Analyzing Global Health Policies for Cardiovascular Disease Prevention
VerifiedAdded on 2023/04/26
|13
|4613
|247
Essay
AI Summary
This essay provides an overview of cardiovascular disease (CVD), highlighting its significant impact on global public health as a leading cause of death worldwide. It discusses the morbidity, mortality, and epidemiology of CVD, referencing data from the World Health Organization (WHO) and other sources. The essay outlines various types of CVD, including coronary heart disease, strokes and TIAs, peripheral arterial disease, and aortic disease. Furthermore, it examines national and international policy documents and initiatives aimed at preventing CVD, such as the Singapore Declaration, Victoria Declaration, and the Global Hearts Initiative. The roles of organizations like WHO, US CDC, NICE, and SACN are discussed in the context of formulating guidelines and policies for CVD prevention, focusing on strategies like tobacco control, promotion of physical activity, salt reduction, and healthcare management. The essay also highlights specific initiatives in England/UK, including government policies on nutrition, obesity, and tobacco control, emphasizing the importance of a multi-faceted approach to tackling CVD risk factors.
Running Head: Public Health
Introduction
This essay is covers the Cardiovascular disease and the different national and international
programs and policy documents that helps in prevent this dangerous disease. CVD is a major
problem in public health that is used to describe a wide range of problem in hearts. This
disease occurs, when heart is not pumping because of blockage in blood vessel. This disease
can also be linked with the mutilation to blood vessel in organs, such as the heart, brain, eyes,
and kidneys etc. Narrowing and blocking of the blood vessels is a common form of heart
disease (Estruch, et.al, 2013).
Cardiovascular Diseases (Morbidity, Mortality, and Epidemiology)
Cardiovascular disease also known as its second name called heart disease and it is one of the
primary causes of death in both men and women all over the world but especially in the USA
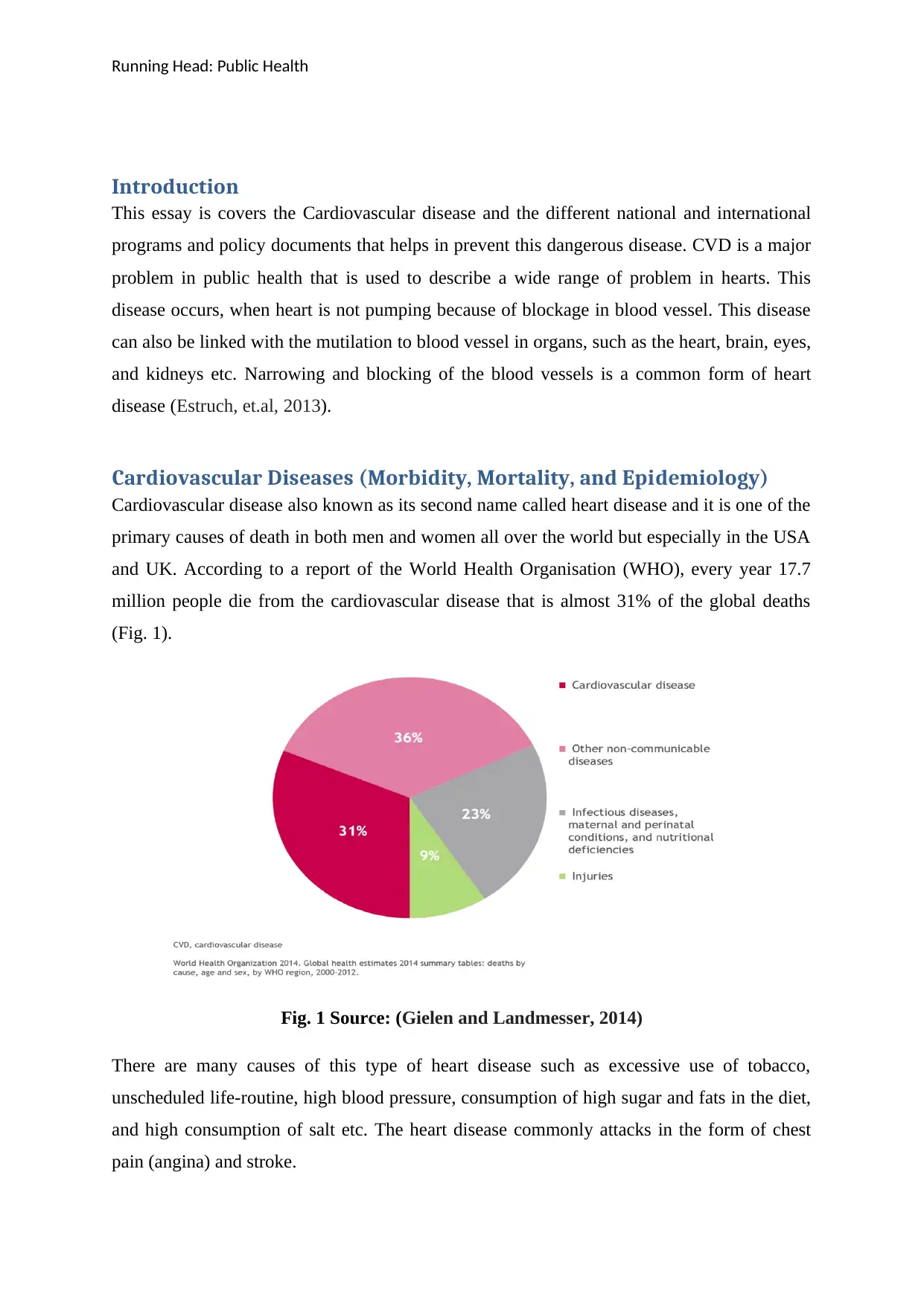
and UK. According to a report of the World Health Organisation (WHO), every year 17.7
million people die from the cardiovascular disease that is almost 31% of the global deaths
(Fig. 1).
Fig. 1 Source: (Gielen and Landmesser, 2014)
There are many causes of this type of heart disease such as excessive use of tobacco,
unscheduled life-routine, high blood pressure, consumption of high sugar and fats in the diet,
and high consumption of salt etc. The heart disease commonly attacks in the form of chest
pain (angina) and stroke.
Introduction
This essay is covers the Cardiovascular disease and the different national and international
programs and policy documents that helps in prevent this dangerous disease. CVD is a major
problem in public health that is used to describe a wide range of problem in hearts. This
disease occurs, when heart is not pumping because of blockage in blood vessel. This disease
can also be linked with the mutilation to blood vessel in organs, such as the heart, brain, eyes,
and kidneys etc. Narrowing and blocking of the blood vessels is a common form of heart
disease (Estruch, et.al, 2013).
Cardiovascular Diseases (Morbidity, Mortality, and Epidemiology)
Cardiovascular disease also known as its second name called heart disease and it is one of the
primary causes of death in both men and women all over the world but especially in the USA
and UK. According to a report of the World Health Organisation (WHO), every year 17.7
million people die from the cardiovascular disease that is almost 31% of the global deaths
(Fig. 1).
