Cerebrovascular Disease Analysis Report
Added on 2022-08-23
8 Pages2282 Words25 Views
Student number:
Mrs. Gwen Boren (80yo) is a patient in your ward.
You receive handover at the start of an early shift.
"Mrs. Boren lives at Sunnivale Nursing Home. At about 0200 this morning, she was found on the floor. The report from the home states
that she wasn't able to explain what happened, and she was rather confused. She was brought in by ambulance.
Mrs. Boren has a history of a cerebrovascular accident with a mild right-sided physical deficit, but no cognitive impairment. She also is
managed for atrial fibrillation. She uses a walking frame to get around.
She had a head CT which noted no further changes.”
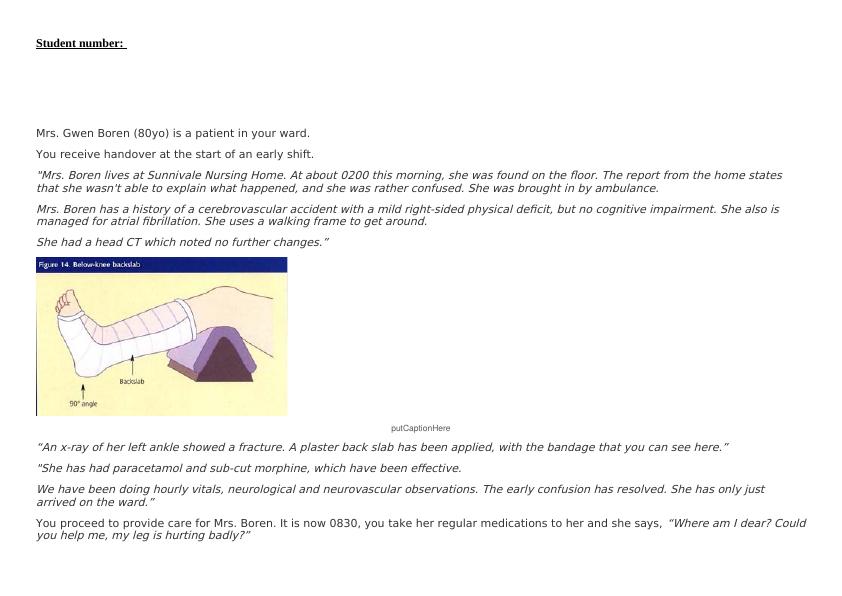
putCaptionHere
“An x-ray of her left ankle showed a fracture. A plaster back slab has been applied, with the bandage that you can see here.”
"She has had paracetamol and sub-cut morphine, which have been effective.
We have been doing hourly vitals, neurological and neurovascular observations. The early confusion has resolved. She has only just
arrived on the ward.”
You proceed to provide care for Mrs. Boren. It is now 0830, you take her regular medications to her and she says,
“Where am I dear? Could
you help me, my leg is hurting badly?”
Mrs. Gwen Boren (80yo) is a patient in your ward.
You receive handover at the start of an early shift.
"Mrs. Boren lives at Sunnivale Nursing Home. At about 0200 this morning, she was found on the floor. The report from the home states
that she wasn't able to explain what happened, and she was rather confused. She was brought in by ambulance.
Mrs. Boren has a history of a cerebrovascular accident with a mild right-sided physical deficit, but no cognitive impairment. She also is
managed for atrial fibrillation. She uses a walking frame to get around.
She had a head CT which noted no further changes.”
putCaptionHere
“An x-ray of her left ankle showed a fracture. A plaster back slab has been applied, with the bandage that you can see here.”
"She has had paracetamol and sub-cut morphine, which have been effective.
We have been doing hourly vitals, neurological and neurovascular observations. The early confusion has resolved. She has only just
arrived on the ward.”
You proceed to provide care for Mrs. Boren. It is now 0830, you take her regular medications to her and she says,
“Where am I dear? Could
you help me, my leg is hurting badly?”
