Chronic Illness Management - Strategies, Treatment, and Complications
VerifiedAdded on 2023/06/10
|9
|1779
|330
AI Summary
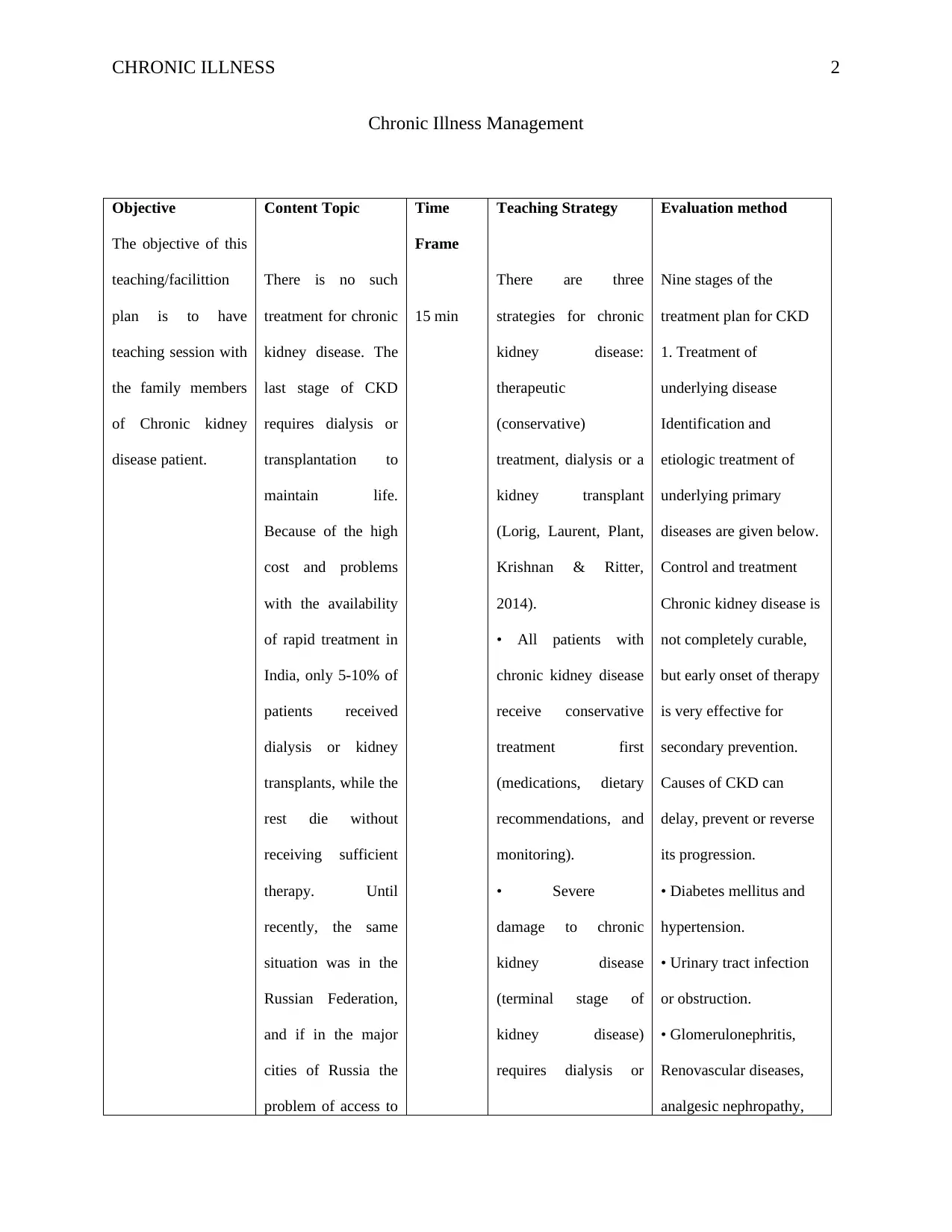
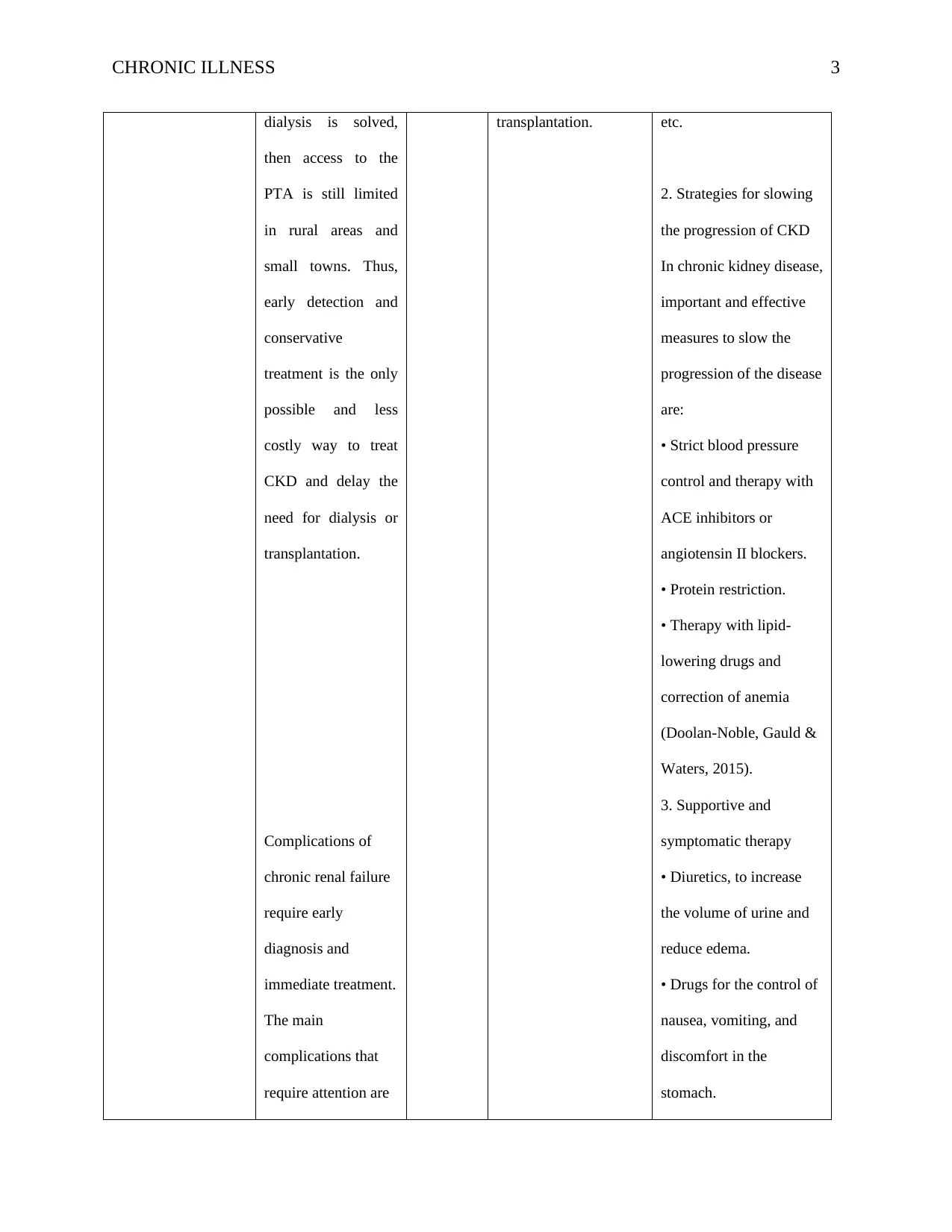
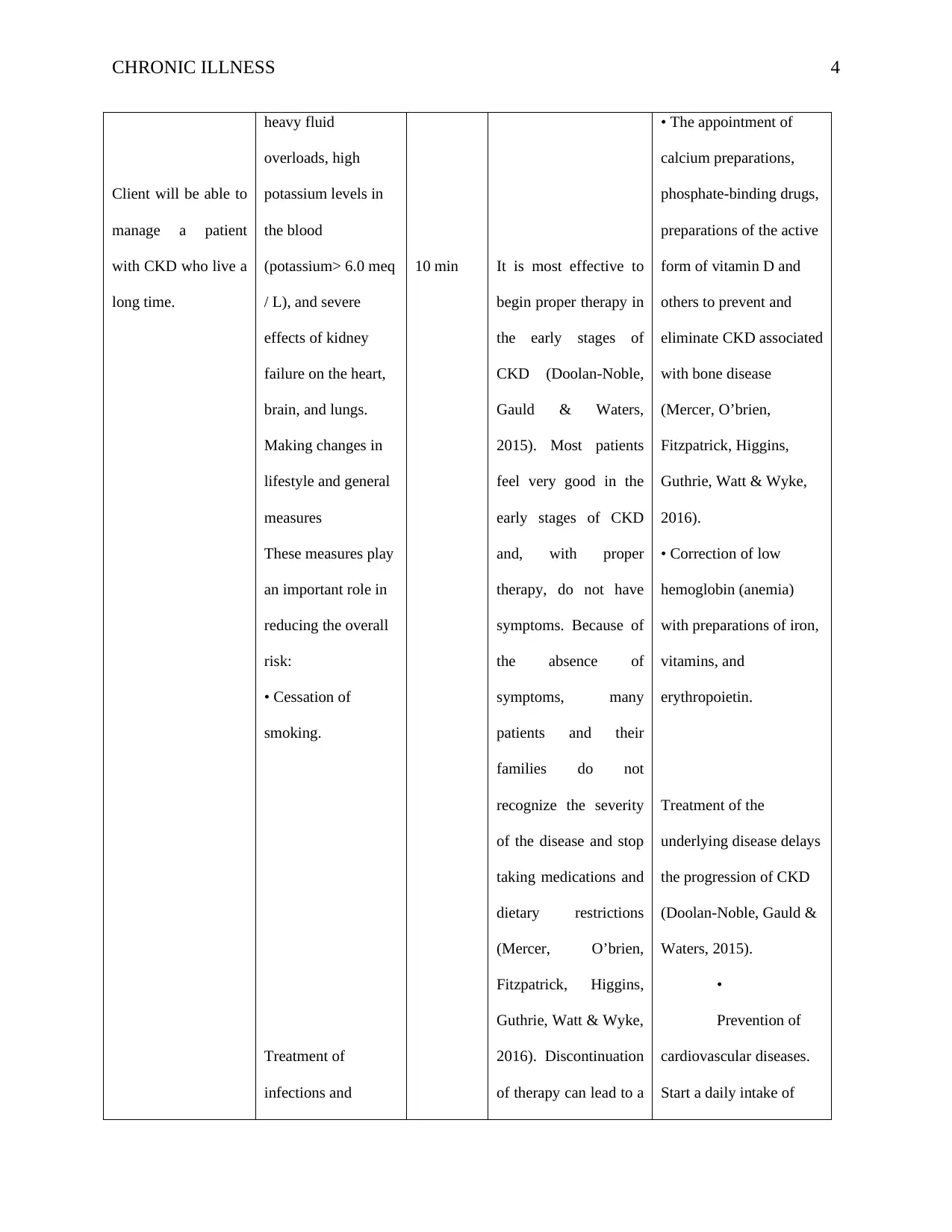
