM will be
established in this study. From, the literature it is evident that occurrence of T1DM is more
prevalent in low socioeconomic class children as compared to the children of high
socioeconomic class children. This difference might be due to less knowledge and awareness
of T1DM among low socioeconomic class people. This study will also establish difference
between male and female children on the occurrence of T1DM.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

This study will be helpful in identifying exact gestation period in which supplementation of
vitamin D can be helpful in exhibiting long duration effect in the children. Outcome if this
study will be helpful in supporting the concept that estimation of vitamin D during whole
gestation period in essential because it can impact pregnant women and children throughout
their life. Dose of vitamin D and brand of vitamin D supplement will also be validated in this
study because data of different brands will be analysed separately. Effect of age of pregnant
women on vitamin D deficiency and women’s response to vitamin D supplementation will be
evaluated in this study. In this study, women in the broad range from 20 – 35 years will be
recruited.
10
vitamin D can be helpful in exhibiting long duration effect in the children. Outcome if this
study will be helpful in supporting the concept that estimation of vitamin D during whole
gestation period in essential because it can impact pregnant women and children throughout
their life. Dose of vitamin D and brand of vitamin D supplement will also be validated in this
study because data of different brands will be analysed separately. Effect of age of pregnant
women on vitamin D deficiency and women’s response to vitamin D supplementation will be
evaluated in this study. In this study, women in the broad range from 20 – 35 years will be
recruited.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
References:
Alvarez, J.A., and Ashraf, A. (2010). Role of vitamin D in insulin secretion and insulin
sensitivity for glucose homeostasis. International Journal of Endocrinology,
351385. doi: 10.1155/2010/351385.
Bennett, S.E., McPeake, J., McCance, D.R., Manderson, J.G., Johnston, P., McGalliard,
R., McGinty, A. (2013). Maternal vitamin D status in type 1 diabetic pregnancy:
impact on neonatal vitamin D status and association with maternal glycaemic
control. PLoS One, 8(9), e74068. doi: 10.1371/journal.pone.0074068.
Brannon, P.M., and Picciano, M.F. (2011). Vitamin D in pregnancy and lactation in
humans. Annual Review of Nutrition, 31, 89–115.
Bookwala, A., Hussain, N., and Bhandari, M. (2011). The three-minute appraisal of a
prospective cohort study. Indian Journal of Orthopaedics, 45(4), 291–293.
Christesen, H.T., Falkenberg, T., Lamont, R.F., and Jorgensen, J.S. (2012). The impact of
vitamin D on pregnancy: a systematic review. Acta Obstetricia et Gynecologica
Scandinavica, 12, 1357–1367.
Chillarón, J.J., Flores Le-Roux, J.A., Benaiges, D., and Pedro-Botet, J. (2014). Type 1
diabetes, metabolic syndrome and cardiovascular risk. Metabolism, 63(2), 181-7.
Chih-Chien, S., Min-Tser, L., Kuo-Cheng, L., and Chia-Chao, W. (2012). Role of
Vitamin D in Insulin Resistance. Journal of Biomedicine and Biotechnology,
634195. doi: 10.1155/2012/634195.
Ginde, A.A., Sullivan, A.F., Mansbach, J.M., and Camargo, C.A. (2010). Vitamin D
insufficiency in pregnant and nonpregnant women of childbearing age in the
United States. American Journal of Obstetrics & Gynecology, 202, 1–8.
Hossein-Nezhad, A., Maghbooli, Z., Vassigh, A.R, Larijani, B. (2007). Prevalence of
gestational diabetes mellitus and pregnancy outcomes in Iranian
women. Taiwanese Journal of Obstetrics and Gynecology, 46, 236–241.
Holick, M. (2007). Vitamin D deficiency. New England Journal of Medicine, 357, 266–
281.
Kharroubi, A.T., and Darwish, H. M. (2015). Diabetes mellitus: The epidemic of the
century. World Journal of Diabetes, 6(6), 850–867.
Kung, A.W. (2007). Iodine nutrition of pregnant and lactating women in Hong Kong,
where intake is of borderline sufficiency. Public Health Nutrition, 10(12A), 1600-
1.
Mukherjee, K. L. (2013). Medical Laboratory Technology. Tata McGraw-Hill Education.
Petrie, A., and Sabin, C. (2009). Medical Statistics at a Glance. John Wiley & Sons.
Soheilykhah, S., Mojibian, M., Rashidi, M., Rahimi-Saghand, S., Jafari, F. (2010).
Maternal vitamin D status in gestational diabetes mellitus. Nutrition in Clinical
Practice, 25, 524–52.
11
Alvarez, J.A., and Ashraf, A. (2010). Role of vitamin D in insulin secretion and insulin
sensitivity for glucose homeostasis. International Journal of Endocrinology,
351385. doi: 10.1155/2010/351385.
Bennett, S.E., McPeake, J., McCance, D.R., Manderson, J.G., Johnston, P., McGalliard,
R., McGinty, A. (2013). Maternal vitamin D status in type 1 diabetic pregnancy:
impact on neonatal vitamin D status and association with maternal glycaemic
control. PLoS One, 8(9), e74068. doi: 10.1371/journal.pone.0074068.