You undertake observations
CNA253 AT2 Scenario: Mrs. Gwen Boren
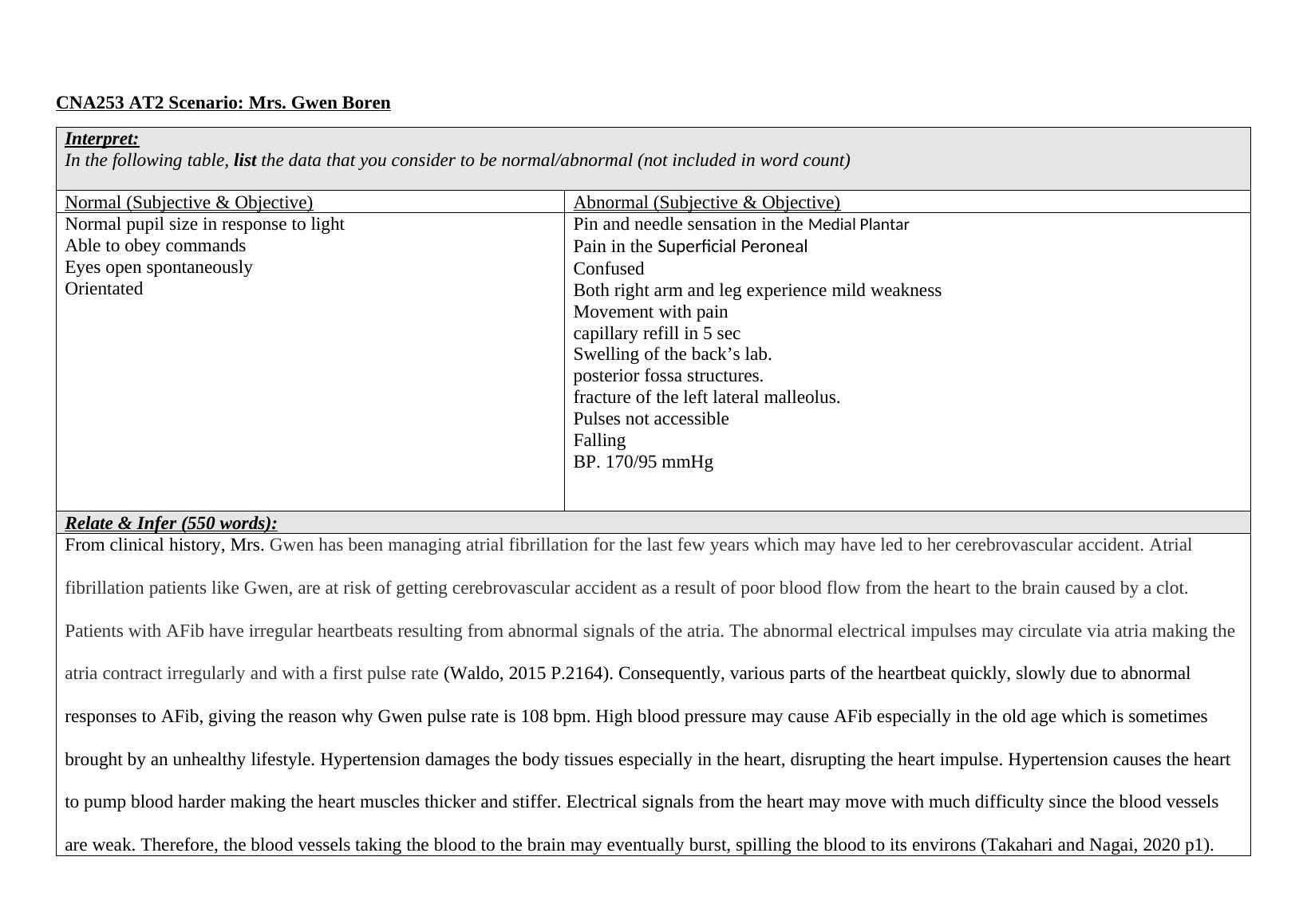
Interpret:
In the following table, list the data that you consider to be normal/abnormal (not included in word count)
Normal (Subjective & Objective) Abnormal (Subjective & Objective)
Normal pupil size in response to light
Able to obey commands
Eyes open spontaneously
Orientated
Pin and needle sensation in the Medial Plantar
Pain in the Superficial Peroneal
Confused
Both right arm and leg experience mild weakness
Movement with pain
capillary refill in 5 sec
Swelling of the back’s lab.
posterior fossa structures.
fracture of the left lateral malleolus.