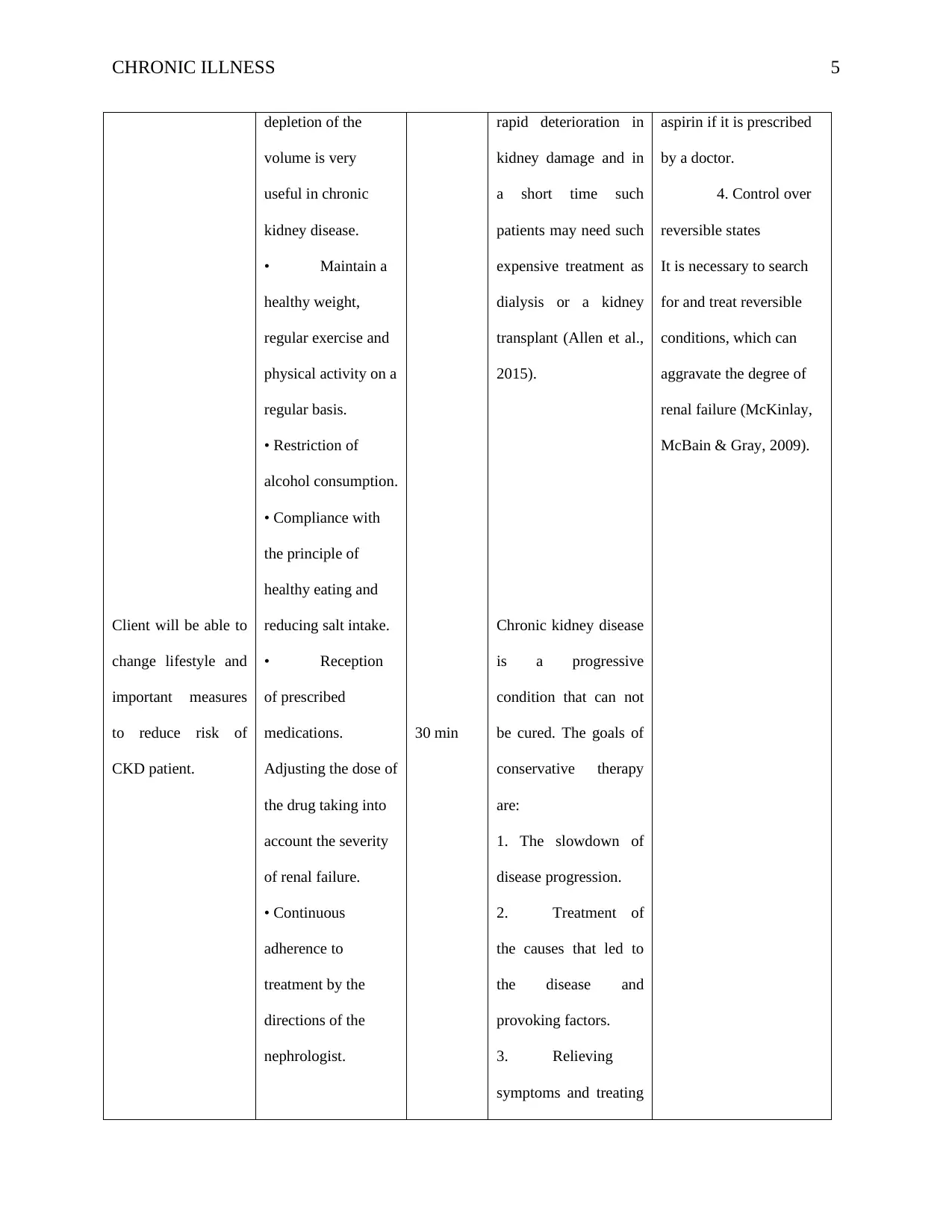
This teaching session covers chronic illness management, including strategies for slowing disease progression, treatment options, and complications. It focuses on chronic kidney disease, discussing the different stages and the dietary restrictions required. The session also covers the complications that require immediate attention and the importance of early diagnosis and treatment. The teaching sources used include studies on fragmented care, whole-person illness, and the development of primary care-based interventions for patients with multimorbidity.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.


1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.