Fig. 1 Source: (Gielen and Landmesser, 2014)
There are many causes of this type of heart disease such as excessive use of tobacco,
unscheduled life-routine, high blood pressure, consumption of high sugar and fats in the diet,
and high consumption of salt etc. The heart disease commonly attacks in the form of chest
pain (angina) and stroke.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Public Health
1
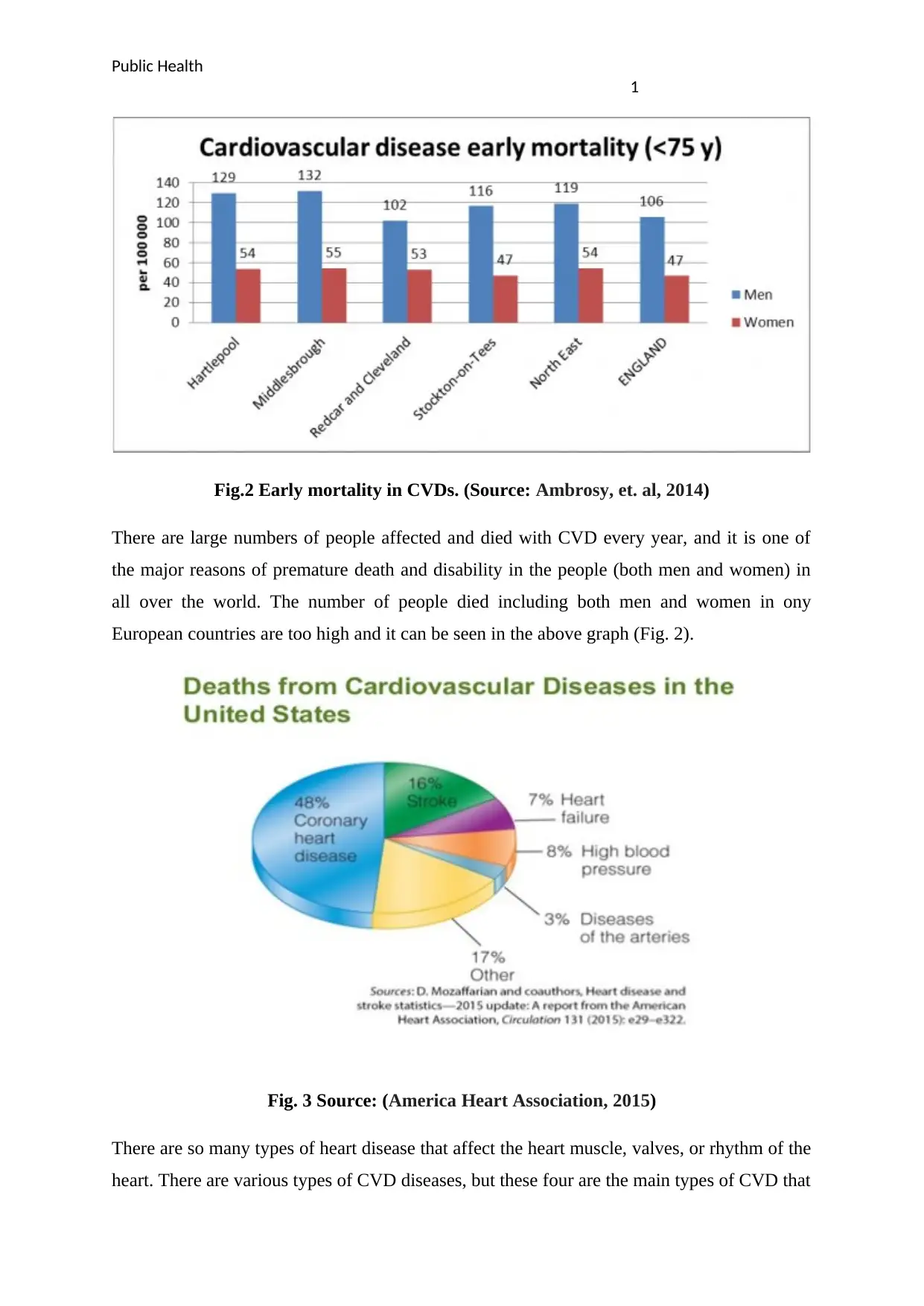
Fig.2 Early mortality in CVDs. (Source: Ambrosy, et. al, 2014)
There are large numbers of people affected and died with CVD every year, and it is one of
the major reasons of premature death and disability in the people (both men and women) in
all over the world. The number of people died including both men and women in ony
European countries are too high and it can be seen in the above graph (Fig. 2).
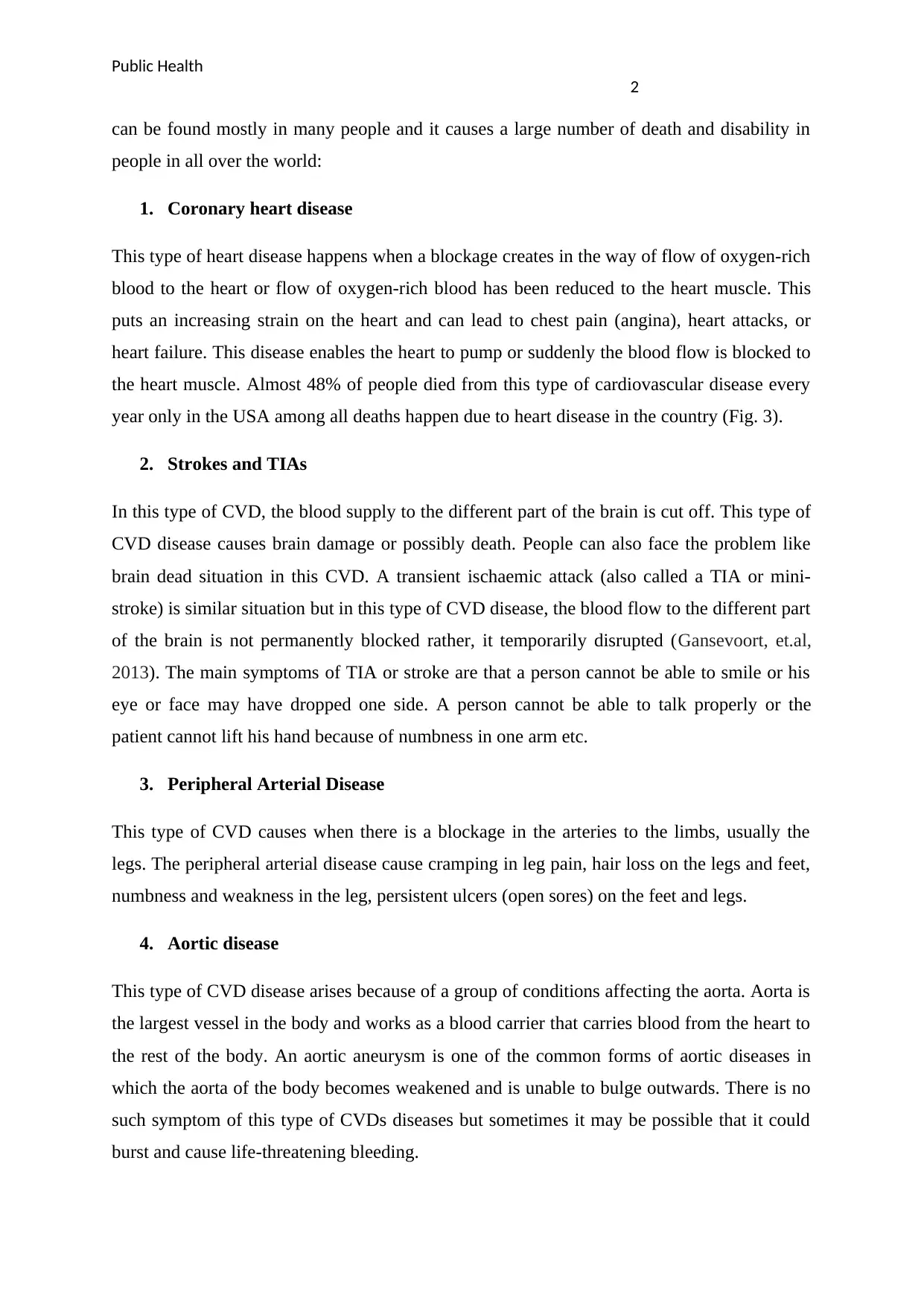
Fig. 3 Source: (America Heart Association, 2015)
There are so many types of heart disease that affect the heart muscle, valves, or rhythm of the
heart. There are various types of CVD diseases, but these four are the main types of CVD that
1
Fig.2 Early mortality in CVDs. (Source: Ambrosy, et. al, 2014)
There are large numbers of people affected and died with CVD every year, and it is one of
the major reasons of premature death and disability in the people (both men and women) in
all over the world. The number of people died including both men and women in ony
European countries are too high and it can be seen in the above graph (Fig. 2).
Fig. 3 Source: (America Heart Association, 2015)
There are so many types of heart disease that affect the heart muscle, valves, or rhythm of the
heart. There are various types of CVD diseases, but these four are the main types of CVD that
Public Health
2
can be found mostly in many people and it causes a large number of death and disability in
people in all over the world:
1. Coronary heart disease
This type of heart disease happens when a blockage creates in the way of flow of oxygen-rich
blood to the heart or flow of oxygen-rich blood has been reduced to the heart muscle. This
puts an increasing strain on the heart and can lead to chest pain (angina), heart attacks, or
heart failure. This disease enables the heart to pump or suddenly the blood flow is blocked to
the heart muscle. Almost 48% of people died from this type of cardiovascular disease every
year only in the USA among all deaths happen due to heart disease in the country (Fig. 3).
2. Strokes and TIAs
In this type of CVD, the blood supply to the different part of the brain is cut off. This type of
CVD disease causes brain damage or possibly death. People can also face the problem like
brain dead situation in this CVD. A transient ischaemic attack (also called a TIA or mini-
stroke) is similar situation but in this type of CVD disease, the blood flow to the different part
of the brain is not permanently blocked rather, it temporarily disrupted (Gansevoort, et.al,
2013). The main symptoms of TIA or stroke are that a person cannot be able to smile or his
eye or face may have dropped one side. A person cannot be able to talk properly or the
patient cannot lift his hand because of numbness in one arm etc.
3. Peripheral Arterial Disease
This type of CVD causes when there is a blockage in the arteries to the limbs, usually the
legs. The peripheral arterial disease cause cramping in leg pain, hair loss on the legs and feet,
numbness and weakness in the leg, persistent ulcers (open sores) on the feet and legs.