Pulses not accessible
Falling
BP. 170/95 mmHg
Relate & Infer (550 words):
From clinical history, Mrs. Gwen has been managing atrial fibrillation for the last few years which may have led to her cerebrovascular accident. Atrial
fibrillation patients like Gwen, are at risk of getting cerebrovascular accident as a result of poor blood flow from the heart to the brain caused by a clot.
Patients with AFib have irregular heartbeats resulting from abnormal signals of the atria. The abnormal electrical impulses may circulate via atria making the
atria contract irregularly and with a first pulse rate (Waldo, 2015 P.2164). Consequently, various parts of the heartbeat quickly, slowly due to abnormal
responses to AFib, giving the reason why Gwen pulse rate is 108 bpm. High blood pressure may cause AFib especially in the old age which is sometimes
brought by an unhealthy lifestyle. Hypertension damages the body tissues especially in the heart, disrupting the heart impulse. Hypertension causes the heart
to pump blood harder making the heart muscles thicker and stiffer. Electrical signals from the heart may move with much difficulty since the blood vessels
CNA253 AT2 Scenario: Mrs. Gwen Boren
Interpret:
In the following table, list the data that you consider to be normal/abnormal (not included in word count)
Normal (Subjective & Objective) Abnormal (Subjective & Objective)
Normal pupil size in response to light
Able to obey commands
Eyes open spontaneously
Orientated
Pin and needle sensation in the Medial Plantar
Pain in the Superficial Peroneal
Confused
Both right arm and leg experience mild weakness
Movement with pain
capillary refill in 5 sec
Swelling of the back’s lab.
posterior fossa structures.
fracture of the left lateral malleolus.
Pulses not accessible
Falling
BP. 170/95 mmHg
Relate & Infer (550 words):
From clinical history, Mrs. Gwen has been managing atrial fibrillation for the last few years which may have led to her cerebrovascular accident. Atrial
fibrillation patients like Gwen, are at risk of getting cerebrovascular accident as a result of poor blood flow from the heart to the brain caused by a clot.
Patients with AFib have irregular heartbeats resulting from abnormal signals of the atria. The abnormal electrical impulses may circulate via atria making the
atria contract irregularly and with a first pulse rate (Waldo, 2015 P.2164). Consequently, various parts of the heartbeat quickly, slowly due to abnormal
responses to AFib, giving the reason why Gwen pulse rate is 108 bpm. High blood pressure may cause AFib especially in the old age which is sometimes
brought by an unhealthy lifestyle. Hypertension damages the body tissues especially in the heart, disrupting the heart impulse. Hypertension causes the heart
to pump blood harder making the heart muscles thicker and stiffer. Electrical signals from the heart may move with much difficulty since the blood vessels
are weak. Therefore, the blood vessels taking the blood to the brain may eventually burst, spilling the blood to its environs (Takahari and Nagai, 2020 p1).
