Chronic Kidney Disease and Diabetic Nephropathy
VerifiedAdded on 2023/01/19
|10
|1365
|80
AI Summary
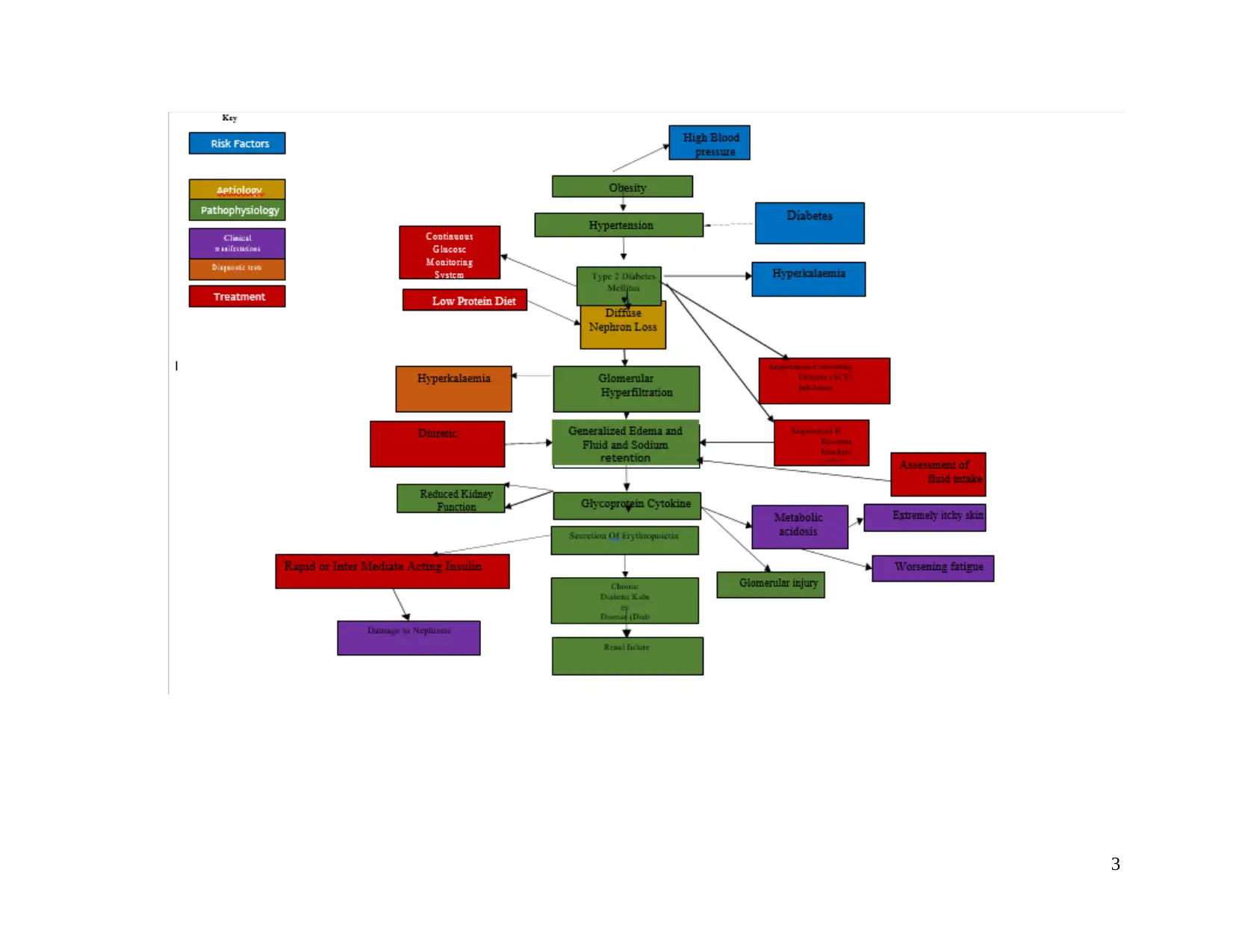
This document discusses the causes, risk factors, and treatment options for chronic kidney disease (CKD) and diabetic nephropathy. It explains how obesity, hypertension, and diabetes contribute to the development of CKD and the impact of hyperkalemia and metabolic acidosis on kidney function. The document also explores pharmacological and non-pharmacological treatment options for managing CKD and diabetic nephropathy. References to relevant books and journals are provided for further reading.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.




1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.