4. Aortic disease
This type of CVD disease arises because of a group of conditions affecting the aorta. Aorta is
the largest vessel in the body and works as a blood carrier that carries blood from the heart to
the rest of the body. An aortic aneurysm is one of the common forms of aortic diseases in
which the aorta of the body becomes weakened and is unable to bulge outwards. There is no
such symptom of this type of CVDs diseases but sometimes it may be possible that it could
burst and cause life-threatening bleeding.
2
can be found mostly in many people and it causes a large number of death and disability in
people in all over the world:
1. Coronary heart disease
This type of heart disease happens when a blockage creates in the way of flow of oxygen-rich
blood to the heart or flow of oxygen-rich blood has been reduced to the heart muscle. This
puts an increasing strain on the heart and can lead to chest pain (angina), heart attacks, or
heart failure. This disease enables the heart to pump or suddenly the blood flow is blocked to
the heart muscle. Almost 48% of people died from this type of cardiovascular disease every
year only in the USA among all deaths happen due to heart disease in the country (Fig. 3).
2. Strokes and TIAs
In this type of CVD, the blood supply to the different part of the brain is cut off. This type of
CVD disease causes brain damage or possibly death. People can also face the problem like
brain dead situation in this CVD. A transient ischaemic attack (also called a TIA or mini-
stroke) is similar situation but in this type of CVD disease, the blood flow to the different part
of the brain is not permanently blocked rather, it temporarily disrupted (Gansevoort, et.al,
2013). The main symptoms of TIA or stroke are that a person cannot be able to smile or his
eye or face may have dropped one side. A person cannot be able to talk properly or the
patient cannot lift his hand because of numbness in one arm etc.
3. Peripheral Arterial Disease
This type of CVD causes when there is a blockage in the arteries to the limbs, usually the
legs. The peripheral arterial disease cause cramping in leg pain, hair loss on the legs and feet,
numbness and weakness in the leg, persistent ulcers (open sores) on the feet and legs.
4. Aortic disease
This type of CVD disease arises because of a group of conditions affecting the aorta. Aorta is
the largest vessel in the body and works as a blood carrier that carries blood from the heart to
the rest of the body. An aortic aneurysm is one of the common forms of aortic diseases in
which the aorta of the body becomes weakened and is unable to bulge outwards. There is no
such symptom of this type of CVDs diseases but sometimes it may be possible that it could
burst and cause life-threatening bleeding.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Public Health
3
National and International Policy Documents to prevent the CVD
Many conventions and policies were formulated in past by numbers of national and
international health organisation to fight with CVD diseases. The principles for CVD
describe in numerous global heart related health conferences: Singapore declaration (1998),
Victoria declaration (1992), Osaka Declaration (2001), Luxemburg Declaration (2005),
European Health Charter (2006), Catalonia Declaration (1996), International principles for
national and regional guidelines on CVD prevention (2004) were some famous conference
held on Heart disease.