The bursting of the arteries in the brain causes a hemorrhagic stroke. From the health history of Mrs. Gwen, she might have had a long experience with
hypertension which led to AFib and consequently cerebrovascular accident. Patients suffering from atrial fibrillation are more susceptible to get high blood
pressure since the conditions go hand in hand, the reason why Mrs. Gwen may be experiencing a blood pressure of BP: 170/95 mmHg. At 0200 Mrs. Bolean
was found on the floor and was unable to tell what happened. Falls are common to patients with cerebrovascular accidents, especially in adults in their old
age (Cho, Yu, and Rhee, 2015 p. 1751) which inhibits their ability in performing personal activities. Mrs. Gwen feels pain in the superficial peroneal. It is
most likely Mrs. Gwen might have contracted compartment syndrome which may have been brought by the fracture of the foot. The pain sensation of the
foot could be a result of tissue pressure exceeds the perfusion pressure of the blood vessels supplying the blood, which later results in ischemia of both the
nerves and muscles. When Mrs. Gwen fell, she broke her ankle which is vivid from the x-ray. Ankle open fractures are the main contributors to acute
compartment syndrome. Pain is the first sign of acute compartment syndrome. A deep posterior compartment will certainly increase the pain due to the
stretching of the affected muscles (Kiel, and Kaiser, 2019 P.1). swelling is also a sign of an acute compartment. Compartment syndrome occurs when there is
swelling in a compartment. When fascia doesn't stretch, it increases pressure in the nerves or capillaries and hence blood can not penetrate through to
transport the oxygen and nutrients to the affected area. If the condition is not treated, muscles may eventually die. From our case scenario, a plaster back slab
has been applied with the bandage to help reduce the swelling and enhance the healing process of the fracture. Due to the pressure exerted in the blood
vessels, they are unable to transport sufficient blood to the tissues, consequently, the lab tests indicate a capillary refill in 5 sec (Islam and Robbs, 2015 p.53).
Physical therapy may be very significant in reducing of compartment syndrome. Normal physical activities should be modified as they allow body physical
fitness, allow proper blood circulation and thereby reducing the risks of the compartment. Alternatively, massage may be effective in reducing moderate
compartment syndrome
The bursting of the arteries in the brain causes a hemorrhagic stroke. From the health history of Mrs. Gwen, she might have had a long experience with
hypertension which led to AFib and consequently cerebrovascular accident. Patients suffering from atrial fibrillation are more susceptible to get high blood
pressure since the conditions go hand in hand, the reason why Mrs. Gwen may be experiencing a blood pressure of BP: 170/95 mmHg. At 0200 Mrs. Bolean
was found on the floor and was unable to tell what happened. Falls are common to patients with cerebrovascular accidents, especially in adults in their old
age (Cho, Yu, and Rhee, 2015 p. 1751) which inhibits their ability in performing personal activities. Mrs. Gwen feels pain in the superficial peroneal. It is
most likely Mrs. Gwen might have contracted compartment syndrome which may have been brought by the fracture of the foot. The pain sensation of the
foot could be a result of tissue pressure exceeds the perfusion pressure of the blood vessels supplying the blood, which later results in ischemia of both the
nerves and muscles. When Mrs. Gwen fell, she broke her ankle which is vivid from the x-ray. Ankle open fractures are the main contributors to acute
compartment syndrome. Pain is the first sign of acute compartment syndrome. A deep posterior compartment will certainly increase the pain due to the
stretching of the affected muscles (Kiel, and Kaiser, 2019 P.1). swelling is also a sign of an acute compartment. Compartment syndrome occurs when there is
swelling in a compartment. When fascia doesn't stretch, it increases pressure in the nerves or capillaries and hence blood can not penetrate through to
transport the oxygen and nutrients to the affected area. If the condition is not treated, muscles may eventually die. From our case scenario, a plaster back slab
has been applied with the bandage to help reduce the swelling and enhance the healing process of the fracture. Due to the pressure exerted in the blood
vessels, they are unable to transport sufficient blood to the tissues, consequently, the lab tests indicate a capillary refill in 5 sec (Islam and Robbs, 2015 p.53).
Physical therapy may be very significant in reducing of compartment syndrome. Normal physical activities should be modified as they allow body physical
fitness, allow proper blood circulation and thereby reducing the risks of the compartment. Alternatively, massage may be effective in reducing moderate
compartment syndrome
End of preview
Want to access all the pages? Upload your documents or become a member.
Related Documents
Normal/Abnormal Data in the Physical Conditionslg...
|6
|2240
|18
The Professional Practicelg...
|11
|1939
|18
Case study of chronic systolic heart failure of a diabetic female studentlg...
|10
|2559
|207
Compartment Syndrome and its Treatmentlg...
|5
|2418
|31
What do you consider to be normal/abnormal?lg...
|6
|2541
|15
Case Study Essay on Acute Exacerbation of Chronic Heart Failurelg...
|7
|2040
|269