Brannon, P.M., and Picciano, M.F. (2011). Vitamin D in pregnancy and lactation in
humans. Annual Review of Nutrition, 31, 89–115.
Bookwala, A., Hussain, N., and Bhandari, M. (2011). The three-minute appraisal of a
prospective cohort study. Indian Journal of Orthopaedics, 45(4), 291–293.
Christesen, H.T., Falkenberg, T., Lamont, R.F., and Jorgensen, J.S. (2012). The impact of
vitamin D on pregnancy: a systematic review. Acta Obstetricia et Gynecologica
Scandinavica, 12, 1357–1367.
Chillarón, J.J., Flores Le-Roux, J.A., Benaiges, D., and Pedro-Botet, J. (2014). Type 1
diabetes, metabolic syndrome and cardiovascular risk. Metabolism, 63(2), 181-7.
Chih-Chien, S., Min-Tser, L., Kuo-Cheng, L., and Chia-Chao, W. (2012). Role of
Vitamin D in Insulin Resistance. Journal of Biomedicine and Biotechnology,
634195. doi: 10.1155/2012/634195.
Ginde, A.A., Sullivan, A.F., Mansbach, J.M., and Camargo, C.A. (2010). Vitamin D
insufficiency in pregnant and nonpregnant women of childbearing age in the
United States. American Journal of Obstetrics & Gynecology, 202, 1–8.
Hossein-Nezhad, A., Maghbooli, Z., Vassigh, A.R, Larijani, B. (2007). Prevalence of
gestational diabetes mellitus and pregnancy outcomes in Iranian
women. Taiwanese Journal of Obstetrics and Gynecology, 46, 236–241.
Holick, M. (2007). Vitamin D deficiency. New England Journal of Medicine, 357, 266–
281.
Kharroubi, A.T., and Darwish, H. M. (2015). Diabetes mellitus: The epidemic of the
century. World Journal of Diabetes, 6(6), 850–867.
Kung, A.W. (2007). Iodine nutrition of pregnant and lactating women in Hong Kong,
where intake is of borderline sufficiency. Public Health Nutrition, 10(12A), 1600-
1.
Mukherjee, K. L. (2013). Medical Laboratory Technology. Tata McGraw-Hill Education.
Petrie, A., and Sabin, C. (2009). Medical Statistics at a Glance. John Wiley & Sons.
Soheilykhah, S., Mojibian, M., Rashidi, M., Rahimi-Saghand, S., Jafari, F. (2010).
Maternal vitamin D status in gestational diabetes mellitus. Nutrition in Clinical
Practice, 25, 524–52.
11
Stephen, B. H., Steven, R. C., Warren S. B., Deborah G. G., Thomas B. N. (2013).
Designing Clinical Research. Lippincott Williams & Wilkins.
Shen, B. (2017). Translational Informatics in Smart Healthcare. Springer.
Sanghani, N. B., Parchwani, D. N., Palandurkar, K. M., Shah, A. M., and Dhanani, J. V.
(2013). Impact of lifestyle modification on glycemic control in patients with type
2 diabetes mellitus. Indian Journal of Endocrinology and Metabolism, 17(6),
1030–1039.
Seung-Hyun, K., Dae-Jung, K., Jong-Heon, P., Kee-Ho, S., Kyungdo, H., Ki-Up, L., and
Kyung-Soo, K. (2016). Trends of antidiabetic drug use in adult type 2 diabetes in
Korea in 2002–2013: Nationwide population-based cohort study. Medicine,
95(27), e4018. doi: 10.1097/MD.0000000000004018.
Svoren, B. M., Volkening, L. K., Wood, J. R., Laffel, M.B. (2009). Significant Vitamin D
Deficiency in Youth with Type 1 Diabetes. Journal of Pediatrics, 154(1), 132–
134.
12
Designing Clinical Research. Lippincott Williams & Wilkins.
Shen, B. (2017). Translational Informatics in Smart Healthcare. Springer.
Sanghani, N. B., Parchwani, D. N., Palandurkar, K. M., Shah, A. M., and Dhanani, J. V.
(2013). Impact of lifestyle modification on glycemic control in patients with type
2 diabetes mellitus. Indian Journal of Endocrinology and Metabolism, 17(6),
1030–1039.
Seung-Hyun, K., Dae-Jung, K., Jong-Heon, P., Kee-Ho, S., Kyungdo, H., Ki-Up, L., and
Kyung-Soo, K. (2016). Trends of antidiabetic drug use in adult type 2 diabetes in
Korea in 2002–2013: Nationwide population-based cohort study. Medicine,
95(27), e4018. doi: 10.1097/MD.0000000000004018.
Svoren, B. M., Volkening, L. K., Wood, J. R., Laffel, M.B. (2009). Significant Vitamin D
Deficiency in Youth with Type 1 Diabetes. Journal of Pediatrics, 154(1), 132–
134.
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.