Cardiovascular disease is one of the main reasons of premature death and disabilities in
people in all over the world and it substantially escalating the cost of health care and
prevention cost globally. The serious case of coronary and cerebrovascular heart disease
frequently occur suddenly and are more dangerous and fatal before medical care can be
given. There are some international health organisations, such as World Health Organisation
(WHO), World Health Federation, and World Stroke Organisation are some international
organisation that makes policy guidelines that help and guide the world about the CVD
(Steptoe and Kivimäki, 2012). Although, some national and private non-government
organisations (NGOs) are also working to prevent this most dangerous disease among all and
try to make aware people about the different types of CVD and its effect to prevent it to
spread. Apart from these health organisations such as Centres for Disease Control and
Prevention (CDC) and the National Institute for Health (NIH) is also providing leadership to
prevent the CVDs and reduce the death rate, which happens because of heart disease. Apart
from this, in the UK, a health organisation that is working for formulating guidelines and
policies for preventing CVD disease is NICE (National Institute for Health and Care
Excellence).
In the global effort to reduce the death rate and disability because of CVD and for the
purpose of CVD prevention and control, The World Herat and Stroke Forum (WHSF),
suggest and recommends all the countries in the world to develop policy on prevention of
cardiovascular diseases. According to WHSF, the national policy regarding prevention of
CVD should be developed by organized and on a systematic basis and on a regular dialogue
among governmental, public health, and other private health professional groups. It is also
considered that the national policy related to CVD prevention should be set in such a way that
guide and control other public health and private health organisations that is appropriate to
3
National and International Policy Documents to prevent the CVD
Many conventions and policies were formulated in past by numbers of national and
international health organisation to fight with CVD diseases. The principles for CVD
describe in numerous global heart related health conferences: Singapore declaration (1998),
Victoria declaration (1992), Osaka Declaration (2001), Luxemburg Declaration (2005),
European Health Charter (2006), Catalonia Declaration (1996), International principles for
national and regional guidelines on CVD prevention (2004) were some famous conference
held on Heart disease.
Cardiovascular disease is one of the main reasons of premature death and disabilities in
people in all over the world and it substantially escalating the cost of health care and
prevention cost globally. The serious case of coronary and cerebrovascular heart disease
frequently occur suddenly and are more dangerous and fatal before medical care can be
given. There are some international health organisations, such as World Health Organisation
(WHO), World Health Federation, and World Stroke Organisation are some international
organisation that makes policy guidelines that help and guide the world about the CVD
(Steptoe and Kivimäki, 2012). Although, some national and private non-government
organisations (NGOs) are also working to prevent this most dangerous disease among all and
try to make aware people about the different types of CVD and its effect to prevent it to
spread. Apart from these health organisations such as Centres for Disease Control and
Prevention (CDC) and the National Institute for Health (NIH) is also providing leadership to
prevent the CVDs and reduce the death rate, which happens because of heart disease. Apart
from this, in the UK, a health organisation that is working for formulating guidelines and
policies for preventing CVD disease is NICE (National Institute for Health and Care
Excellence).
In the global effort to reduce the death rate and disability because of CVD and for the
purpose of CVD prevention and control, The World Herat and Stroke Forum (WHSF),
suggest and recommends all the countries in the world to develop policy on prevention of
cardiovascular diseases. According to WHSF, the national policy regarding prevention of
CVD should be developed by organized and on a systematic basis and on a regular dialogue
among governmental, public health, and other private health professional groups. It is also
considered that the national policy related to CVD prevention should be set in such a way that
guide and control other public health and private health organisations that is appropriate to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Public Health
4
the country (WHO, 2018). The national policy should set the priority, which serves as a
foundation for the development of national guidelines on prevention of cardiovascular
diseases.
The WHO is one of the largest health organisations in the world that is working in
collaboration with United States Centres for Disease (US CDC) to prevent the CVDs through
supporting different governments of different countries and strengthening them in prevention
and control mechanism to reduce the premature death rate, which happens due to CVDs.
They are specially focusing on the US and the UK, because a large number of people died
every year in these two countries from CVD, especially from coronary (WHO, 2018). In
2016, Both WHO and US CDC launched an initiative called ‘Global Hearts Initiative’ to
fight with CVDs. This initiative provides five technical packages that provide a set of high
impact, evidence-based intervention that when used together, will have a major impact on
improving global heart health.
CVD in England/UK and their Prevention Policy
There are more than 124000 people died each year in England because of CVDs. It means
340 people each day or one death every four minutes. Since the BHF was established in the
UK and England, the annual number of deaths has fallen by more than half. According to a
report, more than 5.9 million people are living with heart disease. Only Coronary heart
disease kills 150 people every day in England and more than 1.8 million people living with
Coronary heart disease (CHD) in England. In England and the UK, most of the people died
from CVDs are under the age of 75 years. Despite being recent prevention and control
initiatives, the death numbers in the UK and England is very high.
The WHO work in five packages that contain MPOWER, that is for controlling and
prevention of tobacco products, the ACTIVE package focus on physical activity among
people lie exercise and Yoga, the SHAKE package is focused on salt reduction in foods and
diet, REPLACE package focus on to reduce the industrial products that includes trans fats.
The last package is the HEARTS package that deals in strengthening healthcare management
in all over the world to reduce and prevent the CVDs in primary healthcare (WHO, 2018).
NICE plays an important role in preventing CVD in England by formulating specific
guidelines and prevention policy that is based on the population level. NICE has released
seven related guidance for people to prevent the CVD (Yusuf, et.al, 2015). These guidelines
are related to the prevention of harmful drinking to stop the drinking disorder, promoting
4
the country (WHO, 2018). The national policy should set the priority, which serves as a
foundation for the development of national guidelines on prevention of cardiovascular
diseases.
The WHO is one of the largest health organisations in the world that is working in
collaboration with United States Centres for Disease (US CDC) to prevent the CVDs through
supporting different governments of different countries and strengthening them in prevention
and control mechanism to reduce the premature death rate, which happens due to CVDs.
They are specially focusing on the US and the UK, because a large number of people died
every year in these two countries from CVD, especially from coronary (WHO, 2018). In
2016, Both WHO and US CDC launched an initiative called ‘Global Hearts Initiative’ to
fight with CVDs. This initiative provides five technical packages that provide a set of high
impact, evidence-based intervention that when used together, will have a major impact on
improving global heart health.
CVD in England/UK and their Prevention Policy
There are more than 124000 people died each year in England because of CVDs. It means
340 people each day or one death every four minutes. Since the BHF was established in the
UK and England, the annual number of deaths has fallen by more than half. According to a
report, more than 5.9 million people are living with heart disease. Only Coronary heart
disease kills 150 people every day in England and more than 1.8 million people living with
Coronary heart disease (CHD) in England. In England and the UK, most of the people died
from CVDs are under the age of 75 years. Despite being recent prevention and control
initiatives, the death numbers in the UK and England is very high.
The WHO work in five packages that contain MPOWER, that is for controlling and
prevention of tobacco products, the ACTIVE package focus on physical activity among
people lie exercise and Yoga, the SHAKE package is focused on salt reduction in foods and
diet, REPLACE package focus on to reduce the industrial products that includes trans fats.
The last package is the HEARTS package that deals in strengthening healthcare management
in all over the world to reduce and prevent the CVDs in primary healthcare (WHO, 2018).
NICE plays an important role in preventing CVD in England by formulating specific
guidelines and prevention policy that is based on the population level. NICE has released
seven related guidance for people to prevent the CVD (Yusuf, et.al, 2015). These guidelines
are related to the prevention of harmful drinking to stop the drinking disorder, promoting
Public Health
5
physical activity in both children and young people, primary and secondary prevention of
CVDs by cardiovascular risk assessment. NICE also focuses on the modification of blood
lipids, identifying people who are suffering from CVDs. Apart from this, NICE also provides
them appropriate medical care and tell them about the prevention control guidelines to them,
Smoking cessation services and engage the community to prevent the CVDs in England
(NICE, 2018).
The European Heart Charter (EHC) is another European health organisation that deals in
health promotion and formulates international strategies that help in the management and
detection of people at high CVD risk. The ECH is also responsible for the authorization of
the European Guidelines on Cardiovascular Disease Prevention at the country level.
Government Policy
Government policy also takes many initiatives to control the CVDs. The government is
almost taking all the corrective action and set priorities for action on nutrition, obesity and
tobacco control, and physical activities (Gylling, et.al, 2014). The government operates a
large number of an awareness program for delivering food, spread awareness among people
about the benefit of physical activities, and how prevention of tobacco and smoking can help
in cardiovascular disease control. The government publish large number of documents and
policy guidelines on the prevention and control of CVDs such as “A smoke free future: A
comprehensive tobacco control strategy for England” (DH 2010), “Be active be happy: a plan
for getting the nation moving (DH2009), Active travel strategy, Health Challenge England,
Health inequalities, etc. In the UK, the Scientific Advisory Committee on Nutrition (SACN),
a group of independent experts, advise almost all countries of the UK including England,
Scotland, and Ireland on nutrition issues that how it could affect the health of people and
causes a high level of CVDs especially Coronary (Nichols, Townsend, Scarborough, and
Rayner, 2013). The government and SACN work together to prevent the CVDs while these
bodies in order to prevent CVDs are trying to reduce the plasma total and low-density
lipoprotein (LDL) cholesterol etc. in people’s daily diet (Rees, et.al, 2013).
Policy initiatives that are geared towards tackling CVDs
The WHO and government regulatory bodies both are working on some policy and
guidelines to tackle the risk factors which is related to CVDs. The government and WHO and
some local organisations like NICE and SACN are working to improve awareness among
5
physical activity in both children and young people, primary and secondary prevention of
CVDs by cardiovascular risk assessment. NICE also focuses on the modification of blood
lipids, identifying people who are suffering from CVDs. Apart from this, NICE also provides
them appropriate medical care and tell them about the prevention control guidelines to them,
Smoking cessation services and engage the community to prevent the CVDs in England
(NICE, 2018).
The European Heart Charter (EHC) is another European health organisation that deals in
health promotion and formulates international strategies that help in the management and
detection of people at high CVD risk. The ECH is also responsible for the authorization of
the European Guidelines on Cardiovascular Disease Prevention at the country level.
Government Policy
Government policy also takes many initiatives to control the CVDs. The government is
almost taking all the corrective action and set priorities for action on nutrition, obesity and
tobacco control, and physical activities (Gylling, et.al, 2014). The government operates a
large number of an awareness program for delivering food, spread awareness among people
about the benefit of physical activities, and how prevention of tobacco and smoking can help
in cardiovascular disease control. The government publish large number of documents and
policy guidelines on the prevention and control of CVDs such as “A smoke free future: A
comprehensive tobacco control strategy for England” (DH 2010), “Be active be happy: a plan
for getting the nation moving (DH2009), Active travel strategy, Health Challenge England,
Health inequalities, etc. In the UK, the Scientific Advisory Committee on Nutrition (SACN),
a group of independent experts, advise almost all countries of the UK including England,
Scotland, and Ireland on nutrition issues that how it could affect the health of people and
causes a high level of CVDs especially Coronary (Nichols, Townsend, Scarborough, and
Rayner, 2013). The government and SACN work together to prevent the CVDs while these
bodies in order to prevent CVDs are trying to reduce the plasma total and low-density
lipoprotein (LDL) cholesterol etc. in people’s daily diet (Rees, et.al, 2013).
Policy initiatives that are geared towards tackling CVDs
The WHO and government regulatory bodies both are working on some policy and
guidelines to tackle the risk factors which is related to CVDs. The government and WHO and
some local organisations like NICE and SACN are working to improve awareness among
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Public Health
6
people about the quitting smoking and tobacco or improve the diet plan that helps in
controlling the cholesterol or blood pressure level. Although these guideline and initiatives
help the government to reduce the likelihood of developed CVDs in the country and all over
the world as well. The government and international health organisations focus on those
actions that affect the whole population and that most effectively reduce the risk factors of
CVDs.
The one of the greatest initiative taken by the WHO in collaboration with the US CDC and
other health organisations of the world is to reduce the impact of CVDs and other heart
disease problems related through work in five packages. The five packages of the World
Health Organisation contain MPOWER that is for controlling and prevention of tobacco
products. The second package talks about the ACTIVE package for focus on physical activity
among people such as exercise and Yoga. The third package is SHAKE package that focuses
on salt reduction in foods and diet. The fourth package is REPLACE that focuses on to
reduce the industrial products that includes trans fats. The last package is HEARTS package
that deals in strengthening healthcare management in all over the world to reduce and prevent
the CVDs in primary healthcare (Anderson, et.al, 2013).
The national and local organisations in the UK and England are working together within the
public sector to reduce the health inequalities and improve health among the people in the
country. The NICE guidelines help in guiding the government health care programs, the
NHS, local authorities, and industry and all those whose actions influence the health of
people and their cardiovascular health (Hobbs, et.al, 2016).
The guidance of NHS and government helps the NICE policy but does not replace the NICE
guidelines that regulate and control the use of smoking and tobacco products. However, the
NICE guidelines always work to remove these things from society because these are the
major causes of CVD (Rabar, Harker, O'Flynn, and Wierzbicki, 2014). Apart from these,
NICE guidance also tries to promote physical activity, child nutrition, proper diet,
hypertension, and standard quality products. This guidance also compliments the NICE
guidelines on alcohol misuse. The guidance on CVDs is developed based on the data
collected from the fieldwork, analysis, and step-to-step planning that is done by a large
number of people and NICE's employees (Kopel, Sidi, and Kivity, 2013).
6
people about the quitting smoking and tobacco or improve the diet plan that helps in
controlling the cholesterol or blood pressure level. Although these guideline and initiatives
help the government to reduce the likelihood of developed CVDs in the country and all over
the world as well. The government and international health organisations focus on those
actions that affect the whole population and that most effectively reduce the risk factors of
CVDs.
The one of the greatest initiative taken by the WHO in collaboration with the US CDC and
other health organisations of the world is to reduce the impact of CVDs and other heart
disease problems related through work in five packages. The five packages of the World
Health Organisation contain MPOWER that is for controlling and prevention of tobacco
products. The second package talks about the ACTIVE package for focus on physical activity
among people such as exercise and Yoga. The third package is SHAKE package that focuses
on salt reduction in foods and diet. The fourth package is REPLACE that focuses on to
reduce the industrial products that includes trans fats. The last package is HEARTS package
that deals in strengthening healthcare management in all over the world to reduce and prevent
the CVDs in primary healthcare (Anderson, et.al, 2013).
The national and local organisations in the UK and England are working together within the
public sector to reduce the health inequalities and improve health among the people in the
country. The NICE guidelines help in guiding the government health care programs, the
NHS, local authorities, and industry and all those whose actions influence the health of
people and their cardiovascular health (Hobbs, et.al, 2016).
The guidance of NHS and government helps the NICE policy but does not replace the NICE
guidelines that regulate and control the use of smoking and tobacco products. However, the
NICE guidelines always work to remove these things from society because these are the
major causes of CVD (Rabar, Harker, O'Flynn, and Wierzbicki, 2014). Apart from these,
NICE guidance also tries to promote physical activity, child nutrition, proper diet,
hypertension, and standard quality products. This guidance also compliments the NICE
guidelines on alcohol misuse. The guidance on CVDs is developed based on the data
collected from the fieldwork, analysis, and step-to-step planning that is done by a large
number of people and NICE's employees (Kopel, Sidi, and Kivity, 2013).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Public Health
7
Apart from these, there is a strong agreement among across continental, intercontinental,
international, and national guidelines that they all are working together in the prevention of
CVDs and they will guide each other to reduce the premature death and disabilities in people
that occurs because of CVD diseases (Wild, et.al, 2013). They also in an agreement and in an
international consensus among guidelines that set the goals and a priority level in the
prevention of CVD, risk factor assessment, and use of drug therapies.
Discussion and critiques
In 2003, WHO launched a first global treaty on health that was called "Framework
Convention on tobacco control (2003)" for key tobacco control measures such as increasing
the tax on tobacco products, smoke-free public places, and tobacco advertisement control etc.
(Lavigne and Karas, 2013). Although some initiatives which are taken by both national and
international organisations more effective in substantial reduction in CVD death rate. CVD is
one of the dangerous heart diseases that cause death of a large number of people, and thus it
should be essential for the government to operate different programs that help in preventing
heart diseases (Vandvik, et.al, 2012). However, measuring the impact of these programs is
debatable because of the following reasons:
1. It analyses the impact of CVD healthcare programs because it is difficult to measure
the entire cities, regions, or country.
2. Control sites become so polluted and it is not possible to implement the plan and even
measure the impact of any healthcare programs.
3. The people living in the country not adopt the changes that are required to prevent the
CVDs disease or either behaviour pattern is too slow to measure or observe any
changes (Laslett, et.al, 2013).
4. If the national and international organisation set an unexpected and unreasonable
target for people to change their behaviour, it is difficult to measure the impact of
CVDs healthcare programs.
5. If people are not adopted the guidelines or precaution measures that are required to
prevent the heart disease such as doing daily exercise, proper care in diet schedule,
not quitting smoking and tobacco, then it is difficult to measure the impact of
healthcare programs that prevent CVD (Li and Siegrist, 2012).
6. Failure to address upstream impacts such as manufacturing, commercial, or policy
practices.
7
Apart from these, there is a strong agreement among across continental, intercontinental,
international, and national guidelines that they all are working together in the prevention of
CVDs and they will guide each other to reduce the premature death and disabilities in people
that occurs because of CVD diseases (Wild, et.al, 2013). They also in an agreement and in an
international consensus among guidelines that set the goals and a priority level in the
prevention of CVD, risk factor assessment, and use of drug therapies.
Discussion and critiques
In 2003, WHO launched a first global treaty on health that was called "Framework
Convention on tobacco control (2003)" for key tobacco control measures such as increasing
the tax on tobacco products, smoke-free public places, and tobacco advertisement control etc.
(Lavigne and Karas, 2013). Although some initiatives which are taken by both national and
international organisations more effective in substantial reduction in CVD death rate. CVD is
one of the dangerous heart diseases that cause death of a large number of people, and thus it
should be essential for the government to operate different programs that help in preventing
heart diseases (Vandvik, et.al, 2012). However, measuring the impact of these programs is
debatable because of the following reasons:
1. It analyses the impact of CVD healthcare programs because it is difficult to measure
the entire cities, regions, or country.
2. Control sites become so polluted and it is not possible to implement the plan and even
measure the impact of any healthcare programs.
3. The people living in the country not adopt the changes that are required to prevent the
CVDs disease or either behaviour pattern is too slow to measure or observe any
changes (Laslett, et.al, 2013).
4. If the national and international organisation set an unexpected and unreasonable
target for people to change their behaviour, it is difficult to measure the impact of
CVDs healthcare programs.
5. If people are not adopted the guidelines or precaution measures that are required to
prevent the heart disease such as doing daily exercise, proper care in diet schedule,
not quitting smoking and tobacco, then it is difficult to measure the impact of
healthcare programs that prevent CVD (Li and Siegrist, 2012).
6. Failure to address upstream impacts such as manufacturing, commercial, or policy
practices.

Public Health
8
The one thing is considerable in CVD prevention and control policy that the causes of CVD
are the same all over the world but it has been seen that the prevention approaches of
different countries are very different from one another because of some social, cultural, and
medical reasons.
Conclusion
At the end, it can be concluded that to fight with CVD, it will be required that every country
should follow the national clinical guidelines and policy that helps in prevention and for
better control of CVD diseases. The matter of fact that some underdeveloped and developing
countries do not have proper resources, neither they have adequate finance to fight with this
type of dangerous diseases. Thus, these countries should re-prioritise their health system in
such a way that works in collaboration with the national and international policy to reduce the
burden of CVD. Since the CVDs are the global problem, the international, national, and
regional small health organisations and society of Cardiology need to collaborate together
and defining the strategy for cardiovascular prevention. It has been seen that because of some
social and cultural difference the international standards and policy is not followed by many
countries to prevent the CVD, but it is not right. All the countries and people should work in
such a way that helps them to fight with CVD and helps in reducing the premature death and
disability in people because of heart diseases.
8
The one thing is considerable in CVD prevention and control policy that the causes of CVD
are the same all over the world but it has been seen that the prevention approaches of
different countries are very different from one another because of some social, cultural, and
medical reasons.
Conclusion
At the end, it can be concluded that to fight with CVD, it will be required that every country
should follow the national clinical guidelines and policy that helps in prevention and for
better control of CVD diseases. The matter of fact that some underdeveloped and developing
countries do not have proper resources, neither they have adequate finance to fight with this
type of dangerous diseases. Thus, these countries should re-prioritise their health system in
such a way that works in collaboration with the national and international policy to reduce the
burden of CVD. Since the CVDs are the global problem, the international, national, and
regional small health organisations and society of Cardiology need to collaborate together
and defining the strategy for cardiovascular prevention. It has been seen that because of some
social and cultural difference the international standards and policy is not followed by many
countries to prevent the CVD, but it is not right. All the countries and people should work in
such a way that helps them to fight with CVD and helps in reducing the premature death and
disability in people because of heart diseases.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Public Health
9
References
Ambrosy, A.P., Fonarow, G.C., Butler, J., Chioncel, O., Greene, S.J., Vaduganathan, M.,
Nodari, S., Lam, C.S., Sato, N., Shah, A.N. and Gheorghiade, M. (2014) The global health
and economic burden of hospitalizations for heart failure: lessons learned from hospitalized
heart failure registries. Journal of the American College of Cardiology, 63(12), pp.1123-
1133.
American Heart Association (2015) Cardiovascular disease and risk
management, circulation, 131(1), pp.e29-e322.
Anderson, T.J., Grégoire, J., Hegele, R.A., Couture, P., Mancini, G.J., McPherson, R.,
Francis, G.A., Poirier, P., Lau, D.C., Grover, S. and Genest Jr, J. (2013) 2012 update of the
Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia
for the prevention of cardiovascular disease in the adult. Canadian Journal of
Cardiology, 29(2), pp.151-167.
Estruch, R., Ros, E., Salas-Salvadó, J., Covas, M.I., Corella, D., Arós, F., Gómez-Gracia, E.,
Ruiz-Gutiérrez, V., Fiol, M., Lapetra, J. and Lamuela-Raventos, R.M. (2013) Primary
prevention of cardiovascular disease with a Mediterranean diet. New England Journal of
Medicine, 368(14), pp.1279-1290.
Gansevoort, R.T., Correa-Rotter, R., Hemmelgarn, B.R., Jafar, T.H., Heerspink, H.J.L.,
Mann, J.F., Matsushita, K. and Wen, C.P. (2013) Chronic kidney disease and cardiovascular
risk: epidemiology, mechanisms, and prevention. The Lancet, 382(9889), pp.339-352.
Gielen, S. and Landmesser, U. (2014) The Year in Cardiology 2013: cardiovascular disease
prevention. European heart journal, 35(5), pp.307-312.
Gylling, H., Plat, J., Turley, S., Ginsberg, H.N., Ellegård, L., Jessup, W., Jones, P.J.,
Lütjohann, D., Maerz, W., Masana, L. and Silbernagel, G. (2014) Plant sterols and plant
stanols in the management of dyslipidaemia and prevention of cardiovascular
disease. Atherosclerosis, 232(2), pp.346-360.
Hobbs, F.D.R., Piepoli, M.F., Hoes, A.W., Agewall, S., Albus, C., Brotons, C., Catapano,
A.L., Cooney, M.T., Corra, U., Cosyns, B. and Deaton, C. (2016) 2016 European Guidelines
9
References
Ambrosy, A.P., Fonarow, G.C., Butler, J., Chioncel, O., Greene, S.J., Vaduganathan, M.,
Nodari, S., Lam, C.S., Sato, N., Shah, A.N. and Gheorghiade, M. (2014) The global health
and economic burden of hospitalizations for heart failure: lessons learned from hospitalized
heart failure registries. Journal of the American College of Cardiology, 63(12), pp.1123-
1133.
American Heart Association (2015) Cardiovascular disease and risk
management, circulation, 131(1), pp.e29-e322.
Anderson, T.J., Grégoire, J., Hegele, R.A., Couture, P., Mancini, G.J., McPherson, R.,
Francis, G.A., Poirier, P., Lau, D.C., Grover, S. and Genest Jr, J. (2013) 2012 update of the
Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia
for the prevention of cardiovascular disease in the adult. Canadian Journal of
Cardiology, 29(2), pp.151-167.
Estruch, R., Ros, E., Salas-Salvadó, J., Covas, M.I., Corella, D., Arós, F., Gómez-Gracia, E.,
Ruiz-Gutiérrez, V., Fiol, M., Lapetra, J. and Lamuela-Raventos, R.M. (2013) Primary
prevention of cardiovascular disease with a Mediterranean diet. New England Journal of
Medicine, 368(14), pp.1279-1290.
Gansevoort, R.T., Correa-Rotter, R., Hemmelgarn, B.R., Jafar, T.H., Heerspink, H.J.L.,
Mann, J.F., Matsushita, K. and Wen, C.P. (2013) Chronic kidney disease and cardiovascular
risk: epidemiology, mechanisms, and prevention. The Lancet, 382(9889), pp.339-352.
Gielen, S. and Landmesser, U. (2014) The Year in Cardiology 2013: cardiovascular disease
prevention. European heart journal, 35(5), pp.307-312.
Gylling, H., Plat, J., Turley, S., Ginsberg, H.N., Ellegård, L., Jessup, W., Jones, P.J.,
Lütjohann, D., Maerz, W., Masana, L. and Silbernagel, G. (2014) Plant sterols and plant
stanols in the management of dyslipidaemia and prevention of cardiovascular
disease. Atherosclerosis, 232(2), pp.346-360.
Hobbs, F.D.R., Piepoli, M.F., Hoes, A.W., Agewall, S., Albus, C., Brotons, C., Catapano,
A.L., Cooney, M.T., Corra, U., Cosyns, B. and Deaton, C. (2016) 2016 European Guidelines
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Public Health
10
on cardiovascular disease prevention in clinical practice. European Heart Journal, 37(29),
pp.2315-2381.
Kopel, E., Sidi, Y. and Kivity, S. (2013) Mediterranean diet for primary prevention of
cardiovascular disease. The New England journal of medicine, 369(7), p.672.
Laslett, L.J., Alagona, P., Clark, B.A., Drozda, J.P., Saldivar, F., Wilson, S.R., Poe, C. and
Hart, M. (2012) The worldwide environment of cardiovascular disease: prevalence,
diagnosis, therapy, and policy issues: a report from the American College of
Cardiology. Journal of the American College of Cardiology, 60(25 Supplement), pp.S1-S49.
Lavigne, P.M. and Karas, R.H. (2013) The current state of niacin in cardiovascular disease
prevention: a systematic review and meta-regression. Journal of the American College of
Cardiology, 61(4), pp.440-446.
Li, J. and Siegrist, J. (2012) Physical activity and risk of cardiovascular disease—a meta-
analysis of prospective cohort studies. International journal of environmental research and
public health, 9(2), pp.391-407.
NICE (2018) Cardiovascular disease and prevention [online]. Available from:
https://www.nice.org.uk/guidance/ph25/chapter/2-public-health-need-and-practice [Accessed:
08/02/2019].
Nichols, M., Townsend, N., Scarborough, P. and Rayner, M. (2013) Cardiovascular disease
in Europe: epidemiological update. European heart journal, 34(39), pp.3028-3034.
Rabar, S., Harker, M., O'Flynn, N. and Wierzbicki, A.S. (2014) Lipid modification and
cardiovascular risk assessment for the primary and secondary prevention of cardiovascular
disease: summary of updated NICE guidance. BMJ: British Medical Journal (Online), 349.
Rees, K., Hartley, L., Flowers, N., Clarke, A., Hooper, L., Thorogood, M. and Stranges, S.,
(2013) Mediterranean'dietary pattern for the primary prevention of cardiovascular
disease. Cochrane Database of Systematic Reviews, (8).
Steptoe, A. and Kivimäki, M. (2012) Stress and cardiovascular disease. Nature Reviews
Cardiology, 9(6), p.360.
Vandvik, P.O., Lincoff, A.M., Gore, J.M., Gutterman, D.D., Sonnenberg, F.A., Alonso-
Coello, P., Akl, E.A., Lansberg, M.G., Guyatt, G.H. and Spencer, F.A. (2012) Primary and
10
on cardiovascular disease prevention in clinical practice. European Heart Journal, 37(29),
pp.2315-2381.
Kopel, E., Sidi, Y. and Kivity, S. (2013) Mediterranean diet for primary prevention of
cardiovascular disease. The New England journal of medicine, 369(7), p.672.
Laslett, L.J., Alagona, P., Clark, B.A., Drozda, J.P., Saldivar, F., Wilson, S.R., Poe, C. and
Hart, M. (2012) The worldwide environment of cardiovascular disease: prevalence,
diagnosis, therapy, and policy issues: a report from the American College of
Cardiology. Journal of the American College of Cardiology, 60(25 Supplement), pp.S1-S49.
Lavigne, P.M. and Karas, R.H. (2013) The current state of niacin in cardiovascular disease
prevention: a systematic review and meta-regression. Journal of the American College of
Cardiology, 61(4), pp.440-446.
Li, J. and Siegrist, J. (2012) Physical activity and risk of cardiovascular disease—a meta-
analysis of prospective cohort studies. International journal of environmental research and
public health, 9(2), pp.391-407.
NICE (2018) Cardiovascular disease and prevention [online]. Available from:
https://www.nice.org.uk/guidance/ph25/chapter/2-public-health-need-and-practice [Accessed:
08/02/2019].
Nichols, M., Townsend, N., Scarborough, P. and Rayner, M. (2013) Cardiovascular disease
in Europe: epidemiological update. European heart journal, 34(39), pp.3028-3034.
Rabar, S., Harker, M., O'Flynn, N. and Wierzbicki, A.S. (2014) Lipid modification and
cardiovascular risk assessment for the primary and secondary prevention of cardiovascular
disease: summary of updated NICE guidance. BMJ: British Medical Journal (Online), 349.
Rees, K., Hartley, L., Flowers, N., Clarke, A., Hooper, L., Thorogood, M. and Stranges, S.,
(2013) Mediterranean'dietary pattern for the primary prevention of cardiovascular
disease. Cochrane Database of Systematic Reviews, (8).
Steptoe, A. and Kivimäki, M. (2012) Stress and cardiovascular disease. Nature Reviews
Cardiology, 9(6), p.360.
Vandvik, P.O., Lincoff, A.M., Gore, J.M., Gutterman, D.D., Sonnenberg, F.A., Alonso-
Coello, P., Akl, E.A., Lansberg, M.G., Guyatt, G.H. and Spencer, F.A. (2012) Primary and
Public Health
11
secondary prevention of cardiovascular disease: antithrombotic therapy and prevention of
thrombosis: American College of Chest Physicians evidence-based clinical practice
guidelines. Chest, 141(2), pp.e637S-e668S.
WHO (2018) Action Plan for the Prevention and Control of Noncommunicable Diseases in
the WHO European Region 2016–2025 [online]. Available from:
http://www.euro.who.int/en/health-topics/noncommunicable-diseases/cardiovascular-
diseases/publications/2016/action-plan-for-the-prevention-and-control-of-noncommunicable-
diseases-in-the-who-european-region-20162025 [Accessed: 10/02/2019].
WHO (2018) Cardiovascular disease [online]. Available from:
http://www.euro.who.int/en/health-topics/noncommunicable-diseases/cardiovascular-
diseases/cardiovascular-diseases2 [Available from: 09/02/2019].
WHO (2018) Global Hearts Initiative, working together to promote cardiovascular health
[online]. Available from: https://www.who.int/cardiovascular_diseases/global-hearts/en/
[Accessed: 10/02/2019].
Wild, R.A., Wu, C., Curb, J.D., Martin, L.W., Phillips, L., Stefanick, M., Trevisan, M. and
Manson, J.E. (2013) Coronary heart disease events in the Women's Health Initiative hormone
trials: effect modification by metabolic syndrome: A nested case-control study within the
Women's Health Initiative randomized clinical trials. Menopause (New York, NY), 20(3),
pp.254-260.
Yusuf, S., Wood, D., Ralston, J. and Reddy, K.S. (2015) The World Heart Federation's vision
for worldwide cardiovascular disease prevention. The Lancet, 386(9991), pp.399-402.
11
secondary prevention of cardiovascular disease: antithrombotic therapy and prevention of
thrombosis: American College of Chest Physicians evidence-based clinical practice
guidelines. Chest, 141(2), pp.e637S-e668S.
WHO (2018) Action Plan for the Prevention and Control of Noncommunicable Diseases in
the WHO European Region 2016–2025 [online]. Available from:
http://www.euro.who.int/en/health-topics/noncommunicable-diseases/cardiovascular-
diseases/publications/2016/action-plan-for-the-prevention-and-control-of-noncommunicable-
diseases-in-the-who-european-region-20162025 [Accessed: 10/02/2019].
WHO (2018) Cardiovascular disease [online]. Available from:
http://www.euro.who.int/en/health-topics/noncommunicable-diseases/cardiovascular-
diseases/cardiovascular-diseases2 [Available from: 09/02/2019].
WHO (2018) Global Hearts Initiative, working together to promote cardiovascular health
[online]. Available from: https://www.who.int/cardiovascular_diseases/global-hearts/en/
[Accessed: 10/02/2019].
Wild, R.A., Wu, C., Curb, J.D., Martin, L.W., Phillips, L., Stefanick, M., Trevisan, M. and
Manson, J.E. (2013) Coronary heart disease events in the Women's Health Initiative hormone
trials: effect modification by metabolic syndrome: A nested case-control study within the
Women's Health Initiative randomized clinical trials. Menopause (New York, NY), 20(3),
pp.254-260.
Yusuf, S., Wood, D., Ralston, J. and Reddy, K.S. (2015) The World Heart Federation's vision
for worldwide cardiovascular disease prevention. The Lancet, 386(9991), pp.399-402.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.